Embed Size (px)
Citation preview

Is the chlamydia screening programme worthwhile?
BRITISH SOCIETY FOR MICROBIAL TECHNOLOGY
27th ANNUAL SCIENTIFIC MEETING
18 May 2012
Dr Angie Bone, Director NCSP
http://www.chlamydiascreening.nhs.uk

Outline• Update on the National Chlamydia Screening
Programme• Is chlamydia still an important public health problem?• How do we know if screening is working?• Is it cost-effective?• What are young people’s views?• How is progress being monitored?• What do local areas need to do?
• Olympics and Sexual Health

Chlamydia trachomatis
• Commonest bacterial STI in England• Majority of infections are
asymptomatic• Highest rates of infection among young
people • Easy to detect using NAAT tests• Easy to treat with antibiotics• Untreated infections can cause PID,
ectopic pregnancy, infertility
Chl
amyd
ia in
fect
ed c
ultu
re (
Wel
lcom
e Im
ages
)
The National Chlamydia Screening Programme (NCSP) in England
• Aims to control chlamydia thus reducing transmission and sequelae
• Opportunistic screening of sexually active < 25 year olds - Annually - Change of sexual partner
• Clinical and non-clinical venues
• Standards for treatment and partner notification

5
The NCSP 2003 to 2010: What went well
• High volumes screened• Expansion of sexual health services into community
with range of providers• Early adoption of new technologies• Quality assurance programme• Involvement of men• Reaching those at higher risk and the socio-
economically deprived
6
The NCSP 2003 to 2010: Areas for improvement
• Value for money, cost variations• Lack of integration with other sexual health services• Engagement of some providers e.g. GP’s• Scientific/policy controversies

So, is it worthwhile to continue…?
• Chlamydia remains a cause of serious reproductive morbidity, with costs to the service and individuals
• Evidence of impact on prevalence- Modelling- changes in percentage infected amongst those tested- Seroepidemiology
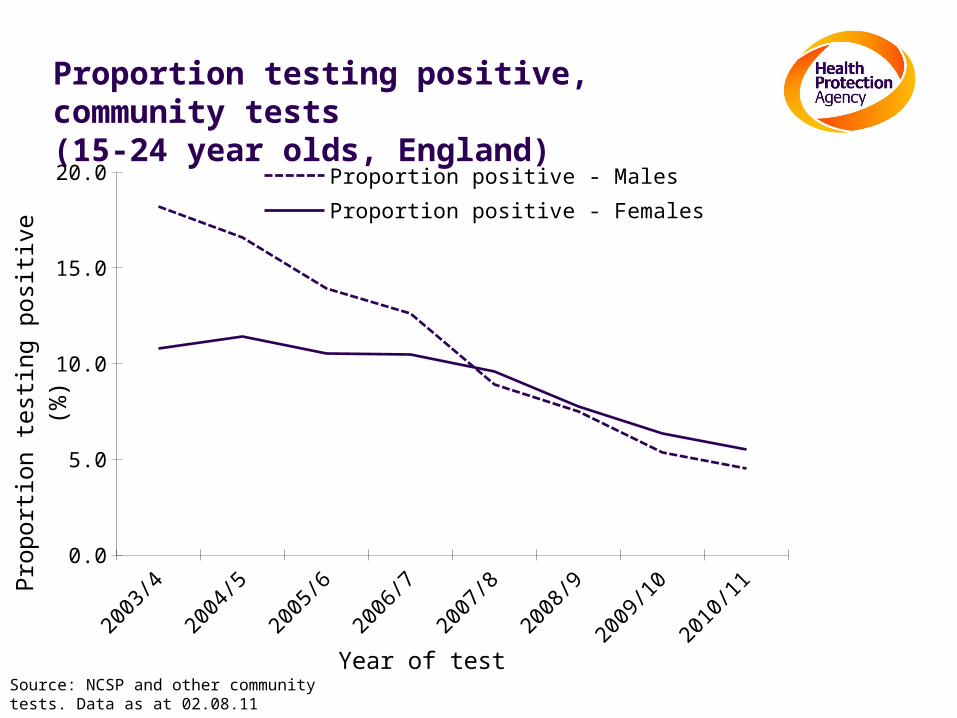
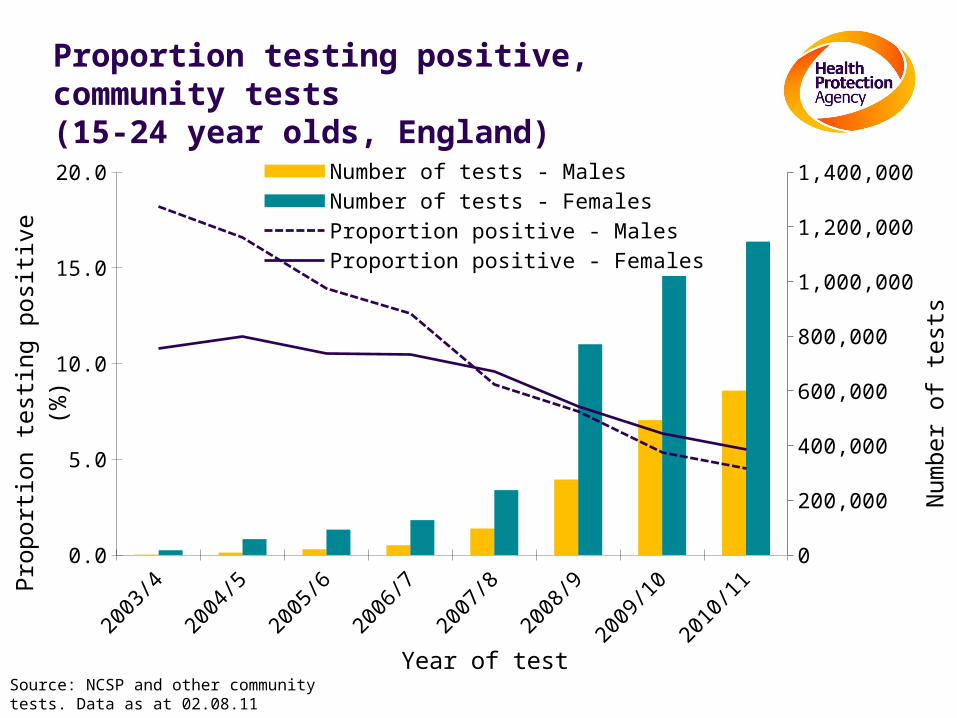
Proportion testing positive, community tests(15-24 year olds, England)
Source: NCSP and other community tests. Data as at 02.08.11
2003/4
2004/5
2005/6
2006/7
2007/8
2008/9
2009/10
2010/11
0.0
5.0
10.0
15.0
20.0 Proportion positive - MalesProportion positive - Females
Year of test
Prop
ortio
n te
sting
pos
itive
(%)
Proportion testing positive, community tests(15-24 year olds, England)
Source: NCSP and other community tests. Data as at 02.08.11
2003/4
2004/5
2005/6
2006/7
2007/8
2008/9
2009/10
2010/11
0.0
5.0
10.0
15.0
20.0
0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000Number of tests - MalesNumber of tests - FemalesProportion positive - MalesProportion positive - Females
Year of test
Prop
ortio
n te
sting
pos
itive
(%)
Num
ber o
f tes
ts
10
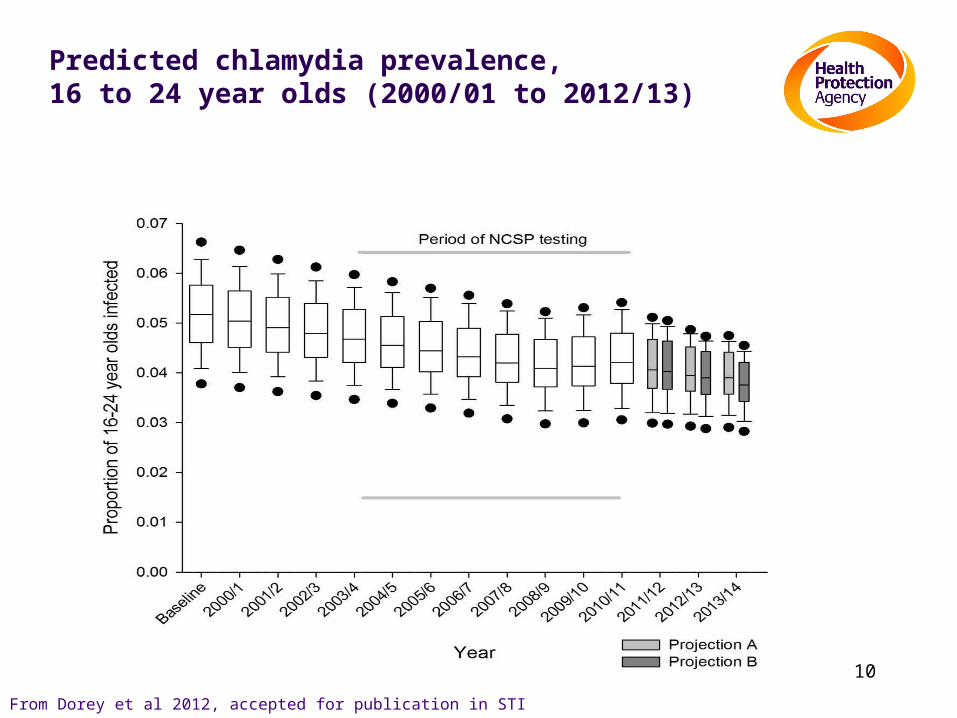
Predicted chlamydia prevalence, 16 to 24 year olds (2000/01 to 2012/13)
From Dorey et al 2012, accepted for publication in STI

So, is it worthwhile to continue…?• Chlamydia remains a cause of serious reproductive
morbidity, with costs to the service and individuals• Evidence of impact on prevalence
- Modelling- changes in percentage infected amongst those tested- seroepidemiology
• Evidence of impact on sequelae- RCT evidence- Changes in PID rates

Rate of PID diagnoses* in General Practice by age group (females 16 to 44 years old)
*Definite/probable PID diagnoses
Source: French et al. STD 2011.
So, is it worthwhile to continue…?
• Remains a cause of reproductive morbidity, with substantial costs• Evidence of impact on prevalence
- Modelling
- changes in percentage infected amongst those tested
- seroepidemiology
• Evidence of impact on sequelae- RCT evidence
- Changes in PID rates
• Wider benefits- Awareness of chlamydia
- Expanding sexual health services into community
- Involving men
- Reducing stigma
Is it cost-effective?
• Three studies indicate screening may be cost-effective
• Depends on parameters used in model both for costs and benefits
• Several elements to screening pathway and huge variety of delivery methods
• Average cost per screen £27; per diagnosis £437*
• Recent policy initiatives to reduce costs and improve sustainability
• Emphasis on partner notification
Adams E and Turner K: Invest to Save in the South West 2012

What are young people’s views?
• Don’t always see chlamydia as relevant to them• Prefer a blanket approach to testing • Want to be asked rather than have to ask for a test• Don’t want to have to give a sexual history• Need to be sure of confidentiality• Want options for testing – hcp/remote testing• Want results quickly• Want support to be available to manage positive
results

So, is it worthwhile to continue…?
YES!

Where we are now
• DH “Future direction” statement July 2011• Drives to reduce outreach and integrate ct screening• Chlamydia Testing Activity Dataset (CTAD)• Move from coverage to diagnosis rate• PH outcomes framework
- A level of at least 2400 chlamydia diagnoses per 100,000 residents aged 15-24
- At present, aim is to achieve HIGH levels of diagnoses
- Recommended level only achievable through widespread testing

East M
idla
nds
East o
f Engla
nd
London
North E
ast
North W
est
South C
entra
l
South E
ast C
oast
South W
est
Wes
t Mid
lands
Yorksh
ire a
nd Hum
ber
ENGLAND
0
500
1000
1500
2000
2500
3000
England - Diagnosis Rate by SHA Q1-3 2010/11 Vs. Q1-3 2011/12
2010/11
2011/12
To
tal D
iag
no
se
s R
ate
pe
r 1
00
,00
0

What do local areas need to do?
1. Safeguard chlamydia screening and other sexual health services during transition
2. Know your data – available on the HPA/NCSP websites
3. Embed chlamydia screening in primary care and sexual health services – general practice is key
4. Enable remote testing
5. Focus outreach on hard to reach groups
6. Emphasise screening annually and on change of partner; partner notification very important
7. Listen to young people
The Olympics and Sexual Health – what might we expect?
• Mass gathering – increased risk of infectious diseases• In terms of STI, possibility of increased transmission:
- increase in casual workers- increase in sex workers- increase in sexual risk taking
• Increased demand on sexual health services• Sydney 2000 (McNulty et al 2003)
- Two fold increase in diagnoses of bacterial STI’s- Increase in new patient visits to sexual health services
(symptomatic or STI contacts)
The Olympics and Sexual Health - preparation and response
• Promotion of contraception, condom use & NHS Choices• LOCOG – Durex sexual health campaign• Effective sign-posting, rapid referral and extended
opening hours to sexual health services• Onsite sexual health services to construction workers• Temporary outreach centre in Stratford• GUM clinicians and labs to be alert to any new or rapidly
increasing infections – report to local HPU• Olympic codes in GUMCAD - surveillance

THANK YOU