Embed Size (px)
Citation preview

Lateral Ankle Sprain Anatomy – Can the Bifurcate Ligament be Consistently
Identified with Ultrasound on CadaversLyman Wood, 1st Year Medical Student

Overview• Objective
• Bifurcate ligament anatomy
• Understanding lateral ankle injury
• Methods & Materials
• Results and clinical significance
• Conclusion

Objective
• Investigate whether the bifurcate ligament could be identified using ultrasound on cadavers as a training exercise for anatomy education, clinical training, and assessment

Introduction• The bifurcate ligament (BFL) is under
appreciated regarding lateral ankle injuries
• Similar orientation to the anterior talofibular ligament (ATFL)
• The BFL supports the joints between the calcaneous, cuboid and naviculus bones

Understanding Lateral Ankle Sprians• Typical Mechanism
– Plantar flexion
– Inversion
• High Recurrence– A survey of 380 athletes
revealed 73.5% of 563 ankle sprains had been previously injured
• Variable Recovery Time– Average non-surgical complete
rehabilitation 36-72 days
Fallat, Grimm, Saracco, 1998

Methods• Literature Search – current imaging text and
online journals
• Dissection – 58 cadavers to identify BFL
– 55 (n=110 sides; 55R:55L) Carolina solution
– 3 (n=6; 3R:3L) Freedom Art solution

Methods• Evaluate Structural Relationships – Digital caliper
measurements between:
– Apex distal fibula (ADF), 5th metatarsal tuberosity (5MT)
– ADF, Proximal aspect of BFL ligament (PBFL)
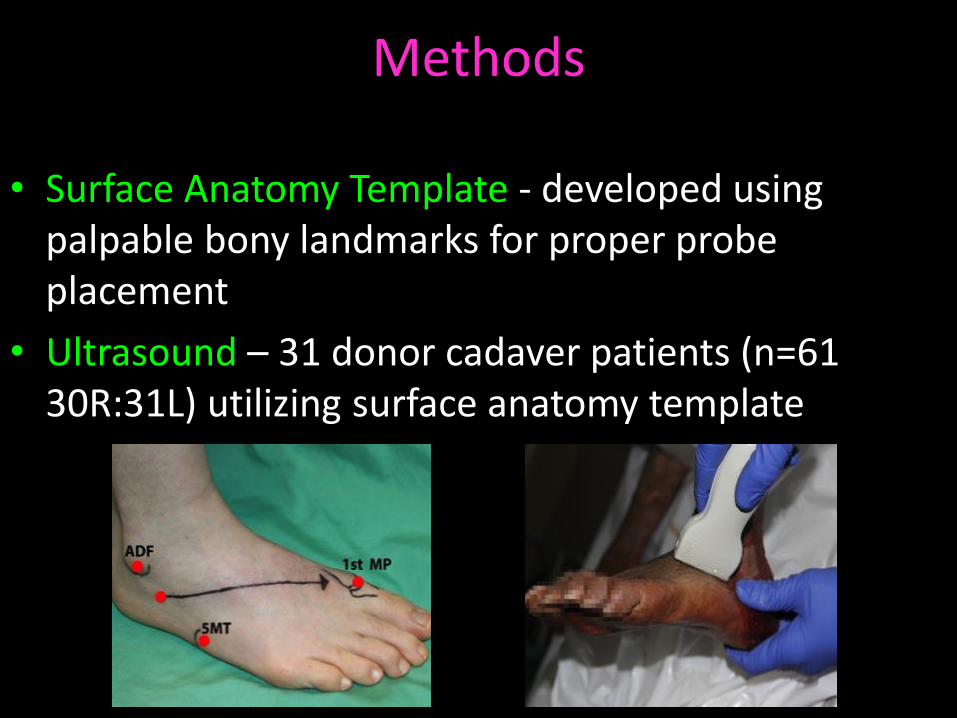
Methods
• Surface Anatomy Template - developed using palpable bony landmarks for proper probe placement
• Ultrasound – 31 donor cadaver patients (n=61 30R:31L) utilizing surface anatomy template

Materials
• Ultrasound systems used
– Sonosite M-Turbo – Classic probe
– Fukuda-Denshi AG760 machines - SonicEye finger probe
Sonosite M-Turbo Fukuda-Denshi AG760

Results
• Literature Search – Revealed no studies of ultrasound (US) identification of BFL on cadavers
– Study of 19 patients revealed 95% positive I.D. by US of ATFL damage (confirmation by Arthroscopy)
• Dissection & Measurements
– ADF – 5MT 60.22mm ± 0.43
– ADF – PBFL 42.18mm ± 0.51
Ratio ADF-PBFL:ADF-5MT = 1/3 from ADF
1/3
2/3
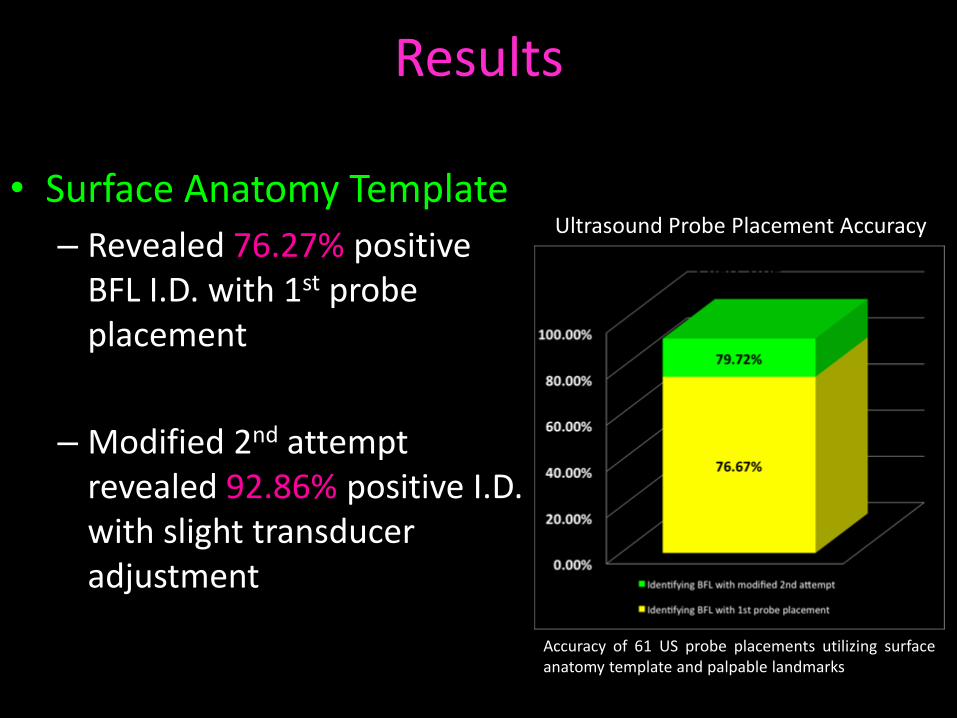
Results
• Surface Anatomy Template
– Revealed 76.27% positive BFL I.D. with 1st probe placement
– Modified 2nd attempt revealed 92.86% positive I.D. with slight transducer adjustment
Ultrasound Probe Placement Accuracy
Accuracy of 61 US probe placements utilizing surfaceanatomy template and palpable landmarks

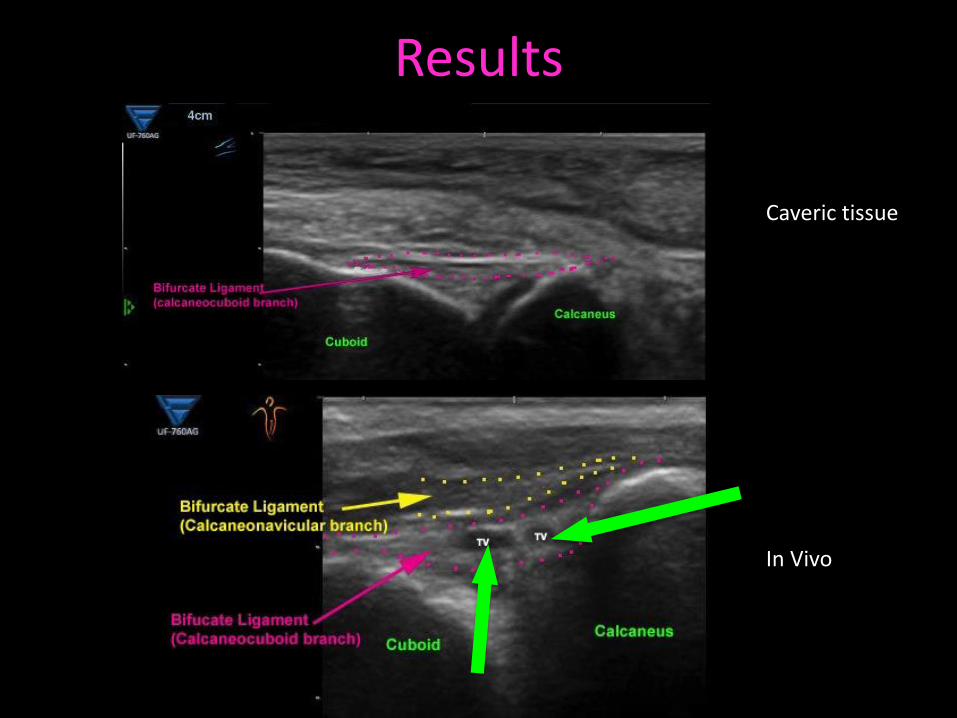
Results
Caveric tissue
In vivo
Results
Caveric tissue
In Vivo

Conclusion & Discussion
• The bifurcate ligament can be positively identified using ultrasound on cadavers
• Utilizing the surface anatomy template provides accurate and efficient I.D. with multiple different ultrasound systems and transducers
• Ultrasound provides cost effective, quality imaging of affected anatomy regarding lateral ankle injuries
• Accurate identification of ALL injured structures can reduce recurrence, recovery time, and improve overall patient care

Acknowledgements
Bryan Beall 4th Year Medical StudentBrion Benninger, MD MSc

References• Anagnostopoulos, D., Bali, N., Alo, K., & McKenzie, J. (2014). (iii) Arthroscopy of the foot and ankle. Orthopaedics and Trauma,
28(1), 18-26.• Anderson, S. J. (2002). Acute ankle sprains. Physician and sportsmedicine, 30(12).• Ansede, G., Lee, J. C., & Healy, J. C. (2010). Musculoskeletal sonography of the normal foot. Skeletal radiology, 39(3), 225-42.• Clanton, T. O., & Porter, D. A. (1997). Primary care of foot and ankle injuries in the athlete. Clinics in sports medicine, 16(3), 435-
66.• Croy, T., Saliba, S., Saliba, E., Anderson, M. W., & Hertel, J. (2012). Differences in lateral ankle laxity measured via stress
ultrasonography in individuals with chronic ankle instability, ankle sprain copers, and healthy individuals. Journal of orthopaedic & sports physical therapy, 42(7), 593-600.
• Fallat, L., Grimm, D. J., & Saracco, J. A. (1998). Sprained ankle syndrome: prevalence and analysis of 639 acute injuries. The journal of foot and ankle surgery, 37(4), 280-5.
• Golanó, P., Vega, J., De Leeuw, P. A., Malagelada, F., Manzanares, M. C., Götzens, V., & Van Dijk, C. N. (2010). Anatomy of the ankle ligaments: a pictorial essay. Knee Surgery, Sports Traumatology, Arthroscopy, 18(5), 557-69.
• Hertel, J. (2002). Functional anatomy, pathomechanics, and pathophysiology of lateral ankle instability. Journal of athletic training, 37(4), 364.
• Hodge, J. C. (1999). Anterior process fracture or calcaneus secundarius: a case report. The Journal of emergency medicine, 17(2), 305-9.
• Hua, Y., Yang, Y., Chen, S., & Cai, Y. (2012). Ultrasound examination for the diagnosis of chronic anterior talofibular ligament injury. Acta Radiologica, 51(10), 1142-5.
• Hubbard, T. J., & Hicks-Little, C. A. (2008). Ankle ligament healing after an acute ankle sprain: an evidence-based approach. Journal of athletic training, 43(5), 523.
• Mei-Dan, O., Kots, E., barchilon, v., Massarwe, S., Nyska, M., & Mann, g. (2009). A dynamic ultrasound examination for the diagnosis of ankle syndesmotic injury in professional athletes a preliminary study. The American journal of sports medicine, 37(5), 1009-1016.
• Oae, K., Takao, M., Uchio, Y., & Ochi, M. (2010). Evaluation of anterior talofibular ligament injury with stress radiography, ultrasonography and MR imaging. Skeletal Radiology, 39(1), 41-7.
• Robbins, M. I., Wilson, M. G., & Sella, E. J. (1999). MR imaging of anterosuperior calcaneal fractures. AJR. American journal of roentgenology, 172(2), 475-9.
• Seybold, J. D., J. R., & Myerson, M. S. (2014) Hindfoot fusions in the flatfood deformity: when and what techniques to use in late stage II and stage III deformities. techniques in foot & ankel surgery, 13(1), 29-38.
• Yeung, M. S., Chan, K. M., So, C. H., & Yuan, W. Y. (1994). An epidemiological survey on ankle sprain. British journal of sports medicine, 28(2), 112-6.
• Weiss, D. B., Jacobson, J. A., & Karunakar, M. A. (2005). The use of ultrasound in evaluating orthopaedic trauma patients. Journal of the American Academy of Orthopaedic Surgeons, 13(8), 525-33.