Upload
cristieristiie
View
254
Download
0
Embed Size (px)
Citation preview
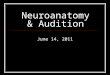
7/27/2019 In Neuroanatomy
1/42
In neuroanatomy, a nucleus is a brain structure consisting of a relatively compact cluster of
neurons. It is one of the two most common forms of nerve cell organization, the other being
layered structures such as the cerebral cortex or cerebellar cortex. In anatomical sections, a
nucleus shows up as a region of gray matter, often bordered by white matter. The
vertebrate brain contains hundreds of distinguishable nuclei, varying widely in shape and
size. A nucleus may itself have a complex internal structure, with multiple types of neuronsarranged in clumps (subnuclei) or layers.
The term "nucleus" is in some cases used rather loosely, to mean simply an identifiably
distinct group of neurons, even if they are spread over an extended area. The reticular
nucleus of the thalamus, for example, is a thin layer of inhibitory neurons that surrounds the
thalamus.
Some of the major anatomical components of the brain are organized as clusters of
interconnected nuclei. Notable among these are the thalamus and hypothalamus, each of
which contains several dozen distinguishable substructures. The medulla and pons also
contain numerous small nuclei with a wide variety of sensory, motor, and regulatory
functions.In the peripheral nervous system, a cluster of neurons is referred to instead as a ganglion.
Examples
Brainstem: red nucleus, vestibular nucleus, inferior olive
Cerebellum: dentate nucleus, emboliform nucleus, globose nucleus, fastigial nucleus
Basal ganglia: striatum (caudate and putamen), pallidum (globus pallidus, medial and
lateral), substantia nigra, subthalamic nucleus
Cranial nerve nuclei
Nucleus Accumbens
The nucleus accumbens (NAcc), also known as the accumbens nucleus or as the nucleus
accumbens septi (Latin for nucleus leaning against the septum) or as part of the pleasure
center, is a collection of neurons and forms the main part of the ventral striatum. It is
thought to play an important role in reward, pleasure, laughter, addiction, aggression, fear,
and the placebo effect.[1][2][3]
Each half of the brain has one nucleus accumbens. It is located where the head of the
caudate and the anterior portion of the putamen meet just lateral to the septum
pellucidum. The nucleus accumbens and the olfactory tubercle collectively form the ventral
striatum, which is part of the basal ganglia.[4]
The nucleus accumbens can be divided into two structuresthe nucleus accumbens core
and the nucleus accumbens shell. These structures have different morphology and function.
The principal neuronal cell type found in the nucleus accumbens is the medium spiny
neuron. The neurotransmitter produced by these neurons is gamma-aminobutyric acid
(GABA), one of the main inhibitory neurotransmitters of the central nervous system. These
neurons are also the main projection or output neurons of the nucleus accumbens.
While 95% of the neurons in the nucleus accumbens are medium spiny GABA-ergic
projection neurons, other neuronal types are also found such as large aspiny cholinergic
interneurons.
[edit]Output and input
http://en.wikipedia.org/wiki/Neuroanatomyhttp://en.wikipedia.org/wiki/Brainhttp://en.wikipedia.org/wiki/Neuronhttp://en.wikipedia.org/wiki/Cerebral_cortexhttp://en.wikipedia.org/wiki/Cerebellumhttp://en.wikipedia.org/wiki/Gray_matterhttp://en.wikipedia.org/wiki/White_matterhttp://en.wikipedia.org/wiki/Vertebratehttp://en.wikipedia.org/wiki/Thalamic_reticular_nucleushttp://en.wikipedia.org/wiki/Thalamic_reticular_nucleushttp://en.wikipedia.org/wiki/Thalamushttp://en.wikipedia.org/wiki/Hypothalamushttp://en.wikipedia.org/wiki/Medulla_oblongatahttp://en.wikipedia.org/wiki/Ponshttp://en.wikipedia.org/wiki/Peripheral_nervous_systemhttp://en.wikipedia.org/wiki/Ganglionhttp://en.wikipedia.org/wiki/Brainstemhttp://en.wikipedia.org/wiki/Red_nucleushttp://en.wikipedia.org/wiki/Vestibular_nucleushttp://en.wikipedia.org/wiki/Inferior_olivehttp://en.wikipedia.org/wiki/Cerebellumhttp://en.wikipedia.org/wiki/Dentate_nucleushttp://en.wikipedia.org/wiki/Emboliform_nucleushttp://en.wikipedia.org/wiki/Globose_nucleushttp://en.wikipedia.org/wiki/Fastigial_nucleushttp://en.wikipedia.org/wiki/Basal_gangliahttp://en.wikipedia.org/wiki/Striatumhttp://en.wikipedia.org/wiki/Caudatehttp://en.wikipedia.org/wiki/Putamenhttp://en.wikipedia.org/wiki/Globus_pallidushttp://en.wikipedia.org/wiki/Substantia_nigrahttp://en.wikipedia.org/wiki/Subthalamic_nucleushttp://en.wikipedia.org/wiki/Cranial_nervehttp://en.wikipedia.org/wiki/Nucleus_(neuroanatomy)http://en.wikipedia.org/wiki/Septumhttp://en.wikipedia.org/wiki/The_pleasure_centerhttp://en.wikipedia.org/wiki/The_pleasure_centerhttp://en.wikipedia.org/wiki/Neuronhttp://en.wikipedia.org/wiki/Ventral_striatumhttp://en.wikipedia.org/wiki/Reward_systemhttp://en.wikipedia.org/wiki/Pleasurehttp://en.wikipedia.org/wiki/Laughterhttp://en.wikipedia.org/wiki/Substance_use_disorderhttp://en.wikipedia.org/wiki/Aggressionhttp://en.wikipedia.org/wiki/Fearhttp://en.wikipedia.org/wiki/Placebo_effecthttp://en.wikipedia.org/wiki/Caudate_nucleushttp://en.wikipedia.org/wiki/Putamenhttp://en.wikipedia.org/wiki/Septum_pellucidumhttp://en.wikipedia.org/wiki/Septum_pellucidumhttp://en.wikipedia.org/wiki/Olfactory_tuberclehttp://en.wikipedia.org/wiki/Ventral_striatumhttp://en.wikipedia.org/wiki/Ventral_striatumhttp://en.wikipedia.org/wiki/Basal_gangliahttp://en.wikipedia.org/wiki/Nucleus_accumbens_corehttp://en.wikipedia.org/wiki/Nucleus_accumbens_shellhttp://en.wikipedia.org/wiki/Medium_spiny_neuronhttp://en.wikipedia.org/wiki/Medium_spiny_neuronhttp://en.wikipedia.org/wiki/Neurotransmitterhttp://en.wikipedia.org/wiki/Gamma-aminobutyric_acidhttp://en.wikipedia.org/wiki/Cholinergichttp://en.wikipedia.org/wiki/Interneuronhttp://en.wikipedia.org/w/index.php?title=Nucleus_accumbens&action=edit§ion=2http://en.wikipedia.org/w/index.php?title=Nucleus_accumbens&action=edit§ion=2http://en.wikipedia.org/wiki/Interneuronhttp://en.wikipedia.org/wiki/Cholinergichttp://en.wikipedia.org/wiki/Gamma-aminobutyric_acidhttp://en.wikipedia.org/wiki/Neurotransmitterhttp://en.wikipedia.org/wiki/Medium_spiny_neuronhttp://en.wikipedia.org/wiki/Medium_spiny_neuronhttp://en.wikipedia.org/wiki/Nucleus_accumbens_shellhttp://en.wikipedia.org/wiki/Nucleus_accumbens_corehttp://en.wikipedia.org/wiki/Basal_gangliahttp://en.wikipedia.org/wiki/Ventral_striatumhttp://en.wikipedia.org/wiki/Ventral_striatumhttp://en.wikipedia.org/wiki/Olfactory_tuberclehttp://en.wikipedia.org/wiki/Septum_pellucidumhttp://en.wikipedia.org/wiki/Septum_pellucidumhttp://en.wikipedia.org/wiki/Putamenhttp://en.wikipedia.org/wiki/Caudate_nucleushttp://en.wikipedia.org/wiki/Placebo_effecthttp://en.wikipedia.org/wiki/Fearhttp://en.wikipedia.org/wiki/Aggressionhttp://en.wikipedia.org/wiki/Substance_use_disorderhttp://en.wikipedia.org/wiki/Laughterhttp://en.wikipedia.org/wiki/Pleasurehttp://en.wikipedia.org/wiki/Reward_systemhttp://en.wikipedia.org/wiki/Ventral_striatumhttp://en.wikipedia.org/wiki/Neuronhttp://en.wikipedia.org/wiki/The_pleasure_centerhttp://en.wikipedia.org/wiki/The_pleasure_centerhttp://en.wikipedia.org/wiki/Septumhttp://en.wikipedia.org/wiki/Nucleus_(neuroanatomy)http://en.wikipedia.org/wiki/Cranial_nervehttp://en.wikipedia.org/wiki/Subthalamic_nucleushttp://en.wikipedia.org/wiki/Substantia_nigrahttp://en.wikipedia.org/wiki/Globus_pallidushttp://en.wikipedia.org/wiki/Putamenhttp://en.wikipedia.org/wiki/Caudatehttp://en.wikipedia.org/wiki/Striatumhttp://en.wikipedia.org/wiki/Basal_gangliahttp://en.wikipedia.org/wiki/Fastigial_nucleushttp://en.wikipedia.org/wiki/Globose_nucleushttp://en.wikipedia.org/wiki/Emboliform_nucleushttp://en.wikipedia.org/wiki/Dentate_nucleushttp://en.wikipedia.org/wiki/Cerebellumhttp://en.wikipedia.org/wiki/Inferior_olivehttp://en.wikipedia.org/wiki/Vestibular_nucleushttp://en.wikipedia.org/wiki/Red_nucleushttp://en.wikipedia.org/wiki/Brainstemhttp://en.wikipedia.org/wiki/Ganglionhttp://en.wikipedia.org/wiki/Peripheral_nervous_systemhttp://en.wikipedia.org/wiki/Ponshttp://en.wikipedia.org/wiki/Medulla_oblongatahttp://en.wikipedia.org/wiki/Hypothalamushttp://en.wikipedia.org/wiki/Thalamushttp://en.wikipedia.org/wiki/Thalamic_reticular_nucleushttp://en.wikipedia.org/wiki/Thalamic_reticular_nucleushttp://en.wikipedia.org/wiki/Vertebratehttp://en.wikipedia.org/wiki/White_matterhttp://en.wikipedia.org/wiki/Gray_matterhttp://en.wikipedia.org/wiki/Cerebellumhttp://en.wikipedia.org/wiki/Cerebral_cortexhttp://en.wikipedia.org/wiki/Neuronhttp://en.wikipedia.org/wiki/Brainhttp://en.wikipedia.org/wiki/Neuroanatomy7/27/2019 In Neuroanatomy
2/42
[edit]
Output
The output neurons of the nucleus accumbens send axon projections to the ventral analog
of the globus pallidus, known as the ventral pallidum (VP). The VP, in turn, projects to the
medial dorsal nucleus of the dorsal thalamus, which projects to the prefrontal cortex as well
as the striatum. Other efferents from the nucleus accumbens include connections with thesubstantia nigra and the pontine reticular formation.
[edit]
Input
Major inputs to the nucleus accumbens include prefrontal association cortices, basolateral
amygdala, and dopaminergic neurons located in the ventral tegmental area (VTA), which
connect via the mesolimbic pathway. Thus the nucleus accumbens is often described as one
part of a cortico-striato-thalamo-cortical loop.
Dopaminergic input from the VTA is thought to modulate the activity of neurons within the
nucleus accumbens. These terminals are also the site of action of highly-addictive drugs such
as cocaine and amphetamine, which cause a manifold increase in dopamine levels in the
nucleus accumbens.
Another major source of input comes from the CA1 and ventral subiculum of the
hippocampus to the dorsomedial area of the Nucleus accumbens. The neurons of the
hippocampus have a noteworthy correlation to slight depolarizations of cells in the nucleus
accumbens, which makes them more positive and therefore more excitable. The correlated
cells of these excited states of the medium spiny neurons in the Nucleus accumbens are
shared equally between the subiculum and CA1. The subiculum neurons are found to
hyperpolarize (increase negativity) while the CA1 neurons "ripple" (fire > 50 Hz) in order to
accomplish this priming. [5]
Caudate nucleus
From Wikipedia, the free encyclopedia
Jump to: navigation, search
Brain: Caudate nucleus
Transverse Cut of Brain (Horizontal Section), basal
ganglia is blue
The caudate nucleus is a nucleus located within the basal ganglia of the brains of many
animal species. The caudate nucleus is an important part of the brain's learning and memory
system.
Anatomy
http://en.wikipedia.org/w/index.php?title=Nucleus_accumbens&action=edit§ion=3http://en.wikipedia.org/wiki/Globus_pallidushttp://en.wikipedia.org/wiki/Medial_dorsal_nucleushttp://en.wikipedia.org/wiki/Thalamushttp://en.wikipedia.org/wiki/Prefrontal_cortexhttp://en.wikipedia.org/wiki/Striatumhttp://en.wikipedia.org/wiki/Substantia_nigrahttp://en.wikipedia.org/wiki/Pontine_reticular_formationhttp://en.wikipedia.org/w/index.php?title=Nucleus_accumbens&action=edit§ion=4http://en.wikipedia.org/wiki/Amygdalahttp://en.wikipedia.org/wiki/Ventral_tegmental_areahttp://en.wikipedia.org/wiki/Mesolimbic_pathwayhttp://en.wikipedia.org/wiki/Recreational_drug_usehttp://en.wikipedia.org/wiki/Cocainehttp://en.wikipedia.org/wiki/Amphetaminehttp://en.wikipedia.org/wiki/Dopaminehttp://en.wikipedia.org/wiki/Basal_gangliahttp://en.wikipedia.org/wiki/Basal_gangliahttp://en.wikipedia.org/wiki/Nucleus_(neuroanatomy)http://en.wikipedia.org/wiki/Basal_gangliahttp://en.wikipedia.org/wiki/Brainhttp://en.wikipedia.org/wiki/File:Telencephalon-Horiconatal.jpghttp://en.wikipedia.org/wiki/Brainhttp://en.wikipedia.org/wiki/Basal_gangliahttp://en.wikipedia.org/wiki/Nucleus_(neuroanatomy)http://en.wikipedia.org/wiki/Basal_gangliahttp://en.wikipedia.org/wiki/Basal_gangliahttp://en.wikipedia.org/wiki/Dopaminehttp://en.wikipedia.org/wiki/Amphetaminehttp://en.wikipedia.org/wiki/Cocainehttp://en.wikipedia.org/wiki/Recreational_drug_usehttp://en.wikipedia.org/wiki/Mesolimbic_pathwayhttp://en.wikipedia.org/wiki/Ventral_tegmental_areahttp://en.wikipedia.org/wiki/Amygdalahttp://en.wikipedia.org/w/index.php?title=Nucleus_accumbens&action=edit§ion=4http://en.wikipedia.org/wiki/Pontine_reticular_formationhttp://en.wikipedia.org/wiki/Substantia_nigrahttp://en.wikipedia.org/wiki/Striatumhttp://en.wikipedia.org/wiki/Prefrontal_cortexhttp://en.wikipedia.org/wiki/Thalamushttp://en.wikipedia.org/wiki/Medial_dorsal_nucleushttp://en.wikipedia.org/wiki/Globus_pallidushttp://en.wikipedia.org/w/index.php?title=Nucleus_accumbens&action=edit§ion=37/27/2019 In Neuroanatomy
3/42
Caudate nucleus within the skull
The caudate nuclei are located near the center of the brain, sitting astride the thalamus.
There is a caudate nucleus within each hemisphere of the brain. Individually, they resemblea C-shape structure with a wider "head" (caput in Latin) at the front, tapering to a "body"
(corpus) and a "tail" (cauda). Sometimes a part of the caudate nucleus is referred to as the
"knee" (genu).[1]
Transverse view of the caudate nucleus from a structural MR image
The head and body of the caudate nucleus form part of the floor of the anterior horn of the
lateral ventricle. After the body travels briefly towards the back of the head, the tail curves
back toward the anterior, forming the roof of the inferior horn of the lateral ventricle. This
means that a coronal (on a plane parallel to the face) section that cuts through the tail will
also cross the body and head of the caudate nucleus.
The caudate nucleus is related anatomically to a number of other structures. It is separated
from the lenticular nucleus (made up of the globus pallidus and the putamen) by the
anterior limb of the internal capsule. Together the caudate and putamen form the dorsal
striatum.
[edit]
http://en.wikipedia.org/wiki/File:Caudate_nucleus.gifhttp://en.wikipedia.org/wiki/Thalamushttp://en.wikipedia.org/wiki/Cerebral_hemisphereshttp://en.wikipedia.org/wiki/MRIhttp://en.wikipedia.org/wiki/Lateral_ventriclehttp://en.wikipedia.org/wiki/Facehttp://en.wikipedia.org/wiki/Lenticular_nucleushttp://en.wikipedia.org/wiki/Globus_pallidushttp://en.wikipedia.org/wiki/Putamenhttp://en.wikipedia.org/wiki/Internal_capsulehttp://en.wikipedia.org/wiki/Striatumhttp://en.wikipedia.org/w/index.php?title=Caudate_nucleus&action=edit§ion=2http://en.wikipedia.org/wiki/File:Caudate_Nucleus_Structural_MRI.pnghttp://en.wikipedia.org/wiki/File:Caudate_nucleus.gifhttp://en.wikipedia.org/wiki/File:Caudate_Nucleus_Structural_MRI.pnghttp://en.wikipedia.org/wiki/File:Caudate_nucleus.gifhttp://en.wikipedia.org/wiki/File:Caudate_Nucleus_Structural_MRI.pnghttp://en.wikipedia.org/wiki/File:Caudate_nucleus.gifhttp://en.wikipedia.org/wiki/File:Caudate_Nucleus_Structural_MRI.pnghttp://en.wikipedia.org/wiki/File:Caudate_nucleus.gifhttp://en.wikipedia.org/w/index.php?title=Caudate_nucleus&action=edit§ion=2http://en.wikipedia.org/wiki/Striatumhttp://en.wikipedia.org/wiki/Internal_capsulehttp://en.wikipedia.org/wiki/Putamenhttp://en.wikipedia.org/wiki/Globus_pallidushttp://en.wikipedia.org/wiki/Lenticular_nucleushttp://en.wikipedia.org/wiki/Facehttp://en.wikipedia.org/wiki/Lateral_ventriclehttp://en.wikipedia.org/wiki/MRIhttp://en.wikipedia.org/wiki/File:Caudate_Nucleus_Structural_MRI.pnghttp://en.wikipedia.org/wiki/Cerebral_hemisphereshttp://en.wikipedia.org/wiki/Thalamushttp://en.wikipedia.org/wiki/File:Caudate_nucleus.gif7/27/2019 In Neuroanatomy
4/42
Neurochemistry
The caudate nucleus is highly innervated by dopamine neurons. These neurons originate
mainly from the ventral tegmental area (VTA) and the substantia nigra pars compacta (SNc).
There are also additional inputs from various association cortices.
[edit]Physiology
[edit]
Learning and memory
Historically, the basal ganglia as a whole have been implicated in higher-order motor
control.[2] The caudate nucleus was initially thought to primarily be involved with control of
voluntary movement. More recently, it has been demonstrated that the caudate is highly
involved in learning and memory,[3] particularly regarding feedback processing.[4] In
general, it has been demonstrated that neural activity will be present within the caudate
while an individual is receiving feedback. People with hyperthymesia appear to have slight
increases in the sizes of the caudate nucleus as well as of the temporal lobe of the cortex.[5]
[edit]
Emotion
The caudate nucleus has been implicated in responses to visual beauty, and has been
suggested as one of the "neural correlates of romantic love".[6][7]
[edit]
Language comprehension
The left caudate in particular has been suggested to have a relationship with the thalamus
that governs the comprehension and articulation of words as they are switched between
languages.[8][9][edit]
Threshold control
The brain contains large collections of neurons reciprocally connected by excitatory
synapses, thus forming large network of elements with positive feedback. It is difficult to see
how such a system can operate without some mechanism to prevent explosive activation.
There is some indirect evidence[10] that the caudate may perform this regulatory role by
measuring the general activity ofcerebral cortex and controlling the threshold potential.
[edit]
Role in obsessive compulsive disorder
It has been theorized that the caudate nucleus may be dysfunctional in persons with
obsessive compulsive disorder (OCD), in that it may perhaps be unable to properly regulate
the transmission of information regarding worrying events or ideas between the thalamus
and the orbitofrontal cortex.
A neuroimaging study with positron emission tomography found that the right caudate
nucleus had the largest change in glucose metabolism after patients had been treated with
paroxetine.[11] Recent SDM meta-analyses ofvoxel-based morphometry studies comparing
people with OCD and healthy controls have found people with OCD to have increased grey
matter volumes in bilateral lenticular nuclei, extending to the caudate nuclei, while
decreased grey matter volumes in bilateral dorsal medial frontal/anterior cingulate
gyri.[12][13] These findings contrast with those in people with other anxiety disorders, whoevince decreased (rather than increased) grey matter volumes in bilateral lenticular /
http://en.wikipedia.org/wiki/Dopaminehttp://en.wikipedia.org/wiki/Neuronshttp://en.wikipedia.org/wiki/Ventral_tegmental_areahttp://en.wikipedia.org/wiki/Substantia_nigrahttp://en.wikipedia.org/wiki/Association_cortexhttp://en.wikipedia.org/w/index.php?title=Caudate_nucleus&action=edit§ion=3http://en.wikipedia.org/w/index.php?title=Caudate_nucleus&action=edit§ion=4http://en.wikipedia.org/wiki/Hyperthymesiahttp://en.wikipedia.org/wiki/Temporal_lobehttp://en.wikipedia.org/w/index.php?title=Caudate_nucleus&action=edit§ion=5http://en.wikipedia.org/w/index.php?title=Caudate_nucleus&action=edit§ion=6http://en.wikipedia.org/wiki/Thalamushttp://en.wikipedia.org/w/index.php?title=Caudate_nucleus&action=edit§ion=7http://en.wikipedia.org/wiki/Excitatory_synapseshttp://en.wikipedia.org/wiki/Excitatory_synapseshttp://en.wikipedia.org/wiki/Positive_feedbackhttp://en.wikipedia.org/wiki/Cerebral_cortexhttp://en.wikipedia.org/wiki/Threshold_potentialhttp://en.wikipedia.org/w/index.php?title=Caudate_nucleus&action=edit§ion=8http://en.wikipedia.org/wiki/Obsessive_compulsive_disorderhttp://en.wikipedia.org/wiki/Thalamushttp://en.wikipedia.org/wiki/Orbitofrontal_cortexhttp://en.wikipedia.org/wiki/Neuroimaginghttp://en.wikipedia.org/wiki/Positron_emission_tomographyhttp://en.wikipedia.org/wiki/Paroxetinehttp://en.wikipedia.org/wiki/Signed_differential_mappinghttp://en.wikipedia.org/wiki/Voxel-based_morphometryhttp://en.wikipedia.org/wiki/Grey_matterhttp://en.wikipedia.org/wiki/Grey_matterhttp://en.wikipedia.org/wiki/Lenticular_nucleushttp://en.wikipedia.org/wiki/Medial_frontal_gyrushttp://en.wikipedia.org/wiki/Anterior_cingulate_cortexhttp://en.wikipedia.org/wiki/Grey_matterhttp://en.wikipedia.org/wiki/Lenticular_nucleushttp://en.wikipedia.org/wiki/Lenticular_nucleushttp://en.wikipedia.org/wiki/Grey_matterhttp://en.wikipedia.org/wiki/Anterior_cingulate_cortexhttp://en.wikipedia.org/wiki/Medial_frontal_gyrushttp://en.wikipedia.org/wiki/Lenticular_nucleushttp://en.wikipedia.org/wiki/Grey_matterhttp://en.wikipedia.org/wiki/Grey_matterhttp://en.wikipedia.org/wiki/Voxel-based_morphometryhttp://en.wikipedia.org/wiki/Signed_differential_mappinghttp://en.wikipedia.org/wiki/Paroxetinehttp://en.wikipedia.org/wiki/Positron_emission_tomographyhttp://en.wikipedia.org/wiki/Neuroimaginghttp://en.wikipedia.org/wiki/Orbitofrontal_cortexhttp://en.wikipedia.org/wiki/Thalamushttp://en.wikipedia.org/wiki/Obsessive_compulsive_disorderhttp://en.wikipedia.org/w/index.php?title=Caudate_nucleus&action=edit§ion=8http://en.wikipedia.org/wiki/Threshold_potentialhttp://en.wikipedia.org/wiki/Cerebral_cortexhttp://en.wikipedia.org/wiki/Positive_feedbackhttp://en.wikipedia.org/wiki/Excitatory_synapseshttp://en.wikipedia.org/wiki/Excitatory_synapseshttp://en.wikipedia.org/w/index.php?title=Caudate_nucleus&action=edit§ion=7http://en.wikipedia.org/wiki/Thalamushttp://en.wikipedia.org/w/index.php?title=Caudate_nucleus&action=edit§ion=6http://en.wikipedia.org/w/index.php?title=Caudate_nucleus&action=edit§ion=5http://en.wikipedia.org/wiki/Temporal_lobehttp://en.wikipedia.org/wiki/Hyperthymesiahttp://en.wikipedia.org/w/index.php?title=Caudate_nucleus&action=edit§ion=4http://en.wikipedia.org/w/index.php?title=Caudate_nucleus&action=edit§ion=3http://en.wikipedia.org/wiki/Association_cortexhttp://en.wikipedia.org/wiki/Substantia_nigrahttp://en.wikipedia.org/wiki/Ventral_tegmental_areahttp://en.wikipedia.org/wiki/Neuronshttp://en.wikipedia.org/wiki/Dopamine7/27/2019 In Neuroanatomy
5/42
caudate nuclei, while also decreased grey matter volumes in bilateral dorsal medial
frontal/anterior cingulate gyri.[13]
Hypophyseal portal system
Vein: Hypophyseal portal system
Latin venae portales hypophysiales
The hypophyseal portal system is the system of blood vessels that link the hypothalamus
and the anterior pituitary in the brain.
It allows endocrine communication between the two structures : the hypothalamus secretes
releasing and inhibitory hormones in the portal system such as corticotropin-releasing
hormone or thyrotropin-releasing hormone, and they are received by the anterior pituitary.
Using these, the anterior pituitary is able to fulfill its function of regulating the other
endocrine glands.
Hypophysiotropic peptides released near the median eminence are transported to the
anterior pituitary, where they exert their physiologic effects. Branches from the internal
carotid artery provide the blood supply to the pituitary. The superior hypophyseal arteries
form the primary capillary plexus that supplies blood to the median eminence. From this
capillary network, the blood is drained in long hypophyseal portal veins into the secondaryplexus. The hypophysiotropic peptides released at the median eminence enter the primary
plexus capillaries. From there, they are transported to the anterior pituitary via the long
hypophyseal portal veins to the secondary plexus. The secondary plexus is a network of
fenestrated sinusoid capillaries that provides the blood supply to the anterior pituitary. The
cells of the anterior pituitary express specific G protein-coupled receptors that bind the
neuropeptides, activating intracellular second-messenger cascades that produce the release
of anterior pituitary hormones. [1]
It is one of the portal systems of circulation of the human body; that is, it involves two
capillary beds connected in series by venules. One other such system is the hepatic portal
system.[2]
[edit]
Hormone transport
Mechanism for hormone transport via hypothalamoportal vessels:
cells regulated by different nuclei in the hypothalamus, i.e., neurons that release
neurotransmitters as hormones in the connective link between the pituitary and the
brain. Hypothalamic hormones stimulate the release of the respective hormone
from the anterior pituitary gland.
ligands (in this case, hormones released by the hypothalamus to activate hormone release
from the anterior pituitary) are picked up by blood vessels, then taken to the
anterior pituitary where they are broken down and released back into blood vessels
http://en.wikipedia.org/wiki/Medial_frontal_gyrushttp://en.wikipedia.org/wiki/Medial_frontal_gyrushttp://en.wikipedia.org/wiki/Anterior_cingulate_cortexhttp://en.wikipedia.org/wiki/Latinhttp://en.wikipedia.org/wiki/Latinhttp://en.wikipedia.org/wiki/Blood_vesselhttp://en.wikipedia.org/wiki/Hypothalamushttp://en.wikipedia.org/wiki/Anterior_pituitaryhttp://en.wikipedia.org/wiki/Brainhttp://en.wikipedia.org/wiki/Endocrine_systemhttp://en.wikipedia.org/wiki/Hormoneshttp://en.wikipedia.org/wiki/Corticotropin-releasing_hormonehttp://en.wikipedia.org/wiki/Corticotropin-releasing_hormonehttp://en.wikipedia.org/wiki/Thyrotropin-releasing_hormonehttp://en.wikipedia.org/wiki/Hormone_receptorhttp://en.wikipedia.org/wiki/Median_eminencehttp://en.wikipedia.org/wiki/Portal_system_of_circulationhttp://en.wikipedia.org/wiki/Capillaryhttp://en.wikipedia.org/wiki/Venulehttp://en.wikipedia.org/wiki/Hepatic_portal_systemhttp://en.wikipedia.org/wiki/Hepatic_portal_systemhttp://en.wikipedia.org/w/index.php?title=Hypophyseal_portal_system&action=edit§ion=1http://en.wikipedia.org/wiki/Neuronshttp://en.wikipedia.org/wiki/Neurotransmittershttp://en.wikipedia.org/wiki/Ligand_(biochemistry)http://en.wikipedia.org/wiki/File:Grays_pituitary.pnghttp://en.wikipedia.org/wiki/Ligand_(biochemistry)http://en.wikipedia.org/wiki/Neurotransmittershttp://en.wikipedia.org/wiki/Neuronshttp://en.wikipedia.org/w/index.php?title=Hypophyseal_portal_system&action=edit§ion=1http://en.wikipedia.org/wiki/Hepatic_portal_systemhttp://en.wikipedia.org/wiki/Hepatic_portal_systemhttp://en.wikipedia.org/wiki/Venulehttp://en.wikipedia.org/wiki/Capillaryhttp://en.wikipedia.org/wiki/Portal_system_of_circulationhttp://en.wikipedia.org/wiki/Median_eminencehttp://en.wikipedia.org/wiki/Hormone_receptorhttp://en.wikipedia.org/wiki/Thyrotropin-releasing_hormonehttp://en.wikipedia.org/wiki/Corticotropin-releasing_hormonehttp://en.wikipedia.org/wiki/Corticotropin-releasing_hormonehttp://en.wikipedia.org/wiki/Hormoneshttp://en.wikipedia.org/wiki/Endocrine_systemhttp://en.wikipedia.org/wiki/Brainhttp://en.wikipedia.org/wiki/Anterior_pituitaryhttp://en.wikipedia.org/wiki/Hypothalamushttp://en.wikipedia.org/wiki/Blood_vesselhttp://en.wikipedia.org/wiki/Latinhttp://en.wikipedia.org/wiki/Anterior_cingulate_cortexhttp://en.wikipedia.org/wiki/Medial_frontal_gyrushttp://en.wikipedia.org/wiki/Medial_frontal_gyrus7/27/2019 In Neuroanatomy
6/42
hypothalamoportal vessels act as a local route for blood flow directly from the
hypothalamus to the anterior pituitary.
Medication Summary
The goals of pharmacotherapy are to reduce morbidity and to prevent complications.
Dopamine agonists
Class Summary
These agents directly stimulate postsynaptic dopamine receptors. Dopaminergic neurons in
tuberoinfundibular processes modulate the secretion of prolactin from the anterior pituitary
by secreting a prolactin inhibitory factor, believed to be dopamine
Bromocriptine (Parlodel)
Semisynthetic ergot alkaloid derivative; strong dopamine D2-receptor agonist; partialdopamine D1-receptor agonist. Inhibits prolactin secretion with no effect on other pituitary
hormones. May be given with food to minimize possibility of GI irritation.
Hyperprolactinemia (Parlodel)
Initial: 1.25-2.5 mg PO qDay
May increase by 2.5 mg/day q2-7Days
Usual therapeutic dosage 5-7.5 mg/day, ranges from 2.5-15 mg/day
Up to 30 mg/day has been used in some patients with amenorrhea &/or galactorrhea
Parkinson Disease (Parlodel)
1.25 mg PO q12hr
May increase dose by 2.5 mg/day q2-4Weeks
Safety >100 mg/day not established
Acromegaly (Parlodel)
1.25-2.5 mg PO qHS for 3 days
May increase by 1.25-2.5 mg/day at q3-7Days
Not to exceed 100 mg/day
Diabetes (Cycloset)
Quick release formulation (Cycloset) is the only bromocriptine product indicated for
diabetes mellitus type 2 as adjunct to diet and exercise to improve glycemic control
Initial dose: 1 tablet (0.8 mg) PO qDay increased weekly by 1 tablet until maximal tolerated
daily dose of 1.6-4.8 mg is achieved
http://reference.medscape.com/drug/parlodel-bromocriptine-343124http://reference.medscape.com/drug/parlodel-bromocriptine-3431247/27/2019 In Neuroanatomy
7/42
Take within 2 hours after waking in the morning with food
Note: Cycloset is not indicated for hyperprolactinemia, Parkinson disease, or acromegaly
Neuroleptic Malignant Syndrome (Off-label)
2.5-5 mg PO 2-3 times/day; not to exceed 45 mg/day
Administration: take with food
Hepatic Impairment
Dose adjustment may be necessary; there are no guidelines
Mechanism of Action
Semisynthetic ergot alkaloid, dopamine receptor agonist, inhibits prolactin secretion, and
lowers blood levels of growth hormone in acromegaly
Quick-release formulation of bromocriptine (Cycloset) is thought to act on circadian
neuronal activities within the hypothalamus to reset abnormally elevated hypothalamic
drive for increased plasma glucose, triglyceride, and free fatty acid levels in fasting and
postprandial states in patients with insulin-resistant
Pharmacokinetics
Half-life elimination: 4-4.5 hr (initial phase); 8-20 hr (terminal phase)
Excretion: 85% feces (via biliary elimination); urine (2.5-5.5%)
Protein bound: 90-96% (to albumin)
Peak plasma time: 1-3 hr
Vd: 61L
Absorption: 28% from GI tract
Bioavailability: 28% (parlodel); 65-95% (cycloset)
Metabolism: Completely in liver, principally by hydrolysis of the amide bond to produce
lysergic acid and a peptide fragment
Cabergoline (Dostinex)
Semisynthetic ergot alkaloid derivative; strong dopamine D2-receptor agonist with low
affinity for D1 receptors.
Hyperprolactinemic Disorders of Either Idiopathic or Pituitary Adenoma Origin
Initital:0.25 mg 2 times per week PO
May increase by 0.25 mg q4Weeks (or longer) up to 1 mg 2 times per week
Pharmacology
http://reference.medscape.com/drug/dostinex-cabergoline-342876http://reference.medscape.com/drug/dostinex-cabergoline-3428767/27/2019 In Neuroanatomy
8/42
Half-life:63-69 hr
Distribution
High levels in pituitary (100x of plasma)
Peak Plasma: 30-70 pg/mL following single oral doses of 0.5-1.5 mg
Excretion
Urine: 22%
Feces: 60%
Other Information
Protein Bound: 40-42%
Metabolism: extensively hydrolyzed
Renal Clearance: 0.08 L/min
Mechanism of Action
Dopamine receptor agonist with high affinity for D2 receptors, thereby inhibiting prolactin
release
Quinagolide (Norprolac)
Pituitary selective dopamine-2 receptor agonist used in cases of bromocriptine resistance or
intolerance. Used in the UK, not available in US.
7/27/2019 In Neuroanatomy
9/42
Medication Summary
Treatment for diabetes insipidus (DI) varies with the form of the disorder. In central DI and
most cases of gestational DI, the primary problem is a deficiency of antidiuretic hormone
(ADH)also known as arginine vasopressin (AVP)and therefore, physiologic replacement
with desmopressin is usually effective. A nonhormonal drug can be used if response is
incomplete or desmopressin is too expensive.
Desmopressin has no role in the treatment of nephrogenic DI or primary polydipsia.
Nonhormonal drugs usually are more effective in treating nephrogenic DI.
Vasopressin-Related Hormones
Class Summary
In patients with central DI, replacement of endogenous ADH with exogenous hormones
prevents complications of DI and reduces morbidity.
View full drug information
Desmopressin (DDAVP, Stimate)
Desmopressin is a synthetic analogue of ADH with potent antidiuretic activity but no
vasopressor activity.
View full drug information
Vasopressin (Pitressin)
Vasopressin has vasopressor and ADH activity. It increases water resorption at collecting
ducts (ADH effect). At high doses, it also promotes smooth muscle contraction throughoutthe vascular bed of renal tubular epithelium (vasopressor effects). However,
vasoconstriction is also increased in splanchnic, portal, coronary, cerebral, peripheral,
pulmonary, and intrahepatic vessels.
Antidiabetics, Sulfonylureas
Class Summary
The hypoglycemic agent chlorpropamide helps to relieve diuresis in patients with DI.
View full drug information
Chlorpropamide
Chlorpropamide promotes renal response to ADH.
Anticonvulsants
Class Summary
Certain antiepileptic drugs, such as carbamazepine, have proven helpful in DI.
View full drug information
Carbamazepine (Tegretol, Carbatrol, Equetro)
http://reference.medscape.com/drug/ddavp-stimate-desmopressin-342819http://reference.medscape.com/drug/ddavp-stimate-desmopressin-342819http://reference.medscape.com/drug/adh-pitressin-vasopressin-342073http://reference.medscape.com/drug/adh-pitressin-vasopressin-342073http://reference.medscape.com/drug/diabinese-chlorpropamide-342704http://reference.medscape.com/drug/diabinese-chlorpropamide-342704http://reference.medscape.com/drug/tegretol-xr-equetro-carbamazepine-343005http://reference.medscape.com/drug/tegretol-xr-equetro-carbamazepine-343005http://reference.medscape.com/drug/tegretol-xr-equetro-carbamazepine-343005http://reference.medscape.com/drug/tegretol-xr-equetro-carbamazepine-343005http://reference.medscape.com/drug/diabinese-chlorpropamide-342704http://reference.medscape.com/drug/diabinese-chlorpropamide-342704http://reference.medscape.com/drug/adh-pitressin-vasopressin-342073http://reference.medscape.com/drug/adh-pitressin-vasopressin-342073http://reference.medscape.com/drug/ddavp-stimate-desmopressin-342819http://reference.medscape.com/drug/ddavp-stimate-desmopressin-3428197/27/2019 In Neuroanatomy
10/42
Carbamazepine possibly ameliorates DI by promoting the release of ADH. It is not useful in
nephrogenic DI and generally is not a first-line drug.
Diuretics, ThiazideClass Summary
Diuretics may reduce flow to the ADH-sensitive distal nephron.
View full drug information
Hydrochlorothiazide (Microzide)
Hydrochlorothiazide is a thiazide diuretic that decreases urinary volume in the absence of
ADH. It may induce mild volume depletion and cause proximal salt and water retention,
thereby reducing flow to the ADH-sensitive distal nephron. Its effects are additive to those
of other agents.
Nonsteroidal Anti-inflammatory Agents (NSAIDs)
Class Summary
The mechanism of action of NSAIDs is not known, but these agents may act by inhibiting
prostaglandin synthesis.
View full drug information
Indomethacin (Indocin)
Inhibition of prostaglandin synthesis reduces the delivery of solute to distal tubules,
reducing urine volume and increasing urine osmolality. Indomethacin is usually used in
nephrogenic DI.
View full drug information
Ibuprofen (Caldolor, Advil, Motrin)
Inhibition of prostaglandin synthesis reduces the delivery of solute to distal tubules,
reducing urine volume and increasing urine osmolality. Ibuprofen is usually used in
nephrogenic DI.
View full drug information
Naproxen (Naprosyn, Naprelan, Aleve, Anaprox)
View full drug information
Diclofenac (Voltaren, Cataflam XR, Zipsor, Cambia)
View full drug informationKetoprofen
http://reference.medscape.com/drug/microzide-hydrodiuril-hydrochlorothiazide-342412http://reference.medscape.com/drug/microzide-hydrodiuril-hydrochlorothiazide-342412http://reference.medscape.com/drug/indocin-indomethacin-343290http://reference.medscape.com/drug/indocin-indomethacin-343290http://reference.medscape.com/drug/advil-motrin-ibuprofen-343289http://reference.medscape.com/drug/advil-motrin-ibuprofen-343289http://reference.medscape.com/drug/aleve-anaprox-naproxen-343296http://reference.medscape.com/drug/aleve-anaprox-naproxen-343296http://reference.medscape.com/drug/voltaren-xr-cataflam-diclofenac-343284http://reference.medscape.com/drug/voltaren-xr-cataflam-diclofenac-343284http://reference.medscape.com/drug/ketoprofen-343291http://reference.medscape.com/drug/ketoprofen-343291http://reference.medscape.com/drug/ketoprofen-343291http://reference.medscape.com/drug/ketoprofen-343291http://reference.medscape.com/drug/voltaren-xr-cataflam-diclofenac-343284http://reference.medscape.com/drug/voltaren-xr-cataflam-diclofenac-343284http://reference.medscape.com/drug/aleve-anaprox-naproxen-343296http://reference.medscape.com/drug/aleve-anaprox-naproxen-343296http://reference.medscape.com/drug/advil-motrin-ibuprofen-343289http://reference.medscape.com/drug/advil-motrin-ibuprofen-343289http://reference.medscape.com/drug/indocin-indomethacin-343290http://reference.medscape.com/drug/indocin-indomethacin-343290http://reference.medscape.com/drug/microzide-hydrodiuril-hydrochlorothiazide-342412http://reference.medscape.com/drug/microzide-hydrodiuril-hydrochlorothiazide-3424127/27/2019 In Neuroanatomy
11/42
Inhibition of prostaglandin synthesis reduces the delivery of solute to distal tubules,
reducing urine volume and increasing urine osmolality.
Diuretics, Potassium-SparingClass Summary
Diuretics may reduce flow to the ADH-sensitive distal nephron.
View full drug information
Amiloride
Amiloride is a potassium-sparing diuretic. Thus, the risk of hypokalemia is decreased when
amiloride is used in combination with hydrochlorothiazide. In addition, the 2 agents are
synergistic with respect to antidiuresis.
http://reference.medscape.com/drug/midamor-amiloride-342406http://reference.medscape.com/drug/midamor-amiloride-342406http://reference.medscape.com/drug/midamor-amiloride-342406http://reference.medscape.com/drug/midamor-amiloride-3424067/27/2019 In Neuroanatomy
12/42
Desmopressin (trade names: DDAVP, DesmoMelt, Stimate, Minirin) is a synthetic
replacement for vasopressin, the hormone that reduces urine production. It may be taken
nasally, intravenously, or as an oral or sublingual tablet. Doctors prescribe desmopressin
most frequently for treatment ofdiabetes insipidus, bedwetting, or nocturia.
Chemistry
Desmopressin (1-desamino-8-D-arginine vasopressin) is a modified form of the normal
human hormone arginine vasopressin, a peptide containing nine amino acids.
Compared to vasopressin, desmopressin's first amino acid has been deaminated, and the
arginine at the eighth position is in the dextro rather than the levo form (see
stereochemistry).
[edit]
Mode of action
Desmopressin works by limiting the amount of water that is eliminated in the urine.
Desmopressin binds to V2 receptors in renal collecting ducts, increasing water reabsorption.It also stimulates release ofvon Willebrand factor from endothelial cells by acting on the V2
receptor.
Desmopressin is degraded more slowly than recombinant vasopressin, and requires less
frequent administration. In addition, it has little effect on blood pressure, while vasopressin
may cause arterial hypertension.
[edit]
Clinical uses
[edit]
Nocturnal EnuresisDoctors prescribe desmopressin frequently for treatment. It is usually in the form of
desmopressin acetate, DDAVP. Patients taking DDAVP are 4.5 times more likely to sleep
without disruption than with placebo. [1] [2] Examples of these situations are overnight
camp and sleepovers.
US drug regulators banned treating bedwetting with desmopressin nasal sprays after two
patients died and 59 other patients suffered seizures. The patients were using desmopressin
when they developed hyponatremia, an imbalance of the body's sodium levels. [3]
FDA regulators said that desmopressin tablets could still be considered safe for nocturnal
enuresis treatment, as long as the patient was otherwise healthy. Patients must stop taking
desmopressin if they become sick and have severe vomiting and diarrhea, fever, the flu, orsevere cold. They should also be very cautious during hot weather or following strenuous
exercise that may make them thirsty.
A healthy body needs to maintain a balance of water and salt (sodium). If sodium levels
become too low (hyponatremia) either as a result of increased water take-up or reduced
salt levels a person may have seizures and, in extreme cases, may die. [4]
[edit]
Coagulation disorders
Desmopressin can be used to promote the release ofvon Willebrand factor (with
subsequent increase in factor VIII survival secondary to vWF complexing) in patients with
coagulation disorders such as von Willebrand disease, mild hemophilia A (factor VIIIdeficiency), and thrombocytopenia. It can be used with uremic induced platelet dysfunction.
https://en.wikipedia.org/wiki/Chemical_synthesishttps://en.wikipedia.org/wiki/Vasopressinhttps://en.wikipedia.org/wiki/Hormonehttps://en.wikipedia.org/wiki/Urinehttps://en.wikipedia.org/wiki/Diabetes_insipidushttps://en.wikipedia.org/wiki/Nocturiahttps://en.wikipedia.org/wiki/Vasopressinhttps://en.wikipedia.org/wiki/Deaminationhttps://en.wikipedia.org/wiki/Argininehttps://en.wikipedia.org/wiki/Stereochemistryhttps://en.wikipedia.org/w/index.php?title=Desmopressin&action=edit§ion=2https://en.wikipedia.org/wiki/Arginine_vasopressin_receptor_2https://en.wikipedia.org/wiki/Kidneyhttps://en.wikipedia.org/wiki/Collecting_ducthttps://en.wikipedia.org/wiki/Von_Willebrand_factorhttps://en.wikipedia.org/wiki/Endothelial_cellhttps://en.wikipedia.org/wiki/Recombinant_DNAhttps://en.wikipedia.org/wiki/Blood_pressurehttps://en.wikipedia.org/wiki/Arterial_hypertensionhttps://en.wikipedia.org/w/index.php?title=Desmopressin&action=edit§ion=3https://en.wikipedia.org/w/index.php?title=Desmopressin&action=edit§ion=4https://en.wikipedia.org/wiki/Hyponatremiahttps://en.wikipedia.org/wiki/Nocturnal_enuresishttps://en.wikipedia.org/wiki/Nocturnal_enuresishttps://en.wikipedia.org/wiki/Sodiumhttps://en.wikipedia.org/wiki/Hyponatremiahttps://en.wikipedia.org/wiki/Seizureshttps://en.wikipedia.org/w/index.php?title=Desmopressin&action=edit§ion=5https://en.wikipedia.org/wiki/Von_Willebrand_factorhttps://en.wikipedia.org/wiki/Factor_VIIIhttps://en.wikipedia.org/wiki/Coagulationhttps://en.wikipedia.org/wiki/Von_Willebrand_diseasehttps://en.wikipedia.org/wiki/Hemophilia_Ahttps://en.wikipedia.org/wiki/Thrombocytopeniahttps://en.wikipedia.org/wiki/Thrombocytopeniahttps://en.wikipedia.org/wiki/Hemophilia_Ahttps://en.wikipedia.org/wiki/Von_Willebrand_diseasehttps://en.wikipedia.org/wiki/Coagulationhttps://en.wikipedia.org/wiki/Factor_VIIIhttps://en.wikipedia.org/wiki/Von_Willebrand_factorhttps://en.wikipedia.org/w/index.php?title=Desmopressin&action=edit§ion=5https://en.wikipedia.org/wiki/Seizureshttps://en.wikipedia.org/wiki/Hyponatremiahttps://en.wikipedia.org/wiki/Sodiumhttps://en.wikipedia.org/wiki/Nocturnal_enuresishttps://en.wikipedia.org/wiki/Nocturnal_enuresishttps://en.wikipedia.org/wiki/Hyponatremiahttps://en.wikipedia.org/w/index.php?title=Desmopressin&action=edit§ion=4https://en.wikipedia.org/w/index.php?title=Desmopressin&action=edit§ion=3https://en.wikipedia.org/wiki/Arterial_hypertensionhttps://en.wikipedia.org/wiki/Blood_pressurehttps://en.wikipedia.org/wiki/Recombinant_DNAhttps://en.wikipedia.org/wiki/Endothelial_cellhttps://en.wikipedia.org/wiki/Von_Willebrand_factorhttps://en.wikipedia.org/wiki/Collecting_ducthttps://en.wikipedia.org/wiki/Kidneyhttps://en.wikipedia.org/wiki/Arginine_vasopressin_receptor_2https://en.wikipedia.org/w/index.php?title=Desmopressin&action=edit§ion=2https://en.wikipedia.org/wiki/Stereochemistryhttps://en.wikipedia.org/wiki/Argininehttps://en.wikipedia.org/wiki/Deaminationhttps://en.wikipedia.org/wiki/Vasopressinhttps://en.wikipedia.org/wiki/Nocturiahttps://en.wikipedia.org/wiki/Diabetes_insipidushttps://en.wikipedia.org/wiki/Urinehttps://en.wikipedia.org/wiki/Hormonehttps://en.wikipedia.org/wiki/Vasopressinhttps://en.wikipedia.org/wiki/Chemical_synthesis7/27/2019 In Neuroanatomy
13/42
It is not effective in the treatment of hemophilia B (factor IX deficiency), severe hemophilia
A, or von Willebrand 2B.
[edit]
Diabetes insipidus
Desmopressin is used in the treatment of central diabetes insipidus (DI), to replaceendogenous ADH that is missing in the central nervous system type of this disorder
(decreased production of ADH from the posterior pituitary). It is also used in the diagnostic
workup for diabetes insipidus, in order to distinguish central from nephrogenic DI.
Radiation Treatment and Radiosurgery
If surgery is unable to remove the entire tumor, then radiation treatment may be necessary
to control the tumor and prevent it from growing. Radiation may also be an option for
patients who are medically unsuitable for surgery or do not want to have surgery.
Conventional radiation treatment directs a small number of radiation beams toward the
entire region around the sella turcica and pituitary gland. This technique results in a
significant area of normal tissue being included in the treatment field. To compensate for
this, conventional radiation treatment is given in daily doses over several weeks. Such
therapy is generally very effective in preventing the tumor from growing. For hormone-
producing tumors, it is also effective in gradually lowering the hormone levels over many
years. Despite the fact that with conventional radiotherapy the optic chiasm receives as
much radiation as does the tumor, the risks of visual complications are very low. However,
the same cannot be said about normal hormonal function. Since both the pituitary and the
hypothalamus (another important hormone control center) receive radiation during
treatment, nearly half the patients treated with conventional radiation will eventually
develop abnormally low hormone levels (hypopituitarism).
Radiosurgery is a new option for treating pituitary adenoma. By focusing the radiation on
only the tumor, this form of treatment minimizes the anatomical spread of radiation to
normal brain. Emerging data indicates that radiosurgery may be more effective than
conventional radiation in lowering abnormal hormone production, and does so over a
shorter time interval.
Most radiosurgery techniques, like surgery itself, require treatment to be delivered as a one-
time procedure. However, some of the unwanted side-ffects of radiation, including the most
feared, visual loss, may be accentuated by delivering the radiation all in one day rather than
over several sessions; this risk of radiation injury is greatest in those patients where the
pituitary is close to or involves the optic chiasm or hypothalamus. In higher risk patients, the
risk of injury to critical brain structures may be reduced by staging the radiosurgical ablation.
https://en.wikipedia.org/w/index.php?title=Desmopressin&action=edit§ion=6https://en.wikipedia.org/wiki/Neurogenic_diabetes_insipidushttps://en.wikipedia.org/wiki/Diabetes_insipidus#Diagnosishttps://en.wikipedia.org/wiki/Diabetes_insipidus#Diagnosishttps://en.wikipedia.org/wiki/Diabetes_insipidus#Diagnosishttps://en.wikipedia.org/wiki/Diabetes_insipidus#Diagnosishttps://en.wikipedia.org/wiki/Neurogenic_diabetes_insipidushttps://en.wikipedia.org/w/index.php?title=Desmopressin&action=edit§ion=67/27/2019 In Neuroanatomy
14/42
Overview
Tumors of the pituitary gland and sellar region represent approximately 10-15% of all brain
tumors,[1] of which the great majority in this region are pituitary adenomas. Pituitary
adenomas predominantly affect females between the third and sixth decades of life;
however, no age group is spared.[2] Pituitary adenomas are uncommon in the pediatric
population, but most tumors of childhood are clinically functioning adenomas and arethought to be more aggressive.[3]
Rates for pituitary tumors in the United States are slightly higher among black persons (2.92
per 100,000 person-years) than among white persons (1.82 per 100,000 person-years).[1]
Incidental adenomas can be found in nearly 10% of autopsied patients.[4, 5]
Comparatively, primary tumors of the neurohypophysis are rare, and in general, they are
similar to primary tumors of the central nervous system (CNS). The neurohypophysis,
however, is a common site for metastases.[6]
The following are histologic examples of the normal pituitary gland and a pituitary adenomafor comparison.
Histology of a normal anterior pituitary gland. The gland is formed by multiple cell types,
including basophilic, eosinophilic, and chromophobic cells (hematoxylin-eosin stain).
Normal pituitary versus pituitary adenoma. Note the delicate acinar pattern of a normal
pituitary gland (left), in contrast with disruption of the normal reticulin network in adenoma
(right) (Wilder's reticulin stain).
Classification
Numerous types of tumors may involve the pituitary gland and sellar region, reflecting the
complex anatomy of this area. These may be classified as shown in Table 1, below).
Table 1. Tumors and Tumorlike Lesions of the Pituitary Gland and Sellar Region (Open Table
in a new window)
Tumors of anterior pituitary Pituitary adenoma
Atypical adenoma
http://refimgshow%282%29/http://refimgshow%281%29/7/27/2019 In Neuroanatomy
15/42
Pituitary carcinoma
Spindle cell oncocytoma
Tumors of posterior pituitary Pituicytoma
Granular cell tumor
Gangliocytoma
Tumors of nonpituitary origin Craniopharyngioma
Meningioma
Chordoma
Langerhans cell histiocytosis
Metastases
Cystic lesions Rathkes cleft cyst
Arachnoid cyst
Epidermoid/dermoid cyst
7/27/2019 In Neuroanatomy
16/42
Inflammatory lesions Lymphocytic hypophysitis
Granulomatous hypophysitis
Sarcoidosis
As noted earlier, the most common tumors, by far, are the pituitary adenomas. In addition
to tumors, a variety of nonneoplastic lesions may affect the pituitary gland, bringing a
number of processes into the differential diagnosis of the tumors involving this region.
The more common lesion types are defined as follows:
Pituitary adenomas are benign epithelial tumors derived from intrinsic cells of the
adenohypophysis
Pituitary carcinomas are characterized by the presence of either craniospinal
dissemination or systemic metastases[7]
Spindle cell oncocytoma of the adenohypophysis is a rare primary tumor that may be
derived from the follicle-stellate cells of the anterior pituitary gland[8]
Pituicytomas are a subtype of low-grade astrocytoma that originates in the posterior
pituitary or infundibulum; in the past, these tumors were designated as posterior
pituitary astrocytomas or infundibulomas[9] ; pituicytomas are believed to originate
from pituicytes, the intrinsic glial cells of the posterior pituitary gland
Granular cell tumors are glial tumors that arise either in the pituitary stalk or posterior
pituitarythey are usually incidental tumors found in adults at autopsies and only
rarely present as symptomatic masses (there are about 60 reported cases in the
literature[10] ); granular cell tumors of the sella are also known as choristoma of the
neurohypophysis, granular cell pituicytoma, granular cell myoblastoma, and granular
cell tumorette
Craniopharyngiomas represent 12% of all intracranial neoplasms and about 10% of the
tumors of the sellar region[11] ; they are histogenetically related to Rathkes cleft
and derive from the pituitary anlagen; although the majority of craniopharyngiomas
differ markedly from Rathkes cleft cysts, rare tumors demonstrating features of
both have been described[12]
Inflammatory hypophysitis is a rare disorder of the pituitary gland characterized by focal
or diffuse inflammatory infiltration and ultimate destruction of the gland.
See also Pituitary Tumors, Pituitary Macroadenomas, Pituitary Microadenomas, Pituitary
Apoplexy, and Pituitary Disease and Pregnancy.
Anterior Pituitary Gland Tumors Pituitary Adenomas
In this section the general characteristics of pituitary adenomas are discussed, followed by
separate sections on subtypes of pituitary adenomas, atypical adenomas, pituitary
carcinomas, and spindle cell oncocytomas.
General characteristics of pituitary adenomas
http://emedicine.medscape.com/article/1157189-overviewhttp://emedicine.medscape.com/article/123223-overviewhttp://emedicine.medscape.com/article/126702-overviewhttp://emedicine.medscape.com/article/1198279-overviewhttp://emedicine.medscape.com/article/1198279-overviewhttp://emedicine.medscape.com/article/127650-overviewhttp://emedicine.medscape.com/article/127650-overviewhttp://emedicine.medscape.com/article/1198279-overviewhttp://emedicine.medscape.com/article/1198279-overviewhttp://emedicine.medscape.com/article/126702-overviewhttp://emedicine.medscape.com/article/123223-overviewhttp://emedicine.medscape.com/article/1157189-overview7/27/2019 In Neuroanatomy
17/42
Pituitary adenomas are classified clinically into 2 groups--clinically functioning adenomas
and clinically nonfunctioning adenomas--according to whether an endocrine syndrome is
present or absent. Most adenomas are functioning tumors; these include prolactin (PRL)
producing, growth hormone (GH)producing, adrenocorticotropic hormone (ACTH)
producing, and thyroid-stimulating hormone (TSH)producing adenomas (see Table 2,
below).[13]
Table 2. Surgical Frequency of Pituitary Adenoma Types at University of Virginia, 1992-2006*
(Open Table in a new window)
Pituitary Adenoma Type Frequency, %
ACTH-secreting adenomas
23
PRL-secreting adenomas 22
Null cell adenomas 19
Gonadotropin-secreting adenomas 18
GH-secreting adenomas 14
GH- and PRL-secreting adenomas 3TSH-secreting adenomas 1*
N = approximately 2600.
Includes silent corticotroph adenomas.
ACTH = adrenocorticotropic hormone; GH = growth hormone; PRL = prolactin; TSH = thyroid-
stimulating hormone.
Nonfunctioning adenomas
About one third of all pituitary adenomas are unassociated with either clinical or
biochemical evidence of hormone excess.[14] In this group are included adenomas that
produce both follicle-stimulating hormone (FSH) and luteinizing hormone (LH), the less
differentiated null cell adenomas, and silent adenomas. These clinically nonfunctioning
adenomas commonly present with signs and symptoms related to local mass effect, such as
headaches, neurologic deficits of the cranial nerves (including visual field disturbances), and
mild hyperprolactinemia due to pituitary stalk compression ("stalk effect").
Classifications based on size, anatomic features, histologic patterns, and hormone content
On the basis of size and anatomic features, adenomas are divided into microadenomas
(tumors < 1 cm in diameter) and macroadenomas (tumors >1 cm in diameter). Giant
adenomas (tumors > 4 cm) may occur but are rare. Macroadenomas show an increased
tendency toward suprasellar extension, gross invasion, and recurrence (see the following
image). A radiologic classification proposed by Hardy[15] is the one most often used in
clinical practice.
7/27/2019 In Neuroanatomy
18/42
Neuroimaging of pituitary adenoma. T1-weighted magnetic resonance image (MRI) without
(left) and with (right) contrast shows macroadenoma compressing optic chiasma.
Grossly, pituitary adenomas are soft lesions with a tan-brown discoloration.
Morphologically, they may show a variety of histologic patterns, including diffuse, papillary,
and trabecular arrangements similar to those of other neuroendocrine tumors. Cytologically,
tumor cells may be acidophilic, basophilic, or chromophobic; however, these tinctorial
characteristics do not identify specific adenoma types (see the images below).
Histology of a normal anterior pituitary gland. The gland is formed by multiple cell types,
including basophilic, eosinophilic, and chromophobic cells (hematoxylin-eosin stain).
Normal pituitary versus pituitary adenoma. Note the delicate acinar pattern of a normal
pituitary gland (left), in contrast with disruption of the normal reticulin network in adenoma
(right) (Wilder's reticulin stain).
Histology of pituitary adenoma. Pituitary adenomas may display several typical
neuroendocrine patterns and have different tinctorial features of tumor cells, including
basophilic, eosinophilic and chromophobic appearances. These cytologic and architectural
qualities, however, are not diagnostic of specific subtypes of adenoma.
Pituitary adenomas are also classified according to the hormone content of the tumor cells
as determined by immunohistochemistry (IHC). This classification provides significant
information for clinical practice.[16] In a few tumors, however, analysis of the adenoma's
ultrastructural aspects is necessary.[17] In this article, we follow the guidelines andclassification scheme for pituitary gland tumors that was released by the World Health
http://refimgshow%284%29/http://refimgshow%283%29/http://refimgshow%282%29/http://refimgshow%281%29/http://refimgshow%284%29/7/27/2019 In Neuroanatomy
19/42
Organization (WHO) in 2004 (see Table 3, below).[18]
Table 3. Morphofunctional Classification of Pituitary Adenomas (Open Table in a new
window)
Clinical Presentation Pituitary Adenoma TypeACTH-secreting adenomas Corticotroph adenoma
PRL-secreting adenomas Sparsely granulated lactotroph adenoma
Densely granulated lactotroph adenoma
GH-secreting adenomas Densely granulated somatotroph adenoma
Sparsely granulated somatotroph adenoma
GH- and PRL-secreting adenomas Mixed GH- and PRL-cell adenoma
Mammosomatotroph-cell adenoma
Acidophilic stem-cell adenoma 3
TSH-secreting adenomas Thyrotroph adenoma
Gonadotropin-secreting adenomas Gonadotroph adenoma
Nonfunctioning adenomas Null-cell adenoma
Oncocytoma
Silent adenomas Silent corticotroph adenoma (subtypes I and II)
Silent adenoma subtype III
7/27/2019 In Neuroanatomy
20/42
ACTH = adrenocorticotropic hormone; GH = growth hormone; PRL = prolactin; TSH = thyroid-
stimulating hormone.
Tumorigenesis
The mechanisms involved in human pituitary tumorigenesis and tumor progression are stillnot well understood. Pituitary adenomas appear to develop through a multistep and
multicausal process to which endocrine factors, hereditary genetic disposition, and specific
somatic mutations may all contribute. An extended review of the mechanisms of pituitary
tumorigenesis is beyond the scope of this article.
Pituitary adenomas arise mostly in a sporadic manner, and only a minority occur as part of
hereditary or familial syndromes.[19] The large majority of adenomas are monoclonal
expansions, as demonstrated by X-chromosomal inactivation analysis.[20] Hereditary
conditions associated with development of pituitary adenomas include the following:
Multiple endocrine neoplasia type 1 (MEN-1), linked to somatic mutations of the MEN-1
gene
Carney complex, linked to mutations of the tumor suppressor gene PRKAR1A
McCune-Albright syndrome, linked to activating mutation of the gsp oncogene (discussed
below)
A few other rare familial syndromes are also associated with pituitary adenomas:
Pituitary adenoma predisposition (PAP), associated with a germline mutation of the AIP
(aryl hydrocarbon receptor-interacting protein) gene
Isolated familial somatotrophinoma (IFS), associated with a loss of heterozygosity at the
11q13 locus but not with the MEN-1 gene
Familial isolated pituitary adenoma (FIPA), for which a single genetic alteration has not
been characterized, although mutations of the AIP gene have been reported to
occur in about 15% of families[21]
In the majority of sporadic adenomas, however, the primary genetic defect remains
unknown. A number of oncogenes and tumor suppressor genes have been recognized as
potential participants in the tumorigenesis of pituitary adenomas.
The most commonly found genetic alteration in sporadic tumors is an activating mutation of
the gsp gene, an oncogene mostly identified in GH-cell adenomas.[22, 23, 24] The gsp
mutation has been identified in about 40% of GH-secreting adenomas,[23, 24, 25] but it is
rare in other pituitary tumor subtypes, occurring in only 10% of clinically nonfunctioning
pituitary adenomas and 5% of corticotroph adenomas.[25]
Other oncogenes and tumor suppressor genes that have been shown to be linked to
pituitary tumorigenesis include the oncogene PTTG (pituitary tumor-transforming gene), the
proto-oncogene H-ras, and the tumor suppressor genes RB and TP53. However, it seems
that these genes are not directly associated with pituitary adenoma tumorigenesis but may
play a role during the progression and malignant transformation of these tumors.[26] For
details, readers may consult any of several outstanding reviews on the subject.
Pituitary Adenoma Subtypes
This section will discuss subtypes of pituitary adenomassuch as prolactin (PRL)secreting,
growth hormone (GH)secreting, mixed GH- and PRL-secreting, adrenocorticotropic
hormone (ACTH)secreting, thyroid-stimulating hormone (TSH)secreting, gonadotropin-
secreting adenomas, and null cell adenomas and oncocytomas, silent adenomas, and
http://emedicine.medscape.com/article/1093723-overviewhttp://emedicine.medscape.com/article/160000-overviewhttp://emedicine.medscape.com/article/1110016-overviewhttp://emedicine.medscape.com/article/1110016-overviewhttp://emedicine.medscape.com/article/160000-overviewhttp://emedicine.medscape.com/article/1093723-overview7/27/2019 In Neuroanatomy
21/42
plurihormonal adenomas.
Prolactin-secreting adenomas
PRL-secreting adenomas, or prolactinomas, account for nearly 80% of functioning adenomas
and about 4050% of all pituitary adenomas.[27, 28] However, most patients with
prolactinomas are treated clinically with dopamine agonists. Therefore, the frequency ofprolactinomas in surgical series tends to be smaller.
In women, the majority of prolactinomas are microadenomas and occur during the
reproductive age period, presenting with oligomenorrhea or amenorrhea, galactorrhea, and
infertility.[27, 28] In contrast, in men and elderly women, prolactinomas are usually
macroadenomas and are most commonly associated with symptoms of tumoral mass,
including headaches, neurologic defects, and visual loss.[28] Impotence and decreased libido
are also common symptoms of hyperprolactinemia in males. The diagnosis of a prolactinoma
is confirmed by sustained hyperprolactinemia and neuroradiologic evidence of a pituitary
tumor.[2, 27]
Histologically, prolactinomas are composed of medium-sized cells with chromophobic or
slightly acidophilic cytoplasm and a central, oval nucleus (see the image below); small
nucleoli can be present. Approximately 10-20% of cases show microcalcifications.
Calcifications and amyloid bodies, although frequently seen in prolactinomas, are not
pathognomonic of this type of adenoma.[29]
Prolactin (PRL)-secreting adenoma. Left: The cells show chromophobic cytoplasm and
central nuclei (hematoxylin-eosin stain). Right: Immunochemistry (IHC) shows reactivity for
PRL in a characteristic dotlike staining pattern located near the nucleus (PRL-IHC stain).
Immunohistochemistry (IHC) shows reactivity for PRL in a very characteristic pattern of
staining, with localization near the nucleus in a dotlike pattern, also known as a Golgi
pattern.[29] On ultrastructural analysis, prolactinomas may be divided into densely and
sparsely granulated variants, although the clinical significance of this distinction is
questionable.[13, 29]
Sparsely granulated PRL cell adenomas are the most common tumors, and their cells
resemble actively secreting lactotrophs of the normal pituitary gland. The adenoma cells are
characterized by a prominent rough endoplasmic reticulum (RER) network, conspicuous
Golgi complexes, and a sparse number of small (150-300 nm) secretory granules. Misplaced
exocytosis (ie, granule extrusions on the lateral cell surfaces) is typical of these tumors.
As noted above, most patients with prolactinomas are treated to some degree with
dopamine agonists. These drugs act directly on the tumor cells, inducing atrophy of
lactotrophs and resultant tumor shrinkage.[27, 28] Histologically, tumors from patients
previously treated with such drugs are composed of smaller tumor cells, with shrinkage of
the cytoplasm and hyperchromasia of the nuclei, in addition to various degrees of
perivascular and interstitial tumoral fibrosis.[30, 31]
Growth hormonesecreting adenomas
http://refimgshow%285%29/7/27/2019 In Neuroanatomy
22/42
GH-secreting adenomas account for about 20% of pituitary adenomas. Patients present with
signs and symptoms ofacromegaly, gigantism, or both, as well as high serum GH and
insulinlike growth factor I (IGF-I) levels.[2] Acromegaly affects both sexes with similar
incidence, and the mean age at diagnosis is 4045 years.[32]
Symptoms of acromegaly are usually slowly progressive, with an average delay ofapproximately 10 years before diagnosis.[32] Less commonly, adenomas arise in children
and adolescents before the epiphyseal closure of the long bones, resulting in gigantism.
Most acromegalic patients have macroadenomas when first diagnosed; many of these
lesions show suprasellar expansion and parasellar invasion.[33] Consequently, symptoms
secondary to an expanding tumor mass, including headaches and visual field defects, may
also be present.
In about 30-50% of patients, co-secretion of PRL with GH by the tumor results in signs and
symptoms of hyperprolactinemia.[32, 33] Mixed GH- and PRL-secreting tumors are discussed
below.
Densely vs sparsely granulated GH cell adenomas
Histologically, GH-secreting adenomas are either eosinophilic or chromophobic on
hematoxylin and eosin (H&E) staining. These histologic attributes reflect the amount of
secretory granules present in the cell cytoplasm and characterize the 2 types of GH cell
adenomas--namely, densely granulated and sparsely granulated.
Densely granulated adenomas are characterized by eosinophilic tumor cells, with the
cytoplasm showing considerable granularity and reflecting great numbers of secretory
granules seen at the ultrastructural level. The nucleus tends to be central and oval, with
prominent nucleoli (see the image below).
Growth hormone (GH)-secreting adenoma. Top left: Densely granulated GH-secreting
adenomas show large cells with an eosinophilic, granular cytoplasm and a central nucleus
with prominent nucleoli (hematoxylin-eosin stain). Top right: The tumor shows intense and
diffuse immunostain for GH (GH-immunohistochemistry [IHC] stain). Bottom left: The
ultrastructure exhibits well-developed organelles and abundant large secretory granules.
Bottom right: A strong immunostain for transcription factor Pit-1 is typically seen in these
adenomas (Pit-1-IHC stain).
Sparsely granulated GH cell adenomas are composed of smaller tumor cells, with
chromophobic cytoplasm and an eccentric nucleus. In the cytoplasm, paranuclear
eosinophilic structures (fibrous bodies) are seen.[34] These structures represent
accumulations of intermediate filaments and tubular formations at the ultrastructural level
and are strongly immunoreactive for cytokeratin (see the following image).
http://emedicine.medscape.com/article/116366-overviewhttp://emedicine.medscape.com/article/925446-overviewhttp://refimgshow%286%29/http://emedicine.medscape.com/article/925446-overviewhttp://emedicine.medscape.com/article/116366-overview7/27/2019 In Neuroanatomy
23/42
Growth hormone (GH)-secreting adenoma. Top left: Sparsely granulated GH-cell adenomas
are characteristically more chromophobic than densely granulated ones (hematoxylin-eosin
stain). Top right: The immunostain for GH is heterogeneous and less prominent than with
densely granulated adenomas (GH-immunohistochemistry [IHC] stain). Bottom left:
Cytokeratin immunostaining highlights fibrous bodies (FBs) typically seen in these sparsely
granulated tumors (cytokeratin-IHC stain). Bottom right: The ultrastructure of sparselygranulated GH cells displays sparse neurosecretory granules and typical FBs.
IHC staining shows a variable degree of GH immunoreactivity (see the image above). In
densely granulated adenomas, GH immunostain diffusely occupies the entire cytoplasm of
the tumor cells and tends to be dispersed diffusely within the entire tumor. By contrast, in
sparsely granulated adenomas, GH immunostain is focal within the tumor and tends to be
localized in a paranuclear distribution, similar to the Golgi pattern seen in
prolactinomas.[34]
A number of GH-secreting adenomas show secondary reactivity for other pituitary
hormones.[33, 35] Immunopositivity for PRL can be seen focally, even in patients without
clinical or biochemical evidence of hyperprolactinemia. Similarly, the presence ofimmunoreactivity for the glycoprotein hormones follicle-stimulating hormone (FSH),
luteinizing hormone (LH), and -TSH can be demonstrated in a number of GH-secreting
adenomas.[33]
Apart from the well-characterized mixed GH-/PRL-secreting adenomas (see below),
plurihormonal differentiation is not clinically symptomatic in the majority of cases.[36]
The 2 subtypes of GH cell adenomas--densely and sparsely granulated--are well
characterized by ultrastructural analysis.[13] Densely granulated adenomas are composed of
adenomatous cells that resemble the normal somatotrophs of the pituitary gland and are
characterized by a well-developed rough endoplasmic reticulum (RER) network, prominent
Golgi complexes, and numerous large (300-600 nm) secretory granules.
Sparsely granulated adenomas have fewer and smaller (100-250 nm) secretory granules. The
most characteristic feature of these adenomas is the presence of fibrous bodies, which
consist of an accumulation of intermediate filaments and tubular smooth-surfaced
endoplasmic reticulum (see the previous image).
The distinction between the 2 subtypes of GH cell adenomas is important in that the
subtypes tumors appear to have different clinical behavior. Sparsely granulated GH
adenomas exhibit more aggressive biologic behavior than densely granulated tumors do.[33,
37, 38] In addition, the response of tumors to adjuvant medical treatment also differs
according to the subtype of GH cell adenoma.[39]
http://refimgshow%287%29/http://refimgshow%287%29/7/27/2019 In Neuroanatomy
24/42
As with prolactinomas, medical therapy for acromegaly with somatostatin receptor ligands,
mainly octreotide, is common practice in endocrinology.[2, 40] However, in treated GH cell
adenomas, significant reduction of tumor cell size is not commonly seen; the most common
changes are varying degrees of perivascular and interstitial fibrosis.[41, 42]
Mixed GH- and PRL-secreting adenomasAs noted in the discussion of GH-secreting adenomas above), a large percentage of these
adenomas also secrete PRL. These tumors overall constitute about 8% of pituitary
adenomas.[43] Patients with such mixed tumors present signs and symptoms of both
acromegaly and hyperprolactinemia.[33] In this group of adenomas, 3 morphologic tumor
types can be identified: (1) mixed GH cell/PRL cell adenoma, (2) mammosomatotroph cell
adenoma, and (3) acidophilic stem cell adenoma.[33, 44]
Diagnosis of these adenomas requires a more complex IHC and ultrastructural analysis of the
tissues. Moreover, their distinction is of fundamental importance in that it has clinical and
prognostic implications. Both mixed GH cell/PRL cell adenomas and mammosomatotroph
adenomas tend to grow more slowly than acidophilic stem cell adenomas do.[43, 45] In theauthors' experience, these mixed tumors behave more aggressively than any pure GH-
secreting adenomas, and the surgical cure rate is lower.[33]
Mixed GH cell/PRL cell adenomas
The predominant clinical feature of mixed GH cell/PRL cell adenomas is acromegaly. Signs
and symptoms of hyperprolactinemia are not always apparent.
Morphologically, the tumors are similar to GH-secreting adenomas, with an eosinophilic or
chromophobic appearance. Immunostains are demonstrated for both GH and PRL, with
varying degrees of staining and distribution (see the first image below). The 2 cell types may
form small groups, or they may be scattered. At the ultrastructural level, these adenomas
are bimorphous tumors, consisting of 2 separate cell populations: (1) densely or sparsely
granulated GH cells and (2) PRL cells (see the second image below).[46]
Mixed growth hormone (GH)-/prolactin (PRL)-secreting adenoma. Top left and right:
Morphologically, mixed GH-/PRL-secreting adenoma may be indistinguishable from GH
adenoma (hematoxylin-eosin stain). Bottom left and right: Immunohistochemistry (IHC)
shows intensive reaction for GH (bottom left: GH-IHC stain) and dotlike PRL immunostain
(bottom right: PRL-IHC stain).
http://refimgshow%288%29/7/27/2019 In Neuroanatomy
25/42
Mixed growth hormone (GH)-/prolactin (PRL)-secreting adenoma. The ultrastructure of
mixed GH-/PRL-secreting adenoma shows bimorphous cell population with densely
granulated GH cells and PRL cells.Mammosomatotroph cell adenomas
Mammosomatotroph cell adenoma is rare, accounting for fewer than 2% of all pituitary
adenomas and about 8% of tumors associated with acromegaly.[43, 47, 48] Like mixed GH
cell/PRL cell adenomas, these tumors are associated with elevated circulating GH levels and
acromegaly; hyperprolactinemia is less common.
Histologically, these adenomas are acidophilic on H&E staining, and IHC demonstrates the
presence of GH and PRL in the cytoplasm of the same tumor cell. These findings have been
confirmed by double-labeling studies, as well as by immunoelectron microscopy.[47]
Ultrastructural analysis demonstrates a well-differentiated adenoma composed of a
monomorphous cell population that contains features of GH and PRL cells.[47] The tumor
cells are mostly similar to densely granulated GH cells, but with irregular secretory granules
of variable sizes (2002000 nm) and containing granule extrusions and extracellular deposits
of secretory material, a feature consistent with PRL cell differentiation (see the image
below).
Mammosomatotroph cell adenoma. The ultrastructure of mixed growth hormone (GH)-
/prolactin (PRL)-secreting adenoma shows a monomorphous cell population exhibiting largesecretory granules and granular extrusion figures (arrows).
http://refimgshow%289%29/http://refimgshow%2810%29/http://refimgshow%289%29/7/27/2019 In Neuroanatomy
26/42
Acidophilic stem cell adenomas
Acidophilic stem cell adenoma is very rare, representing only a small minority of GH-/PRL-
producing tumors.[33, 43] Unlike patients with the other 2 subtypes, most patients with this
tumor present with symptoms of hyperprolactinemia[45] ; acromegaly is uncommon, and
GH levels are often normal.
The majority of the tumors are rapidly growing macroadenomas with invasive features.
Because most of the patients have clinical features of hyperprolactinemia, the diagnosis is of
clinical importance in that these tumors may be mistaken for the more benign
prolactinomas.
By light microscopy, acidophilic stem cell adenomas are chromophobic, with focal oncocytic
changes of the cytoplasm. Immunoreactivity for PRL and, to a lesser extent, GH is present in
the cytoplasm of the same tumor cells.
Electron microscopy is necessary for precise identification of these adenomas.[13, 45] They
are composed of a single population of immature cells exhibiting features reminiscent of
both sparsely granulated GH cells and PRL cells. Oncocytic change, with the presence of
giant mitochondria, is characteristic of these adenomas.
Adrenocorticotropic hormonesecreting adenomas
ACTH-secreting adenomas associated with Cushing disease represent approximately 10-15%
of all adenomas.[49] Cushing disease has a peak incidence between the ages of 30 and 40
years and tends to be more frequent in females (3.5:1 female-to-male ratio).[50] In children,
Cushing disease is rare and tends to have a more aggressive clinical course and lower cure
rate.[51, 52] Cushing disease arising in prepubertal children is more common in males than
femalesthe opposite of the adult preponderance.[53] (See also Cushing Syndrome.) The
great majority of ACTH-secreting adenomas are microadenomas, and approximately 15% are
invasive at the time of surgery.[54]
On rare occasions, corticotroph cell hyperplasia may be the source of Cushing disease.
However, there is considerable controversy, from both clinical and pathologic viewpoints,
regarding this event.[55]
Histologically, ACTH-secreting adenomas are usually basophilic on H&E staining and are
often strongly positive with periodic acid-Schiff (PAS) staining (see the following image). The
cytoplasm is very granular, and the nucleus is large, with coarse chromatin and a prominent
nucleolus. Some degree of nuclear pleomorphism can be present. The cells have very
distinct cytoplasmic borders and tend to touch each other in a tilelike arrangement. Papillary
formations are very common.
Adrenocorticotropic hormone (ACTH)-secreting adenoma. Left: Corticotroph cell adenomas
are composed of large cells with angular, slightly basophilic cytoplasm and a large nucleus
(hematoxylin-eosin stain). Right: Immunohistochemistry (IHC) for ACTH shows intenseimmunoreactivity (ACTH-IHC stain).
http://emedicine.medscape.com/article/117365-overviewhttp://refimgshow%2811%29/http://emedicine.medscape.com/article/117365-overview7/27/2019 In Neuroanatomy
27/42
Occasionally, hyaline bundles that encircle the cytoplasm, yielding a "target cell"
appearance, are observed. These represent Crookes hyaline changes, which correspond to
the accumulation of cytokeratin intermediate filaments and appear to be a direct effect of
high serum levels of cortisol on pituitary cells.[56] Crookes changes are also present in the
normal pituitary gland of Cushing disease patients (see the image below) and in patients
with other pathologic or iatrogenic hypercortisolemic states.
Crooke's changes in the anterior pituitary gland of a patient with Cushing disease. Left:
Several "target cells" consistent with corticotroph cells with hyaline bundles in the
cytoplasm can be seen (hematoxylin-eosin stain). Right: Cytokeratin immunostain highlights
Crooke's changes in corticotroph cells (cytokeratin-immunohistochemistry [IHC] stain).IHC demonstrates the presence of ACTH with various degrees of immunoreactivity. In
addition, other peptides related to the proopiomelanocortin (POMC) precursor molecule,
including -lipotropin, -endorphin, and -melanocyte-stimulating hormone, are also
expressed by tumor cells.[57] In practice, demonstration of these related peptides is less
relevant than demonstration of ACTH. Immunostaining for cytokeratin shows accumulation
in the cytoplasm, either diffuse or forming Crookes changes (see the image above).
Ultrastructurally, ACTH-secreting adenomas are characterized by well-differentiated cells
that resemble normal corticotrophs.[55] The cells contain well-developed organelles,
including RER, smooth endoplasmic reticulum (SER), conspicuous Golgi complexes, and
numerous large (250500 nm) secretory granules. The secretory granules are often of
different shapes (eg, spherical or heart-shaped) and vary in electron density. Bundles of
intermediate filaments lying adjacent to the nucleus or forming large circles (Crookes
changes) are easily identified.
Ultrastructural analysis of clinically functioning ACTH-cell adenomas is not obligatory;
histologic and immunohistochemical studies are sufficient to provide an accurate diagnosis.
Thyroid-stimulating hormonesecreting adenomas
TSH-secreting, or thyrotroph cell, adenomas are the least frequent pituitary adenomas.[58]
Clinically, they may present with inappropriately elevated TSH levels and hyperthyroidism,
but these tumors may also arise in the setting of hypothyroidism or in clinically euthyroidpatients.[59] Most TSH-secreting adenoma are invasive macroadenomas.[59]
Histologically, thyrotroph cell adenomas are frequently chromophobic by light microscopy
and are composed of elongated, angular, or irregular cells. Some degree of desmoplasia is
commonly seen within the tumors, which causes a slight firm consistency.[58]
Immunostains usually reveal variable -TSH positivity. IHC is also commonly positive for the
alpha subunit (-SU) of the glycoproteins.
At the ultrastructural level, the cells are moderately differentiated, with scant RER network
and Golgi complexes.[13] Secretory granules are small (100200 nm), spherical, and evenly
electron dense, and they are typically lined up along the cytoplasmic membrane.
http://refimgshow%2812%29/7/27/2019 In Neuroanatomy
28/42
The diagnosis of TSH-secreting adenoma can be problematic if the clinical presentation and
TSH immunoreactivity are not convincing. In this situation, electron microscopy is
mandatory for appropriate diagnosis.
Gonadotropin-secreting adenomas
Gonadotropin-secreting adenomas, or gonadotroph adenomas, are adenomas that secretethe gonadotropins FSH and LH. Unlike other secreting adenomas, gonadotroph adenomas
do not usually cause a clinical syndrome related to hormone overproduction. The hormonal
production from these tumors is inefficient, and the detection of excess hormone levels is
challenging. Gonadotroph adenomas account for a large proportion of clinically
nonfunctioning adenomas and about 20% of all adenomas.[60]
Gonadotroph adenomas are most frequent in the sixth decade of age and older and have a
slight male predominance.[14] Typically, they present as clinically nonfunctioning tumors
with symptoms related to local mass effects, including visual deficits, hypopituitarism,
headaches, and cranial nerve palsies.[60, 61]
Histologically, most gonadotroph adenomas are composed of chromophobic cells with
nuclei displaying a fine chromatin pattern. The tumor cells may be arranged in a diffuse
pattern, but distinct papillary arrangements are commonly seen.[60] The papillary structures
are characterized by elongated cytoplasmic processes around blood vessels, occurring in a
pattern resembling perivascular pseudorosette formation.
Monoclonal antibodies to specific -FSH, -LH, and -SU are recommended for IHC
characterization of gonadotroph adenomas, because these lesions may demonstrate varying
degrees of reactivity for 1 or more of the gonadotropin subunits. Immunoreactive cells may
be scattered throughout the adenoma but are often clustered. Immunoreactivity for -FSH
tends to be more frequent, with a stronger and broadly distributed pattern thanimmunoreactivity for the other glycoproteins.[60]
Ultrastructurally, gonadotroph adenomas are characterized by elongated, polar cells
containing scant numbers of small (50200 nm) secretory granules. The secretory granules
are distributed unevenly within the cytoplasm or, more commonly, along the cytoplasmic
membrane. A sex-linked dichotomy between gonadotroph adenomas of male and female
patients has been described.[13, 62] In women, most of the adenomas display a typical
vacuolar transformation of the Golgi complex, giving the Golgi apparatus a honeycomb
appearance.
Characterization of gonadotroph adenomas by ultrastructural means is of scientific interest
but does not alter clinical patient management. The correlation between -FSH and -LH
immunoreactivity, degree of ultrastructural differentiation, and clinical symptoms is
relatively poor in patients with gonadotroph adenomas. At present, most patients are
treated as having a clinically nonfunctioning adenoma, and the therapeutic goals are
restoration of visual deficits, preservation of pituitary function, and prevention of
recurrence.[14]
Null cell adenomas and oncocytomas
Approximately 20% of adenomas show neither clinical nor IHC evidence of hormone
production.[14, 63] The term "null cell adenoma" is given to these tumors, based largely on
the absence of ultrastructural features providing specific differentiation.
The clinical presentation of null cell adenoma resembles that of gonadotroph adenoma;
7/27/2019 In Neuroanatomy
29/42
patients present with signs and symptoms of a mass lesion.[14, 63] Null cell adenomas most
commonly arise in postmenopausal females and elderly males, with the great majority
macroadenomas at presentation.
Histologically, null cell adenomas are chromophobic on light microscopy, and the tumor cells
may be arranged in several neuroendocrine patterns, including trabecular, papillary, anddiffuse. Oncocytic change can be seen in a number of cases, and consequently, the
designation of oncocytoma (oncocytic var