Embed Size (px)
Citation preview
FUNCTIONAL ANATOMY: EXTREMITIES


www.thezonafitnessacademy.com © Zona Health and Performance Inc. 2004-2013 All rights reserved. No part of this publication may be reproduced or redistributed in any form without the prior written permission of the publishers.

DISCLAIMER This work and/or manual are not designed to diagnose any medical conditions. Please refer to a qualified healthcare professional.

TABLE OF CONTENTS Introduction
Objectives Muscle Classification Based on Function Tonic and Phasic Musculature Spurt and Shunt Musculature Phase Shift
Structure and Function
Shoulder Girdle Pectoralis Minor Rhomboids Serratus Anterior Trapezius
Glenohumeral Joint
Deltoid Infraspinatus/Teres Minor Latissimus Dorsi/Teres Major Pectoralis Major Subscapularis Supraspinatus
Elbow Joint
Biceps Brachii Brachialis Brachioradialis Triceps Brachii

TABLE OF CONTENTS Structure and Function
Hip Joint Adductors Gluteus Medius/Minimus Gluteus Maximus Iliopsoas Sartorius
Knee Joint
Quadriceps Hamstrings
Ankle Foot Complex
Gastrocnemius Peroneals (Fibularis Group) Plantaris Soleus Tibialis Anterior
Glossary
References

Introduction INTRODUCTION Objectives Functional Anatomy for Fitness Professionals focuses on functional anatomy, with an emphasis on weight training. Through the emphasis on biomechanics, neurology, and muscle physiology, participants will gain an understanding that goes beyond origin and insertion, and reps and sets. After completing the course, you will now be able to describe the function of upper and lower extremity based on anatomy, biomechanics, and physics. In addition to introduction, there are 6 modules, which can be completed in any order.
• Shoulder Girdle • Shoulder (Glenohumeral) • Elbow • Hip • Knee • Ankle
Included with each module are the related muscles. There are also “research tidbits” for each muscle. You will be updated regularly on the latest research as it applies to exercise and weight training.

Introduction INTRODUCTION
Classification of Muscles Based on Function
Muscles may also be categorized according to their role while producing the movement.
Agonist (prime mover)
A muscle that causes a specific movement (or several movements) via its own contraction.
Antagonist
A muscle that opposes the movement (or movements) caused by the agonist.
Synergist
A muscle the performs or helps to perform the movement (or movements) caused by the agonist.
Neutralizing (counter-acting) synergists prevent unwanted movement produced by the prime mover.
Stabilizing (fixating) synergists, on the other hand, prevent or control movement at joints proximal to the
moving joint.
In the next section, antagonists and synergists will be labeled as (A) and (S), respectively.

Introduction INTRODUCTION Tonic and Phasic Musculature I would like to introduce you to taxonomy for muscle classification. Again, this classification schema is based on muscle fibre characteristics, but also on muscle architecture. Tonic and phasic muscle theory takes into account the body’s inherent design. That is, it relates to function. The beauty of this theory and its application is allows to avoid “cook-book” approaches in program design and assessment. Rather it fosters a problem-solving, individualistic approach. Dr. Vladimir Janda, the renowned Czechoslovakian physician coined the term tonic and phasic in the late 1960’s. Based on EMG and clinical studies, he found that certain muscles, which he termed tonic, had an anti-gravity function. These muscles had a higher resting “tonus” as they were constantly active. In fact, these muscles were founded to have a shorter than normal resting length. Tonic muscles are predominately type I or slow-twitch fibres. They consist of many mitochondria and thus, their oxidative capacity is quite high. More importantly, however, is that they are innervated by small, alpha a2 motor nerves. In other words, they are easily stimulated. This characteristic is important as these muscles must receive constant messages in order to control and correct posture. With this, comes a down side. Due to their relative ease of activation, these muscles are constantly firing, resulting in short, tight muscles. Phasic muscles, on the other hand, were under voluntary control, but did not respond to gravity. Unlike their tonic counterparts, these muscles were prone to inhibition and weakness Phasic muscles, on the other hand, consist mainly of type II or fast-twitch fibres. Due to their innervation by large, alpha a1 motor nerves, they require more stimulation to become active. Once activated, however, they have a greater capacity for force generation, but fatigue easily. This class of muscle is not designed to take on a postural or endurance role. Dysfunction of phasic muscles is manifested by weakness and inhibition. Short, tight tonic muscles often lead to weak, flaccid phasic muscles. For example, in Lower crossed syndrome, again coined by Janda in 1994, is characterized by tight hip flexors (iliopsoas) and lumbar spine erectors, and weak abdominals and gluteals. Upper crossed syndrome involves a tight pectoralis minor and posterior cervical extensors, and weak rhomboids and deep cervical flexors. (For a complete list of tonic and phasic muscles, refer to Table 1.) With this being said, muscles no longer need to be randomly stretched and/or strengthened. Weak (phasic) muscles often remain weak despite the best attempts at strengthening them. This is usually due to their tight antagonist muscle, which is usually tonic. These short, tight antagonist muscles need to be lengthened prior to strengthening these weak muscles. Furthermore, phasic muscles rarely need to be stretched as they are already inhibited.

Introduction INTRODUCTION Tonic and Phasic Musculature Table 1. Tonic and Phasic Musculature Table 2. Characteristics of Tonic and Phasic Muscles
Tonic Iliopsoas
Rectus Femoris
Hamstrings
Piriformis
Tensor Fascia Latae
Gastrocnemius
Soleus
Upper Trapezius
Pectoralis Major
Pectoralis Minor
Levator Scapula
Bicep Brachii
Subscapularis
Phasic
Gluteus Maximus
Gluteus Medius
Vasti (Medialis/Lateralis)
Tibialis Anterior
Fibularis
Rhomboids
Middle and Lower Traps
Tricep Brachii
Deltoid
Supraspinatus
Infraspinatus
Rectus Abdominus
Obliques
Transversus Abdominus
Tonic Phasic Prone to Prone to
hyperactivity inhibition
Function Posture Movement Susceptibility to Fatigue Late Early Reaction to Faulty Loading Shortening Weakening

Introduction INTRODUCTION Spurt and Shunt Musculature The other taxonomy used to classify muscles is the based on muscle architecture. A spurt muscle is a muscle that possesses a line of pull across a joint such that it favours rotary force or torque. Another characteristic is that the distal attachment is close to the joint at which the muscle acts resulting in a greater rotatory component compared with its stabilizing component. A shunt muscle is a muscle that has a line of pull that is oriented predominantly along the long axis of a bone (thus mostly a joint stabilizing force). These shunt muscles have their more proximal attachment close to the joint, and their action is said to be more for stabilization than for rotation The biceps brachii muscle is often presented as an example of a spurt muscle and the brachioradialis muscle as an example of a shunt muscle. Table 3. Spurt and Shunt Muscles Due to the duel nature of certain muscles, they remain unclassified.
Spurt Shunt
Adductors Biceps Brachii
Gastrocnemius Hamstrings
Sartorius Soleus
Tibialis Anterior
Brachialis Deltoids
Gluteus Maximus Gluteus Medius
Infraspinatus/Teres Minor Lateral Rotators of Hip
Latissimus Dorsi Pectoralis Major
Introduction INTRODUCTION Phase Shift The third concept I would like to explore is one of the phase shift. First coined by the human anatomist, David Gorman, it refers to the ability of a two-joint muscle to retain its resting length while performing complex functions. Why is this important, and secondly, what are examples of it? To answer the first question, one must understand the relationship between length of a muscle and force production. This is known as the length-tension relationship, and can be described as follows:
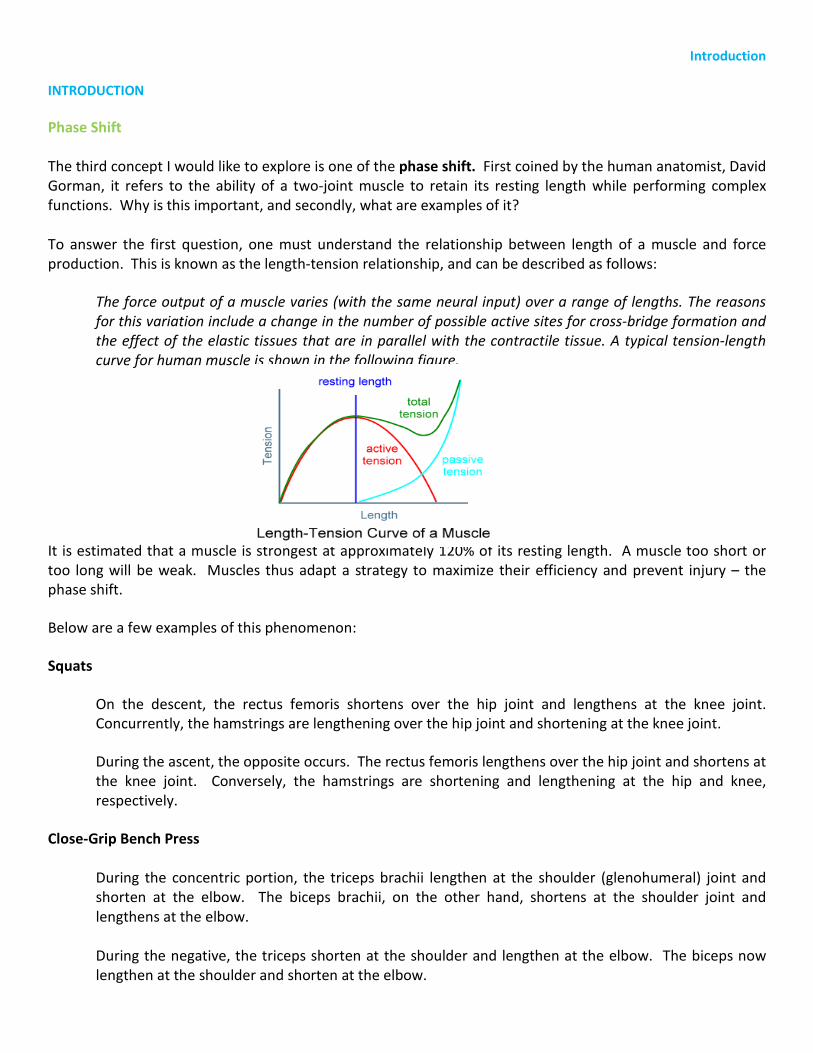
The force output of a muscle varies (with the same neural input) over a range of lengths. The reasons for this variation include a change in the number of possible active sites for cross-bridge formation and the effect of the elastic tissues that are in parallel with the contractile tissue. A typical tension-length curve for human muscle is shown in the following figure.
It is estimated that a muscle is strongest at approximately 120% of its resting length. A muscle too short or too long will be weak. Muscles thus adapt a strategy to maximize their efficiency and prevent injury – the phase shift.
Below are a few examples of this phenomenon:
Squats
On the descent, the rectus femoris shortens over the hip joint and lengthens at the knee joint. Concurrently, the hamstrings are lengthening over the hip joint and shortening at the knee joint.
During the ascent, the opposite occurs. The rectus femoris lengthens over the hip joint and shortens at the knee joint. Conversely, the hamstrings are shortening and lengthening at the hip and knee, respectively.
Close-Grip Bench Press
During the concentric portion, the triceps brachii lengthen at the shoulder (glenohumeral) joint and shorten at the elbow. The biceps brachii, on the other hand, shortens at the shoulder joint and lengthens at the elbow.
During the negative, the triceps shorten at the shoulder and lengthen at the elbow. The biceps now lengthen at the shoulder and shorten at the elbow.

Structure and Function STRUCTURE AND FUNCTION Shoulder Girdle Without proper movement of this joint, the glenohumeral joint cannot move efficiently. The shoulder girdle is the articulation between the scapula and thorax, as well as the glenohumeral joint, previously mentioned. Due its muscular attachments, the shoulder girdle functions intricately with the vertebral column (neck and thorax). Postural faults, such as rounded shoulders and anterior head carriage, collectively known as upper crossed syndrome, limit the range of motion at this joint. A common fault seen in many gyms is training the muscles of the shoulder girdle as if they were strictly postural. Many of the muscles at this joint, while attached to the spine, function more dynamically than one would think. The most noticeable of these are the rhomboids. The ranges of motion about the shoulder girdle are difficult to quantify, but asymmetries can easily be detected.

Structure and Function
Nerve Supply: Medial pectoral nerve: C8 - T1 Function(s): 1. Protraction of scapula (S) Serratus anterior (A) Rhomboids, middle fibres of trapezius 2. Medial rotation of scapula (S) Levator scapula, rhomboids (A) Trapezius, serratus anterior
STRUCTURE AND FUNCTION Shoulder Girdle Pectoralis Minor
Introduction A troublesome, muscle, the pectoralis minor contributes to many postural faults, such as upper crossed syndrome and anterior head carriage, albeit indirectly. The muscle is important for smooth movements of the shoulder girdle by improving functional range of motion and deceleration forces. Characteristics The pectoralis minor is comprised of 60% slow-twitch fibres. Exercises Incline bench press (with either dumbbell or barbell) are superior in activating the pec minor as compared to flat or incline variations. Also, push-ups with a plus are effective at activating the pectoralis minor. Since this muscle is prone to tightening, it must be stretched. PNF stretching works best. Instruct the client to protract the shoulders against resistance for approximately 10 seconds. Upon relaxation, gently move their shoulders into retraction and hold for approximately 10 seconds. Repeat.

Structure and Function STRUCTURE AND FUNCTION Shoulder Girdle Pectoralis Minor Research Tidbits Shoulder (subacromial) Impingement
Researchers have shown that a shortened pectoralis minor limits proper movement of the scapula, resulting in subacromial impingement.
Borstad JD, Ludewig PM. The effect of long versus short pectoralis minor resting length on scapular kinematics in healthy individuals. Journal of Orthopaedic Sports Physical Therapy. 2005 Apr; 35(4):227-38.
Scapular stabilization
In a study referred to by most rehabilitation practitioners, including chiropractors and physiotherapists, researchers found the following four exercises to be most effective at activating the scapular muscles are the following: scaption (scapular plane elevation), seated rows, push-ups with a plus, and press-ups.
The scapular muscles examined were upper, middle, and lower trapezius; levator scapula; rhomboids; pectoralis minor; and the middle and lower serratus anterior.
Moseley JB Jr, Jobe FW, Pink M, Perry J, Tibone J. EMG analysis of the scapular muscles during a shoulder rehabilitation program. American Journal of Sports Med. 1992 Mar-Apr; 20(2):128-34.

Structure and Function
Nerve Supply: Dorsal scapular: C5 Function(s) 1. Adduction of scapula (S) Middle trapezius (A) Serratus anterior, pectoralis minor 2. Elevation of scapula (S) Upper fibres of trapezius, levator scapula (A) Lower fibres of trapezius, pectoralis minor, serratus anterior 3. Downward rotation of scapula (S) Latissimus dorsi (A) Levator scapular 4. Scapular stabilization
STRUCTURE AND FUNCTION Shoulder Girdle Rhomboids
Introduction Contrary to popular belief, the rhomboids are not postural. Rather, they function phasically to position the shoulder blades for various movements. For instance, if one were to isometrically retract their scapula, they would reduce the range of their shoulder joint in both abduction and flexion. The rhomboids attach to the cervical spine and are closely related to neck movements. Characteristics To illustrate the phasic characteristic of the rhomboids, their fibre composition is only 45% slow-twitch. Exercises The best exercise for rhomboids is seated rows or variations thereof. Performing lateral and front raises also causes activation of the rhomboids.

Structure and Function STRUCTURE AND FUNCTION Shoulder Girdle Rhomboids Research Tidbits Scapular stabilization
In a study referred to by most rehabilitation practitioners, including chiropractors and physiotherapists, researchers found the following four exercises to be most effective at activating the scapular muscles are the following: scaption (scapular plane elevation), seated rows, push-ups with a plus, and press-ups.
The scapular muscles examined were upper, middle, and lower trapezius; levator scapula; rhomboids; pectoralis minor; and the middle and lower serratus anterior.
Moseley JB Jr, Jobe FW, Pink M, Perry J, Tibone J. EMG analysis of the scapular muscles during a shoulder rehabilitation program. Am J Sports Med. 1992 Mar-Apr;20(2):128-34.
Rhomboid injury in during overhead movements
Muscle injury during overhead sports and movements have been shown to injure the rhomboids due to the positioning of the scapular and deceleration of the scapular during the follow-through motion of a pitcher or volleyball player, as well as lowering the weight from a snatch position. Balcom WB, Pappas AM. Musculotendinous sport injuries of the shoulder. In: Pappas AM, editor. Upper extremity injuries in the athlete. New York: Churchill Livingstone Inc; 1995. P. 229.

Structure and Function
Nerve Supply: Long thoracic nerve: C5-C7 Function(s) 1. Protraction of scapula (S) Pec Minor (A) Rhomboids, middle fibres of trapezius 2. Lateral rotation of scapula (S) Trapezius (A) Levator scapula, rhomboids, pectoralis minor
STRUCTURE AND FUNCTION Shoulder Girdle Serratus Anterior
Introduction The diminutive serratus anterior is crucial in movement of the upper limb. It is responsible for upward rotation of the scapula, necessary during abduction and flexion. It is also required for providing a stable base of support from which the rotator cuff muscles operate. The serratus anterior is commonly injured, which is evident in scapular winging. Exercises The serratus anterior is a synergist in most movements and should be trained as such. Lateral raises and front raises are examples. Incorporating a scapular stabilization program (see research tidbits) will address the serratus anterior.

Structure and Function STRUCTURE AND FUNCTION Shoulder Girdle Serratus Anterior Research Tidbits Scapular stabilization
Researchers have demonstrated that the bench press on a stable surface is superior when it comes to improving serratus anterior strength compared to pushups and wall pushups on a stable or unstable surface, and superior to bench press on an unstable surface.
Martins J, Tucci HT, Andrade R, Araújo RC, Bevilaqua-Grossi D, Oliveira AS. Electromyographic amplitude ratio of serratus anterior and upper trapezius muscles during modified push-ups and bench press exercises. Journal of Strength and Conditioning Research. 2008 Mar;22(2):477-84.
Isolating the serratus anterior
It has been shown that the best way to isolate the serratus anterior while simultaneously reducing muscular activity of other shoulder girdle muscles is to do the following: place hand on your opposite shoulder and move one’s arm through extension, abduction, and internal rotation.
Dexter Witt, PT, DPT, OCS, Nancy Talbott, PT, PhD, and Susan Kotowski, PhD. Electromyographic activity of scapular muscles during diagonal patterns using elastic resistance and free weights. International Journal of Sports Physical Therapy. 2011 December; 6(4): 322–332.

Structure and Function
Nerve Supply: Spinal accessory nerve: C4-C5 Function(s) 1. Elevation of scapula (S) Levator scapula (A) Pectoralis minor, pectoralis major, latissimus dorsi 2. Lateral rotation of scapula (S) Serratus anterior (A) Levator scapula, rhomboids, pectoralis minor
STRUCTURE AND FUNCTION Shoulder Girdle Upper Trapezius
Introduction The trapezius is an odd muscle in that while sharing a common nerve supply, it has three functionally distinct and opposing parts. The upper and lower fibres, which synergist in upward rotation of the scapula, are antagonistic in elevation and depression, respectively. The trapezius is often shortened due to occupational stresses, injuries, and poor technique. This is partly due to the dominance of the upper fibres as compared to the antagonist lower fibres. Characteristics The trapezius is predominantly slow-twitch fibres, hovering around 53%. Exercises The best exercise for the trapezius is dumbbell or barbell shrugs. This muscle is also active during deadlifts, squats, and military presses.

Structure and Function
Nerve Supply: Spinal accessory nerve: C4-C5 Function(s) 1. Lateral rotation of scapula (S) Serratus anterior (A) Levator scapula, rhomboids, pectoralis minor 3. Retraction of scapula (S) Rhomboids (A) Pectoralis minor, serratus anterior
Nerve Supply: Spinal accessory nerve: C4-C5 Function(s) 1. Lateral rotation of scapula (S) Serratus anterior (A) Levator scapula, rhomboids, pectoralis minor 3. Retraction of scapula (S) Rhomboids (A) Pectoralis minor, serratus anterior
STRUCTURE AND FUNCTION Shoulder Girdle Middle Trapezius
Lower Trapezius
Structure and Function STRUCTURE AND FUNCTION Shoulder Girdle Lower Trapezius Research Tidbits Scapular stabilization
In a study referred to by most rehabilitation practitioners, including chiropractors and physiotherapists, researchers found the following four exercises to be most effective at activating the scapular muscles are the following: scaption (scapular plane elevation), seated rows, push-ups with a plus, and press-ups.
The scapular muscles examined were upper, middle, and lower trapezius; levator scapula; rhomboids; pectoralis minor; and the middle and lower serratus anterior.
Moseley JB Jr, Jobe FW, Pink M, Perry J, Tibone J. EMG analysis of the scapular muscles during a shoulder rehabilitation program. Am J Sports Med. 1992 Mar-Apr;20(2):128-34.
Differential trapezius activation
The unilateral shoulder shrug exercise was found to produce the greatest EMG activity in the upper trapezius. For the middle trapezius, the greatest EMG amplitudes were generated with shoulder horizontal extension with external rotation and the overhead arm raise in line with the lower trapezius muscle in the prone position. The arm raise overhead exercise in the prone position produced the maximum EMG activity in the lower trapezius
Ekstrom RA, Donatelli RA, Soderberg GL. Surface electromyographic analysis of exercises for the trapezius and serratus anterior muscles. J Orthop Sports Phys Ther. 2003 May;33(5):247-58.

Structure and Function STRUCTURE AND FUNCTION Glenohumeral (GH) Joint Unlike the hip joint, the GH joint is designed for mobility. There are no ligamentous supports. Rather, the rotator cuff complex (supraspinatus, subscapularis, infraspinatus, and teres minor) assume the supportive role. The movements at this joint are dynamic. A considerable range of motion must be permitted to allow for certain movements. The muscles of the GH joint must not only create movement, but must also, often simultaneously, add stability to an already unstable joint. As such, the incidence of overuse is high. The GH joint is also affected by the position of the thorax and neck, which in turn affects the shoulder girdle. Even dysfunction in the lower limb can create havoc at this delicate joint. The shoulder can abduct and forward flex to 180 degrees. In the absence of dysfunction, the shoulder can rotate medially and laterally up to 90 degrees. Finally, extension and adduction are limited to 60 and 75 degrees, respectively.
Structure and Function STRUCTURE AND FUNCTION Glenohumeral Joint Joint The shoulder joint is a ball-and-socket joint, similar to the hip joint. Unlike the hip joint, however, this is an incongruent joint – the concave and convex surfaces are NOT uniformly equidistant. As such, it lacks the stability of a congruent joint. Ligaments There are no true supportive ligaments of the GH joint. The muscles provide dynamic stability, along with creating movement.
Glenoid Labrum
The glenoid labrum deepens the joint, increasing the congruity and stability of it.
Capsule
The joint capsule surrounds the joint, and also provides stability to the joint. This is assisted by the coracohumeral ligament.
Biomechanics The motion of the GH joint is intricately linked to the movement of the scapula. For every 2 degrees of humeral rotation, the scapula rotates 1 degree. Furthermore, during abduction and flexion of the GH joint, the joint must externally rotate to prevent subacromial impingement.

Structure and Function
Nerve Supply: Axillary: C5, C6 Function(s): 1. Flexion of shoulder (anterior) (S) Long head of biceps brachii, pectoralis major, coracobrachialis (A) Posterior deltoid, latissimus dorsi, long head of triceps 2. Horizontal Adduction (anterior) (S) Pectoralis major (A) Posterior deltoid 3. Humeral stabilization (ant/post) (S) Rotator cuff complex, long head of biceps brachii
STRUCTURE AND FUNCTION Glenohumeral Joint Anterior Deltoid
Introduction This penniform muscle functions intricately with the supraspinatus. Its main function includes abduction, flexion, and extension of the shoulder joint. These actions are carried out by the middle, anterior, and posterior portions of the deltoid, respectively. Its multipennate formation is designed for strength at the expense of speed. It was once thought that the deltoid initiated abduction and the supraspinatus completed it. We now know this to be false. EMG activity increases with increasing abduction (and flexion) in both muscles. In fact, these muscles are most active between 90 and 180 degrees of abduction (and flexion). Characteristics The distribution of slow-twitch fibres in the deltoid is approximately 60%.

Structure and Function
Nerve Supply: Axillary: C5, C6 Function(s): 1. Abduction of shoulder (S) Supraspinatus, long head of biceps, (upper trapezius, rhomboids), triceps brachii (A) Latissimus dorsi, teres major, teres minor
STRUCTURE AND FUNCTION Glenohumeral Joint Middle Deltoid
Exercises The muscle is most active in 90 to 180 degrees of abduction. As such, the muscle should be trained in this range. The problem is that above 90 degrees, there is less torque placed upon the muscle. To address this, the arm must be maintained in position parallel to the ground. Before modifying the exercise to capitalize on sustained torque, thus resistance, let us first explore the most effective exercises to stimulate the deltoid. Middle deltoid
• Incline dumbbell side laterals • Standing dumbbell side laterals* • Seated dumbbell side laterals • Cable side laterals
Anterior deltoid
• Seated front dumbbell raises • Standing front dumbbell raises** • Seated front dumbbell raises
* While performing standing dumbbell side laterals, hold onto an incline with the opposite arm. During the movement, lean away from the bench. ** While performing standing front dumbbell raises, flex at the trunk during the movement. Be sure to keep the lumbar spine in neutral.

Structure and Function
Nerve Supply: Axillary: C5, C6 Function(s): 1. Shoulder extension (posterior) (S) Latissimus dorsi, long head of triceps brachii, teres major/minor (A) Biceps brachii, anterior deltoid 5. Humeral stabilization (ant/post) (S) Rotator cuff complex, long head of biceps brachii
STRUCTURE AND FUNCTION Glenohumeral Joint Posterior Deltoid

Structure and Function STRUCTURE AND FUNCTION Glenohumeral Joint Deltoid Research Tidbits . Hand position does matter
A neutral grip is superior at recruiting the posterior deltoid compared to a pronated grip during posterior pec deck flies.
Schoenfeld, Brad MSc, CSCS; Gul Tiryaki Sonmez, R. PhD; Kolber, Morey J. PT, PhD, CSCS; Contreras, Bret MA, CSCS; Harris, Robert MSc; Ozen, Serife Effect of hand position on EMG activity of the posterior shoulder musculature during a horizontal abduction exercise. Journal of Strength & Conditioning Research
Heads of the deltoid
Researchers have shown that the deltoid muscle could be divided into seven segments separated by their intramuscular tendons. What’s most interesting is that these seven segments may be controlled differentially by the central nervous system. Furthermore, they display different fibre type characteristics, contractile properties, and architectural differences.
E. Audenaert and E. Barbaix. Separate segments within the deltoid muscle: Anatomical variants or wishful thinking? Int J Shoulder Surg. 2008 Jul-Sep; 2(3): 69–70 Yoshimasa Sakoma, Hirotaka Sano, Nobuhisa Shinozaki,Yoshiaki Itoigawa,Nobuyuki Yamamoto,Toshifumi Ozaki, and Eiji Itoi. Anatomical and functional segments of the deltoid muscle. J Anat. 2011 February; 218(2): 185–190.

Structure and Function
Nerve Supply: Suprascapular nerve: C5 – C6 Function(s): 1. Lateral rotation of shoulder (S) Teres minor (A) Latissimus dorsi, pectoralis major, teres major, subscapularis 2. Depression of humeral head (S) Teres minor, subscapularis (A) Deltoid, supraspinatus
STRUCTURE AND FUNCTION Glenohumeral Joint Infraspinatus
Introduction As two of the four rotator cuff muscles, the infrapinatus and teres minor act to stabilize the head of the humerus via a downward pull. They function as lateral rotators regardless of position of the arm. In fact, their activity increases with increased flexion of the shoulder up to 120 degrees. In cases of subacromial impingement, these muscles are usually implicated. Without the contraction of this pair of muscles, the deltoid and supraspinatus exert an unbalanced, upward pull on the humerus. As a result, the tendon of the biceps, supraspinatus, and a bursa can all become compressed. Characteristics These muscles are approximately 45% slow-twitch fibres. They function phasically in response to various arm movements.

Structure and Function
Nerve Supply: Axillary nerve: C5 – C6 Function(s): 1. Lateral rotation of shoulder (S) Infraspinatus (A) Latissimus dorsi, pectoralis major, teres major, subscapularis 2. Depression of humeral head (S) Infraspinatus, subscapularis (A) Deltoid, supraspinatus
STRUCTURE AND FUNCTION Glenohumeral Joint Teres Minor

Structure and Function STRUCTURE AND FUNCTION Glenohumeral Joint Infraspinatus/Teres Minor Exercises There are a myriad of rotator cuff exercises. Which ones you use depend on the presence of an injury, and if present, which stage of injury. For the sake of this course, we’ll assume that your client is injury free.
• External rotation in either shoulder abduction or shoulder neutral. Keep in mind that the line of resistance must be in the same plane of movement. Client can either stand of lay on his/her side. In either case, place a towel between the upper arm and torso to ensure adequate blood flow to the ‘avascular’ shoulder region.
• Shoulder abduction or flexion. The activity of both the infraspinatus and teres minor increase with increasing abduction and flexion.
Research Tidbits Two muscles: one functional unit?
When the shoulder is positioned in 90 degrees of abduction, with full internal rotation, and 30 degrees of forward flexion and maintained against resistance, not only do the supraspinatus and deltoid fire, but so does the infraspinatus. Interestingly, the teres minor was not active throughout the test. The teres minor and infraspinatus have previously been described as a functional unit, which is not in agreement with this study.
Rowlands LK, Wertsch JJ, Primack SJ, Spreitzer AM, Roberts MM. Kinesiology of the empty can test. Am J Phys Med Rehabil. 1995 Jul-Aug;74(4):302-4.
Rotator cuff muscles as abductors
Not only do the infraspinatus and teres minor depress the humeral head and laterally rotate the arm, they may also assist in abduction. The relationship is not as direct as one might think. The inferior rotator cuff muscles, as well as the supraspinatus take the load off the deltoid during abduction by clearing the humeral head from the acromion process.
Sharkey NA, Marder RA, Hanson PB. The entire rotator cuff contributes to elevation of the arm. J Orthop Res. 1994 Sep;12(5):699-708.

Structure and Function
Nerve Supply: Thoracodorsal nerve: C6 – C8 Function(s): 1. Adduction of shoulder (S) Pectoralis major, teres major (A) Deltoid, supraspinatus 2. Medial rotation of shoulder (S) Pectoralis major, teres major, subscapularis (A) Infraspinatus, teres minor 3. Extension of shoulder (S) Posterior deltoid, long head of triceps brachii, teres major, teres minor (A) Biceps brachii, anterior deltoid
STRUCTURE AND FUNCTION Glenohumeral Joint Latissimus Dorsi
Introduction The latissimus is another complex muscle. Due to its attachments, bony and fascial, to the vertebral column, scapula, and humerus, it serves as a link between the upper and lower bodies during many functional movements. When stimulated, it extends, adducts, and medially rotates the shoulder joint. With the upper limb fixed, it extends the lower thoracic and lumbar spine. The latissimus dorsi is related to the opposite gluteus maximus and bicep femoris through extensive attachments to the thoracolumbar fascia, as well as the sacrotuberous ligament. So much so, that many athletic activities require simultaneous contraction of the latissimus and opposite glutes and hamstrings. Similarly, these same activities require simultaneous relaxation of these muscles. Characteristics It contains roughly equal amounts of slow- and fast-twitch muscle fibres.

Structure and Function
Nerve Supply: Lower subscapular nerve: C6 – C8 Function(s): 1. Adduction of shoulder (S) Pectoralis major, latissimus dorsi (A) Deltoid, supraspinatus 2. Medial rotation of shoulder (S) Pectoralis major, latissimus dorsi, subscapularis (A) Infraspinatus, teres minor 3. Extension of shoulder (S) latissimus dorsi, posterior deltoid, long head of triceps brachii, teres minor (A) Biceps brachii, anterior deltoid
STRUCTURE AND FUNCTION Glenohumeral Joint Teres Major

Structure and Function STRUCTURE AND FUNCTION Glenohumeral Joint Latissimus Dorsi/Teres Major Exercises Controversy exists as to which exercises best activate the lats. The consensus seems to be that those movements that begin with the shoulder in flexion are superior. These include bent-over barbell rows, one-arm dumbbell rows, and T-bar rows. Other effective exercises include seated rows, lat pulldowns, chin-ups, and dips. The deadlift is a great exercise as it requires forceful shoulder extension against a relatively heavy load. Research Tidbits Hand position during lat pulldowns
In a study investigating the effects of different hand positions on the electromyographic (EMG) activity of shoulder muscles during the performance of the lat pull-down exercise, researchers found that changes in handgrip position do affect the activities of specific muscles during the lat pull-down movement. Most notably, the performance of the latissimus pull-down exercise using a wide-grip hand position produced greater muscle activity in the latissimus dorsi than any other hand position during both the concentric or eccentric phases of the movement.
Signorile JF, Zink AJ, Szwed SP.A comparative electromyographical investigation of muscle utilization patterns using various hand positions during the lat pull-down. J Strength Cond Res. 2002 Nov;16(4):539-46.
Olympic lifting and the latissimus dorsi
Both the clean and jerk and snatch have resulted in significant muscular activity of the latissimus dorsi during all phases of the lifts.
Mohan C Narayana. Muscle activity pattern in Olympic lifting: latissimus dorsi and pectoralis major – an EMG study. Br J Sports Med2010;44:i28

Structure and Function
Nerve Supply: Medial and lateral pectoral nerves: C5- T1 Function(s): 1. Adduction of shoulder (S) Latissimus dorsi, teres major (A) Deltoid, supraspinatus 2. Flexion of shoulder (S) Long head of biceps brachii Anterior deltoid, coracobrachialis (A) Posterior deltoid, latissimus dorsi, teres major/minor 3. Medial rotation of shoulder (S) Subscapularis, latissimus dorsi, teres major (A) Infraspinatus, teres minor
STRUCTURE AND FUNCTION Glenohumeral Joint Pectoralis Major
Introduction The pectoralis major affects three joints, namely, the sternoclavicular joint, the acromioclavicular joint, and the shoulder joint. It has extensive attachments to the clavicle, sternum, intercostal cartilages, and the external oblique. Its actions go beyond bench pressing and push-ups. It is required for swinging a golf club, batting a baseball, and swimming. When stimulated, the pectoralis major adducts, medially rotates and flexes the arm at the shoulder. Theses functions are important when selecting appropriate exercises. Characteristics The pectoralis major contains roughly 60% fast-twitch muscle fibres.

Structure and Function STRUCTURE AND FUNCTION Glenohumeral Joint Pectoralis Major Exercises Decline bench press (with either dumbbells or barbells) are superior in activating the pec major as compared to flat or incline variations. Why? As one assumes a decline position, the adductor component is increased. With incline, the abduction component is now increased. in other words, the sternal portion, responsible for adduction is called upon during decline press. The same holds true for dips. Research Tidbits Big bench for a big swing
The pectoralis major was shown to be the main contributor to the acceleration phase of the golf swing. This study illustrates the importance of upper body weight training for golfing.
Pink M, Jobe FW, Perry J. Electromyographic analysis of the shoulder during the golf swing. Am J Sports Med. 1990 Mar-Apr;18(2):137-40.
The bench press vs. the pec deck for pectoralis major development
According to researchers, the bench press and pec deck were equally as effective at recruiting the pectoralis major and anterior deltoid. Valdinar de Araújo Rocha Júnior, Paulo Gentil, Elke Oliveira and Jake do Carmo. Comparison among the EMG activity of the pectoralis major, anterior deltoidis and triceps brachii during the bench press and peck deck exercises. Rev Bras Med Esporte _ Vol. 13, Nº 1 – Jan/Fev, 2007

Structure and Function
Nerve Supply: Upper/lower subscapular nerves: C5-C7 Function(s) 1. Medial rotation of shoulder (S) Pectoralis major, latissimus dorsi, teres major (A) Infraspinatus, teres minor 2. Depression of humeral head (S) Teres minor, infraspinatus (A) Deltoid, supraspinatus 3. Adduction of Shoulder (S) Pectoralis major, latissimus dorsi, teres major (A) Deltoid, supraspinatus, biceps brachii
STRUCTURE AND FUNCTION Glenohumeral Joint Subscapularis
Introduction As one of the four rotator cuff muscles, the subscapularis acts to stabilize the head of the humerus via a downward pull. It functions as medial rotator, along with the pectoralis major, latissimus dorsi, and teres major. In cases of subacromial impingement, this muscle is usually implicated. Without the contraction of this muscle, along with the infraspinatus and teres minor, the deltoid and supraspinatus exert an unbalanced, upward pull on the humerus. As a result, the tendon of the biceps, supraspinatus, and a bursa can all become compressed. Characteristics This muscle is approximately 60% slow-twitch fibres and functions tonically. Exercises There are a myriad of rotator cuff exercises. Which ones you use depend on the presence of an injury, and if present, which stage of injury. For the sake of this course, we’ll assume that your client is injury free. See research tidbits for exercises.

Structure and Function STRUCTURE AND FUNCTION Glenohumeral Joint Subscapularis Research Tidbits Subscapularis testing
The upper and lower portions of the subscapularis muscle are independently innervated and activated, as was shown in a recent study. Humeral abduction was found to have a strong influence on the selective activation of the upper versus the lower subscapularis as the upper subscapularis muscle activity was greater than lower subscapularis muscle activity for all exercises except for internal rotation with 0 degrees of humeral abduction. In addition, the push-up plus and diagonal exercises were found to be superior to traditional internal rotation exercises for activating both functional portions of the subscapularis muscle.
Our results showing that the upper and lower portions of the subscapularis muscle are functionally independent may affect training or rehabilitation protocols for the rotator cuff muscles. Decker MJ, Tokish JM, Ellis HB, Torry MR, Hawkins RJ. Subscapularis muscle activity during selected rehabilitation exercises. Am J Sports Med. 2003 Jan-Feb;31(1):126-34.

Structure and Function
Nerve Supply: Suprascapular: C5, C6 Function(s): 1. Abduction of shoulder (S) Deltoids, long head of biceps, (upper trapezius, rhomboids), triceps brachii (A) Pectoralis major, latissimus dorsi, teres major
STRUCTURE AND FUNCTION Glenohumeral Joint Supraspinatus
Introduction This muscle functions intricately with the deltoid. Unlike the deltoid, its main function includes abduction of the shoulder joint. It was once thought that the deltoid initiated abduction and the supraspinatus completed it. We now know this to be false. EMG activity increases with increasing abduction (and flexion) in both muscles. In fact, these muscles are most active between 90 and 180 degrees of abduction (and flexion). In cases of subacromial impingement, this muscle is usually the most damaged. The shoulder region, especially the supraspinatus tendon has very little blood supply. As such, damage to it results in degeneration and prolonged healing. Characteristics This muscle is approximately 60% slow-twitch fibres and functions tonically.

Structure and Function STRUCTURE AND FUNCTION Glenohumeral Joint Supraspinatus Exercises There are a myriad of rotator cuff exercises. Which ones you use depend on the presence of an injury, and if present, which stage of injury. For the sake of this course, we’ll assume that your client is injury free. Like the deltoid, the supraspinatus is most active in 90 to 180 degrees of abduction. As such, the muscle should be trained in this range. The problem is that above 90 degrees, there is less torque placed upon the muscle. To address this, the arm must be maintained in position parallel to the ground.
• Incline dumbbell side laterals • Standing dumbbell side laterals* • Seated dumbbell side laterals • Cable side laterals
* While performing standing dumbbell side laterals, hold onto an incline with the opposite arm. During the movement, lean away from the bench. These exercises are identical to that of the deltoid. Research Tidbits Supraspinatus strengthening
Researchers set out to determine which exercises were best for strengthening the supraspinatus muscle. They concluded that the empty can and full can exercises were most effective in activating the supraspinatus muscle.
Takeda Y, Kashiwaguchi S, Endo K, Matsuura T, Sasa T. The most effective exercise for strengthening the supraspinatus muscle: evaluation by magnetic resonance imaging. Am J Sports Med. 2002 May-Jun;30(3):374-81.

Structure and Function STRUCTURE AND FUNCTION Elbow Joint The elbow joint is complex joint in that it functions closely with the hand and wrist complex. Many authorities consider the elbow to move through only flexion and extension and consider supination and pronation to occur only at the wrist. This is misleading as supination also occurs at the elbow joint, or more specifically, at the proximal radio-ulnar joint. For the purposes of this course, only flexion and extension will be considered. Elbow extension can reach up to 10 degrees, especially in those with ligament laxity. Flexion is limited by the soft-tissues of the arm (biceps and forearm flexors) to approximately 135 degrees. There is one degree of motion at the elbow joint proper (humeroulnar and humeroradial) and at the superior radio-ulnar joint, resulting in two degrees of motion, total. Joint The elbow joint consists of the following three joints:
Humeroulnar Joint
This medial joint consists of the ulna and the trochlea of the humerus.
Humeroradial Joint
This lateral joint consists the head of the radius cupped in the capitellum.
Radioulnar Joint
This proximal joint is the articular between the head of the radius and ulna.

Structure and Function STRUCTURE AND FUNCTION Elbow Joint Ligaments
Capsule The capsule surrounds all three joints of the elbow. Injury at any one of these joints will cause the capsule to swell. Medial Collateral The medial collateral ligament of the elbow connects the humerus to the ulna. It stabilizes against valgus stress, especially during flexion. Furthermore, it aids in joint approximation. Lateral Collateral The lateral collateral also attaches the humerus to the ulna, but is weaker than its medial counterpart. It stabilizes against varus stresses. Annular Ligament The annular ligament surrounds the head of the radius. Quadrate Ligament This ligament maintains the radial head to the radial notch, located on the ulna, controlling both supination and pronation.

Structure and Function STRUCTURE AND FUNCTION Elbow Joint Biomechanics Flexion and extension occur at the humeroulnar joint. Flexion is limited by the tension of the muscles of the forearm, while extension is limited by bone on bone. Furthermore, pronation reduces the range of flexion at the elbow joint. Pronation and supination occur at the proximal radio-ulnar joint and the distal radio-ulnar joint (to be discussed with the wrist). Furthermore, the head of the radial spins in the capitellum of the humerus during pronation and supination. Finally, the carrying angle of the elbow is 5 and 10-15 degrees in males and females, respectively. This structural difference has clinical indications, to be discussed later.

Structure and Function
Nerve Supply: Musculocutaneous: C5, C6 Function(s): 1. Shoulder flexion (S) Anterior deltoid (A) Posterior deltoid, latissimus dorsi, teres major/minor 2. Shoulder abduction (S) Middle deltoid, supraspinatus (A) Latissimus dorsi, pectoralis major, teres major, long head of triceps 3. Elbow Flexion (S) Brachioradialis, brachialis (A) Triceps brachii 4. Supination (S) Supinator (A) Pronator teres and quadratus 5. Stabilization of humeral head (S) Rotator cuff complex, long head of biceps brachii 6. Horizontal adduction of shoulder (S) Coracobrachialis, pectoralis major (A) Posterior deltoid
STRUCTURE AND FUNCTION Elbow Joint Biceps Brachii
Introduction This two-headed muscle, as the name implies, is one of the most complex in the entire body. Its most evident functions are elbow and shoulder flexion, as well as supination of the forearm (with the elbow flexed to 90 degrees). If the arm is medially rotated, shoulder flexion is more efficient. With the arm in lateral rotation, it assists in GH abduction. Its most important function, however, is its least obvious - stabilization of the humeral head via an upward pull.

Structure and Function STRUCTURE AND FUNCTION Elbow Joint Biceps Brachii Characteristics The bicep brachii has a roughly even distribution of slow-twitch to fast-twitch fibres. Studies have reported the muscle to have anywhere from 45 to 52% slow-twitch fibres. Exercises Depending on position of the shoulder joint, this muscle can be made to be more or less effective. With the shoulder in extension, as in incline curls, there is an increase in efficiency due to a pre-stretch of both heads. Conversely, shortening the muscle via shoulder flexion, as in preacher curls, weakens it, causing increased usage of the underlying brachialis.
• Bicep curls o Dumbbell or barbell o Incline, standing, or preacher
• Close-grip chin-ups/lat pulldowns Research Tidbits Biceps: more than just for the beach.
Patients with selective atrophy of the biceps brachii did not demonstrate a reduction in the ability to flex the elbow. They did, however, experience a partial dislocation of the humeral head from the glenoid cavity when lifting a heavy weight. Due to its upward pull on the humerus, the bicep brachii is absolutely necessary when lifting a heavy weight.
Duchenne, GB. Physiology of Motion, translated by E.B. Kaplan, J.B Lippincott, Philadelphia, 1949 (p. 98)
Training speed does in fact alter muscle recruitment activity.
Researchers have demonstrated that training speed can have effect on muscle recruitment. Analysis of EMG parameters suggests that muscle fatigue mainly involves the biceps brachii when movements were slow and wide, and the brachioradialis when they were rapid and short. This study makes it possible to take these specificities into account in order to adjust the physical training program.
Guevel A, Hogrel JY, Marini JF. Fatigue of elbow flexors during repeated flexion-extension cycles: effect of movement strategy. Int J Sports Med. 2000 Oct;21(7):492-8.
Structure and Function
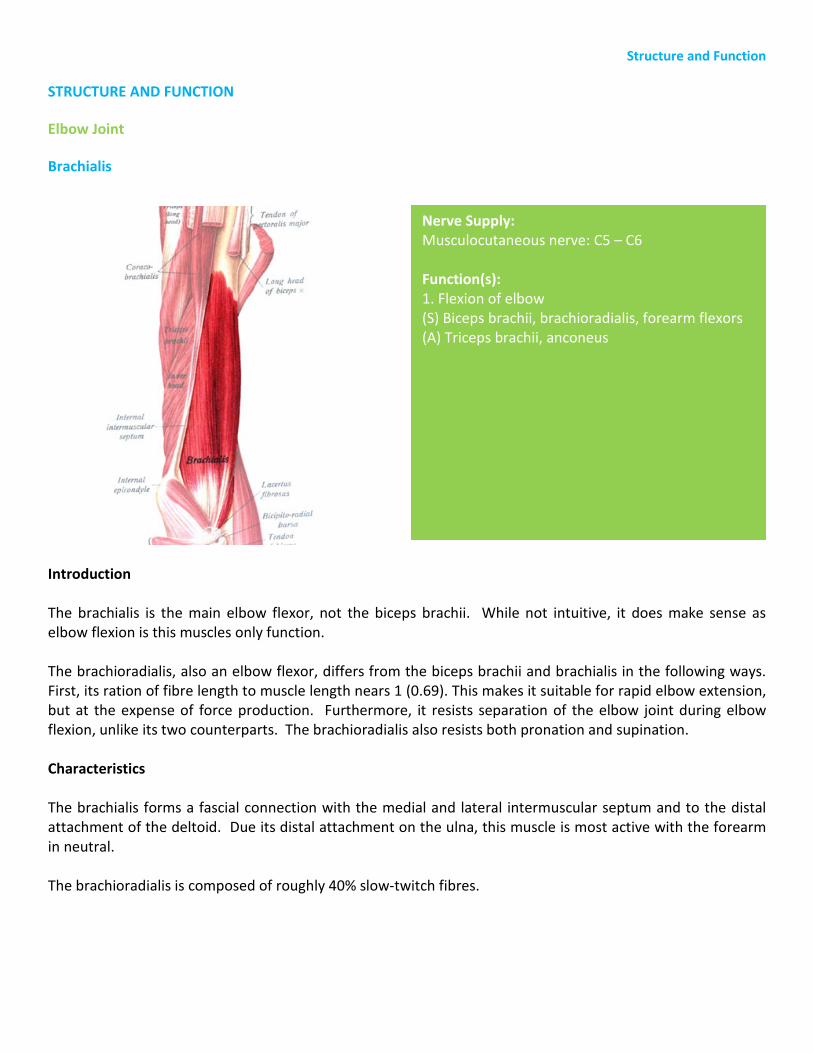
Nerve Supply: Musculocutaneous nerve: C5 – C6 Function(s): 1. Flexion of elbow (S) Biceps brachii, brachioradialis, forearm flexors (A) Triceps brachii, anconeus
STRUCTURE AND FUNCTION Elbow Joint Brachialis
Introduction The brachialis is the main elbow flexor, not the biceps brachii. While not intuitive, it does make sense as elbow flexion is this muscles only function. The brachioradialis, also an elbow flexor, differs from the biceps brachii and brachialis in the following ways. First, its ration of fibre length to muscle length nears 1 (0.69). This makes it suitable for rapid elbow extension, but at the expense of force production. Furthermore, it resists separation of the elbow joint during elbow flexion, unlike its two counterparts. The brachioradialis also resists both pronation and supination. Characteristics The brachialis forms a fascial connection with the medial and lateral intermuscular septum and to the distal attachment of the deltoid. Due its distal attachment on the ulna, this muscle is most active with the forearm in neutral. The brachioradialis is composed of roughly 40% slow-twitch fibres.

Structure and Function
Nerve Supply: Radial nerve: C5 – C7 Function(s): 1. Flexion of elbow (S) Biceps brachii, brachialis, forearm flexors (A) Triceps brachii, anconeus
STRUCTURE AND FUNCTION Elbow Joint Brachioradialis Exercises
Since these muscles do not cross the shoulder joint, they are not affected directly by shoulder position. Increasing or decreasing the efficiency of the biceps brachii via modification of shoulder joint position will ultimately decrease or increase the reliance on these two muscles, respectively. Placing the forearm in neutral also increases activation of the brachialis.
• Bicep curls o Dumbbell or barbell o Incline, standing, or preacher
• Close-grip chin-ups/lat pulldowns

Structure and Function STRUCTURE AND FUNCTION Elbow Joint Brachioradialis Research Tidbits Training speed does in fact alter muscle recruitment activity.
Researchers have demonstrated that training speed can have effect on muscle recruitment. Analysis of EMG parameters suggests that muscle fatigue mainly involves the biceps brachii when movements were slow and wide, and the brachioradialis when they were rapid and short. This study makes it possible to take these specificities into account in order to adjust the physical training program.
Guevel A, Hogrel JY, Marini JF. Fatigue of elbow flexors during repeated flexion-extension cycles: effect of movement strategy. Int J Sports Med. 2000 Oct;21(7):492-8.
Age is really just a number
After 12 weeks of heavy resistance training, elderly males showed a significant increase in muscle size in both the brachialis and biceps brachii. Furthermore, strength was improved as was work capacity.
Roman WJ, Fleckenstein J, Stray-Gundersen J, Alway SE, Peshock R, Gonyea WJ. Adaptations in the elbow flexors of elderly males after heavy-resistance training. J Appl Physiol. 1993 Feb;74(2):750-4.

Structure and Function
Nerve Supply: Radial nerve: C7, C8 Function(s) 1. Shoulder extension (S) Posterior deltoid, latissimus dorsi, teres major, teres minor (A) Biceps brachii, anterior deltoid 2. Shoulder adduction (S) Latissimus dorsi, teres major, pectoralis major (A) Middle deltoid, supraspinatus 3. Elbow extension (S) Anconeus (A) Biceps brachii, brachioradialis, brachialis 4. Stabilization of humeral head (S) Rotator cuff complex, long head of biceps brachii
STRUCTURE AND FUNCTION Elbow Joint Triceps Brachii
Introduction This muscle makes up the bulk of the arm. Due to its attachments on the scapula, it not only extends elbow, but also extends the shoulder. Characteristics The triceps are comprised of anywhere between 32 and 40% slow-twitch fibres. The medial head of the triceps has been shown to have 60% slow-twitch fibres.

Structure and Function STRUCTURE AND FUNCTION Elbow Joint Triceps Brachii Exercises Like its antagonist, the biceps brachii, the position of the shoulder joint can cause this muscle to be more or less effective. With the shoulder in flexion, there is an increase in efficiency due to a pre-stretch of the long head. Conversely, shortening the muscle via shoulder extension. as in dips and kick-backs, weakens the long-head, causing increased usage of the underlying medial and lateral heads In order from greatest to least activation, the following is a list of suitable tricep exercises:
• Decline tricep extension • Tricep pushdown • Tricep dip between benches • One-arm cable tricep extension • Overhead rope extension • Seated-one arm dumbbell extension • Close-grip bench press
Research Tidbits Hand position “doesn’t matter”…but width does
Regardless of whether lifters used a supinated or neutral grip, a narrow grip bench press resulted in greater tricep recruitment compared to a wide grip bench press. Lehman, Gregory J..The Influence of Grip Width and Forearm Pronation/Supination on Upper-Body Myoelectric Activity During the Flat Bench Press. Journal of Strength & Conditioning Research: August 2005
Similarly, narrow stance pushups result in greater tricep activation as compared to wider stance variations.
Cogley, Robert M.; Archambault, Teasha A.; Fibeger, Jon F.; Koverman, Mandy M.; Youdas, James W.; Hollman, John H. Comparison of Muscle Activation Using Various Hand Positions During the Push-Up Exercise. Journal of Strength & Conditioning Research: August 2005

Structure and Function STRUCTURE AND FUNCTION Hip Joint A common error when training the hip joint is the overemphasis on range of motion. Unlike many other joints, the hip is tightly bound by strong ligaments, checking its motion, especially in extension. The function of the muscles, on the other hand, is to steady the hip during weight-bearing, gait, and other functional activities. Unlike the shoulder, the main function of the hip is to provide stability. Despite having limited ranges of motion (except for flexion), the hip has three degrees of freedom. That is, it can flex and extend; abduct and adduct, and rotate medially and laterally. Depending on the activity, the movement often involves a combination of these. The interesting thing about the muscles that surround the hip, is that their function may change depending on position of the hip. To describe each of these exceptions is beyond the scope of this course. The range of motion at the hip in flexion and extension is 135 degrees and 30 degrees, respectively. However, with the knee extended, as in a straight leg raise or hurdler’s stretch, the range is reduced to between 90 and 120 degrees (sources vary). Extreme caution must be used when stretching clients beyond these ranges as injuries can result. The range of motion in adduction and abduction are both 20-30 degrees. Medial and lateral rotation are checked by the ligaments at 45 and 60, respectively. Joint The hip joint is actually the articulation between four bones – the femur and the ischium, ilium, and pubic bones, which form at their epiphyseal growth plates in the acetabulum. The acetabulum is deep, increasing the congruency for the head of the femur. In fact, the hip joint is the most congruent in the body. An interesting configuration of this joint is that the head of the femur faces medial, superior, and anterior. The acetabulum faces lateral, inferior, and also anterior. This joint, despite being designed for stability, has three degrees of motion – flexion/extension, adduction/abduction, and internal/external rotation.

Structure and Function STRUCTURE AND FUNCTION Hip Joint Ligaments
Acetabular Labrum
This piece of fibrocartilage provides a deeper socket for the head of the femur. Transverse Acetabular Ligament Iliofemoral and Pubofemoral These two ligaments make up the Z-ligament, attaching at an angle, traveling infero-laterally. Ischiofemoral These fibres, located posteriorly, run superiorly and laterally, wrapping around the neck of the femur. The iliofemoral, pubofemoral, and ischiofemoral ligaments tighten during extension (and loosen during flexion). Thus, in neutral posture, we hang on these ligaments. Joint Capsule This capsule surrounds the joint and holds the head of the femur in the acetabulum. Its fibres run in four directions, longitudinal, oblique, arcuate, and circular. This capsule strengthens the joint, increasing its stability.

Structure and Function STRUCTURE AND FUNCTION Hip Joint Biomechanics The two main functions of the hip joint are transmission of forces to (and from) the head, arms, and trunk; and stability. Furthermore, it is a unique joint in that it usually operates in a closed-kinetic chain and is characterized by the following:
• Large area of muscle of attachment • Many bi-articular muscles (crossing two joints) • Large cross section of muscle • Great ROM
Many of the muscles that cross the hip undergo inversion. In other words, the function of many muscles is dependent on the position of the joint. The adductors, for example, act as flexors with the hip in extension and as extensors with the hip in flexion. The closed-pack position, providing the most stability, is 90 degrees of flexion, slight medial rotation, and slight abduction. The open-pack or loose position is flexion, adduction, and lateral rotation. Weight-Bearing Structure of the Hip Joint The weight bearing function of the hip joint is reflected in the trabecular pattern of the femur and pelvis.
1. Medial Trabecular System 2. Lateral Trabecular System 3. Sacrum-Ischium 4. Pubic Rami

Structure and Function
Nerve Supply: Inferior gluteal nerve: L5 – S2 Function(s): 1. Extension of hip (S) Hamstrings (A) Iliopsoas, sartorius, tensor fascia lata, hip adductor group 2. Lateral rotation of hip (S) Posterior lateral rotators, sartorius, Iliopsoas (A) Tensor fascia lata, hip adductors, gluteus medius and minimus
STRUCTURE AND FUNCTION Hip Joint Gluteus Maximus
Introduction The gluteus maximus is the strongest muscle in your body. Not only does this muscle insert onto the femur, but it forms a broad attachment with the iliotibial band. The gluteus maximus is the main extensor and abductor of the hip. It is called upon during explosive activities, such as sprinting, jumping, and squatting. Characteristics Believe it or not, the gluteus maximus is composed of predominantly slow twitch fibres. The ratio of slow-twitch to fast-twitch is in the neighbourhood of 2:1 or 68% slow-twitch. Nevertheless, this muscle is only recruited during powerful activities. One of the reasons for this is the hamstrings are always recruited first during hip extension.

Structure and Function STRUCTURE AND FUNCTION Hip Joint Gluteus Maximus Exercises Due to its muscular attachments, muscle fibre composition, and neuromuscular characteristics, the following exercises are superior when it comes to training the gluteus maximus.
• Squats • Deadlifts • Lunges • Step-ups • Various plyometrics
Research Tidbits Does squat depth really matter?
As squat depth increases, the contribution of the gluteus maximus increases during the concentric portion of the lift. The relative contributions of the gluteus maximus during partial-, parallel, and deep squats were 16.9, 28.0, and 35.4%, respectively. Caterisano A, Moss RF, Pellinger TK, Woodruff K, Lewis VC, Booth W, Khadra T. The effect of back squat depth on the EMG activity of 4 superficial hip and thigh muscles. Strength Cond Res. 2002 Aug;16(3):428-32.
Spinning for your glutes?
Despite what many spinning instructors may tell you, you cannot work the gluteus maximus during a spinning class. Regardless of saddle height or foot position, there was no contribution of the gluteus maximus during cycling. Ericson, MO. Journal of Rehabilitative Medicine 1985 17: 53-61.
Structure and Function
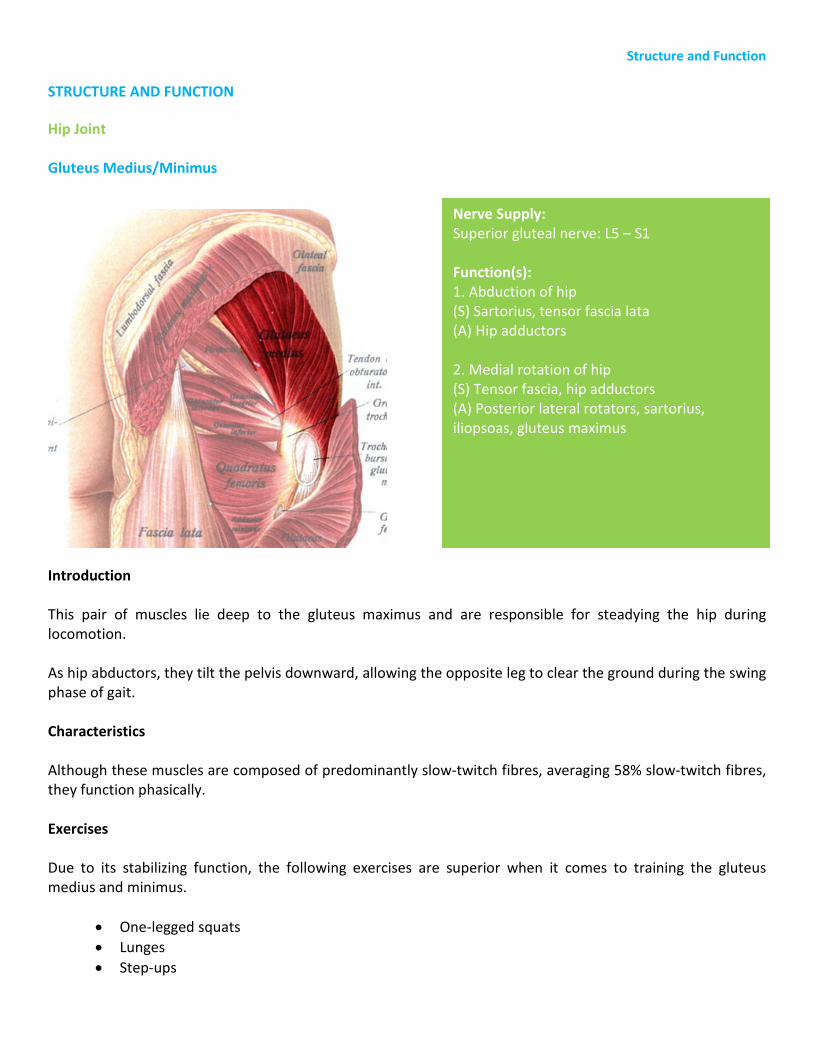
Nerve Supply: Superior gluteal nerve: L5 – S1 Function(s): 1. Abduction of hip (S) Sartorius, tensor fascia lata (A) Hip adductors 2. Medial rotation of hip (S) Tensor fascia, hip adductors (A) Posterior lateral rotators, sartorius, iliopsoas, gluteus maximus
STRUCTURE AND FUNCTION Hip Joint Gluteus Medius/Minimus
Introduction This pair of muscles lie deep to the gluteus maximus and are responsible for steadying the hip during locomotion. As hip abductors, they tilt the pelvis downward, allowing the opposite leg to clear the ground during the swing phase of gait. Characteristics Although these muscles are composed of predominantly slow-twitch fibres, averaging 58% slow-twitch fibres, they function phasically. Exercises Due to its stabilizing function, the following exercises are superior when it comes to training the gluteus medius and minimus.
• One-legged squats • Lunges • Step-ups

Structure and Function
Nerve Supply: Superior gluteal nerve: L5 – S1 Function(s): 1. Abduction of hip (S) Sartorius, tensor fascia lata (A) Hip adductors 2. Medial rotation of hip (S) Tensor fascia, hip adductors (A) Posterior lateral rotators, sartorius, iliopsoas, gluteus maximus
STRUCTURE AND FUNCTION Hip Joint Gluteus Medius/Minimus
Research Tidbits Spinning for your glutes: part 2?
Even though the gluteus maximus is not recruited during cycling, the gluteus medius (and minimus) increase in activity with increasing pedaling rate, resistance, saddle height, and the posterior foot position.
Spinning can be a great rehab exercise for those with weak or atrophied glutes. On the other hand, spinning may actually exacerbate an overuse injury in the gluteus medius and minimus.
Ericson, MO. Journal of Rehabilitative Medicine 1985 17: 53-61.
Prevent ankle injuries by increasing strength of the gluteus medius
Researchers have found that individuals with previous ankle inversion sprains demonstrate more rapid recruitment of the gluteus medius during conditions that place the ankle into inversion. This seems to be a protective mechanism, thereby preventing further sprains. This altered recruitment pattern of the gluteus medius may lead to some unwanted changes. That is, degenerative changes, altered joint reaction forces, and muscle imbalances.
Beckman SM, Buchanan TS. Ankle inversion injury and hypermobility: effect on hip and ankle muscle electromyography onset latency. Arch Phys Med Rehabil. 1995 Dec;76(12):1138-43

Structure and Function
Nerve Supply: Femoral Nerve: L2 – L3 (and L 1) Function(s): 1. Flexion of the hip (S) Rectus femoris, tensor fascia lata, sartorius (A) Gluteus maximus, hamstrings 2. Lateral flexion of the vertebral column (S) Erector spinae, quadratus lumborum (A) Opposite iliopsoas and quadratus lumborum 3. Stabilization of hip
STRUCTURE AND FUNCTION Hip Joint Iliopsoas
Introduction The iliopsoas actually consists of 3 muscles: the psoas major; psoas minor; and iliacus. Collectively, these muscles flex and externally rotate the hip. The psoas major and minor also act upon the lumbar spine, stabilizing it, extending it, and laterally flexing it. The iliopsoas, with the soleus, is active constantly. This is why it is so troublesome. Many cases of low back and hip can be attributed to hypertonicity in this muscle group. Characteristics The iliopsoas is classified as tonic. Exercises Due to its tendency to tightness, the iliopsoas should be restored to its normal length. Keep in mind, however, that its range of motion is limited to 10 degrees of hip extension and anything greater than this can lead to muscle and joint damage.

Structure and Function
Nerve Supply: Femoral Nerve: L2 – L3 (and L 1) Function(s): 1. Flexion of the hip (S) Rectus femoris, tensor fascia lata, sartorius (A) Gluteus maximus, hamstrings 2. Lateral flexion of the vertebral column (S) Erector spinae, quadratus lumborum (A) Opposite iliopsoas and quadratus lumborum 3. Stabilization of hip
STRUCTURE AND FUNCTION Hip Joint Iliopsoas
Research Tidbits Full sit-ups: the controversy remains.
Controversy continues when it comes to curl-ups vs. sit-ups. Performing a curl-up (isolated trunk flexion without hip flexion) is thought to be superior at the targeting and isolating the abdominals*. Is this true?
Let’s examine this from a biomechanical perspective. When performing a curl-up, the abdominals resist the weight of trunk. However, when performing a full sit-up (hip flexion with sustained abdominal flexion), the abdominals not only resist the weight of the trunk, but also the extension moment created by the iliopsoas.
The recommendation to perform full sit-ups is controversial, as it should be. In the absence of contra-indications, one may want to include this exercise into their training regime along with transversus abdominus stability work.
*Abdominals include rectus abdominus, and obliques.

Structure and Function
Nerve Supply: Femoral Nerve: L2 – L3 (and L 1) Function(s): 1. Flexion of the hip (S) Rectus femoris, tensor fascia lata, sartorius (A) Gluteus maximus, hamstrings 2. Lateral flexion of the vertebral column (S) Erector spinae, quadratus lumborum (A) Opposite iliopsoas and quadratus lumborum 3. Stabilization of hip
STRUCTURE AND FUNCTION Hip Joint Iliopsoas

Structure and Function
Nerve Supply: Femoral Nerve: L2-L3 Function(s) 1. Abduction of hip (S) Gluteus medius and minimus (A) Hip adductors (magnus, brevis, and longus), pectineus, gracilis, tensor fascia lata 2. Flexion of hip (S) Iliopsoas, rectus femoris, tensor fascia lata, hip adductor group (A) Gluteus maximus, hamstrings 3. External rotation of hip (S) Gluteus maximus, posterior lateral hip rotators, iliopsoas (A) Gluteus medius and minimus, tensor fascia lata
STRUCTURE AND FUNCTION Hip Joint Sartorius
Introduction The sartorius is commonly known as the “tailor’s muscle” as it is necessary to assume the crossed-legged position of the tailor. It is similar to the tensor fascia lata in hip flexion and abduction, but laterally rotates the thigh. It provides stability to knee in activities that require lateral movements and pivoting on one leg. Sports include soccer, rugby, and basketball. Characteristics The sartorius contains roughly 50% slow-twitch fibres, but functions phasically. Exercises This muscle is active during most single leg, weight-bearing exercises. This muscle will get sufficient work in closed-kinetic chain, weight-bearing exercises.

Structure and Function
Nerve Supply: Femoral nerve: L2, L3 Obturator nerve: L2 – L4 (20%) Function(s): 1. Adduction of hip (S) Tensor fascia lata (A) Gluteus medius and minimus, sartorius 2. Flexion hip (S) Iliopsoas, sartorius, tensor fascia lata, rectus femoris (A) Gluteus maximus, hamstrings
STRUCTURE AND FUNCTION Hip Joint Pectineus
Introduction The adductor group actually consists of five different muscles: the adductor longus, brevis and magnus; the gracilis; and the pectineus. Collectively, this group brings the leg towards the midline. Their function is not as a prime mover, but rather a stabilizer of the hip and knee. The various adductor muscles are active during different stages of gait. For example, the longus is active at toe-off and the magnus is active at heel-strike and ascending stairs. This stability function is so ingrained that even at 70% of adductor strength (tested via an adductor machine), there is only a mild impairment in walking, stair-climbing or jumping. Characteristics Due to their arrangement, these muscles function primarily as hip adductors. As mentioned in the previous section, the adduction moment is to resist movement at both the hip and knee. The adductor magnus, due to its attachment on the ischial tuberosity, functions like the hamstrings, producing hip extension. The adductor muscles are predominantly slow-twitch fibres, ranging anywhere from 53.5 to 63.6% Type I fibres. As a result, they are tonic.

Structure and Function
Nerve Supply: Obturator nerve: L2 – L4 Function(s): 1. Adduction of hip (S) Tensor fascia lata (A) Gluteus medius and minimus, sartorius 2. Flexion hip (S) Iliopsoas, sartorius, tensor fascia lata, rectus femoris (A) Gluteus maximus, hamstrings 3. Knee flexion (S) Hamstrings, plantaris, popliteus (A) Quadriceps
STRUCTURE AND FUNCTION Hip Joint Gracilis
Exercises Unless one’s goal is hypertrophy of the inner thigh, these muscles are best trained in closed-kinetic chain, weight-bearing exercises. The following are examples:
• Lunges (stationary and walking lunges) • Step-ups • Squats (wide stance) • Sumo deadlifts
Structure and Function
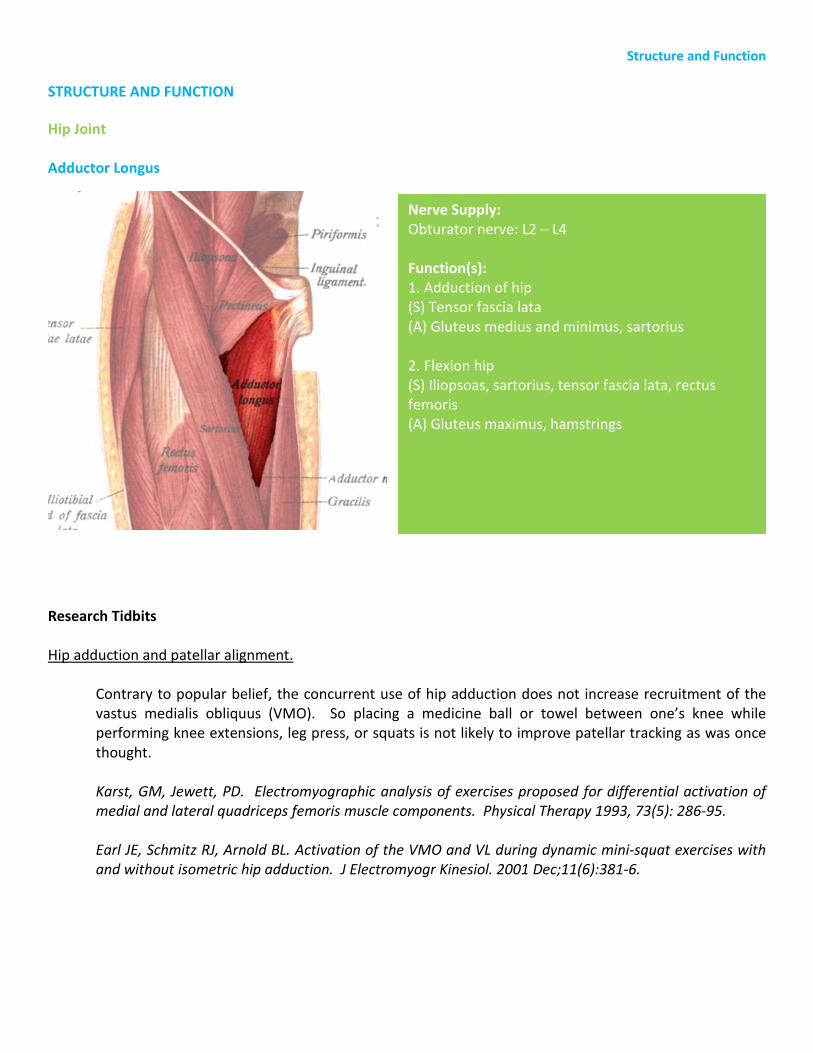
Nerve Supply: Obturator nerve: L2 – L4 Function(s): 1. Adduction of hip (S) Tensor fascia lata (A) Gluteus medius and minimus, sartorius 2. Flexion hip (S) Iliopsoas, sartorius, tensor fascia lata, rectus femoris (A) Gluteus maximus, hamstrings
STRUCTURE AND FUNCTION Hip Joint Adductor Longus
Research Tidbits Hip adduction and patellar alignment.
Contrary to popular belief, the concurrent use of hip adduction does not increase recruitment of the vastus medialis obliquus (VMO). So placing a medicine ball or towel between one’s knee while performing knee extensions, leg press, or squats is not likely to improve patellar tracking as was once thought.
Karst, GM, Jewett, PD. Electromyographic analysis of exercises proposed for differential activation of medial and lateral quadriceps femoris muscle components. Physical Therapy 1993, 73(5): 286-95.
Earl JE, Schmitz RJ, Arnold BL. Activation of the VMO and VL during dynamic mini-squat exercises with and without isometric hip adduction. J Electromyogr Kinesiol. 2001 Dec;11(6):381-6.

Structure and Function
Nerve Supply: Obturator nerve: L2 – L4 Function(s): 1. Adduction of hip (S) Tensor fascia lata (A) Gluteus medius and minimus, sartorius 2. Flexion hip (S) Iliopsoas, sartorius, tensor fascia lata, rectus femoris (A) Gluteus maximus, hamstrings 3. Knee flexion (S) Hamstrings, plantaris, popliteus (A) Quadriceps
STRUCTURE AND FUNCTION Hip Joint Adductor Brevis
Research Tidbits Strength or flexibility: Their role in injury prevention.
In a study to determine whether hip muscle strength and flexibility play a role in the incidence of adductor and hip flexor strains in National Hockey League ice hockey team players, researchers determined that adduction strength was 95% of abduction strength in the uninjured players but only 78% of abduction strength in the injured players. Interestingly, preseason hip adductor flexibility was not different between players who sustained adductor muscle strains and those who did not.
Researchers concluded that a player was 17 times more likely to sustain an adductor muscle strain if his adductor strength was less than 80% of his abductor strength.
Tyler TF, Nicholas SJ, Campbell RJ, McHugh MP. The association of hip strength and flexibility with the incidence of adductor muscle strains in professional ice hockey players. American Journal of Sports Medicine 2001, 29(2): 124-8.

Structure and Function
Nerve Supply: Obturator nerve: L2 – L4 Function(s): 1. Adduction of hip (S) Tensor fascia lata (A) Gluteus medius and minimus, sartorius 2. Flexion hip (S) Iliopsoas, sartorius, tensor fascia lata, rectus femoris (A) Gluteus maximus, hamstrings 3. Knee flexion (S) Hamstrings, plantaris, popliteus (A) Quadriceps 3. Hip extension (S) Hamstrings, gluteus maximus (A) Iliopsoas, sartorius, tensor fascia lata, rectus femoris
STRUCTURE AND FUNCTION Hip Joint Adductor Magnus

Structure and Function STRUCTURE AND FUNCTION Knee Joint For such a complex joint, the knee can only flex and extend. There is minimal rotation at this joint, but it is involuntary. The rotation of the lower limb occurs at the hip and at the ankle-foot complex. Since the knee is surrounded by the powerful quadriceps and hamstrings, the ligamentous structure must be very strong to withstand the resultant stresses. Various ligaments check rotation and others increase the congruity of the joint in order to ensure safe and efficient movement. With the ankle and hip in neutral, the range of motion in knee extension and flexion are 15 and 135 degrees. Many of the muscles that act on the knee have their origins at the hip joint. As such, the two joints are often related in many functional activities. Joints
Tibiofemoral Joint The tibiofemoral joint is a synovial joint with two degrees of freedom of motion – flexion/extension and medial/lateral rotation The femoral articular surface consists of a lateral and medial condyle, both medial to the femoral head. This causes the shaft of the femur to run obliquely. The medial tibial plateau is 50% larger than the lateral, and its articular cartilage is three times as thick. These tibial plateaus are separated by two bony spines called intercondylar tubercles, which lock during knee extension. Patellofemoral Joints The patellofemoral joint is the articulation between the femur and the patella. The patella acts as an anatomical pulley and a mechanism to reduce friction between the quadriceps tendon and femoral condyles. This joint is the least congruent in the entire body.
Index of Insall and Salviti These indices measure the length of the patella in relation to the length of the patellar ligament (tibial tuberosity to inferior border of patella). The normal ratio is 1:1, with the limit being 1:1.3.
• Patella Alta (>1:1.3) • Grasshopper Patella (lateral rotation of the patella with feet straight) • Squinting Patella (medial rotation of the patella) • Baja Patella (<1:1)
Structure and Function STRUCTURE AND FUNCTION
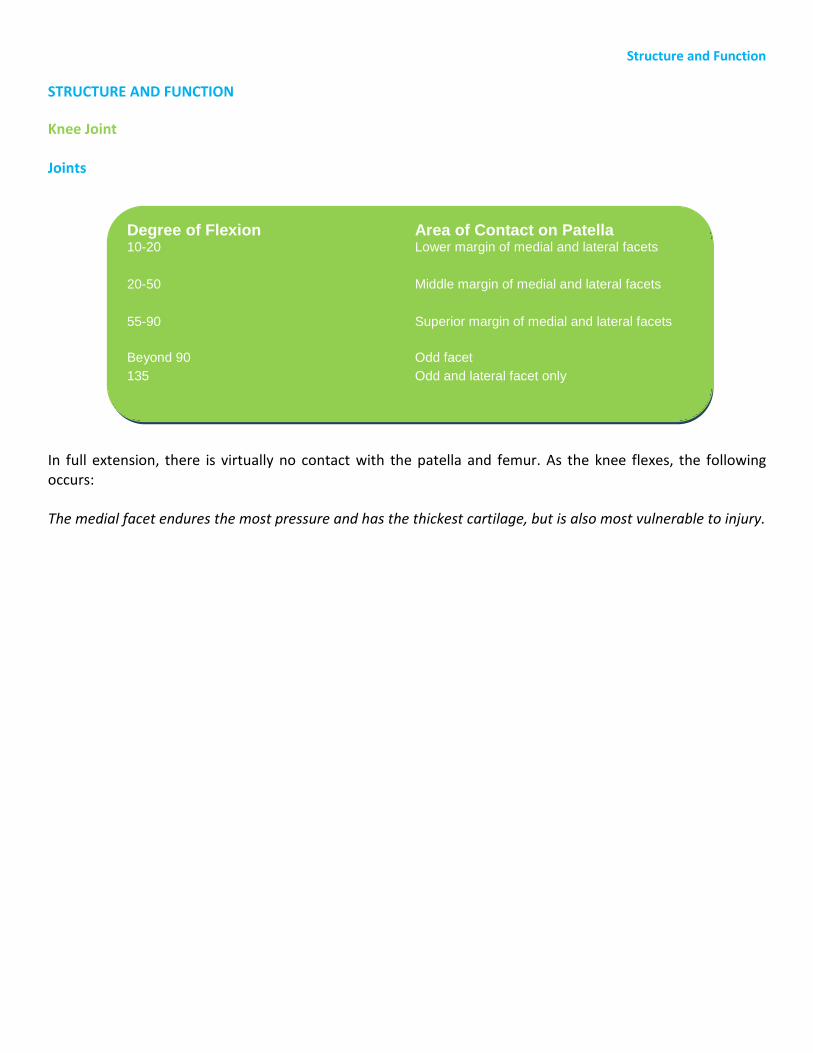
Knee Joint Joints In full extension, there is virtually no contact with the patella and femur. As the knee flexes, the following occurs: The medial facet endures the most pressure and has the thickest cartilage, but is also most vulnerable to injury.
Degree of Flexion Area of Contact on Patella 10-20 Lower margin of medial and lateral facets
20-50 Middle margin of medial and lateral facets
55-90 Superior margin of medial and lateral facets
Beyond 90 Odd facet 135 Odd and lateral facet only
Structure and Function STRUCTURE AND FUNCTION
Knee Joint Ligaments
Menisci The lateral and medial menisci, comprised of fibrocartilage, are thin centrally and thick peripherally. The functions of the menisci are as follows:
1. Increase congruity of the joint, reducing the stress on the tibial plateau and hyaline cartilage.
2. Spread lubrication from hyaline cartilage around the joint. 3. Increases nutrition of the joint. 4. Spreads weight-bearing forces on the joint, reducing mass per unit area. 5. Reduces joint friction. 6. Decreases risk of hyperextension.
Due to its firm attachment, the medial menisci is 20 times more likely to be injured than the lateral menisci. Furthermore, the semimembranosus and popliteus are attached to the medial and lateral meniscus, respectively, preventing trapping by the femur during flexion. Medial Collateral Ligament The MCL prevents genuvalgum and offers some resistance to lateral rotation and extension. It is most effective in full extension when the ligament is taut.
Lateral Collateral Ligament The LCL prevents genuvarum and also offers some resistance to lateral rotation and extension. Anterior Cruciate Ligament The ACL attaches posteriorly on the femur and anterior on the tibia, preventing anterior tibial translation (and medial rotation). Posterior Cruciate Ligament The PCL attaches anteriorly on the femur and posterior on the tibia, preventing posterior tibial translation (and medial rotation)

Structure and Function STRUCTURE AND FUNCTION
Knee Joint Biomechanics
Flexion/Extension During the flexion of the knee, the tibia moves from a slightly lateral position to a position medial to the femur due to the oblique axis. Furthermore, the axis moves posterior-superior with increasing flexion. Also, the femur must glide anteriorly during flexion to prevent the femur from rolling off the tibia. Locking and Unlocking During extension, the knee locks via medial rotation of the femur on the tibia in open-chain or lateral rotation of the tibia on the femur during closed chain. Ligament tautness, as well as joint architecture contributes to this phenomena. Conversely, the femur rotates laterally on the tibia in open chain or the tibia medially rotates on the femur during closed chain. This action is assisted by the popliteus. Patellar Forces In full extension, there is no joint compression on the patella. This force increases between 30-70 degrees of flexion. Due to the angle of the femur and the pull of the quadriceps, the patella tends to drift laterally, sometimes resulting in dislocation.

Structure and Function
Nerve Supply: Sciatic nerve: L5 – S1 Function(s): 1. Extension of hip (S) Gluteus maximus (A) Rectus femoris, iliopsoas, sartorius, tensor fascia lata, hip adductor group 2. Flexion of knee (S) Gastrocnemius, plantaris, popliteus (A) Quadriceps
STRUCTURE AND FUNCTION
Knee Joint The Hamstrings
Introduction The hamstrings play a huge role in most athletic activities. Not only do they attach to the pelvis and lower leg, they also form a fascial connection with the ligamentous structures of the pelvis and lumbar spine. As such, they are involved in explosive activities such as jumping, sprinting, and cycling. Like so many other muscles, the hamstrings function to restrict movement as much as creating movement. This is evident during trunk flexion, walking, running, jumping, and cycling as they fire eccentrically to control hip flexion. In controlling the lumbo-pelvic rhythm, the hamstrings are the first to contract, followed by the gluteus maximus, and finally, the erector spinae. During quiet standing, the hamstrings demonstrate very little activity. During walking, these muscles contract just prior to heel-strike and are active until toe-off. Characteristics The hamstrings are composed primarily of fast-twitch muscle fibres. Some sources report this percentage to be as high as 60.4%. These muscles do function tonically, however.

Structure and Function
Nerve Supply: Sciatic nerve: L5 – S1 Function(s): 1. Extension of hip (S) Gluteus maximus (A) Rectus femoris, iliopsoas, sartorius, tensor fascia lata, hip adductor group 2. Flexion of knee (S) Gastrocnemius, plantaris, popliteus (A) Quadriceps
STRUCTURE AND FUNCTION
Knee Joint The Hamstrings
Exercises Relatively, there has been a lot of research done on the hamstrings. So much so, separate studies have been conducted on activation patterns of the bicep femoris and the semitendinosus/semimembranosus. In order of greatest to least EMG activity, the following are the best exercises for the bicep femoris:
• Standing leg curls • Lying leg curls • Seated leg curls • Stiff-legged deadlifts
As for the semitendinosus/semimembranosus, the exercises are as follows:
• Seated leg curls • Standing leg curls • Lying leg curls • Stiff-legged deadlifts

Structure and Function
Nerve Supply: Sciatic nerve: L5 – S1 Function(s): 1. Extension of hip (S) Gluteus maximus (A) Rectus femoris, iliopsoas, sartorius, tensor fascia lata, hip adductor group 2. Flexion of knee (S) Gastrocnemius, plantaris, popliteus (A) Quadriceps
STRUCTURE AND FUNCTION
Knee Joint The Hamstrings
Research Tidbits Negative training for positive gains
A preseason strength training programme for the hamstring muscle group - emphasising eccentric overloading, enhanced performance and reduced injuries in elite Swedish male soccer players.
Askling C, Karlsson J, Thorstensson A. Hamstring injury occurrence in elite soccer players after preseason strength training with eccentric overload. Scand J Med Sci Sports. 2003 Aug;13(4):244-50.
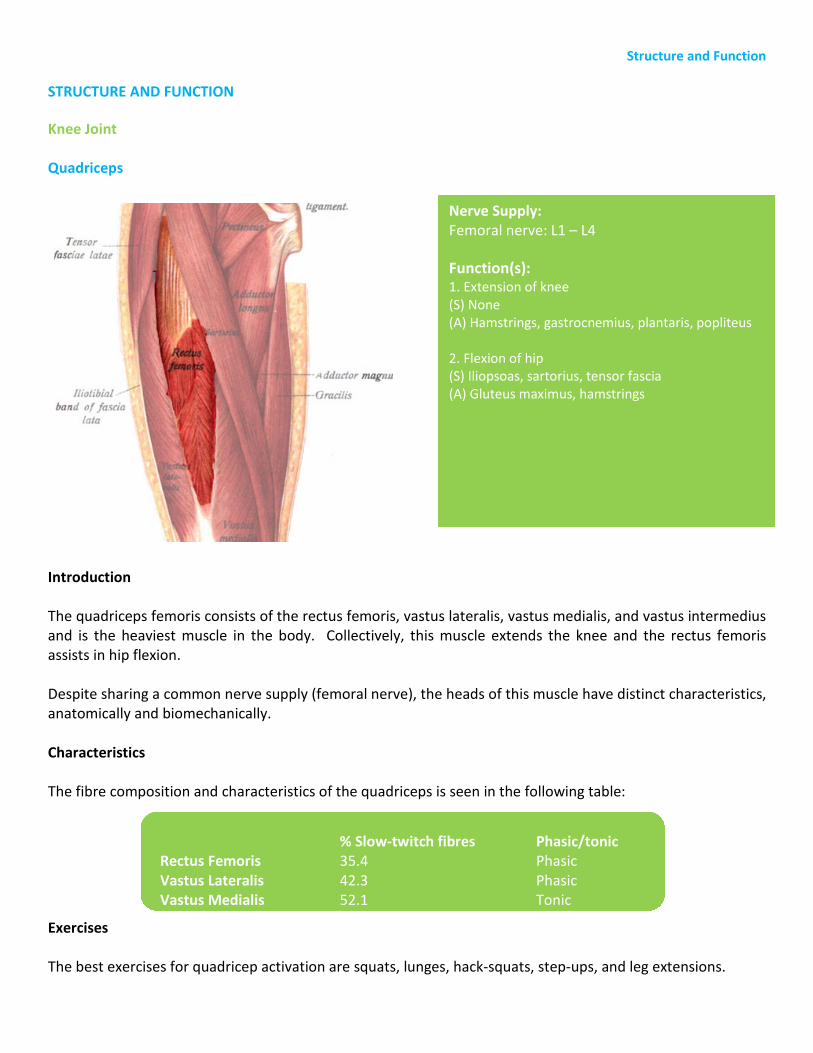
Structure and Function
Nerve Supply: Femoral nerve: L1 – L4 Function(s): 1. Extension of knee (S) None (A) Hamstrings, gastrocnemius, plantaris, popliteus 2. Flexion of hip (S) Iliopsoas, sartorius, tensor fascia (A) Gluteus maximus, hamstrings
STRUCTURE AND FUNCTION
Knee Joint Quadriceps
Introduction The quadriceps femoris consists of the rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius and is the heaviest muscle in the body. Collectively, this muscle extends the knee and the rectus femoris assists in hip flexion. Despite sharing a common nerve supply (femoral nerve), the heads of this muscle have distinct characteristics, anatomically and biomechanically. Characteristics The fibre composition and characteristics of the quadriceps is seen in the following table: Exercises The best exercises for quadricep activation are squats, lunges, hack-squats, step-ups, and leg extensions.
% Slow-twitch fibres Phasic/tonic Rectus Femoris 35.4 Phasic Vastus Lateralis 42.3 Phasic Vastus Medialis 52.1 Tonic

Structure and Function
Nerve Supply: Femoral nerve: L1 – L4 Function(s): 1. Extension of knee (S) None (A) Hamstrings, gastrocnemius, plantaris, popliteus 2. Flexion of hip (S) Iliopsoas, sartorius, tensor fascia (A) Gluteus maximus, hamstrings
STRUCTURE AND FUNCTION
Knee Joint Quadriceps
Research Tidbits Does depth matter?
Researchers studied the various contributions of the vastus lateralis (VL), vastus medialis obliquus (VMO), bicep femoris (BF), and gluteus maximus (GM) during squat at different depths .There were no significant differences between the relative contributions of the BF, the VMO, and the VL at different squatting depths. However, the GM, rather than the BF, the VMO, or the VL, becomes more active in concentric contraction as squat depth increases. Caterisano A, Moss RF, Pellinger TK, Woodruff K, Lewis VC, Booth W, Khadra T. The effect of back squat depth on the EMG activity of 4 superficial hip and thigh muscles. J Strength Cond Res. 2002 Aug;16(3):428-32.\

Structure and Function
Nerve Supply: Femoral nerve: L1 – L4 Function(s): 1. Extension of knee (S) None (A) Hamstrings, gastrocnemius, plantaris, popliteus 2. Flexion of hip (S) Iliopsoas, sartorius, tensor fascia (A) Gluteus maximus, hamstrings
STRUCTURE AND FUNCTION
Knee Joint Quadriceps
Research Tidbits Closed versus open-kinetic chain: the debate continues.
Researchers attempted to quantify knee joint biomechanics during open-kinetic chain exercises (OKCE) and closed-kinetic chain exercises (CKCE). The OCKE exercise was leg extension and the CKCE exercises were squats and leg press. The results were as follows: Overall, the squat generated approximately twice as much hamstring activity as the leg press and knee extensions. Quadriceps muscle activity was greatest in CKCE when the knee was near full flexion and in OKCE when the knee was near full extension. OKCE produced more rectus femoris activity while CKCE produced more vasti muscle activity. Tibiofemoral compressive force was greatest in CKCE near full flexion and in OKCE near full extension. Peak tension in the posterior cruciate ligament was approximately twice as great in CKCE, and increased with knee flexion. Tension in the anterior cruciate ligament was present only in OKCE, and occurred near full extension. Patellofemoral compressive force was greatest in CKCE near full flexion and in the mid-range of the knee extending phase in OKCE. Escamilla RF, Fleisig GS, Zheng N, Barrentine SW, Wilk KE, Andrews JR. Biomechanics of the knee during closed kinetic chain and open kinetic chain exercises. Med Sci Sports Exerc. 1998 Apr;30(4):556-69.

Structure and Function STRUCTURE AND FUNCTION Ankle Foot Complex The ankle joint, along with the joints of the foot, have two mutually exclusive functions – stability and mobility. This ankle-foot complex must adapt to uneven terrain and dissipate the forces of gait, while providing a rigid lever for toe-off and other weight-bearing activities. The movements at the ankle-foot complex are actually a combination of various joint rotations. The details of these, however, are beyond the scope of this course. Rather, the movements that are caused by the muscles that cross the ankle joint, will be discussed. These are principally plantarflexion, dorsiflexion, inversion, and eversion. With the knee extended, the range of motion for plantarflexion and dorsiflexion are 50 and 20, respectively. With the knee flexion, the range of motion in dorsiflexion increases slightly due to the reduced strain on the gastrocnemius muscle. Extreme dorsiflexion is limited by the contact of the talus with the distal tibiofibular joint. In some pathological conditions, such as subluxation of the talus, the range of dorsiflexion is reduced prematurely. Stretching the plantarflexors in this instance is not indicated. Rather, joint mobilizations and/or adjustments are required. Regardless of the position of the knee (or ankle for that matter), eversion and inversion are limited to 5 degrees each. Joints
Ankle Joint The ankle joint or mortis joint is the articulation between the talus and distal tibia/fibula The foot is actually laterally inclined 10-15 degrees from medial to lateral. There is one degree of motion, dorsiflexion and plantarflexion, at this joint. Tibiofibular Joint There are actually two tibiofibular joints, one distal and one proximal. The proximal joint (close to the knee) is a synovial joint and moves in the superior-inferior and anterior-posterior direction. The distal joint is rigid and considered a syndesmosis (fibrous). The direction of this fibrous ligament is inferior from lateral to medial, preventing superior movement of the fibula on the tibia. Subtalar Joint The subtalar joint allows for movement talus and calcaneus. Talocalcaneonavicular Joint; Transverse Tarsal Joint; Tarsal-Metatarsal Joint(s)

Structure and Function STRUCTURE AND FUNCTION Ankle Foot Complex Ligaments
Spring Ligament The spring ligament attaches the calcaneus to the navicular and acts to support the head of the talus. During pronation, the spring ligament provides a dampening effect, holding up the head of the talus. Medial Ligaments Lateral Ligaments Plantar Fascia

Structure and Function STRUCTURE AND FUNCTION Ankle Foot Complex Biomechanics
Spanish Windlass Effect During extension of the toes, plantar fascia (aponeurosis) tightens and pulls on the more proximal attachments, causing the foot to go into supination. Supination causes the foot structure to tighten, providing a rigid lever for toe-off. Arches of Foot
1. Medial Longitudinal Arch 2. Lateral Longitudinal Arch 3. Transverse Arch
Osteoligamentous Plate The vertically stacked ankle bones and horizontally stacked foot bones provide an arrangement by which vertically transmitted force forces all toes to be in contact with ground during toe off. This is achieved via tightening up of this plate. Strut/Tie-rod System The calcaneus, forefoot and plantar fascia act like a very stiff spring, offering a lot of resistance. With increasing load, the calcaneus moves posteriorly and forefoot moves anteriorly, tightening the aponeurosis between. Weight Distribution 50% of the weight loaded on one leg goes to the calcaneus, the other 50% going to the forefoot. There is 2:1 ratio of weight being distributed to the talus/navicular and calcaneus/cuboid, respectively. Metatarsals (2:1:1:1:1) – from medial (big toe) to lateral.

Structure and Function
Nerve Supply: Tibial nerve: S1 – S2 Function(s): 1. Plantarflexion (S) Soleus, plantaris (A) Tibialis anterior, extensor hallucis longus, extensor digitorum longus 2. Flexion of the knee (S) Hamstrings, gastrocnemius, popliteus (A) Quadriceps
STRUCTURE AND FUNCTION Ankle Foot Complex Gastrocnemius
Introduction The gastrocnemius is the visible muscle on the back of the leg. It consists of two portions, the lateral and medial heads. Unbeknownst to many, this muscle crosses the knee joint, imparting stability during weight-bearing. The main function of the gastrocnemius is plantarflexion of the ankle. Due to passive insufficiency, this function diminishes with increasing degrees of knee flexion. As mentioned previously, the gastrocnemius resists knee extension during weight bearing. When performing knee flexion exercises (leg curls), the gastrocnemius provides assistance to the hamstrings. Characteristics Depending on the source, the percentage of slow-twitch fibres in the gastrocnemius ranges from 43.5 to 56%. Interestingly, however, is the discrepancy in fibre type distribution between the medial and lateral head. More than half of the fibres in the lateral head are slow-twitch, whereas the medial head has been shown to have as little as 43.5% slow-twitch fibres. Even though this muscle can be classified as both phasic and tonic, it is usually deemed as phasic only.

Structure and Function STRUCTURE AND FUNCTION Ankle Foot Complex Gastrocnemius Characteristics As compared to most muscles, with an average ratio of 500 muscle fibres per motor unit, the gastrocnemius (and soleus) have a ratio of 2000 muscle fibres per motor unit. What are the implications? Of all the muscles in the human body, these two have the least refined motor control. Exercises Based on integrated EMG (IEMG) analysis, the following exercises are the best at recruiting the gastrocnemius (from highest to lowest activation)
• Donkey calf raises • Standing one-leg raises • Standing two-leg raises • Seated calf raises
Research Tidbits Achilles tendinosis and weight training
Researchers have demonstrated that heavy-load, eccentric calf training had a greater effect on symptom reduction of Achilles tendinosis (tendon degeneration) than did conventional treatment, consisting of rest, NSAIDS, Orthotics and/or physical therapy.
Alfredson H, Pietila T, Jonsson P, Lorentzon R. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med. 1998 May-Jun;26(3):360-6.
Active range of motion: the importance of specificity.
Researchers studying the effects of a 6-week program of static stretching of the calf muscle-tendon unit (MTU) on active ankle dorsiflexion range of motion (ADFROM) in healthy subjects found no significant improvement in active range of motion with a daily, 2 minute protocol of static stretching.
Youdas JW, Krause DA, Egan KS, Therneau TM, Laskowski ER. The effect of static stretching of the calf muscle-tendon unit on active ankle dorsiflexion range of motion. Orthop Sports Phys Ther. 2003 Jul;33(7):408-17.

Structure and Function
Nerve Supply: Superficial fibular nerve: L5 – S2 Function(s): 1. Eversion (S) None (A) Tibialis anterior, tibialis posterior
STRUCTURE AND FUNCTION Ankle Foot Complex Peroneals (Fibularis Group)
Introduction The peroneals are the evertors of the ankle joint. Like many other muscles, they function to resist movement rather than produce it. Characteristics The peroneals are predominantly slow-twitch, at around 63% and function tonically. Exercises This muscle is active during most weight-bearing exercises. Unless one wishes to rehabilitate the peroneals, as in cases of ankle sprains, this muscle will get sufficient work in closed-kinetic chain, weight-bearing exercises.

Structure and Function STRUCTURE AND FUNCTION Ankle Foot Complex Peroneals (Fibularis Group) Research Tidbits Preventing Ankle Sprains
In the Journal of Athletic Therapy, researchers published a study to determine whether patients with chronic ankle instability or a history of ankle sprains without chronic instability had worse proprioception or less invertor and evertor muscle strength than those with normal ankles. The results were as follows: statistical analysis indicated significantly less accurate active position sense for the instability group compared with the control group at a position close to maximal inversion. The instability group also showed significantly lower relative eversion muscle strength (% body weight). No significant differences were observed between the control group and the groups with past sprains without instability. The researchers concluded suggest that the possible cause of chronic ankle instability is a combination of diminished proprioception and evertor muscle weakness. They emphasized proprioception and strength training in the rehabilitation program for ankle instability. Willems T, Witvrouw E, Verstuyft J, Vaes P, De Clercq D. Proprioception and Muscle Strength in Subjects With a History of Ankle Sprains and Chronic Instability. J Athl Train. 2002 Dec;37(4):487-493.

Structure and Function
Nerve Supply: Tibial nerve: S1-S2 Function(s) 1. Plantarflexion (S) Gastrocnemius (A) Tibialis anterior, extensor hallucis longus, extensor digitorum longus
STRUCTURE AND FUNCTION Ankle Foot Complex Soleus
Introduction The soleus lies deep to the gastrocnemius, to which it shares a common insertion on the Achilles tendon. The only function of the soleus is plantarflexion of the ankle. Unlike the gastrocnemius, this function does not diminish with increasing degrees of knee flexion. Rather, the soleus is called upon solely during knee flexion. The soleus, as well as the iliopsoas, is active during quiet standing. Characteristics Most sources agree that the percentage of slow-twitch fibres in the soleus is around 75%. This should make sense as this muscle is constantly activity in all weight-bearing activities. As compared to most muscles, with an average ratio of 500 muscle fibres per motor unit, the soleus (and gastrocnemius) have a ratio of 2000 muscle fibres per motor unit. What are the implications? Of all the muscles in the human body, these two have the least refined motor control. Exercises Based on integrated EMG (IEMG) analysis, the following exercise is the best at recruiting the soleus:
• Seated calf raises

Structure and Function STRUCTURE AND FUNCTION Ankle Foot Complex Soleus Research Tidbits Achilles tendinosis and weight training
Researchers have demonstrated that heavy-load, eccentric calf training had a greater effect on symptom reduction of Achilles tendinosis (tendon degeneration) than did conventional treatment, consisting of rest, NSAIDS, orthotics and/or physical therapy.
Alfredson H, Pietila T, Jonsson P, Lorentzon R. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med. 1998 May-Jun;26(3):360-6.
Active range of motion: the importance of specificity.
Researchers studying the effects of a 6-week program of static stretching of the calf muscle-tendon unit (MTU) on active ankle dorsiflexion range of motion (ADFROM) in healthy subjects found no significant improvement in active range of motion with a daily, 2 minute protocol of static stretching.
Youdas JW, Krause DA, Egan KS, Therneau TM, Laskowski ER. The effect of static stretching of the calf muscle-tendon unit on active ankle dorsiflexion range of motion. Orthop Sports Phys Ther. 2003 Jul;33(7):408-17.

Structure and Function
Nerve Supply: Deep fibular nerve: L4-L5 Function(s) 1. Dorsiflexion (S) Extensor digitorum/hallucis longus, peroneus tertius (A) Gastrocnemius, soleus, tibialis posterior, flexor digitorum/hallucis longus 2. Inversion (S) Tibialis posterior (A) Peroneals
STRUCTURE AND FUNCTION Ankle Foot Complex Tibialis Anterior
Introduction The tibialis anterior is the major dorsiflexor of the ankle. In weight-bearing, it controls backward sway and helps maintain the medial arch of the foot. During walking, running, and sprinting, it allows the foot to clear the ground shortly after toe-off and just before heel-strike (swing phase). Characteristics Its slow-twitch fibres predominate at around 73% (sources vary). Exercises This muscle is active during most weight-bearing exercises. Furthermore, it is usually implicated in cases of shin splints and/or compartment syndrome. Unless one’s goal is hypertrophy or rehabilitation, this muscle is better left untouched.
Glossary GLOSSARY
Active Insufficiency
The inability of a two-joint (or multi-joint) muscle to generate an effective force when placed in a fully shortened position.
Adaptive Shortening
Tightness that occurs as a result of a muscle remaining in a shortened position.
Agonist
A contracting muscle whose action is opposed by another muscle (antagonist).
Antagonist
A muscle that works in opposition to another muscle (agonist); opponent.
Concentric Muscle Action
Muscle shortening under tension. This shortening occurs when the net moment developed by a muscle and its synergists is greater than the moment caused by the external forces acting on the segment to which the muscle is attached.
Contraindication
A sign or symptom that indicates that a particular treatment or procedure is not appropriate.
Dysfunction
Inability to function properly.
Eccentric Muscle Action
Muscle lengthening under tension. This lengthening occurs when the external force acting on the segment to which a muscle is attached causes a net moment that is greater than the moment that is being developed by the muscle and its synergists.
Force-Velocity Relationship
At any given length, the speed of shortening or lengthening of a muscle that is stimulated at a constant level will depend on the force that is applied to the ends of the muscle. The Hill equation, best known of the force-velocity equations, describes mathematically the fact that light loads can be lifted quickly but heavy loads only slowly. Although it is often stated that maximal muscle force is available at zero velocity (isometric action), the highest loads are achieved during eccentric muscle action.

Glossary GLOSSARY
Indication
A sign or symptom that indicates that a particular treatment or procedure is appropriate.
Insertion
The more distal attachment of the muscle or the attachment that is more mobile. Again, this is an ambiguous term for which attachment should be substituted.
lsokinetic Muscle Action
Muscle action in which the rate of shortening or lengthening of the muscle is constant. Because joint geometry makes this impossible to determine in vivo, the definition is usually relaxed to apply either to a constant velocity of the load being lifted or resisted, or to a constant angular velocity of the joint.
Isometric Muscle Action
Muscle action that involves no change in length of the muscle or joint.
Isotonic Muscle Action
Muscle action that involves the production of a constant force. For in vivo muscle actions, the term is also commonly used both when the joint moment is constant over a range of motion and when a constant load is being moved through a distance. It is important to realize, however, that because of the leverage effects at the joint; the force developed by the muscles in both these cases will actually be changing, rendering them non-isotonic.
Origin
The source or beginning of a muscle. The term generally refers to the more fixed end or the more proximal end.
This is an ambiguous term for any muscle that has attachments that are equally mobile or with both attachments in the same transverse plane. Use of the term tends to encourage the mistaken notion that muscles have their only action at the moveable rather than the fixed end. The same tension is, of course, applied to both ends. The term attachment is more appropriate for reference to either end of the muscle.
Overstretch Weakness
Weakness in a two-joint (or multi-joint) muscle resulting from repetitive movements or habitual positions that elongate the muscle beyond normal range of muscle length.

Glossary GLOSSARY
Passive Insufficiency
Shortness of a two-joint (or multi-joint) muscle; the length of a muscle is not sufficient to permit normal elongation over both joints simultaneously.
Power
Power is the rate of doing work. Power is equal to the work done divided by the time during which the work is being done: P = W/t.
Stretch Weakness
Weakness that results from muscles remaining in an elongated condition, however slight, beyond he neutral physiological rest position, but not beyond the normal range of muscle length.
Tension-Length Relationship
The variation in force output of a muscle, with the same neural input, over a range of lengths. The reasons for this variation include a change in the number of possible active sites for cross-bridge formation and the effect of the elastic tissues that are in parallel with the contractile tissue.
The moment that the muscle can develop about a joint will vary both according to the tension-length relationship and as a function of the geometry of the joint (the location of its attachments and so forth).
Work
Work is done when a force moves an object through a distance. Whenever a constant force exists and motion takes place in a straight line, then work equals the magnitude of the force (F) times the distance (d) through which the object moves: W = F × d
According to this definition, no mechanical work is done during isometric action of a muscle. An ongoing debate about the implications of this exists because any muscle action clearly involves the expenditure of metabolic energy.


References REFERENCES Saal, JA, Saal, JS (1989) Nonoperative treatment of herniated lumbar intervertebral disc with radiculopathy. An outcome study. Journal of Biomechanics, 14: 4321-437. Parks, KA, Crichton, KS, Goldford, RJ, McGill, Sm. A comparison of lumbar range of motion with functional ability scores on low back pain patients: Assessment of the validity of range of motion. Marras, WS, Davids KG, Heaney, CA, Maronitis,AB, Allread, WG, (2000) The influence of psychosocial stress, gender, and personality on mechanical loading of the lumbar spine. Spine 25: 3045-3054. Porter, RW (1987) Does hard work prevent disc protrusion? Clinical Biomechanics, 2: 196-198. Videman, T, Battie, MC, Gill, K, Manninen, H, Gibbons, LE, Fisher, LD (1995). Magnetic resonance imaging findings and their relationships in the thoracic and lumbar spine. Insights into the etiopathogenesis of spinal degeneration. Spine, 20 (8): 928-935. Biering-Sorenson, F. (1984). Physical measurements as risk indicators for low-back trouble over a one-year period. Spine, 9: 106-119. Luoto, S, Heliovaara, M, Hurri, H, Alarenta, M. (1995). Static back endurance and the risk of low back pain. Clinical biomechanics, 10: 323-324. Axler, CT, McGill, SM (1997). Choosing the best abdominal exercise based on knowledge of tissue loads. Medicine and Science in Sports and Exercise, 29: 804-811. Battie, MC, Gigos, SJ, Fisher, LD, Spengler, Dm, Hansoson, TH, Nachemson, Al, Wortley, MD. (1990). The role of spinal flexibility in back pain complaints with industry: A prospective study. Spine 15: 768-773. Burton, AL, Tillsotson, KM, Troup, JDG. (1989) Prediction of low back trouble frequency in a working population. Spine, 14: 939-946. Adams, MA, Hutton, WC, Stott, JRR (1980). The resistance to flexion of the lumbar intervertebral joint. Spine 5: 245. Bigos, SJ, Spengler, Dm, Martin, NA, Zeh, A, Fisher, L, Nachemson, A, and Wange, MH (1986). Back injuries in industry: A retrospective study. II Injury factors, Spine 11: 246-251. Marras, WS, Lavender, SA, Leurgans, SE, Fathallah, FA, Ferguson, SA, Allread, WG, and Rajulu, Sl (1995). Biomechanical risk factors for occupationally related low back disorders. Ergonomics, 38: 377-410. Norman, R, Wells, R, Neumann, P, Frank, P, Shannon, H, Kerr, M (1988). A comparison of peak vs. cumulative physical work exposure risk factors for the reporting of low back pain in the automotive industry. Clinical Biomechanics, 13: 561-573.

References REFERENCES Punnet, L, Fine, LJ, Keyerseling, Wm, Herrin, GD, Chaffin, DA (1991). Back disorders and non-neutral trunk postures of automobile assembly workers. Scandinavian Journal of Work Environment and Health, 17: 337-346. Arendt-Nelson, L, Graven-Neilson, T, Starrer, H, Svensson, P. (1995). The influence of low back pain on muscle activity and coordination during gait. Pain 64: 231-240. Grabiner, MD, Koh, TJ, Ghazawi, AE (1992). Decoupling of bilateral excitation in subjects with low back pain Spine, 17: 1219-1223. Rantanen, j, Hurme, M, Falck, B (1993). The lumbar multifidus five years after surgery for a lumbar intervertebral disc herniation. Spine, 18: 568-574. McGill, SM, Sharratt, MT, Seguin, JP (1995) Loads on spinal tissues during simultaneous lifting and ventilatory challenge. Ergonomics, 38: 1772-1792. Callaghan, J, McGill, Sm (1996). Mechanical stability of the in vivo lumbar spine: Implications for injury and chronic low back pain. Clinical Biomechanics, 11 (1): 1-15. (Ch. 11) McGill, SM (2001) Low back stability: From formal description to issues for performance and rehabilitation. Exercise and Sports Science Reviews, 29(1): 26-31. Porterfield, JA, DeRosa, C. (1998). Mechanical low back pain: Perspectives in functional anatomy. Philadelphia, WB Saunders. Lehman, G, McGill, Sm (2001). Quantification of the differences in EMG magnitude between upper and lower rectus abdominus during selected trunk exercises. Physical Therapy, 81: 1096-1101. Henke, KG, Sharratt, MT, Pegelow, D, Dempsey, JA (1988). Regulation of end-expiratory lung volume during exercise. Journal of Applied Physiology, 64: 135-146. Juker, D, McGill, SM, Kropf, P, Steffen, T. (1998). Quantitative intramuscular myoelectric activity of lumbar portions of psoas and the abdominal wall during a wide variety of tasks. Medicine and Science in Sports and Exercise, 30 (2): 301-310. Santaguida, P, McGill, SM (1995). The psoas major muscle: a three-dimensional mechanical modeling study with respect to the spine based on MRI measurement. Journal of Biomechanics, 28: 339-345. Tesh, KM, Dunn, J, Evans, JH 91987). The abdominal muscles and vertebral stability. Spine, 12(5): 501 Macintosh, JE, Bogduk, N, Gracovetsky, S, (1987). The biomechanics of the thoracolumbar fascia. Clinical Biomechanics, 2: 78. McGill, Norman, RW (1988). The potential of lumbodorsal fascia forces to generate back extension moments during squat lifts. Journal of Biomedical Engineering, 10:312.

References REFERENCES Adams, M, Dolan, P. (1995). Recent advances in lumbar spinal mechanics and their clinical significance. Clinical Biomechanics, 10 (1): 3. Callaghan, JP, McGill, SM, Norman, RW (1999). The IAP mechanism for stabilizing the lumbar spine. Journal of biomechanics, 32(1): 13-17.