-
7/24/2019 Goiter journal 1.docx
1/3
BackgroundIn 1656, Thomas Wharton described the distinct nature
of what he termed the thyroid gland,
distinguishing it from the larynx, as this structure had been
considered a laryngeal gland from the
time of Andreas Vesalius in the 16th century. It was nearly !!
more years before the function ofthe thyroid was elucidated. The
normal adult thyroid gland weighs 1!"5 g and has lobes
connected by an isthmus. #early 5!$ of thyroid glands exhibit a
%yramidal lobe arising from thecenter of the isthmus.
&ongitudinal dimensions of the lobes of the thyroid range u% to
5 cm, as
shown in the image below.
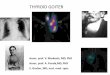
Thyroid nuclear scan of a %atient with a euthyroid goitershowing
different %ro'ections.
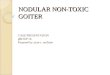
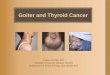
A goiter is an enlarged thyroid gland, and it may be diffuse or
nodular. A goiter may extend into
the retrosternal s%ace, with or without substantial anterior
enlargement. (ecause of the anatomic
relationshi% of the thyroid gland to the trachea, larynx,
su%erior and inferior laryngeal ner)es,and eso%hagus, abnormal
growth may cause a )ariety of com%ressi)e syndromes. Thyroid
function may be normal *nontoxic goiter+, o)eracti)e *toxic
goiter+, or underacti)e *hy%othyroid
goiter+.
Pathophysiology
The thyroid gland is controlled by thyroid"stimulating hormone
*T- also /nown as
thyrotro%in+, secreted from the %ituitary gland, which in turn
is influenced by the thyrotro%in"releasing hormone *T0-+ from the
hy%othalamus. T- %ermits growth, cellular differentiation,
and thyroid hormone %roduction and secretion by the thyroid
gland. Thyrotro%in acts on T-
rece%tors located on the thyroid gland. Thyroid hormones are
synthesied from iodination oftyrosine. The iodine is trans%orted
from %lasma into the thyroid cell )ia a sodium"iodide
sym%orter. This is an acti)e %rocess resulting in an
intracellular iodine le)el exceeding ! times
the %lasma iodine le)el. This iodine trans%ort acti)ity is
controlled by T-.213 erum thyroid
-
7/24/2019 Goiter journal 1.docx
2/3
hormones le)othyroxine and triiodothyronine feed bac/ to the
%ituitary, regulating T-
%roduction. Interference with this T0-"T- thyroid hormone axis
causes changes in the
function and structure of the thyroid gland. timulation of the
T- rece%tors of the thyroid byT-,T-"rece%tor antibodies, or T-
rece%tor agonists, such as chorionic gonadotro%in, may
result in a diffuse goiter. When a small grou% of thyroid cells,
inflammatory cells, or malignant
cells metastatic to the thyroid is in)ol)ed, a thyroid nodule
may de)elo%.
A deficiency in thyroid hormone synthesis or inta/e leads to
increased T- %roduction.Increased T- causes increased cellularity
and hy%er%lasia of the thyroid gland in an attem%t to
normalie thyroid hormone le)els. If this %rocess is sustained, a
goiter is established. 4auses of
thyroid hormone deficiency include inborn errors of thyroid
hormone synthesis, iodinedeficiency,23 and goitrogens.
A goiter may result from a number of T- rece%tor agonists. T-
rece%tor stimulators include
T- rece%tor antibodies, %ituitary resistance to thyroid hormone,
adenomas of the hy%othalamus
or %ituitary gland, and tumors %roducing human chorionic
gonadotro%in.
EpidemiologyFrequency
United States
Autopsy studies suggest a frequency of greater than 50% for
thyroid nodules; with high-resolutionultrasonography the !alue
approaches "0% of patients with nonthyroidal illness# $n the ickham
study fromthe &nited 'ingdom ()% of the population had a
goiter#*+, $n the ramingham study ultrasonography re!ealedthat +%
of men older than )0 years had thyroid nodules while +)% of women
aged ".-5/ years had thyroidnodules#*", $n the &nited tates
most goiters are due to autoimmune thyroiditis 1ie 2ashimoto
disease3#
4he incidence of thyroid cancer has een rising worldwide# 4he
reasons are unclear ut this trend may erelated to etter detection
and diagnostic methods#*5,
International
orldwide the most common cause of goiter is iodine
deficiency#*6, $t is estimated that goiters affect as many as600
million of the /00 million people who ha!e a diet deficient in
iodine#
$n a 7erman study )+5 people underwent ultrasonographic thyroid
screening as well as asal 42measurement during a pre!enti!e-health
checkup# *), 4hyroid nodules were detected in "+6 1)/%3 of
thepersons screened; in a pre!ious 7erman study ultrasonographic
screening of more than .0000 peopledetected thyroid nodules in ++%
of the normal population# 4he authors of the latter report
attriuted thisdifference to the fact that patients in their study
were screened using (+ 829 ultrasonographic scanners whichwere more
sensiti!e than the :#5 829 scanners used in the pre!ious study#
According to the in!estigators theirresults indicated that the
question of routine iodine supplementation requires renewed
attention#
Mortality/Morbidity
8ost goiters are enign causing only cosmetic disfigurement#
8oridity or mortality may result fromcompression of surrounding
structures thyroid cancer hyperthyroidism or hypothyroidism#
Race
o racial predilection e
-
7/24/2019 Goiter journal 1.docx
3/3
$n the ickham study 6)% of women had a goiter compared to :% of
men#*+,
4hyroid nodules are less frequent in men than in women ut when
found they are more likely to e
malignant#
Age
4he frequency of goiters decreases with ad!ancing age# 4he
decrease in frequency differs from the incidenceof thyroid nodules
which increases with ad!ancing age#
James R Mulinda, MD, FAC>onsulting taff ?epartment of
Endocrinology Endocrinology Associates $nc
Source:
http://emedicine.medscape.com/article/120034-overview#showall