How Low Can We Go? Readdressing Antibiotic Duration for Common Childhood Infections
Rebecca Levorson, MD Andrew Nuibe, MD, MSCI
Pediatric Infectious Diseases
Disclosures
Dr. Rebecca Levorson: I have no financial interests to disclose Dr. Andrew Nuibe: I have no financial interests to disclose
Duration of therapy should be tailored to each individual case
Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies
Background • Antimicrobials are the most prescribed medication
class in pediatrics1 • Prolonged antimicrobial use has consequences
• Higher costs • Increased risk for adverse outcome, e.g. rash • Selects for resistant pathogens
1 Chai G et al. Pediatrics 2012
Rationale
• 20-50% of all antibiotics prescribed in U.S. acute care hospitals are either unnecessary or inappropriate
• The misuse of antibiotics has also contributed to the growing problem of antibiotic resistance, which has become one of the most serious and growing threats to public health.
http://www.cdc.gov/getsmart/healthcare/implementation/core-elements.html
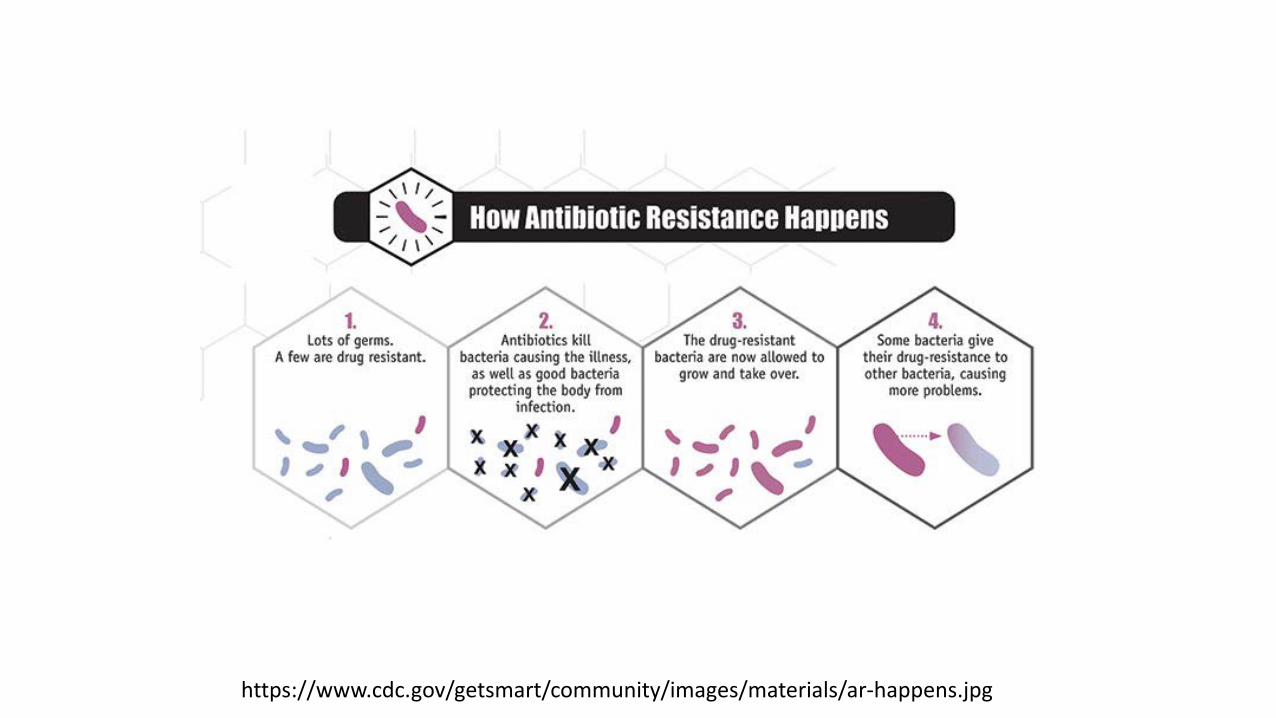
https://www.cdc.gov/getsmart/community/images/materials/ar-happens.jpg
In the United States
• Over 2,000,000 people infected with antibiotic-resistant organisms
• Approximately 23,000 deaths annually in the United States due to antibiotic resistant infections.
http://www.cdc.gov/getsmart/healthcare/implementation/core-elements.html
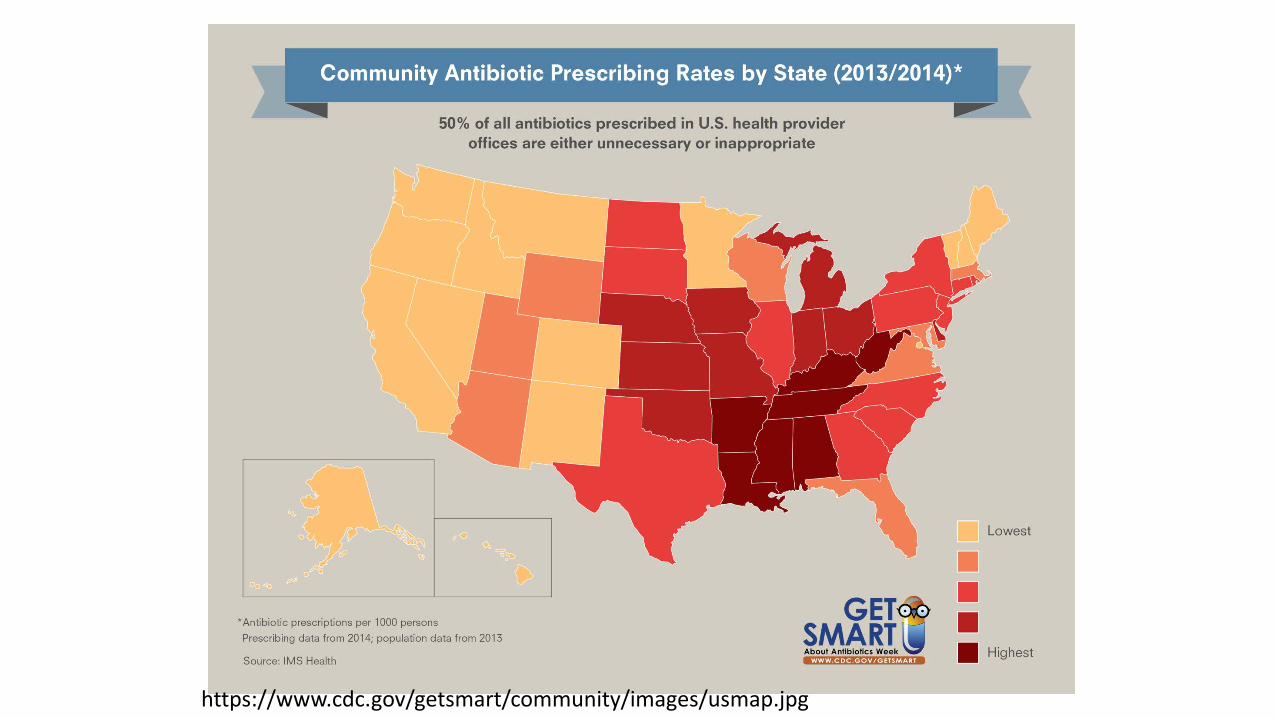
https://www.cdc.gov/getsmart/community/images/usmap.jpg
• 262.5 million courses of antibiotics are written in the outpatient setting yearly. • >5 prescriptions/6 people/year in the United
States.
• Local outpatient prescribing practices contribute to local resistance patterns.
• Azithromycin and amoxicillin are among the most commonly prescribed antibiotics.
In the United States
http://www.cdc.gov/getsmart/week/educational-resources/hcp.html
… We Have a PROBLEM!
Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies
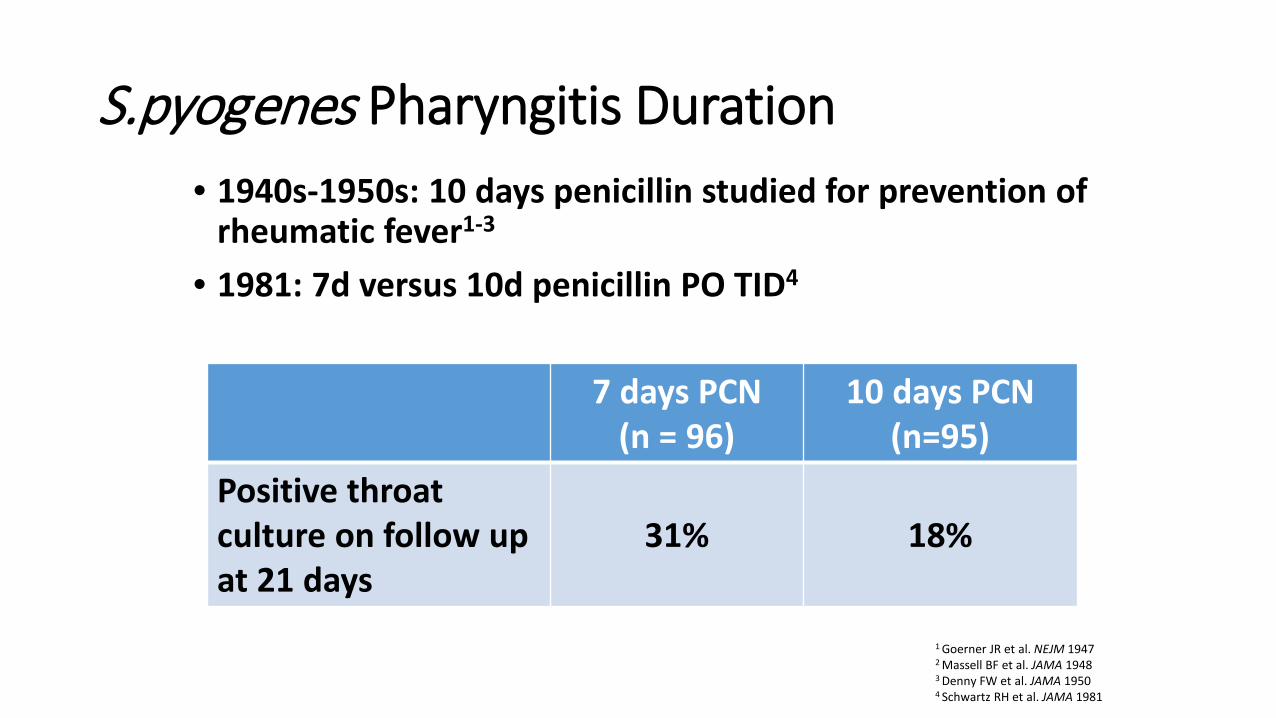
S.pyogenes Pharyngitis Duration • 1940s-1950s: 10 days penicillin studied for prevention of
rheumatic fever1-3 • 1981: 7d versus 10d penicillin PO TID4
1 Goerner JR et al. NEJM 1947 2 Massell BF et al. JAMA 1948
3 Denny FW et al. JAMA 1950
4 Schwartz RH et al. JAMA 1981
7 days PCN (n = 96)
10 days PCN (n=95)
Positive throat culture on follow up at 21 days
31% 18%

S.pyogenes Pharyngitis • 1991: 5 days azithromycin versus 10 days penicillin PO
q6h1
• Similar improvement and eradication • Current U.S. macrolide resistance as high as 50%2,3 • Recommended dosing: 12 mg/kg/dose for 5 days4
• 1996: 6 days amoxicillin BID versus 10 days penicillin PO TID5
• Similar improvement and eradication
1 Hooton TM Am J Med 1991 2 Green M et al. Antimicrob Agents Chemother 2004 3 Martin JM et al. NEJM 2002 4 Shulman ST et al. CID 2012 5 Cohen R et al. PIDJ 1996
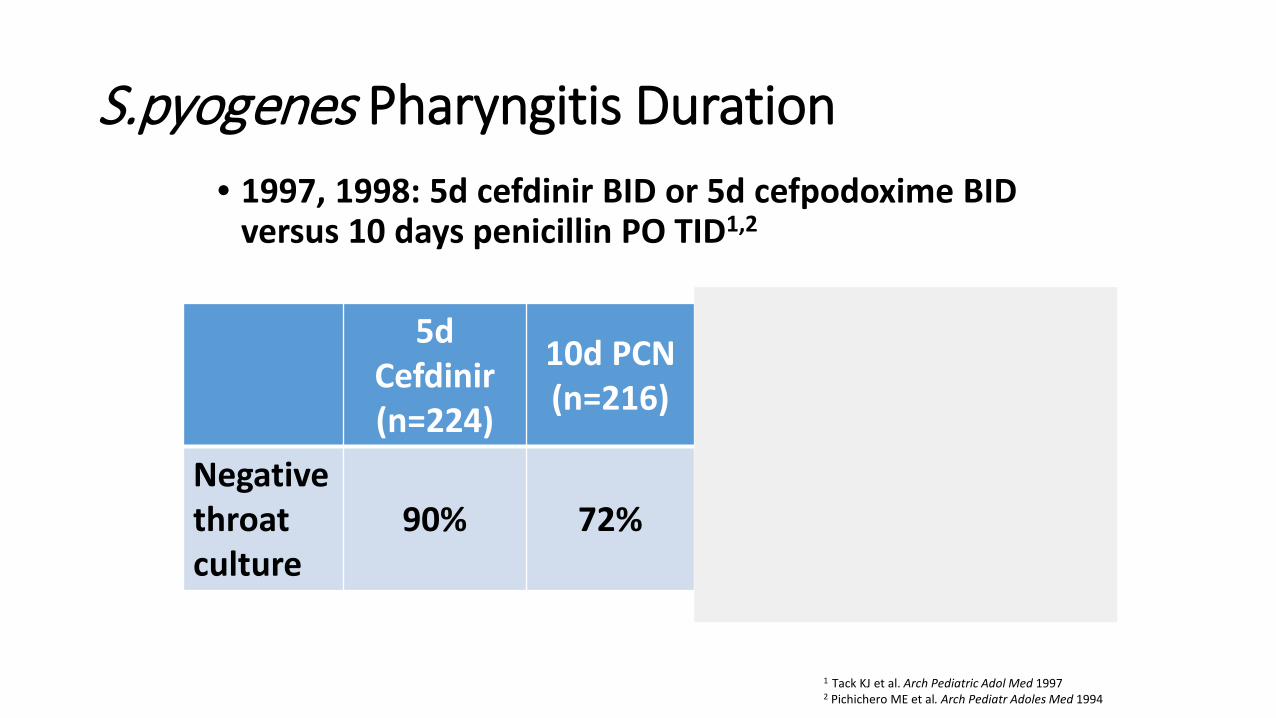
S.pyogenes Pharyngitis Duration • 1997, 1998: 5d cefdinir BID or 5d cefpodoxime BID
versus 10 days penicillin PO TID1,2
1 Tack KJ et al. Arch Pediatric Adol Med 1997 2 Pichichero ME et al. Arch Pediatr Adoles Med 1994
5d Cefdinir (n=224)
10d PCN (n=216)
5d Cefpodoxime
(n=126)
10d PCN (n=130)
Negative throat culture
90% 72% 75% 76%

S. pyogenes Pharyngitis Duration Conclusions: • 10 days of penicillin or amoxicillin recommended first
line therapy for optimal eradication1 • < 10 days of amox, azithro, cefdinir, cefpodoxime
effective for symptom relief and eradication • Unclear whether < 10 days therapy is effective in
preventing rheumatic fever
1 Shulman ST et al. CID 2012
Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies

Uncomplicated CAP Duration
• S.pneumoniae considered major bacterial pathogen in immunized, previously healthy1
• 10 days of amoxicillin BID is standard, cost-effective choice for S.pneumoniae CAP1,2
1 Bradley JS et al. CID 2012 2 Lorgelly PK et al. Eur Resp J 2010
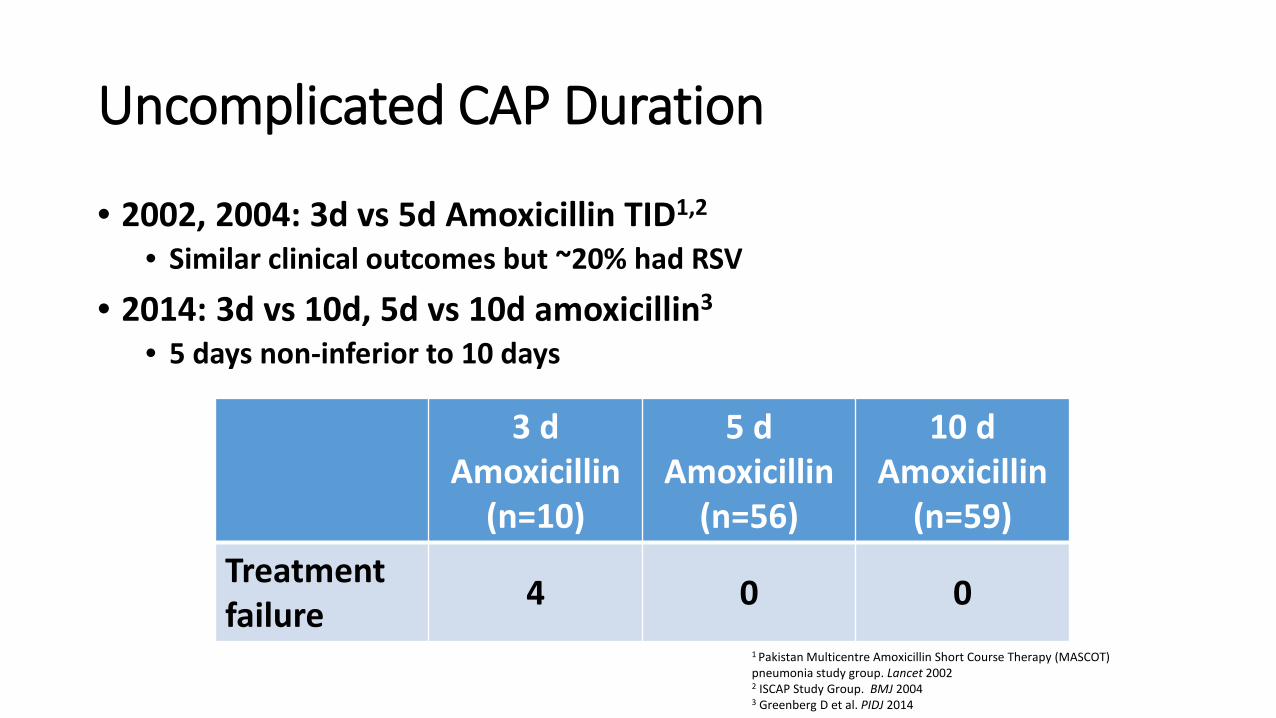
Uncomplicated CAP Duration
• 2002, 2004: 3d vs 5d Amoxicillin TID1,2 • Similar clinical outcomes but ~20% had RSV
• 2014: 3d vs 10d, 5d vs 10d amoxicillin3 • 5 days non-inferior to 10 days
1 Pakistan Multicentre Amoxicillin Short Course Therapy (MASCOT) pneumonia study group. Lancet 2002 2 ISCAP Study Group. BMJ 2004 3 Greenberg D et al. PIDJ 2014
3 d Amoxicillin
(n=10)
5 d Amoxicillin
(n=56)
10 d Amoxicillin
(n=59) Treatment failure 4 0 0
Uncomplicated CAP Duration Conclusions: • 10 days of amoxicillin recommended for mild-to-
moderate S.pneumoniae CAP1 • 5-10 days of amoxicillin 90 mg/kg/day is acceptable
for mild outpatient CAP1 • Be wary of using oral cephalosporins and macrolides
for S.pneumoniae CAP
1 Bradley JS et al. CID 2012
Atypical CAP Duration
Mycoplasma pneumoniae CAP Azithromycin • 3 d at 10/kg vs. 5 d at 10/kg x1 then 5/kg x 4 d

Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies
Uncomplicated Cellulitis Duration
• Typically due to S. aureus and S. pyogenes • Increasing cellulitis incidence in MRSA era1
• Wide variation in management for SSTIs2,3
• 2004: 5d vs 10d levofloxacin for cellulitis4 • Similar clinical outcomes in both groups
• 2016: < 7 days for non-suppurative cellulitis5 • Therapy < 7 days not associated with higher recurrence cf.
longer therapy
1 Dukc VM et al. PLoS One 2013 2 Mistry RD et al. Acad Emerg Med 2010 3 Moore SJ et al. PIDJ 2014 4 Hepburn MJ et al. Arch Int Med 2004 5 Shuler CL Pediatrics 2016
Uncomplicated Cellulitis Duration
Conclusions: • 5 days of therapy for S. aureus and S. pyogenes
acceptable for uncomplicated cellulitis1 • Can extend duration if not improving
1 Stevens DL et al. CID 2014

Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies
Acute Osteoarticular Infection Duration
• 1967: Arbitrarily treated for 5 weeks1 • Thought that debrided bone took 4 weeks to revascularize2
• Parenteral therapy < 3 weeks tied to chronic disease3,4
• Typically treat pyogenic arthritis for 2-3 weeks and osteomyelitis for 4-6 weeks
1 Green JH. Br Med J 1967 2 Lazzarini L et al. J Bone Joint Surg 2004 3 Dich VQ et al. Am J Dis Child 1975 4 O’Brien et al. J Bone Joint Surg 1982
Acute Osteoarticular Infection Duration
• 1997: 3-4 wks of 1G cephalosporin or clindamycin for acute S.aureus osteomyelitis1
• No treatment failure or long term sequelae
• 2009: 10d vs 30d 1G cephalosporin or clindamycin for S.aureus pyogenic arthritis2
• No treatment failure with shorter course if initial clinical response was robust
1 Peltola et al. Pediatrics 1997 2 Peltola et al. CID 2009
Acute Osteoarticular Infection Duration
Conclusions: • Pyogenic arthritis can be treated for 10-21 days if initial robust
response • Osteomyelitis can be treated for 3-4 weeks if initial robust response
Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies

Urinary Tract Infections
Pediatric UTIs
• Pyuria + Positive Urine Culture • 85% E. coli • AAP guidelines 2011 (2 mo to 2 years) • UA + antibiogram initial empiric therapy • Increasing MDRO UTIs in USA (esp. DC area)
Lower UTIs • 1981: 1 d vs. 10 d: short course less effective in
preventing recurrent infection1
• 2002, 2012: No difference in persistent bacteriuria or recurrence between 2-4 days and 7-14 days of oral antibiotics.2,3
• 2011: Adult guidelines suggest 3-5 days antibiotics4
1 McCracken et al., Pediatrics 1981; 67; 796-801. 2 Michael M, et al., Short versus standard duration oral antibiotic therapy for acute urinary tract infection in children. Cochrane Database Syst Rev 2003; 1:CD003966. 3 Fitzgerald A, et al., Antibiotics for treating lower urinary tract infection in children. Cochrane Database Syst Rev 2012; 8: CD006857. 4 Gupta K, et al., CID 2011:52, 5:e103-120
Acute Pyelonephritis and Febrile UTIs • IV oral vs. all oral antibiotics for 14 days
no difference in renal scarring or recurrence rates even in bacteremia 1, 2
• 1-3 day courses inferior to 7-10 day courses for febrile UTIs 3, 4
• Ongoing NIH sponsored trial for 5 days vs. 10 days for febrile UTI, Acute Pyelonephritis in kids
1 Bocquet N, et al. Randomized trial of oral versus sequential IV/oral antibiotic for acute pyelonephritis in children. Pediatrics 2012; 129:e269-75. 2 Hoberman A, et al., Oral versus initial intravenous therapy for urinary tract infections in young febrile children. Pediatrics 1999; 104:79-86. 3 Grimwood K, et al., N Z Med J 1988; 24;101 4 AAP 2011: UTI clinical practice guidelines; Pediatrics
Pediatric UTI Treatment
Conclusions • Uncomplicated cystitis: 3-5 days
• Febrile UTI & Pyelonephritis: • IV vs. po equal • 7-14 days current AAP guidelines • Awaiting NIH sponsored study results
• 5 vs. 10 days for pediatric pyelonephritis
Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies

http://www.poormd.com/2015/03/appendix-comic.html
Sawyer RG, et al., N Engl J Med 2015;372:1996-2005.
• Complicated intraabdominal infection, adequate source control, randomized to antibiotics for 2 days after resolution of fever, leukocytosis, and ileus with max of 10 days (control) vs. 4+/- 1 day of antibiotics
• Approximately 4 days were similar to those after a longer course of antibiotics (approximately 8 days) that extended until after the resolution of physiological abnormalities.
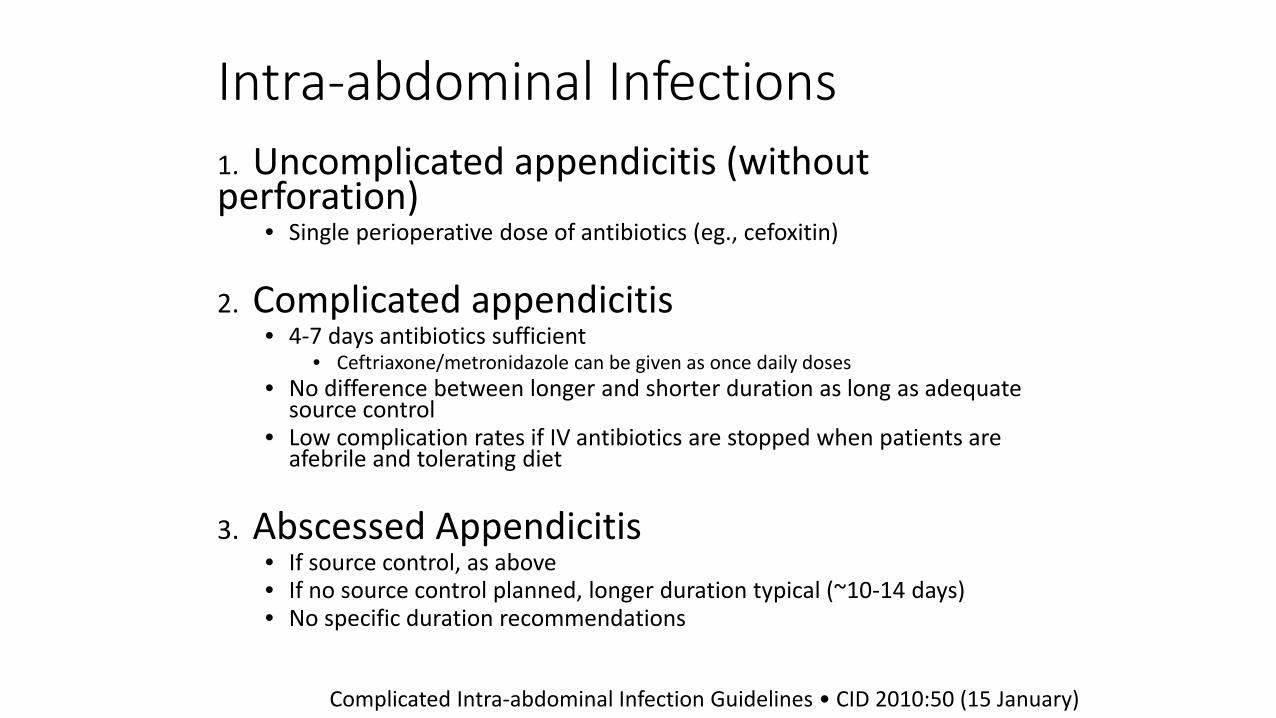
Intra-abdominal Infections 1. Uncomplicated appendicitis (without perforation)
• Single perioperative dose of antibiotics (eg., cefoxitin)
2. Complicated appendicitis • 4-7 days antibiotics sufficient
• Ceftriaxone/metronidazole can be given as once daily doses • No difference between longer and shorter duration as long as adequate
source control • Low complication rates if IV antibiotics are stopped when patients are
afebrile and tolerating diet
3. Abscessed Appendicitis • If source control, as above • If no source control planned, longer duration typical (~10-14 days) • No specific duration recommendations
Complicated Intra-abdominal Infection Guidelines • CID 2010:50 (15 January)

Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies

Acute Bacterial Sinusitis Definition Acute URI with: Persistent illness (nasal discharge [of any quality] or daytime cough or both lasting more than 10 days without improvement)
OR A worsening course (worsening or new onset of nasal discharge, daytime cough, or fever after initial improvement)
OR Severe onset (concurrent fever >102.2 F and purulent nasal discharge for at least 3 consecutive days)
Wald E, et al., Pediatrics 2013; 132; e262

Acute Bacterial Sinusitis Pathogens • Estimated proportions in ABS based on middle ear infections1
• S. pneumoniae (30% cases) • H. influenzae (30% cases) • M. catarrhalis (10% cases) • 25% sterile cultures
1 Casey JR, et al., PIDJ 2010
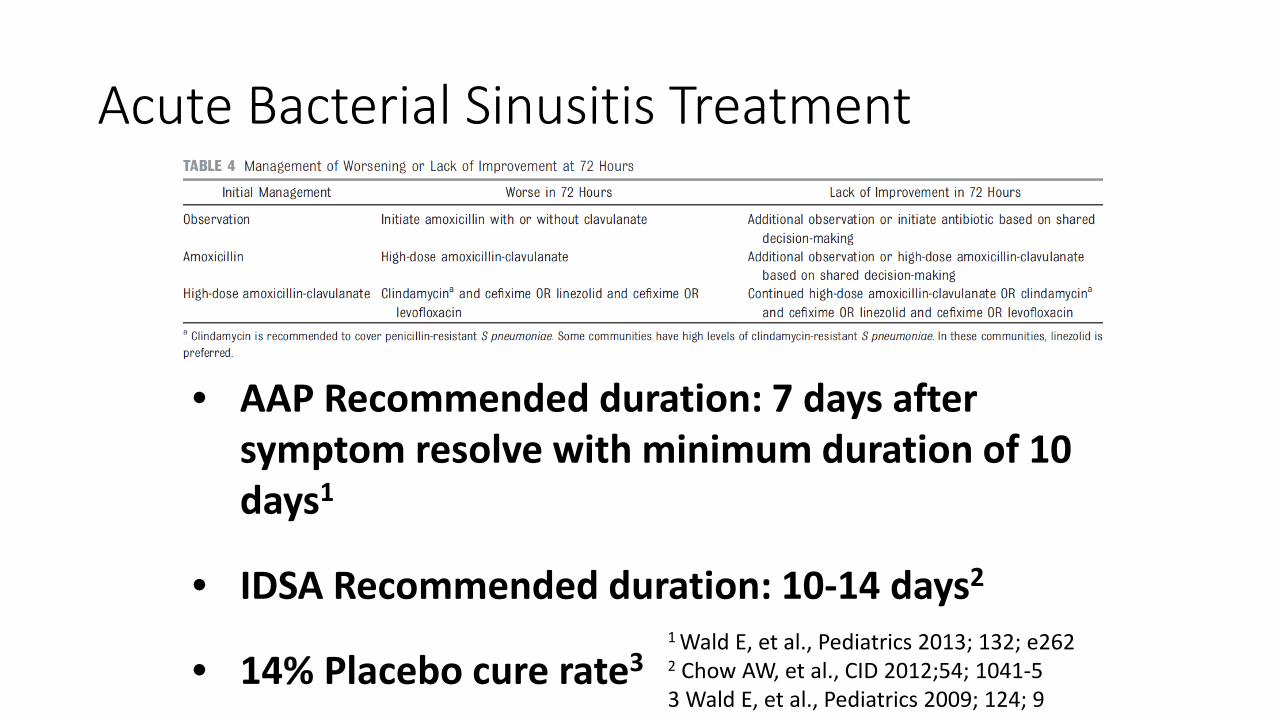
Acute Bacterial Sinusitis Treatment
• AAP Recommended duration: 7 days after symptom resolve with minimum duration of 10 days1
• IDSA Recommended duration: 10-14 days2
• 14% Placebo cure rate3 1 Wald E, et al., Pediatrics 2013; 132; e262 2 Chow AW, et al., CID 2012;54; 1041-5 3 Wald E, et al., Pediatrics 2009; 124; 9
Objectives Review Recommended Duration of Antimicrobial Therapy for Common Childhood Infections including:
• Group A Streptococcal Pharyngitis
• CAP • Typical & Atypical
• Cellulitis • Acute osteomyelitis
• UTI • Cystitis • Pyelonephritis
• Intra-abdominal Infections
• Sinusitis • Otitis Media
Based on Clinical Guidelines and Clinical Studies
Acute Otitis Media
• Pathogens same as Acute Bacterial Sinusitis • 2004 AAP Guidelines help with AOM diagnostic criteria, watch/wait • 10 day course derived from S.pyogenes pharyngitis therapy1
• 1997: Augmentin BID 5d or 10d versus Augmentin TID2 • 5 d not as effective, especially in < 2 yo
1 Lieberthal AS et al. Pediatrics 2013 2 Hoberman A et al. PIDJ 1997

Who to treat?
Start Antibiotics Severe <2 yo Nonsevere bilateral <2 yo
Close Observation OR Start Antibiotics Nonsevere Unilateral < 2yo Nonsevere AOM >2 yo

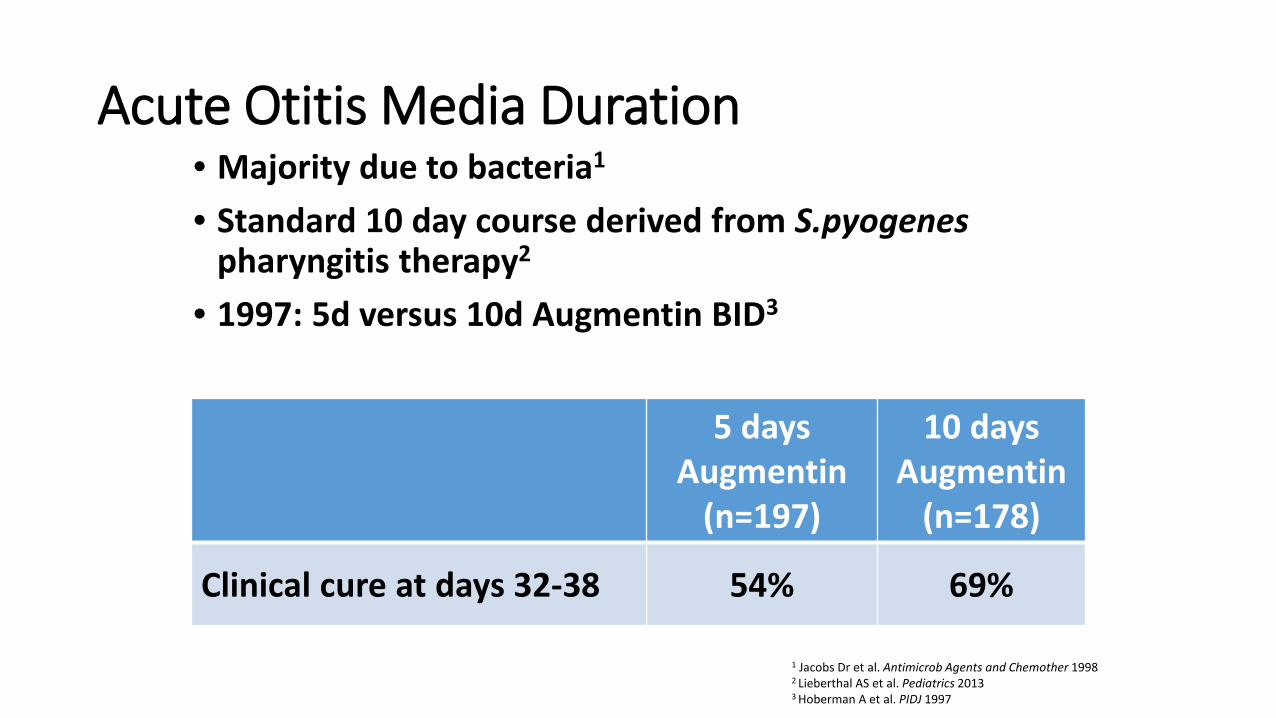
Acute Otitis Media Duration • Majority due to bacteria1
• Standard 10 day course derived from S.pyogenes pharyngitis therapy2
• 1997: 5d versus 10d Augmentin BID3
1 Jacobs Dr et al. Antimicrob Agents and Chemother 1998 2 Lieberthal AS et al. Pediatrics 2013 3 Hoberman A et al. PIDJ 1997
5 days Augmentin
(n=197)
10 days Augmentin
(n=178)
Clinical cure at days 32-38 54% 69%

Acute Otitis Media Duration
• 2001: Antibiotics for 5, 7, or 10 days
Pichichero ME et al. Otolaryngol Head Neck Surg 2001
5 days (n=707)
7 days (n=423)
10 days (n=1042)
All ages Cured + Improved 82% 82% 83%
≤ 2 yo Cured + Improved 75% 73% 76%
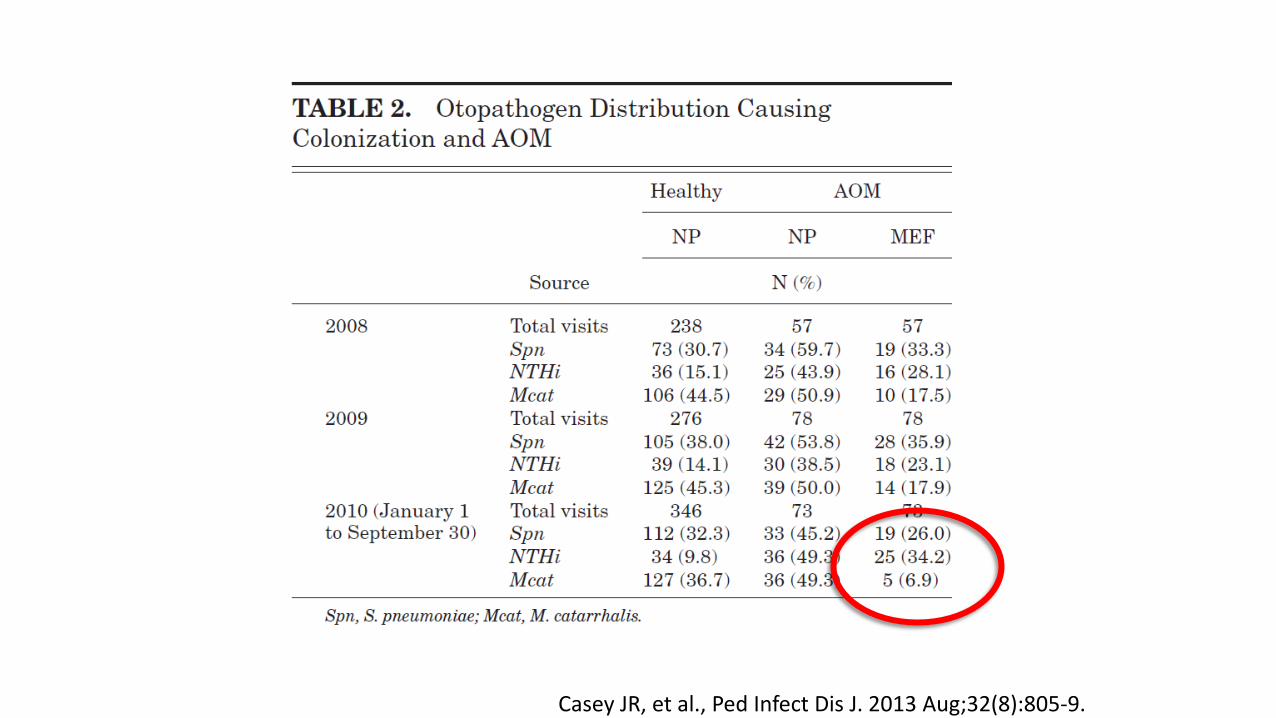
Casey JR, et al., Ped Infect Dis J. 2013 Aug;32(8):805-9.
Acute Otitis Media Duration
Conclusions: • < 2 yo should get 10 days of amoxicillin • 2-5 yo can get 7 days of amoxicillin • > 6 yo can get 5-7 days of amoxicillin • Be wary of using oral cephalosporins and macrolides for
S.pneumoniae1
1 Lieberthal AS et al. Pediatrics 2013
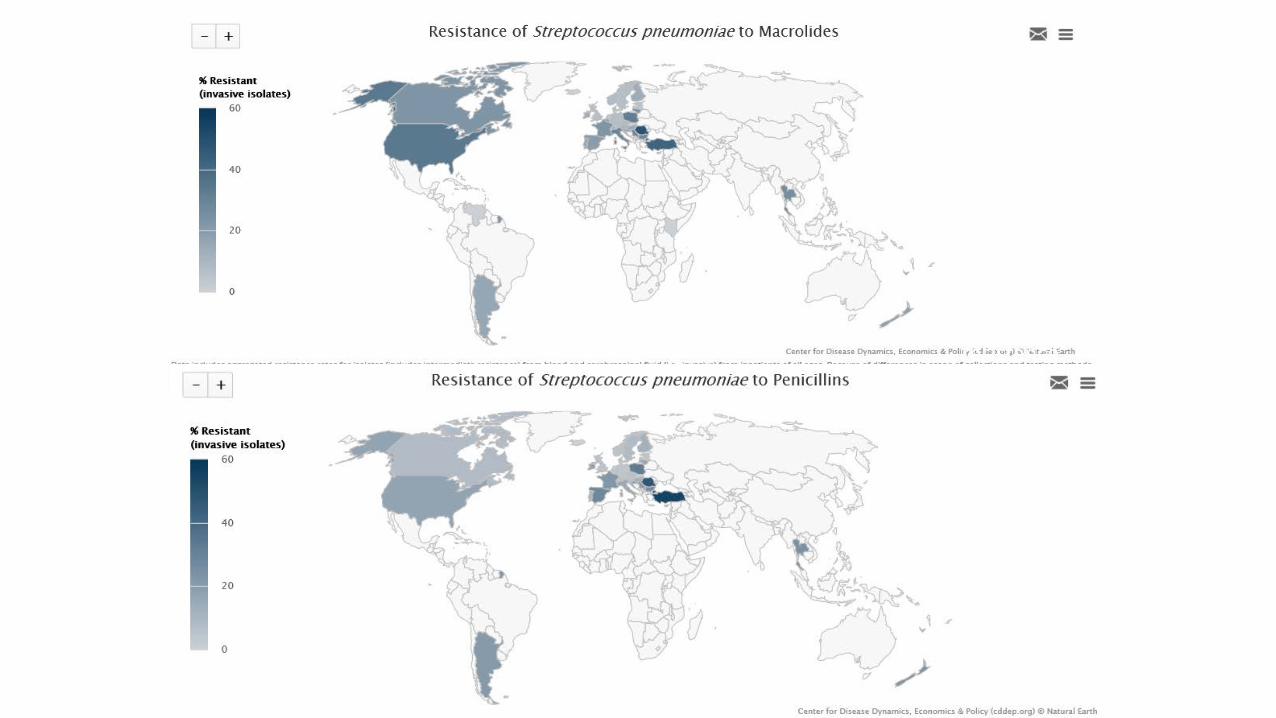
USA: 34% Strep pneumo
macrolide resistance
17% Strep pneumo Penicillin
resistance
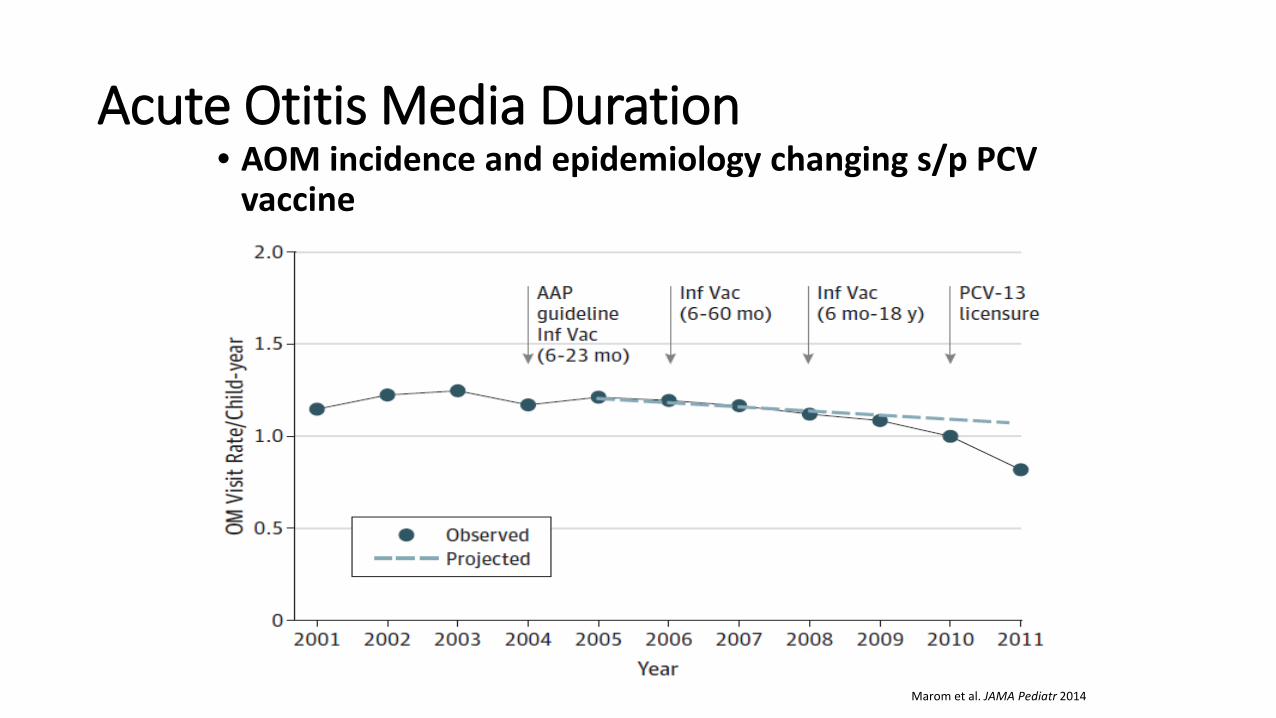
Acute Otitis Media Duration • AOM incidence and epidemiology changing s/p PCV
vaccine
Marom et al. JAMA Pediatr 2014
Summary • Opportunities remain to determine optimal length
of therapy for many infections • Thoughtfully consider the patient’s response to
therapy • “Return for Re-evaluation” vs. “Finish the Whole
Bottle” • Educate Everyone including Patients and Parents as
Antibiotics are a Shared Resource


PSV Pediatric Infectious Diseases
Dr. Daniel Keim Dr. Rebecca Levorson Dr. Katherine Moyer Dr. Andrew Nuibe Dr. Brittany Goldberg
Recommended