Embed Size (px)
Citation preview

Original Articles
DISEASE PROGRESSION AND SURVIVAL OF PATIENTS WITHPOSITIVE LYMPH NODES AFTER RADICAL PROSTATECTOMY. IS
THERE A CHANCE OF CURE?
PIA BADER, FIONA C. BURKHARD, REGULA MARKWALDER AND URS E. STUDERFrom the Department of Urology and Institute of Pathology, University of Bern, Bern, Switzerland
ABSTRACT
Purpose: In prostate cancer involvement of regional lymph nodes is regarded as a poorprognostic factor. Is this also true for micrometastasis if a meticulous lymph node dissection isperformed? We determined progression rate and survival of patients with positive nodes follow-ing radical prostatectomy according to the number of metastases.
Materials and Methods: Between 1989 and 1999, 367 patients with clinically organ confinedprostate cancer underwent meticulous pelvic lymph node dissection and radical prostatectomy.None of the patients received immediate adjuvant therapy.
Results: Of the patients 92 (25%) had histologically proven lymph node metastases. Followupof more than 1 year was available in 88 patients (96%), and median followup was 45 months(range 13 to 141). Of 19 patients (22%) who died of prostate cancer 16 had more than 1 positivenode. Of the 39 patients with only 1 positive node 15 (39%) remained without signs of clinical orchemical progression. Whereas of the 20 and 29 patients with 2 or more positive lymph nodesonly 2 (10%) and 4 (14%), respectively, remained disease-free. Time to prostate specific antigenrelapse, symptomatic progression and tumor related death were significantly affected by thenumber of positive nodes.
Conclusions: Meticulous lymph node dissection reveals a high rate of metastases (25%). Inpatients with positive nodes time to progression is significantly correlated with the number ofdiseased nodes. Some patients with minimal metastatic disease remain free of prostate specificantigen relapse for more than 10 years after prostatectomy without any adjuvant treatment.Meticulous pelvic lymph node dissection, particularly in patients with micrometastases, seemsnot only to be a staging procedure, but may also have a positive impact on disease progressionand long-term disease-free survival.
KEY WORDS: prostatic neoplasms, lymphatic metastasis, prostatectomy; survival, disease progression
The incidence of nodal metastases in patients with pre-sumed clinically localized prostate cancer decreased from20% to 40% in the 1970s and 1980s1, 2 to 4% to 6% recently,3, 4
depending on patient selection and technique of lymph nodedissection. Previously involvement of regional lymph nodesin prostate cancer was regarded as a poor prognostic factorindicating systemic disease with limited long-term survivalregardless of treatment. However, retrospective data showedlong-term survival of patients with positive lymph nodesafter radical prostatectomy.5, 6 Nevertheless, many surgeonsrefrain from performing radical prostatectomy when positivelymph nodes are histologically identified, and patients usu-ally receive hormonal therapy or radiotherapy. Others com-plete surgery to avoid local complications in the future.
In bladder cancer, usually a more aggressive disease thanprostate cancer, presence of positive lymph nodes has beenconsidered a sign of systemic disease. However, patients inwhom micrometastases were removed had a 30% probability
of 5-year survival.7, 8 Additionally, meticulous lymph nodedissection revealed more positive nodes than expected.Skinner was the first to emphasize the curability of somenode positive cases using meticulous lymph node dissectionat radical cystectomy.9 Other examples of carcinomas forwhich removal and extent of lymph node metastases influ-ence the progression rate are penile cancer,10 melanoma, andcarcinoma of the breast11 and colon.12 Why should this not beso for prostate cancer? Perhaps such an advantage for pa-tients with minimal lymph node involvement has not beenconfirmed to date because the lymph node dissection was notmeticulous enough.
In studies on progression rate and survival in lymph nodepositive prostate cancer the areas of lymph node dissectionand the number of lymph nodes removed are rarely specifiedand vary considerably making it difficult to compare theresults. To our knowledge there is no study comparing theoutcome of patients with extended versus limited lymphad-enectomy at radical prostatectomy. To date an extensive,meticulous, radical, modified, limited or simple lymph nodedissection is not clearly defined. There are some retrospectivestudies showing that patients with lymph node positive pros-tate cancer undergoing radical prostatectomy have a better
Accepted for publication September 6, 2002.
Editor’s Note: This article is the first of 5 published in thisissue for which category 1 CME credits can be earned. In-structions for obtaining credits are given with the questionson pages 118 and 119.
0022-5347/03/1693-0849/0 Vol. 169, 849–854, March 2003THE JOURNAL OF UROLOGY® Printed in U.S.A.Copyright © 2003 by AMERICAN UROLOGICAL ASSOCIATION DOI: 10.1097/01.ju.0000049032.38743.c7
849

cancer specific survival than those with lymph node dissec-tion alone,2, 6, 13–15 probably reflecting patient selection aswell. However, there is evidence that the extent of lymphnode involvement may have a significant impact on progres-sion, although most of the patients received adjuvant therapyafter radical prostatectomy. Additionally, the extent of lymphnode dissection is rarely mentioned.
To our knowledge there is no prospective study to deter-mine the natural history of lymph node positive prostatecancer after a defined, meticulous lymph node dissectionwith or without radical prostatectomy. We evaluated theinfluence of the number of positive nodes on progression rateand survival after radical prostatectomy and extendedlymphadenectomy with no adjuvant therapy to determine ifradical surgical treatment alone could prevent prostate spe-cific antigen (PSA) relapse in some patients.
PATIENTS AND METHODS
Between 1989 and 1999, 367 patients with clinically organconfined prostate cancer, negative preoperative abdominal/pelvic computerized tomography, bone scan and chest x-ray,and no preoperative treatment for prostate cancer such asandrogen blockade or radiotherapy underwent radical retro-pubic prostatectomy and meticulous lymphadenectomy, andwere prospectively followed for tumor progression. Medianpatient age was 64 years (range 44 to 76) and median pre-operative PSA was 11.9 ng./ml. (0.4 to 172). Patients withpathologically enlarged lymph nodes on the preoperativestaging investigations or with incomplete preoperative diag-nostic evaluation (no computerized tomography or bone scan)were not eligible for study. An increased PSA level was not anexclusion criterion because sometimes a transitional zonecancer was suspected which is known to be associated withincreased PSA and low potential for metastases.16
All patients underwent meticulous open lymph node dis-section followed by radical retropubic prostatectomy. Pre-serving the lymphatics overlying the external iliac artery,lymph node dissection was performed along the external iliacvein, the caudal limit being the deep circumflex iliac vein andfemoral canal. All lymphatic vessels from the lower extrem-ities were meticulously ligated. The proximal border wasbifurcation of the common iliac artery, and all tissue in the
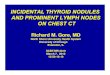
angle between the external and internal iliac arteries andobturator nerve was removed. All fatty, connective and lym-phatic tissue of the obturator fossa along the obturator mus-cle was removed leaving the obturator nerve and vessels bare(fig. 1). Thereafter the internal iliac artery and, as far aspossible, the internal iliac vein (hypogastric vessels) wereskeletonized. Three different tissue samples on each sidelabeled external iliac vein, obturator fossa and hypogastricvessels were sent separately for histological evaluation. Nofrozen sections were performed routinely. In 2 cases theoperation was aborted after lymph node dissection because oflarge palpable lymph node masses. These 2 cases are notincluded in the study.
All lymph node specimens removed during the operationwere fixed in neutral buffered 4% formaldehyde for 24 hoursand then placed in acetone for dissolving the fatty tissue.Lymph nodes were meticulously searched and counted man-ually. Each node was cut in 3 mm. slices which were sepa-rately embedded in paraffin, stained with hematoxylin andeosin and examined microscopically for the presence of can-cer by the pathologists. No immunohistochemical stains forkeratin, PSA or reverse-transcriptase polymerase chain re-action technology were used. Principally no adjuvant therapysuch as hormonal treatment or radiotherapy was recom-mended until symptoms of disease progression occurred (forexample bladder outlet obstruction, gross hematuria or hy-dronephrosis due to local progression, pain or lymphedemafrom bone or lymph node metastases).
Kaplan-Meier projection curves were constructed for allpatients for PSA increase, symptomatic progression andcause specific death in relation to the number of positivelymph nodes (1 versus 2 versus greater than 2), tumor stage,histological grade and Gleason score. Log rank test was donefor statistical analysis of these curves. The Cox proportionalhazards model was used for regression analysis to determineif the number of diseased lymph nodes had a significantimpact on survival and progression (95% CI).
RESULTS
The median number of lymph nodes removed from the 367patients was 21 (range 6 to 50), and 92 patients (25%) had
FIG. 1. Lymph node dissection field in our study shows external iliac vein (1), obturator fossa (2) and internal iliac vessels (3) which wereanalyzed separately.
SURVIVAL AND PROGRESSION AFTER PROSTATECTOMY FOR NODE POSITIVE DISEASE850

positive lymph nodes. The median number of nodes removedfrom these 92 patients was also 21 (range 6 to 41) and themedian number of positive nodes was 2 (range 1 to 19). Of the92 patients 41 (45%) had 1, 22 (24%) had 2 and 29 (32%) hadmore than 2 positive lymph nodes. Preoperative PSA was lessthan 20 ng./ml. in 49 patients (53%) and less than 10 ng./ml.in 20 (22%).
The postoperative pathological tumor stage for the entirestudy group and the 92 patients with lymph node involve-ment is shown in table 1. Of the 92 patients with positivenodes 27 (29%) had confirmed organ confined disease, 15(16%) had tumor beyond the capsule, 47 (51%) had infiltra-tion of the seminal vesicle and 3 (3%) had infiltration of thebladder neck or skeletal muscle. The incidence of lymph nodemetastases increased with the extent of local disease (table1). The Gleason score of the prostate specimen is shown intable 2.
There were no perioperative deaths. In 3 patients withpositive lymph nodes (3.3%) lymphoceles developed, whichrequired rehospitalization and secondary drainage. This per-centage is slightly higher than that of the whole group ofpatients treated with meticulous lymphadenectomy and rad-ical prostatectomy (7 of 367, 1.9%). Of the 367 patients 10(2.7%) had a postoperative pulmonary embolism that wasmanaged conservatively by anticoagulation, of whom 3 hadpositive nodes, for a slightly higher percentage (3.3%) ofpulmonary embolism in this group.
Followup data for more than 1 year were available for 88(96%) patients with positive lymph nodes (table 3). After amedian followup of 45 months (range 13 to 141) 8% of the 39patients with only 1 positive lymph node died of prostatecancer, 44% had symptomatic disease progression (metastat-ic disease and/or anastomotic recurrence), 18% had anasymptomatic PSA increase only and 39% remained com-
pletely disease-free. However, of 20 patients with 2 lymphnode metastases 25% had a tumor related death, 60% hadsymptomatic disease progression, 30% had exclusively anasymptomatic PSA increase and only 10% remained tumor-free. Results in the 29 patients with more than 2 positivenodes were 36% cancer related death, 62% symptomatic dis-ease, 24% an asymptomatic PSA increase only and 14%tumor-free (table 3).
During followup 22 patients died. In 3 patients death wasnot related to prostate cancer, but to chronic obstructivepulmonary disease, choledochus duct cancer and pancreaticcancer. Of these 3 patients 2 were free of prostate cancer atthe time of death and 1 had an asymptomatic PSA increase to5.5 ng./ml. without evident metastases. The remaining 19patients (22%) died of prostate cancer after a median of 43months (range 19 to 76), 16 of whom had had more than 1positive node. Median time to PSA progression as well assymptomatic disease progression increased with the numberof nodes involved (table 4).
Univariate Cox regression analysis showed that the num-ber of lymph node metastases was significantly related toprogression and cancer specific death (p �0.001). The prob-ability for PSA relapse, symptomatic progression and tumorrelated death increased with each additional lymph nodeinvolved. The hazards ratio was 1.36 (95% CI 1.17–1.59) forPSA relapse, 1.28 (1.15–1.42) for symptomatic progressionand 1.31 (1.17–1.47) for cancer related death. In a multivar-iate Cox proportional hazards model including the number oflymph node metastases, tumor stage and Gleason score thenumber of positive nodes was the only variable affectingprogression and cancer specific death.
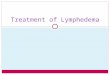
Kaplan-Meier projection curves show that patients with 1lymph node involved had a significantly lower biochemicalprogression rate than those with 2 or more positive nodes(p � 0.0082, fig. 2, A). The same phenomenon was observedfor the number of lymph node metastases in relation tosymptomatic tumor progression (p � 0.0313, fig. 2, B) andcancer related death (p � 0.0039, fig. 2, C). Time to symp-tomatic tumor progression of patients with positive nodesalso depended on the Gleason score of the prostate specimen(0.0141) (not shown). Most likely due to the small number ofpatients in the various subgroups, significant correlationcould not be found between time to PSA relapse, symptom-
TABLE 1. Postoperative pathological tumor stage of the entire studygroup and patients with lymph node involvement
Tumor Stage(1997 TNM) Total No. Pts. No. Pts. With Pos. Nodes
(25%)
pT1–pT2b 206 27 (13)pT3a 60 15 (25)pT3b 97 47 (49)pT4 4 3 (75)
TABLE 2. Postoperative pathological Gleason score of patients with lymph node involvement
No. Pos. Nodes No. Pts. No. GleasonScore 2–5 (%)
No. GleasonScore 6 (%)
No. GleasonScore 7 (%)
No. GleasonScore 8–10 (%)
No. GleasonUnknown (%)
1 41 12 (29) 17 (42) 2 (5) 8 (20) 2 (5)2 22 7 (32) 5 (23) 2 (9) 8 (36) 0Greater than 2 29 5 (17) 3 (10) 7 (24) 12 (41) 2 (7)
Totals 92 24 (26) 25 (27) 11 (12) 28 (30) 4 (4)
TABLE 3. Outcome of patients with lymph node metastases from prostate cancer after a median followup of 45 months
No. Pos. Nodes No. Pts. No. No PSARelapse (%)
No. AsymptomaticPSA Relapse (%)
No. SymptomaticProgression (%)
No. Ca RelatedDeath (%)
1 39 15 (39) 7 (18) 17 (44) 3 (8)2 20 2 (10) 6 (30) 12 (60) 5 (25)Greater than 2 29 4 (14) 7 (24) 18 (62) 11 (36)
Totals 88 21 (24) 20 (23) 47 (53) 19 (22)
TABLE 4. Outcome and median time to progression of patients with lymph node metastases from prostate cancer after a median followupof 45 months
No. Pos. Nodes No. Pts. No. PSARelapse (%)
Median Time toPSA Relapse
(range)
No. SymptomaticProgression (%)
Median Time toSymptomatic Progression
(range)
1 39 24 (61) 28 (0–80) 17 (44) 46 (8–122)2 20 18 (90) 26 (5–107) 12 (60) 40 (15–102)Greater than 2 29 25 (86) 7 (0–71) 18 (62) 24 (2–73)
Overall 88 67 (76) 21 (0–107) 47 (53) 29 (2–12)
SURVIVAL AND PROGRESSION AFTER PROSTATECTOMY FOR NODE POSITIVE DISEASE 851
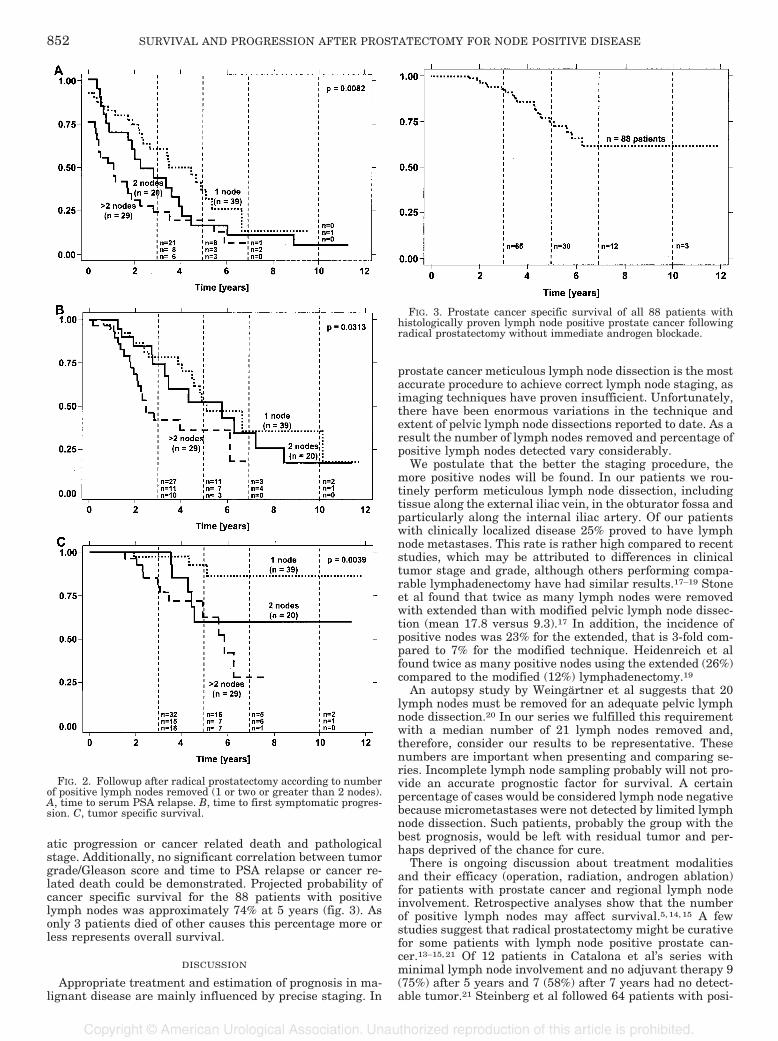
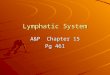
atic progression or cancer related death and pathologicalstage. Additionally, no significant correlation between tumorgrade/Gleason score and time to PSA relapse or cancer re-lated death could be demonstrated. Projected probability ofcancer specific survival for the 88 patients with positivelymph nodes was approximately 74% at 5 years (fig. 3). Asonly 3 patients died of other causes this percentage more orless represents overall survival.
DISCUSSION
Appropriate treatment and estimation of prognosis in ma-lignant disease are mainly influenced by precise staging. In
prostate cancer meticulous lymph node dissection is the mostaccurate procedure to achieve correct lymph node staging, asimaging techniques have proven insufficient. Unfortunately,there have been enormous variations in the technique andextent of pelvic lymph node dissections reported to date. As aresult the number of lymph nodes removed and percentage ofpositive lymph nodes detected vary considerably.
We postulate that the better the staging procedure, themore positive nodes will be found. In our patients we rou-tinely perform meticulous lymph node dissection, includingtissue along the external iliac vein, in the obturator fossa andparticularly along the internal iliac artery. Of our patientswith clinically localized disease 25% proved to have lymphnode metastases. This rate is rather high compared to recentstudies, which may be attributed to differences in clinicaltumor stage and grade, although others performing compa-rable lymphadenectomy have had similar results.17–19 Stoneet al found that twice as many lymph nodes were removedwith extended than with modified pelvic lymph node dissec-tion (mean 17.8 versus 9.3).17 In addition, the incidence ofpositive nodes was 23% for the extended, that is 3-fold com-pared to 7% for the modified technique. Heidenreich et alfound twice as many positive nodes using the extended (26%)compared to the modified (12%) lymphadenectomy.19
An autopsy study by Weingartner et al suggests that 20lymph nodes must be removed for an adequate pelvic lymphnode dissection.20 In our series we fulfilled this requirementwith a median number of 21 lymph nodes removed and,therefore, consider our results to be representative. Thesenumbers are important when presenting and comparing se-ries. Incomplete lymph node sampling probably will not pro-vide an accurate prognostic factor for survival. A certainpercentage of cases would be considered lymph node negativebecause micrometastases were not detected by limited lymphnode dissection. Such patients, probably the group with thebest prognosis, would be left with residual tumor and per-haps deprived of the chance for cure.
There is ongoing discussion about treatment modalitiesand their efficacy (operation, radiation, androgen ablation)for patients with prostate cancer and regional lymph nodeinvolvement. Retrospective analyses show that the numberof positive lymph nodes may affect survival.5, 14, 15 A fewstudies suggest that radical prostatectomy might be curativefor some patients with lymph node positive prostate can-cer.13–15, 21 Of 12 patients in Catalona et al’s series withminimal lymph node involvement and no adjuvant therapy 9(75%) after 5 years and 7 (58%) after 7 years had no detect-able tumor.21 Steinberg et al followed 64 patients with posi-
FIG. 2. Followup after radical prostatectomy according to numberof positive lymph nodes removed (1 or two or greater than 2 nodes).A, time to serum PSA relapse. B, time to first symptomatic progres-sion. C, tumor specific survival.
FIG. 3. Prostate cancer specific survival of all 88 patients withhistologically proven lymph node positive prostate cancer followingradical prostatectomy without immediate androgen blockade.
SURVIVAL AND PROGRESSION AFTER PROSTATECTOMY FOR NODE POSITIVE DISEASE852

tive nodes 60 and 80 months after radical prostatectomy, ofwhom 83% and 68%, respectively were still free of detectabletumor.13 They found that the tumor burden of the diseasedlymph nodes was an independent prognostic factor. Pound etal followed 1,623 men with clinically localized prostate can-cer after radical prostatectomy.15 The overall recurrence ratewas 17%, and in patients with lymph node micrometastasisthe 10-year metastasis-free survival rate was 68% withoutany adjuvant therapy. However, Hull et al reported only18.5% and 7.4% progression-free survival rate after 5 and 10years, respectively.22
Retrospective data on patients who underwent radicalprostatectomy and immediate androgen ablation showedcomparable 5 and 10-year tumor specific survival for patientswith a single lymph node metastasis or negative lymphnode.5 Messing et al described the results of a prospectivestudy of men with node positive prostate cancer after radicalprostatectomy and hormonal therapy.23 They reported a sur-vival advantage for immediate versus delayed hormonaltreatment (observation group). After a median followup of 7.1years only 16% of the patients without adjuvant treatmenthad no evidence of tumor. This result is much lower com-pared to our result and that of Pound et al.15 Although thetumor burden was not specified, the results of Messing et alsuggest that some patients with lymph node involvementmay be cured after radical surgery only.23 The percentage ofthese patients may have been higher if a meticulous completepelvic lymph node dissection had been done. In our series24% of the patients with positive lymph nodes and 39% ofthose with only 1 lymph node involved remained withoutevidence of tumor after a median followup of 3.8 years.
Many of the aforementioned studies represent highly se-lect patient groups because only those with micrometastasesthat had been missed by frozen section were included. Mostof these studies were retrospective and not randomized, andthe treatment options depended on surgeon preference. Ob-viously, a selection bias may have had a major role. Anotherimportant issue is that node positive prostate cancer today isnot the same disease entity it was a decade ago when itrepresented locally and systemically advanced disease. To-day most of the patients with positive nodes only have mi-croscopic metastatic deposits and may have a chance of curewith radical surgical treatment alone. Some of our patientsremain clinically and biochemically tumor-free more than 11years after prostatectomy without adjuvant therapy. Overallprojected probability of cancer specific survival in lymphnode positive prostate cancer is approximately 74% and 58%at 5 and 10 years, respectively, and more than 80% in pa-tients with micrometastasis only.
If there is only minimal involvement of lymph nodes, thelead time bias, that is the time by which the diagnosis isadvanced using early detection methods, must be considered.With meticulous surgical lymph node dissection lymph nodemetastases are found at an early stage. This time advantagemay disappear with the length of followup. Indeed, whenlooking at patients without PSA relapse despite many yearsof followup we may well be observing the natural history oflow volume disease. However a minimal longer surgical timeseems a small price to pay for a potential advantage.
Our progression rate was 67% during a mean followup of45 months if serum PSA greater than 0.4 ng./ml. is consid-ered progression (table 3). The number of diseased lymphnodes had a significant impact on PSA relapse, symptomatictumor progression and tumor specific death. Due to the smallnumber (19) of patients who died of prostate cancer in ourseries the last point is difficult to prove. Tumor grade/Gleason score and tumor stage seem to be less important. Wecannot exclude that the significant differences in progressionin our collective (1 versus 2 versus greater than 2 positivelymph nodes) series may also reflect the metastatic tumor
burden or, ultimately, the biological aggressiveness of themetastatic cancer.
Our data suggest a delay in progression for patients withminimal lymph node involvement in prostate cancer whenradical surgery is performed. Followup is still too short tomake a final decision as to the possibility of a curative effect.However, dependent on the tumor burden or the number ofdiseased lymph nodes, radical surgical treatment seems toimprove outcome in a not yet exactly defined but neverthe-less important percentage of patients. Thus, meticulous pel-vic lymph node dissection to remove all diseased nodes andprovide a correct staging combined with radical prostatec-tomy is recommended for clinically organ confined prostatecancer. The promising survival rate of patients with minimalnode disease makes the value of routine immediate androgenablation in all patients with positive lymph nodes at leastquestionable, especially when considering the negative sideeffects. The subgroup with a potential benefit from immedi-ate adjuvant androgen ablation still needs to be defined.
CONCLUSIONS
There is a relatively high incidence of positive lymph nodesin clinically organ confined prostate cancer. In lymph nodepositive prostate cancer time to asymptomatic PSA increase,time to symptomatic tumor progression and time to tumorspecific death significantly correlate with the number oflymph node metastases. Some patients have remaineddisease-free more than 11 years after radical prostatectomyand meticulous lymph node dissection without any adjuvanttreatment. Therefore, we think that there may be a chance ofcure in some patients with minimal lymph node involvementprovided these nodes are meticulously removed. Meticulouslymph node dissection for prostate cancer not only providesaccurate staging, but may also have a positive effect onprogression and survival after radical prostatectomy.
Statistical analysis was performed by Institute of Socialand Preventive Medicine, University of Bern.
REFERENCES
1. Fowler, J. E., Jr. and Whitmore, W. F., Jr.: The incidence andextent of pelvic lymph node metastases in apparently localizedprostatic cancer. Cancer, 47: 2941, 1981
2. Zincke, H.: Extended experience with surgical treatment of stageD1 adenocarcinoma of prostate. Significant influences of im-mediate adjuvant hormonal treatment (orchiectomy) on out-come. Urology, suppl., 33: 27, 1989
3. Petros, J. A. and Catalona, W. J.: Lower incidence of unsus-pected lymph node metastases in 521 consecutive patientswith clinically localized prostate cancer. J Urol, 147: 1574,1992
4. Han, M. H., Partin, A. W., Pound, C. R., Epstein, J. I. and Walsh,P. C.: Long-term biochemical disease-free and cancer-specificsurvival following anatomical radical retropubic prostatecto-my: the 15-year Johns Hopkins experience. Urol Clin NorthAm, 28: 555, 2001
5. Cheng, L., Zincke, H., Blute, M. L., Bergstralh, E. J., Scherer, B.and Bostwick, D. G.: Risk of prostate carcinoma death inpatients with lymph node metastasis. Cancer, 91: 66, 2001
6. Ghavamian, R., Bergstralh, E. J., Blute, M. L., Slezak, J. andZincke, H.: Radical retropubic prostatectomy plus orchiectomyversus orchiectomy alone for pT�N� prostate cancer: amatched comparison. J Urol, 161: 1223, 1999
7. Stein, J. P., Lieskovsky, G., Cote, R., Groshen, S., Feng, A. C.,Boyd, S. et al: Radical cystectomy in treatment of invasivebladder cancer: long-term results in 1,054 patients. J ClinOncol, 19: 666, 2001
8. Mills, R. D., Turner, W. H., Fleischmann, A., Markwalder, R.,Thalmann, G. N. and Studer, U. E.: Pelvic lymph node metas-tases from bladder cancer: outcome in 83 patients after radicalcystectomy and pelvic lymphadenectomy. J Urol, 166: 19, 2001
9. Skinner, D. G.: Management of invasive bladder cancer: a me-ticulous pelvic node dissection can make a difference. J Urol,128: 34, 1982
SURVIVAL AND PROGRESSION AFTER PROSTATECTOMY FOR NODE POSITIVE DISEASE 853

10. Srinivas, V., Morse, M. J., Herr, H. W., Sogani, P. C. and Whitmore,W. F., Jr.: Penile cancer: relation of extent of nodal metastasis tosurvival. J Urol, 137: 880, 1987
11. Habal, N., Giuliano, A. E. and Morton, D. L.: The use of sentinellymphadenectomy to identify candidates for postoperative ad-juvant therapy of melanoma and breast cancer. Semin Oncol,28: 41, 2001
12. Calaluce, R., Miedema, B. W. and Yesus, Y. W.: Micrometastasisin colorectal carcinoma: a review. J Surg Oncol, 67: 194, 1998
13. Steinberg, G. D., Epstein, J. I., Piantadosi, S. and Walsh, P. C.:Management of stage D1 adenocarcinoma of the prostate: theJohns Hopkins experience 1974 to 1987. J Urol, 144: 1425,1990
14. Frazier, H. A., 2nd, Robertson, J. E. and Paulson, D. F.: Doesradical prostatectomy in the presence of positive pelvic lymphnodes enhance survival? World J Urol, 12: 308, 1994
15. Pound, C. R., Partin, A. W., Epstein, J. I. and Walsh, P. C.:Prostate-specific antigen after anatomic radical retropubicprostatectomy. Patterns of recurrence and cancer control. UrolClin North Am, 24: 395, 1997
16. Stamey, T. A., Dietrick, D. D. and Issa, M. M.: Large, organconfined impalpable transition zone prostate cancer: associa-tion with metastatic levels of prostate specific antigen. J Urol,149: 510, 1993
17. Stone, N. N., Stock, R. G. and Unger, P.: Laparoscopic pelvic
lymph node dissection for prostate cancer: comparison of theextended and modified techniques. J Urol, 158: 1891, 1997
18. Wawroschek, F., Vogt, H., Weckermann, D., Wagner, T., Hamm,M. and Harzmann, R.: Radioisotope guided lymph node dis-section for prostate cancer. J Urol, 166: 1715, 2001
19. Heidenreich, A., Varga, Z. and von Knobloch, R.: Extended pelviclymphadenectomy in patients undergoing radical prostatec-tomy: high incidence of lymph node metastasis. J Urol, 167:1681, 2002
20. Weingartner, K., Ramaswamy, A., Bittinger, A., Gerharz, E. W.,Voge, D. and Riedmiller, H.: Anatomical basis for pelviclymphadenectomy in prostate cancer: results of an autopsystudy and implications for the clinic. J Urol, 156: 1969, 1996
21. Catalona, W. J., Miller, D. R. and Kavoussi, L. R.: Intermediate-term survival results in clinically understaged cancer patientsfollowing radical prostatectomy. J Urol, 140: 540, 1988
22. Hull, G. W., Rabbani, F., Abbas, F., Wheeler, T. M., Kattan,M. W. and Scardino, P. T.: Cancer control with radical pros-tatectomy alone in 1,000 consecutive patients. J Urol, 167:528, 2002
23. Messing, E. M., Manola, J., Sarosdy, M., Wilding, G., Crawford,E. D. and Trump, D.: Immediate hormonal therapy comparedwith observation after radical prostatectomy and pelviclymphadenectomy in men with node-positive prostate cancer.N Engl J Med, 341: 1781, 1999
SURVIVAL AND PROGRESSION AFTER PROSTATECTOMY FOR NODE POSITIVE DISEASE854