Embed Size (px)
Citation preview

n Feature Article
MAY/JUNE 2017 | Volume 40 • Number 3
Chronic soft tissue deficiencies of the abductor musculature, poste-rior capsule, and fascia encoun-
tered during revision total hip arthroplasty (THA) remain a significant challenge. Most studies of soft tissue deficiency in
revision THA have focused on reconstruc-tion of chronic abductor deficiency.1-11 In limited series, the use of allograft tis-sue for abductor reconstruction, includ-ing Achilles tendon allograft or extensor mechanism allograft, has been success-ful.4,11 Muscle transfers, including the vastus lateralis and gluteus maximus, also have been described and avoid the risks of disease transfer, the requirement for stor-age, and the cost of allograft tissue.1,2,4-7
Gluteus Maximus Advancement Flap Procedure for Reconstruction of Posterior Soft Tissue Deficiency in Revision Total Hip ArthroplastyBenjamin F. RicciaRdi, md; PeteR W. HendeRson, md, mBa; alexandeR s. mclaWHoRn, md, mBa; GeoFFRey H. WestRicH, md; matHias P. BostRom, md; lloyd B. Gayle, md
The authors are from the Adult Reconstruc-tion and Joint Replacement Service (BFR, ASM, GHW, MPB), Hospital for Special Surgery, and the Division of Plastic and Reconstructive Sur-gery (PWH), Department of Surgery, Weill Cor-nell Medical College, New York; and the Division of Plastic Surgery (LBG), Department of Surgery, Maimonides Medical Center, Brooklyn, New York.
Drs Ricciardi, Henderson, McLawhorn, and Gayle have no relevant financial relationships to disclose. Dr Westrich is a paid consultant for Stryker, Exactech, DJO Orthopedics, and Mallinckrodt Company. Dr Bostrom is a paid con-sultant for Smith & Nephew.
Correspondence should be addressed to: Benjamin F. Ricciardi, MD, Adult Reconstruction and Joint Replacement Service, Hospital for Spe-cial Surgery, 535 E 70th St, New York, NY 10021 ([email protected]).
Received: November 4, 2016; Accepted: Feb-ruary 6, 2017.
doi: 10.3928/01477447-20170308-06
The current study describes the surgical technique and early outcomes of a gluteus maximus advancement flap procedure for the treatment of posterior soft tissue insufficiency among patients with complex revision total hip arthroplasty. This retrospective case series was conducted with a prospective, single-institu-tion arthroplasty registry. Patients who underwent a gluteus maximus advance-ment flap procedure in the setting of revision total hip arthroplasty between January 2012 and January 2016 were eligible for inclusion (N=7). Primary in-dications for the gluteus maximus flap procedure included periprosthetic infec-tion with persistent wound breakdown (n=4), persistent symptomatic aseptic pseudotumor in the setting of adverse local tissue reaction after unsuccessful operative debridement (n=2), and abductor insufficiency with recurrent hip in-stability after unsuccessful placement of a constrained liner (n=1). All patients who underwent a gluteus maximus advancement flap procedure for chronic periprosthetic infection or adverse local tissue reaction had healing of the wound and were infection-free at the last follow-up. In the early postoperative period, 2 patients had recurrent wound infection that required flap elevation. The patients remained infection-free after the subsequent procedure. No patient had repeat instability, and no complications of flap necrosis or nerve palsy oc-curred. The gluteus maximus advancement flap procedure provides a diverse range of soft tissue coverage options for patients with recalcitrant periprosthetic joint infection, adverse local tissue reaction with pseudotumor, or recurrent in-stability. [Orthopedics. 2017; 40(3):e495-e500.]
abstract
e495

Copyright © SLACK inCorporAted
n Feature Article
Local transfer of the vastus lateralis mus-cle on its vascular pedicle to the intact abductors proximally has been described in distal irreparable abductor tendon tears.4-7 Another promising reconstructive technique is the gluteus maximus muscle transfer as described by Whiteside.1,2
Abductor deficiency is a challenging aspect of revision arthroplasty. Posterior capsular and fascial deficiencies also can adversely affect revision outcomes, and few studies have focused on these com-plex problems.8-10,12-14 One technique that has been described uses an Achilles allograft sling around the greater trochan-ter to augment the posterior capsule and provides compressive forces across the hip articulation in at-risk leg positions for recurrent posterior instability.8,10 Chronic infection and pseudotumors as a result of adverse local tissue reaction also create significant soft tissue deficiency, and fail-ure to address the soft tissues can lead to chronic seroma or hematoma cavities with fluid accumulation, impaired eradication of infection, and incisional breakdown. The ideal procedure for soft tissue recon-struction in revision THA would provide
soft tissue coverage of the proximal femur in the setting of fascial defects, reduce dead space for fluid accumulation for patients with seroma or hematoma, and reconstitute the posterior soft tissue enve-lope, including the abductor musculature or posterior capsule.
The current study described the sur-gical technique and early outcomes of the gluteus maximus advancement flap procedure in the setting of posterior soft tissue insufficiency in complex revision THA. To the authors’ knowledge, this is the first study to illustrate the versatility of this muscle transfer technique in the setting of fascial insufficiency secondary to persistent periprosthetic joint infection or adverse local tissue reaction, seroma or hematoma cavity, and posterior capsular insufficiency.
Materials and MethodsThe current report describes a ret-
rospective case series that used a pro-spective, single-institution arthroplasty registry. Patients undergoing a gluteus maximus advancement flap procedure in the setting of previous revision THA be-
tween January 2012 and January 2016 were eligible for study inclusion (N=7) (Table). Mean follow-up was 17 months (range, 6-37 months). All gluteus maxi-mus flap procedures were performed by a single surgeon (L.B.G.) with fellowship training in plastic and microvascular sur-gery.
All gluteus maximus flap procedures were planned before the surgical date, and no procedures were emergent. Primary indications for the gluteus maximus flap procedure included periprosthetic infec-tion with persistent wound breakdown in the setting of a seroma or hematoma cav-ity (n=4); persistent symptomatic aseptic pseudotumor in the setting of adverse lo-cal tissue reaction with previous unsuc-cessful operative debridement, with or without abductor insufficiency (n=2); and abductor insufficiency with recurrent hip instability after unsuccessful placement of a constrained liner (n=1). Preoperative diagnoses included chronic periprosthetic infection (n=4), adverse local tissue reac-tion with pseudotumor (n=3; 1 also had chronic periprosthetic infection), place-ment of a constrained liner for recurrent
Table
Patient CharacteristicsPatient No./Sex/Age, y
Body Mass Index, kg/m2 Diagnosis Surgical Indication
No. of Previous Revisions Concomitant Revision
1/M/58 29 Adverse local tissue reaction Chronic abductor insuffi-ciency
1 No; previous revision of both components
2/M/66 29 Adverse local tissue reaction Persistent pseudotumor 1 Yes; head and liner exchange
3/M/67 37 Adverse local tissue reaction and chronic prosthetic joint
infection
Fascial defect and wound breakdown
2 No; irrigation and debridement
4/M/58 30 Chronic prosthetic joint infection
Fascial defect and wound breakdown
8 Yes; spacer placement
5/F/58 34 Chronic prosthetic joint infection
Fascial defect 4 Yes; spacer placement
6/F/38 26 Chronic prosthetic joint infection
Wound breakdown 2 No; girdlestone
7/F/69 28 Recurrent dislocation Chronic abductor insuffi-ciency
5 Yes; femoral revision and liner exchange
Abbreviations: F, female; M, male.
e496

MAY/JUNE 2017 | Volume 40 • Number 3
n Feature Article
instability (n=2; 1 also had chronic peri-prosthetic infection), abductor deficiency with inability to abduct against gravity preoperatively (n=3; n=2 in the setting of adverse local tissue reaction), and peri-prosthetic fracture (n=1).
Periprosthetic Joint InfectionAll patients with chronic periprosthet-
ic infection (n=4) had persistent wound breakdown and drainage despite previous revision attempts before the gluteus maxi-mus flap procedure. In addition, 3 patients had immune disorders preoperatively (dermatomyositis on chronic steroids, n=1; lupus on chronic steroids and immu-nosuppressive medication, n=1; hepatitis C, n=1). The mean number of previous re-vision surgeries was 4 (range, 2-8). These included irrigation and debridement alone (8 cases, 4 patients), placement of an an-tibiotic spacer (3 cases, 3 patients), resec-tion arthroplasty (1 case, 1 patient), open reduction of spacer dislocation (1 case, 1 patient), placement of a constrained liner for recurrent instability (2 cases, 1 patient), aseptic revision THA with de-bridement (1 case, 1 patient). All patients had a polymicrobial infection. Organisms isolated included methicillin-resistant and -sensitive Staphylococcus aureus, methicillin-resistant S epidermidis, coag-ulase-negative Staphylococcus, Klebsiella species, Proteus species, anaerobes, and Mycobacterium avium.
Adverse Local Tissue ReactionOf the patients who had a primary di-
agnosis of persistent aseptic pseudotumor (n=2), 1 had a preoperative diagnosis of type II diabetes mellitus. Both patients had persistent lateral swelling and tro-chanteric pain on examination because of recurrent pseudotumor, and 1 also had concomitant abductor deficiency. The mean number of previous revisions was 1 and consisted of revision of the primary implant to a ceramic-on-polyethylene bearing surface with debridement of the pseudotumor.
Recurrent Hip InstabilityThe patient who had a primary diagno-
sis of recurrent instability had 5 previous revision attempts as a result of recurrent instability. These included revision of an acetabular component, placement of a constrained liner, and placement of a dual mobility bearing. The patient had mild concomitant abductor deficiency but was able to abduct against gravity.
Surgical TechniqueThe patient is placed in the lateral de-
cubitus position with standard patient po-sitioning devices. During skin preparation, care is taken to allow exposure proximal to the iliac crest and as posterior as possible. The first step is to expose and mobilize the gluteus maximus muscle. A curvilinear in-cision, similar to that performed with a pos-terolateral approach to the hip, is marked over the gluteus maximus, extending onto the lateral aspect of the proximal thigh as it courses inferiorly. The incision crosses the tip of the greater trochanter and extends distally over the posterior one-third of the lateral femur. The incision is carried down to the gluteus maximus fascia proximally and the iliotibial band distally. A soft tissue flap superficial to the gluteus maximus fas-cia is developed posteriorly, exposing the
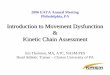
muscle belly. This flap can be carried all the way to its insertion posteriorly and distally. To begin muscle advancement, the fascia is then incised with monopolar electrocau-tery on the posterior aspect of the muscle in line with its superolateral border (Figure 1). This incision is performed perpendicu-lar to the vector of advancement. The in-terval between the gluteus medius and the gluteus maximus is developed proximally, creating a free edge of the gluteus maximus muscle. The superolateral free margin of the muscle is undermined and mobilized. The sciatic nerve is identified to minimize the risk of dissection injury and obviate compression when advancing the gluteus muscle. For additional excursion, the distal insertion and the superior insertion are par-tially released if necessary. In the setting of infection, adverse local tissue reaction, or recurrent instability, careful debridement of the seroma cavity lining is necessary to reduce fluid accumulation and encourage tissue healing (Figure 2).
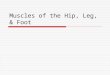
The next step is to advance and inset the muscle. The origin and insertion are left intact, and the mobilized free margin of the muscle is advanced (Figure 3). To re-duce dead space, the muscle can be rolled into the periarthroplasty defect (Video). Additionally, the muscle can be advanced through the posterior aspect of the greater trochanter through drill holes, and the free
Figure 1: Release of the posterior (Post) fascia of the gluteus maximus. To begin muscle advance-ment, a relaxing incision (*) is made in the glu-teus maximus fascia (M) posteriorly in line with its superolateral border. Abbreviations: Ant, anterior; Dist, distal; Prox, proximal.
Figure 2: Debridement of the seroma cavity. Removal of all seroma cavity lining in the set-ting of infection, adverse local tissue reaction, or recurrent instability is important to allow for a well-vascularized bed for soft tissue healing. Ab-breviations: Ant, anterior; Dist, distal; GT, greater trochanter; LT, lesser trochanter; Post, posterior; Prox, proximal.
e497

Copyright © SLACK inCorporAted
n Feature Article
end is sutured to help support the poste-rior capsule (Figure 4). Alternatively, the muscle can be sutured to the vastus latera-lis through drill holes to help support ab-ductor function (Figure 5). The muscle is repaired to the femur with nonresorbable suture. The remaining closure is an im-
bricating layer of the gluteus maximus to the tensor fascia lata anteriorly to further support abductor function in the setting of instability and complete dead space closure and reestablish soft tissue coverage over the femur in the setting of fascial defect. The superficial fascia is closed with 0 ab-sorbable sutures, the deep dermal layer is closed with 2-0 absorbable sutures, and the skin is closed with either a subcuticular ab-sorbable barbed suture or an over-and-over monofilament suture.
Postoperative trochanteric precautions and toe touch weight bearing for a mini-mum of 6 weeks were recommended for all patients. Subfascial and subcutaneous large-bore drains were removed once out-put was less than 30 mL/d for at least 2 consecutive days (usually 1-3 weeks). Pa-tients were progressed to full weight bear-ing by 3 months (governed by the require-ments of the arthroplasty).
resultsChronic Periprosthetic Joint Infection
All patients who underwent a gluteus maximus advancement flap procedure for chronic periprosthetic infection had heal-
ing of the wound and were infection-free at the last follow-up. Because of multiple treatment failures, 3 of the 4 patients re-ceived maintenance therapy with long-term oral suppressive antibiotics. All pa-tients ambulated with assistive devices at the last follow-up.
Two patients underwent reoperation after the initial gluteus maximus flap pro-cedure. One patient had recurrent drainage from the incision 3 months after surgery. The flap was elevated and had excellent viability, and the patient underwent irriga-tion and debridement, with readvancement of the flap an additional 5 cm to improve coverage of the proximal femur. The pa-tient remained infection-free after this sec-ond procedure. The second patient also had recurrence of drainage 3 months after the initial gluteus maximus flap procedure. A 1-stage exchange of the prosthesis with ir-rigation and debridement was performed, with readvancement of the flap. The pa-tient remained infection-free after this pro-cedure despite reelevation of the flap and recurrent wound closure over the flap.
Adverse Local Tissue Reaction Of the patients undergoing a gluteus
maximus flap procedure for recurrent asep-tic pseudotumor, both had healing of the wound and neither had recurrence of lateral swelling. Neither patient had further reop-eration. In both patients, abductor lurch improved but was still present. Trochan-teric pain improved and was rated as mild at the last follow-up. Abductor strength improved by 1 strength level (ie, able to abduct against gravity, or 3 of 5, from un-able to abduct against gravity, or 2 of 5) in the patient who had concomitant abductor deficiency.
Recurrent Hip InstabilityIntraoperatively, the patient with recur-
rent instability had a large seroma cavity and no posterior capsule in addition to a partial chronic tear at the abductor inser-tion. This patient underwent extensive debridement of the seroma cavity, con-
Figure 5: Abductor reconstruction. Alternatively, the muscle can be advanced through drill holes onto the abductor insertion in conjunction with imbricating the tensor fascia lata (*) to create additional support for abductor function. Abbre-viations: Ant, anterior; Dist, distal; Fem, femur; GM, gluteus maximus; Post, posterior; Prox, proximal.
Figure 3: Muscle advancement. The free edge of the gluteus maximus (GM) can be advanced with minimal tension on the muscle and preservation of its neurovascular supply. The asterisk indicates the residual posterior capsule. Abbreviations: Ant, anterior; Dist, distal; GT, greater trochanter; Post, posterior; Prox, proximal.
Figure 4: Posterior soft tissue reconstruction. The fascia overlying the gluteus maximus (M) can be used for fixation of the flap, and the muscle can be advanced into the posterior (Post) soft tissue defect through drill holes in the greater trochan-ter (GT). Abbreviations: Ant, anterior; Dist, distal; Prox, proximal.
e498

MAY/JUNE 2017 | Volume 40 • Number 3
n Feature Article
comitant revision of the femoral compo-nent to increase femoral anteversion, and exchange of the constrained liner at the time of the gluteus maximus flap proce-dure, with no recurrence of hip instability.
discussionSoft tissue loss in the setting of chronic
periprosthetic infection, pseudotumor, or chronic recurrent instability can result in posterior capsular insufficiency, fas-cial defects, abductor tears, and seroma or hematoma cavities. The current study showed the versatility of the gluteus maxi-mus advancement flap procedure and pro-vided examples of its use in scenarios in which previous conventional revision op-tions were unsuccessful. This technique offers numerous advantages. First, no functional impairment occurs with this technique because it does not disrupt the origin, insertion, and innervation of the gluteus maximus muscle. Second, the advanced tissue is thick but pliable, well suited for inset because of its overlying fascia, and well vascularized. Therefore, it functions as both an obliterator of dead space and a means of transferring an antibiotic-carrying blood supply directly to the site. Third, it can help to assist ab-ductor function.
Chronic soft tissue deficiency with wound breakdown is a devastating com-plication of chronic periprosthetic infec-tion and impairs successful eradication of infection. Current surgical management consists of 1- or 2-stage exchange of the prosthetic components with antibiotic therapy tailored to isolated organisms.15,16 Some studies report greater than 90% suc-cess with eradication of infection with a similar range of protocols.15 However, a study by Gomez et al16 suggested that fail-ure of reimplantation after spacer place-ment, secondary procedures, and overall morbidity in these patients may be higher than appreciated. Providing a vascularized muscle bed to cover the proximal femur and reducing the potential space for fluid collection may improve antibiotic pen-
etration into the peritrochanteric region and allow more effective skin healing. Other studies described the successful use of pedicled vastus lateralis and rectus abdominis flaps in cases of recalcitrant periprosthetic hip infection.17,18 The cur-rent study showed successful wound heal-ing and infection control with the gluteus maximus flap procedure as an adjuvant to conventional treatments. In 2 patients, the flap had to be elevated within 3 months of surgery because of persistent drainage. The flap showed excellent viability, with subsequent infection control after repeat irrigation and debridement.
Pseudotumor caused by metal-on- metal or modular THA corrosion remains a challenging problem, and high rates of infection and dislocation have been re-ported after revision THA.19,20 Recurrent massive fluid collections provide a favor-able environment for bacterial growth, re-sult in wound breakdown, and can create symptomatic lateral thigh pain as a result of fluid pressure. Elimination of this se-roma or hematoma cavity may help to reduce the incidence of infection. Poste-rior capsular deficiency and abductor de-ficiency are common in this setting, and the gluteus maximus flap can be tailored to help support a deficient posterior cap-sule or serve as abductor reconstruction in addition to its role in reducing dead space.
Use of the gluteus maximus as a recon-structive option for abductor insufficiency was described previously by Whiteside1,2 and Whiteside et al.3 Of 10 patients, 9 re-gained the ability to abduct the hip against gravity in the setting of abductor insuffi-ciency after THA with a technique involv-ing a split transfer of the gluteus maxi-mus and tensor fascia lata to the greater trochanter.2 In the current study, patients with abductor deficiency had improved lateral pain and some improvement in ab-duction against gravity, but the primary goals were to address capsular deficiency and reduce dead space in the posterior soft tissues. Reapproximation of the posterior capsule and external rotators substantially
reduces the rate of dislocation after the posterior approach for THA, and recon-stitution of these structures may assist prosthetic and bone procedures during revision for recurrent instability.21 The se-nior author (L.B.G.) has used a modifica-tion of this technique that is similar to that of Whiteside et al1,2 for primary abductor reconstruction in the setting of isolated native hip chronic abductor tears, but this is outside the scope of the current study.
LimitationsLimitations of this study include its
small size and the short follow-up period. This technique was reserved for use as a salvage option when conventional revi-sion techniques were unsuccessful, lim-iting the number of patients who could be included. Although follow-up in this study was short, the patients had continu-ous wound problems, fluid collections, or recurrent dislocations that subsided only after the flap procedure. The current find-ings suggested that at least in the short term, the repetitive revision cycle was broken. Long-term follow-up is needed to examine the durability of the results.
conclusionThe gluteus maximus advancement
flap procedure offers a diverse range of benefits in revision THA, including soft tissue coverage of the proximal femur in the setting of fascial deficiency, volu-metric reduction of seroma or hematoma cavities, and reconstruction of the abduc-tor and posterior capsule.
references 1. Whiteside LA. Surgical technique: glu-
teus maximus and tensor fascia lata trans-fer for primary deficiency of the abductors of the hip. Clin Orthop Relat Res. 2014; 472(2):645-653.
2. Whiteside LA. Surgical technique: transfer of the anterior portion of the gluteus maximus muscle for abductor deficiency of the hip. Clin Orthop Relat Res. 2012; 470(2):503-510.
3. Whiteside LA, Nayfeh T, Katerberg BJ. Glu-teus maximus flap transfer for greater tro-
e499

Copyright © SLACK inCorporAted
n Feature Article
chanter reconstruction in revision THA. Clin Orthop Relat Res. 2006; 453:203-210.
4. Fehm MN, Huddleston JI, Burke DW, Geller JA, Malchau H. Repair of a deficient abduc-tor mechanism with Achilles tendon allograft after total hip replacement. J Bone Joint Surg Am. 2010; 92(13):2305-2311.
5. Wang K, Cole S, White DC, Armstrong MS. Vastus lateralis transfer for severe hip abduc-tor deficiency: a salvage procedure. Hip Int. 2014; 24(2):180-186.
6. Beck M, Leunig M, Ellis T, Ganz R. Ad-vancement of the vastus lateralis muscle for the treatment of hip abductor discontinuity. J Arthroplasty. 2004; 19(4):476-480.
7. Kohl S, Evangelopoulos DS, Siebenrock KA, Beck M. Hip abductor defect repair by means of a vastus lateralis muscle shift. J Arthro-plasty. 2012; 27(4):625-629.
8. Van Warmerdam JM, McGann WA, Don-nelly JR, Kim J, Welch RB. Achilles allograft reconstruction for recurrent dislocation in total hip arthroplasty. J Arthroplasty. 2011; 26(6):941-948.
9. Lavigne MJ, Sanchez AA, Coutts RD. Recur-rent dislocation after total hip arthroplasty: treatment with an Achilles tendon allograft.
J Arthroplasty. 2001; 16(8 suppl 1):13-18.
10. McGann WA, Welch RB. Treatment of the unstable total hip arthroplasty using modular-ity, soft tissue, and allograft reconstruction. J Arthroplasty. 2001; 16(8 suppl 1):19-23.
11. Drexler M, Abolghasemian M, Kuzyk PR, et al. Reconstruction of chronic abductor defi-ciency after revision hip arthroplasty using an extensor mechanism allograft. Bone Joint J. 2015; 97-B(8):1050-1055.
12. Strømsøe K, Eikvar K. Fascia lata plasty in recurrent posterior dislocation after total hip arthroplasty. Arch Orthop Trauma Surg. 1995; 114(5):292-294.
13. Clough TM, Hodgkinson JP. Two-stage re-vision with pseudocapsular resection for re-current dislocation of total hip prostheses. J Arthroplasty. 2000; 15(8):1017-1019.
14. Morrey BF. Instability after total hip ar-throplasty. Orthop Clin North Am. 1992; 23(2):237-248.
15. Shanmugasundaram S, Ricciardi BF, Briggs TW, Sussmann PS, Bostrom MP. Evaluation and management of periprosthetic joint in-fection: an international, multicenter study. HSS J. 2014; 10(1):36-44.
16. Gomez MM, Tan TL, Manrique J, Deirmen-
gian GK, Parvizi J. The fate of spacers in the treatment of periprosthetic joint infection. J Bone Joint Surg Am. 2015; 97(18):1495-1502.
17. Choa R, Gundle R, Critchley P, Giele H. Suc-cessful management of recalcitrant infection related to total hip replacement using pedicled rectus femoris or vastus lateralis muscle flaps. J Bone Joint Surg Br. 2011; 93(6):751-754.
18. d’Ettorre G, Marchetti F, Ceccarelli G, et al. Surgical debridement with muscle flap trans-position and systemic teicoplanin therapy for infected hip arthroplasty. Hip Int. 2010; 20(2):255-257.
19. Stryker LS, Odum SM, Fehring TK, Springer BD. Revisions of monoblock metal-on-metal THAs have high early complication rates. Clin Orthop Relat Res. 2015; 473(2):469-474.
20. Wyles CC, Van Demark RE III, Sierra RJ, Trousdale RT. High rate of infection after aseptic revision of failed metal-on-metal to-tal hip arthroplasty. Clin Orthop Relat Res. 2014; 472(2):509-516.
21. Pellicci PM, Bostrom M, Poss R. Posterior approach to total hip replacement using en-hanced posterior soft tissue repair. Clin Or-thop Relat Res. 1998; 355:224-228.
e500