Embed Size (px)
DESCRIPTION
scienceaortic occlusion terapeutic possibilitiesblood flow and metabolismcerebralartificial blood comprehensive study
Citation preview

aor_1419 185..193
Liposome-Encapsulated Hemoglobin Improves EnergyMetabolism in Skeletal Muscle Ischemia and
Reperfusion in the Rat
*†Daisuke Kurita, *Akira T. Kawaguchi, ‡Kensuke Aso, §Mariko Yamano,‡Haruyuki Minamitani, and *¶Munetaka Haida
*Tokai University School of Medicine; †Tokai University IT Education Center; ‡Keio University Faculty of Science andTechnology; ¶Tokai University Junior College of Nursing and Medical Technology, Kanagawa; and §Osaka Prefecture
University, Habikino, Osaka, Japan
Abstract: The effect of liposome-encapsulated hemoglo-bin (LEH) was tested in a rodent model of limb ischemiaand reperfusion—causing local reperfusion injury and acascade of systemic responses. Intracellular pH (pHi) andphosphocreatine (PCr)/inorganic phosphate (Pi) ratio wereserially monitored using 31P-nuclear magnetic resonancespectroscopy with a 2-cm solenoid coil on a rodent hindlimb. After baseline measurements, the right hind limbunderwent ischemia for 70 min, followed 10 min later byintravenous administration of LEH (10 mL/kg, n = 6),homologous red blood cells (RBCs, n = 6), saline (n = 6), orno treatment (n = 6). Reperfusion was then observed for anadditional 60 min. While pHi decreased precipitously afterthe onset of ischemia and even following reperfusion,LEH-treated rats had significantly milder intracellular aci-dosis compared with all other groups during ischemia, andafter reperfusion as well throughout the observation with
the saline-treated rats. In contrast, the PCr/Pi ratiodecreased regardless of treatment after ischemia until rep-erfusion, when the ratio returned toward normal or theenergy status improved only in the LEH-treated rats, whilethe ratio remained depressed in the control animals receiv-ing RBC, saline, or no treatment. Morphological studies7 days later revealed a tendency toward suppressed mono-nuclear cell infiltration with preservation of muscular massand structure in the LEH-treated rats. LEH treatment afterearly limb ischemia appeared to improve intracellularenergy metabolism and eventually preserve skeletal musclein a rodent model of limb ischemia and reperfusion.Key Words: 31P-nuclear magnetic resonance—Myopathicnephrotic metabolic syndrome—Phosphocreatine—High-energy phosphate complex—Inorganic phosphate—Intracellular pH—Anaerobic metabolism—Aerobicmetabolism.
Skeletal muscle is reported to be one of the mostvulnerable tissues to ischemia (1). Depending on theseverity and duration of limb ischemia, clinicalimpact varies widely from limited local damage tosystemic and multimodal consequences due to meta-bolic effluence from the affected limb, leading tosystemic acidosis, hyperkalemia, nephropathy, andcirculatory collapse (1–4). As liposome-encapsulatedhemoglobin (LEH) (5) has been reported to improvecirculation in tissues with ischemia or deranged
perfusion (6–11), we investigated its effects on limbischemia and early reperfusion using 31P-nuclearmagnetic resonance spectroscopy (31P-NMR) (12–17), following changes in intracellular pH (pHi) andhigh-energy phosphate (phosphocreatine, PCr) to theinorganic phosphate (Pi) ratio (PCr/Pi) in compari-son with animals receiving homologous red bloodcells (RBCs), saline, or no treatment as control. 31P-NMR was first used to detect energy metabolism inexcised muscle (14), whole body (15), skeletal muscleof hind limb (16–19), brain (20–22), and myocardium(23,24) because its noninvasiveness allows repeatedstudies for longitudinal observations. Based on thesecharacteristics, we evaluated the hypothesis thatLEH might efficiently supply oxygen (O2), maintainaerobic energy metabolism, and therefore amelio-rate ischemia and reperfusion injury by means of
doi:10.1111/j.1525-1594.2011.01419.x
Received April 2011; revised September 2011.Address correspondence and reprint requests to Dr. Akira T.
Kawaguchi, Tokai University School of Medicine, Shimokasuya143, Isehara, Kanagawa 259-1193, Japan. E-mail [email protected]
Artificial Organs36(2):185–193, Wiley Periodicals, Inc.© 2012, Copyright the AuthorsArtificial Organs © 2012, International Center for Artificial Organs and Transplantation and Wiley Periodicals, Inc.
185
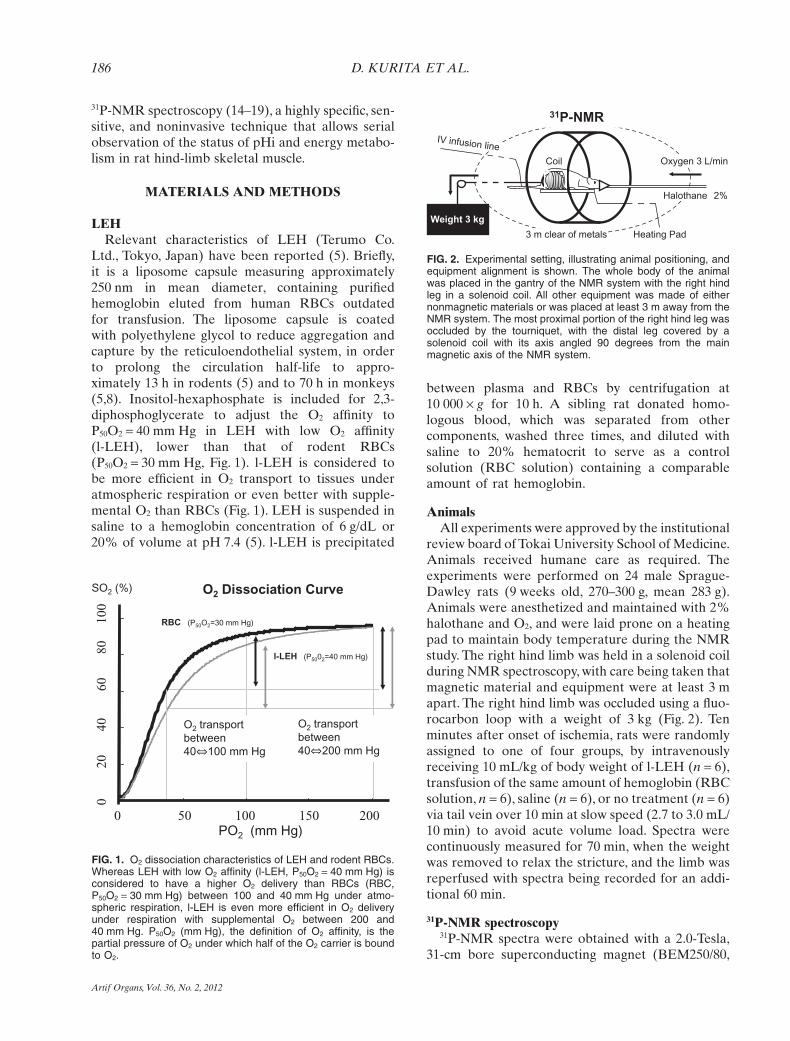
31P-NMR spectroscopy (14–19), a highly specific, sen-sitive, and noninvasive technique that allows serialobservation of the status of pHi and energy metabo-lism in rat hind-limb skeletal muscle.
MATERIALS AND METHODS
LEHRelevant characteristics of LEH (Terumo Co.
Ltd., Tokyo, Japan) have been reported (5). Briefly,it is a liposome capsule measuring approximately250 nm in mean diameter, containing purifiedhemoglobin eluted from human RBCs outdatedfor transfusion. The liposome capsule is coatedwith polyethylene glycol to reduce aggregation andcapture by the reticuloendothelial system, in orderto prolong the circulation half-life to appro-ximately 13 h in rodents (5) and to 70 h in monkeys(5,8). Inositol-hexaphosphate is included for 2,3-diphosphoglycerate to adjust the O2 affinity toP50O2 = 40 mm Hg in LEH with low O2 affinity(l-LEH), lower than that of rodent RBCs(P50O2 = 30 mm Hg, Fig. 1). l-LEH is considered tobe more efficient in O2 transport to tissues underatmospheric respiration or even better with supple-mental O2 than RBCs (Fig. 1). LEH is suspended insaline to a hemoglobin concentration of 6 g/dL or20% of volume at pH 7.4 (5). l-LEH is precipitated
between plasma and RBCs by centrifugation at10 000 ¥ g for 10 h. A sibling rat donated homo-logous blood, which was separated from othercomponents, washed three times, and diluted withsaline to 20% hematocrit to serve as a controlsolution (RBC solution) containing a comparableamount of rat hemoglobin.
AnimalsAll experiments were approved by the institutional
review board of Tokai University School of Medicine.Animals received humane care as required. Theexperiments were performed on 24 male Sprague-Dawley rats (9 weeks old, 270–300 g, mean 283 g).Animals were anesthetized and maintained with 2%halothane and O2, and were laid prone on a heatingpad to maintain body temperature during the NMRstudy. The right hind limb was held in a solenoid coilduring NMR spectroscopy, with care being taken thatmagnetic material and equipment were at least 3 mapart. The right hind limb was occluded using a fluo-rocarbon loop with a weight of 3 kg (Fig. 2). Tenminutes after onset of ischemia, rats were randomlyassigned to one of four groups, by intravenouslyreceiving 10 mL/kg of body weight of l-LEH (n = 6),transfusion of the same amount of hemoglobin (RBCsolution, n = 6), saline (n = 6), or no treatment (n = 6)via tail vein over 10 min at slow speed (2.7 to 3.0 mL/10 min) to avoid acute volume load. Spectra werecontinuously measured for 70 min, when the weightwas removed to relax the stricture, and the limb wasreperfused with spectra being recorded for an addi-tional 60 min.
31P-NMR spectroscopy31P-NMR spectra were obtained with a 2.0-Tesla,
31-cm bore superconducting magnet (BEM250/80,
O2 Dissociation Curve
l-LEH (P5002=40 mm Hg)
RBC (P50O2=30 mm Hg)
0 50 100 150 200PO2 (mm Hg)
SO2 (%)
O2 transport
between
40 200 mm Hg
O2 transport
between
40 100 mm Hg
0
2
0
40
60
80
100
FIG. 1. O2 dissociation characteristics of LEH and rodent RBCs.Whereas LEH with low O2 affinity (l-LEH, P50O2 = 40 mm Hg) isconsidered to have a higher O2 delivery than RBCs (RBC,P50O2 = 30 mm Hg) between 100 and 40 mm Hg under atmo-spheric respiration, l-LEH is even more efficient in O2 deliveryunder respiration with supplemental O2 between 200 and40 mm Hg. P50O2 (mm Hg), the definition of O2 affinity, is thepartial pressure of O2 under which half of the O2 carrier is boundto O2.
Weight 3 kg
31P-NMR
Coil
3 m clear of metals
Halothane 2%
Oxygen 3 L/min
Heating Pad
IV infusion line
FIG. 2. Experimental setting, illustrating animal positioning, andequipment alignment is shown. The whole body of the animalwas placed in the gantry of the NMR system with the right hindleg in a solenoid coil. All other equipment was made of eithernonmagnetic materials or was placed at least 3 m away from theNMR system. The most proximal portion of the right hind leg wasoccluded by the tourniquet, with the distal leg covered by asolenoid coil with its axis angled 90 degrees from the mainmagnetic axis of the NMR system.
D. KURITA ET AL.186
Artif Organs, Vol. 36, No. 2, 2012

Phospho-Energetic, Inc., Philadelphia, PA, USA)operating at 34.53 MHz for 31P nuclei.A 2-cm double-turn solenoid coil was used to acquire spectra fromthe right hind limb. The coil was placed at the mosthomogeneous portion of the magnetic field. Shim-ming of the magnetic field was performed by optimiz-ing the shape and intensity of the spectrum of waterprotons. Homogeneity was adjusted for at least 0.3parts per million (ppm) for each rat. The 31P-NMRspectra were acquired using a single 90-degree pulse(18 ms) and collected with 2048 data points and5000 Hz spectral width. Spectra were accumulatedfor 3 min with a repetition time of 10 s at 3-minintervals. We previously confirmed that a repetitiontime of 10 s was optimal for the accumulation ofspectra over 3 min without affecting the PCr/Pi ratiofor the hind limb muscle. Prior to fast Fourier trans-form, 18 averaged free-induction decays were multi-plied by an exponential window function of 10 Hz.
31P-NMR spectra interpretationThe 31P-NMR spectrum during rest was obtained
for 3 min prior to limb ischemia.Then the time courseof any changes in the 31P-NMR spectra during limbentrapment and reperfusion was measured. For spec-tral analysis, special software (OriginPro ver.7 PeakFitting Module, OriginLab Corporation, Northamp-ton, MA, USA) was used for each spectrum. Eachpeak area and center was obtained by Levenberg–Marquart nonlinear least squares curve fitting usingthe Voigt function (15), which was the convolutionfunction of Gaussian and Lorentzian. The peak areasand centers of a baseline, Pi, PCr, and g-, a-, andb-adenosine triphosphate (ATP), were determined
by a minimum c2 value. In the normal skeletal muscle(12–14), peaks of Pi, PCr, and ATPs were observedand identified by 31P-NMR (Fig. 3, left). The dynam-ics of PCr and Pi in intact tissues were measured.When anaerobic metabolism prevailed due to O2
depletion (Fig. 3, right), PCr decreased and Piincreased because of degradation of the high-energyphosphate complex. Thus, their ratio, PCr/Pi, mayserve as a sensitive and reliable measure of the mus-cular energy metabolism and status (12–17); changesin PCr/Pi ratio were followed by its measured valuesand presented as the changes from preischemicvalues (%PCr/Pi) as well. Any changes in pHi aregiven by the following equation (16): pHi = 6.77 + log(d - 3.29)/(5.58 - d), where d is the chemicalshift of Pi from PCr. The area ratio of PCr/Pi can beused as an index of muscular energy metabolism.
Other variablesBefore and after acquisition of 31P-NMR spectra,
venous blood (<0.1 mL) was taken through thetail vein for hematocrit and volumes of l-LEH(LEHcrit). Systemic blood pressure was monitored inthe left femoral artery of some rats from each group.In these animals, blood samples were analyzed within30 min of the end of NMR spectra measurement forplasma electrolytes and lactate using a portable clini-cal analyzer (i-stat, FUSO Pharmaceutical Industries,Ltd., Tokyo, Japan). Then, the animals were reversedfrom anesthesia and returned to cages with water andfed ad libitum under room air. Seven days later, theanimals were anesthetized for final NMR spectros-copy recordings.
FIG. 3. Typical 31P-NMR spectrum of skel-etal muscle under normal condition(Normal) and ischemia (Anoxia), showingincrease in inorganic phosphate (Pi) anddecrease in phosphocreatine (PCr). As aresult, the PCr/Pi ratio decreased as thecellular aerobic condition changed fromnormal (left) to ischemia (right). In con-trast, peaks for ATP showed no changeeven under ischemia, suggesting that deg-radation of PCr supplied energy to main-tain ATP levels for cellular survival.
31P-NMR
PCr
Pi
ATP
α βγ
-20 -15 -10 -5 0 5 10 15 20
ppm
PCr
Pi
ATP
α βγ
↑
↓
PCr / Pi ↑↓ = Normal Anoxia
ARTIFICIAL O2 CARRIER ALLEVIATES MUSCULAR ISCHEMIA 187
Artif Organs, Vol. 36, No. 2, 2012

Morphological studiesAfter recording the final NMR spectrum 7 days
after ischemia/reperfusion, all animals were sacri-ficed under deep anesthesia. The bilateral soleusmuscles were excised for pathological studies by anauthor, who was blinded to the study protocol (M.Y.).The specimens were fixed and stained withhematoxylin-eosin (H&E) and Masson’s trichromefor microscopic observation.
Statistical analysisThe physiologic determinants and other values of
the rats were averaged for each group, presented asmean � standard deviation, and compared amonggroups by least significant difference method unlessotherwise defined. A P value <0.05 was consideredsignificant.
RESULTS
Hematocrit, LEHcrit, O2 content, and bloodpressure changes
Before and after ischemia/reperfusion, hematocritincreased significantly only in the RBC transfusiongroup (45.5 � 1.8% to 47.9 � 1.2%, P < 0.05), whilethere were no changes in the group receiving l-LEH(46.6 � 2.0% to 45.9 � 1.1%), saline (45.4 � 1.7% to44.0 � 1.0%), or no treatment (47.1 � 2.0% to47.3 � 3.1%). Furthermore, 10 mL/kg of l-LEH infu-sion yielded LEHcrit of 1.8 � 0.6%. These volumesof RBCs and l-LEH allowed calculation of the O2
content in whole blood and plasma fraction (includ-ing LEH) before ischemia and after reperfusion
(Fig. 4). While all the groups had similar O2 contentbefore, RBC-treated rats had the highest O2 contentin whole blood, and LEH-treated rats had the highestO2 content in the plasma fraction (Fig. 4) because ofthe presence of l-LEH. Systemic blood pressureshowed a temporary elevation in response to legischemia followed by administration of solution, butreturned to baseline by 30 min after the onset ofischemia was seen in all groups. Releasing the loopfor reperfusion did not alter the mean systemic pres-sure significantly in any group. Among the determi-nants in blood samples drawn after NMR recording,there was no significant or consistent difference inarterial blood gases, plasma electrolytes, glucose, orlactate levels in rats that received LEH (1.63 �0.5 mg/dL), saline (1.97 � 0.5 mg/dL), RBCs (1.87 �0.5 mg/dL), or no treatment (1.57 � 0.1 mg/dL).
pHiWhereas pHi declined precipitously in all animals
(Fig. 5A), progression of intracellular acidosis wasslower in the l-LEH-treated rats, with a significantdifference (*P < 0.05) being observed in the saline-treated rats starting even during infusion (18 min)and throughout the observation (127 min). In con-trast, pHi was least different in rats with no treat-ment, which showed a significant difference in theprogression of acidosis starting from 18 min until rep-erfusion, as in the rats treated with RBCs (63 min,#P < 0.05). Thus, the level of pHi at the end ofischemia varied according to the treatment:6.54 � 0.04 in l-LEH, 6.39 � 0.04 in RBC, 6.32 � 0.13in saline (P < 0.05 vs. LEH), 6.47 � 0.09 in the non-
FIG. 4. Oxygen contents in whole bloodand plasma fraction. Volume changes inRBC (hematocrit) and LEH (LEHcrit)allowed O2 content calculation in wholeblood (upper panels) and plasma fraction(lower panels) before (left panels) andafter infusion (right panels) in each treat-ment group; l-LEH (heavy solid line), RBC(dotted line), saline (masked line), and notreatment (thin solid line). While the preis-chemic condition was the same among thegroups, O2 content in whole blood becamehighest in the RBC-transfused and non-treated groups, and O2 content in theplasma fraction was elevated only in LEH-treated animals. Note that the amount ofO2 contained in the plasma fraction withl-LEH was less than 1/20 of the O2 contentin whole blood. Some lines were superim-posed on each other.0 20 40 60 80 100 0 20 40 60 80 100
PO2 mm Hg PO2 mm Hg
O2
Co
nte
nt (O
2m
L/d
L)
Wh
ole
Blo
od
Pla
sm
a
LEH group
20
10
0
10
20
0
O2
Co
nte
nt (O
2m
L/d
L)
Pre Post1
0.5
0
1
0.5
0
Saline group
Pre Post
D. KURITA ET AL.188
Artif Organs, Vol. 36, No. 2, 2012

Ischemia
Intr
ace
llula
r p
H
Time after Occlusion (min)
5.6
6.1
6.6
7.1
A
B
C
-1 9 18 27 36 45 54 63 72 82 91 100 109 118 127
LEH
Saline
RBC
None
Infu
sio
n
0
20
40
60
80
100
-1 9 18 27 36 45 54 63 72 82 91 100 109 118 127
LEH
NS
RBC
NO
Ischemia
Time after Occlusion (min)
%P
Cr
/ P
i
LEH
Saline
RBC
None
Infu
sio
n
%P
Cr/
Pi
LEH Saline RBC None
0
10
20
30
40
50
%
FIG. 5. NMR spectroscopy changes.Intracellular pH (A) decreased precipi-tously in each group even followingreperfusion. The animals treated withl-LEH had significantly higher pHi, startingduring infusion up to reperfusion, com-pared to RBC-treated rats and animalswithout treatment (#P < 0.05), andthroughout the observation in rats treatedwith saline (*P < 0.05). The PCr/Pi ratio(B) compared to self-preischemic value(%PCr/Pi) decreased after the onset ofischemia in all groups until reperfusion,when the ratio reversed to increase (nor-malize) only in the LEH-treated animals(#P < 0.05 vs. nontreated control), whilethe ratio varied or remained unchangedin the other groups. The %PCr/Pi ratio7 days later (C) showed a tendencytoward better preservation in the LEH-treated rats, with no significant differencefrom the other treatment groups.
ARTIFICIAL O2 CARRIER ALLEVIATES MUSCULAR ISCHEMIA 189
Artif Organs, Vol. 36, No. 2, 2012

treated group. The tendency of intracellular acidosisremained progressive even after releasing the tourni-quet, further reducing pHi at the end of observation,or 60 min after reperfusion, when pHi reductionappeared to have leveled off (6.21 � 0.14 in LEH,6.14 � 0.13 in RBC, 5.96 � 0.32 in saline, 6.16 � 0.13in the nontreated group), with less significant differ-ences among the groups because of a large variationafter reperfusion.
PCr/PiWhile ATP did not change much in response to
ischemia (Fig. 3), PCr decreased and Pi increasedat the same time, rendering their ratio, PCr/Pi, todecrease precipitously after the onset of ischemia,with no difference among groups during ischemia(Fig. 5B). After release of the tourniquet, however,the PCr/Pi ratio reversed to increase in all animals inthe LEH-treated group significantly (2.9 � 2.8% to13.7 � 8.4%, P < 0.05) significantly (#P < 0.05) com-pared to the nontreated group (1.3 � 1.1% to1.8 � 1.9%). The values of the other control groupswere between these two groups, having significantdifference with LEH-treated rats only at 72 and82 min (*P < 0.05), with no significant time-dependent change on average (3.7 � 7.2% to5.6 � 8.4% in saline-treated group, 2.3 � 3.0% to7.3 � 8.4% in RBC-treated group). The %PCr/Piratio 7 days after reperfusion showed variable results(Fig. 5C), ranging from 20 to 30% of the valuesobtained before ischemia. The rats treated withl-LEH tended to have a higher ratio, although only31 � 8%, than the other treatment groups (20–23%on average).
Morphological changesIn a typical H&E staining of the core of the soleus
muscle 7 days after reperfusion (Fig. 6A), there wasdiffuse muscular necrosis determined by widenedintercellular space, muscular atrophy, anisocytosis,and eosinophilic cytoplasm with karyolysis. In theperiphery of the soleus muscle (Fig. 6B), diffusemononuclear cell infiltration, or inflammation, waspersistent in all groups, suggesting that a replacementprocess was underway. These findings appeared to beless severe in animals treated with l-LEH.
DISCUSSION
Treatment for and outcome of limb ischemia andreperfusion failed to be improved even during recentyears when various techniques were developed forother organs to suppress reperfusion injury andresultant organ dysfunction. It became clear that
minimizing the ischemic damage and reperfusioninjury is crucial for suppressing skeletal muscledamage to the affected limb as well as a subsequentsystemic inflammatory response (1–4). Using 31P-NMR during ischemia and early reperfusion, wetested the effects of LEH, which has been reportedto be beneficial in various experimental cases offocal as well as global ischemia and reperfusion (5)—highly protective against brain edema after perma-nent occlusion of the middle cerebral artery (6),preserving the cortex after reperfusion in the rat (7)as well as in the monkey (8), protective in cochlearischemia/reperfusion (9), accelerated gastric (inpreparation) as well as skin wound healing (10), andenhanced cancer radiotherapy (11). Moreover, LEHhas been manufactured to have a lower oxygen affin-ity (l-LEH; P50 = 40 mm Hg [5]) than RBC to trans-fer O2 efficiently under atmospheric or supplementalO2 respiration (Fig. 1). Thus, we tested l-LEHwith O2 respiration in an early phase of skeletalmuscle ischemia induced by tourniquet occlusion,finding that l-LEH-treated rats had significantlymilder intracellular acidosis, while the PCr/Pi ratiodecreased regardless of treatment after onset ofischemia until reperfusion 70 min later, when thePCr/Pi ratio returned toward normal only in theLEH-treated rats.
Intracellular energy metabolism was followed by31P-NMR spectroscopy to detect subtle intracellularchanges in the rodent hind limb undergoing abruptischemia followed by reperfusion. In preliminarystudies, we tested various methods to induce legischemia that would be severe enough to be associ-ated with a steady increase in Pi by 31P-NMR.Arterial inflow occlusion by ligation, thromboticocclusion, or stripping of the femoral artery yieldsonly a temporary increase in Pi, which returns tobaseline, suggesting that a compensatory mecha-nism(s) quickly reinstates aerobic metabolism in therodent hind limb. Since we learned that circumferen-tial heavy ligation induced skeletal muscle ischemia(25), we developed the current tourniquet system toallow remote control of tightening for ischemia andreleasing for reperfusion while keeping the animal inplace for continued NMR observation. Then, occlu-sion pressure was increased by changing the weightfrom 2.0 to 2.5 kg and then to 3.0 kg to induce steadyand serious ischemia. Finally, the duration ofischemia was adjusted to 70 min, not long enough toinduce muscular necrosis (1,16), in order to allowobservation of the reperfusion response in theskeletal muscle, but not of the systemic conse-quences, which were undetectable by the currentprotocol.
D. KURITA ET AL.190
Artif Organs, Vol. 36, No. 2, 2012

Although the occlusion pressure was higher thanthose reported in mice (25) or in rats (26), significantdeceleration in intracellular acidosis starting soonafter infusion suggested penetration of l-LEH acrossthe high occlusion pressure. As pHi largely dependson the levels of intracellular lactate in a dynamicbalance between its production and washout (16–19,23), LEH treatment was considered to be associ-ated with aerobic metabolism, reducing lactateproduction and thereby decelerating the progression
of intracellular acidosis. This may be the first directevidence that LEH is effective during ischemia, as allthe previous studies but one (7) showed benefits ofLEH only after reperfusion (6,8–11), leaving theinevitable possibility that LEH is effective not as anO2 carrier, but as an agent that reduces oxidativestress after reperfusion. During brain ischemia,plasma flow has been reported to be persistent,although decreased, even to the core of the ischemia(27). There might be a similar effect of LEH under
FIG. 6. Morphological study. In a typicalH&E staining of the core of the soleusmuscle 7 days after reperfusion (A), therewas diffuse muscular necrosis determinedby widened intercellular space, muscularatrophy, anisocytosis, and eosinophilic cyto-plasm with karyolysis. In the periphery of thesoleus muscle (B), diffuse mononuclear cellinfiltration was persistent in all groups, sug-gesting a prevailing replacement process.These findings appeared to be less severein animals treated with l-LEH.
H&E staining
LEH
RBCRBC
g 1 week later (x 10)
Saline
C NoneC None
RBC None
H&E stainin
LEH
A
B
ng 1 week later (x 10)
Saline
ARTIFICIAL O2 CARRIER ALLEVIATES MUSCULAR ISCHEMIA 191
Artif Organs, Vol. 36, No. 2, 2012

the permanent occlusion of the middle cerebralartery (7), where reduction in brain edema was highlysignificant in various parts of the brain despite theabsence of reperfusion. Thus, the benefits of LEHmay be described as its perfusion with O2 delivery,supporting aerobic energy metabolism and preserv-ing pHi during ischemia, which ameliorates the rein-statement of microcirculation early after reperfusion.
In contrast to pHi, the PCr/Pi ratio decreasedabruptly during ischemia without any differencesamong treatment groups, and there was also notmuch difference in the ATP levels among the groups,similar to a previous observation by Morikawa et al.(16), who reported that changes occurred in the orderof PCr reduction, Pi increase, and pHi decrease, fol-lowed by beta-ATP reduction after 3 h. This mightsuggest that O2 delivery with LEH is obviously notenough, and that PCr degradation and Pi productionoccurred at a similar rate regardless of the treatment,as it is the in-common step for muscular energystorage and metabolism (14–17) to keep the ATPlevel constant, the final energy source for cellularsurvival (1,16,23). These phenomena are compatiblewith the observations by Hayes et al. (12), whoreported that myocyte glycogen and PCr weredepleted initially, in preference to ATP, in skeletalmuscle (13), as well as in the myocardium (23). Aftera longer ischemic interval, diminishing ATP levelscorrelated closely with worsening muscle necrosis(13), suggesting that the current ischemia for only70 min is not severe enough to deplete ATP or tocause muscular necrosis (13,16). After reperfusion,however, only LEH-treated rats had significantlyimproved PCr/Pi ratio, while the nontreated animalsfailed to show any improvement in energy status (Fig.5B). This may be due to the effect of intravenousinfusion (10 mL/kg) during ischemia in the LEH,RBC, and saline treatment groups, which may help toreduce viscosity and retain plasma flow in capillariesduring ischemia and facilitate recovery of microcir-culation after reperfusion. These speculations arecompatible with the report by Hammersen (13), whoprecisely followed the morphological changes in cap-illaries during ischemia and reperfusion. In contrast,nontreatment might have led to increased blood vis-cosity, which would likely be associated with throm-botic occlusion of the vessels (14), further delayingthe recovery of intracellular acidosis and energystatus.
This discrepancy, improving energy status (PCr/Pi)under worsening intracellular acidosis, may be due tothe delay in recovery of pHi (14,18), being related toprolonged anaerobic metabolism (14,19), consumingintracellular buffering materials, accumulated lactate
(18), and failure in immediate reperfusion in someanimals that may even deter the recovery of micro-circulation and lactate washout (13,28), as in the non-treated control rats. The important difference may bethe source of energy regeneration and transfer toreproduce PCr, either aerobic or anaerobic; the latteris much less efficient, with lactate production asthe end metabolite (23–25,28). Thus, pHi changesbecame similar and leveled off after reperfusion,when O2 became available for aerobic energy pro-duction in viable cells. The presence of LEH in theplasma was associated with increased O2 availability,which had ameliorated the PCr/Pi ratio withoutimproving pHi (14) after reperfusion. Such persistingmetabolic failure may result in the observations7 days later, when cell shrinkage and necrosis in thecore of ischemia and diffuse neutrophil infiltration inthe periphery were noted. These findings were inaccordance with the 31P-NMR observation that thePCr/Pi ratio tended to be higher (albeit only 31%) inLEH-treated rats than in the other animals, with 20 to23% of preischemic control (24).
These precise and sensitive observations of pHiand energy status were afforded by 31P-NMR, whichin turn made it difficult to obtain systemic and physi-ologic determinants, such as blood pressure, systemicacid-base balance, and electrolyte levels. While theobserved changes in pHi and energy status appearedto be irrelevant to reperfusion pressure, hematocrit,whole blood O2 content, pH, or buffering capacity ofinfused solutions, these physiologic parameters areimportant as the systemic symptoms after reperfu-sion, and they will need to be followed in futurestudies.
CONCLUSION
l-LEH (10 mL/kg) early after onset of ischemiaappeared to hamper progressive intracellular acido-sis of skeletal muscle and improve energy regenera-tion after reperfusion, suggesting exertion of aprotective effect on energy metabolism duringischemia and early reperfusion. A tendency towardless severe neutrophil infiltration, and preservation ofPCr/Pi, muscular structure, and muscle mass 7 dayslater may suggest improved muscular viability in ratstreated with l-LEH. While the current results arecompatible with the hypothesis, the mechanism(s)remains speculative, and successive systemic influ-ences need to be determined in future studies.
Acknowledgments: We gratefully acknowledgethe assistance and technical support of the Tokai Uni-versity Education and Research Support Center.
D. KURITA ET AL.192
Artif Organs, Vol. 36, No. 2, 2012

Funding: This study was supported in part by:A) Grant-in-Aid for Scientific Research
(A16209037 and A20249072) from the Ministry ofEducation, Culture, Science and Technology, Tokyo,Japan. This was granted to A. Kawaguchi.
B) New Energy Development Organization(NEDO), Tokyo, Japan. This was granted to TerumoCo. Ltd. and Tokai University.
C) Japan Science and Technology Agency (JST),Japan. This was granted to A. Kawaguchi.
Conflicts of interest and author contribution: D.Kurita, A. Kawaguchi, and M. Haida are clinicians/scientists responsible for the organization and sum-marization of this study. At the time of theexperiments, they were attached to Tokai UniversitySchool of Medicine, where all animal experimentswere carried out. K. Aso and H. Minamitani wereresearchers belonging to Keio University School ofScience and Technology at the time of this work. M.Yamano was doing research at Osaka PrefectureUniversity and did the anatomical studies. As theseauthors had individual research funds (specified pre-viously), there are no monetary dependencies or con-flicts of interest.
REFERENCES
1. Blaisdell FW. The pathophysiology of skeletal muscleischemia and the reperfusion syndrome: a review. CardiovascSurg 2002;10:620–30.
2. Cryer HG. Therapeutic approaches for clinical ischemia andreperfusion injury. Shock 1997;8:26–32.
3. Eliason JL, Wainess RM, Proctor MC, et al. A national andsingle institutional experience in the contemporary treatmentof acute lower extremity ischemia. Ann Surg 2003;238:382–90.
4. Walker PM, Romaschin AD, Davis S, Piovesan J. Lower limbischemia: phase 1 results of salvage perfusion. J Surg Res1999;84:193–8.
5. Kaneda S, Ishizuka T, Goto H, Kimura T, Inaba K, KasukawaH. Liposome-encapsulated hemoglobin, TRM-645: currentstatus of the development and important issues for clinicalapplication. Artif Organs 2009;33:146–52.
6. Kawaguchi AT, Fukumoto D, Haida M, Murayama M, OgataY, Tsukada H. Liposome-encapsulated hemoglobin reducesthe size of cerebral infarction in the rat. Evaluation with pho-tochemically induced thrombosis of the middle cerebralartery. Stroke 2007;38:1626–32.
7. Kawaguchi AT, Kurita D, Furuya H, Yamano M, Ogata Y,Haida M. Liposome-encapsulated hemoglobin alleviates brainedema after permanent occlusion of the middle cerebral arteryin the rat. Artif Organs 2009;33:153–8.
8. Kawaguchi AT, Haida M, Yamano M, Fukumoto D, Ogata Y,Tsukada H. Liposome-encapsulated hemoglobin amelioratesischemic stroke in nonhuman primates: an acute study. J Phar-macol Exp Ther 2010;332:429–36.
9. Okada M, Kawaguchi AT, Hakuba S, et al. Liposome-encapsulated hemoglobin alleviates hearing loss after tran-sient cochlear ischemia and reperfusion in the gerbil. ArtifOrgans 2012;36:178–84.
10. Fukui T, Kawaguchi AT, Tanaka R, et al. Liposome-encapsulated hemoglobin ameliorates skin wound healing inmice. Artif Organs 2012;36:161–9.
11. Murayama C, Kawaguchi AT, Kamijo A, et al. Liposome-encapsulated hemoglobin ameliorates tumor hypoxia andenhances radiation therapy to suppress tumor growth in mice.Artif Organs 2012;36:170–7.
12. Hayes G, Liauw S, Romaschin AD, Walker PM. Separation ofreperfusion injury from ischemia-induced necrosis. SurgForum 1988;39:306–8.
13. Hammersen F. The ultrastructure of microvessels and theircontents following ischemia on reperfusion. Prog Appl Micro-circ 1988;13:1–26.
14. Hoult DI, Busby SJ, Gadian DG. Observation of tissuemetabolites using 31P nuclear magnetic resonance. Nature1974;252:285–7.
15. Ackerman JJH, Grove TH. Mapping of metabolism in wholeanimals by 31P NMR using surface coils. Nature 1980;283:167–70.
16. Morikawa S, Kido C, Inubushi T. Observation of rat hindlimb skeletal muscle during arterial occlusion and reperfusionby 31P MRS and 1H MRI. Magn Reson Imaging 1991;9:269–74.
17. Richardson RS. Lactate efflux from exercising human skeletalmuscle: role of intracellular pO2. J Appl Physiol 1998;85:627–34.
18. Jacobs DO, Maris J. In vivo phosphorus 31 magnetic resonancespectroscopy of rat hind limb skeletal muscle during sepsis.Arch Surg 1998;123:1425–8.
19. Greenhaff PL, Timmons JA. Interaction between aerobic andanaerobic metabolism during intense muscle contraction.Exerc Sport Sci Rev 1998;26:1–30.
20. Petroff OA, Prichard JW, Behar KL, Alger JR, den HollanderJA, Shulman RG. Cerebral intracellular pH by 31P nuclearmagnetic resonance spectroscopy. Neurology 1985;35:781–8.
21. Ackerman JJ, Berkowitz BA, Deuel RK. Phosphorus-31 NMRof rat brain in vivo with bloodless perfluorocarbon perfusedrat. Biochem Biophys Res Commun 1984;119:913–9.
22. Kurita D, Haida M, Shinohara M. Energy metabolism andcerebral blood flow during cytotoxic brain edema induced by6-aminonicotinamide. Acta Neurochir 2003;86:41–4.
23. Garlick PB, Radda GK, Seeley PJ. Studies of acidosis in theischemic heart by phosphorous nuclear magnetic resonance.Biochem J 1979;184:547–54.
24. Hitchins S, Cieslar JM, Dobson GP. 31P NMR quantificationof phosphorus metabolism in rat heart and skeletal muscle invivo. Am J Physiol Heart Circ Physiol 2001;281:H882–7.
25. Bonheur JA, Albadawi H, Patton GM, Watkins MT. A nonin-vasive murine model of hind limb ischemia-reperfusion injury.J Surg Res 2004;116:55–63.
26. Dick F, Li J, Giraud MN, Kalka C, Schmidli J, Tevaearai H.Basic control of reperfusion effectively protects against reper-fusion injury in a realistic rodent model of acute limb ischemia.Circulation 2008;118:1920–8.
27. Theilen H, Schrock H, Kuchinsky W. Gross persistence ofcapillary plasma perfusion after middle cerebral artery occlu-sion in the rat brain. J Cereb Blood Flow Metab 1994;14:1055–61.
28. Wells RE. Rheology of blood in the microvasculature. N EnglJ Med 1964;70:832–9.
ARTIFICIAL O2 CARRIER ALLEVIATES MUSCULAR ISCHEMIA 193
Artif Organs, Vol. 36, No. 2, 2012


























![Liposome [GoR]](https://img.dokumen.tips/doc/110x75/54f49f044a795997318b4927/liposome-gor.jpg)


