Embed Size (px)
Citation preview
How Low Can We Go? Readdressing Antibiotic Duration for Common Childhood Infections
Rebecca Levorson, MD Andrew Nuibe, MD, MSCI
Pediatric Infectious Diseases
Disclosures
Dr. Rebecca Levorson: I have no financial interests to disclose Dr. Andrew Nuibe: I have no financial interests to disclose
Duration of therapy should be tailored to each individual case
Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies
Background • Antimicrobials are the most prescribed medication
class in pediatrics1 • Prolonged antimicrobial use has consequences
• Higher costs • Increased risk for adverse outcome, e.g. rash • Selects for resistant pathogens
1 Chai G et al. Pediatrics 2012
Rationale
• 20-50% of all antibiotics prescribed in U.S. acute care hospitals are either unnecessary or inappropriate
• The misuse of antibiotics has also contributed to the growing problem of antibiotic resistance, which has become one of the most serious and growing threats to public health.
http://www.cdc.gov/getsmart/healthcare/implementation/core-elements.html
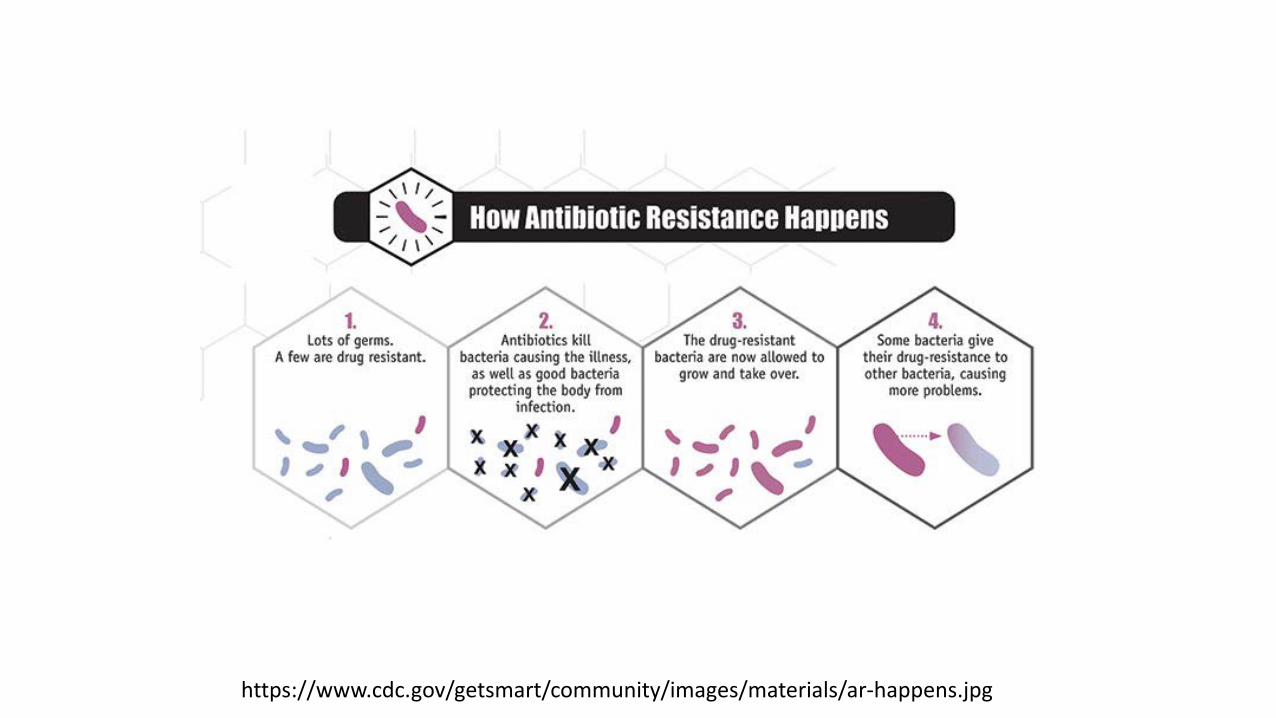
https://www.cdc.gov/getsmart/community/images/materials/ar-happens.jpg
In the United States
• Over 2,000,000 people infected with antibiotic-resistant organisms
• Approximately 23,000 deaths annually in the United States due to antibiotic resistant infections.
http://www.cdc.gov/getsmart/healthcare/implementation/core-elements.html
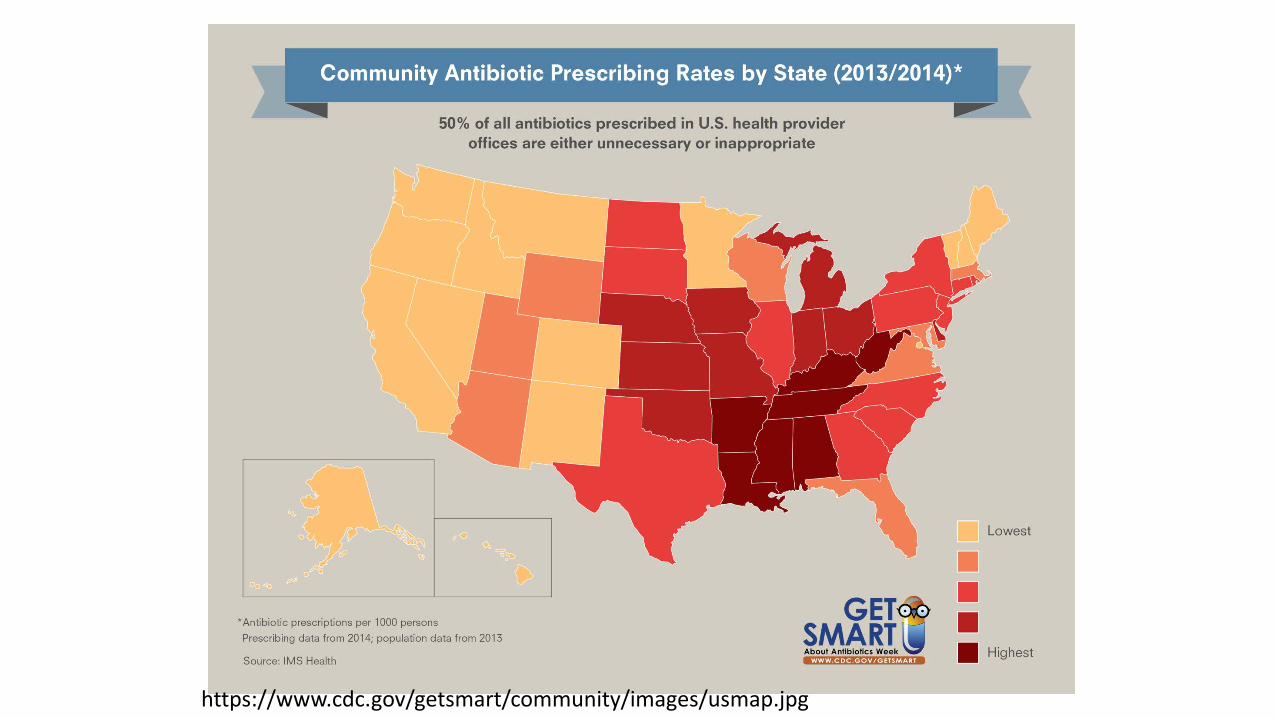
https://www.cdc.gov/getsmart/community/images/usmap.jpg
• 262.5 million courses of antibiotics are written in the outpatient setting yearly. • >5 prescriptions/6 people/year in the United
States.
• Local outpatient prescribing practices contribute to local resistance patterns.
• Azithromycin and amoxicillin are among the most commonly prescribed antibiotics.
In the United States
http://www.cdc.gov/getsmart/week/educational-resources/hcp.html
… We Have a PROBLEM!
Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies
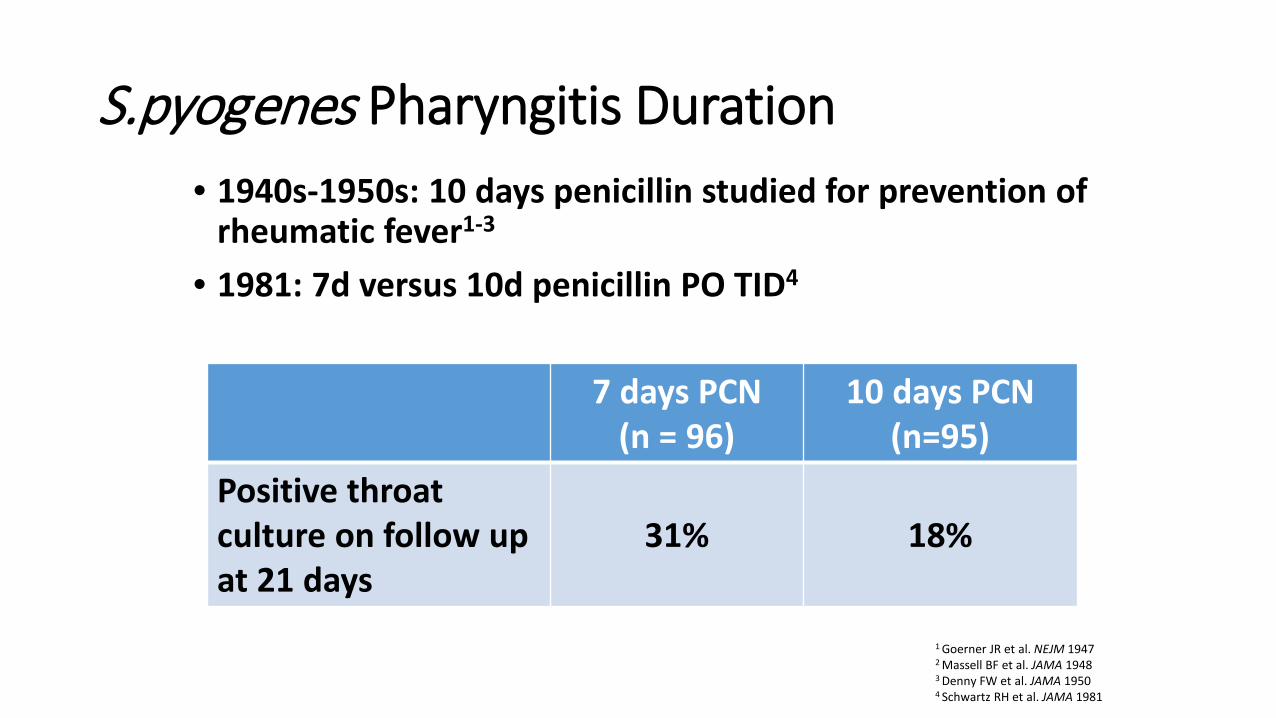
S.pyogenes Pharyngitis Duration • 1940s-1950s: 10 days penicillin studied for prevention of
rheumatic fever1-3 • 1981: 7d versus 10d penicillin PO TID4
1 Goerner JR et al. NEJM 1947 2 Massell BF et al. JAMA 1948
3 Denny FW et al. JAMA 1950
4 Schwartz RH et al. JAMA 1981
7 days PCN (n = 96)
10 days PCN (n=95)
Positive throat culture on follow up at 21 days
31% 18%

S.pyogenes Pharyngitis • 1991: 5 days azithromycin versus 10 days penicillin PO
q6h1
• Similar improvement and eradication • Current U.S. macrolide resistance as high as 50%2,3 • Recommended dosing: 12 mg/kg/dose for 5 days4
• 1996: 6 days amoxicillin BID versus 10 days penicillin PO TID5
• Similar improvement and eradication
1 Hooton TM Am J Med 1991 2 Green M et al. Antimicrob Agents Chemother 2004 3 Martin JM et al. NEJM 2002 4 Shulman ST et al. CID 2012 5 Cohen R et al. PIDJ 1996
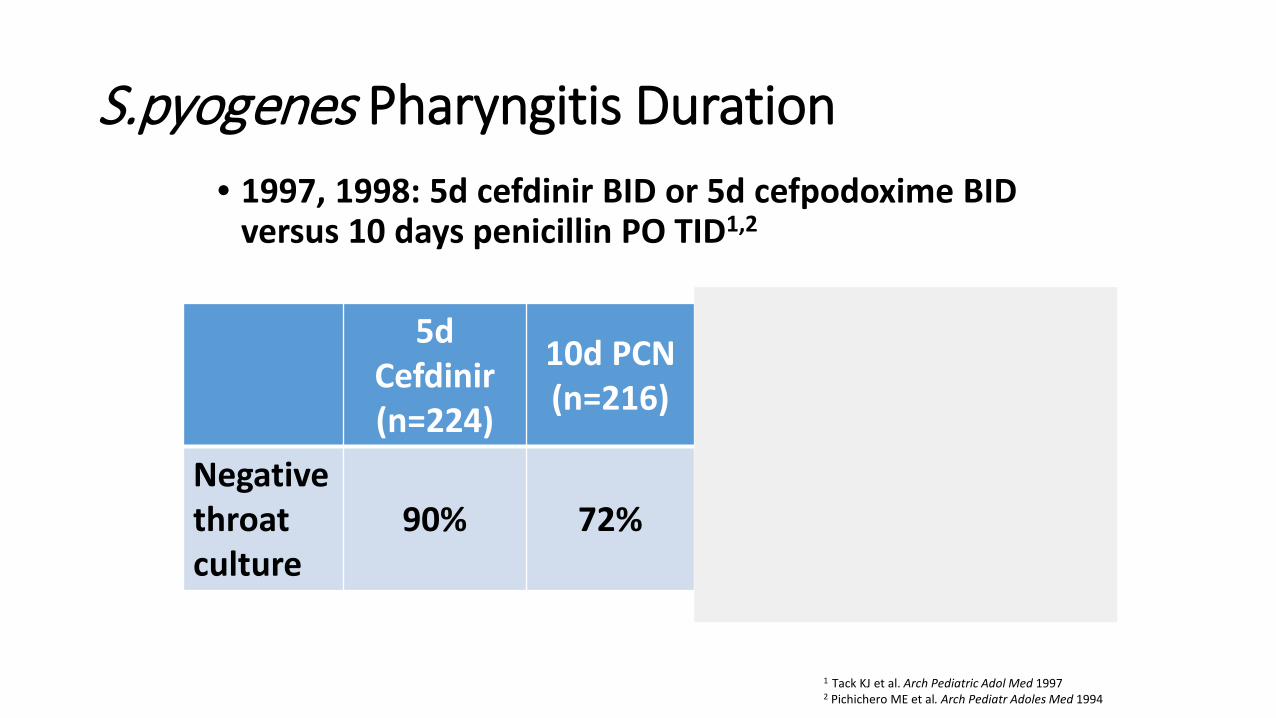
S.pyogenes Pharyngitis Duration • 1997, 1998: 5d cefdinir BID or 5d cefpodoxime BID
versus 10 days penicillin PO TID1,2
1 Tack KJ et al. Arch Pediatric Adol Med 1997 2 Pichichero ME et al. Arch Pediatr Adoles Med 1994
5d Cefdinir (n=224)
10d PCN (n=216)
5d Cefpodoxime
(n=126)
10d PCN (n=130)
Negative throat culture
90% 72% 75% 76%

S. pyogenes Pharyngitis Duration Conclusions: • 10 days of penicillin or amoxicillin recommended first
line therapy for optimal eradication1 • < 10 days of amox, azithro, cefdinir, cefpodoxime
effective for symptom relief and eradication • Unclear whether < 10 days therapy is effective in
preventing rheumatic fever
1 Shulman ST et al. CID 2012
Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies

Uncomplicated CAP Duration
• S.pneumoniae considered major bacterial pathogen in immunized, previously healthy1
• 10 days of amoxicillin BID is standard, cost-effective choice for S.pneumoniae CAP1,2
1 Bradley JS et al. CID 2012 2 Lorgelly PK et al. Eur Resp J 2010
Uncomplicated CAP Duration
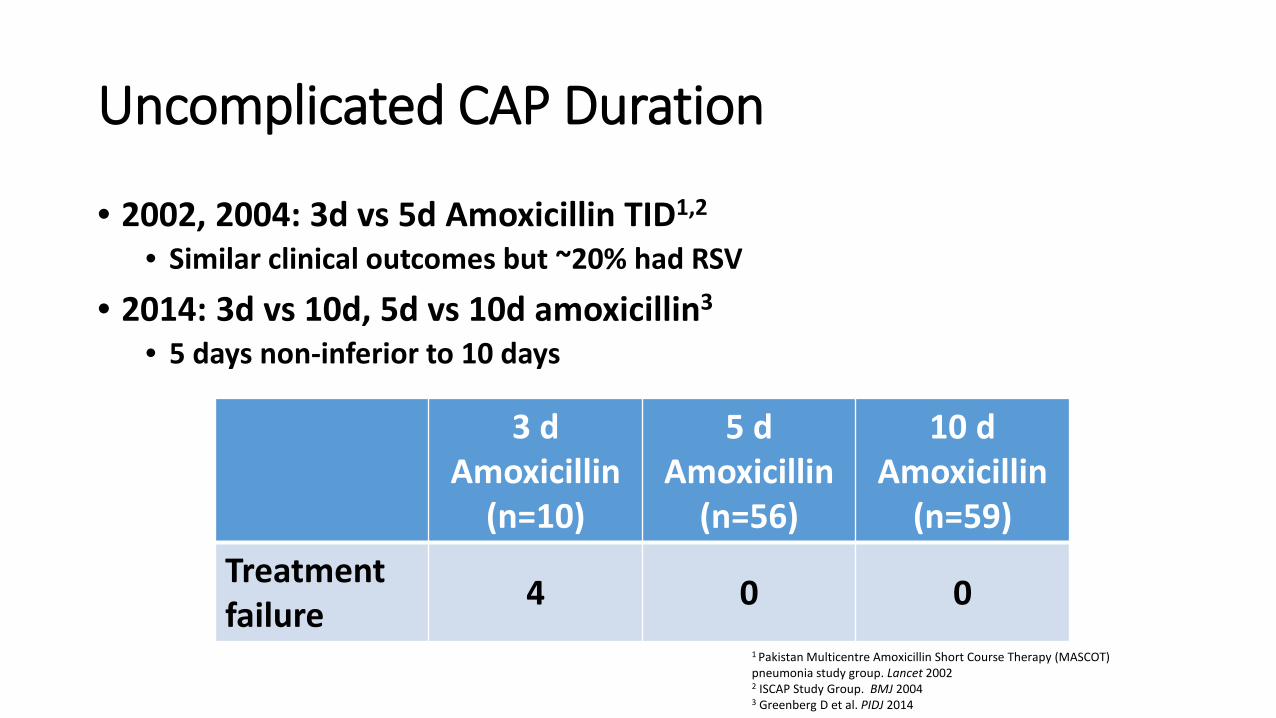
• 2002, 2004: 3d vs 5d Amoxicillin TID1,2 • Similar clinical outcomes but ~20% had RSV
• 2014: 3d vs 10d, 5d vs 10d amoxicillin3 • 5 days non-inferior to 10 days
1 Pakistan Multicentre Amoxicillin Short Course Therapy (MASCOT) pneumonia study group. Lancet 2002 2 ISCAP Study Group. BMJ 2004 3 Greenberg D et al. PIDJ 2014
3 d Amoxicillin
(n=10)
5 d Amoxicillin
(n=56)
10 d Amoxicillin
(n=59) Treatment failure 4 0 0
Uncomplicated CAP Duration Conclusions: • 10 days of amoxicillin recommended for mild-to-
moderate S.pneumoniae CAP1 • 5-10 days of amoxicillin 90 mg/kg/day is acceptable
for mild outpatient CAP1 • Be wary of using oral cephalosporins and macrolides
for S.pneumoniae CAP
1 Bradley JS et al. CID 2012
Atypical CAP Duration
Mycoplasma pneumoniae CAP Azithromycin • 3 d at 10/kg vs. 5 d at 10/kg x1 then 5/kg x 4 d

Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies
Uncomplicated Cellulitis Duration
• Typically due to S. aureus and S. pyogenes • Increasing cellulitis incidence in MRSA era1
• Wide variation in management for SSTIs2,3
• 2004: 5d vs 10d levofloxacin for cellulitis4 • Similar clinical outcomes in both groups
• 2016: < 7 days for non-suppurative cellulitis5 • Therapy < 7 days not associated with higher recurrence cf.
longer therapy
1 Dukc VM et al. PLoS One 2013 2 Mistry RD et al. Acad Emerg Med 2010 3 Moore SJ et al. PIDJ 2014 4 Hepburn MJ et al. Arch Int Med 2004 5 Shuler CL Pediatrics 2016
Uncomplicated Cellulitis Duration
Conclusions: • 5 days of therapy for S. aureus and S. pyogenes
acceptable for uncomplicated cellulitis1 • Can extend duration if not improving
1 Stevens DL et al. CID 2014

Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies
Acute Osteoarticular Infection Duration
• 1967: Arbitrarily treated for 5 weeks1 • Thought that debrided bone took 4 weeks to revascularize2
• Parenteral therapy < 3 weeks tied to chronic disease3,4
• Typically treat pyogenic arthritis for 2-3 weeks and osteomyelitis for 4-6 weeks
1 Green JH. Br Med J 1967 2 Lazzarini L et al. J Bone Joint Surg 2004 3 Dich VQ et al. Am J Dis Child 1975 4 O’Brien et al. J Bone Joint Surg 1982
Acute Osteoarticular Infection Duration
• 1997: 3-4 wks of 1G cephalosporin or clindamycin for acute S.aureus osteomyelitis1
• No treatment failure or long term sequelae
• 2009: 10d vs 30d 1G cephalosporin or clindamycin for S.aureus pyogenic arthritis2
• No treatment failure with shorter course if initial clinical response was robust
1 Peltola et al. Pediatrics 1997 2 Peltola et al. CID 2009
Acute Osteoarticular Infection Duration
Conclusions: • Pyogenic arthritis can be treated for 10-21 days if initial robust
response • Osteomyelitis can be treated for 3-4 weeks if initial robust response
Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies

Urinary Tract Infections
Pediatric UTIs
• Pyuria + Positive Urine Culture • 85% E. coli • AAP guidelines 2011 (2 mo to 2 years) • UA + antibiogram initial empiric therapy • Increasing MDRO UTIs in USA (esp. DC area)
Lower UTIs • 1981: 1 d vs. 10 d: short course less effective in
preventing recurrent infection1
• 2002, 2012: No difference in persistent bacteriuria or recurrence between 2-4 days and 7-14 days of oral antibiotics.2,3
• 2011: Adult guidelines suggest 3-5 days antibiotics4
1 McCracken et al., Pediatrics 1981; 67; 796-801. 2 Michael M, et al., Short versus standard duration oral antibiotic therapy for acute urinary tract infection in children. Cochrane Database Syst Rev 2003; 1:CD003966. 3 Fitzgerald A, et al., Antibiotics for treating lower urinary tract infection in children. Cochrane Database Syst Rev 2012; 8: CD006857. 4 Gupta K, et al., CID 2011:52, 5:e103-120
Acute Pyelonephritis and Febrile UTIs • IV oral vs. all oral antibiotics for 14 days
no difference in renal scarring or recurrence rates even in bacteremia 1, 2
• 1-3 day courses inferior to 7-10 day courses for febrile UTIs 3, 4
• Ongoing NIH sponsored trial for 5 days vs. 10 days for febrile UTI, Acute Pyelonephritis in kids
1 Bocquet N, et al. Randomized trial of oral versus sequential IV/oral antibiotic for acute pyelonephritis in children. Pediatrics 2012; 129:e269-75. 2 Hoberman A, et al., Oral versus initial intravenous therapy for urinary tract infections in young febrile children. Pediatrics 1999; 104:79-86. 3 Grimwood K, et al., N Z Med J 1988; 24;101 4 AAP 2011: UTI clinical practice guidelines; Pediatrics
Pediatric UTI Treatment
Conclusions • Uncomplicated cystitis: 3-5 days
• Febrile UTI & Pyelonephritis: • IV vs. po equal • 7-14 days current AAP guidelines • Awaiting NIH sponsored study results
• 5 vs. 10 days for pediatric pyelonephritis
Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies

http://www.poormd.com/2015/03/appendix-comic.html
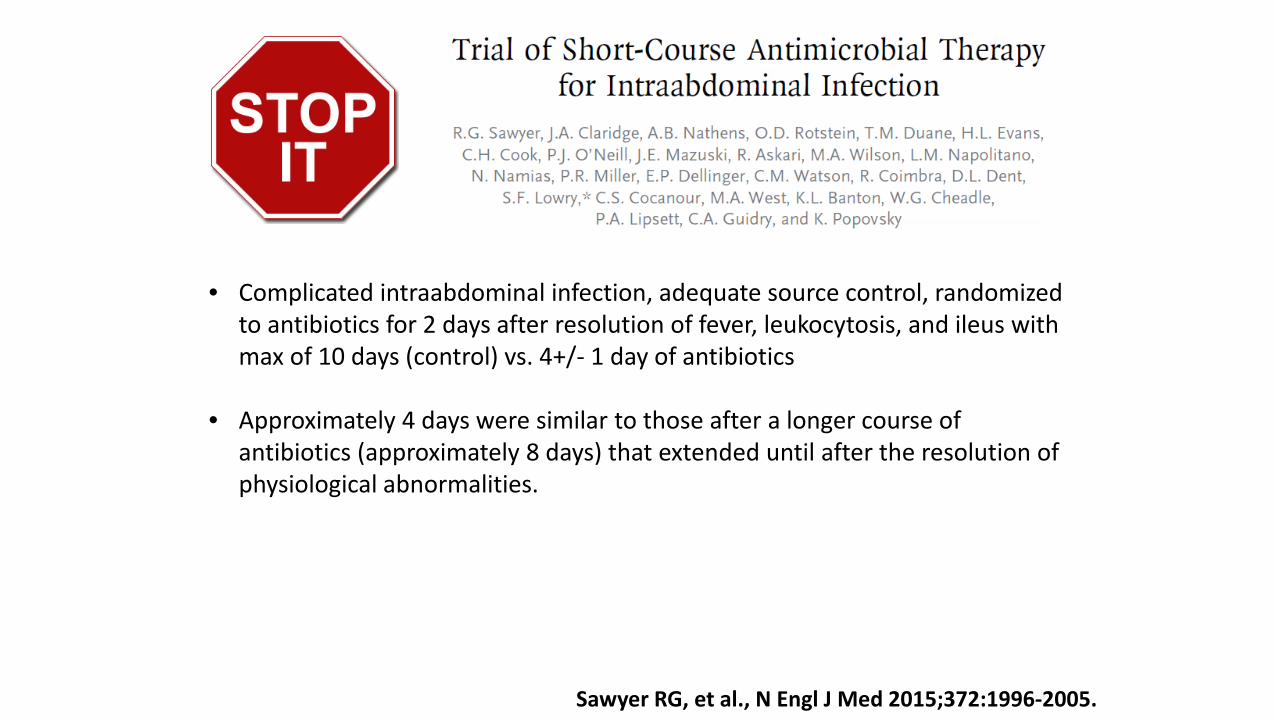
Sawyer RG, et al., N Engl J Med 2015;372:1996-2005.
• Complicated intraabdominal infection, adequate source control, randomized to antibiotics for 2 days after resolution of fever, leukocytosis, and ileus with max of 10 days (control) vs. 4+/- 1 day of antibiotics
• Approximately 4 days were similar to those after a longer course of antibiotics (approximately 8 days) that extended until after the resolution of physiological abnormalities.
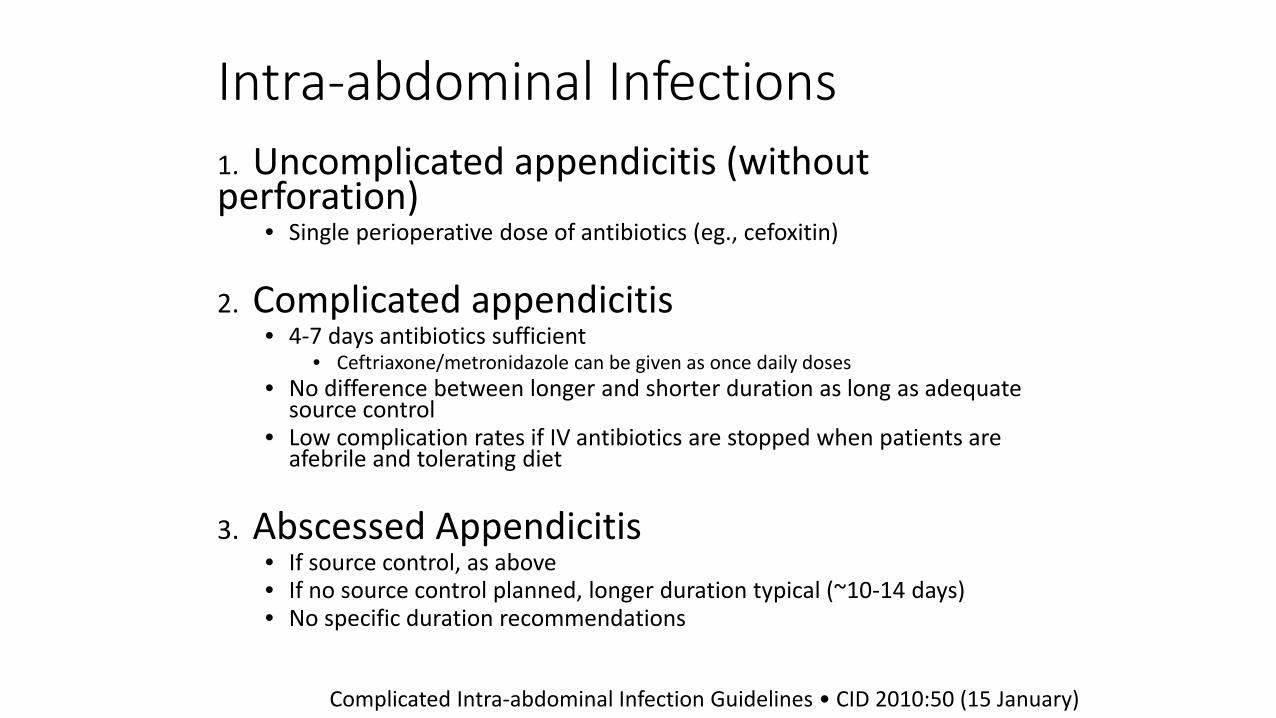
Intra-abdominal Infections 1. Uncomplicated appendicitis (without perforation)
• Single perioperative dose of antibiotics (eg., cefoxitin)
2. Complicated appendicitis • 4-7 days antibiotics sufficient
• Ceftriaxone/metronidazole can be given as once daily doses • No difference between longer and shorter duration as long as adequate
source control • Low complication rates if IV antibiotics are stopped when patients are
afebrile and tolerating diet
3. Abscessed Appendicitis • If source control, as above • If no source control planned, longer duration typical (~10-14 days) • No specific duration recommendations
Complicated Intra-abdominal Infection Guidelines • CID 2010:50 (15 January)

Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies

Acute Bacterial Sinusitis Definition Acute URI with: Persistent illness (nasal discharge [of any quality] or daytime cough or both lasting more than 10 days without improvement)
OR A worsening course (worsening or new onset of nasal discharge, daytime cough, or fever after initial improvement)
OR Severe onset (concurrent fever >102.2 F and purulent nasal discharge for at least 3 consecutive days)
Wald E, et al., Pediatrics 2013; 132; e262

Acute Bacterial Sinusitis Pathogens • Estimated proportions in ABS based on middle ear infections1
• S. pneumoniae (30% cases) • H. influenzae (30% cases) • M. catarrhalis (10% cases) • 25% sterile cultures
1 Casey JR, et al., PIDJ 2010
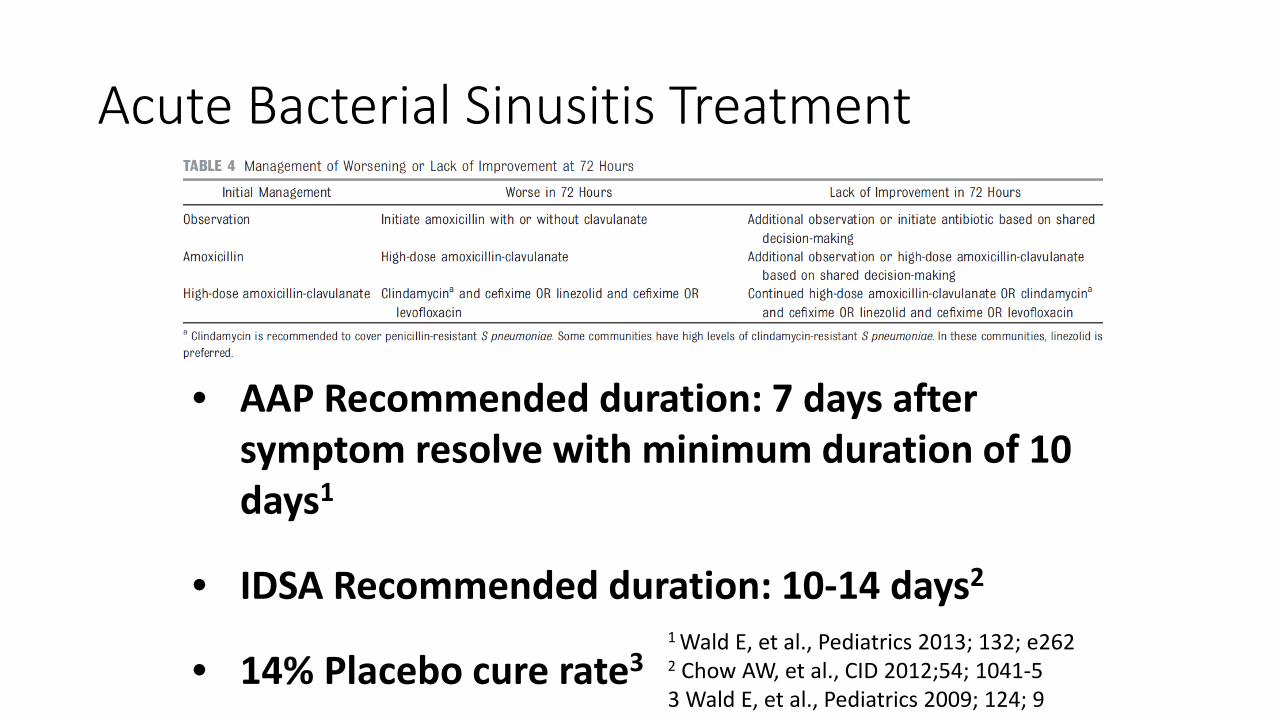
Acute Bacterial Sinusitis Treatment
• AAP Recommended duration: 7 days after symptom resolve with minimum duration of 10 days1
• IDSA Recommended duration: 10-14 days2
• 14% Placebo cure rate3 1 Wald E, et al., Pediatrics 2013; 132; e262 2 Chow AW, et al., CID 2012;54; 1041-5 3 Wald E, et al., Pediatrics 2009; 124; 9
Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies
Acute Otitis Media
• Pathogens same as Acute Bacterial Sinusitis • 2004 AAP Guidelines help with AOM diagnostic criteria, watch/wait • 10 day course derived from S.pyogenes pharyngitis therapy1
• 1997: Augmentin BID 5d or 10d versus Augmentin TID2 • 5 d not as effective, especially in < 2 yo
1 Lieberthal AS et al. Pediatrics 2013 2 Hoberman A et al. PIDJ 1997

Who to treat?
Start Antibiotics Severe <2 yo Nonsevere bilateral <2 yo
Close Observation OR Start Antibiotics Nonsevere Unilateral < 2yo Nonsevere AOM >2 yo

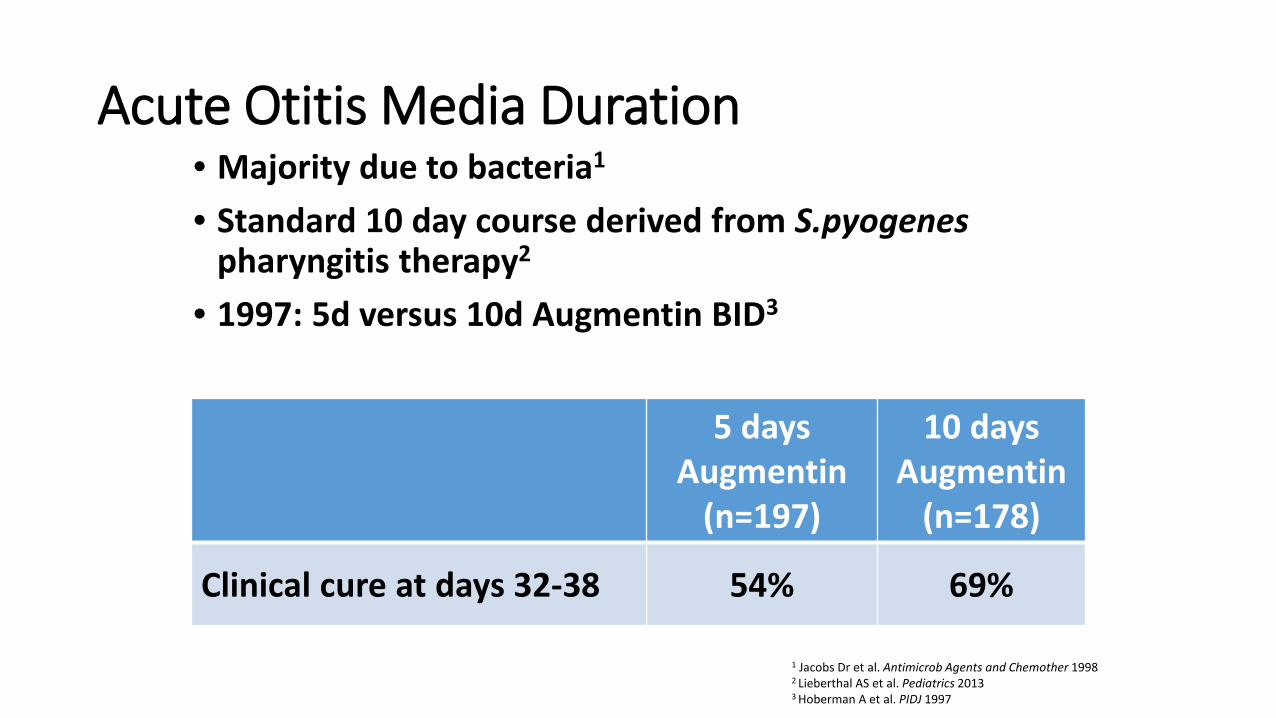
Acute Otitis Media Duration • Majority due to bacteria1
• Standard 10 day course derived from S.pyogenes pharyngitis therapy2
• 1997: 5d versus 10d Augmentin BID3
1 Jacobs Dr et al. Antimicrob Agents and Chemother 1998 2 Lieberthal AS et al. Pediatrics 2013 3 Hoberman A et al. PIDJ 1997
5 days Augmentin
(n=197)
10 days Augmentin
(n=178)
Clinical cure at days 32-38 54% 69%

Acute Otitis Media Duration
• 2001: Antibiotics for 5, 7, or 10 days
Pichichero ME et al. Otolaryngol Head Neck Surg 2001
5 days (n=707)
7 days (n=423)
10 days (n=1042)
All ages Cured + Improved 82% 82% 83%
≤ 2 yo Cured + Improved 75% 73% 76%
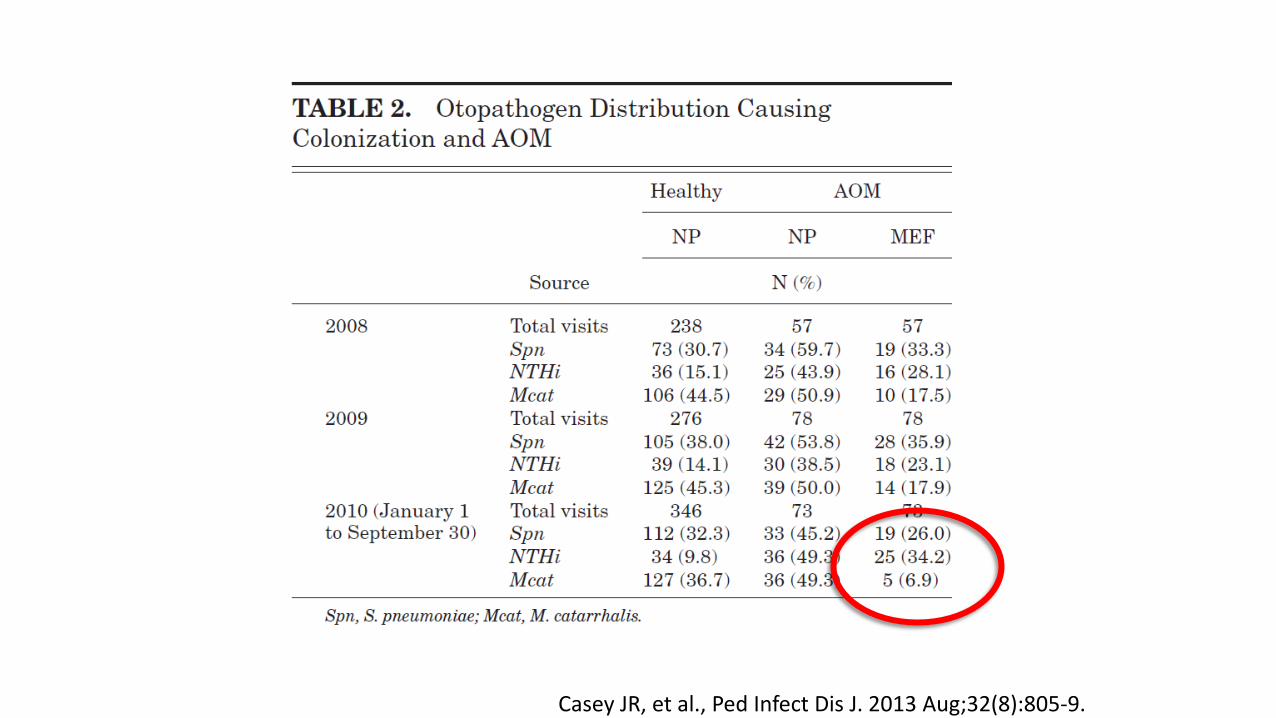
Casey JR, et al., Ped Infect Dis J. 2013 Aug;32(8):805-9.
Acute Otitis Media Duration
Conclusions: • < 2 yo should get 10 days of amoxicillin • 2-5 yo can get 7 days of amoxicillin • > 6 yo can get 5-7 days of amoxicillin • Be wary of using oral cephalosporins and macrolides for
S.pneumoniae1
1 Lieberthal AS et al. Pediatrics 2013
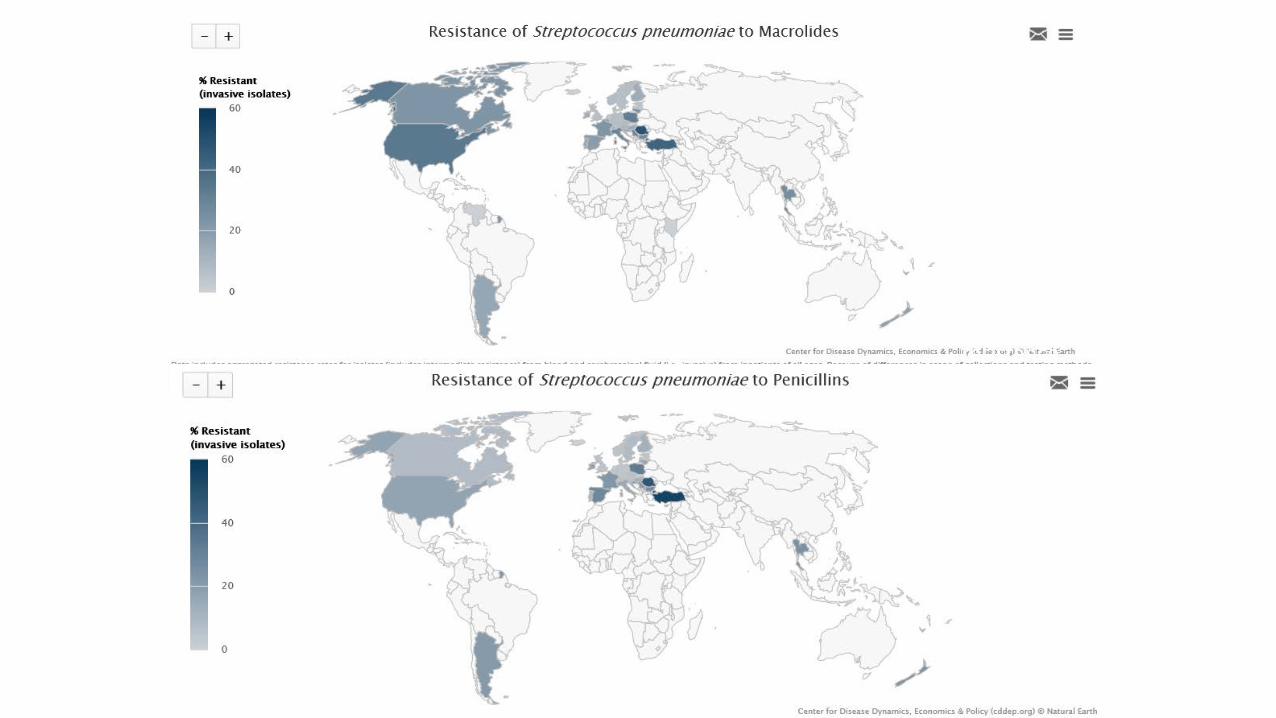
USA: 34% Strep pneumo
macrolide resistance
17% Strep pneumo Penicillin
resistance
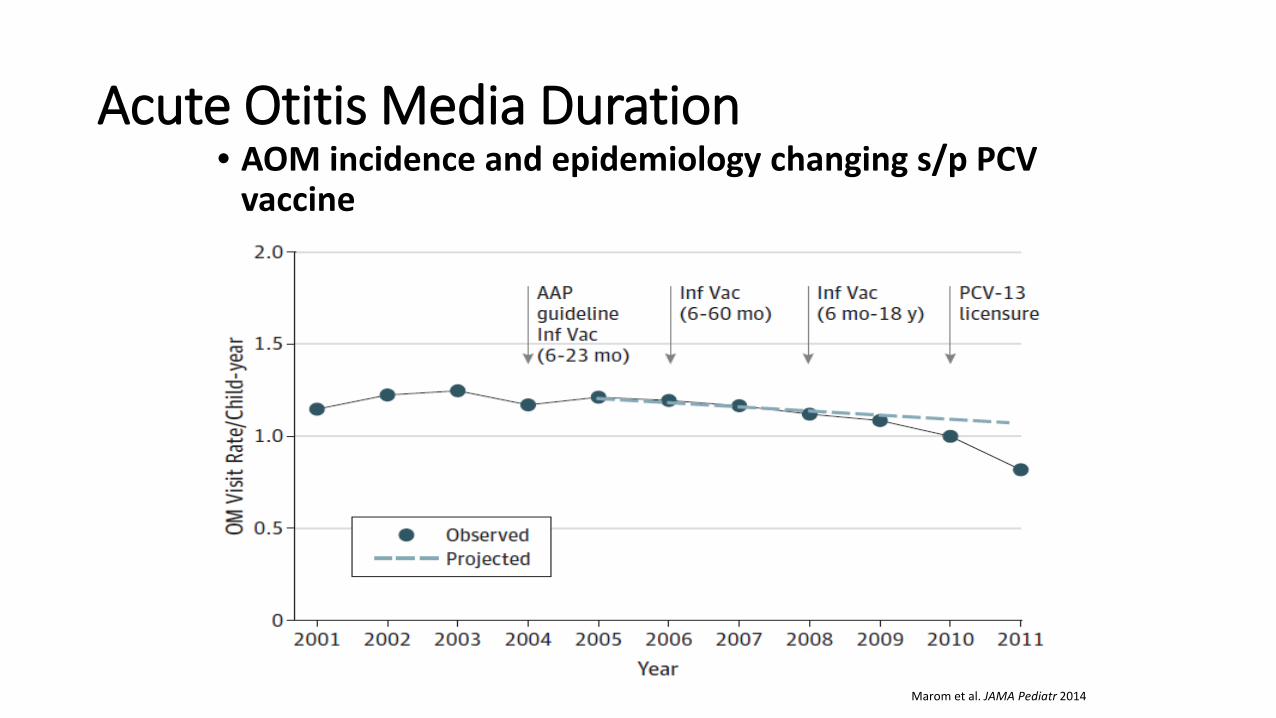
Acute Otitis Media Duration • AOM incidence and epidemiology changing s/p PCV
vaccine
Marom et al. JAMA Pediatr 2014
Summary • Opportunities remain to determine optimal length
of therapy for many infections • Thoughtfully consider the patient’s response to
therapy • “Return for Re-evaluation” vs. “Finish the Whole
Bottle” • Educate Everyone including Patients and Parents as
Antibiotics are a Shared Resource


PSV Pediatric Infectious Diseases
Dr. Daniel Keim Dr. Rebecca Levorson Dr. Katherine Moyer Dr. Andrew Nuibe Dr. Brittany Goldberg