-
J Korean Neurosurg Soc/Volume 28/November, 1999 1606
KISEP Clinical Research J Korean Neurosurg Soc 28::::1606-1612,
1999
거대뇌하수체선종의 외과적 치료*
성균관대학교 의과대학 삼성서울병원 신경외과학교실
김종현·박 관·조병문·남도현·이정일·황순구·김종수·홍승철·신형진·어 환 = Abstract =
Surgical Management of Giant Pituitary Adenomas
Jong Hyun Kim, M.D., Kwan Park, M.D., Byung Moon Cho, M.D.,
Do-Hyun Nam, M.D., Jung Il Lee, M.D., Soon-Gu Hwang, M.D.,
Jong-Soo Kim, M.D., Seung-Chyul Hong, M.D., Hyung-Jin Shin,
M.D., Whan Eoh, M.D.
Department of Neurosurgery, Samsung Medical Center, Sung Kyun
Kwan University School of Medicine, Seoul, Korea
bjective:Giant pituitary adenomas are rare. The location of
these adenomas are close to vital neural and vascular structures
with widespread extensions that makes the radical surgical
management difficult.
Methods:From October 1994 to August 1998, we experienced 20
patients with giant pituitary adenomas out of 178 surgically
treated pituitary adenoma patients. Giant pituitary adenoma was
diagnosed on the basis of the longest
diameter of being more than 4cm in MRI scan. We reviewed the
clinical presentation, types of tumor, size and degree
of suprasellar or parasellar extension, routes of surgical
approach, postoperative surgical outcomes and complica-
tions.
Resuts:The incidence of giant pituitary adenomas was 11%. The
most common chief complaint was visual disturb-ance(n=16). The
non-functioning adenoms(n=16) were the majority and the other 4
patients were functioning
adenomas(prolactinoma n=2, acromegaly n=1, cushing’s disease
n=1). The patients underwent transsphenoidal approach(TSA)(n=15) or
transcranial approach(TCA)(n=5). Gross total or subtotal removal
were achieved in 60%
of TSA group(9 of 15) and 40% of TCA group(2 of 5).
Postoperative complications were in 6 patients with TSA;
cerebrospinal fluid(CSF) leakages(n=2), postoperative
bleeding(n=2), transient diabetes insipidus(DI)(n=2).
Visual function was improved in 69%(9 of 13) after TSA and 40%
after TCA. Surgical results in the TSA group were
better than those in transcranial approach group, and there were
fewer and less severe postoperative complications.
Conclusion:Even in the giant pituitary adenomas, conventional
transsphenoidal approach was effective as the initial treatment
modality in terms of effective decompression, functional recovery,
and low morbidity. KEY WORDS:Giant pituitary adenoma·Transsphenoial
approach·Transcranial approach.
서 론
거대 뇌하수체 선종(giant pituitary adenoma)은 뇌하수체
선종의 6∼23%를 차지하며 조직학적으로 양성으로 서서히
성장하지만 침습적 성향을 보인다8)9)12)24). 이러한 성향으로
상당한 예에서 종양의 크기가 매우 커지거나 주위조직을 침
범한 뒤에야 진단되어 그 치료결과가 만족스럽지 못하고 치
료법의 선택에 있어 이견이 많다8). Jefferson14)이 1940년
최초로 12명의 거대뇌하수체선종 환자를 보고하여 높은 사망
률을 보고한 이래 1979년 Symon24)등이 40mm이상의 안상
진전(suprsellar extension)이 있거나, 몬로공(foramen of
Monro)에서 6mm이내까지 안상 진전이 있는 경우를 거대
뇌하수체 선종이라 정의하고 있으나 아직까지 확립된 명확
OOOO
*본 논문의 성균관 대학교 의과대학 삼성서울병원 임상 연구비의 지원
으로 이루어졌음.
-
김종현 · 박 관 · 조병문 · 남도현 · 이정일 · 황순구 · 김종수 · 홍승철 · 신형진 · 어 환
J Korean Neurosurg Soc/Volume 28/ November, 1999 1607
한 기준이 없다. 임상적으로 거대 뇌하수체 선종은 수술 사
망률이 4.6∼35%까지 높게 보고되고 있으며(Table 1), 일
반적인 뇌하수체 선종에 비하여 시력 및 시야 장애, 뇌압 상
승 소견, 뇌신경 마비, 전두부 증후군 등의 유발이 흔하여, 뇌
신경 기능의 보존과 정상 뇌하수체 기능을 유지시키는 데 수
술적 치료시 적절한 접근법의 선택이 중요하다8)20)28). 따라
서 저자들은 거대뇌하수체선종의 임상적 특성 및 치료방침
에 따른 성적을 분석 관찰하여 적절한 치료방침을 설정하고
자 본 연구를 시행하였다.
대상 및 방법
1. 대상 및 방법
1994년 10월부터 1998년 10월까지 뇌하수체선종으로 수
술적 가료를 시행한 178예 중 자기공명영상(MRI)상 최대
직경이 40mm이상이었고, 터키안내의 침윤정도와 터키안 상
부 팽창 정도를 Hardy분류에 의하여 grade와 stage를 분
류하였을 때 grade Ⅳ 이상, stage D 이상인 침윤성 거대 뇌
하수체 선종 20예를 대상으로 하였다. 환자의 연령 및 성별
분포, 내분비학적 검사에 의한 기능적 분류, 환자의 임상소견
과 방사선학적 소견, 치료방법, 시력 및 시야의 호전 정도, 수
술적 접근에 따른 합병증에 대해 분석하였다.
2. 수술의 선택과 수술법
경접형동 접근법(transsphenoidal approach, TSA)으로
수술을 시행한 경우가 전체 20예에서 15예, 경두개 접근법
(transcranial approach, TCA)은 5예에서 시행하였다. 수
술방법의 선택 기준은 환자의 전신상태가 불량하거나, 고령,
급격한 시력장애 및 뇌하수체 졸증(pituitary apoplexy), 영상
학적 소견에서 접형골동을 침윤하고 파괴하면서 두개강내 다
방면으로 확장되어 종양을 전적출할 수 없을 경우에 TSA를
우선 선택하여 시행하였고, 또한 MRI에서 종양내 낭포, 출혈
등과 T1강조영상에서 저신호 강도(low signal intensity),
T2강조영상에서 고신호 강도(high signal intensity)를 보이
는 경우 종양의 진전방향을 감안하여 TSA로 접근하였다.
TCA으로 수술을 시행한 경우는 종양이 측두엽, 전두엽 등으
로 심한 진전이 있을 때와, 터어키안이 정상이면서 dumbbell
shape의 종양, 접형골동 및 비강에 감염이 있는 경우에 시
술하였다. TSA의 접근법은 transcolumellar transseptal
approach로 하였고 종양제거는 종양의 내부부터 점진적으
로 제거하여 상부의 종양이 하방으로 밀려 내려오게 하였다.
종양의 하강이 불충분하면 술전 준비해둔 요추천자 부위로
생리식염수를 10∼20cc 정도 주입하여 하강을 촉진하였다.
그러나 주위조직과 유착이 있는 경우나, 종양하강이 일률적으
로 되지 않아 주머니(pouch)를 형성하여 종양을 제거할 수
없는 경우는 내려온 지주막을 부드럽게 올려 rotating ring
currette으로 종양을 확인하면서 제거하였다. 종양이 부분
적출 되었을 경우에 종양출혈이 많았는데 bipolar coagulator
및 thrombin soaked gelfoam으로 지혈을 하였다.
결 과
1. 연령분포, 성별 및 임상증상
거대 뇌하수체 선종은 수술적 가료를 받은 전체 뇌하수체
선종 환자 178예 중 20예로 11%를 차지하였고(Table 2),
남녀의 비는 15:5로 남자에 호발하였다. 평균연령은 47.5세
였으며 주증상으로는 시신경로의 압박에 의한 시력 및 시야
장애가 16예(80%)로 가장 많았고, 의식장애 2예(10%),
두통 및 우연히 발견되었던 경우가 각각 1예였다(Table 3).
2. 거대 뇌하수체 선종의 분류
거대 뇌하수체 선종중 16예가 비기능성 선종 이었으며, 프
로락틴분비 선종 2예, 성장호르몬분비 선종 1예, 부신피질
호르몬분비 선종 1예였다(Table 2). MRI에서 종양의 최대
Table 1. Surgical mortality in giant pituitary adenoma20)29)
Year Mortality(%)
G. Jefferson 1940 35 Heimbach / Krayenbuhl 1959 21.7 Wirth /
Schwartz 1974 18 Symon 1979 18.7 Pia 1984 14.2 Yasargil 1996
4.6
Table 2. Endocrinologic type for 178 cases of pituitary
ade-noma
Type Micro Macro Giant Total
Non-functioning 1 33 16 50 Prolactinoma 23 51 2 76 Acromegaly 4
43 1 48 Cushing’s disease 2 1 1 4
Total No. of cases 30 128 20 178
Table 3. Clinical symptoms and signs
Chief complaint No. of cases
Visual disturbance 16(80%)
-Partial loss 3
-Hemianopsia 10
-Blind or light perception 3
Mental change 2(10%)
Headache 1( 5%)
Incidental finding 1( 5%)
-
거대뇌하수체선종의 외과적 치료
J Korean Neurosurg Soc/Volume 28/ November, 1999 1608
직경이 4.0∼9.2cm으로 평균 5.5cm 이었다. MRI에서 종양
의 진전 방향에 따른 분류를 보면 suprasellar 5예, supras-
ellar and parasellar 4예, preor retrosellar 5예, intras-
phenoidal 6예로 비슷한 분포를 보였다(Table 4). 또 10예
에서 종양내 낭포(cyst)를 형성하거나 종양내 출혈이 관찰
되었다.
3. 수술 결과
TSA로 수술을 시행한 15예 중 9예에서 아전적출 이상
의 종양제거가 되었고, 부분적출을 시행한 경우는 6예였다
(Table 5, Fig. 1). TCA로 수술한 경우는 5예 중 2예에서
만 아전적출을, 3예에서는 부분적출이 가능하였다(Table 5,
Fig. 2). 수술전 시력장애가 있었던 18예에서 TSA로 수술
한 13예에서 9예가 호전되었고, TCA로 수술한 경우는 5예
중 2예가 호전되었으며, 1예에서는 오히려 악화되었다(Table
6). 수술 후 방사선 치료를 시행한 경우는 7예였다. 수술 후
합병증으로는 TSA로 수술한 경우, 일시적 요붕증이 2예에
서 관찰되었고, 뇌척수액비루가 2예, 수술후 종양 제거 부위
에 혈종이 발생하여 재수술이 필요한 경우가 2예 있었다. 뇌
척수액비루가 있었던 환자는 요추천자 배액술로 약 1주간의
안정을 취한후 치료가 되었다. TCA로 수술한 경우는 일시적
요붕증 2예, 경막하수종 2예, 시신경손상 1예가 관찰되었고
이중 1예에서 수술후 심한 뇌부종으로 사망하였다(Table 7).
Table 4. Direction of growth extension
Direction No. of cases
Suprasellar only 5
Suprasellar & parasellar 4
Pre-or retrosellar 5
Intrasphenoidal 6
Table 5. Extent of surgical removal
Surgical removal Initial OP type
NTR STR PR
TSA(n=15) 3 6 6 TCA(n=15) - 2 3 TSA:transsphenoidal approach
TCA:transcranial approach NTR:near total removal STR:subtotal
removal PR:partial removal
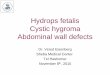
Fig. 1. Enhanced T1 weighted MR images obtained in a 39-year-old
woman who underwent TSA. A & B:Preoperative MR im-ages showing
non-functioning giant pituitary adenoma with a massive suprasellar
extension of the tumor. C & D:Posto-perative MR images showing
near totally removed status via TSA.
AAAA BBBB
CCCC DDDD
-
김종현 · 박 관 · 조병문 · 남도현 · 이정일 · 황순구 · 김종수 · 홍승철 · 신형진 · 어 환
J Korean Neurosurg Soc/Volume 28/ November, 1999 1609
고 찰
거대 뇌하수체 선종은 전체 뇌하수체 선종의 6∼23%를
차지하는 종양으로 정의 및 치료방법 있어 보고자에 따라 이
견이 많은 상태이다9)12)14)24)28). Jefferson14)은 1940년 12예
의 거대 뇌하수체 선종을 발표하면서 35%의 사망률을 보고하
였고, 1969년 pneumocephalogram에서 안상 진전이 7cm를
초과하거나 몬로공에서 6mm이내 까지 안상 진전이 있는 경
우 수술은 불가능하다고 보고하면서 방사선 치료를 권장하
였다1)13). 이후 Kunicki등15)은 전신상태가 양호한 경우 근치적
제거를 시도해야한다고 주장한 반면, Guiot 와 Derome10)은
가능한 부분절제만이라도 시행해야 예후를 향상시킬 수 있
다고 보고하였다. Symon등24)은 midline of jugum sphen-
oidale로부터 어느 방향이나 40mm이상의 진전을 보이거나
몬로공에서 6mm이내까지 자란 종양, 안상에서 두 방향 이
상으로 자란 경우를 거대뇌하수체선종으로 분류하고, 부분
Table 6. Postoperative visual outcome
OP type Visual symptoms
TSA (n=13) TCA (n=5)
Improved 9 2 Not changed 4 2 Aggravated - 1 Total 13 5
TSA:transsphenoidal apporach TCA:transcranial approach
Table 7. Complications
TSA (n=15) TCA(n=5)
Transient DI 2 2 CSF rhinorrhea 2 - Optic nerve damage - 1
Subdural hygroma - 2 Postop. bleeding 2 - Death - 1
TSA:transsphenoidal approach TCA:transcranial approach
DI:diabetes insipedus *Cause of death:severe brain swelling
Fig. 2. Enhanced T1 weighted MR images obtained in a 45-year-old
man who underwent TCA. A & B:Preoerative MR images showing
non-functioning giant pituitary adenoma with a massive suprasellar
& parasellar extension of the tumor. C & D:Postoperative MR
images showing sub-totally removed status via TCA.
AAAA BBBB
CCCC DDDD
-
거대뇌하수체선종의 외과적 치료
J Korean Neurosurg Soc/Volume 28/ November, 1999 1610
적출을 시행할 경우 종양으로의 혈류장애가 생겨 종양 내
경색 혹은 부종으로 인한 합병증 때문에 가능한 부분적출을
피하라고 하였다. Goel등8)은 거대뇌하수체선종의 전적출은
불가능하며 수술 할 때는 혈관손상을 피하고, 종양으로 인
한 뇌신경압박에 대해 적당한 감압을 시도한 뒤에, 수술후
방사선 치료를 함으로서 종양의 성장을 줄일 수 있다고 보
고하였다. Yasagil등29)은 Large pituitary adenoma를 종양
의 크기에 따라 moderate(2∼4cm), large(4∼6cm), giant
(>6cm)으로 분류하였고, 종양의 진전에 따라 Type Ⅰ-Ⅲ
까지 분류하기도 하였다. 본 연구에서 거대 뇌하수체 선종
은 MRI에서 최대직경이 4cm을 초과하는 경우로 분류하였
고, 전체 뇌하수체 선종 중 약 11%를 차지하였다. 종양은
대부분 주위조직을 침범하여 Wilson등25)의 방사선학적 분
류에 따르면 진전범위 C(n=10), D(n=5), E(n=5)에 해당
하며, 터어키안의 침범정도 Ⅲ, Ⅳ에 해당한다. 또 Yasagil
등29)의 Large pituitary adenoma 분류에 의한 Type Ⅲ
(giant and invasive type)에 해당되는 예들이었다.
저자들이 치험한 거대 뇌하수체 선종은 주로 중년 남자에
서 호발하였고, 10예에서 뇌하수체 기능저하증이 관찰되었다.
보고자에 따라 주로 젊은 남자에서 호발하고 임상 증상과 종
양의 크기와는 상관이 없다고 하였으며6)17)21), Grote등20)의
보고에서는 남녀의 비에서 차이가 없고 주로 40∼50대에서
호발하며, 내분비학적 증상 없이 시야장애가 오는 것이 특
징이라고 하였다. 또한 종양이 터어키안 밖으로 탈출되어
자라는 경우가 대부분이기 때문에 환자에 있어 뇌하수체 기능
저하증의 기회는 많지 않다고 보고하고 있다17).
거대뇌하수체선종의 수술 목적은 가능한 종양 조직을 많
이 제거함으로서 뇌신경의 압박 증상을 회복하고 정상 기능
을 유지하는데 있다. 뇌하수체 종양의 수술 방법으로 1962
년 Hardy11)가 X-ray 및 수술 현미경을 TSA에 도입한 이
래 터어키안와 위쪽 정중선에서 대칭적으로 자라난 종양이
나, 후하방 접형골동으로 자란 경우, 측방 해면 정맥동으로
자란 침윤성 종양의 경우도 수술적 제거가 가능하게 되었다.
Wilson26)이나 Fahlbusch등5)은 뇌하수체 종양이 침윤성이
건 아니건 간에 90%이상 TSA 수술법으로 종양을 해결 할
수 있다고 하였다(Table 8). 반면 Symon과 Jakubowski
등24)이 거대 뇌하수체 종양을 TCA로 수술하여 보고한 이
래 대부분 TCA 접근법을 선호하였으나, Snow등23)은 MRI
의 long TR에서 고신호 강도를 보이는 경우에서 종양이 부
드러워 일차적으로 TSA를 고려하여야 한다고 보고하였다.
최근 Saito등22)의 보고에 의하면 open sellar method와 in-
tentionally staged operation의 도입으로 안상 진전이 심한
종양이라도 좋은 결과를 얻을 수 있다고 하였고, Goel등8)은
거대 뇌하수체 선종 일지라도 일차적으로 TSA 접근법을
선호한다고 하였다5)10). 또한 TSA와 TCA를 병행하여 수술
할 경우에 Ciric등4)은 TCA로 먼저 시술하게 되면 지주막의
개방으로 인한 시신경, 주요혈관의 수술후 유착으로 TSA로
접근이 어렵다고 보고하였다(Fig. 3). 이렇게 보고자에 따라
거대 뇌하수체 선종의 경우 TSA나 TCA 접근법을 선택하는
데 이견이 많지만, 저자의 경우, 전체 뇌하수체 선종의 96.1%
를 TSA로 수술을 시행 할 수 있었으며, 거대 뇌하수체 선
종의 경우도 종양의 크기보다는 종양이 전두와, 측두와 및 후
두와로 심하게 진전된 경우와 정상 크기의 터어키안, 혈관
기형, 접형골동염 등을 제외하고, 안상 위로 심하게 자라나간
경우라 하더라도, 고도의 수술 기법을 통해 뇌실질, 뇌신경, 뇌
혈관의 손상 없이 종양을 충분히 제거 할 수 있었다. 그리고
MRI상 종양의 성질이 부드럽거나, 출혈, 낭포를 형성한 경
우에 TSA로의 접근이 용이하였다3)18)19)23).
본 예의 수술적 제거율을 보면 TSA로 수술을 시행한 15
예에서 아전적출 이상의 종양제거는 9예에서 가능하였고 부분
적출을 시행한 경우는 6예였으며, TCA로 수술한 경우는 5예
중 2예에서만 아전적출을, 3예에서는 부분적출이 가능하여 비
록 상대적인 결과이지만 TSA로 수술한 경우가 우수한 결
과를 보였다(Table 5).
최근 Ciric등4)이 문헌보고를 중심으로 통계 분석하여 보고
한 TSA의 합병증으로는 뇌하수체 기능손상(19.4%), 요붕증
(17.8%), 부비동염(8.5%), 비중격파열(6.7%), 뇌척수액비루
(3.9%), 종양출혈(2.9%), 시력장애(1.8%), 사망률(0.9%)등
이 있다. 거대 뇌하수체 선종의 임상 증상중 시야 및 시력장애
경우에 Ciric등3)은 수술후 시력장애는 27%에서 호전, 63%
에서 완전 회복을 보이며 시야결손 개선률은 90%라고 보
고하였다. 또한 Laws등16)은 86%에서 시력장애가 호전된
다고 하였고, 악화되는 경우도 1.5∼6.9%까지 보고되고 있
다2)3)27). 본 연구에서도 TSA로 접근한 경우 13예에서 9예가
호전을, TCA로 접근한 경우는 5예에서 2예가 호전되었으며,
1예에서는 오히려 악화되었다. 다른 합병증으로 TSA로 접근
한 경우 종양이 부분적출 되었을 경우 지혈의 어려움 때문에
Table 8. Operative approaches of pituitary adenoma20)29)
No. of patients TSA(%) TAC(%)
Guiot/Derome 1976 681 89 11 Wison 1979 480 98 2 Hardy 1980 947
93 7 Ciric, et al 1983 108 96 4 Landolt 1990 430 98.8 1.2 Authors
1998 178 96.1 3.9
TSA:transsphenoidal approach TCA:transcranial approach
-
김종현 · 박 관 · 조병문 · 남도현 · 이정일 · 황순구 · 김종수 · 홍승철 · 신형진 · 어 환
J Korean Neurosurg Soc/Volume 28/ November, 1999 1611
종양 제거부위에 출혈이 발생하여 재수술 혹은 개두술에 의한
혈종 제거가 필요한 경우가 2예 있었고, TCA으로 접근한 경
우, 수술후 심한 뇌부종으로 사망한 1예가 있었다(Table 7).
이렇게 거대 뇌하수체 선종의 치료시, 수술적 접근법을
선택하는데 있어서 서로의 장단점과 그 적응증에 있어서 비
교하기가 어렵지만 환자의 연령, 임상증상, 종양의 진전방향,
침습정도, MRI소견, 합병증 등을 고려하여 적절한 수술법을
선택하는 것이 중요하다.
결 론
거대뇌하수체선종의 치료에 있어서 종양의 크기보다는 종
양이 전두와, 측두와 및 후두와로 심하게 진전된 경우를 제
외하고 안상위로 심하게 자라나간 종양이라도 경접형동 접
근법을 통해 뇌신경 및 뇌혈관의 손상없이 종양을 충분히
제거 할 수 있으며 경두개골 접근법에 비햐여 합병증 발생
이 적어 거대뇌하수체선종의 일차적인 수술법으로 선택하는
것이 좋을 것으로 사료된다.
• 논문접수일:1999년 3월 30일 • 심사완료일:1999년 6월 23일 • 책임저자:김 종 현
135-230 서울 강남구 일원동 50번지
성균관대학교 의과대학 삼성서울병원 신경외과학교실 전화:02) 3410-3490/3499
전송:02) 3410-0048/0275
References
1) Bakay L:The result of 300 pituitary adenoma operation. J
Neurosurg 7:240-255, 1950
2) Barrow DL, Tindall GT:Loss of vison after transsphenoidal
surgery. Nuerosurgery 27:60-68, 1990
3) Ciric I, Mikhael M, Stafford T, et al:Transsphenoidal
micro-surgery of pituitary macroadenomas with long term follow-up
results. J Neurosurg 59:395-401, 1983
4) Ciric I, Ragin A, Baumgartner C, et al:Complications of
Tran-ssphenoidal Surgery:Result of a National Survey, Review of the
Literature, and Personal Experience:Neurosurgery 40:225-237,
1997
5) Fahlbusch R, Buchfelder M:Current management of inva-sive
pituitary adenoma. Contemporary Neurosurgery, Vol 11 (17), 1989
6) Feiring EH, Davidoff LM, Zimmerman HM:Primary ca-rcinoma of
the pituitary. Neuropathol Exp Neurol 12:205-223, 1953
7) Fraioli B, Esposito V, Palma L, et al:Hemorrhagic pituitary
adenomas:clinicopathological features and surgical treatment.
Neurosurgery 27:741-747, 1990
8) Goel A, Nadkarni T:Surgical Management of Giant Pit-uitary
Tumors-A Review of 30 Cases. Acta Neurochir(Wien) 138:1042-1049,
1996
9) Grote E:Characteristics of giant pituitary adenomas. Acta
Neurochir 60:141-153, 1982
Fig. 3. Enhanced T1 weighted MR images showing a massive
suprasellar extension of the tumor, Which is indicated in combined
approach(TSA & TCA).
-
거대뇌하수체선종의 외과적 치료
J Korean Neurosurg Soc/Volume 28/ November, 1999 1612
10) Guiot G, Derome P:Surgical problems of pituitary adeno-mas.
Edited by H Krayenbuhl. Advances and Technical Stand-ards in
Neurosurgery. Wien, New York. Springer-Verlag, 1976 Vol 3,
pp3-33
11) Hardy J, Wigser SM:Transsphenoidal surgery of pituitary
fossa tumors with televised radiofluoroscopic control. J Neur-osurg
23:612-619, 1965
12) Hashimoto N, Handa H, Yamashita J, et al:Long term
fo-llow-up of large or invasive pituitary adenoma. Surg Neurol
25:49-54, 1986
13) Jefferson A:Chromophobe pituitary adenoma. The size of the
suprasellar portion in relation to the safety of operation. J
Neurol Neurosurg Psychiat 32:632(abstract), 1969
14) Jefferson G:Extrasellar extension of pituitary adenomas.
Pre-sident’s address. Procedings of the Royal Societ of Medicine
33:433-458, 1940
15) Kunicki A, Grochowski W, Czernicki ZB:Szerzenie sie
grucz-olakow przysadki mozgowej poza siedeko tureckie. Neurolo-gia
Neurochirurgia Polska 9:626-629, 1975
16) Lamberts SW, Herder WW, Kwekkeboom DJ, et al:Current tools
in the diagnosis of pituitary tumors. Acta Endocrinol 129:6-12,
1993
17) Martins AN, Hayes GJ, Kempe LG:Invasive pituitary aden-omas.
J Neurosurg 22:268-276, 1965
18) Mohr G, Hardy J, Comtois R, et al:Surgical management of
giant pituitary adenomas. CanJ Neurol Sci 17:62-66, 1990
19) Onesti ST, Post KD:Complications of transsphenoidal
mi-crosurgery, in Post KD, Friedman ED, McCormick
P(eds):Postoperative Complications in Intracranial Neurosurgery.
Chicago:Thieme Medical Publishers, 1993, pp61-73
20) Pia HW, Grote E, Hildebrandt G:Giant pituitary adenomas.
Neurosurg. Rev 8:207-220, 1985 21) Rovit RL, Duane TD:Cushing’s
syndrome and pituitary tu-
mors:pathophysiology and ocular manifestations of
ACTH-secreating pituitary adenomas. Am J Med 46:416-427, 1969
22) Saito K, Kuwayama A, Yamamoto N, et al:The transsphe-noidal
removal of nonfunctioning pituitary adenomas with suprasellar
extensions:The open sella method and inten-tionally staged
operation. Neurosurgery 36:668-676, 1995
23) Snow RB, Johnson CE, Morgello S, et al:Is magnetic
reson-ance imaging useful in guiding the operative approach to
large pituitary tumor? Neurosurgery 26:801-803, 1990
24) Symon L, Jakubowski J, Kendall B:Surgical treatment of giant
pituitary adenomas. J Neurol Neurosurg Psychiat 42:973-982,
1979
25) Wilson CB:Neurosurgical management of large and inva-sive
pituitary tumors. Edited by GT Tindall, WF Collins. Clini-cal
Management of Pituitary Disorders. New York. Raven Press, 1979,
pp335-342
26) Wilson CB:Role of surgery in the management of pituitary
tumor. Neurosurgery Clinics of North america. Vol 1. No 1. Edited
by ML Rosenblum, WB Saunder Co. p139-159, 1990
27) Wilson CB, Dempsey LC:Transsphenoidal microsurgical removal
of 250 pituitary adenomas. J Neurosurg 48:13-22, 1978
28) Wirth P, Schwartz HG, Schwestschenau PR:Pituitary
adeno-mas:factors in treatment. Clinical Neurology 21:8-25,
1974
29) Yasargil MG:Transcranial Surgery for Large Pituitary
Ade-nomas, in Curcic M, Valavanis A, Yasargil
DCH(eds):Mi-croneurosurgery of CNS Tumors, New York:GTV, Stuttgart,
1996, Vol IV B, pp200-204