Embed Size (px)
Citation preview

Henry Ford Health SystemHenry Ford Health System Scholarly Commons
Case Reports Medical Education Research Forum 2019
5-2019
Gluteus Maximus Transfer for Trendelenburg GaitFollowing Total Hip ArthroplastyKaren NelsonHenry Ford Health System
Melissa MartinezHenry Ford Health System
Fremont ScottHenry Ford Health System
JJ Goldman
K Chaiyasate
Follow this and additional works at: https://scholarlycommons.henryford.com/merf2019caserpt
This Poster is brought to you for free and open access by the Medical Education Research Forum 2019 at Henry Ford Health System ScholarlyCommons. It has been accepted for inclusion in Case Reports by an authorized administrator of Henry Ford Health System Scholarly Commons. Formore information, please contact [email protected].
Recommended CitationNelson, Karen; Martinez, Melissa; Scott, Fremont; Goldman, JJ; and Chaiyasate, K, "Gluteus Maximus Transfer for TrendelenburgGait Following Total Hip Arthroplasty" (2019). Case Reports. 93.https://scholarlycommons.henryford.com/merf2019caserpt/93

Abstract Post Operative Follow UpIntroduction: Lateral approach total hip arthroplasty (THA) accounts for 12% of the total hip reconstructions performed annually. Approximately 4.4% of these patients experience postoperative rupture of the gluteus medius (routinely taken down and repaired during the surgery), resulting in loss of abduction and a contralateral hip drop (Trendelenburg gait). While functional muscle transfer has been proposed for use at the time of implant revision surgery, to our knowledge, no report exists of dynamic repair in patients with a functioning implant and early muscle rupture. Case: A 47-year-old female presented to clinic with MRI proven rupture of the gluteus medius and failed secondary repair. The patient noted significant discomfort with activities of daily living. A review of the literature was performed, and joint decision-making was utilized to consent for a superior gluteus maximus transfer. An interdisciplinary team (plastic and orthopedic) performed the surgery with modifications to a technique previously described. Results: Surgery was performed in 2 hours and 49 minutes. Postoperative course was uneventful. At 4 months post-op, the patient has a significant increase in abduction strength. The patient is able to stand without hip drop and continues extensive physical therapy for balance and gait given the 2 years of atrophy and maladaptation. The patient reports improvement in quality of life, and physical therapy notes indicate improvement across all gait, stance, and strength studies. Conclusion: The superior gluteus maximus muscle transfer for gluteus medius rupture is a viable option in patients with Trendelenburg gait, warranting further clinical study.
Introduction
Conclusion & DiscussionAbductor deficiency can be secondary to repair failure following total hip arthroplasty or from severe metallosis, damage to the superior gluteal nerve, or attritional rupture of the abductor complex1. The Hardinge Direct Lateral approach or modified Watson Jones Anterolateral approach to total hip arthroplasty (THA) accounts for 12% of the total hip reconstructions performed annually3. Through this approach the gluteus medius and minimus tendons are taken down and repaired. Approximately 4.4% of these patients experience postoperative rupture of the gluteus medius, resulting in loss of abduction and a contralateral hip drop (Trendelenburg gait). Other complications include pain, feeling of instability, weakness in abduction, and possible increased rate of dislocation7. While functional muscle transfer has been proposed for use at the time of implant revision surgery, to our knowledge, no report exists of dynamic repair in patients with a functioning implant and early muscle rupture. !
Case Report
References1. Davies H, Zhaeetan S, Tavakkolizadeh A, Janes G. Surgical repair of chronic tears of the hip abductor mechanism. Hip Int. 2009;19:372–376. !!2. Bird PA, Oakley SP, Shnier R, Kirkham BW. Prospective evaluation of magnetic resonance imaging and physical examination findings in patients with greater trochanteric pain syndrome. Arthritis Rheum. 2001;44:2138–2145. !!3. Baker AS, Bitounis VC. Abductor function after total hip replacement. An electromyographic and clinical review. J Bone Joint Surg Br. 1989;71:47–50. !!4. Daly PJ, Morrey BF. Operative correction of an unstable total hip arthroplasty. J Bone Joint Surg Am. 1992;74:1334–1343. !!5. Fehm MN, Huddleston JI, Burke DW, Geller JA, Malchau H. Repair of a deficient abductor mechanism with Achilles tendon allograft after total hip replacement. J Bone Joint Surg Am. 2010;92:2305–2311. !!6. Kohl S, Evangelopoulos DS, Siebenrock KA, Beck M. Hip abductor defect repair by means of a vastus lateralis muscle shift. J Arthroplasty. 2012;27:625–629. !!7. Whiteside LA. Surgical technique: Transfer of the anterior portion of the gluteus maximus muscle for abductor deficiency of the hip. Clin Orthop Relat Res. 2012;470:503–510. !!8. Whiteside LA. Surgical technique: Gluteus maximus and tensor fascia lata transfer for primary deficiency of the abductors of the hip. Clin Orthop Relat Res. 2014;472:645–653.
A 47 year old female patient underwent left total hip arthroplasty for primary osteoarthritis through an anterolateral approach. Her past medical history does include systemic arterial hypertension, hypercholesterolemia, and stroke without residual deficits. Five months after her initial surgery, and completion of her 12 weeks of routine physical therapy, she had persistent weakness and abnormal gait. She underwent MRI which revealed rupture of the gluteus medius and minimus. She then underwent Left gluteus medius repair with all-suture bone anchors. She again continued to have weakness in hip abduction with a trendelenburg gait even after completing 8 sessions of physical therapy. She was sent to another orthopedic surgeon for a second opinion and it was recommended that she undergo a functional muscle transfer versus a tendon allograft reconstruction. At that time she had an EMG which revealed normal neurologic function. A review of the literature was performed, and joint decision-making was utilized to consent for a superior gluteus maximus transfer. An interdisciplinary team (plastic and orthopedic surgery) performed the surgery with a modified technique previously described by Whiteside for use at the time of hip revision. !The patient was placed in a lateral decubitus position and an incsion was carried out through the prior incision and extended superiorly in a curvilinear fashion towards the PSIS. The gluteus maximus muscle and tensor fascia lata with the iliotibial band were exposed. Approximately half of the gluteus maximus muscle was split in line with it’s fibers and carried down to the fascia lata which was split in line with its fibers. The gluteus maximus flap was elevated to produce a triangular shaped flap. It was noted at this time that there was no deficiency of the posterior short external rotators or capsule and the second limb of the flap was not dissected. The greater trochanter was prepped with a rasp down to bleeding bone utilizing the proximal 4cm of the greater trochanter. Next the proximal vastus laterals was dissected in a T shape, subperiosteally down to bone. 8 bone tunnels were drilled into the greater trochanter. The flap was laid into the groove and a heavy non absorbable suture was used to anchor the flap to bone. This was tensioned with the hip in 15 degrees of abduction. The very distal end of the flap was sewn into the vastus laterals and the limbs were oversewn. A drain was left in place for 1 week. !Surgery was performed in 2 hours and 49 minutes. Postoperative course was uneventful. Post operatively the patient was placed in a hip abduction orthosis. She was toe touch weight bearing for 6 weeks with progressive weight bearing since then. She was made full weight bearing at 3 months without the abduction orthosis. She has continued physical therapy for strengthening. At 4 months post-op, the patient has a significant increase in abduction strength (0-1 to 2-3). The patient is able to stand without hip drop but continues to require extensive physical therapy for balance and gait given the 2 years of atrophy and mal-adaptation. She continues to ambulate with a cane. The patient reports improvement in quality of life, and physical therapy notes indicate improvement across all gait, stance, and strength studies.
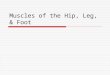
Figure 4. Intraoperative image demonstrating the triangular shaped anterior gluteus maximus muscle flap. The image on the right is the final position of the tendon over the greater trochanter.
Lateral approach to total hip arthroplasty is a commonly used approach for joint replacement. However, some patients may have abductor deficiency with continued lateral hip pain with the most serious complication being hip instability. This complication increases with each hip surgery. Injury to the superior gluteal nerve must be evaluated before proceeding with any surgical intervention. There are several repair techniques described in the literature, but when those options have been exhausted, there are very few procedures to address trendelenburg gait. There were two techniques specifically reviewed prior to this case. The first was described by Fehm et al5, in which an achilles tendon allograft was used to repair the abductor mechanism. The second option was originally described by Whiteside7 for a gluteus maximus muscle transfer where the anterior fibers of the gluteus maximus are transferred to the greater trochanter to recreate the gluteus medius and minims complex. In our technique we chose to transfer the anterior fibers of the gluteus maximus with a sleeve of the ilitobial band and anchoring the tissue into the greater trochanter. Whiteside described a second flap to stabilize the posterior joint capsule and short external rotators. This was not necessary because our patient had intact posterior complex. There are several limitations to the study. This is a single case report with short follow up. There is also no comparative group. However, despite all the limitations, we feel that this is a viable technique for patients with a trendelenburg gait following total hip arthroplasty that affects their quality of life. !Conclusion: The superior gluteus maximus muscle transfer for gluteus medius rupture is a viable option in patients with Trendelenburg gait, warranting further clinical study.
Gluteus Maximus Transfer for Trendelenburg Gait Following Total Hip Arthroplasty
MM Martinez, KE Nelson DO, JJ Goldman MD, FL Scott DO, K Chaiyasate MD Henry Ford Health System, Clinton Township, Michigan
Figure 5. Intraoperative image demonstrating the final suture into the greater trochanter with closure of the muscle.
Figure 3. Pictured on the right is an Intraoperative image demonstrating rupture of the gluteus medius and minimus.
Figure 2. Pictured on the left is an MRI of the Left hip demonstrating complete rupture of the gluteus medius.
Figure 1. Pictured on the left are preoperative radiographs of the left hip demonstrating severe degenerative osteoarthritis. Pictured on the right are immediate post operative radiographs following left total hip arthroplasty.
Figure 6. 4 month followup image without a hip drop.