Embed Size (px)
Citation preview

Insights in tumorigenesis and metastasis of uveal melanomaNotting, I.C.
CitationNotting, I. C. (2009, January 27). Insights in tumorigenesis and metastasis ofuveal melanoma. Retrieved from https://hdl.handle.net/1887/13532 Version: Corrected Publisher’s Version
License: Licence agreement concerning inclusion of doctoral thesisin the Institutional Repository of the University of Leiden
Downloaded from: https://hdl.handle.net/1887/13532 Note: To cite this publication please use the final published version (ifapplicable).

Introductionto
Insights of Tumorigenesisand
Metastasisof
Uveal Melanoma
I.C. Notting

Although considerable progress has been made in elucidating the biological mechanisms underlying uveal melanoma growth and dissemination, further investigation is required as there is still no effective treatment available for metastasis in uveal melanoma patients. Identification of genes, proteins and pathways involved in the metastatic disease has started to provide some insight in the dissemination of uveal melanoma. In order to be able to treat or prevent metastatic disease, development of novel anti-cancer strategies is urgent and requires more sensitive and less invasive methods, to detect and monitor in vivo tumor growth and metastatic disease in cancer models.The main objective of this thesis is to develop a new model in which local tumor growth and metastatic disease can be studied and to explore tumor growth mechanisms of uveal melanoma.
Uveal melanoma - Clinical aspects
Uveal melanoma is the most common primary malignant intraocular tumor in adults, with an annual incidence of 6–8 per million in Caucasians 1 . The incidence increases from the age of 30 up to the age of 70, with a peak incidence in the sixth decade 2, 3 . Uveal melanoma develops in one of the most capillary-rich tissues of the body and has a hematogenous dissemination. The therapy of uveal melanoma remains problematic due to a high rate of metastatic dissemination irrespective of the success of treatment of the primary tumor. This suggests that dissemination and metastasis are early events during uveal melanoma development. There is no evidence that early detection of micrometastasis has led to improved survival. It is, however, important to note that formation of micrometastasis is the pathological basis for the occurrence of clinically overt metastasis. Therefore, development of therapeutic strategies aimed towards interfering with initial events in organ colonization and dissemination of metastasis is required.Metastases are predominantly localized in the liver (87%), lungs (46%) and bone (29%) 4 . Upon diagnosis of uveal melanoma the patient’s median survival time is 6,5 years 5 . Once hepatic metastases have been diagnosed, the patient’s life expectancy is less than 7 months 4, 6-8 .
Diagnosis and treatment
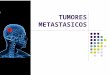
Melanocytes are embryologically derived from the neural crest. In the mature eye melanocytes occur in choroidal stroma and provide its brown color (Figure 1). Melanocytes contain fine pigment granules (melanosomes), are 0.3-0.4µm wide, oval in shape, yellowish to darkbrown in color and smaller than those of the retinal pigment epithelium 9 . The diagnosis of uveal
Aim of the thesis
10
Chap
ter 1

melanoma can usually be made by recognition of the typical ophthalmoscopic features of the neoplasm (Figure 2A and B) 10 .
Illustration of the Eye
Figure 1: Schematic overview of the eye. Melanocytes of the uvea are present in the choroid, iris and cilliary muscle (Charlie Web, [email protected]).
Ancillary diagnostic studies as ultrasonography and fluorescein angiography are important aids in the diagnosis. In atypical cases, the use of sophisticated techniques such as magnetic resonance imaging and transocular fine-needle aspiration biopsy, may provide further diagnostic assistance 11-13 .The management of malignant melanoma of the posterior uvea has been a topic of great controversy 14-16. A number of authorities have challenged the traditional treatment by enucleation of the tumor-containing eye, and clinicians more frequently are using alternative methods of management when possible. Current management ranges from periodic observation and fundus photography of selected small lesions that appear dormant, to thermotherapy, plaque radiotherapy, beam teleradiotherapy, local resection or a combination of these treatment modalities 17, 18 . In case the tumor is far advanced (largest tumor diameter >16 mm and/or thickness >8mm) and there is no hope for eye saving treatment or useful vision, enucleation is often inevitable 19 . Enucleation is performed in less than 20% of cases today. In cases with massive orbital extension, orbital exenteration might be necessary 20-23 .However, choosing the optimal therapy is a complex issue and treatment must be individualized in each case. In selecting a therapeutic approach, certain factors should be carefully weighed. These include the visual acuity and intraocular pressure in the affected eye, the size of the melanoma, its extent and location, scleral outgrowth and cytogenetic features, apparent melanoma activity, the condition of the opposite eye, age and general health of the patient,
Introduction 11

the exclusion of distant metastasis (figure 3) and the psychological status of the patient.
A B
Figure 2A: Picture of a uveal melanoma of the choroid(*) detected with funduscopyFigure 2B: Picture of an enucleated eye with an uveal melanoma of the choroid (*)
Figure 3: Picture of multiple pigmented liver metastasis of a uveal melanoma. Reproduced with permission of Prof. Tollenaar, Department of Surgery, Leiden University Medical Center, the Netherlands.
Pathogenesis of uveal melanoma
Histologically, uveal melanoma cells have been classified as 1) spindle-shaped, 2) epithelioid or 3) mixed types. The epithelioid phenotype has been associated with poor prognosis and metastatic behavior 24-26 . Well-known established prognostic factors are tumor thickness, diameter and localization, cell type, monosomy of chromosome 3 especially in combination with concurrent loss of chromosome 1, number of mitosis and vascular loops 8, 27-29 . Monosomy of chromosome 3 and a large tumor diameter are the most significant factors
! !
*
*
12
Chap
ter 1

determining survival of patients 30 .Monosomy 3 occurred in around 50% of cases 31, 32 . It has been suggested that this aberration plays an important role as initiator or as an early step in melanoma development 33-35 .
OncogenesThe c-myc oncogene locus has been found in 65% of uveal melanoma 36, 37 and an association was established with c-myc amplification and increased tumor size 38 . Expression of c-met (proto-oncogene) was found in uveal melanoma cell lines 39 , but the c-met ligand, hepatocyte growth factor/scatter factor (HGF/SF) was not expressed. Interestingly, uveal melanoma tissue with liver metastasis expressed HGF/SF most intense at the level of the choriocapillaris which may be a site of dissemination, suggesting that it may play a role in the metastatic process 39 . The importance of oncogenic mutations in the RAS/RAF/MEK/ERK pathway has been well documented in human cancers. More than 15% of all human cancers harbor point mutations of RAS 40 . Although several studies showed no mutations for this specific pathway 41-44 , a recent report proved that BRAF (v-raf murine sarcoma viral oncogene homolog B1) is mutated in 50% of uveal melanoma 45 .
Tumor suppressor genesThe Rb (retinoblastoma) gene and p53 transcription factor play an important role in several tumors like retinoblastoma and osteosarcoma 46, 47 , but no Rb or p53 mutations or selected genes in these pathways (p14, p15, p16, and TGF-β R2), have been found in uveal melanoma 48-50 . Van der Velden et al., demonstrated that hypermethylation of p16 is a cause of inactivation of this gene, which interestingly was more frequently in tumors from patients with metastatic disease 51 . However, uveal melanoma may contain functional abnormalities in the Rb and p53 pathways, rather than mutations in these factors themselves. For instance, expression of 15% or more of cyclin D1, an activator of Rb kinase and HDM2 (human homologue of murine double minute) protein, an inhibitor of p53 in uveal melanoma is associated with an unfavorable outcome 52, 53 .
Dissemination and metastasis Blood vessels are assembled during embryonic development by vasculogenesis, which is a primitive vascular network is established from endothelial precursors. The process of blood vessel formation from ore-existing ones is known as angiogenesis or neovascularization. Angiogenesis is critical to chronic inflammation and fibrosis, to tumor growth, and to the vascularization of ischemic tissues. Tumors stimulate the growth of host blood vessels, which is essential for supplying nutrients to the tumor. Tumors cannot grow beyond 1 to 2 mm in diameter or thickness unless they are vascularized 54 (see section 1.4 Angiogenesis and vasculogenic mimicry). Angiogenesis is a requisite not only for continued tumor growth, but also for metastasis. Without access to the vasculature, the tumor cells cannot spread to distant sites. Tumor blood vessels differ from the normal vasculature by being tortuous and irregularly shaped and being leaky. The leakiness is attributed largely to the increased
Introduction 13

production of VEGF (vascular endothelial growth factor). Tumor cells may line structures that resemble capillaries, a phenomenon called vascular mimicry 28, 55 .In order to acquire motility and invasiveness, carcinoma cells must shed many of their epithelial phenotypes, detach from epithelial sheets, and undergo a drastic alteration: the epithelial–mesenchymal transition (EMT) 56 . Recall that the EMT involves a shedding by epithelial cells of their characteristic morphology and gene expression pattern and the assumption of a shape and transcriptional program characteristic of mesenchymal cells. This major shift in epithelial cell phenotype is necessary for the reconstruction of epithelial cell layers after wounding. The EMT is used even more widely in certain morphogenetic steps occurring during embryogenesis, when tissue remodeling depends on EMT executed by various types of epithelial cells. It is plausible that all types of carcinoma cells must undergo an EMT in order to become motile and invasive. The cellular changes associated with EMT encompass the loss of cytokeratin, E-cadherin expression and cell polarity. EMT also coincides with the acquisition of motility, invasiveness, vimentin, altered adhesion suppresion and proteinase secretion. Invasion and metastasis are biological hallmarks of malignant tumors. The acquisition of an invasive phenotype through the expression of proteolytic enzymes provides mechanisms for uveal melanoma cell to overcome the physical constraints imposed on them by intercellular junctions and the extra-cellular matrix. The matrix metalloproteinase (MMP) family of enzymes is involved in the degradation of extra-cellular matrix components at the tumor-host tissue interface. This is a key event in the invasive process 57, 58 . MMP2 and MMP9 expression has been associated with metastasizing primary uveal melanoma and reduced survival 59-62 .The migration of neuroepithelial cells, like melanocytes, from the neural crest into the mesenchyme of early vertebrate embryos also depends on a transformation of cell phenotype that can best be described as an EMT. Expression of E-cadherin and cytokeratins - hallmarks of epithelial cell protein expression - is repressed, while the expression of vimentin, an intermediate filament component of the mesenchymal cell cytoskeleton, is induced. Epithelial cells that have undergone an EMT often begin to make fibronectin, an extracellular matrix protein that is normally secreted only by mesenchymal cells such as fibroblasts. At the same time expression of a typical fibroblastic marker - N-cadherin - is often acquired in stead of E-cadherin. These and alike observations indicate the involvement of certain heterotypic signals that originate in the reactive stroma of primary carcinomas, which impinge on neoplastic cells located at the outer edges of the epithelial cell mass, and induce these cells to undergo an EMT. N-cadherin is expressed in fibroblast and invasive carcinomas like uveal melanoma 63 . A micro-array study showed that primary uveal melanoma can be divided into 2 classes: a group with low risk and an aggressive group with high risk for metastatic death. One of the genes discovered is Id2 (helix-loop-helix inhibitor), which was down-regulated in the aggressive group. Id2 seemed to suppress the epithelial-like phenotype by inhibiting the E-cadherin promoter 64 . Abundant evidence indicates that transforming growth factor
14
Chap
ter 1

(TGF) β is an important agent for conveying these stromal signals 65 . TGFβ is known to be capable of suppressing the growth of normal human melanocytes but this response is lost in melanoma cells 66-69 . TGF-β has a potential dual role in controlling uveal melanoma invasion: down-regulation of adhesion and up-regulation of protease secretion. 70, 71 . Uveal melanomas could be regulated by both autocrine and paracrine stimulation of TGF-β. TGF-β can modulate a wide variety of immune reactions 72, 73 and it has been documented that TGF-β, at concentrations found in the aqueous humor of the eye, can significantly alter MHC (major histocompatibility complex) class I antigen expression and the susceptibility of ocular melanoma cells to natural killer cell mediated cytolysis 74, 75 . TGF-β may specifically regulate interaction of uveal melanoma cells with hepatic endothelium by promoting adhesion.Another member of the TGFβ superfamily, Bone Morphogenetic Protein -7 (BMP7), has been shown to induce Mesenchymal-to-Epithelial Transition (MET) (and/or inhibit EMT) (see section 1.3 Bone Morphogenetic Protein family members in the TGFβ pathway) 76, 77 .
Bone Morphogenetic Proteins (BMPs) are multi-functional growth factors belonging to the transforming growth factor β superfamily. Fifteen BMPs have been identified, which have the unique function of inducing bone formation 78 . Although BMPs are synthesized by skeletal cells, their synthesis is not limited to bone because they are expressed by a variety of extraskeletal tissues in which they play a critical role in development and cell function. A fundamental function of BMPs is to induce differentiation of mesenchymal cells toward cells of the osteoblast lineage thus promoting osteoblastic maturation and function 79 . As osteoblasts undergo terminal differentiation and the cellular matrix mineralizes, they undergo apoptosis 80 .Besides in skeletal development BMPs (and their antagonists) play a crucial role in organogenesis and postnatal development . Gene inactivation of various BMPs often result in significant phenotypic changes in various organs. For example: BMP7 null mice display lack of eye and glomerular development, leading to renal failure and neonatal death 81-83 . These mice also have modest forms of skeletal abnormalities including fused ribs and vertebral or skull defects. Furthermore, BMPs play an important role in the pathophysiology of several diseases including osteoporosis 84 , arthritis 85 , kidney diseases 65, 86, 87 , pulmonary hypertension 88 , cerebrovascular diseases 89 and cancer 90 . BMP signaling is precisely regulated by BMP antagonists 91, 92 . The interplay between BMPs and their antagonists governs developmental and cellular processes like establishment of induction of neural tissue, formation of the eye and formation of joints in the skeletal system 85 . Mesenchymal cell lines, bone marrow cells, osteoblast precursors, myoblasts, fibroblasts and neural cells all respond to BMPs.Recent research shows a disparate role of BMP in the stem cell biology 93 . Stem cells originating from neural crest tissue give rise to diverse cell types including uveal melanocytes
Bone morphogenetic protein family members of TGFβ superfamily
Introduction 15

94 . These neural crest stem cells treated with TGFβ differentiate into specific cell types 95 . BMPs have been shown to differentiate mouse embryonic stem cells 96 . Neural crest cells and metastatic cancer cells share phenotypic similarities such as high motility and invasiveness and can follow the same migratory pathways 97 . BMPs consist of dimers the chains of which are connected by disulfide bonds and this dimerization is a prerequisite for bone induction. BMPs are both active as homodimer and heterodimer molecules.
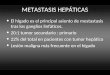
Figure 4: BMPs can bind to a type II specific receptor present on the cell membrane and recruit a type I receptor, forming a complex. These receptors are transmembrane serine/threonine kinase proteins that self-phosphorylate after formation of the BMP-receptor II-receptor I complex and acquire the ability to phosphorylate Smad proteins, a family of TGF β transducers.
One member of the BMP family, the 35-kDa homodimeric protein BMP7, appears to be a prerequisite for induction of condensation and epitheliazation of metanephric mesenchyme in the kidney 65, 98, 99 . Furthermore, knockout studies have shown that BMP7 (and BMP4) are essential for early morphogenesis of the eye 81-83, 100, 101 . BMP7 knockout mice revealed deficient ocular growth, resulting in epithelial development disturbances, e.g. absence of the lens and abnormal retinal organization, with disorganization of the pigment layer of the retina 82 . BMP7 also plays a role in various pathological conditions (inflammation, diabetic retinopathy, fibrosis). In mesangial cells of the kidney BMP7 counteracted TGFβ induced fibrosis, reversing the process of chronic renal injury and maintaining an epithelial phenotype. Moreover, BMP7 experimental therapy showed to halt progression and reverse the effects of chronic progressive kidney disease 65, 84, 86 . BMP7 counteracts the increased expression of several extracellular matrix (EMC) proteins and CTGF (connective tissue growth factor) 84,
102 .
16
Chap
ter 1

One member of the family of BMP antagonists, differential screening-selected gene aberrative in neuroblastoma (DAN, also known as NO3) encodes a secreted protein in the cysteine knot super family 103 . Nakamura et al. 104 found that endogenous DAN mRNA was up regulated during retinoic acid-induced neuroblastoma differentiation, indicating that DAN might be involved in neuronal differentiation. During some stages of embryogenesis DAN has been found in the eye 105, 106 . Biochemical analyses have demonstrated that DAN bound directly to BMP2 107, 108 and interfered with BMP4 activity 107, 109 . Over-expression of DAN in transformed cell lines suppressed the transformed phenotype and reduced growth rate 103,
110 . In animal models, DAN exhibited BMP antagonist activity 92, 107, 109, 111 and Wnt inhibition 105, 106, 112 . Expression of DAN was significantly reduced in malignant fibroblast cells and similarly over expression of DAN inhibited proliferation of these cells 103, 110 .
Angiogenesis and vasculogenic mimicry
Angiogenesis (physiologic) or neovascularization (pathologic) is defined as the formation of blood vessels from pre-existing vessels. It extends and remodels the primitive vasculature, giving rise to a complex vascular network. Angiogenesis is a multi-step process, which is regulated by soluble factors and cell matrix interactions 113, 114 . Activation of endothelial cells by angiogenic stimuli derived from non-endothelial cells 115 resulted in expression of proteolytic enzymes 116 and in site-directed proteolytic activity 117 . The extracellular matrix components surrounding the endothelial cells are degraded locally by proteases, allowing for chemotactic migration of endothelial cells toward angiogenic stimuli. Endothelial cells thereupon proliferate and form a new vessel with a lumen. Adjacent sprouts anastomose and form loops, which become perfused with circulating blood. In growing tumors it became apparent that the driving force triggering the formation of a vascular network is oxygen tension. If a tumor reaches the critical size of > 2mm3 the process of diffusion is no longer sufficient to cover all tissue and there will be a decrease in oxygen level. Under conditions of hypoxia functional HIF-1 (hypoxia-inducible factor) accumulates in the cell, which in turn drives the expression of a number of genes whose products encourage angiogenesis. Prominent among these is VEGF-A 115 . Other angiogenic factors may also play a role in the angiogenic process of uveal melanoma. High expression of SPARC (secreted protein acidic and rich in cysteine), Cyr (cysteine rich) 61 and TF (tissue factor) in uveal melanoma is correlated with blood vessel rich areas of the tumor and an aggressive phenotype 118 . TSP2 (thrombospondin), an anti-angiogenic protein, was associated with smaller areas of blood vessels 119 . Endoglin, a transmembrane regulatory receptor for TGFβ, has been suggested to be a specific marker for angiogenesis in uveal melanoma 120 .The phenomenon of angiogenic switch is an important step in tumor progression. The body purposefully denies its cells the ability to readily induce angiogenesis. By doing so, the body erects yet another impediment to block the development of large tumors. The angiogenic
Introduction 17

switch is the moment when the tumor successfully breaks this defensive barrier and cancer cells get the ability to induce blood vessel growth. Part of these tumor blood vessels is leaky and immature because the pericytes and smooth muscle cells are usually poorly recruited to the tumors.Lymphatic vessels are also part of the vascular circulatory system. The lymphatic system is made up of an extensive network of capillaries, collecting vessels and ducts that permeate most of the organs 121 . Unlike the blood vasculature, which forms a continuous loop, the lymphatic system is an open ended, one-way transit system. The vessels collect extravasated protein-rich fluid and lymphocytes that are transferred from lymphatic capillaries to the collecting lymphatic vessels and ultimately into venous circulation. The lymphatic vessels form a part of the immune system by continuously transporting the white blood cells within the lymphoid organs (spleen, tonsils lymph nodes etc.) and bone marrow 122 . Abnormal function of lymphatic vessels is implicated in conditions such as lymphedema, inflammation and immune disease. Perhaps most importantly, the lymphatic vessels are involved in tumor metastasis 123, 124 . Lymphangiogenesis is not present in the normal eye or in uveal melanoma 125 .Vasculogenic mimicry describes the formation of perfusion pathways in tumors by highly invasive, genetically deregulated tumor cells 28, 55 . It is termed vasculogenic because, although these pathways do not form from pre-existing vessels, they distribute plasma and may contain red blood cells. It is termed mimicry because the pathways are no real blood vessels, but vascular function is mimicked. In vasculogenic mimicry of the patterned matrix type highly invasive tumor cells form looping patterns rich in extracellular matrix (ECM) in vitro 28 . Vasculogenic mimicry patterns are composed of laminin, collagen IV and VI, fibronectin and glycosaminoglycans 126-129 . There is a strong association between the histological proof of vasculogenic mimicry patterns in primary uveal melanoma and subsequent death by metastasis 28, 130 .
VEGF family of growth factors and VEGF receptors
The vascular endothelial growth factor (VEGF) family consists of 7 members (VEGF-A to E and placenta growth factor 1 and 2 (PIGF-1 and-2)). Their expression pattern is correlated with pathological and physiological angiogenesis 131, 132 . The VEGF family factors mediate signals by activating VEGF-receptor (VEGFR) including VEGF-R1, -2 and –3 133 .Five isoforms of VEGF-A are generated from the human VEGF-A gene by alternative splicing (VEGF-A 121, VEGF-A 145, VEGF-A 165, VEGF-A 189 and VEGF-A 205) 134, 135 . VEGF-A is expressed by many cell types throughout the body and acts as a paracrine factor on endothelial cells and non-endothelial cells such as tumor cells 131 . At sites of apparent angiogenesis VEGF-A levels are increased in cells surrounding sprouting tissue. In adults VEGF-A expression is mostly related to conditions of pathological angiogenesis as indicated
18
Chap
ter 1

by increased VEGF-A expression like in highly vascularized tumors or ocular diseases e.g. diabetic retinopathy 115 . Consistent with this the expression of VEGF-A is potentiated in response to hypoxia and by activated oncogenes as well as a variety of cytokines 136, 137 . Protein levels of VEGF-A 165 in the aqueous humor of eyes with uveal melanoma are correlated with patient survival, basal tumor diameter and tumor height 138, 139 . One report suggests that uveal melanomas express VEGF-A 140 . In most ciliochoriodal melanomas VEGF-immunoreactivity is correlated with necrosis, but not with the occurrence of systemic metastasis or tumor angiogenesis 141 .VEGF-B is most closely related to VEGF-A. VEGF-B is, according to expression and gene targeting studies, supposed to play a role in vascularization of heart and skeletal muscles 142,
143 . VEGF-B is likely to act in a paracrine fashion as its receptor is almost exclusively located on endothelial cells 144 . Several studies show that VEGF-B is present in malignant tumors 145,
146 and therefore may induce tumor angiogenesis.VEGF-C stimulates the migration of endothelial cells and increases vascular permeability and endothelial cell proliferation, but at higher concentrations than VEGF-A. Unlike VEGF-A, the expression of VEGF-C does not appear to be regulated by hypoxia, but is increased in response to proinflammatory cytokines 147, 148 . VEGF-C can regulate physiological and pathological blood vessel growth in vivo. Furthermore, VEGF-C has been shown to
Figure 5: Binding of VEGFs to the various receptors is depicted.
regulate the growth of lymphatic vessels. The angiogenic versus lymphangiogenic responses to VEGF-C may depend on the degree of proteolytic processing of its precursor and on the expression of its receptors in the blood versus lymphatic endothelial cells of the target tissue. Signals for endothelial cells are probably mediated through VEGFR-2 (KDR) in
Introduction 19

blood vascular endothelial cells and via VEGFR-3 (Flt 4) in lymphatic endothelial cells 149 . VEGF-C furthermore acts synergistic with VEGF-A during the induction of angiogenesis 150 . In a molecular profiling study 151 , VEGF-C was significantly upregulated (30-fold) in highly versus poorly invasive uveal melanoma cells. Clarijs et al. 125 showed that VEGF-C was not able to induce lymphangiogenesis in the normal eye and in uveal melanoma. VEGF-C has been found to induce the formation of new blood vessels, but only in early development or in certain pathological settings such as tumorigenesis 124 .VEGF-D is the most recently discovered member of the family and shares 61% sequence identity with VEGF-C. These two growth factors bind to the same receptors on human endothelial cells. VEGF-D has been shown to be able to stimulate the proliferation of endothelial cells 152 . Stacker et al.153 showed that VEGF-D can induce lymphangiogenesis and thereby allow the access of tumor cells to the lymphatic network.
Animal models related to uveal melanoma development, progression and metastasis
Prospective and retrospective data of clinical studies are important factors in uveal melanoma research. Registries of ocular pathology have also played an essential role in acquiring knowledge of this malignant neoplasm. One of the main limitations of research is the low incidence of this tumor, making it difficult to achieve a representative number of cases. Moreover, with the increasing use of conservative treatments in the last few decades the number of enucleation specimens for pathology has decreased. For these reasons the development and use of experimental models is necessary 154 . Many attempts have been made to develop a suitable animal model to study more effectively the etiology, pathogenesis, diagnosis, metastasis and therapy of uveal melanoma. Uveal melanoma may spontaneously occur in some animals, specifically mammals 155-158 . The different histological features, metastatic behavior and unpredictable nature of occurrence of these uncommon spontaneous tumors in comparison to human ocular melanoma diminish their suitability as a model. Several models have been developed to induce an intraocular tumor chemically or by radiation of animals 159-162 . Some of these induced tumors might resemble human uveal melanoma, although the majority originates from retinal pigment epithelium. Various viruses have been used to biologically induce uveal proliferations, disadvantages is the high mortality among infected animals. Injected animals often develop disseminated viral infections and secondary tumors induced by virus shed from primary intraocular melanoma rather than metastases 163-165 . Inoculation of tissue culture of hamster-, murine- or human melanoma cells into animal eyes have the advantage that the inoculation site and size may be controlled 166-168 . Unfortunately, immune suppression occurs in some models. Transgenic murine models have been developed, using the promoter region of tyrosinase gene to target expression of oncogenes in melanine producing cells 169 . The tyrosinase gene was chosen because it drives the expression of downstream genes in melanocytes 170 . Human uveal melanoma cell lines are also used to
20
Chap
ter 1

induce orthotopical tumors and distant metastasis 171 . Cells can be injected into the anterior chamber of the eye of nude mice 172 . Some cell lines will develop distant metastasis after enucleation of the orthotopically-induced tumor 154, 165, 173 . Disadvantages of these models are problems with monitoring tumor growth during the experiment and localization of the metastasis.In conclusion, the ideal animal model of uveal melanoma should meet a number of conditions 174 :
There should be structural similarities between the animal eye and the human eye.•The cellular physiological behavior and reaction to drug administration should be •similar for animals and humans.The etiology and evolution of the disease should be comparable to the human •pattern.The rate of tumor outgrowth should be as high as possible (near 100%) in order to •minimize the use of animals.Tumor growth should be follow-able directly and quantitatively for adequate follow-•up of the disease and the effect of the treatments administered.
Several animal models have been used to study primary and metastatic uveal melanoma as well as treatments for these tumors and ways to prevent metastasis.In the study of Clark et al. 175 the effect of the angiostatic agent anecortave acetate was studied in an animal model of a murine uveal melanoma cell line injected into the anterior chamber of the eye. Restricted growth was observed after topical treatment. Interferon-alpha-2b was tested for its effect on metastatic disease of melanoma cells inoculated into the posterior chamber of the eye 176 . It resulted in decreased development of metastasis.Ma et al. 177 developed a human uveal melanoma model in nude mice with viral overexpression of PAI-1, which resulted in a reduction of liver metastasis. They also studied the relation of epidermal growth factor receptor (EGFR) expression and metastasis of uveal melanoma in nude mice model.
Outline of the thesis
The studies described in this thesis are an attempt to increase the knowledge with respect to biological mechanisms in uveal melanoma in vitro, in vivo and in patients. This knowledge might be used to consider new treatment modalities for uveal melanoma and its metastatic disease. A new animal model for uveal melanoma described in Chapter 2 provides a method to follow tumors cells in a living animal. This xenograft model, based on real time bioluminescent imaging of luciferase-expressing human melanoma cells, allows for cell tracking and non-invasive monitoring of tumor growth, metastasis and therapeutic response. The role of BMP7 in tumor progression was studied, using a human uveal melanoma cell
Introduction 21

line and transfecting this cell line with the gene of interest, BMP7 (Chapter 3). In the study described in Chapter 4 we investigated the tumor suppressor gene DAN, an antagonist of the BMP pathway, in enucleation specimens of uveal melanoma patients.Angiogenesis as an important process in melanoma development is described in Chapters 5 & 6. Chapter 5 describes the VEGF-family factors and their profile in vitro, in vivo and in patients at a molecular level. The study in Chapter 6 presents the correlation of tumor parameters with the presence of angiogenic factor VEGF-A in the aqueous humor of patients. In the Discussion (Chapter 7) implications of the findings presented in this thesis on the understanding of the biological mechanisms are discussed in detail, with special emphasis on their relevance to uveal melanoma tumor growth and metastatic behavior.
References
1. Egan KM, Seddon JM, Glynn RJ, Gragoudas ES, Albert DM. Epidemiologic aspects of uveal
melanoma. Surv Ophthalmol. 1988;32:239-251.
2. Jensen OA. Malignant melanomas of the uvea in Denmark 1943-1952. A clinical, histopathological,
and prognostic study. Acta Ophthalmol (Copenh). 1963;43:Suppl-220.
3. Raivio I. Uveal melanoma in Finland. An epidemiological, clinical, histological and prognostic study.
Acta Ophthalmol Suppl. 1977:1-64.
4. Gragoudas ES, Egan KM, Seddon JM, et al. Survival of patients with metastases from uveal melanoma.
Ophthalmology. 1991;98:383-389.
5. McLean IW, Foster WD, Zimmerman LE, Martin DG. Inferred natural history of uveal melanoma.
Invest Ophthalmol Vis Sci. 1980;19:760-770.
6. Kath R, Hayungs J, Bornfeld N, Sauerwein W, Hoffken K, Seeber S. Prognosis and treatment of
disseminated uveal melanoma. Cancer. 1993;72:2219-2223.
7. Rajpal S, Moore R, Karakousis CP. Survival in metastatic ocular melanoma. Cancer. 1983;52:334-336.
8. Seddon JM, Albert DM, Lavin PT, Robinson N. A prognostic factor study of disease-free interval and
survival following enucleation for uveal melanoma. Arch Ophthalmol. 1983;101:1894-1899.
9. Wollf’s Anatomy of the eye: Hodder Arnhold; 1998.
10. Shields JA, Young SE. Malignant tumors of the uveal tract. Curr Probl Cancer. 1980;5:1-35.
11. Bakri SJ, Sculley L, Singh AD. Imaging techniques for uveal melanoma. Int Ophthalmol Clin.
2006;46:1-13.
12. Shields JA, Shields CL, De Potter P, Singh AD. Diagnosis and treatment of uveal melanoma. Semin
Oncol. 1996;23:763-767.
13. Sisley K, Nichols C, Parsons MA, Farr R, Rees RC, Rennie IG. Clinical applications of chromosome
analysis, from fine needle aspiration biopsies, of posterior uveal melanomas. Eye. 1998;12 ( Pt
2):203-207.
14. Zimmerman LE, McLean IW, Foster WD. Does enucleation of the eye containing a malignant
melanoma prevent or accelerate the dissemination of tumour cells. Br J Ophthalmol. 1978;62:420-425.
22
Chap
ter 1

15. Manschot WA, van Peperzeel HA. Choroidal melanoma. Enucleation or observation? A new approach.
Arch Ophthalmol. 1980;98:71-77.
16. Seigel D, Myers M, Ferris F, III, Steinhorn SC. Survival rates after enucleation of eyes with malignant
melanoma. Am J Ophthalmol. 1979;87:761-765.
17. De Potter P, Shields CL, Shields JA. New treatment modalities for uveal melanoma. Curr Opin
Ophthalmol. 1996;7:27-32.
18. Shields CL, Shields JA, DePotter P, Kheterpal S. Transpupillary thermotherapy in the management of
choroidal melanoma. Ophthalmology. 1996;103:1642-1650.
19. Shields JA, Shields CL, Donoso LA. Management of posterior uveal melanoma. Surv Ophthalmol.
1991;36:161-195.
20. Oosterhuis JA, Journee-de Korver HG, Kakebeeke-Kemme HM, Bleeker JC. Transpupillary
thermotherapy in choroidal melanomas. Arch Ophthalmol. 1995;113:315-321.
21. Gragoudas ES, Seddon JM, Egan K, et al. Long-term results of proton beam irradiated uveal
melanomas. Ophthalmology. 1987;94:349-353.
22. De Potter P, Shields JA, Shields CL, Santos R. Modified enucleation via lateral orbitotomy for
choroidal melanoma with orbital extension: a report of two cases. Ophthal Plast Reconstr Surg.
1992;8:109-113.
23. Shields JA. Management of uveal melanoma. A continuing dilemma. Cancer. 1993;72:2067-2068.
24. McLean IW, Foster WD, Zimmerman LE, Gamel JW. Modifications of Callender’s classification of
uveal melanoma at the Armed Forces Institute of Pathology. Am J Ophthalmol. 1983;96:502-509.
25. Hendrix MJ, Seftor EA, Seftor RE, et al. Biologic determinants of uveal melanoma metastatic
phenotype: role of intermediate filaments as predictive markers. Lab Invest. 1998;78:153-163.
26. Callender GR. Malignant melanotic tumors of the eye: a study of histology in 111 cases. Trans Am
Acad Ophthalmol Otolaryngol. 1931;36:131-142.
27. Folberg R, Rummelt V, Parys-Van Ginderdeuren R, et al. The prognostic value of tumor blood vessel
morphology in primary uveal melanoma. Ophthalmology. 1993;100:1389-1398.
28. Maniotis AJ, Folberg R, Hess A, et al. Vascular channel formation by human melanoma cells in vivo
and in vitro: vasculogenic mimicry. Am J Pathol. 1999;155:739-752.
29. Coleman K, Baak JP, Van Diest P, Mullaney J, Farrell M, Fenton M. Prognostic factors following
enucleation of 111 uveal melanomas. Br J Ophthalmol. 1993;77:688-692.
30. Kilic E, van Gils W, Lodder E, et al. Clinical and cytogenetic analyses in uveal melanoma. Invest
Ophthalmol Vis Sci. 2006;47:3703-3707.
31. Maat W, Jordanova ES, Zelderen-Bhola SL, et al. The heterogeneous distribution of monosomy 3
in uveal melanomas: implications for prognostication based on fine-needle aspiration biopsies. Arch
Pathol Lab Med. 2007;131:91-96.
32. Sisley K, Rennie IG, Parsons MA, et al. Abnormalities of chromosomes 3 and 8 in posterior uveal
melanoma correlate with prognosis. Genes Chromosomes Cancer. 1997;19:22-28.
33. Sisley K, Parsons MA, Garnham J, et al. Association of specific chromosome alterations with tumour
phenotype in posterior uveal melanoma. Br J Cancer. 2000;82:330-338.
34. Prescher G, Bornfeld N, Becher R. Two subclones in a case of uveal melanoma. Relevance of
Introduction 23

monosomy 3 and multiplication of chromosome 8q. Cancer Genet Cytogenet. 1994;77:144-146.
35. White JS, Becker RL, McLean IW, Director-Myska AE, Nath J. Molecular cytogenetic evaluation of 10
uveal melanoma cell lines. Cancer Genet Cytogenet. 2006;168:11-21.
36. Speicher MR, Prescher G, du MS, et al. Chromosomal gains and losses in uveal melanomas detected by
comparative genomic hybridization. Cancer Res. 1994;54:3817-3823.
37. Ghazvini S, Char DH, Kroll S, Waldman FM, Pinkel D. Comparative genomic hybridization
analysis of archival formalin-fixed paraffin-embedded uveal melanomas. Cancer Genet Cytogenet.
1996;90:95-101.
38. Parrella P, Caballero OL, Sidransky D, Merbs SL. Detection of c-myc amplification in uveal melanoma
by fluorescent in situ hybridization. Invest Ophthalmol Vis Sci. 2001;42:1679-1684.
39. Hendrix MJ, Seftor EA, Seftor RE, et al. Regulation of uveal melanoma interconverted phenotype by
hepatocyte growth factor/scatter factor (HGF/SF). Am J Pathol. 1998;152:855-863.
40. Davies H, Bignell GR, Cox C, et al. Mutations of the BRAF gene in human cancer. Nature.
2002;417:949-954.
41. Cohen C, Zavala-Pompa A, Sequeira JH, et al. Mitogen-actived protein kinase activation is an early
event in melanoma progression. Clin Cancer Res. 2002;8:3728-3733.
42. Edmunds SC, Cree IA, Di Nicolantonio F, Hungerford JL, Hurren JS, Kelsell DP. Absence of
BRAF gene mutations in uveal melanomas in contrast to cutaneous melanomas. Br J Cancer.
2003;88:1403-1405.
43. Zuidervaart W, van Nieuwpoort F, Stark M, et al. Activation of the MAPK pathway is a common
event in uveal melanomas although it rarely occurs through mutation of BRAF or RAS. Br J Cancer.
2005;92:2032-2038.
44. Weber A, Hengge UR, Urbanik D, et al. Absence of mutations of the BRAF gene and constitutive
activation of extracellular-regulated kinase in malignant melanomas of the uvea. Lab Invest.
2003;83:1771-1776.
45. Maat W, van der Velden PA, Out-Luiting C, et al. Epigenetic inactivation of RASSF1a in uveal
melanoma. Invest Ophthalmol Vis Sci. 2007;48:486-490.
46. Harbour JW, Lai SL, Whang-Peng J, Gazdar AF, Minna JD, Kaye FJ. Abnormalities in structure and
expression of the human retinoblastoma gene in SCLC. Science. 1988;241:353-357.
47. Friend SH, Bernards R, Rogelj S, et al. A human DNA segment with properties of the gene that
predisposes to retinoblastoma and osteosarcoma. Nature. 1986;323:643-646.
48. Chana JS, Wilson GD, Cree IA, et al. c-myc, p53, and Bcl-2 expression and clinical outcome in uveal
melanoma. Br J Ophthalmol. 1999;83:110-114.
49. Kishore K, Ghazvini S, Char DH, Kroll S, Selle J. p53 gene and cell cycling in uveal melanoma. Am J
Ophthalmol. 1996;121:561-567.
50. Edmunds SC, Kelsell DP, Hungerford JL, Cree IA. Mutational analysis of selected genes in the
TGFbeta, Wnt, pRb, and p53 pathways in primary uveal melanoma. Invest Ophthalmol Vis Sci.
2002;43:2845-2851.
51. van der Velden PA, Metzelaar-Blok JA, Bergman W, et al. Promoter hypermethylation: a common
cause of reduced p16(INK4a) expression in uveal melanoma. Cancer Res. 2001;61:5303-5306.
24
Chap
ter 1

52. Brantley MA, Jr., Harbour JW. Deregulation of the Rb and p53 pathways in uveal melanoma. Am J
Pathol. 2000;157:1795-1801.
53. Coupland SE, Anastassiou G, Stang A, et al. The prognostic value of cyclin D1, p53, and MDM2
protein expression in uveal melanoma. J Pathol. 2000;191:120-126.
54. Missotten GS, Notting IC, Schlingemann RO, et al. Vascular endothelial growth factor a in eyes with
uveal melanoma. Arch Ophthalmol. 2006;124:1428-1434.
55. Folberg R, Hendrix MJ, Maniotis AJ. Vasculogenic mimicry and tumor angiogenesis. Am J Pathol.
2000;156:361-381.
56. Weinberg RA. Biology of Cancer; 2006: Chapter 13 and 14.
57. Nakajima M, Welch DR, Belloni PN, Nicolson GL. Degradation of basement membrane type IV
collagen and lung subendothelial matrix by rat mammary adenocarcinoma cell clones of differing
metastatic potentials. Cancer Res. 1987;47:4869-4876.
58. Fessler LI, Duncan KG, Fessler JH, Salo T, Tryggvason K. Characterization of the procollagen IV
cleavage products produced by a specific tumor collagenase. J Biol Chem. 1984;259:9783-9789.
59. Cottam DW, Rennie IG, Woods K, Parsons MA, Bunning RA, Rees RC. Gelatinolytic
metalloproteinase secretion patterns in ocular melanoma. Invest Ophthalmol Vis Sci.
1992;33:1923-1927.
60. El Shabrawi Y, Ardjomand N, Radner H, Ardjomand N. MMP-9 is predominantly expressed in
epithelioid and not spindle cell uveal melanoma. J Pathol. 2001;194:201-206.
61. Vaisanen A, Kallioinen M, von Dickhoff K, Laatikainen L, Hoyhtya M, Turpeenniemi-Hujanen T.
Matrix metalloproteinase-2 (MMP-2) immunoreactive protein--a new prognostic marker in uveal
melanoma? J Pathol. 1999;188:56-62.
62. Baker AH, Edwards DR, Murphy G. Metalloproteinase inhibitors: biological actions and therapeutic
opportunities. J Cell Sci. 2002;115:3719-3727.
63. Kim K, Daniels KJ, Hay ED. Tissue-specific expression of beta-catenin in normal mesenchyme and
uveal melanomas and its effect on invasiveness. Exp Cell Res. 1998;245:79-90.
64. Onken MD, Ehlers JP, Worley LA, Makita J, Yokota Y, Harbour JW. Functional gene expression
analysis uncovers phenotypic switch in aggressive uveal melanomas. Cancer Res. 2006;66:4602-4609.
65. Zeisberg M, Hanai J, Sugimoto H, et al. BMP-7 counteracts TGF-beta1-induced epithelial-to-
mesenchymal transition and reverses chronic renal injury. Nat Med. 2003;9:964-968.
66. Krasagakis K, Garbe C, Schrier PI, Orfanos CE. Paracrine and autocrine regulation of human
melanocyte and melanoma cell growth by transforming growth factor beta in vitro. Anticancer Res.
1994;14:2565-2571.
67. Krasagakis K, Garbe C, Zouboulis CC, Orfanos CE. Growth control of melanoma cells and
melanocytes by cytokines. Recent Results Cancer Res. 1995;139:169-182.
68. Rodeck U, Bossler A, Graeven U, et al. Transforming growth factor beta production and responsiveness
in normal human melanocytes and melanoma cells. Cancer Res. 1994;54:575-581.
69. Hu DN, McCormick SA, Ritch R, Pelton-Henrion K. Studies of human uveal melanocytes in vitro:
isolation, purification and cultivation of human uveal melanocytes. Invest Ophthalmol Vis Sci.
1993;34:2210-2219.
Introduction 25

70. Woodward JK, Rennie IG, Burn JL, Sisley K. A potential role for TGFbeta in the regulation of
uveal melanoma adhesive interactions with the hepatic endothelium. Invest Ophthalmol Vis Sci.
2005;46:3473-3477.
71. Myatt N, Aristodemou P, Neale MH, et al. Abnormalities of the transforming growth factor-beta
pathway in ocular melanoma. J Pathol. 2000;192:511-518.
72. Fontana A, Constam DB, Frei K, Malipiero U, Pfister HW. Modulation of the immune response by
transforming growth factor beta. Int Arch Allergy Immunol. 1992;99:1-7.
73. Granstein RD, Staszewski R, Knisely TL, et al. Aqueous humor contains transforming growth
factor-beta and a small (less than 3500 daltons) inhibitor of thymocyte proliferation. J Immunol.
1990;144:3021-3027.
74. Ma D, Niederkorn JY. Transforming growth factor-beta down-regulates major histocompatibility
complex class I antigen expression and increases the susceptibility of uveal melanoma cells to natural
killer cell-mediated cytolysis. Immunology. 1995;86:263-269.
75. Esser P, Grisanti S, Bartz-Schmidt K. TGF-beta in uveal melanoma. Microsc Res Tech.
2001;52:396-400.
76. Buijs JT, Rentsch CA, van der Horst G, et al. BMP-7, a putative regulator of epithelial homeostasis in
the human prostate, is a potent inhibitor of prostate cancer bone metastasis In Vivo. Am J Pathol. 2007.
77. Buijs JT, Henriquez NV, van Overveld PGM, et al. BMP7 inhibits tumor progressionin orthotopicand
bone metastatic breast cancer models. Cancer Research. 2007.
78. Kawabata M, Imamura T, Miyazono K. Signal transduction by bone morphogenetic proteins. Cytokine
Growth Factor Rev. 1998;9:49-61.
79. Gitelman SE, Kirk M, Ye JQ, Filvaroff EH, Kahn AJ, Derynck R. Vgr-1/BMP-6 induces osteoblastic
differentiation of pluripotential mesenchymal cells. Cell Growth Differ. 1995;6:827-836.
80. Pereira RC, Economides AN, Canalis E. Bone morphogenetic proteins induce gremlin, a protein that
limits their activity in osteoblasts. Endocrinology. 2000;141:4558-4563.
81. Dudley AT, Lyons KM, Robertson EJ. A requirement for bone morphogenetic protein-7 during
development of the mammalian kidney and eye. Genes Dev. 1995;9:2795-2807.
82. Jena N, Martin-Seisdedos C, McCue P, Croce CM. BMP7 null mutation in mice: developmental defects
in skeleton, kidney, and eye. Exp Cell Res. 1997;230:28-37.
83. Luo G, Hofmann C, Bronckers AL, Sohocki M, Bradley A, Karsenty G. BMP-7 is an inducer
of nephrogenesis, and is also required for eye development and skeletal patterning. Genes Dev.
1995;9:2808-2820.
84. Wang S, Chen Q, Simon TC, et al. Bone morphogenic protein-7 (BMP-7), a novel therapy for diabetic
nephropathy. Kidney Int. 2003;63:2037-2049.
85. Reddi AH. Initiation and promotion of endochrondral bone formation by bone morphogenetic proteins:
potential implications for avian tibial dyschondroplasia. Poult Sci. 2000;79:978-981.
86. Hruska KA, Guo G, Wozniak M, et al. Osteogenic protein-1 prevents renal fibrogenesis associated with
ureteral obstruction. Am J Physiol Renal Physiol. 2000;279:F130-F143.
87. Klahr S. The bone morphogenetic proteins (BMPs). Their role in renal fibrosis and renal function. J
Nephrol. 2003;16:179-185.
26
Chap
ter 1

88. Miyazono K, Kusanagi K, Inoue H. Divergence and convergence of TGF-beta/BMP signaling. J Cell
Physiol. 2001;187:265-276.
89. Morse JH, Deng Z, Knowles JA. Genetic aspects of pulmonary arterial hypertension. Ann Med.
2001;33:596-603.
90. Rubin LL, de Sauvage FJ. Targeting the Hedgehog pathway in cancer. Nat Rev Drug Discov.
2006;5:1026-1033.
91. Massague J, Blain SW, Lo RS. TGFbeta signaling in growth control, cancer, and heritable disorders.
Cell. 2000;103:295-309.
92. Canalis E, Economides AN, Gazzerro E. Bone morphogenetic proteins, their antagonists, and the
skeleton. Endocr Rev. 2003;24:218-235.
93. Varga AC, Wrana JL. The disparate role of BMP in stem cell biology. Oncogene. 2005;24:5713-5721.
94. Anderson DJ. Genes, lineages and the neural crest: a speculative review. Philos Trans R Soc Lond B
Biol Sci. 2000;355:953-964.
95. Shah NM, Groves AK, Anderson DJ. Alternative neural crest cell fates are instructively promoted by
TGFbeta superfamily members. Cell. 1996;85:331-343.
96. Ying QL, Nichols J, Chambers I, Smith A. BMP induction of Id proteins suppresses differentiation and
sustains embryonic stem cell self-renewal in collaboration with STAT3. Cell. 2003;115:281-292.
97. Gammill LS, Bronner-Fraser M. Genomic analysis of neural crest induction. Development.
2002;129:5731-5741.
98. Dorai H, Vukicevic S, Sampath TK. Bone morphogenetic protein-7 (osteogenic protein-1) inhibits
smooth muscle cell proliferation and stimulates the expression of markers that are characteristic of
SMC phenotype in vitro. J Cell Physiol. 2000;184:37-45.
99. Dudley AT, Godin RE, Robertson EJ. Interaction between FGF and BMP signaling pathways regulates
development of metanephric mesenchyme. Genes Dev. 1999;13:1601-1613.
100. Furuta Y, Piston DW, Hogan BL. Bone morphogenetic proteins (BMPs) as regulators of dorsal
forebrain development. Development. 1997;124:2203-2212.
101. You L, Kruse FE. Differential effect of activin A and BMP-7 on myofibroblast differentiation and the
role of the Smad signaling pathway. Invest Ophthalmol Vis Sci. 2002;43:72-81.
102. Abreu JG, Ketpura NI, Reversade B, De Robertis EM. Connective-tissue growth factor (CTGF)
modulates cell signalling by BMP and TGF-beta. Nat Cell Biol. 2002;4:599-604.
103. Ozaki T, Sakiyama S. Molecular cloning and characterization of a cDNA showing negative regulation
in v-src-transformed 3Y1 rat fibroblasts. Proc Natl Acad Sci U S A. 1993;90:2593-2597.
104. Nakamura Y, Ozaki T, Ichimiya S, Nakagawara A, Sakiyama S. Ectopic expression of DAN enhances
the retinoic acid-induced neuronal differentiation in human neuroblastoma cell lines. Biochem Biophys
Res Commun. 1998;243:722-726.
105. Gerlach-Bank LM, Ellis AD, Noonen B, Barald KF. Cloning and expression analysis of the chick DAN
gene, an antagonist of the BMP family of growth factors. Dev Dyn. 2002;224:109-115.
106. Gerlach-Bank LM, Cleveland AR, Barald KF. DAN directs endolymphatic sac and duct outgrowth in
the avian inner ear. Dev Dyn. 2004;229:219-230.
107. Hsu DR, Economides AN, Wang X, Eimon PM, Harland RM. The Xenopus dorsalizing factor Gremlin
Introduction 27

identifies a novel family of secreted proteins that antagonize BMP activities. Mol Cell. 1998;1:673-683.
108. Pearce JJ, Penny G, Rossant J. A mouse cerberus/Dan-related gene family. Dev Biol. 1999;209:98-110.
109. Stanley E, Biben C, Kotecha S, et al. DAN is a secreted glycoprotein related to Xenopus cerberus.
Mech Dev. 1998;77:173-184.
110. Ozaki T, Nakamura Y, Enomoto H, Hirose M, Sakiyama S. Overexpression of DAN gene product in
normal rat fibroblasts causes a retardation of the entry into the S phase. Cancer Res. 1995;55:895-900.
111. Dionne MS, Skarnes WC, Harland RM. Mutation and analysis of Dan, the founding member of the
Dan family of transforming growth factor beta antagonists. Mol Cell Biol. 2001;21:636-643.
112. Hemmati HD, Nakano I, Lazareff JA, et al. Cancerous stem cells can arise from pediatric brain tumors.
Proc Natl Acad Sci U S A. 2003;100:15178-15183.
113. Ingber DE. Extracellular matrix as a solid-state regulator in angiogenesis: identification of new targets
for anti-cancer therapy. Semin Cancer Biol. 1992;3:57-63.
114. Conway EM, Collen D, Carmeliet P. Molecular mechanisms of blood vessel growth. Cardiovasc Res.
2001;49:507-521.
115. Folkman J. Angiogenesis in cancer, vascular, rheumatoid and other disease. Nat Med. 1995;1:27-31.
116. Mandriota SJ, Seghezzi G, Vassalli JD, et al. Vascular endothelial growth factor increases urokinase
receptor expression in vascular endothelial cells. J Biol Chem. 1995;270:9709-9716.
117. Kroon ME, Koolwijk P, van Goor H, et al. Role and localization of urokinase receptor in the formation
of new microvascular structures in fibrin matrices. Am J Pathol. 1999;154:1731-1742.
118. Walker TM, Van Ginkel PR, Gee RL, et al. Expression of angiogenic factors Cyr61 and tissue factor in
uveal melanoma. Arch Ophthalmol. 2002;120:1719-1725.
119. Ordonez JL, Paraoan L, Hiscott P, et al. Differential expression of angioregulatory matricellular
proteins in posterior uveal melanoma. Melanoma Res. 2005;15:495-502.
120. Ziemssen F, Wegner R, Wegner J, et al. Analysis of neovasculature in uveal melanoma by targeting
the TGFbeta-binding receptor endoglin: is there prognostic relevance of proliferating endothelium?
Graefes Arch Clin Exp Ophthalmol. 2006;244:1124-1131.
121. Ryan TJ, Mortimer PS, Jones RL. Lymphatics of the skin. Neglected but important. Int J Dermatol.
1986;25:411-419.
122. Jussila L, Alitalo K. Vascular growth factors and lymphangiogenesis. Physiol Rev. 2002;82:673-700.
123. Karpanen T, Alitalo K. Lymphatic vessels as targets of tumor therapy? J Exp Med. 2001;194:F37-F42.
124. Pepper MS. Lymphangiogenesis and tumor metastasis: myth or reality? Clin Cancer Res.
2001;7:462-468.
125. Clarijs R, Schalkwijk L, Ruiter DJ, de Waal RM. Lack of lymphangiogenesis despite coexpression of
VEGF-C and its receptor Flt-4 in uveal melanoma. Invest Ophthalmol Vis Sci. 2001;42:1422-1428.
126. Clarijs R, Otte-Holler I, Ruiter DJ, de Waal RM. Presence of a fluid-conducting meshwork
in xenografted cutaneous and primary human uveal melanoma. Invest Ophthalmol Vis Sci.
2002;43:912-918.
127. Smetsers TF, van de Westerlo EM, ten Dam GB, et al. Localization and characterization of melanoma-
associated glycosaminoglycans: differential expression of chondroitin and heparan sulfate epitopes in
melanoma. Cancer Res. 2003;63:2965-2970.
28
Chap
ter 1

128. Chen X, Maniotis AJ, Majumdar D, Pe’er J, Folberg R. Uveal melanoma cell staining for CD34 and
assessment of tumor vascularity. Invest Ophthalmol Vis Sci. 2002;43:2533-2539.
129. Folberg R, Chen X, Boldt HC, et al. Microcirculation patterns other than loops and networks in
choroidal and ciliary body melanomas. Ophthalmology. 2001;108:996-1001.
130. Maniotis AJ, Chen X, Garcia C, et al. Control of melanoma morphogenesis, endothelial survival, and
perfusion by extracellular matrix. Lab Invest. 2002;82:1031-1043.
131. Ferrara N, Henzel WJ. Pituitary follicular cells secrete a novel heparin-binding growth factor specific
for vascular endothelial cells. Biochem Biophys Res Commun. 1989;161:851-858.
132. Yancopoulos GD, Davis S, Gale NW, Rudge JS, Wiegand SJ, Holash J. Vascular-specific growth
factors and blood vessel formation. Nature. 2000;407:242-248.
133. Neufeld G, Tessler S, Gitay-Goren H, Cohen T, Levi BZ. Vascular endothelial growth factor and its
receptors. Prog Growth Factor Res. 1994;5:89-97.
134. Senger DR, Van de WL, Brown LF, et al. Vascular permeability factor (VPF, VEGF) in tumor biology.
Cancer Metastasis Rev. 1993;12:303-324.
135. Houck KA, Ferrara N, Winer J, Cachianes G, Li B, Leung DW. The vascular endothelial growth factor
family: identification of a fourth molecular species and characterization of alternative splicing of RNA.
Mol Endocrinol. 1991;5:1806-1814.
136. Grugel S, Finkenzeller G, Weindel K, Barleon B, Marme D. Both v-Ha-Ras and v-Raf
stimulate expression of the vascular endothelial growth factor in NIH 3T3 cells. J Biol Chem.
1995;270:25915-25919.
137. Shweiki D, Itin A, Soffer D, Keshet E. Vascular endothelial growth factor induced by hypoxia may
mediate hypoxia-initiated angiogenesis. Nature. 1992;359:843-845.
138. Missotten GS, Notting IC, Schlingemann RO, et al. Vascular endothelial growth factor a in eyes with
uveal melanoma. Arch Ophthalmol. 2006;124:1428-1434.
139. Boyd SR, Tan D, Bunce C, et al. Vascular endothelial growth factor is elevated in ocular fluids of
eyes harbouring uveal melanoma: identification of a potential therapeutic window. Br J Ophthalmol.
2002;86:448-452.
140. Boyd SR, Tan DS, de Souza L, et al. Uveal melanomas express vascular endothelial growth factor and
basic fibroblast growth factor and support endothelial cell growth. Br J Ophthalmol. 2002;86:440-447.
141. Sheidow TG, Hooper PL, Crukley C, Young J, Heathcote JG. Expression of vascular endothelial
growth factor in uveal melanoma and its correlation with metastasis. Br J Ophthalmol.
2000;84:750-756.
142. Grimmond S, Lagercrantz J, Drinkwater C, et al. Cloning and characterization of a novel human gene
related to vascular endothelial growth factor. Genome Res. 1996;6:124-131.
143. Olofsson B, Jeltsch M, Eriksson U, Alitalo K. Current biology of VEGF-B and VEGF-C. Curr Opin
Biotechnol. 1999;10:528-535.
144. Aase K, Lymboussaki A, Kaipainen A, Olofsson B, Alitalo K, Eriksson U. Localization of VEGF-B
in the mouse embryo suggests a paracrine role of the growth factor in the developing vasculature. Dev
Dyn. 1999;215:12-25.
145. van der Pluijm G, Sijmons B, Vloedgraven H et al. Monitoring metastatic behavior of human
Introduction 29

tumor cells in mice with species-specific polymerase chain reaction: elevated expression of
angiogenesis and bone resorption stimulators by breast cancer in bone metastases. J Bone Miner Res.
2001;16:1077-1091.
146. Salven P, Lymboussaki A, Heikkila P, et al. Vascular endothelial growth factors VEGF-B and VEGF-C
are expressed in human tumors. Am J Pathol. 1998;153:103-108.
147. Enholm B, Paavonen K, Ristimaki A, et al. Comparison of VEGF, VEGF-B, VEGF-C and Ang-1
mRNA regulation by serum, growth factors, oncoproteins and hypoxia. Oncogene. 1997;14:2475-2483.
148. Ristimaki A, Narko K, Enholm B, Joukov V, Alitalo K. Proinflammatory cytokines regulate
expression of the lymphatic endothelial mitogen vascular endothelial growth factor-C. J Biol Chem.
1998;273:8413-8418.
149. Joukov V, Pajusola K, Kaipainen A, et al. A novel vascular endothelial growth factor, VEGF-C,
is a ligand for the Flt4 (VEGFR-3) and KDR (VEGFR-2) receptor tyrosine kinases. EMBO J.
1996;15:1751.
150. Pepper MS, Mandriota SJ, Jeltsch M, Kumar V, Alitalo K. Vascular endothelial growth factor
(VEGF)-C synergizes with basic fibroblast growth factor and VEGF in the induction of angiogenesis in
vitro and alters endothelial cell extracellular proteolytic activity. J Cell Physiol. 1998;177:439-452.
151. Seftor EA, Meltzer PS, Schatteman GC, et al. Expression of multiple molecular phenotypes
by aggressive melanoma tumor cells: role in vasculogenic mimicry. Crit Rev Oncol Hematol.
2002;44:17-27.
152. Marconcini L, Marchio S, Morbidelli L, et al. c-fos-induced growth factor/vascular endothelial growth
factor D induces angiogenesis in vivo and in vitro. Proc Natl Acad Sci U S A. 1999;96:9671-9676.
153. Stacker SA, Caesar C, Baldwin ME, et al. VEGF-D promotes the metastatic spread of tumor cells via
the lymphatics. Nat Med. 2001;7:186-191.
154. Dithmar S, Rusciano D, Grossniklaus HE. A new technique for implantation of tissue culture melanoma
cells in a murine model of metastatic ocular melanoma. Melanoma Res. 2000;10:2-8.
155. Dubielzig RR. Ocular neoplasia in small animals. Vet Clin North Am Small Anim Pract.
1990;20:837-848.
156. Saunders LZ, Barron CN. Primary pigmented intraocular tumors in animals. Cancer Res.
1958;18:234-245.
157. Acland GM, McLean IW, Aguirre GD, Trucksa R. Diffuse iris melanoma in cats. J Am Vet Med Assoc.
1980;176:52-56.
158. Petit G. La mêcanisme de la pigmentation dans le sarcome mêlanique. Rec mêd vêt. 1919:121-125.
159. Benson WR. Intraocular tumor after ethionine and N-2-fluorenylacetamide. Arch Pathol.
1962;73:404-406.
160. Patz A, Wulff LB, Rogers SW. Experimental production of ocular tumors. Am J Ophthalmol.
1959;48:98-117.
161. Taylor GN, Lloyd RD, Miller SC, Muggenburg BA. Radium-induced eye melanomas in dogs. Health
Phys. 2000;79:196-198.
162. Folberg R, Barron BC, Reeves R.D. Primary melanocytic lesions of the rabbit choroid following
topical application of 7,12-dimethylbenz[a]-anthracene: preliminary observations. J Toxicol Cutan Ocul
30
Chap
ter 1

Toxicol. 1990;9:313-334.
163. McCullough B, Schaller J, Shadduck JA, Yohn DS. Induction of malignant melanomas associated with
fibrosarcomas in gnotobiotic cats inoculated with Gardner-feline fibrosarcoma virus. J Natl Cancer
Inst. 1972;48:1893-1895.
164. Albert DM, Shadduck JA, Craft JL, Niederkorn JY. Feline uveal melanoma model induced with feline
sarcoma virus. Invest Ophthalmol Vis Sci. 1981;20:606-624.
165. Niederkorn JY, Shadduck JA, Albert D. Enucleation and the appearance of second primary tumors in
cats bearing virally induced intraocular tumors. Invest Ophthalmol Vis Sci. 1982;23:719-725.
166. Greene HS. The heterologous transplantation of human melanomas. Yale J Biol Med. 1950;22:611-620.
167. Greene HS. A spontaneous melanoma in the hamster with a propensity for amelanotic alteration and
sarcomatous transformation during transplantation. Cancer Res. 1958;18:422-425.
168. Greene HSN. Heterologous transplantation of mammalian tumors. II. The transfer of human tumors to
alien species. J Exp Med. 1941:475-489.
169. Kramer TR, Powell MB, Wilson MM, Salvatore J, Grossniklaus HE. Pigmented uveal tumours in a
transgenic mouse model. Br J Ophthalmol. 1998;82:953-960.
170. Tanaka S, Yamamoto H, Takeuchi S, Takeuchi T. Melanization in albino mice transformed by
introducing cloned mouse tyrosinase gene. Development. 1990;108:223-227.
171. Rygaard J, Povlsen CO. Heterotransplantation of a human malignant tumour to “Nude” mice. Acta
Pathol Microbiol Scand. 1969;77:758-760.
172. Giovanella BC, Yim SO, Stehlin JS, Williams LJ, Jr. Development of invasive tumors in the “nude”
mouse after injection of cultured human melanoma cells. J Natl Cancer Inst. 1972;48:1531-1533.
173. Grossniklaus HE, Wilson MW, Barron BC, Lynn MJ. Anterior vs posterior intraocular melanoma.
Metastatic differences in a murine model. Arch Ophthalmol. 1996;114:1116-1120.
174. Morilla-Grasa A. Animal models in uveal melanoma: establishment and research. Can J Ophthalmol.
2004;39:433-440.
175. Clark AF, Mellon J, Li XY, et al. Inhibition of intraocular tumor growth by topical application of the
angiostatic steroid anecortave acetate. Invest Ophthalmol Vis Sci. 1999;40:2158-2162.
176. Dithmar S, Rusciano D, Lynn MJ, Lawson DH, Armstrong CA, Grossniklaus HE. Neoadjuvant
interferon alfa-2b treatment in a murine model for metastatic ocular melanoma: a preliminary study.
Arch Ophthalmol. 2000;118:1085-1089.
177. Ma D, Gerard RD, Li XY, Alizadeh H, Niederkorn JY. Inhibition of metastasis of intraocular
melanomas by adenovirus-mediated gene transfer of plasminogen activator inhibitor type 1 (PAI-1) in
an athymic mouse model. Blood. 1997;90:2738-2746.
Introduction 31

32
Chap
ter 1