Embed Size (px)
Citation preview

British HeartJournal, I974, 36, 732-736.
Echocardiographic findings in persistent truncusarteriosus in a young adult
Premindra A. N. Chandraratna, Udayan Bhaduri, Benjamin B. Littman, and Frank J. HildnerWith the technical assistance of Dale GindlespergerFrom the Division of Cardiology, Department of Medicine, Mount Sinai Medical Center, Miami Beach,Florida, U.S.A.
The clinical, haemodynamic, and echocardiographic features of persistent truncus arteriosus in a young adultare presented. Several echocardiographic abnormalities were observed, namely (I) diastolic fluttering of theanterior mitral leaflet, (2) dilatation of the 'aortic' root, (3) four 'aortic' valve cusp echoes, (4) separationof the 'aortic' cusps during diastole, (5) dilatation of the right ventricle with paradoxical motion of the septum,(6) the anterior wall of the 'aorta' was anterior to the septum and the posterior 'aortic' wall posterior to theclosed position of the mitral valve.
The significance of these findings is discussed.
Since the introduction of echocardiography in I954by Edler and Hertz (I954), several workers haveconfirmed its usefulness in the evaluation of patientswith valvular heart disease (Joyner and Reid, I963;Joyner et al., I967; Gramiak and Shah, I970). Morerecently this technique has been found to be a valu-able aid in the diagnosis of congenital heart disease.Characteristic findings have been described in atrialseptal defect (Diamond et al., I97I), Ebstein's ano-maly (Lundstrom, I973), double outlet right ventri-cle (Chesler et al., I97I), transposition of the greatarteries (Gramiak et al., I973), and tetralogy ofFallot (Chung et al., 1973).
Patients with truncus arteriosus usually presentwith cardiac failure and cyanosis during the neo-natal period. Survival to adult life is rare (Tandon,Hauck, and Nadas, I963). In this report we describethe haemodynamic and echocardiographic featuresof truncus arteriosus with associated ventricularseptal defect, atrial septal defect, and incompetenceof the truncal valve, in a 2i-year-old woman.
Case reportA 2i-year-old white woman was admitted to MountSinai Hospital in March I973. She was noted to becyanotic at birth, and she had had fatigue and dyspnoeasince childhood. She had been subject to frequent respir-atory infections in the past. There was no history ofsquatting, syncope, chest pain, or palpitations. Twoyears before admission she was seen at another hospitalwith mild cardiac failure and was started on digitalis
and diuretic therapy. Several phlebotomies were per-formed in order to correct her polycythaemia. Her symp-toms gradually increased, and at the time of admissionshe had dyspnoea on walking a short distance on thelevel. There was no family history of congenital heartdisease.On examination she was a thin, underdeveloped
woman, I45 cm in height and 35 kg in weight. Therewas pronounced cyanosis and clubbing of her fingersand toes. The peripheral pulses were normal and peri-pheral oedema was not present. Her blood pressure wasI I0/70 mmHg, and she was in normal sinus rhythm witha heart rate of 8o a minute. The venous pressure wasnot raised, and the apex beat was in the sixth interspace,i cm outside the midclavicular line. A systolic thrill anda right ventricular lift were present at the left sternalborder. A loud ejection click and grade 4/6 ejection sys-tolic murmur were heard at the base. A grade 4/6 holo-diastolic blowing murmur was present at the left sternaledge. The second sound was closely split; this findingwas confirmed by phonocardiography. Her lungs wereclear. The abdomen and central nervous system wereclinically normal.The electrocardiogram showed sinus rhythm, right
axis deviation (axis plus i200), and biventricular hyper-trophy. The chest x-ray showed a boot-shaped heart,with dilatation of the ascending 'aorta' and absence ofthe main pulmonary artery segment. The pulmonaryvascular markings were slightly increased, and there wasno valvular calcification on fluoroscopy.
Echocardiography was performed with the patientsupine, and the transducer was placed in the third inter-costal space, i cm from the left sternal edge. Fine dia-stolic fluttering of the anterior mitral leaflet was seen
on July 15, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.36.7.732 on 1 July 1974. D
ownloaded from

Echocardiographic findings in persistent truncus arteriosus in a young adult 733
a
A
1_*~~~~~~~iI.ILECG
Phoco
KG
AW "Ao"
"AV
PW ttAo"
b
B
wr- w = s- - a-
--
z st .s sweN ^- oot ./Xt-4.R m: 7msS
-* >w t S S t.-z+¢st r.tt w t- *
:. eNsf + i: t E. w *9 s s
s---- lll - W -|l
c
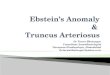
FIG. i Echocardiograms of the valves. a) Echocardiogram of the anterior mitral leafletshowing diastolic fluttering of the valve. The right panel is a blow-up which demonstrates thefluttering more clearly. b) Echocardiogram of the 'aortic root' (truncus). The 'aortic (truncal)valve' ('A V') is seen. Phono = Phonocardiogram, AW 'Ao'= anterior wall of 'aorta', PW'Ao'=posterior wall of 'aorta'. c) Echocardiogram of the 'aortic' (truncal) valve. Four cuspechoes are seen (AI, A2, A3, A4). There is abnormal separation of the cusps in diastole (Panel B).
AO
on July 15, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.36.7.732 on 1 July 1974. D
ownloaded from

734 Chandraratna, Bhaduri, Littman, and Hildner
ECG
cw
RVWW
'vsmSMVPLV_
-4-
b
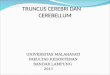
FIG. 2 Echocardiograms of the ventricular septum. a) The right and left ventricles are shown.Paradoxical motion of the septum (IVS) is evident. CW=chest wall; RVW= anterior wall ofright ventricle; MV=anterior mitral leaflet; PLV=posterior wall of left ventricle. b) Therelation between the 'aortic' root (truncus), the interventricular septum (IVS), and the mitralvalve (MV). AW 'Ao' = anterior wall of 'aorta'; PW 'Ao' =posterior wall of 'aorta';AV= 'Aortic' valve.
pp,
II
:I
L-2
on July 15, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.36.7.732 on 1 July 1974. D
ownloaded from

Echocardiographic findings in persistent truncus arteriosus in a young adult 735
Fig. ia). The 'aortic root' (truncus) was grossly dilatedand it was 4-6 cm (3 9 cm/M2) in diameter (Fig. ib).(Upper limit of normal is 3-7 cm or 2-2 cm/M2) (Feigen-baum, I972). Four aortic valve (truncal valve) cuspechoes were seen during systole (Fig. Ic). There wasincomplete apposition or separation of the valve cuspsduring diastole (Fig. Ic). The maximal separation ofthe valve cusps during systole was 2-5 cm (normal i-6-2-6 cm) (Feigenbaum, 1972). The right ventricle (Fig. 2a)was dilated and measured 3-3 cm or 2-7 cm/M2 (upperlimit of normal 2-3 cm or I-2 cm/M2) (Feigenbaum,I972). The interventricular septum showed paradoxicalmotion (anterior motion during systole).
Fig. 2b shows the relation between the 'aortic root'and the interventricular septum. This was achieved byangling the transducer from an initial medial and super-ior position to a lateral and inferior position. In thenormal heart the anterior wall of the aorta is continuouswith the septum, and the posterior wall is continuouswith the closed position of the mitral valve. In ourpatient the anterior wall of the 'aorta' is anterior to theseptum. Thus, the 'aorta' overrides the septum. Theposterior wall of the 'aorta' is posterior to the closedposition of the mitral valve. However, there appears tobe continuity between the aortic valve (in the openposition) and the mitral valve (in the closed position).Tricuspid valve movement did not show any obviousabnormality.
Right and left heart catheterization, 9 days after shewas admitted, showed a right atrial mean pressure of4mmHg and a right ventricular pressure of I32/8 mmHg.The pressure in the 'aorta' was I32/87 mmHg with amean of II mmHg, and the left ventricular pressurewas I32/Il mmHg. The pulmonary artery was notentered. During right heart catheterization the leftatrium was entered via an atrial septal defect. The mixedvenous oxygen saturation was 59 per cent and there wasno oxygen step-up in the right ventricle. The oxygensaturation in the pulmonary vein was 97 per cent, leftatrium go per cent, left ventricle 7 I per cent, and femoralartery 67 per cent.A right ventricular angiogram showed filling of the
' aorta' and the left ventricle, but the pulmonary arterieswere not visualized. 'Aortic root' injection showed pro-nounced dilatation of the 'ascending aorta', moderate' aortic' regurgitation, and three 'aortic valve' cuspswere identified. The main pulmonary artery arose fromthe posterior aspect of the ascending 'aorta'. The angio-graphic findings were suggestive of Type II truncusarteriosus (Tandon et al., I963; Collett and Edwards,I949; Van Praagh and Van Praagh, I965).
Discussion
The physical signs, chest x-ray, and angiograms inour patient are typical of truncus arteriosus. Aventricular septal defect is invariably associated withthis anomaly (Van Praagh and Van Praagh, I965)and incompetence of the truncal valve is not un-common (Tandon et al., I963).
Several echocardiographic abnormalities were
noted. Diastolic fluttering of the mitral valve wasprobably due to truncal valve incompetence. Thisfinding helped to identify the holodiastolic murmuras being of 'aortic' origin as opposed to being due toa pulmonary incompetence which may be associatedwith an Eisenmenger ventricular or atrial septal de-fect. The 'aortic root' was very dilated. Though dila-tation of the ascending aorta occurs in tetralogy ofFallot, this degree of enlargement is probably more infavour oftruncus arteriosus. Another unusual featurewas the recording of four echoes from the aorticvalve cusps. There are several possible explanationsfor this. Multiple echoes from the valve cusps havebeen described in calcific aortic stenosis (Gramiakand Shah, I970). Against this are the absence of'aortic' calcification on fluoroscopy, the absence ofan ' aortic' valve gradient, and the systolic separationof the valve cusps of 2-5 cm, which is in the uppernormal range, whereas in a calcified aortic valve themobility of the cusps is diminished, and, therefore,the systolic separation is less than normal. Twoanatomical features of the semilunar valve in truncusarteriosus deserve comment. Calder and associates(I97I) observed that the truncal valve faces anteri-orly and leftward as opposed to the orientation ofthe normal aortic valve. Van Praagh and Van Praagh(I965) described thick, fleshy polypoid truncal leaf-lets as being a frequent occurrence. These abnor-malities may help to explain multiple 'aortic' valveechoes. The four cusp echoes may also be explainedon the basis of four truncal leaflets. The angiogram,however, showed only three leaflets, though thisdoes not completely exclude the presence of a fourthcusp. Splitting of the second sound which was ob-served in our patient raises the possibility of thepresence of more than three cusps, as suggested byTandon and associates (I963). The lack of apposi-tion of the 'aortic' valve cusps during diastole mayexplain the 'aortic' incompetence that was seen inour patient. Feigenbaum (I972) made a similar ob-servation in a patient with truncus arteriosus.The dilatation of the right ventricle and para-
doxical movement of the septum suggest volumeoverloading of the right ventricle. The absence ofan oxygen step-up in the right heart precludes asignificant left-to-right shunt at atrial or ventricularlevel at the present time. Truncal valve incompetenceis another cause of right ventricular volume over-load in our patient. Selective streaming of blood isa possible explanation for the absence of an oxygenstep-up in the right ventricle, in the presence oftruncal valve incompetence. The much increasedright ventricular pressure probably contributed tothe dilatation of the right ventricle but paradoxicalseptal motion is not a feature of right ventricularpressure overload (Feigenbaum, 1972).
on July 15, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.36.7.732 on 1 July 1974. D
ownloaded from

736 Chandraratna, Bhaduri, Littman, and Hildner
The anterior wall of the 'aorta' was anterior tothe septum, indicating that there was overriding ofthe aorta. This also occurs in tetralogy of Fallot.Chung and associates (I973) observed that in patientswith tetralogy the posterior wall of the aorta waseither continuous with or anterior to the closedposition of the mitral valve; whereas in our patientthe posterior 'aortic' wall was posterior to the mitralvalve. In double outlet right ventricle, on the otherhand, there is discontinuity between the closedposition of the mitral valve and the posterior wallof the aorta, but the septum is continuous with theanterior aortic wall (Chesler et al., 197I).
In summary, several echocardiographic abnor-malities were noted in a 2i-year-old woman withpersistent truncus arteriosus. Though some of theseobservations are not specific for this defect, thecombination of findings may provide useful cluesto the diagnosis of this anomaly.
ReferencesCalder, A. L., Van Praagh, R., Van Praagh, S., and Sears,
W. P. (I97I). Diagnosis of truncus arteriosus (abstract).Circulation, 44, Suppl. II, 148.
Chesler, E., Joffe, H. S., Beck, W., and Schrire, V. (I97I).Echocardiographic recognition of mitral-semilunar valvediscontinuity. Circulation, 43, 725.
Chung, K. J., Nanda, N. C., Manning, J. A., and Gramiak, R.(1973). Echocardiographic findingslin tetralogy of Fallot(abstract). American Journal of Cardiology, 31, I26.
Collett, R. W., and Edwards, J. E. (1949). Persistent truncusarteriosus: a classification according to anatomic types.Surgical Clinics of North America, 29, I245.
Diamond, M. A., Dillon, J. C., Haine, C. L., Chang, S., andFeigenbaum, H. (I97i). Echocardiographic features ofatrial septal defect. Circulation, 43, I29.
Edler, I., and Hertz, C. H. (I954). Use of ultrasonic reflecto-scope for the continuous recording of movements of heartwalls. Kungliga Fysiografiska Sallskapets i Lund Forhand-lingar, 24, 5.
Feigenbaum, H. (1972). Echocardiography, pp. I37, I96, and2I6. Lea and Febiger, Philadelphia.
Gramiak, R., Chung, K. J., Nanda, N., and Manning, J.(I973). Echocardiographic diagnosis of transposition ofthe great vessels. Radiology, xo6, I87.
Gramiak, R., and Shah, P. M. (1970). Echocardiography ofthe normal and diseased aortic valve. Radiology, 96, i.
Joyner, C. R., Hey, E. B., Jr., Johnson, J., and Reid, J. M.(I967). Reflected ultrasound in the diagnosis of tricuspidstenosis. American Journal of Cardiology, I9, 66.
Joyner, C. R., and Reid, J. M. (I963). Applications of ultra-sound in cardiology and cardiovascular physiology. Pro-gress in Cardiovascular Diseases, 5, 482.
Lundstrom, N. R. (I973). Echocardiography in the diagnosisof Ebstein's anomaly of the tricuspid valve. Circulation,47, 597.
Tandon, R., Hauck, A. J., and Nadas, A. S. (I963). Persistenttruncus arteriosus. Circulation, 28, 1050.
Van Praagh, R., and Van Praagh, S. (1965). The anatomy ofcommon aorticopulmonary trunk (truncus arteriosus com-munis) and its embryologic implications. American3Journalof Cardiology, I6, 406.
Requests for reprints to Dr. P. A. N. Chandraratna,Cardiology Unit, Mount Sinai Medical Center, 4300Alton Road, Miami Beach, Florida 33I40, U.S.A.
on July 15, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.36.7.732 on 1 July 1974. D
ownloaded from