Embed Size (px)
Citation preview
THE KURUME MEDICAL JOURNAL
Vol. 39, p. 77-82, 1992
Invisible Cardia Cancer Metastasis to the Diaphragm
JINRYO TAKEDA, KEN HASHIMOTO, HIROSHI UMETANI, TAKAHO TANAKA, KIKUO KOUFUJI
AND TERUO KAKEGAWA
Department of Surgery, Kurume University School of Medicine, Kurume, 830 Japan
Received for publication January 22, 1992
Summary : The best surgical procedure to treat a carcinoma in the gastric cardia remains a controversy because the carcinoma is often advanced and there are other unknown factors. In this article the incidence of invisible metastasis from cardia cancer to the diaphragm will be analyzed using an experimental cardia cancer model and clinical studies. An experimental cardia cancer was induced by an endoscopic injection of VX2 cancer cells into the submucosal layer of the esophago-gastric junction in rabbits using a 27G needle and an Olympus BF-4B2 bronchofiberscope. A total of 26 cardia cancer models for Borrmann type 2 or 3 were produced. Of these, six (23%) had visible cancer metastases in the diaphragm, including 4 cases with direct invasion and 2 cases with peritoneal dissemination on the surface of the dia-phragm. Four (20%) of the remaining 20 were histologically found to have macroscopically-invisible cancer metastases mainly in the lymph vessels of the left hemidiaphragm. From 1985 to 1988, 22 clinical cases of cardia cancer were managed by a combined total gastrectomy with a partial diaphragm resection through a left thoracoabdominal approach. When widely resected, reconstruc-tion was performed using a latissimus dorsi muscle flap. Six (27%) of these 22 were also histologically found to have macroscopically-invisible cancer me-tastases to the diaphragm, including 1 (11%) of the 9 well-differentiated type and 5 (39%) of 13 poorly-differentiated type adenocarcinomas. For patients with stage II, III or IV cardia cancers with no hepatic metastasis and no peri-toneal dissemination, the 2-year survival rate was 64% for those who under-went a combined resection of the diaphragm and 42% for those who under-went a non-combined resection. The postoperative mortality in this series was zero. This is the first report of invisible cancer metastases from cardia cancer to the diaphragm.
Key words : cardia cancer-VX2 cancer-broncofiberscope-diaphragm-
invisible metastasis-latissimus dorsi muscle flap-mortality
Introduction
The prognosis for a patient with an
adenocarcinoma in the gastric cardia is
generally poorer than for an adenocar-
cinoma in the corpus or distal stomach.
This can be attributed to the difficulty
in detecting the cancer in the cardia at
an early stage because of the character-
istically early infiltration into deeper tis-
sue layers, and the rapid advancement
due to the thin wall of the cardia. The
high proportion of advanced cancers is
related to the wide variation and distri-
bution patterns of lymph node metasta-
ses, involving both the mediastinal and
77

78 TAKEDA, ET AL.
the abdominal regions, with infiltration to adjacent organs because of their ana-tomical characteristics.
The diaphragm is probably the nearest
organ to the cardia. Coupled with the
absence of serosa on the outer posterior
wall of the cardia, which is directly in
contact with the diaphragm, there is a
high proportion of cardia cancers having
diaphragm involvement.
The route of lymphogenous metastasis of cardia cancer to the diaphragm was investigated experimentally using VX2 cancer cells (Kidd and Rous, 1940; Rous, 1965) injected into the cardia of rabbits and with metastases flowing through lymph vessels into the diaphragm. While such metastases were macroscopically-invisible, pathological studies confirmed the diaphragmatic metastases. Clinically, a new combined total gastrectomy was adopted with partial resection of the dia-
phragm, through the left thoracoab-dominal approach. Invisible cancer me-tastases were observed in the diaphragm even in cases with negative peritoneal dissemination. There is no other report of an invisible cancer metastasis of car-dia cancer to the diaphragm.
The details of the experimental studies
and the new clinical approach which has
led to zero operative mortality in clinical
cardia cancers with invisible metastasis
to the diaphragm are described in this
report.
Materials and Methods
Experimental Studies
White rabbits of 2-3 kg body weight were selected for the experimental study. VX2 cancer cells, 0.5ml (106-107/ml), were injected into the submucosa of the esophagogastric (EG) junction using a 27G needle and an Olympus BF-4B2 broncho-f iberscope (BF) under Nembutal, 25mg/kg intravenous, and endotracheal (3mm)
intubation anesthesia.
After 3-4 weeks, the formation of Borrmann type 2 or 3 cardia cancer was confirmed by BF under the same anes-thesia. After a left thoracoabdominal ap-
proach plus sternotomy, CH44 carbon Ink (CH44), 0.1-0.2ml, was injected into the submucosa of the distal portion of the cardea cancer. Esophagectomy plus total
gastrectomy and combined resection of the total diaphragm was then performed immediately after CH44 injection. Lymph nodes that appeared to be black from the CH44 stain, were investigated macroscop-ically. Pathological studies were then
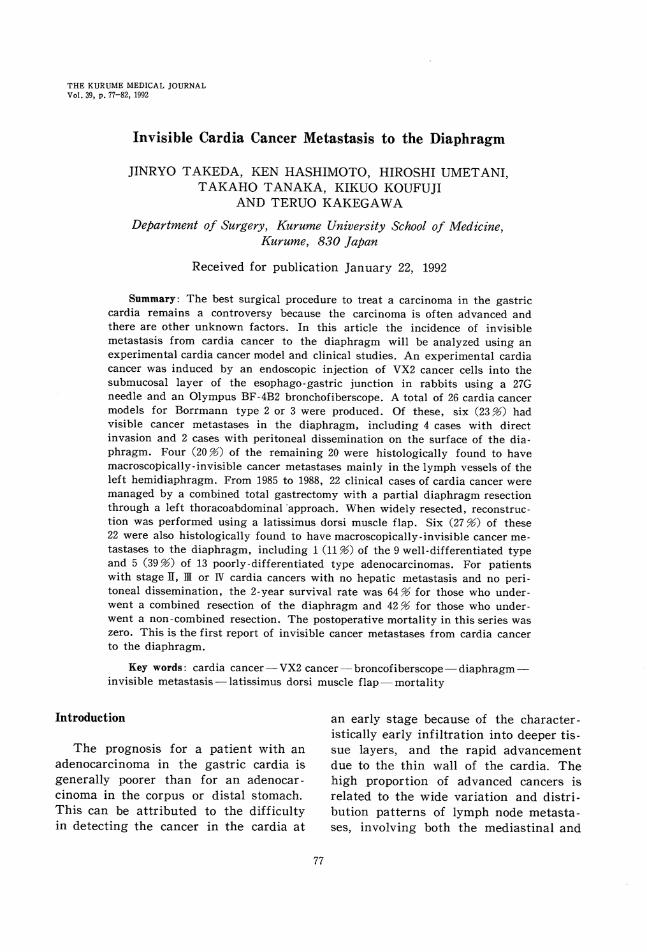
performed on the combined mass-resected together of the esophagus with the stom-ach and diaphragm, using hematoxylin eosin (HE) and Elastica Von Gieson (EVG) staining. Figure 1b shows an example of a rabbit cardia cancer of Borrmann type 2.
Clinical Prospective Studies of an Improved Surgical Procedure
From 1985 to 1988, 22 cardia cancers
were managed by the newly-adopted sur-
Fig. 1a. Summary of invisible cardia
cancer metastases in 4 experimental cases.
CARDIA CANCER METASTASIS TO DIAPHRAGM 79
gical procedure following the experimen-tal results on invisible metastases. This new procedure involved a combined total
gastrectomy with a partial resection of the diaphragm involving an 18-wide re-section, as shown in Fig. 2. The resec-tion was made through the left thoraco-abdominal approach. The indication for resection was positive serosal infiltration
(S2, S3), no hepatic metastasis (H0) and no peritoneal dissemination (P0). After wide a resection, reconstruction was per-formed using a latissimus dorsi muscle flap (Rives et al. 1942; Fujita et al. 1988). Figure 3 shows a widely-resected left hemidiaphragm and cardia cancer, viewed from the upper thoracic side. Eighteen especially-lone blocks were produced from each specimen on the average. The blocks were stained with HE and EVG. Figure 4 shows one of the long blocks of the dia-
phragm together with the lower esopha-gus and cardia with HE stain that was 16 cm in diameter. The left hemidia-
phragm was widely resected leaving a 5 cm anterior margin for reconstruction to the muscle flap after the lower esophag-ectomy plus total gastrectomy. The pos-terior attachment of the diaphragm was resected including the esophageal hiatus together with the lower mediastinal lymph nodes, in combination with a radi-cal tetal gastrectomy usual with pancre-atico-splecectomy and resection of the
paraaortic lymph nodes (No.16).
Results
Experimental Studies
A total of 26 rabbit cardia cancer models were produced from 32 rabbits that were injected. The cancer depth was s0 in 9, se in 14 and sei (infiltration to adjacent organs) in 2, according to the classification of the Japanese Research Society for Gatstric Cancer (1981). Six (23%) of the 26 had diaphragmatic me-
Fig. 1b. An example of a rabbit cardia
cancer of Borrmann type 2.
Fig. 2. A combined resected specimen
of the cardia and left hemidiaphragm in-
volving an 18-wide resection of 16 cm max-
imal diameter.
Fig. 3. The lower esophagus and cardia
together with the left diaphragm, viewed
from the upper thoratic side.
80 TAKEDA, ET AL.
tastases macroscopically, involving 2 with direct invasion and 4 with peritoneal dis-semination on the surface of the dia-
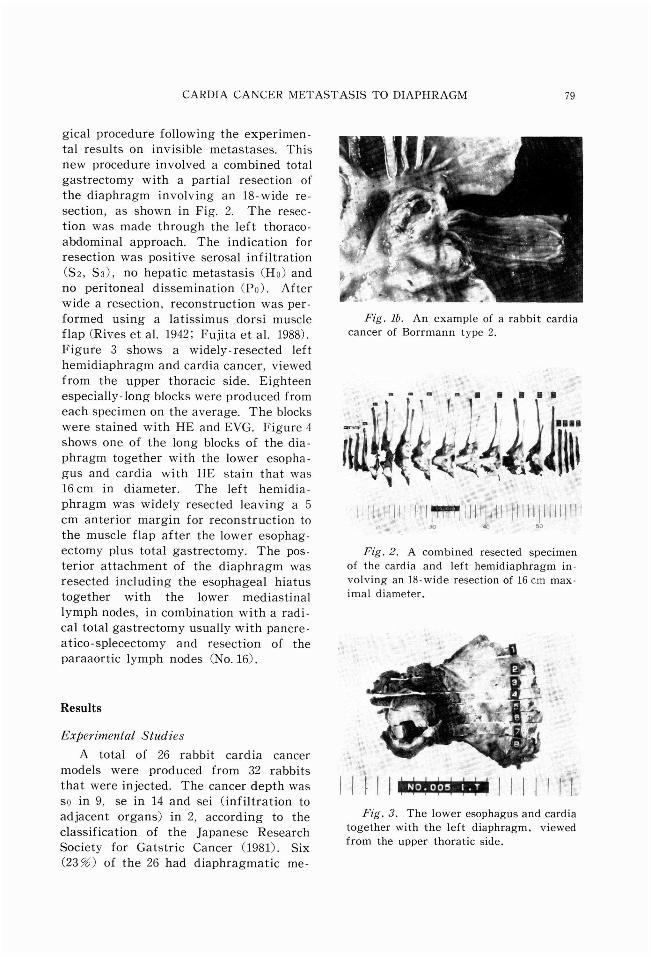
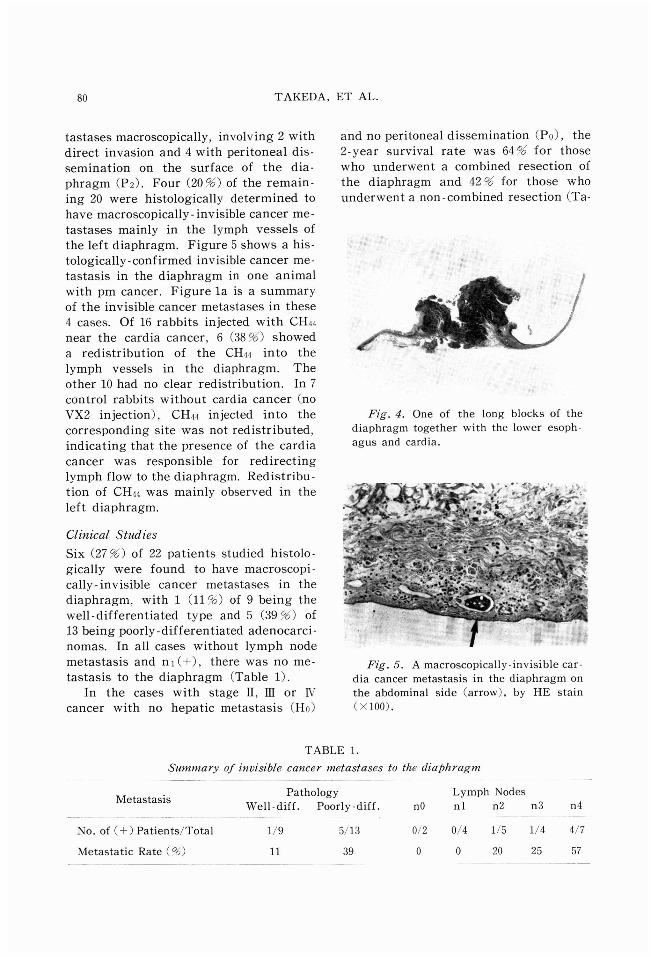
phragm (P2). Four (20%) of the remain-ing 20 were histologically determined to have macroscopically-invisible cancer me-tastases mainly in the lymph vessels of the left diaphragm. Figure 5 shows a his-tologically-confirmed invisible cancer me-tastasis in the diaphragm in one animal with pm cancer. Figure la is a summary of the invisible cancer metastases in these 4 cases. Of 16 rabbits injected with CH44 near the cardia cancer, 6 (38%) showed a redistribution of the CH44 into the lymph vessels in the diaphragm. The other 10 had no clear redistribution. In 7 control rabbits without cardia cancer (no VX2 injection), CH44 injected into the corresponding site was not redistributed, indicating that the presence of the cardia cancer was responsible for redirecting lymph flow to the diaphragm. Redistribu-tion of CH44 was mainly observed in the left diaphragm.
Clinical Studies
Six (27%) of 22 patients studied histolo-
gically were found to have macroscopi-cally-invisible cancer metastases in the diaphragm, with 1 (11%) of 9 being the well-differentiated type and 5 (39%) of 13 being poorly-differentiated adenocarci-nomas. In all cases without lymph node metastasis and n1(+), there was no me-tastasis to the diaphragm (Table 1).
In the cases with stage II, III or IV
cancer with no hepatic metastasis (H0)
and no peritoneal dissemination (P0), the
2-year survival rate was 64% for those
who underwent a combined resection of the diaphragm and 42% for those who
underwent a non-combined resection (Ta-
Fig. 4. One of the long blocks of the
diaphragm together with the lower esoph-
agus and cardia.
Fig. 5. A macroscopically-invisible car-
dia cancer metastasis in the diaphragm on
the abdominal side (arrow), by HE stain
(•~100).
TABLE 1.
Summary of invisible cancer metastases to the diaphragm
CARDIA CANCER METASTASIS TO DIAPHRAGM 81
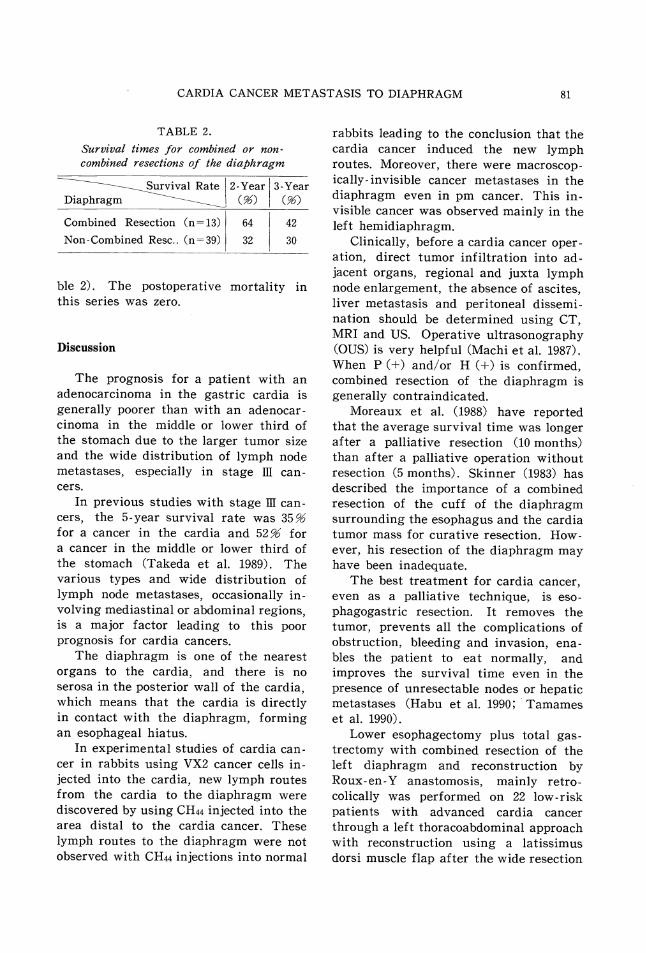
TABLE 2.
Survival times for combined or non-combined resections of the diaphragm
ble 2). The postoperative mortality in this series was zero.
Discussion
The prognosis for a patient with an
adenocarcinoma in the gastric cardia is
generally poorer than with an adenocar-
cinoma in the middle or lower third of
the stomach due to the larger tumor size
and the wide distribution of lymph node
metastases, especially in stage III can-
cers.
In previous studies with stage III can-cers, the 5-year survival rate was 35% for a cancer in the cardia and 52% for a cancer in the middle or lower third of the stomach (Takeda et al. 1989). The various types and wide distribution of lymph node metastases, occasionally in-volving mediastinal or abdominal regions, is a major factor leading to this poor
prognosis for cardia cancers. The diaphragm is one of the nearest
organs to the cardia, and there is no
serosa in the posterior wall of the cardia,
which means that the cardia is directly
in contact with the diaphragm, forming
an esophageal hiatus.
In experimental studies of cardia can-cer in rabbits using VX2 cancer cells in-
jected into the cardia, new lymph routes from the cardia to the diaphragm were discovered by using CH44 injected into the area distal to the cardia cancer. These lymph routes to the diaphragm were not observed with CH44 injections into normal
rabbits leading to the conclusion that the
cardia cancer induced the new lymph
routes. Moreover, there were macroscop-
ically-invisible cancer metastases in the
diaphragm even in pm cancer. This in-
visible cancer was observed mainly in the
left hemidiaphragm.
Clinically, before a cardia cancer oper-ation, direct tumor infiltration into ad-
jacent organs, regional and juxta lymph node enlargement, the absence of ascites, liver metastasis and peritoneal dissemi-nation should be determined using CT, MRI and US. Operative ultrasonography
(OUS) is very helpful (Machi et al. 1987). When P (+) and/or H (+) is confirmed, combined resection of the diaphragm is
generally contraindicated. Moreaux et al. (1988) have reported
that the average survival time was longer after a palliative resection (10 months) than after a palliative operation without resection (5 months). Skinner (1983) has described the importance of a combined resection of the cuff of the diaphragm surrounding the esophagus and the cardia tumor mass for curative resection. How-ever, his resection of the diaphragm may have been inadequate.
The best treatment for cardia cancer, even as a palliative technique, is eso-
phagogastric resection. It removes the tumor, prevents all the complications of obstruction, bleeding and invasion, ena-bles the patient to eat normally, and improves the survival time even in the
presence of unresectable nodes or hepatic metastases (Habu et al. 1990; Tamames et al. 1990).
Lower esophagectomy plus total gas-
trectomy with combined resection of the
left diaphragm and reconstruction by
Roux-en-Y anastomosis, mainly retro-
colically was performed on 22 low-risk
patients with advanced cardia cancer
through a left thoracoabdominal approach
with reconstruction using a latissimus
dors muscle flap after the wide resection

82 TAKEDA, ET AL.
of the diaphragm. The 2-year survival rate for a combined resection of the dia-
phragm was 64%, while it was only 42% for a non-combined resection. The com-bined resection of the diaphragm with extensive lymph node dissection led to improved clinical survival rates. These results can be understood in light of the
possible incidence of macroscopically-in-visible cancer metastases. The lymph-adenectomy in the combined resection has a higher curativity-involving a more ex-tended lymph node dissection, including both mediastinal and abdominal lymph nodes with the hiatus. The highest fre-
quency (25%) of paraaortic lymph node (No.16) metastasis occurred in cardia cancers rather than in middle or lower third cancers (Hashimoto et al. 1990).
To improve the surgical results for advanced cardia cancer, especially in-volving a serosal exposure, an extended total gastrectomy is required with a rad-ical lymph node dissection. When indi-cated, a combined resection of the dia-phragm through a left thoracoabdominal approach should be performed. An early diagnosis is, of course, an added advan-tage (Tanaka et al. 1990). There is no other report of a macroscopically-invisible cancer metastasis from a cardia cancer to the diaphragm.
References
FUJITA, M., HASHIMOTO, K., TAKEDA, J., MACHI, J. and KAKEGAWA, T. (1988). Diaphragmatic re-construction using latissimus dorsi muscle flap following wide resection of the dia-phragm combined with esophago-gastrec-tomy for cardia cancer. Jpn. J. Surg. 18, 480-482.
HABU, H., SAITO, N., SATO, Y., TAKESHITA, K., SUGAWA, M, et al. (1990). Results of surgery
in patients with gastric cancer extending to adjacent organs. Hepato-Gastroenterol. 37, 417-420.
HASHIMOTO, K., TAKEDA, J., TANAKA, T., KOUFUJI,
K., IWAI, T, et al. (1990). Significance and actual status of the dissection of paraaortic lymph nodes in cases with gastric cancer. Kurume Med. J. 37, 159-164.
Japanese Research Society for Gastric Cancer. (1981). The general rules for gastric cancer study in surgery and pathology. Jpn. J. Surg. 11, 127-139.
KIDD, J. G. and Rous, P. (1940). A transplantable rabbit carcinoma in a virus-induced papil-loma and containing the virus musked or
altered form. J. Expt. Med. 71, 813-815.MACHI, J., TAKEDA, J., KAKEGAWA, T., YAMANA, H.,
FUJITA, H, et al. (1987). The detection of
gastric and esophageal tumor extention by high-resolution ultrasound during surgery. World J. Surg. 12, 664-671.
MOREAUX, J, and MSIKA, S. (1988). Carcinoma of the gastric cardia. Surgical management and long-term survival. World J. Surg. 12, 229-235.
RIVES, J. D. and BAKER, D. D. (1942). Anatomy of the attachment of the diaphragm. Their relation to the problems of the surgery of diaphragmatic hernia. Ann. Surg. 115, 745-755.
Rous, P. (1965). Virus and tumor causation. An appraisal of present knowledge. Nature 207, 457-461.
SKINNER, D. B. (1983). En bloc resection for neo-
plasms of esophagus and cardia. J. Thorac. Cardiovasc. Surg. 85, 59-71.TAKEDA, J., HASHIMOTO, K., KOUFUJI, K., TANAKA,
T., UMEZU, T, et al. (1989). Esophageal in-vasion by an upper gastric cancer. Retro-spective evaluation and prognosis. Kurume Med. J. 36, 75-79.
TAMAMES, S., DEVEGA, D. S. and TAMAMES, S. JR. (1990). Surgical management of malignant tumors of the esophagogastric junction. Int. Surg. 75, 417-420.
TANAKA, T., TAKEDA, J., HASHIMOTO, K., KOUFUJI, K., YANO, S. et al. (1990). Clinical and path-ological evaluation of early cancer in the
gastric cardia. Kurume Med. J. 37, 265-269.