Embed Size (px)
Citation preview

PROBLEMS IN DIAGNOSTIC IMAGING
Fluoroscopic Angiography in the Gross AnatomyDissection Laboratory: Visualizing the Aortic
Arch and Its Branches in a Cadaver
KEITH M. VOGT, COURTNEY Y. KAUH, DAVID M. HOLDER,AND ROBERT M. DEPHILIP*
Division of Anatomy, College of Medicine, The Ohio State University, Columbus, Ohio
We present fluoroscopic images of the aortic arch and its branches obtained ina first year medical gross anatomy teaching laboratory after an aberrant rightsubclavian artery was discovered during dissection. The aortic arch and itsbranches in the cadaver were filled with contrast medium in molten agar. Afterthe agar solidified, a portable fluoroscope was used to obtain radiographicimages. These post-mortem images were then compared with computed to-mography images obtained while the individual was living. The embryology,prevalence, and clinical findings of this arterial variation are reviewed, and theimportance of recognizing the presence of an aberrant right subclavian arterybefore performing various procedures is discussed. This exercise gave stu-dents the unique opportunity to compare the three-dimensional anatomy seenin the dissection laboratory with the two-dimensional presentation of thatsame anatomy in the radiographic images that they will see in clinical practice.Clin. Anat. 24:253–257, 2011. VVC 2010 Wiley-Liss, Inc.
Key words: aberrant subclavian artery; anatomical variation; fluoroscopy;retroesophageal subclavian artery
INTRODUCTION
Dissection in an introductory anatomy course pro-vides students with a unique opportunity to appreci-ate how variations in anatomical structure haveimplications for predisposition to illness, interpreta-tion of clinical findings including imaging studies, andthe planning of clinical procedures (Zucconi et al.,2002). In the case presented here, medical studentsin a first year anatomy course identified a commonvariation in the branching pattern of the aortic arch.This discovery raised several questions: Was the do-nor aware of this anatomical variation while living?Had the variation produced any symptoms duringlife? Could this variation have been identified onimaging studies performed while the donor was liv-ing? To simulate the appearance of a chest radio-graph of the donor taken while he was living, thestudents developed a procedure using fluoroscopy tovisualize the aortic arch and its branches in acadaver. They filled the aortic arch and its brancheswith radiologic contrast medium in molten agar, and
after allowing the agar to solidify, obtained imagesusing a portable fluoroscope that had been retiredfrom hospital service. In addition, they received per-mission from the donor’s family to obtain the medicalrecords of the donor and were then able to correlatetheir findings from dissection and post-mortemimaging with the donor’s medical history and withimages obtained while the donor was alive. Theresults of their investigation are presented here as aproblem in diagnostic imaging. An anterior view ofthe aortic arch and its branches in this cadaver wasobtained using fluoroscopy and is shown in Figure 1.
*Correspondence to: Robert M. DePhilip, Division of Anat-omy, College of Medicine, The Ohio State University, 279Hamilton Hall, 1645 Neil Avenue, Columbus, OH 43210,USA. E-mail: [email protected]
Received 2 July 2010; Revised 15 September 2010; Accepted16 September 2010
Published online 29 October 2010 in Wiley Online Library(wileyonlinelibrary.com). DOI 10.1002/ca.21080
VVC 2010 Wiley-Liss, Inc.
Clinical Anatomy 24:253–257 (2011)

The reader is challenged to identify the branches ofthe aortic arch, given the hint that this image dem-onstrates the most common arterial variation of theaortic arch. We then discuss the embryology andprevalence of this variation, and the importance ofbeing aware of it as invasive procedures in the neckand upper thorax are being performed.
MATERIALS AND METHODS
A mixture of 1% agarose in radiologic contrastmedium was prepared by adding 1 g of agarose, mo-lecular biology grade (Sigma Chemical Company, St.Louis, MO) to 100 ml of Hypaque-Cysto (DiatrizoateMeglumine Injection, USP) 30% (Amersham Health,Inc., Princeton, NJ) with stirring on a hotplate. Whenthe agarose was dissolved completely, the mixturewas added to a 50-cc syringe fitted with a 10-inchlength of plastic tubing. The tubing was inserted indi-vidually into the vessels branching from the aorticarch and each vessel was filled selectively with themolten medium, and the mixture was allowed toharden. Finally, the arch of the aorta was filled withthe molten mixture. Smaller vessels, such as thevertebral arteries or the internal thoracic arterieswere not filled intentionally, so that the aortic arch
and the great vessels could be viewed without over-lap of these other vessels. Vessels that had been cutinadvertently during the student dissection wereclosed with suture to prevent leakage of the contrastmedium. These sutures were removed after the mol-ten mixture hardened and before the specimen wasimaged and photographed. The students performedthe above procedures under the guidance of the fac-ulty author (RMD).
The fluoroscope was a Model 9400 manufacturedby OEC Medical Systems, Inc. (Salt Lake City, UT).To minimize radiation exposure, all personnel whowere present in the lab during fluoroscopic imagingwore lead aprons and stood as far from the x-raygenerator as possible. Only the faculty author oper-ated the fluoroscope and his radiation exposure wasmonitored using a whole-body badge dosimeter.
ANSWER AND COMMENTARY
Figure 2A is a labeled version of the fluorographshown in Figure 1 and identifies an aberrant right sub-clavian artery (ARSA) labeled ‘‘a.’’ In this anteriorview, the right common carotid artery and the ARSAare superimposed, and in the area of overlap, theyresemble the more familiar appearance of the
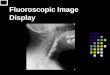
Fig. 1. Fluoroscopic aortogram (anterior view) ofthe cadaver of a 79-year-old male whose cause ofdeath was colon cancer with lung metastases. Theaortic arch and its branches were filled with contrastmedium in molten agar that was allowed to solidify
before imaging with a portable fluoroscope. Theheart was removed during dissection and does notappear here. Can the branches of the aortic arch beidentified? Can any aberrant branches of the arch beidentified?
254 Vogt et al.

brachiocephalic trunk. The fluorograph in Figure 2B isan oblique view showing that the ARSA and the rightcommon carotid artery are indeed separate struc-tures. Figure 2C is a photograph of the dissected spec-imen from the same anterior view as the fluorographin Figure 2A. The portion of the ARSA posterior to thetrachea and esophagus is hidden from view. Figure 2Dis a photograph of the dissected specimen in the sameoblique view as the fluorograph in Figure 2B. The tra-
chea and the esophagus have been removed to showthe retroesophageal course of the ARSA.
DISCUSSION
Normally, the right subclavian artery is formedfrom three components: the fourth pharyngeal archartery on the right side, the proximal part of the dor-
Fig. 2. A: Fluoroscopic aortogram (anterior view).This is a labeled version of Figure 1. The arrowheadsindicate the retroesophageal portion of the ARSA. B:Fluoroscopic aortogram (same specimen as in A,but now an oblique view, 308 off the anterior viewshown in A. C: Photograph of the dissected specimen,taken from an anterior view corresponding to A. D:Photograph of the dissected specimen, taken from an
oblique view corresponding to B. In D, the trachea andupper part of the esophagus have been removed tobetter visualize the course of the ARSA. a, ARSA; b,right common carotid artery; c, left common carotidartery; d, left subclavian artery; arrowheads, retroeso-phageal portion of the ARSA; E, esophagus; G, lobesof the thyroid gland; S, anterior scalene muscles; T,trachea.
255Fluoroscopy in the Dissection Laboratory

sal aorta between the fourth arch artery and the sev-enth intersegmental artery, and the seventh inter-segmental artery itself (Moore and Persaud, 2008).An ARSA forms when the right fourth pharyngealarch artery and the proximal right dorsal aorta bothinvolute, and the distal part of the right dorsal aortamaintains a connection between the right seventhintersegmental artery and the thoracic aorta (Mooreand Persaud, 2008). The origin of the ARSA from thethoracic aorta is usually just distal to the origin ofthe left subclavian artery. A diverticulum may bepresent at the point at which the ARSA branchesfrom the aorta (Salomonowitz et al., 1984). Themost common course of the ARSA as it crossesthe midline is between the vertebral column and theesophagus, though passage between the tracheaand esophagus, or anterior to both structures hasbeen reported (Holzapfel, 1899).
Felson et al. (1950) set the prevalence of an ARSAat 0.4–2.0%, based on a review of various authorsreporting findings made at autopsy. More recently,Easterbrook et al. (1992) and Phillips et al. (1993)studied magnetic resonance images of the cervicalspine and reported the prevalence of an ARSA to be1.3% and 0.6%, respectively. In a retrospectivestudy, Ramaswamy et al. (2008) searched the pedi-atric echocardiography database at their institutionand found a total of 226 (1.42%) instances of anaberrant subclavian artery in a total of 15,871 echo-cardiograms. Of these 226, 171 (1.1%) were anARSA associated with a left-sided aortic arch, and 55(0.3%) were an aberrant left subclavian artery asso-ciated with a right-sided aortic arch.
The anomalous origin and course of the ARSAdemonstrated in this study were discovered whenfirst-year medical students dissected the neck andthorax of the cadaver of a 79-year-old male. In thisindividual, the right common carotid artery was thefirst branch of the aortic arch, taking an obliquecourse across the midline, and approximating thepath of the brachiocephalic trunk, if that artery had
been present. The right common carotid artery thenturned and followed a normal course in the neck.The left common carotid and left subclavian arteriesbranched in normal sequence from the arch. Noother arterial or venous branching abnormalitieswere noted and there was no diverticulum present atthe origin of the ARSA.
The medical records of this patient were reviewedto determine whether this anatomical variation hadproduced any symptoms. Although an ARSA is themost common variation of the branches of the aorticarch, and a dramatic variation at that, it is usuallyasymptomatic. When present, symptoms includedysphagia from compression of the esophagus and,less commonly, brachial claudication from occlusionof the artery (Kieffer et al., 1994). This donor had norecord of clinical symptoms that could be correlatedwith his aberrant anatomy.
Our donor was diagnosed with colon cancer andlung metastases, and had frequent chest radio-graphs and computed tomography (CT) scansperformed over the course of several years to eval-uate the progression of disease. Plain chest radio-graphs did not reveal any mediastinal abnormalities.Our post-mortem fluoroscopic study was under-taken to determine how the aberrant artery mighthave appeared on a conventional chest radiographobtained during life. As shown in an anterior view(Fig. 2A), the right carotid artery is superimposedon the ARSA and gives the appearance of a singlestructure resembling the brachiocephalic trunk withtwo terminal branches. However, an image obtainedat an oblique angle (308 off the anterior view) dif-ferentiates the two arteries masquerading as one(Fig. 2B).
Proto et al. (1987) noted three signs on anteriorchest radiographs and three other signs on lateralchest radiographs of patients with a proven ARSA.The radiodensity produced by the ARSA at thearrowheads in Figure 2A resembles the ‘‘vesselthrough trachea’’ sign as the artery passes posterior
Fig. 3. Axial slices from a contrast-enhanced,computed tomography scan of the thorax of the donorobtained from his medical records. Slice A is superiorto slice B. In A, the ARSA (arrow) is seen in its posi-tion between the esophagus and the vertebral column.
Note compression of the esophagus by the ARSA.In B, the ARSA (arrow) is seen near its originfrom the aorta, distal to the origin of the left subcla-vian artery. The left subclavian artery is indicatedwith an asterisk.
256 Vogt et al.

to the trachea and esophagus. The effort made bythese authors to provide signs of an ARSA on chestradiographs suggests the difficulty of visualizing thisstructure using conventional radiography.
On the other hand, contrast-enhanced CT studiesclearly demonstrated the ARSA, as shown in Figure 3.This finding emphasizes how multislice axial imagingcan resolve anatomical features that may be unclearin conventional radiographic images. It was interest-ing that the presence of the ARSA was not noted inthe radiology reports from any of the several CTstudies performed on this patient during his life.
Recognition of an ARSA is of obvious importancein those cases where the abnormal course of the ar-tery provides an explanation for the patient’s pre-senting symptoms. Moreover, a number of casereports show that asymptomatic individuals canbenefit from identification of variations in the anat-omy of their right subclavian artery as they undergovarious invasive procedures or surgeries. Nasogas-tric intubation in an otherwise healthy 17-year-oldpostpartum patient with an unknown retroesopha-geal ARSA resulted in an arterio-esophageal fistulathat caused massive hematemesis and, ultimately,exsanguination (Merchant et al., 1977). In anothercase involving repair of an aortic aneurysm, anunrecognized, distally branching ARSA contributed tocerebral ischemia when the aorta was cross-clampedproximal to both subclavian arteries, compromisingblood flow to the vertebral arteries, leading to comaand death (Weinberger et al., 1977). A more positiveoutcome was achieved when an ARSA was recog-nized during surgical repair of an aortic aneurysmand the aberrant artery was used to maintaincerebral vascular supply (Bednarkiewicz et al.,2003). It has also been emphasized that prior knowl-edge of an ARSA will inform the surgeon duringthyroid surgery that the laryngeal nerve will not bein its usual recurrent position and may reach thelarynx as a direct branch of the vagus nerve (Coadyet al., 2000).
This exercise answered the questions raised ini-tially by the students when they discovered this vari-ant anatomy during dissection. Since there was nomention of dysphagia in the medical records of thedonor, the ARSA probably did not produce clinicalsymptoms, and it is likely that the donor wasunaware of his variant anatomy during life. The stu-dents learned that an ARSA is difficult to identify ona conventional chest radiograph, and though easilyrecognized on a contrast-enhanced CT scan, it is notalways reported. Finally, the students becameacutely aware that knowledge of anatomical varia-tion can play a role in the interpretation of a patient’ssymptoms and the planning for surgery or aninvasive procedure. The exercise underscores thepotential of the dissection laboratory to provide an
investigative experience that can engage students incritical thinking and problem solving.
ACKNOWLEDGMENTS
The authors thank Duane L. Hart, Clinical Engi-neering Manager, Ohio State University Hospitals,for arranging the transfer of the fluoroscope to theDivision of Anatomy, and Jeanne C. McGuire, HealthPhysicist, and Robert E. Peterson, Jr., UniversityRadiation Safety Officer, Ohio State University Envi-ronmental Health and Safety, for fluoroscopy per-sonnel training and for performing annual safetyinspections of the instrument.
REFERENCES
Bednarkiewicz M, Bruschweiler I, Christenson JT. 2003. Undiag-nosed aberrant right subclavian artery: Pitfall in aortic surgery.Cardiovasc Surg 11:61–63.
Coady MA, Adler F, Davila JJ, Gahtan V. 2000. Nonrecurrent laryn-geal nerve during carotid artery surgery: Case report and litera-ture review. J Vasc Surg 32:192–196.
Easterbrook JS. 1992. Identification of aberrant right subclavian ar-tery on MR images of the cervical spine. J Magn Reson Imaging2:507–509.
Felson F, Cohen S, Courter SR, McGuire J. 1950. Anomalous rightsubclavian artery. Radiology 54:340–349.
Holzapfel G. 1899. Ungewohnlicher Ursprung und Verlauf der Arteriasubclavia dextra. Anat Hefte 12:369–523.
Kieffer E, Bahnini A, Koskas F. 1994. Aberrant subclavian artery:surgical treatment in thirty-three adult patients. J Vasc Surg19:100–109.
Merchant FJ, Nichols RL, Bombeck CT. 1977. Unusual complicationof nasogastric esophageal intubation-erosion into an aberrantright subclavian artery. J Cardiovasc Surg (Torino) 18:147–150.
Moore KL, Persaud TVN. 2008. The Developing Human: ClinicallyOriented Embryology. 8th Ed. Philadelphia: Saunders Elsevier.p 317–325.
Phillips WE II, Murtagh FR, Brenner J. 1993. Recognition of theaberrant right subclavian artery on cervical spine. MR AJNR Am JNeuroradiol 14:1405–1406.
Proto AV, Cuthbert NW, Raider L. 1987. Aberrant right subclavianartery: Further observations. AJR Am J Roentgenol 148:253–257.
Ramaswamy P, Lytrivi ID, Thanjan MT, Nguyen T, Srivastava S,Sharma S, Ko HH, Pamess IA, Lai WW. 2008. Frequency ofaberrant subclavian artery, arch laterality, and associated intra-cardiac anomalies detected by echocardiography. Am J Cardiol101:677–682.
Salomonowitz E, Edwards JE, Hunter DW, Castaneda-Zuniga WR,Lund G, Cragg AH, Amplatz K. 1984. The three types of aorticdiverticula. AJR Am J Roentgenol 142:673–679.
Weinberger G, Randall PA, Parker FB, Kieffer SA. 1977. Involvementof an aberrant right subclavian artery in dissection of thethoracic aorta: Diagnostic and therapeutic implications. AJR AmJ Roentgenol 129:653–655.
Zucconi WB, Guelfguat M, Solounias N. 2002. Approach to the edu-cational opportunities provided by variant anatomy, illustratedby discussion of a duplicated vena cava. Clin Anat 15:165–168.
257Fluoroscopy in the Dissection Laboratory