-
British Heart_Journal, I970, 32, 453-457.
Use of propranolol in atrial flutter
Douglas A. L. Watt, W. R. Livingstone, R. K. S. MacKay, and E.
N. ObinecheFrom Stobhill General Hospital, Glasgow N.I
Seven consecutive patients with atrial flutter are described, in
six of whom sinus rhythm wasrestored by a combination of digoxin
and propranolol. It is suggested that propranolol, used inthis way,
is a valuable addition to the available measures for the control of
this arrhythmia.
Atrial flutter is a notoriously difficult arrhyth-mia to control
by pharmacological means. Itis a rhythm in which alterations in
degree ofatrioventricular block may produce wild fluc-tuations in
ventricular rate. At the same time,it may be regarded as unstable
in nature, beingintermediate between sinus rhythm and
atrialfibrillation, and capable of being transformed,either by
therapeutic measures or spontane-ously, into one or other of these
relativelystable rhythms.
It is generally accepted that atrial flutter,with these inherent
potentially lethal proper-ties, is less desirable than either
controlledatrial fibrillation, or the ideal, sinus rhythm,and
various measures have been proposed toconvert it to one or other of
these.The traditional drugs for this purpose are
digitalis and quinidine, either alone or to-gether. Classically,
digitalis converts therhythm to atrial fibrillation, after
which,quinidine restores sinus rhythm.Most observers, while
accepting that this
course can occur, are disappointed by itsrarity. In fact three
possible outcomes aremore commonly met. First, digoxin may,
byitself, restore sinus rhythm. Secondly, itmay produce atrial
fibrillation which does notconvert to sinus rhythm with sub-toxic
dosesof quinidine. Thirdly, atrial flutter may bepersistent, and
fail to respond to drug treat-ment except by ventricular
slowing.
In contrast to this unpredictable and refrac-tory behaviour when
challenged by drugs,atrial flutter responds gratifyingly easily
todirect current (DC) countershock, so that incentres where this
facility is available, it isthe treatment of choice. There are,
however,still many situations in which DC counter-shock is not
available. Even where it is avail-able, however, it may happen that
atrial flutterhas been unrecognized and treated as atrialReceived
24 October I969.
fibrillation, or recognized and a preliminarytrial of digoxin
given. In this situation, DCshock may be dangerous unless digoxin
isdiscontinued for a period of days, a delaythat may be
undesirable.
It is in these contexts that an alternativepharmacological
approach to atrial flutterwould be desirable. The obvious drug
fortrial is the fl-adrenergic blocking agent,propranolol.
Reports of its use, however, have been uni-formly disappointing.
The manufacturers(Imperial Chemical Industries Ltd.) in theirI965
manual, quote complete control (i.e.restoration of sinus rhythm) in
only one of sixcases. Their later manual (December I967)does not
mention this arrhythmia.We have now treated seven successive
patients with atrial flutter, in six of whom acombination of
digoxin and propranolol hasbeen followed by restoration and
maintenanceof sinus rhythm.
Case reports
Case I A man of 54 years had sustained a myo-cardial infarction
three years previously, followedby persistent angina pectoris.
Hospital admissionfollowed a further antero-septal myocardial
in-farction. He was moderately hypotensive and inearly congestive
cardiac failure for which digoxinwas administered. On the ninth
day, while receiv-ing digoxin O025 mg. twice daily, he was notedto
have atrial flutter with an atrial rate of 300 perminute and 2: I
AV block. Carotid sinus massageproduced no significant slowing.
Propranolol, 3mg., was given intravenously without apparenteffect,
but when carotid massage was repeated,sinus rhythm was restored.
Oral propranolol,IO mg. 8-hourly, along with digoxin, was
con-tinued until four days later, when it was with-drawn because of
mild hypotension. Sinus rhythmremained unaltered over the next
month, whenhe was discharged from hospital.
on April 7, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.453 on 1 July 1970.
Dow
nloaded from
http://heart.bmj.com/
-
454 Watt, Livingstone, MacKay, and Obineche
_4At
-
Use of propranolol in atrial flutter 455
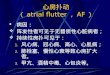
20 April '6 bfore propranolol 20 April '68 after propronolol 21
April '68
FIG. 2 Electrocardiogram, Case 4.
admitted to hospital in mild congestive cardiacfailure. Six
years previously he had experiencedpain in the arm, relieved by
glyceryl trinitrate,and attributed to myocardial ischaemia. After
ad-mission he was digitalized before a regular cardiacrhythm was
identified as atrial flutter with 3:Iblock. After one week of
digoxin, oral propranolol(io mg. thrice daily) was added to the
regimen,and after 48 hours he was found to have returnedto sinus
rhythm. Propranolol was then stopped,and sinus rhythm persisted. At
review one monthlater, there had been no recurrence of
atrialflutter.
Case 7 A man of 56 years was admitted to asurgical ward because
of swelling of ankles andabdomen, with hepatomegaly. He was found
tohave congestive cardiac failure with tachycardia,and was
digitalized. The electrocardiogramshowed atrial flutter. Two days
later, atrial flutterpersisted with stable 4: I block. Intravenous
pro-pranolol (3 mg.) produced no change, after whichoral
propranolol, 5 mg., then IO mg. eight-hourly, had no effect over
the next two days. Thedose of propranolol was raised to 20 mg.
eight-hourly for the next two days, by which time thecardiac rhythm
was atrial fibrillation with a ven-tricular rate of 64 a minute.
Both propranolol anddigoxin were withdrawn, but six hours
later,nodal bradycardia supervened which did notrespond to a total
of 3 mg. atropine, and whichpersisted for six hours before giving
way to sinusrhythm.On the following day he developed a
left-sided
hemiparesis which seemed likely to be due tocerebral embolism,
and which improved spon-taneously. Two further episodes of atrial
flutteroccurred during the next IO days, both
subsidingspontaneously. He developed bronchopneumoniaand
progressively deteriorated, dying on the 26thday after
admission.
DiscussionThese cases have been presented in detailbecause all
but one follow an almost identicalpattern of behaviour in the
presence of pro-pranolol. In each case the immediate effect
wasenhanced sensitivity to vagal stimulation andincrease in
atrioventricular block. In Case i,carotid massage restored sinus
rhythm at thisstage. In all the others, however, the conver-sion to
sinus rhythm occurred after an intervalof I2 to 48 hours.Had this
sequence of events been noted on
only one occasion, the association betweenpropranolol
administration and restoration ofnormal rhythm could well be
disputed. Itsoccurrence in the identical fashion on fivesuccessive
occasions appears reasonable evi-dence that there is a causal
relation betweentreatment and outcome.
It is well recognized that the effects ofpropranolol are a
mixture of fl-adrenergicblockade and 'quinidine-like' action, much
ofthe anti-arrhythmic potential being attribu-table to the latter
effect. It is also clear thatthese effects are not equally related
to thedosage of the drug, the anti-arrhythmic dose,for example, may
be homeopathic in com-parison with the anti-anginal dose. It
appearsfrom these reports that there is, in addition, adifferent
time factor involved, in that theP-adrenergic blocking, or
vagus-potentiating,effect appears immediately, manifesting itselfas
increased atrioventricular block, whereasthe quinidine-like effect
on ectopic atrialactivity, to which we attribute the restorationof
sinus rhythm, takes many hours to be mani-fest. Whether this is due
to delay in action,
FIG. 3 Electrocardiogram, Case 5.
30:) Auag.'bB before propronolol 31 Aug.'68 after propranolol
Sept.'68
on April 7, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.453 on 1 July 1970.
Dow
nloaded from
http://heart.bmj.com/
-
456 Watt, Livingstone, MacKay, and Obineche
or to cumulative effect, is, of course, notapparent in this
series, nor did we try theeffect of using larger doses of
propranolol tosee if they might be more rapidly effective.We are
wary of the use of large doses of pro-pranolol in the presence of
digoxin (Watt,I968).
It is apparent that most authors have re-garded conversion of
atrial flutter to sinusrhythm with propranolol as an
exceptionaloccurrence. It is also clear that in almost allof the
successful occurrences, propranololhas been used in combination
with other anti-arrhythmic agents, usually digitalis
(Table).Rowlands, Howitt, and Markman (I965)
comment that in none of their cases did pro-pranolol influence
the atrial rate in atrialflutter though the ventricular rate was
slowed.This, however, was a study of response to asingle dose of
propranolol. Harrison, Griffin,and Fiene (I965) restored sinus
rhythm inone patient of 5 years with atrial flutter. Thispatient
was already digitalized. Cherchi et al.(I966) showed increased AV
block, but nocorrection of the arrhythmia in a group ofpatients
treated both orally and intravenously.Nielsen and J0rgensen (I966)
restored sinusrhythm in one patient after a week of com-bined
digitalis and propranolol. Likewise,Luria, Adelson, and Miller
(I966) report onepatient with paroxysmal flutter in whom treat-ment
with digitalis and propranolol restoredsinus rhythm.
Gianelly, Griffin, and Harrison (i967) con-verted atrial flutter
to sinus rhythm in one outof seven patients. Wolfson and his
colleagues(I967) restored sinus rhythm in one patientwith
post-operative flutter by combined digi-talis and
propranolol.McLean, Stoughton, and Kagey (I967) suc-
ceeded only in reducing the ventricular rate
in two patients with atrial flutter. Irons, Ginn,and Orgain
(I967) had no conversions to sinusrhythm among six patients with
flutter treatedwith propranolol, though three showed ven-tricular
slowing.
Reynolds and VanderArk (I967) describesuccessful treatment of
two patients withparoxysmal atrial flutter with a combinationof
quinidine and propranolol.Sloman and Stannard (i967) record one
success with propranolol where digoxin failedto control atrial
flutter.We believe that, in combination with dig-
oxin, propranolol is an effective drug in themanagement of
atrial flutter, both chronic andparoxysmal.
It lacks the speed and effectiveness ofdirect current
countershock which must re-main the most satisfactory procedure in
atrialflutter. Where, however, this facility is notavailable, or
where circumstances render itsuse undesirable, we feel that
pre-treatmentwith digitalis followed by propranolol con-version may
well be the treatment of choice.
We are grateful to Dr. J. B. Rennie and Dr. J. L.Markson for
perm ssion to treat patients undertheir care.
ReferencesCherchi, A., Lixi, M., Mazza, B., and Camoglio, E.
(I966). Prime osservazioni cliniche sull'azione anti-aritmica di
un nuovo bloccante dei recettori beta:il propranololo. Minerva
Medica (Parte sci.), 57,317.
Gianelly, R., Griffin, J. R., and Harrison, D. C.
(1967).Propranolol in the treatment and prevention ofcardiac
arrhythmias. Annals of Internal Medicine,66, 667.
Harrison, D. C., Griffin, J. R., and Fiene, T. J. (I965).Effects
of beta-adrenergic blockade with proprano-lol in patients with
atrial arrhythmias. New England3'ournal of Medicine, 273, 4IO.
TABLE Effect of combined therapy with propranolol on response of
atrial flutter
Propranolol alone Propranolol+ quinidine Propranolol+ digoxinNo.
No. No. restored No. No. No. restored No. No. No. restored
Authors improved sinus rhythm improved sinus rhythm improved
sinus rhythm
Harrison et al. (I965) I I - - 4 2 ICherchi et al. (966) 2
2Nielsen and J0rgensen (I966) 4 3 - I - ILuria et al. (I966) - I
IGianelly et al. (I967) 5 5 - - 2 I IWolfson et al. (I967) I I - I
IMcLean et al. (I967) 3 2Irons et al. (I967) 6 3Reynolds and
VanderArk (I967) - 2 2 -Sloman and Stannard (I967) - I ICurrent
series - - 7 6
Total 22 I7 0 2 0 2 I7 3 12
on April 7, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.453 on 1 July 1970.
Dow
nloaded from
http://heart.bmj.com/
-
Use of propranolol in atrial flutter 457
Irons, G. V., Ginn, W. N., and Orgain, E. S. (I967).Use of a
beta adrenergic receptor blocking agent(propranolol) in the
treatment of cardiac arrhyth-mias. American journal of Medicine,
43, I6I.
Luria, M. H., Adelson, E. I., and Miller, A. J. (I966).Acute and
chronic effects of an adrenergic beta-receptor blocking agent
(propranolol) in treatmentof cardiac arrhythmias. Circulation, 34,
767.
McLean, C. E., Stoughton, P. V., and Kagey, K. S.(I967).
Experiences with beta-adrenergic blockade.Vascular Surgery, i,
io8.
Nielsen, B. L., and J0rgensen, F. S. (I966). Pro-pranolol
('Inderal') in cardiac arrhythmias. ActaMedica Scandinavica, I8o,
63I.
Reynolds, E. W., and VanderArk, C. R. (1967). Treat-ment of
quinidine-resistant arrhythmias with the
combined use of quinidine and propranolol.Circulation, 36,
Suppl. 2, p. 22I.
Rowlands, D. J., Howitt, G., and Markman, P. (I965).Propranolol
('Inderal') in disturbances of cardiacrhythm. British Medical
Journal, i, 89I.
Sloman, G., and Stannard, M. (I967). Beta-adrenergicblockade and
cardiac arrhythmias. British MedicalJ7ournal, 4, 5o8.
Watt, D. A. L. (I968). Sensitivity to propranolol afterdigoxin
intoxication. British Medical Journal, 3,413.
Wolfson, S., Herman, M. V., Sullivan, J. M., andGorlin, R.
(I967). Conversion of atrial fibrillationand flutter by
propranolol. British Heart J7ournal,29, 305.
on April 7, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.32.4.453 on 1 July 1970.
Dow
nloaded from
http://heart.bmj.com/