Embed Size (px)
Citation preview
Lorelei Goodyear, MPH
PATH
Rob Quick, MD MPH
Centers for Disease Control and Prevention
Integration Achieves Results
Malawi ANC/Hygiene Kit Model
What do we know about adoption and sustained use of HWTS?
• Commercial success = 5-10% penetration
• Social marketing increases knowledge of need to treat, brand awareness, and product trial
• Safe Water System (chlorine + safe storage container) has global reach
• Challenging to exceed 10-15% adoption
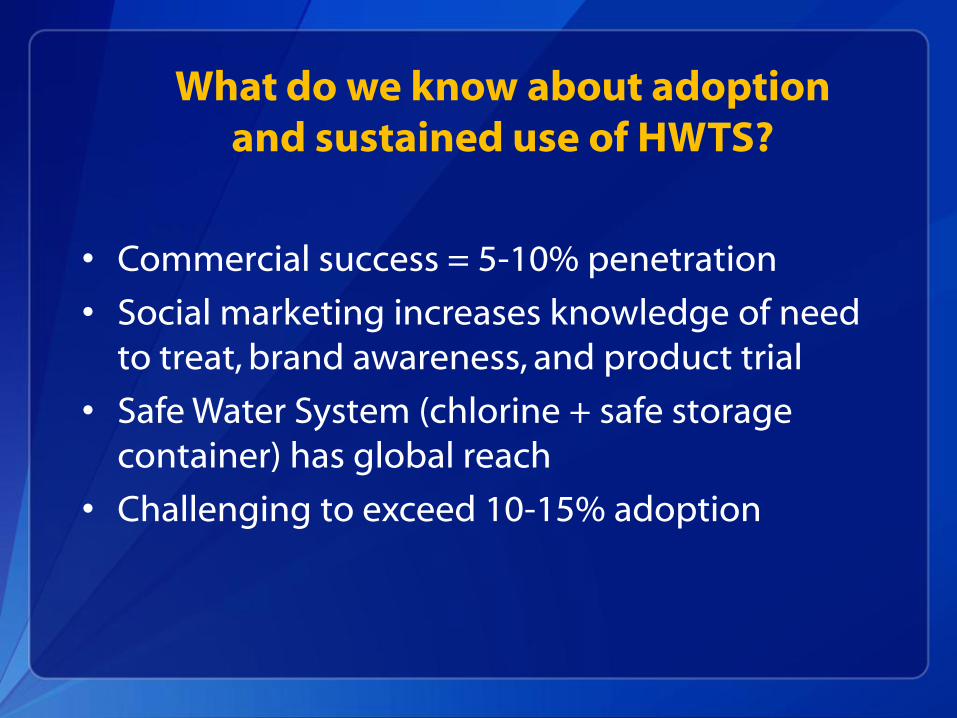
Product Need Value/relevance
Awareness Action Maintenance
Trial/initial use Current Use
Purchase Sustained Use
Behavior Change Continuum

Blantyre and Salima Program
• Training of clinic staff
• 15,000 water hygiene kits
• 3 free refills of WaterGuard and soap at ANC, delivery, and postnatal visits as incentive for clinic attendance
• Health Surveillance Assistant home visits, education and monitoring
• PSI advertising and product distribution
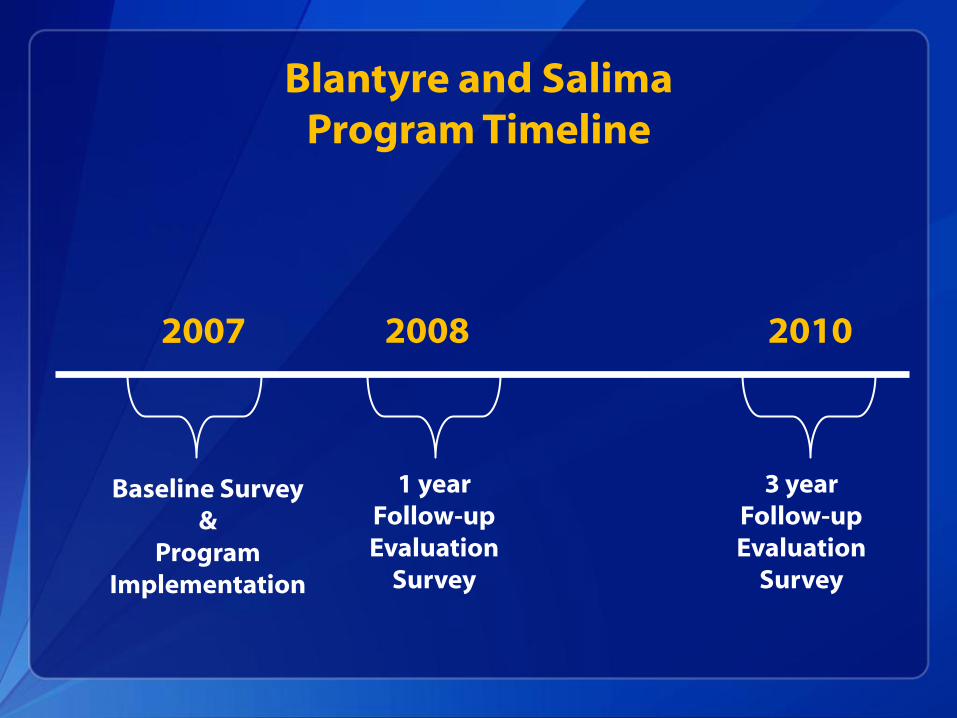
Blantyre and Salima Program Timeline
Baseline Survey &
Program Implementation
2007 2008 2010
1 year Follow-up Evaluation
Survey
3 year Follow-up Evaluation
Survey
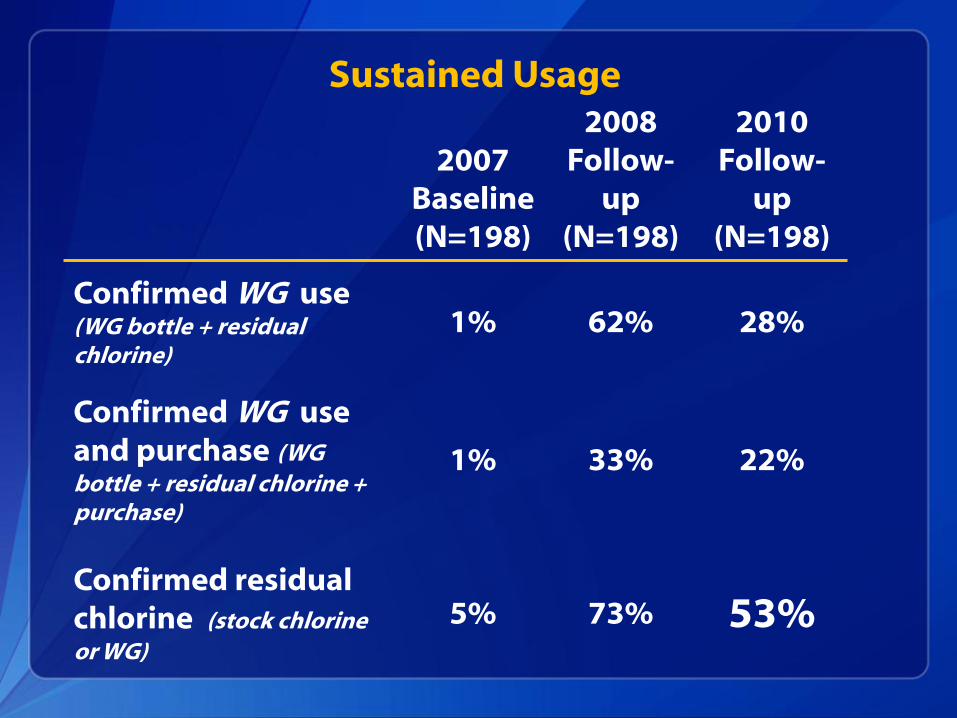
Sustained Usage
2007 Baseline (N=198)
2008 Follow-
up (N=198)
2010 Follow-
up (N=198)
Confirmed WG use (WG bottle + residual chlorine)
1% 62% 28%
Confirmed WG use and purchase (WG bottle + residual chlorine + purchase)
1% 33% 22%
Confirmed residual chlorine (stock chlorine or WG)
5% 73% 53%

Effective Incentive
Water Hygiene Kit

Trusted Sources
Health Surveillance Assistants
ANC Nurses
“Teachable Moment”
Can results be replicated?

Machinga Implementation-2009-2011
25,000 Water and Hygiene Kits distributed in 15 health facilities throughout Machinga District
Up to 4 free refills of WaterGuard and soap provided at ANC and postnatal visits to promote clinic attendance
Home visits by Health Surveillance Assistant (HSA) assured ongoing education and monitoring
Required presence of husband or partner of pregnant woman at ANC visit to receive Water Hygiene Kit to increase their participation

WaterGuard Results
Baseline (n=106)
Follow-up (n=97)
Confirmed WG use (WG bottle + positive chlorine test) *
0% 69%
Confirmed WG use AND purchase of WG *
0% 36%
* p < 0.0001

ANC Services and Outcome of Pregnancy
Malawi DHS( 2010)
Participants (n=97)
4 or more antenatal visits 21% 56%
Delivery at health facility 72% 90%
Baby returned for 6 week infant check-up
--- 90%

Partner Involvement HIV Testing and Prevention Services
Participants (n=97)
Partner came to ANC visit 100%
Partner VCT 99%
Participant VCT 99%
Couple disclosure of HIV status 98%
HIV-exposed infants on ARV prophylaxis
90%

2 Pilot Cost Comparison
Original ANC program
(Blantyre & Salima)
9 months
Relative per
person cost
% of Cost
CHAI program
(Machinga) Year 2
Relative per
person cost
% of Cost
Hygiene kit costs $70,407 4.69 55% $113,031 4.52 67%
Program management $21,481 1.43 17% $17,404 0.69 7%
MOH management
and supervision
$10,416 0.69 8% $32,425 1.30 19%
Promotion and
Advertising
$19,678 1.31 15% $5,517 0.22 3%
Training Costs $6,793 0.45 5% $1,371 0.06 1%
TOTAL $128,775 $169,748
Number of participants 15,000 25,000
Per participant costs $8.58 $6.79
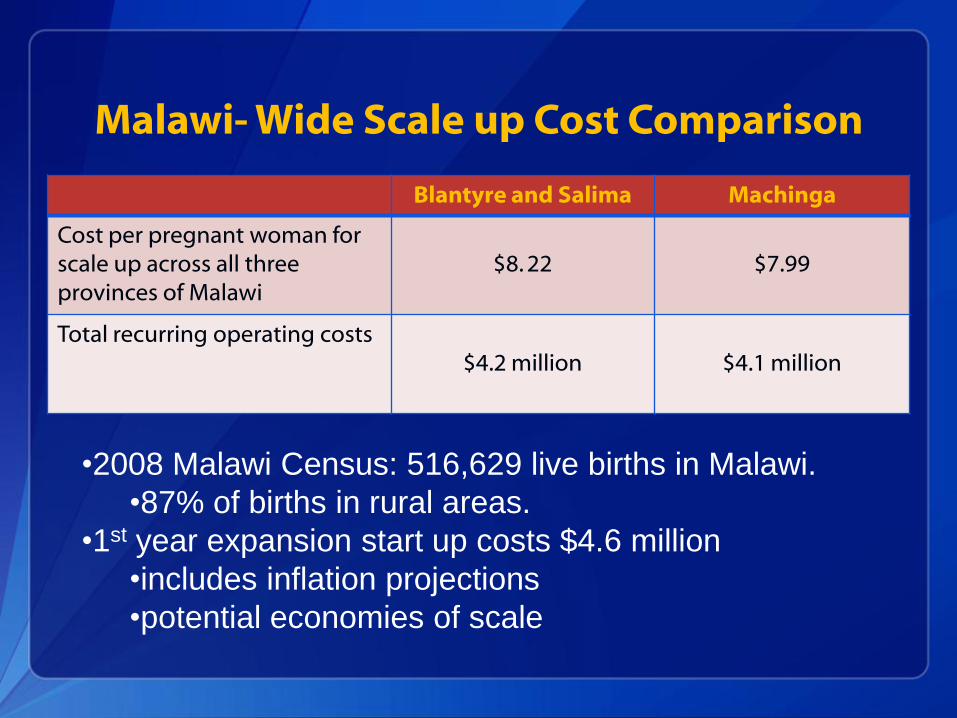
Malawi- Wide Scale up Cost Comparison
Blantyre and Salima Machinga
Cost per pregnant woman for scale up across all three provinces of Malawi
$8. 22
$7.99
Total recurring operating costs $4.2 million
$4.1 million
•2008 Malawi Census: 516,629 live births in Malawi.
•87% of births in rural areas.
•1st year expansion start up costs $4.6 million
•includes inflation projections
•potential economies of scale

Evaluation Limitations
Women in survey population may have received more HSA visits than other program participants
Some survey participants were lost to follow-up (<20%)
Behavior change may have been influenced by additional unrelated events or other programs

Conclusions
Prenatal care is an effective platform for promoting HWTS and HIV prevention in Malawi
Conclusions
Social marketing is complemented by sustained interpersonal communication between new mothers and trusted providers at teachable moments
Integration efficiently enhances outcomes and achieves lasting results.

Future Directions for ANC/Hygiene Kit Model
• Scale up in Malawi
• Evaluation of consistent use and health outcomes
• Replicate in other countries
• Potential adaptations
– Offer HWTS product choice
– Emphasize immunization, nutrition, and post-partum family planning
• Build stronger health/WASH alliances

Partner Acknowledgments
Implementation Partners Ministry of Health Malawi Population Services International (PSI) Clinton Health Access Initiative (CHAI) UNICEF Evaluation Partners: Centers for Disease Control and Prevention (CDC) PATH Abt Associates Donors: USAID Bill and Melinda Gates Foundation

Observed WG bottle in home Positive test for chlorine in stored water
+
Confirmed WaterGuard Use
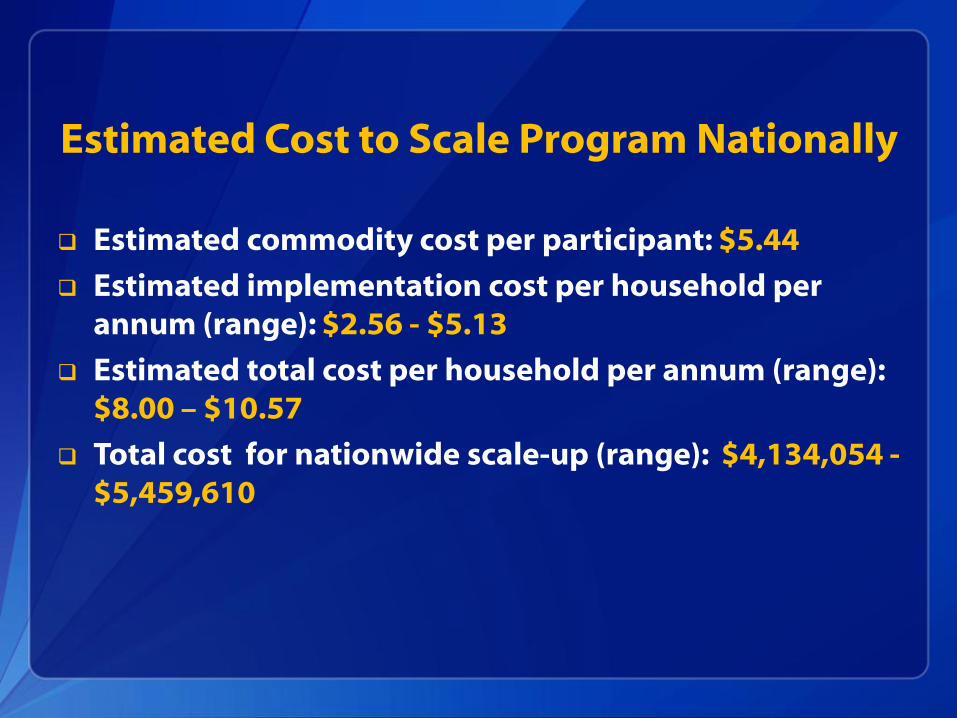
Estimated Cost to Scale Program Nationally
Estimated commodity cost per participant: $5.44
Estimated implementation cost per household per annum (range): $2.56 - $5.13
Estimated total cost per household per annum (range): $8.00 – $10.57
Total cost for nationwide scale-up (range): $4,134,054 - $5,459,610

Observed WG bottle in home
Positive test for chlorine in stored
water
+ +
Reports WG purchase after
free bottles
Confirmed WG Use and Purchase
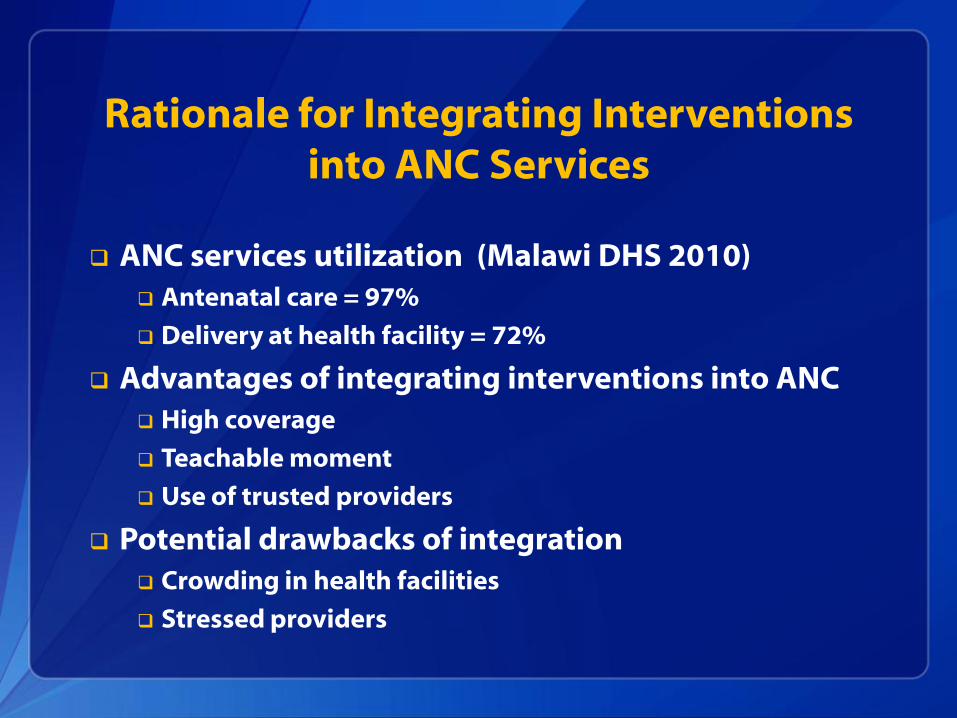
ANC services utilization (Malawi DHS 2010) Antenatal care = 97%
Delivery at health facility = 72%
Advantages of integrating interventions into ANC High coverage
Teachable moment
Use of trusted providers
Potential drawbacks of integration Crowding in health facilities
Stressed providers
Rationale for Integrating Interventions
into ANC Services