Embed Size (px)
Citation preview
1
Hodgkin Lymphomas: An Updatep
Roberto N. Miranda, M.D.Professor
UT MD Anderson Cancer Center
Huntington Beach, CaliforniaNovember 2nd, 2017
UT MD Anderson Cancer Center
Disclosures
• No conflict of interest: Nothing to disclose
• 2017 Revised 4th Edition WHO compatible
Hodgkin Lymphomas
• Classical Hodgkin Lymphoma (CHL): 90%– Nodular sclerosis– Mixed cellularity– Lymphocyte rich– Lymphocyte depleted
• Nodular Lymphocyte Predominant• Nodular Lymphocyte Predominant Hodgkin Lymphoma (NLPHL): 10%– A & B: Typical– C – F: Variants
Outline CHL• Clinical, histopathology, immunophenotype• Therapy
P th i• Pathogenesis– Cell of origin– Cell biology and molecular targets
• Loss of B-cell antigens• Proliferative advantage• Microenvironment• Microenvironment
• HL and immunodeficiency

2
CHL: Definition
• Nodal disease• Neoplastic cells are a minority in the
infiltrate (< 10%)• Majority of the cells in infiltrate are reactive
– Small lymphocytes, eosinophils, neutrophils, histiocytes plasma cells and fibroblastshistiocytes, plasma cells, and fibroblasts
WHO 2008Revised WHO 2017
CHL: Neoplastic Cells
Mononuclear: Hodgkin cell
Rare neoplastic cells: 0.1 – 10 %
Multilobated: Reed-Sternberg cell
Immunophenotype
CD30+ PAX5+
CD15+ CD45-
Other Useful Markers
EBER+ MUM1+EBER+ MUM1+
CD79- OCT2-

3
Background Cells
CD4
Subtypes
• Nodular sclerosis (NS) 66%• Mixed cellularity (MC) 27%• Mixed cellularity (MC) 27%• Lymphocyte-rich (LR) 6%• Lymphocyte-depleted (LD) 1%
Differences:• Clinical features• Histopathology• EBV association
Nodular Sclerosis HL• Median age, 28 years
• No male predominance
• Stage II disease in most patients
– Mediastinal involvement in 80%
• B-symptoms in 40%
Nodular Sclerosis HL
4
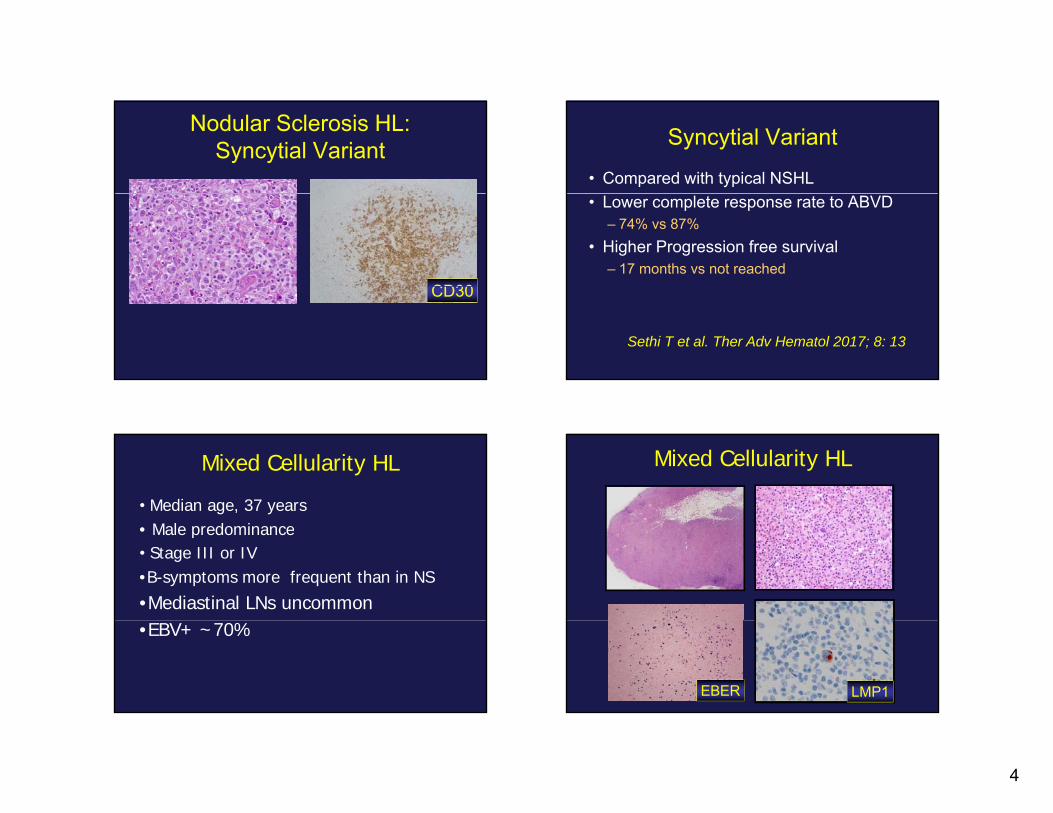
Nodular Sclerosis HL:Syncytial Variant
CD30CD30
Syncytial Variant
• Compared with typical NSHL• Lower complete response rate to ABVD
– 74% vs 87%• Higher Progression free survival
– 17 months vs not reached
Sethi T et al. Ther Adv Hematol 2017; 8: 13
Mixed Cellularity HL
• Median age, 37 years• Male predominance• Male predominance• Stage III or IV•B-symptoms more frequent than in NS
•Mediastinal LNs uncommon•EBV+ ~70%
Mixed Cellularity HL
LMP1EBER

5
Lymphocyte-rich HLNodular >> Diffuse Lymphocyte-Rich HL
Nodular pattern
CD30CD20
Lymphocyte-Depleted HL
• Advanced age• B-symptoms (80%)• Stage III or IV disease
– Extensive subdiaphragmatic disease– Abdominal LNs
M t i f f HL• Most aggressive form of HL• Very rare
Lymphocyte Depleted HL
• Diffuse fibrosis: Fibroblastic proliferation• Reticular: Abundant HRS cells

6
HL: Therapy
• Chemotherapy (ABVD or BEACOPP) + R di ti St d d f i USARadiation: Standard of care in USA– 90% 5-y OS– 60% 5-y FFS
• Chemotherapy alone for early stage HL
Nat Oncol 2008; 5:543
CHL: Prognosis
• Current therapy has made HL curable in th j it fthe majority of cases
• Histologic subtype is currently less relevant for prognosis
• Combined pathologic, laboratory, clinical stage appear more important thanstage appear more important than histologic subtype, and determine mode of therapy
Secondary MDS/AML in German GHSG Trials
• N= 11,805• 86 (0.72% developed MDS/AML)
– Early stages: 6• < 4 cycles
– Intermediate stage: 18– Advanced stage: 62Advanced stage: 62
• > 4 cycles
Eichenauer, Blood 2010
CHL Therapy
• Stanford V– Lower cumulative doses of chemotherapy
(adriamycin or bleomycin) to reduce risks of• Acute leukemia, MDS• Cardiopulmonary toxicity
– Lessen volume and dose of Radiation to d i k freduce risks of
• Second cancers• Cardiovascular toxicity

7
CHL Therapy
• Challenges for the future– Risk assessment to decrease secondary
toxicity– Hope in targeted therapy
Targeted Therapy:Vedotin Brentuximab (Anti-CD30)• Auristatin is bound to anti-CD30Auristatin is bound to anti CD30
• Potent anti-tubulin (vincristine like) arrests G2-M phase and triggers apoptosis
• FDA-approved for relapsed and refractory CHL
• Studies underway for other CD30+ ylymphomas of B- or T-cell lineage
Exp Op Inv Drugs 2011; 20: 141Berger et al. Crit Rev Oncol/Hem 2017Viviani et al. Tumori 2017; 103: 101
Pathogenesis of HL
• Nature of the malignant cell– B-cell, very abnormal, pre-apoptotic
• Many reactive cells– HRS cells secrete cytokines that attract
inflammatory cells: IL-4, IL-5, TNF-α, GM-CSF
Cell Biology of HRS Cells
8
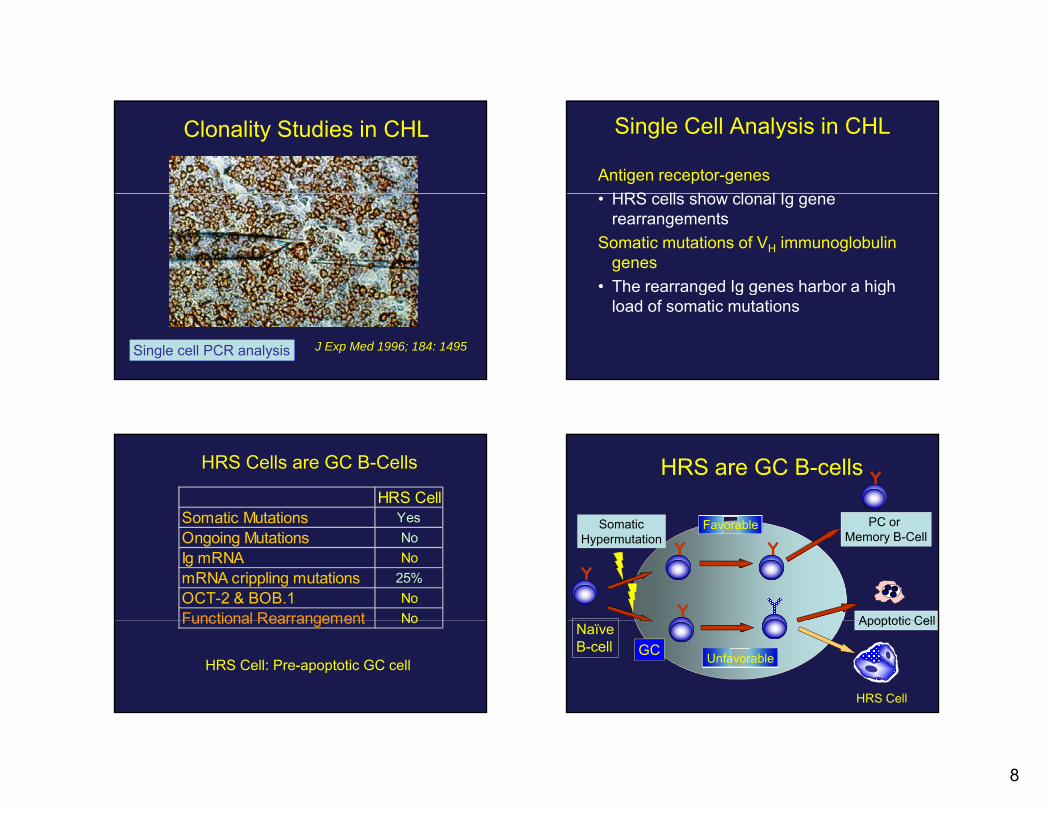
Clonality Studies in CHL
J Exp Med 1996; 184: 1495Single cell PCR analysis
Single Cell Analysis in CHL
Antigen receptor-genesHRS ll h l l I• HRS cells show clonal Ig gene rearrangements
Somatic mutations of VH immunoglobulin genes
• The rearranged Ig genes harbor a high• The rearranged Ig genes harbor a high load of somatic mutations
HRS Cells are GC B-Cells
HRS CellSomatic Mutations YesOngoing Mutations NoIg mRNA NomRNA crippling mutations 25%OCT-2 & BOB.1 NoFunctional Rearrangement NoFunctional Rearrangement No
HRS Cell: Pre-apoptotic GC cell
HRS are GC B-cells
Somatic Favorable PC or SomaticHypermutation
FavorableMemory B-Cell
Apoptotic CellNaïveB-cell
Unfavorable
Apoptotic Cell
HRS Cell
GC

9
What is the cause of B-cell Downregulation in CHL?
Leukemia 2008; 22: 1587Nat Immunol 2006; 7:207
CD20 (-) Pax-5 dim (+)
Downregulation of B-cell genes CD19, CD20 and CD79a
• Aberrant expression of Id2 and ABF1Aberrant expression of Id2 and ABF1– Inactivate E2A (Early B factor)
• Notch-1 antagonizes B-cell transcription factors E2A and EBF(early B-cell factor)(early B cell factor)
Leukemia 2008; 22: 1587Nat Immunol 2006; 7:207
B-cell Downregulation in HL
ABF1
PAX5 OCT-2
PU.1
E2A
E2A
E2AABF1
Id2
NOTCH1
B-CELL GENES
Ann Rev Pathol Mech Dis 2009; 4: 151
BOB.1
NOTCH1
EBF
Does Reconstitution of BOB.1 and OCT-2 lead to Ig production?
• No• This finding suggests the presence of
other mechanisms such as: – Epigenetic changes: Inactive chromatin– Inhibition of transcription
Blood 2004; 104: 3326

10
Methylation: Epigenetic Silencing
• Loss of function as a mechanism of carcinogenesis, but without changing DNA sequence
• Results from aberrant methylation of promotersof genes in regions rich with CpG (Cytidine Guanidine dinucleotide)Guanidine dinucleotide)
Epigenetics in HL• Downregulation of B-cell transcription factors
BCMA– BCMA– LCK– SYK– TCL1
• Downregulation of B-cell genesCD19– CD19
– CD79a– Ig
Leukemia 2008; 22: 835
Hypomethylation in CHL
• In refractory CHL– Heavily treated
• Partial response to azacytidine (Hypomethylating agent)
Falchi et al. J Hematol Oncol 2016; 30: 132
Targeted Therapy in HL
Hi t d t l i hibit• Histone deacetylases inhibitors– Panobinostat: 86% response rate in ASCT
failures
Blood 2012; 119: 4017Am J Hematol 2012; 87: 277Exp Op Inv Drugs 2011; 20: 141
11
Consequences of Apoptosis and B-Cell Downregulation
• Cell death• However HRS cells survive
– Antiapoptosis• Extrinsic Pathway• Intrinsic Pathway
– Proliferation signals• NFkB
Canonical pathwayAlternative pathway
Hum Pathol 2007; 38:103
Proliferative advantage in CHL: Activation of NFκB pathway
• NFkB pathway may be a transformingNFkB pathway may be a transforming master in CHL– NFkB is a family of transcription factors
involved in activation and survival of immune cells
– Abnormally activated in HL• Other factors: JAK/STATs and AP1
Targeted Therapy in HL• NFkB Pathway
Arsenic containing compo nds– Arsenic-containing compounds• Target IKK and downregulate NFkB pathway
– Bortezomib: May be useful in combination
Blood 2012; 119: 4017Am J Hematol 2012; 87: 277Exp Op Inv Drugs 2011; 20: 141
The Microenvironment in HL

12
Role of the Microenvironment in HL
• Reactive cellular infiltrate– Favors neoplastic proliferation
• Cytokines, chemokines and members of the TNF receptor family– Foster a favorable environment around HRS
cellscells– Inhibit CD8 function
J Clin Oncol 2005; 23: 6379
PD1, PDL-1 and the Immune Checkpoint Inhibitors in CHL
• PD1 is normally expressed in effector T cells, b t i hibit d th h PDL 1/2 b APC llbut inhibited through PDL-1/2 by APC cells
• HRS cells express – PDL-1/CD274, PDL-2/CD273– JAK2 (JAK/STAT)
• Tumor cells overexpress PDL 1 to evade• Tumor cells overexpress PDL-1 to evade immune response
Viviani et al. Tumori 2017; 103: 101Ok & Young; J Hem Oncol 2017; 10: 103
Immune Checkpoint Inhibitors in HL• PDL-1 or PDL-2 increase due to gains and
amplification of 9p24.1• EBV can induce PDL-1 expression• Immune checkpoint inhibitors nivolumab and
pembrolizumab restore immune response– Block interaction of PD1 with PDL-1– FDA approved in 2016 for refractory HL
Green et al. Clin Cancer Res 2012; 18: 1611Ok & Young; J Hem Oncol 2017; 10: 103Jelinek T et al. Immunology 2017; 1
Role of EBV
LMP-1 EBV encoded RNA(EBER)
(Most sensitive test)
13
CHL: EBV• 70% in MC and LD CHL• 20% in NS CHL• EBV infected HRS
– Are monoclonal: Infection occurred before clonal expansion
– LMP1: Activation (~CD40)LMP2A: Rescue from apoptosis (~BCR)– LMP2A: Rescue from apoptosis (~BCR)
J Clin Pathol 2007; 60: 1342
Targeted Therapy for EBV• EBV
LMP2A specific c toto ic l mphoc tes– LMP2A-specific cytotoxic lymphocytes• Useful in relapsed EBV+ cases
• Microenvironment– Immunomodulators: Thalidomide,
lenalidomide
Exp Op Inv Drugs 2011; 20: 141
Cellular Changes and Possible Mechanisms
Feature MechanismB-cell Neoplasm Monoclonal IGH GRHRS Cell GC cell rescued from apoptosisCD45 (-) Inactivation of b2MAbsent Ig Absent OCT2, BOB.1, PU.1B-cell Downregulation NOTCH1, ID2Antiapoptosis c-FLIP, XIAP, LMP2AIncreased proliferation NFkBActivation: CD40 LMP1
Evolving ConceptEvolving Concept
HL and Immunodeficiency

14
HL and Immunodeficiency• CHL is variable
– Immunocompetent: NS > MC– Immunosuppressed: MC > NS– HIV: If CD4+:
0.2 x 109/L: HL<0.05 x 109/L: BL or DLBCL
• HL may regress in:y g– Patients with autoimmune diseases receiving
MTX, anti-TNF– Post-transplant LPD
• Decrease with reduction of immunosuppression
Case Discussion
• Adult patient with a history of rheumatoid arthritis
• Therapy with methotrexate and etanercept (anti-TNFα)
• Lymphadenopathy with B-symptomsy p p y y p
CD30 CD15
CD45EBER
15
• Other iatrogenic immunodeficiency-i t d LPD
WHO Entity:
associated LPD– Immunosuppression other than in transplant– MTX– Immunomodulators: Anti-TNFα
• Polymorphic to full-blown NHL or HLPolymorphic to full blown NHL or HL• 40% extranodal: GI, skin, liver, spleen
Nodular Lymphocyte Predominant Hodgkin Lymphoma
(NLPHL)( )
NLPHL
• Sites: Cervical, axillary, inguinal nodes• Mostly males in 4th and 5th decades• Rare in mediastinum, spleen and BM• Most patients present in stage I or II• 5 – 20 % present with stage III or IV• Natural history:
– Slow development– Frequent relapses, but rarely fatal
WHO, 2008
NLPHL• Nodular or nodular and diffuse pattern• Large cells: LP or “popcorn” cells• Contained within large nodular meshworks of
dendritic cells• LP cell is a B cell, CD20 in 100% of cases• Reactive background: mainly B lymphocytes• CD15 (-) / CD30 (-)CD15 ( ) / CD30 ( )
16
Histopathology
Nodules are larger than follicles of follicular lymphoma or follicular hyperplasia
Histopathology
LP cells surrounded by small lymphocytes
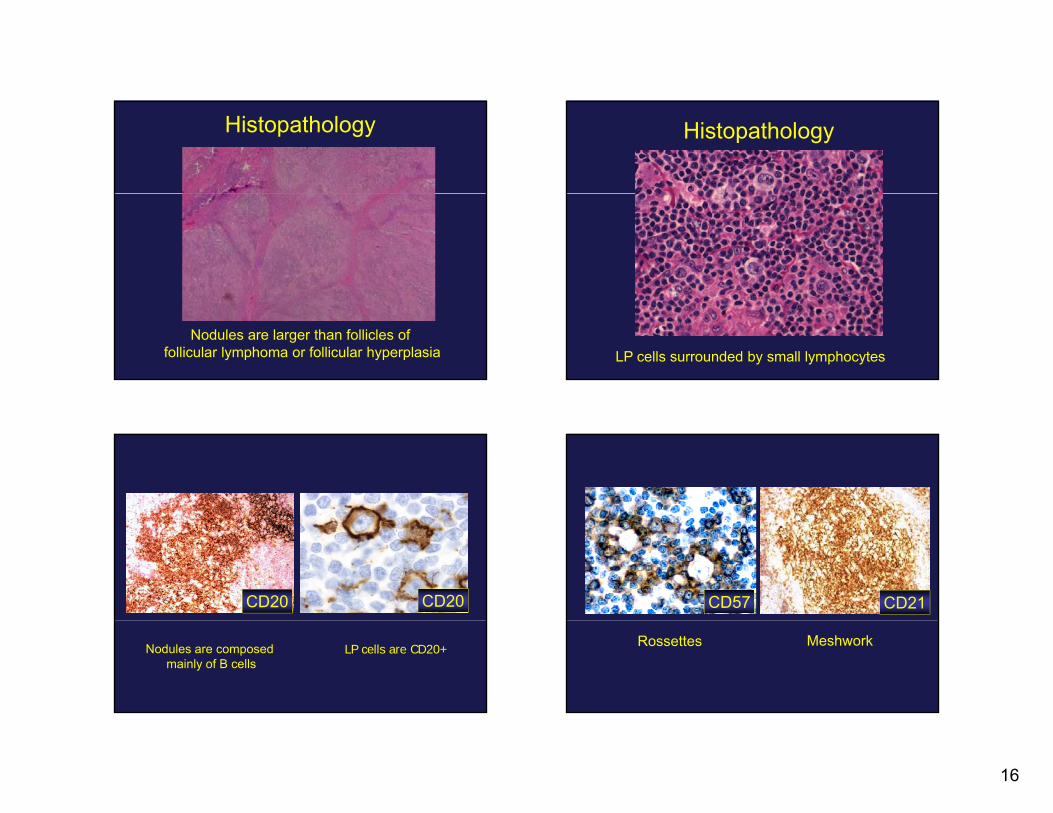
CD20 CD20
Nodules are composed mainly of B cells
LP cells are CD20+
CD57 CD21
Rossettes Meshwork

17
OCT-2 and BOB.1
• OCT-2 is a transcription factor that i d I th i b ti ti thinduces Ig synthesis by activating the promoter of the Ig genes in conjunction with BOB.1
• (+) 100 % in NLPHL– Stronger in LP cells > surrounding small B-Stronger in LP cells surrounding small B
cells• (+) 20 % in CHL
Blood 2001; 97: 496Eur J Haematol 2000; 30: 458 - 469
NLPHL: Variant Patterns• 137 biopsies
U d H&E CD3 CD20 d CD21• Used H&E, CD3, CD20 and CD21• 6 immunoarchitectural patterns
A. Nodular B-cell richB. SerpiginousC. Nodular with prominent extranodular LP cellsD. Nodular T-cell richE. Diffuse with increased T-cells: THRBCL-likeF. Diffuse with B-cell rich pattern
Fan et al, Am J Surg Pathol 2003: 27: 1346
A. Typical Nodular Pattern A. Typical Nodular B-cell Rich
B-cell nodules“Popcorn” cells
CD21 MeshworkInterfollicular T-cells
67 % of all cases

18
A. Typical Nodular B-cell Rich
CD20
B. “Serpiginous”: Interconnected Nodular
6 % of all cases
CD20
C. Nodular with prominent extranodular L&H cells
7 % of all cases
CD20
D. Nodular T-Cell Rich
CD3
12 % of all cases
19
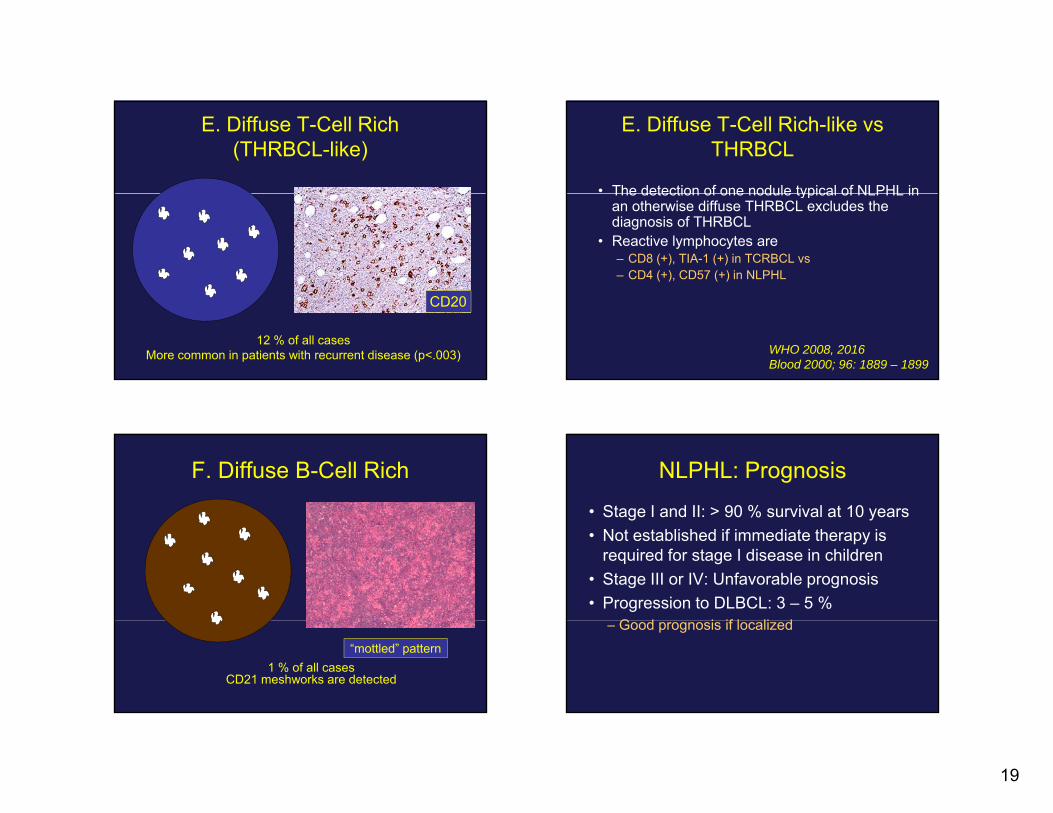
E. Diffuse T-Cell Rich (THRBCL-like)
12 % of all casesMore common in patients with recurrent disease (p<.003)
CD20
E. Diffuse T-Cell Rich-like vs THRBCL
• The detection of one nodule typical of NLPHL inThe detection of one nodule typical of NLPHL in an otherwise diffuse THRBCL excludes the diagnosis of THRBCL
• Reactive lymphocytes are – CD8 (+), TIA-1 (+) in TCRBCL vs – CD4 (+), CD57 (+) in NLPHL
WHO 2008, 2016Blood 2000; 96: 1889 – 1899
F. Diffuse B-Cell Rich
1 % of all casesCD21 meshworks are detected
“mottled” pattern
NLPHL: Prognosis
• Stage I and II: > 90 % survival at 10 years• Not established if immediate therapy is
required for stage I disease in children• Stage III or IV: Unfavorable prognosis• Progression to DLBCL: 3 – 5 %
G d i if l li d– Good prognosis if localized

20
Prognosis of NLPHL:Typical vs Variants
• German Hodgkin Study Group, 423 pts• Typical NLPHL: Patterns A and B (n= 308)• Variants: Patterns C, D, E and F (n= 105)• Adverse prognosis in variants
– > Advanced disease: 29.5% vs 14.6%% %– > Relapse rate: 18.1% vs 6%
Hartmann S et al. Blood 2013; 122: 4246
LRHL vs NLPHL
Overall Survival Failure-free Survival
Summary• HLs are heterogeneous B-cell neoplasms
HRS ll P t ti ll• HRS cell: Pre-apoptotic cell – Does not produce Ig and lacks many B cell genes– Rescued with anti-apoptotic mechanisms– Important role of targeted therapy
NLPHL ll A l d B ll• NLPHL cell: Ag selected B-cell– Produces Ig and has a full set of B cell functioning
genes– Predictive value of variants
















![Indolent T- and NK-cell lymphoproliferative disorders of ... · extranodal site of occurrence of non-Hodgkin lymphomas [1]. Most GI lymphomas are of B-cell lineage, and T-cell lymphomas](https://img.dokumen.tips/doc/110x75/5f93d293a1c10d3ed34c6b11/indolent-t-and-nk-cell-lymphoproliferative-disorders-of-extranodal-site-of.jpg)












