Embed Size (px)
Citation preview

L
PRa
b
c
a
ARRAA
KISCG
1
tctieircO1bdM2a2aLn
H
0d
Neuropsychologia 47 (2009) 2866–2875
Contents lists available at ScienceDirect
Neuropsychologia
journa l homepage: www.e lsev ier .com/ locate /neuropsychologia
esion neuroanatomy of the Sustained Attention to Response task
ascal Molenberghs a, Céline R. Gillebert a, Hanne Schoofs b, Patrick Dupont a,onald Peeters c, Rik Vandenberghe a,b,∗
Cognitive Neurology Laboratory, Experimental Neurology Section, K.U. Leuven, BelgiumNeurology Department, University Hospitals Leuven, Herestraat 49, 3000 Leuven, BelgiumRadiology Department, University Hospitals Leuven, Herestraat 49, 3000 Leuven, Belgium
r t i c l e i n f o
rticle history:eceived 19 February 2009eceived in revised form 20 May 2009ccepted 14 June 2009vailable online 21 June 2009
a b s t r a c t
The Sustained Attention to Response task is a classical neuropsychological test that has been used by manycentres to characterize the attentional deficits in traumatic brain injury, ADHD, autism and other disorders.During the SART a random series of digits 1–9 is presented repeatedly and subjects have to respond toeach digit (go trial) except the digit ‘3’ (no-go trial). Using voxel-based lesion symptom mapping (VLSM) in
eywords:nferior frontaltrokeognitive controlo no-go
a consecutive series of 44 ischemic unifocal non-lacunar hemispheric stroke patients we determined theneuroanatomy of 4 SART parameters: commission and omission error rate, reaction time variability andpost-error slowing. Lesions of the right inferior frontal gyrus significantly increased commission errorrate. Lesions of the middle third of the right inferior frontal sulcus (IFS) reduced post-error slowing, ameasure of how well subjects can utilize errors to adjust cognitive resource allocation. Omissions andreaction time variability had less localising value in our sample. To conclude, commission errors and
SART
post-error slowing in the. Introduction
The Sustained Attention to Response task (SART) is a conven-ional neuropsychological test for sustained attention and cognitiveontrol (Robertson, Manly, Andrade, Baddeley, & Yiend, 1997). Inhe original version sequences of digits 1–9 are visually presentedn random order up to 25 times and subjects have to respond toach digit except for the digit ‘3’. The SART differs from typical vig-lance tasks in being relatively short and in requiring very frequentesponses and rare withholding of responses. It differs from typi-al go no-go task by the disproportion of go trials over no-go trials.ver the past 15 years, the SART (Robertson, Manly, Andrade, et al.,997) has been intensively used in children and adults by a num-er of centres to analyze the attentional deficits arising in frequentisorders such as traumatic brain injury (Chan, 2001; Robertson,anly, Andrade, et al., 1997; Whyte, Grieb-Neff, Gantz, & Polanksy,
006), ADHD (Belgrove, Hawi, Gill, & Robertson, 2006; Johnson etl., 2007; Shallice, Marzocchi, Coser, DelSavio, Meuter, & Rumiati,
002), and autism (Johnson et al., 2007). The SART has been useds an outcome measure for therapy (O’Connell, Bellgrove, Dockree,au, Fitzgerald, & Robertson, 2008) and also to define an endophe-otype for studying the genetics of attention (Greene, Bellgrove,∗ Corresponding author at: Neurology Department, University Hospitals Leuven,erestraat 49, 3000 Leuven, Belgium. Tel.: +32 16 344280; fax: +32 16 3444285.
E-mail address: [email protected] (R. Vandenberghe).
028-3932/$ – see front matter © 2009 Elsevier Ltd. All rights reserved.oi:10.1016/j.neuropsychologia.2009.06.012
mainly probe right inferior frontal integrity.© 2009 Elsevier Ltd. All rights reserved.
Gill, & Robertson, 2009). The neuroanatomy and electrophysiol-ogy has been studied in cognitively intact volunteers by meansof functional imaging (Fassbender et al., 2004; Manly et al., 2003)and evoked potentials (Zordan, Sarlo, & Stablum, 2008). One ele-ment however that is lacking at the moment is a validation interms of brain lesion neuroanatomy. We prospectively recruited aconsecutive series of non-lacunar hemispheric stroke patients inde-pendently of lesion site to determine the cognitive neuroanatomyof the SART. In a voxel-based manner we aimed to define whichbrain regions are critically implicated in the SART using a similarapproach as we have applied in previous studies of spatial atten-tional deficits (Molenberghs, Gillebert, Peeters, & Vandenberghe,2008).
Different behavioral measures that capture different aspects ofsustained attention and cognitive control can be derived from theSART. SART omission errors and reaction time variability likelyrelate to the ability to sustain attention across trials (Stuss, Shallice,Alexander, & Picton, 1995; Wilkins, Shallice, & McCarthy, 1987).Compared to more typical vigilance tasks which have a low targetfrequency, the SART can pick up lapses of attention in a sensitiveway thanks to the high target frequency allowing to monitor theattentional level nearly continuously during the entire task course.
These fluctuations will be manifest as increased reaction time vari-ability or, if they are more severe, response omissions. Commissionerrors in the SART may also reflect a sustained attention prob-lem: when subjects fail to maintain the task goal on-line (Braver,Reynolds, & Donaldson, 2003; Duncan, Emslie, & Williams, 1996),
psycho
amrrioec1tirfiveaaidietFibl(Dmt
pmSeMsmilanuTRJpti1pewMRG
cmisN2tfO
P. Molenberghs et al. / Neuro
n automatic response mode driven by the highly frequent go trialsay start to dominate behavior and subjects may neglect the task
equirement of perceptual identification of the digit prior to a goesponse decision. Alternatively, commission errors may arise frommpaired inhibitory control (Drewe, 1975): subjects may be awaref the task goal but the time needed to identify the stimulus mayxceed the period of time during which the prepotent go responsean be stopped (Aron, Robbins, & Poldrack, 2004; Logan & Cowan,984). Behaviorally, it is challenging to discriminate between thesewo accounts. Manly et al. (2003) introduced a variant of the SARTn which digits are presented in a fixed series of 1–9 rather than in aandom sequence (Manly et al., 2003), increasing predictability. Thexed version is more sensitive to frontal damage than the randomersion (Manly et al., 2003). During the fixed version a commissionrror is more typically preceded by electrophysiological markers offailure to maintain the task goal on-line (Braver et al., 2003), suchs increased alpha synchronization or a diminished late positiv-ty potential (O’Connell et al., 2008). In contrast, commission errorsuring the random version of the SART are associated with a dimin-
shed inhibitory event-related potential (ERP) complex (O’Connellt al., 2008), indicative of a problem at the level of inhibitory con-rol. A fourth measure of interest, post-error slowing (Fellows &arah, 2005; Picton et al., 2007; Rabbitt, 1966), reflects the abil-ty to adjust cognitive resources on-line when a mismatch occursetween actual outcome and task goal. Changes in this feedback
oop may arise at the level of error evaluation or error utilizationKonow & Pribram, 1970; Scheffers, Coles, Bernstein, Gehring, &onchin, 1996; Stuss et al., 1995). Alternatively, post-error slowingay also reflect a ‘hangover’ from erroneous processes engaged in
he previous trial.From paradigms that resemble the SART we derived a couple of a
riori hypotheses. On the go no-go paradigm frontal patients makeore commission errors than non-frontal patients (Alexander,
tuss, Picton, Shallice, & Gillingham, 2007; Drewe, 1975; Pictont al., 2007) and show increased response time variability (Stuss,urphy, Binns, & Alexander, 2003). A related paradigm, the stop-
ignal reaction time (SSRT) (Logan & Cowan, 1984) paradigm,easures the ability to interrupt a planned motor response. SSRT
s increased in patients with lesions of the right frontal opercu-um (Aron, Fletcher, Bullmore, Sahakian, & Robbins, 2003; Aron etl., 2004). Regions outside prefrontal cortex may also contribute:eglect patients are impaired on tasks that require the detection ofnfrequent targets in an auditory stream of distracters (Hjaltason,egner, Tham, Levander, & Ericson, 1996; Husain & Rorden, 2003;obertson, Manly, Beschin, et al., 1997; Samuelsson, Hjelmquist,
ensen, Ekholm, & Blomstrand, 1998), similarly to prefrontal lesionatients (Richer & Lepage, 1996; Wilkins et al., 1987). The atten-ional dwell time, a measure of cognitive resource allocation, is alsoncreased in neglect patients (Husain, Shapiro, Martin, & Kennard,997). Since neglect is most often associated with right inferiorarietal lesions, this suggested to us that the right inferior pari-tal lobule contributes to SART performance in addition to itsell-established role in spatial attention (Husain & Rorden, 2003;ennemeier et al., 1994; Robertson, Manly, Beschin, et al., 1997;
obertson, Mattingley, Rorden, & Driver, 1998; Vandenberghe,itelman, Parrish, & Mesulam, 2001).
Functional magnetic resonance imaging (fMRI) experiments ofognitive control in healthy volunteers provide an anatomicallyore refined and more complicated picture than the lesion stud-
es. fMRI studies implicate the junction between the inferior frontalulcus (IFS) and the inferior precentral sulcus (IFJ) (Derrfuss, Brass,
eumann, & von Cramon, 2005; Hon, Epstein, Owen, & Duncan,006; Nakahara, Hayashi, Konishi, & Miyashita, 2002), the middlehird of the IFS (Derrfuss et al., 2005; Duncan & Owen, 2000), therontal operculum extending into the anterior insula (Duncan &wen, 2000), the dorsolateral prefrontal cortex (McDonald, Cohen,logia 47 (2009) 2866–2875 2867
Stenger, & Carter, 2000; Sohn, Ursu, Anderson, Stenger, & Carter,2000) and the anterior cingulate (Botvinick, Nystrom, Fissell, Carter,& Cohen, 1999; Carter et al., 1998; Duncan & Owen, 2000; Kerns etal., 2004; McDonald et al., 2000) in different cognitive control pro-cesses. fMRI studies of response inhibition have often found theright inferior frontal gyrus (IFG) to be part of an extensive networkthat includes IFS, anterior cingulate (Konishi et al., 1999; Konishi,Nakajima, Uchida, Sekihara, & Miyashita, 1998) and also the inferiorparietal lobule (Bunge, Dudukovic, Thomason, Vaidya, & Gabrieli,2002; Fassbender et al., 2004; Garavan, Ross, & Stein, 1999), partic-ularly in case of go no-go compared to SSRT tasks (Garavan et al.,1999; Rubia et al., 2001).
In the majority of previous lesion studies of cognitive control,lesions were classified using a region-based template (Alexanderet al., 2007; Alexander, Stuss, Shallice, Picton, & Gillingham, 2005;Aron et al., 2003, 2004; Drewe, 1975; Fellows & Farah, 2005; Pictonet al., 2007; Wilkins et al., 1987). The functional demarcationshowever within prefrontal cortex cannot be directly derived fromstructural anatomical boundaries (Stuss et al., 1995). Voxel-basedlesion-symptom mapping (VLSM) allows one to quantify a deficiton a continuous scale and relate the degree of impairment to lesionsite in a voxelwise manner (Bates et al., 2003; Rorden, Karnath,& Bonilha, 2007) without need for an a priori region-based tem-plate. VLSM provides coordinates of critical lesion sites that can bedirectly compared to those obtained using fMRI in healthy volun-teers (Molenberghs et al., 2008).
We examined which SART parameters are linked to specificcortical lesion sites (Husain & Rorden, 2003; Robertson, Manly,Andrade, et al., 1997; Robertson et al., 1998). We predicted thatapart from prefrontal cortex, the inferior parietal lobule would alsobe involved (Garavan et al., 1999; Hjaltason et al., 1996; Robertson,Manly, Andrade, et al., 1997; Rubia et al., 2001; Samuelsson et al.,1998).
2. Methods
2.1. Subjects
All participants gave written informed consent in accordance with the Declara-tion of Helsinki. The ethical commission, University Hospitals Leuven, approved theexperimental protocol.
We screened a consecutive series of 616 ischemic stroke patients during theirhospitalization at the stroke unit or on occasion of their first follow-up visit to theoutpatient clinic. Fifty-six of these patients fulfilled the study criteria, 44 of whomconsented to the study (Table 1). All participants had suffered a recent non-lacunarunifocal ischemic hemispheric stroke, confirmed on clinical Fluid Attenuation Inver-sion Recovery (FLAIR) or Diffusion-Weighted Imaging (DWI) magnetic resonanceimaging (MRI). Patients were recruited via the acute stroke unit (n = 29) or via theirfirst follow-up visit to the outpatient stroke clinic (n = 15). Twenty of the patientsalso participated in a study of spatial attention reported previously (Molenberghset al., 2008). Exclusion criteria were age above 85 years, pre-existing periventricu-lar or subcortical white matter lesions or a pre-existing stroke on MRI, insufficientbalance to sit autonomously and general inability to understand and carry out acomputerized task. The anatomical distribution of the ischemic lesions is shown inFig. 1. Visual fields were intact except in case 10 (left hemianopia), 14 (right lowerquadrantanopia), 15 (left upper quadrantanopia) and 32 (left lower quadrantanopia).
A control group of 19 healthy subjects (10 women), aged between 51 and 73years (mean 61.2 years, S.D. 7.1) underwent the same protocol.
2.2. Stimuli and tasks
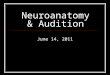
Subjects were seated at 114 cm distance from a 19 in. computer screen. UsingSuperlab for PC version 2.0 (Cedrus, Phoenix, AR, USA) each of nine digits was foveallypresented 25 times in pseudorandom order over a total period of 4.3 min (Fig. 2). Inthe version used in the current study the digits were randomized across the entirerun rather than per sequences of 1–9. Each digit (luminance = 105 cd/m2) was pre-sented for 250 ms on a black background, followed by a 900 ms white mask, after
which the next trial started immediately. This resulted in a total task duration of4 min 19 s. The mask consisted of a ring (diameter = 5.51◦; width = 105 cd/m2) witha diagonal cross in the middle. The digits were presented in one of five randomlyallocated font sizes (48, 72, 94, 100 or 120 points symbol font size; height rang-ing between 2.28 and 5.51 visual degrees). Subjects were instructed to respond toeach digit with a key press (response box from Cedrus, Phoenix, AR, USA) except to
2868 P. Molenberghs et al. / Neuropsychologia 47 (2009) 2866–2875
Table 1Behavioral parameters
Case Age Side Size (cm3) Time (days) Bells Bisection (%) Sustained Attention to Response task
L/M/R comm./25 omiss./200 post (ms) mean RT (ms) S.D./mean (ms)
1 43 R 26.9 4 0/0/1 +5.8 2 6 105 408 0.232 82 R 20.2 5 1/0/0 +3.7 5 12 288 526 0.343 44 R 302.7 4 1/0/1 −5.3 8 2 −20 485 0.174 69 L 19.0 6 0/0/0 +0.7 7 10 276 473 0.385 53 L 108.0 4 3/0/3 +4.1 12 4 −45 580 0.156 88 R 84.1 7 2/2/4 +8.1 2 3 31 655 0.157 72 L 46.8 3 2/4/0 −1.7 1 8 114 704 0.278 65 R 17.0 5 2/0/0 +5.8 2 1 7 414 0.359 80 R 29.8 6 0/0/0 +1.2 3 17 94 508 0.34
10 74 R 173.0 6 14/0/1 +20.5 3 2 117 363 0.2511 73 L 16.4 4 0/0/0 −0.3 6 15 8 625 0.3212 79 L 4.8 3 2/1/1 +1.9 9 5 62 471 0.2113 79 L 2.1 6 0/0/1 +1.7 7 5 −37 638 0.2114 47 L 13.9 5 0/1/0 +3.8 3 3 124 647 0.1915 52 R 14.3 147 2/1/0 −5.9 7 20 51 415 0.2516 68 R 11.0 154 0/0/0 −3.0 2 23 79 486 0.3117 64 R 216.0 5 15/4/2 +18.4 8 2 38 539 0.1718 79 R 191.0 4 15/4/0 +33.4 6 8 −19 465 0.2019 75 R 15.4 3 2/1/0 +1.2 8 12 −16 308 0.1520 74 R 117.0 7 0/0/1 −1.7 1 3 81 581 0.1521 84 L 12.5 6 0/0/0 +9.6 5 10 −47 400 0.2022 61 L 1.0 217 0/0/0 +2.0 5 2 21 423 0.2023 37 L 11.2 21 0/0/0 +0.4 7 5 47 346 0.1624 76 L 4.0 5 1/1/2 +4.6 5 2 101 558 0.1625 79 R 40.8 14 2/1/1 −3.8 2 4 94 625 0.1326 65 R 49.5 10 1/1/1 +4.0 0 1 no errors 501 0.3027 62 R 89.7 4 2/0/0 +5.3 1 5 10 483 0.1428 37 R 84.8 14 2/0/1 +0.9 15 9 −54 392 0.4329 42 R 43.4 6 4/3/1 +18.7 8 8 104 661 0.4230 54 R 30.2 5 2/0/0 +6.6 7 7 102 421 0.3131 42 L 13.8 133 2/1/1 +2.1 8 6 −8 404 0.2332 64 R 197.0 196 2/0/0 −5.3 17 4 38 491 0.1833 77 L 17.2 126 0/0/1 −5.9 6 1 6 502 0.2334 34 L 64.9 168 0/1/0 3.9 9 2 11 360 0.2135 66 L 95.1 126 1/1/2 +0.5 6 5 318 389 0.2536 55 R 2.6 140 1/0/0 −3.6 7 5 260 460 0.3637 64 R 107.0 196 3/0/1 +4.1 18 3 64 477 0.1738 61 L 18.5 7 0/0/1 +5.2 12 3 103 422 0.2639 62 L 17.0 133 0/0/0 +0.4 11 1 74 414 0.3540 35 L 64.4 63 0/0/0 +0.1 11 2 −46 332 0.2141 60 R 29.6 168 1/1/0 −1.8 2 1 234 533 0.1942 44 R 161.0 91 0/0/0 +5.0 18 8 1 490 0.4643 71 L 25.8 14 1/0/1 +2.1 2 4 62 613 0.1744 80 R 64.6 126 3/1/0 +6.3 1 13 −31 521 0.28
B egendt missi
teip
2
2
bDt(1d
old: Significantly different from normals at P < 0.05 (Crawford & Howell, 1998). Lime = time to stroke onset. post = post error slowing. comm.: total number of com
he digit 3. In case of a “3” they had to withhold from responding. Throughout thexperiment subjects used their preferred hand. Subjects were asked to give equalmportance to accuracy and speed in doing the task. Each subject started with aractice run consisting of 16 go and 2 no-go trials.
Our 2 accuracy measures (Table 1) were:
1. Total number of commission errors: Key press responses to a digit “3”.. Total number of omission errors: Missed responses to a digit other than 3.
Our 2 reaction time (RT) measures (Stuss et al., 2003; Picton et al., 2007) were:
1. Post-error slowing: RT during the trial following a commission error minus thatpreceding the commission error, divided by the mean RT in that subject.
. RT variability: Standard deviation of the RTs on correct response trials, dividedby the mean RT in that subject
Subjects also received a more extensive conventional neuropsychological test
attery consisting, among other tests, of target cancellation (Bells test) (Gauthier,ehaut, & Joanette, 1989), line bisection (Schenkenberg, Bradford, & Ajax, 1980),he number location test from the Visual Object Space Perception Battery (VOSP)Warrington & James, 1991), Coloured Progressive Matrices (Raven, Court, & Raven,995), visual extinction (Bender, 1952), BORB (Riddoch & Humphreys, 1993) andigit span (Wechsler, 1998).
: side: hemispheric side of the lesion. L: Left. R: Right. M: Middle. Size: Lesion size.on errors; omiss.: total number of omission errors.
2.3. Image acquisition and preprocessing
A 3 T Philips Intera system (Best, Netherlands) equipped with a head volumecoil provided T1 images (TR = 1975 ms, TE = 30 ms, in-plane resolution 1 mm) aswell as Fluid Attenuation Inversion Recovery (FLAIR) 3D images (TR = 10741 ms,TE = 150 ms) in each patient. Using SPM2 (http://www.fil.ion.ucl.ac.uk, WelcomeTrust Centre for Neuroimaging, London, UK) the T1 and FLAIR images were co-registered. The T1 scan was normalized to the Montreal Neurological Institute(MNI) T1 template in Talairach space (Friston et al., 1995; Talairach & Tournoux,1988). The spatial normalization involved both linear (12 affine transforma-tions) and nonlinear (7 × 9 × 7 basis functions, 16 reiterations) transformations(Ashburner & Friston, 1999). High regularization was used to constrain the non-linear part of the algorithm and penalize unlikely deformations associated withthe presence of lesions (Ashburner & Friston, 1999; Tyler, Marslen-Wilson, &Stamatakis, 2005). The same normalization matrix was applied to the FLAIRimages. The match between each patient’s normalized brain and the brain tem-plate was carefully evaluated through visual inspection and use of a cross-hairyoked between the template image and the normalized image. After verifi-
cation of the normalization, lesions were semi-automatically delineated usingMRIcro version 1.37 (http://www.sph.sc.edu/comd/rorden/mricro.html) and man-ually set intensity thresholds (Rorden et al., 2007). Subsequently the lesionvolumes were imported into the MRIcron lesion-symptom mapping software(http://www.sph.sc.edu/comd/rorden/mricron). A voxel was included in the analysisonly if it was lesioned in at least 4 of the subjects.
P. Molenberghs et al. / Neuropsychologia 47 (2009) 2866–2875 2869
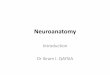
Fig. 1. Total group. Lesion distribution volume. The color code indicates in how many individuals of our patient sample (n = 44) a given voxel was lesioned (ranging from 1 to 13).(A) Transverse sections. (B) Projection on the Population-Average, Landmark and Surface based (PALS) (van Essen, 2005) atlas using Computerized Anatomical Reconstructiona ol of ME
2
2
theamc(
2
(s(wWieaht(
2
sd
at
nd Editing Toolkit (sideview and ventral view) (CARET, Washington University Schossen et al., 2001)).
.4. Statistical analysis
.4.1. Factor analysis of neuropsychological test scoresThe neuropsychological data were subjected to a principal components fac-
or analysis with orthogonal rotation (Statistical Package for the Social Sciences,ttp://www.spss.com/spss/). We included the 4 SART parameters (commissionrror rate, omission error rate, post-error slowing and within-subject RT vari-bility) as well as contra- versus ipsilesional omissions on the Bells test,ean percentage deviation on the line bisection (ipsilesional deviation being
oded positively), and the score on the number location test of the VOSPTable 1).
.4.2. Voxel-based lesion symptom mapping of SARTEach of the 4 SART parameters was entered separately into a VLSM analysis
Rorden et al., 2007). We examined which voxels when lesioned were associated withignificantly worse scores compared to patients in whom these voxels were intactBrunner and Munzel t test; Brunner & Munzel, 2000). Our significance thresholdas set at P < 0.05, with a Bonferroni correction for the brain search volume (Family-ise Error correction; Rorden et al., 2007). When VLSM yielded a significant effect
n a particular region, we determined the origin of the finding in further detail: wevaluated the average scores in the patient group who had a lesion in that regionnd the group who did not have a lesion in that region. Furthermore, we evaluatedow many of the individuals with a lesion in that region had a significant deficit athe individual level compared to cognitively intact controls using a modified t testCrawford & Howell, 1998).
.4.3. Linear regression analysesWe conducted a multiple linear regression with age, lesion extent and time to
troke onset as independent variables and the different SART parameters as depen-ent variables.
We also conducted two simple linear regression analyses with reaction timess independent variable and omission error rate and commission error rate, respec-ively, as dependent variables.
edicine, Department of Anatomy and Neurobiology, http://brainmap.wustl.edu(van
3. Results
3.1. Factor analysis
In the total study population, a factor analysis of the neuropsy-chological data revealed 3 factors with an Eigenvalue higher than 1:the first factor explained 31.0% of the total variance (Eigenvalue =2.17) and clustered the target cancellation (r = 0.94), line bisection(r = 0.86), and the number location score (r = 0.72). The secondfactor (Eigenvalue = 1.36) explained 18.7% of the total varianceand clustered RT variability (r = 0.84) and omission error rate(r = 0.63). A third factor (Eigenvalue = 1.16) explained 13.9% of thevariance and clustered the commission error rate (r = 0.85) andpost-error slowing (r = −0.61).
3.2. VLSM of SART
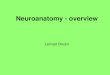
When we used commission error rate as input for the VLSM anal-ysis, lesions of the right IFG (centre of mass x = 43, y = 25, z = 14,ext. 16,586 mm3, P < 0.05) were associated with significantly morecommission errors than was seen in patients in whom this regionwas intact (Fig. 3A). Six patients (cases 3, 17, 28, 32, 37, 42) hada lesion that overlapped with this right IFG region. Their average
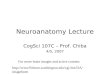
commission error rate was 14.0 (S.D. 4.77) whereas the averagecommission error rate in the remainder of the patients was 5.29(S.D. 3.36), similarly to what we saw in controls (mean 7.6, S.D.2.53). At the individual level, 4 out of 6 patients with a right IFGlesion (cases 28, 32, 37, 42) had a significantly higher commis-
2870 P. Molenberghs et al. / Neuropsycho
Fr
s(
flrsthcspe
sSlwowAtrlnle
ig. 2. Experimental paradigm. In the main experiment subjects were instructed toespond to each digit with a key press except to the digit 3 (no-go trial).
ion error rate than controls (P < 0.05; Crawford & Howell, 1998)Fig. 4).
In order to examine the apparent right-sided laterality weipped the right IFG VLSM result and examined whether the flippedegion belonged to the VLSM lesion distribution volume and howubjects behaved who had a left-sided lesion that overlapped withhe flipped region. Four left-hemispheric patients (cases 5, 7, 35, 40)ad a lesion that overlapped with the flipped region. The averageommission error rate in these 4 patients was 7.5 (S.D. 5.06) closelyimilar to the normal values. At the individual level, none of theatients with a left IFG lesion showed a pathological commissionrror rate (Crawford & Howell, 1998).
Overall, left-hemispheric lesions (29.3 voxels, S.D. 32.5) wereignificantly smaller than right-hemispheric lesions (84.7 voxels,.D. 79.6) (P < 0.01) (Figs. 1 and 5). This could cause a spuriousaterality effect in favor of the right hemisphere. For that reason
e conducted a VLSM analysis with the left-hemispheric patientsnly. This did not yield any significant effect in the left IFG, even ife lowered the significance threshold to an uncorrected P < 0.05.similar analysis with the right-sided lesion patients confirmed
he results from the main analysis (corrected P < 0.05). Within the
ight-hemispheric group, commission error rate tended to corre-ate with lesion size (Pearson r = 0.376, P = 0.06) but this couldot account for the right IFG result since patients with similar-sizedesions sparing the right IFG did not show an increased commissionrror rate (Fig. 5).
logia 47 (2009) 2866–2875
When we used post-error slowing as input for the VLSM anal-ysis, lesions of the middle third of the right IFS (centre of massx = 35 mm, y = 33 mm, z = 27 mm, ext. 718 mm3, P < 0.05) wereassociated with a significant decrease in post-error slowing com-pared to what was seen in patients in whom this region was intact(Fig. 3B). Six patients (cases 3, 17, 18, 28, 32 and 42) had a lesionoverlapping with this right IFS lesion. They responded as fast aftera commission error (479 ms, S.D. 84) as before (481 ms, S.D. 58)while patients who did not have an IFS lesion showed post-errorslowing (post-commission error: 539 ms (S.D. 125), prior to com-mission error: 463 ms (S.D. 116)) similar in degree to what we sawin the healthy controls (post-error: 477 ms, S.D. 206; prior to error360 ms, S.D. 47) (Fig. 6). At the individual level, the reduction inpost-error slowing did not reach significance in any of the 6 patientscompared to controls (Crawford & Howell, 1998).
The functional dissociation between the right IFG and the rightmiddle IFS was confirmed when we lowered the threshold of theVLSM analysis to an uncorrected P < 0.001: even at this lowerthreshold, commission error rate and post-error slowing localisedto two nearby but anatomically distinct areas.
If we used the difference in reaction times before and after acommission error as VLSM input without dividing by the individ-ual’s mean RT, results were entirely comparable (corrected P <0.05). At a slightly lower significance threshold, this was also trueif the reaction times following a correctly withheld response ratherthan those preceding a commission error were subtracted from thereaction times following a commission error.
VLSM analysis of omission error rate and RT variability did notyield any significant results at the pre-set significance threshold.
In order to evaluate whether the absence of any parietal involve-ment in the SART was due to lack of sensitivity for parietalinvolvement in the specific patient sample examined, we testedwhether a VLSM with the spatial bias measure of the targetcancellation task as input yielded the predicted parietal effects(Molenberghs et al., 2008; Mort et al., 2003). Lesions of right inferiorparietal cortex extending into the lower bank of IPS were associatedwith a significantly higher rightward bias than what was seen in theabsence of inferior parietal lesions.
Our a priori measures of sustained attention did not captureperformance changes over time. In order to evaluate whether thisexplained the absence of parietal involvement, we calculated foreach subject the difference between commission error rate in thefirst 12 no-go trials and in the last 12 no-go trials. Likewise, forthe omission error rate and the reaction time variability we cal-culated the difference between the first 100 go trials and the last100 go trials. Each of these measures were used as input for VLSMbut none of these analyses yielded any inferior parietal effect,even if we lowered the threshold to an uncorrected P < 0.05. Fur-thermore we performed a linear regression analysis with reactiontime as dependent variable and trial position as the independentvariable and used the regression coefficient as input for VLSM.No parietal effect was seen, even when the threshold was low-ered at an uncorrected P < 0.05. In a final effort to relate anychanges in task performance over time to inferior parietal cortex,we divided the trial series into 5 epochs (one epoch per 45 tri-als) and conducted a linear regression analysis with epoch orderas independent variable (1–5) and commission or omission errorrates per 45-trials epoch as dependent variable. These coefficientswere used as input for VLSM. No significant effects were obtained inIPL.
3.3. Linear regression analyses
A multiple linear regression analysis with commission error rateas outcome and with age, lesion size and time-to-stroke onsetas independent variables showed a significant effect (F(3, 40) =

P. Molenberghs et al. / Neuropsychologia 47 (2009) 2866–2875 2871
F .05 (Bc
5sro
r
ig. 3. Total group. Lesion-symptom maps thresholded at Bonferroni corr. P < 0ommission error rate as input.
.39, P < 0.005). Surprisingly, commission error rate correlatedignificantly and inversely with age (r = −0.33, P = 0.021). The cor-
elation with lesion size (r = 0.27, P = 0.056) and time-to-strokenset (r = 0.25, P = 0.079) did not reach significance.Post-error slowing, reaction time variability and omission errorate did not correlate with age, lesion size or time-to-stroke onset
Fig. 4. (A–D) Lesions of the four subjects with a pat
runner-Munzel test). (A) VLSM with post-error slowing as input. (B) VLSM with
(F(3, 39) = 0.90, P = 0.45, F(3, 40) = 1.11, P = 0.36 and F(3, 40) =1.08, P = 0.37, respectively).
According to a linear regression analysis with reaction times asindependent variable and commission error rate as dependent vari-able, commission errors tended to be more frequent with fasterreaction times (Pearson correlation coefficient −0.30, P = 0.051).
hological commission error rate on the SART.

2872 P. Molenberghs et al. / Neuropsycho
Fig. 5. Regression plot. X-axis: Lesion size. Y-axis: Commission error rate. Legend:ETal
Ar
3
3
iiaaata‘ot
mrtoCsga
Fwpf
mpty squares: left-hemispheric patients. Full circles: Right-hemispheric patients.he datapoints from subjects with a lesion that overlapped with the right IFG resultre labelled with their case number. Scores that fall above the dashed line are patho-ogical compared to healthy controls.
similar analysis with omission error rate as dependent variableemained far below significance.
.4. Ancillary experiments
.4.1. Commission errorsWe investigated whether the pathological commission error rate
n case of a right-sided IFG lesion was due to the low probabil-ty of the ‘no-go’ events, the ‘no-go’ character of those events, or
combination of both. We contacted each of the 7 cases who hadright IFG lesion. Cases 3 and 42 were available for re-testing, 4
nd 2 years after the first evaluation, respectively. The tasks werehe SART using a randomization scheme per sequence of 1–9 andvariant of the SART in which subjects had to respond to a digit
3’ but not to any of the other digits. Subjects first performed theriginal SART version, subsequently an unrelated visuoperceptualask (45 min) and the SART variant thereafter.
On the original SART version cases 3 and 42 made 18 and 15 com-ission errors, respectively, out of 25 no-go trials, confirming the
esults obtained in the main study. On the SART variant with propor-ionally more no-go trials, case 3 made only one commission errorut of 200 no-go trials and one omission error out of 25 go trials.
ase 42 made one commission error and no omission errors. Theseubjects therefore were able to correctly withhold responses to no-o trials when the no-go trials were highly expected and were alsoble to correctly respond to low-probability trials if these consistedig. 6. Mean reaction times before and after a commission error in controls, patientsith and patients without an IFS lesion. Light gray: Mean reaction time in trials
receding a commission error (and S.D.). Dark gray: Mean reaction time in trialsollowing a commission error (and S.D.).
logia 47 (2009) 2866–2875
of go trials. When however no-go trials had a low probability, as inthe original SART version, they failed to withhold their responses.
3.4.2. Post-error slowingWe conducted two further variants of the SART to further elu-
cidate the source of the reduced post-error slowing. Cases 3 and42 each participated in one of these variants, which was per-formed after another unrelated visuoperceptual task (duration5 min). Stimuli and task were identical to those of the original SART(i.e. high-probability go trials and low-probability no-go trials) withone exception: we instructed case 3 to pronounce the word ‘hit’when he had made a commission error to a no-go trial. Case 3 made22 commission errors and pronounced the word ‘hit’ in 20 of those22 trials. He also pronounced ‘hit’ to the 3 no-go trials where hecorrectly withheld responses and never did in go trials. The subjecttherefore gave proof of knowledge of a distinction between the digit‘3’ trials and the other ones and was able to use this knowledge topositively respond to the ‘3’ trials in a discriminate way even whenhe was not able to withhold his response to this type of trial.
Finally, in case 42 we provided auditory feedback with a hightone for correct responses and a low tone for errors to examinewhether increased error awareness was able to restore post-errorslowing. When case 42 was tested on this version, he made 18 com-mission errors but did not show post-error slowing even whennegative feedback was provided explicitly (mean RT pre-error:545 ms, S.D. 99; mean RT post-error: 493 ms, S.D. 99).
4. Discussion
Accurate performance of the SART in the current patient samplerelied principally on the integrity of right inferior frontal cortex, inagreement with our first a priori hypothesis. Our data did not pro-vide evidence for our second hypothesis regarding the contributionof the right inferior parietal lobule. The two outcome measures withmost localising value were the commission error rate and post-errorslowing. Our two other outcome measures, omission error rate andreaction time variability, were not linked to any particular lesionsite.
The reduction in post-error slowing with IFS lesions cannotbe accounted for by a ‘hang-over’ from the erroneous processesengaged in the previous trial. If that were the case, one would expectan increase in post-error slowing in patients compared to controlsrather than a decrease.
The right-sided laterality must be interpreted with caution. Theaverage lesion size was smaller in left than in right hemispherepatients due to exclusion of patients with significant languagecomprehension deficits. This may bias the sensitivity of the VLSManalysis in favor of the right hemisphere. When we conducted aVLSM analysis separately in the left and in the right hemispherepatients, this confirmed the right-sided effect in the absence of asignificant left IFG effect. Previous studies have also suggested thatright IFG lesions may cause more response inhibition problems thanleft IFG lesions (Aron et al., 2004).
Our consecutive series did not include cases of anterior cerebralartery ischemia. Our data therefore are neutral to the possible con-tribution of anterior cingulate or other medial frontal regions tocognitive control (Alexander et al., 2005, 2007; Fellows & Farah,2005; Picton et al., 2007). Medial frontal lesions may cause anincrease in both omission (Picton et al., 2007) and commissionerrors during a go-no go task (Drewe, 1975) as well as increased
response variability (Picton et al., 2007). According to single neu-ron recording studies (Schall, Stuphorn, & Brown, 2002), patientlesion studies (Swick & Turken, 2002) and fMRI of the intact brain(Garavan, Ross, Kaufman, & Stein, 2003; Lütcke & Frahm, 2008) theanterior cingulate plays a role in monitoring of conflict (Botvinick
psycho
ecasa
atMoableasotnlrirgbvrldirAaaia2alm
rsc2mdofbarbpvg
cajriwlIf
P. Molenberghs et al. / Neuro
t al., 1999; Carter et al., 1998; McDonald et al., 2000) and error. In aase study of an anterior cingulate lesion, error-related negativity,n event-related potential thought to reflect the activity of a neuralystem responsible for error detection (Scheffers et al., 1996), wasbolished (Swick & Turken, 2002).
Inferior parietal lesions were not associated with changes inny of the SART parameters compared to other lesion sites, con-rary to our a priori hypothesis (Hjaltason et al., 1996; Robertson,
anly, Beschin, et al., 1997; Samuelsson et al., 1998). In previ-us studies (Hjaltason et al., 1996; Robertson, Manly, Beschin, etl., 1997; Samuelsson et al., 1998), patients were selected on theasis of the presence of a clinical neglect syndrome, regardless of
esion extent or site. The lesion in individual neglect patients how-ver often extends beyond the parietal lobe. Possibly, the sustainedttention deficits seen in neglect patients are due to collateral right-ided inferior frontal damage. Alternatively, if response variabilityr other measures of sustained attention rely on a brain circuithat includes other areas besides IPL, patients with IPL lesions mayot be significantly different on this parameter from patients with
esions of this circuit outside IPL. Conceivably, variations of the cur-ent paradigm could modify the exact sustained attention demandsncreasing the sensitivity of this task for parietal damage but thisemains to be tested empirically. For instance, had we reversed theo no-go rule, the need to inhibit automatic responses would haveeen much reduced and the relative contribution of inferior frontalersus inferior parietal cortex might have been reversed. The SARTequires subjects to attend to the identity of the digit rather than itsocation (Malhotra, Coulthard, & Husain, 2009). Had we placed theigits at peripheral locations and requested the subjects to mon-
tor stimulus location rather digit identity, we would predict thatight inferior parietal involvement would have been much stronger:ccording to a recent lesion study in neglect patients (Malhotra etl., 2009), right IPL lesions impair sustained attention mainly whenttention is directed to locations compared to object identity. Thiss in agreement with a previous fMRI study implicating the rightngular gyrus in spatial short-term memory (Vandenberghe et al.,001). Had we presented the digits at varying peripheral locationsnd instructed subjects to maintain attention to a selection of theseocations, right inferior parietal involvement could have been much
ore prominent (Malhotra et al., 2009).We did not obtain any significant lesion correlate for intrasubject
esponse variability. This differs from an earlier region-based lesiontudy implicating the lateral convexity and medial wall of prefrontalortex in increased individual performance variability (Stuss et al.,003) during forced-choice simple target detection tasks and evenore so during more complex tasks, such as detection of a target
efined by feature conjunction (Stuss et al., 2003). In that study onlyrbitofrontal lesions did not affect RT variability. The effect of pre-rontal lesions on RT variability in previous studies was principallyased on comparisons with normal control populations (Picton etl., 2007; Stuss et al., 2003). If RT variability can be affected by aelatively wide range of prefrontal regions, it may not be detectedy VLSM since VLSM compares the measure of interest betweenatients who have a lesion in a given voxel to those in whom theoxel is spared: the comparison group, i.e. the patients in whom aiven voxel is intact, may also show a deficit of this parameter.
Our findings confirm the critical role of the right IFG in inhibitoryontrol (Bunge et al., 2002; Fassbender et al., 2004; Garavan etl., 1999; Konishi et al., 1998, 1999). In the SSRT paradigm, sub-ects with right inferior opercular lesions are able to abort theiresponses only when the delay interval between go- and stop-signal
s relatively brief compared to controls or patients with lesions else-here in prefrontal cortex. The extent of the right inferior frontalesion correlates positively with SSRT (Aron et al., 2003, 2004).n healthy controls, transcranial magnetic stimulation of the rightrontal operculum shortens the delay between go- and stop-signal
logia 47 (2009) 2866–2875 2873
that is required to interrupt the go-response, in the absence of anyeffect upon go trials (Chambers et al., 2006). Because no-go trialsare relatively rare in the SART and the intertrial interval is fixed,subjects will have a propensity to respond to each trial. Identifi-cation of a “3” may be analogous to a stop signal. In patients withright inferior frontal lesions the time required to identify a stimulusmay exceed that needed to interrupt the motor plan, resulting in acommission error.
Post-error slowing relies on a reaction time contrast betweentwo temporally juxtaposed trials within a same subject. Post-errorslowing can be calculated in a variety of ways, e.g. by subtractingeither the reaction time prior to the false-positive trial or by sub-tracting the reaction time following a correctly withheld response.One can normalize the post-error slowing by mean response timeor not. Whichever formula is used, the VLSM results were closelysimilar. Post-error slowing was significantly reduced in patientswith lesions confined to the middle third of the right IFS (Fig. 3),superiorly and anteriorly to the relatively large IFG region impli-cated in commission errors. In a previous region-based study,post-error slowing was reversed in patients with left dorsolat-eral prefrontal lesions (more rapid responses following errors) andreduced in patients with right dorsolateral prefrontal lesions (Stusset al., 2003). Several of the lesions in that study included the rightIFS (Stuss et al., 2003). Reduced post-error slowing results fromalterations of a feedback loop that encompasses the evaluation ofmismatches between actual outcome and task goal and the adap-tation of behavioral schemata (Shallice, 1988) on the basis of themismatch. In a classical case study, a frontal lesion patient wasable to verbally report errors he or others made but failed to usethese errors to modify his behavior (Konow & Pribram, 1970). A setof follow-up experiments we carried out provides evidence thatsubjects were aware of the distinction between go and no-go tri-als. Even when they received feedback, they did not slow theirresponses, compatible with a deficiency in error utilization (Konow& Pribram, 1970) rather than error evaluation.
According to a recent and influential model of the neuroanatomyof spatial and nonspatial attention (Corbetta & Shulman, 2002), aventral network consisting of the right temporoparietal junction,inferior and middle frontal gyrus, is implicated in stimulus-drivenreorienting. This ventral network has been proposed as an alertingsystem that detects novel stimuli (Corbetta & Shulman, 2002). Ourdata call for some modification of this model. The contribution ofIFS in our study was, strictly speaking, not exogenously driven: itwas driven by the error made in response to the no-go stimulus.The reduction of post-error slowing following lesions of the middlethird of the right IFS provides strong evidence that this region isinvolved in on-line readjustment of attentional resources and thatthe role of this region is not limited to exogenous, stimulus-drivenreorienting conditions.
To conclude, commission error rate and post-error slowing in therandom version of the SART rely in particular on the integrity of theright inferior frontal cortex. We did not find any positive argumentsin favor of a contribution of the inferior parietal lobule.
Acknowledgements
Supported by FWO grants G.0076.02 and G0668.07 (EuroCores)(R.V.), KU Leuven Research grants OT/04/41 and EF/05/014 (R.V.),and Inter-University Attraction Pole P6/29. R.V. is a Clinical Investi-gator of the Fund for Scientific Research (FW0), Flanders (Belgium),and CRG an FWO research fellow.
References
Alexander, M., Stuss, D., Picton, T., Shallice, T., & Gillingham, S. (2007). Regionalfrontal injuries cause distinct impairments in cognitive control. Neurology, 68,1515–1523.

2 psycho
A
A
A
A
B
B
B
B
B
B
B
C
C
C
C
C
D
D
D
D
F
F
F
G
G
G
G
H
H
H
H
J
K
K
K
874 P. Molenberghs et al. / Neuro
lexander, M., Stuss, D., Shallice, T., Picton, T., & Gillingham, S. (2005). Impaired con-centration due to frontal lobe damage from two distinct lesion sites. Neurology,65, 572–579.
ron, A., Fletcher, P., Bullmore, E., Sahakian, B., & Robbins, T. (2003). Stop-signalinhibition disrupted by damage to right inferior frontal gyrus in humans. NatureNeuroscience, 6, 115–116.
ron, A., Robbins, T., & Poldrack, R. (2004). Inhibition and the right inferior frontalcortex. Trends of Cognitive Neuroscience, 8, 170–177.
shburner, J., & Friston, K. (1999). Nonlinear spatial normalization using basis func-tions. Human Brain Mapping, 7, 254–266.
ates, E., Wilson, S. M., Saygin, A. P., Dick, F., Sereno, M. I., Knight, R. T. ,., et al. (2003).Voxel-based lesion-symptom mapping. Nature Neuroscience, 6, 448–450.
elgrove, M., Hawi, Z., Gill, M., & Robertson, I. (2006). The cognitive genetics ofattention deficit hyperactivity disorder: Sustained attention as a candidate phe-notype. Cortex, 42, 838–845.
ender, M. (1952). Disorders in perception (with particular reference to the phenomenaof extinction and displacement). Springfield, IL: C. C. Thomas.
otvinick, M., Nystrom, L., Fissell, K., Carter, C., & Cohen, J. (1999). Conflict monitoringversus selection-for-action in anterior cingulate cortex. Nature, 402, 179–181.
raver, T., Reynolds, J., & Donaldson, D. (2003). Neural mechanisms of transient andsustained cognitive control during task switching. Neuron, 39, 713–726.
runner, E., & Munzel, U. (2000). The nonparametric Behrens-Fisher problem:Asymptotic theory and a small-sample approximation. Biometric Journal, 1,17–25.
unge, S., Dudukovic, N., Thomason, M., Vaidya, C., & Gabrieli, J. (2002). Immaturefrontal lobe contributions to cognitive control in children: Evidence from fMRI.Neuron, 33, 301–311.
arter, C., Braver, T., Barch, D., Botvinick, M., Noll, D., & Cohen, J. (1998). Anteriorcingulate cortex, error detection, and the online monitoring of performance.Science, 280, 747–749.
hambers, C., Bellgrove, M., Stokes, M., Henderson, T., Garavan, H., Robertson, I. ,.,et al. (2006). Executive “brake failure” following deactivation of human frontallobe. Journal of Cognitive Neuroscience, 18, 444–455.
han, R. (2001). A further study on the sustained attention to response task (SART):The effect of age, gender and education. Brain Injury, 15, 819–829.
orbetta, M., & Shulman, G. (2002). Control of goal-directed and stimulus-drivenattention in the brain. Nature Review Neuroscience, 3, 201–215.
rawford, J., & Howell, D. (1998). Comparing an individual’s test score against normsderived from small samples. Clinical Neuropsychology, 12, 482–486.
errfuss, J., Brass, M., Neumann, J., & von Cramon, D. (2005). Involvement of theinferior frontal junction in cognitive control: Meta-analyses of switching andStroop studies. Human Brain Mapping, 25, 22–34.
rewe, E. (1975). An experimental investigation of Luria’s theory on the effects offrontal lobe lesions in man. Neuropsychologia, 13, 421–429.
uncan, J., Emslie, H., & Williams, P. (1996). Intelligence and the frontal lobe: Theorganization of goal-directed behavior. Cognitive Psychology, 30, 257–303.
uncan, J., & Owen, A. M. (2000). Common regions of the human frontal loberecruited by diverse cognitive demands. Trends in Neurosciences, 23, 475–483.
assbender, C., Murphy, K., Foxe, J. J., Wylie, G., Javitt, D. C., & Robertson, I. (2004). Atopography of executive functions and their interactions revealed by functionalmagnetic resonance imaging. Cognitive Brain Research, 20(2), 132–143.
ellows, L., & Farah, M. (2005). Is anterior cingulate cortex necessary for cognitivecontrol? Brain, 128, 788–796.
riston, K., Holmes, A., Worsley, K., Poline, J., Frith, C., Heather, J. ,., et al. (1995).Statistical parametric maps in functional imaging: A general approach. HumanBrain Mapping, 2, 189–210.
aravan, H., Ross, T., Kaufman, J., & Stein, E. (2003). A midline dissociation betweenerror-processing and response-conflict monitoring. Neuroimage, 20, 1132–1139.
aravan, H., Ross, T., & Stein, E. (1999). Right hemispheric dominance of inhibitorycontrol: An event-related functional MRI study. Proceedings of National Academyof Sciences of United States of America, 96, 8301–8306.
authier, L., Dehaut, F., & Joanette, Y. (1989). The bells test: A quantitative and quali-tative test for visual neglect. International Journal of Clinical Neuropsychology, 11,49–54.
reene, C., Bellgrove, M., Gill, M., & Robertson, I. (2009). Noradrenergic genotypepredicts lapses in sustained attention. Neuropsychologia, 47, 591–594.
jaltason, H., Tegner, R., Tham, K., Levander, M., & Ericson, K. (1996). Sustained atten-tion and awareness of disability in chronic neglect. Neuropsychologia, 34(12),1229–1233.
on, N., Epstein, R., Owen, A., & Duncan, J. (2006). Frontoparietal activity with min-imal decision and control. Journal of Neuroscience, 26, 9805–9809.
usain, M., & Rorden, C. (2003). Non-spatially lateralized mechanisms in hemispatialneglect. Nature Review Neuroscience, 4, 26–36.
usain, M., Shapiro, K., Martin, J., & Kennard, C. (1997). Abnormal temporal dynamicsof visual attention in spatial neglect patients. Nature, 385, 154–156.
ohnson, K. A., Robertson, I. H., Kelly, S. P., Silk, T. J., Barry, E., Dáibhis, A. ,., et al. (2007).Dissociation in performance of children with adhd and high-functioning autismon a task of sustained attention. Neuropsychologia, 45, 2234–2245.
erns, J., Cohen, J., MacDonald, A., Cho, R., Stenger, V., & Carter, C. (2004). Anterior cin-gulate conflict monitoring and adjustments in control. Science, 303, 1023–1026.
onishi, S., Nakajima, K., Uchida, I., Kikyo, H., Kameyama, M., & Miyashita, Y. (1999).Common inhibitory mechanism in human inferior prefrontal cortex revealed byevent-related functional mri. Brain, 122, 981–991.
onishi, S., Nakajima, K., Uchida, I., Sekihara, K., & Miyashita, Y. (1998). No-go dom-inant brain activity in human inferior prefrontal cortex revealed by functionalmagnetic resonance imaging. European Journal of Neuroscience, 10, 1209–1213.
logia 47 (2009) 2866–2875
Konow, A., & Pribram, K. (1970). Error recognition and utilization produced by injuryto the frontal cortex in man. Neuropsychologia, 8, 489–491.
Logan, G., & Cowan, W. (1984). On the ability to inhibit thought and action: A theoryof an act of control. Psychological Review, 91, 295–327.
Lütcke, H., & Frahm, J. (2008). Lateralized anterior cingulate function during errorprocessing and conflict monitoring as revealed by high-resolution fMRI. CerebralCortex, 18, 508–515.
Malhotra, P., Coulthard, E., & Husain, M. (2009). Role of right posterior parietal cortexin maintaining attention to spatial locations over time. Brain, 132, 645–660.
Manly, T., Owen, A. M., McAvinue, L., Datta, A., Lewis, G. H., Scott, S. K. ,., et al.(2003). Enhancing the sensitivity of a sustained attention task to frontal damage:Convergent clinical and functional imaging evidence. Neurocase, 9(4), 340–349.
McDonald, A., Cohen, J., Stenger, V., & Carter, C. (2000). Dissociating the role of thedorsolateral prefrontal and anterior cingulate cortex in cognitive control. Science,288, 1835–1838.
Mennemeier, M., Chatterjee, A., Watson, R., Wertman, E., Carter, L., & Heilman, K.(1994). Contributions of the parietal and frontal lobes to sustained attentionand habituation. Neuropsychologia, 32, 703–716.
Molenberghs, P., Gillebert, C., Peeters, R., & Vandenberghe, R. (2008). Convergencebetween lesion-symptom mapping and fmri of spatially selective attention inthe intact brain. Journal of Neuroscience, 28, 3359–3373.
Mort, D., Malhotra, P., Mannan, S., Rorden, C., Pambakian, A., Kennard, C. ,., et al.(2003). The anatomy of visual neglect. Brain, 126, 1986–1997.
Nakahara, K., Hayashi, T., Konishi, S., & Miyashita, Y. (2002). Functional MRIof Macaque monkeys performing a cognitive set-shifting task. Science, 295,1532–1536.
O’Connell, R., Bellgrove, M., Dockree, P., Lau, A., Fitzgerald, M., & Robertson, I. (2008).Self-alert training: Volitional modulation of autonomic arousal improves sus-tained attention. Neuropsychologia, 46, 1379–1390.
Picton, T., Stuss, D., Alexander, M., Shallice, T., Binns, M., & Gillingham, S. (2007).Effects of focal frontal lesions on response inhibition. Cerebral Cortex, 17,826–838.
Rabbitt, P. (1966). Errors and error-correction in choice-response tasks. Journal ofExperimental Psychology, 71, 264–272.
Raven, J., Court, J., & Raven, J. (1995). Coloured progressive matrices. Oxford: OxfordPsychologists Press.
Richer, F., & Lepage, M. (1996). Frontal lesions increase post-target interference inrapid stimulus streams. Neuropsychologia, 34, 509–514.
Riddoch, M., & Humphreys, G. (1993). Birmingham object recognition battery. Hove,UK: Lawrence Erlbaum Associates Ltd.
Robertson, I., Manly, T., Andrade, J., Baddeley, B., & Yiend, J. (1997). ‘oops!’: Perfor-mance correlates of everyday attentional failures in traumatic brain injured andnormal subjects. Neuropsychologia, 35(6), 747–758.
Robertson, I., Manly, T., Beschin, N., Daini, R., aeske Dewick, H., Homberg, V. ,., etal. (1997). Auditory sustained attention is a marker of unilateral spatial neglect.Neuropsychologia, 35(12), 1527–1532.
Robertson, I., Mattingley, J., Rorden, C., & Driver, J. (1998). Phasic alerting ofneglect patients overcomes their spatial deficit in visual awareness. Nature, 395,169–172.
Rorden, C., Karnath, H., & Bonilha, L. (2007). Improving lesion-symptom mapping.Journal of Cognitive Neuroscience, 19, 1081–1088.
Rubia, K., Russell, T., Overmeyer, S., Brammer, M., Bullmore, E., Sharma, T. ,., et al.(2001). Mapping motor inhibition: Conjunctive brain activations across differentversions of go/no-go and stop tasks. NeuroImage, 13, 250–261.
Samuelsson, H., Hjelmquist, E., Jensen, C., Ekholm, S., & Blomstrand, C. (1998).Nonlateralized attentional deficits: An important component behind persist-ing visuospatial neglect? Journal of Clinical and Experimental Neuropsychology,20, 73–88.
Schall, J., Stuphorn, V., & Brown, J. (2002). Monitoring and control of action by thefrontal lobes. Neuron, 36, 309–322.
Scheffers, M., Coles, M., Bernstein, P., Gehring, W., & Donchin, E. (1996). Event-relatedbrain potentials and error-related processing: An analysis of incorrect responsesto go and no-go stimuli. Psychophysiology, 33, 42–53.
Schenkenberg, T., Bradford, D., & Ajax, E. (1980). Line bisection and unilateral visualneglect in patients with neurologic impairment. Neurology, 30, 509–517.
Shallice, T. (1988). From neuropsychology to mental structure. Cambridge: CambridgeUniversity Press.
Shallice, T., Marzocchi, G., Coser, S., DelSavio, M., Meuter, R., & Rumiati, R. (2002).Executive function profile of children with attention deficit hyperactivity disor-der. Developmental Neuropsychology, 21, 43–71.
Sohn, M., Ursu, S., Anderson, J., Stenger, V., & Carter, C. (2000). The role of prefrontalcortex and posterior parietal cortex in task switching. Proceedings of NationalAcademy of Sciences of United States of America, 97, 13448–13453.
Stuss, D., Murphy, K., Binns, M., & Alexander, M. (2003). Staying on the job: Thefrontal lobes control individual performance variability. Brain, 126, 2363–2380.
Stuss, D., Shallice, T., Alexander, M., & Picton, T. (1995). A multidisciplinary approachto anterior attentional functions. Annals of New York Academy of Sciences, 769,191–212.
Swick, D., & Turken, A. (2002). Dissociation between conflict detection and errormonitoring in the human anterior cingulate cortex. Proceedings of National
Academy of Sciences of United States of America, 99, 16354–16359.Talairach, J., & Tournoux, P. (1988). Co-planar stereotaxic atlas of the human brain. NewYork: Thieme Medical Publishers, Inc.
Tyler, L., Marslen-Wilson, W., & Stamatakis, E. (2005). Dissociating neuro-cognitivecomponent processes: Voxel-based correlational methodology. Neuropsycholo-gia, 43, 771–778.

psycho
v
v
V
W
P. Molenberghs et al. / Neuro
an Essen, D. (2005). A population-average, landmark- and surface-based (PALS)atlas of human cerebral cortex. Neuroimage, 28, 635–662.
an Essen, D., Drury, H., Dickson, J., Harwell, J., Hanlon, D., & Anderson, C. (2001). An
integrated software suite for surface-based analyses of cerebral cortex. Journalof American Medical Informatics Association, 8, 443–459.andenberghe, R., Gitelman, D., Parrish, T., & Mesulam, M. (2001). Location- orfeature-based targeting of peripheral attention. NeuroImage, 14, 34–47.
arrington, E., & James, M. (1991). Visual object and space perception battery. ThamysValley Test Company Ltd.
logia 47 (2009) 2866–2875 2875
Wechsler, D. (1998). Wechsler Memory Scale-III. San Antonio, TX: The PsychologicalCorporation.
Whyte, J., Grieb-Neff, P., Gantz, C., & Polanksy, M. (2006). Measuring sustained atten-
tion after traumatic brain injury: Differences in key findings from the sustainedattention to response task. Neuropsychologia, 44, 2007–2014.Wilkins, A., Shallice, T., & McCarthy, R. (1987). Frontal lesions and sustained attention.Neuropsychologia, 25, 359–365.
Zordan, L., Sarlo, M., & Stablum, F. (2008). ERP components activate by the ‘GO’ and‘withhold’ conflict in the random SART. Brain Cognition, 66, 57–64.