Embed Size (px)
Citation preview

Diagnostikk av akutt og
kronisk nyresvikt sett fra
klinisk synsvinkel på St Olav
Cecilia Montgomery Øien
St Olavs Hospital
10.10.12

AKUTT NYRESVIKT


Definitions – Acute kidney injury
• 0-7 days, often spontanous recovery
• Non-renal causes
– Acute kidney disease
• 7-180 days, can be treatable
• Acute glomerulonephritis, acute interstitial nephritis,
vasculitis, intoxication
– Chronic kidney disease
• 180 days +, difficult to reverse
• Chronic glomerulonephritis, diabetes, HT,
atherosclerosis, hereditary diseases (ADPCKD), …

INTENSIVE CARE UNIT CLASSIFICATION

Akpesso. Intens Care
Med 2000; 400
•Obstruktiv (postrenal)
22 %
•Prerenal 24 %
•Renal 54 %
Differensialdiagnoser

Epidemiology
2 per 1000 admissions
needed dialysis
Other studies: Only 1 of 4 are registered, correct frequency are 80 per 1000 admissions

Prognosis: mortality
Patients with severe AKI requiring dialysis
Adjusted regression analysis of mortality risk RR 8 after adjusting for age, sex, race
RR 4 after adjusteing also for comorbidity & other hospital problems
Study (n) In-hospital mortality 1 year mortality
Schiffl (425) 47% 35%
Lins (293) 51% 22%
Basgshaw (240) 61% 64%

Prognosis: kidney function
• Patients with severe AKI requiring dialysis
AKI in patients without previous CKD can expect full recovery
Acute on chronic kidney disease can result in ESRD
Study (n) Previous CKD RRT at discharge RRT at 1 year
Schiffl (425) None 0 % 0.5%
Lins (293) None 5% 5%
Basgshaw (240) Some 33% 22%
(2/3 with pre CKD)

Acute kidney injury
Fluid
overload
Electrolyte/acid–base
abnormalities
Impaired innate
immunity
Chronic kidney
disease
Figure 2 | Acute kidney injury (AKI) can have both immediately recognizable consequences as well as less noticeable or delayed
consequences. Fluid overload and electrolyte/acid–base abnormalities represent well known, easily recognized consequences of
AKI.
Contrary, impaired innate immunity and chronic kidney disease do not manifest themselves immediately

Causes of acute kidney injury

Nephrotoxic agents N
ephro
toxic
agents

Bare kreatinin og
urinmengde?

Figure 1. Origin of acute kidney injury biomarkers within
a single nephron. GST, glutathione S-transferase; GT, glutamyl
transpeptidase; KIM, kidney injury molecule; L-FABP, liver-type fatty
acid-binding protein; NAG, N-acetyl-β-D-glucosaminidase; NGAL,
neutrophil gelatinase-associated lipocalin; RBP, retinol binding
protein.
Ostermann et al. Critical Care 2012, 16:233
NEW MARKERS
Unanswered questions
The new biomarkers of AKI have enhanced our understanding
of some of the biological and biochemical
processes during AKI; however, to date their clinical
utility remains unclear. It is not known whether any of
the new biomarkers add anything beyond clinical evaluation
and traditional renal function tests and whether
they can guide clinical management and ultimately alter
the outcome of patients with AKI. There is also concern
that a single biomarker may not be able to fulfil all criteria
as outlined in Table 1, and that it is more realistic to
search for a panel of different biomarkers that, in combination,
may provide the necessary data to manage patients with AKI.
Ostermann et al. Critical Care 2012, 16:233

MARKERS OF INTEREST
Kreatinin, karbamid, K, St bikarbonat, urinmengde, urinmicro
KLINIKK

Ultralyd:
Ekkorike nyrer dag 2,
Kreatinin 437
Urinmikroskopi:
Sigarformede
kalsiumoksalatkrystaller
- monohydratform
ETYLENGLYCOL

KRONISK NYRESVIKT

KDOQI CKD klassifikasjon
2002
≈ PROTEINURIA

CKD in Norway vs USA
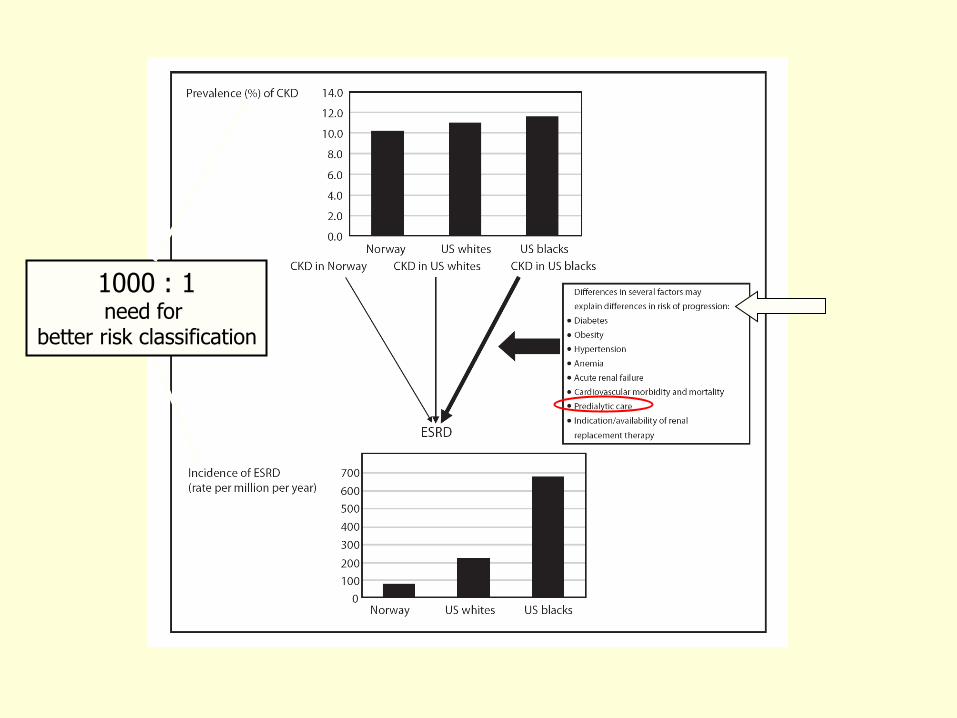
1000 : 1 need for
better risk classification

Problemer med CKD
klassifiseringen • Svært få av CKD pasienter progredierer til
ESRD
• Spesiellt stort misforhold for eldre og
kvinner
Hallan et al. BMJ 2006; 333: 1047-1053
ESRD
fre
esu
rviv
al
Time (yrs)
GFR N ESRD
> 60 62 066 0.0%
45-59 2 389 0.4%
30-44 548 1.3%
15-29 120 18.3%
Hallan et al. BMJ 2006; 333: 1047-1053
ESRD
fre
esu
rviv
al
Time (yrs)
GFR N ESRD
> 60 62 066 0.0%
45-59 2 389 0.4%
30-44 548 1.3%
15-29 120 18.3%

ESRD INCIDENCE
Norwegian Nephrology Register Annual Reports


Okinawa study
100 x
Iseki et al. Am J Kidney Dis 2004; 44: 806-814
Rates of ESRD (n=95 000, observed for 7 years)
1000 x

Fordeler med CKD klassifiseringen
• Økt søkelys på tidlige stadier av nyresykdom
med muligheter for bedre forebygging av ESRD
• Muliggjør internasjonale sammenligninger
• Gir også mulighet for forbedret CV
risikostratifisering
Astor et al. Am J Epidemiol 2008; 167.
NHANES III

Summay 1: CKD classification
4 146 (1 187 - 14 482) 2 036 (594.3 - 6 973) 641.1 (143.6 - 2 862) 196.3 (27.6 - 1 397)
6 957 (2 286 - 21 165) 3 167 (1066 - 9 403) 1 108 (285.8 - 4 297) 306.6 (50.3 - 1 871)
Macroalbuminuria
2 202 (632.5 - 7 669) 448.9 (133.7 - 1 508) 146.5 (42.7 - 502.7) 27.3 (8.8 - 84.5)
3 833 (1 265 - 11 611) 740.6 (246.7 - 2 222) 227.4 (72.8 - 710.2) 33.9 (11.2 - 102.6)
Microalbuminuria
368.7 (69.2 - 1 964) 51.9 (11.5 - 233.5) 23.4 (6.7 - 82.1) 1.0
583.1 (120.5 - 2 822) 76.0 (18.5 - 313.2) 30.8 (9.30 - 102.2) 1.0
Normal ACR
eGFR 15 - 29 eGFR 30 - 44 eGFR 45 - 59 eGFR ? 60
HIGH RISK
Macroalbuminuria
RISK MODERATE
Microalbuminuria
LOW RISK
Normal ACR
eGFR 15 - 29 eGFR 30 - 44 eGFR 45 - 59 eGFR 60




• Lifetime risk of ESRD.
• Turin TC, Tonelli M, Manns BJ, Ahmed SB, Ravani P, James M, Hemmelgarn BR.
• Source
• Division of Nephrology, Foothills Medical Centre, 1403 29th Street NW, Calgary, AB, Canada T2N
2T9. [email protected].
• Abstract
• Lifetime risk is the cumulative risk of experiencing an outcome between a disease-free index age
and death. The lifetime risk of ESRD for a middle-aged individual is a relevant and easy to
communicate measure of disease burden. We estimated lifetime risk of ESRD in a cohort of
2,895,521 adults without ESRD from 1997 to 2008. To estimate lifetime risk of ESRD by level of
baseline kidney function, we analyzed a cohort of participants who had a serum creatinine
measurement. We also estimated the sex- and index age-specific lifetime risk of incident ESRD
and accounted for the competing risk of death. Among those individuals without ESRD at age 40
years, the lifetime risk of ESRD was 2.66% for men and 1.76% for women. The risk was higher in
persons with reduced kidney function: for eGFR=44-59 ml/min per 1.73 m(2), the lifetime risk of
ESRD was 7.51% for men and 3.21% for women, whereas men and women with relatively
preserved kidney function (eGFR=60-89 ml/min per 1.73 m(2)) had lifetime risks of ESRD of
1.01% and 0.63%, respectively. The lifetime risk of ESRD was consistently higher for men at all
ages and eGFR strata compared with women. In conclusion, approximately 1 in 40 men and 1 in
60 women of middle age will develop ESRD during their lifetimes (living into their 90s). These
population-based estimates may assist individuals who make decisions regarding public health
policy.

whether the associations of eGFR and albuminuria
with all-cause mortality, cardiovascular mortality and
ESRD differ between men and women.
Objective
To assess • • •

CKD Prognosis Consortium (CKD-PC): Established in 2009
Compiles and meta-analyzes the best available data to provide
comprehensive evaluation of the impact of CKD on prognosis
46 cohorts (~2 million participants,
54% women) with data on serum
creatinine (eGFR) and albuminuria
o General population (GP) (n=1,861,052)
o At high risk (HR) for cardio-
vascular disease (n=151,494)
o CKD cohorts (n=38,612)
Methods-Study population
(Lancet 2010, KI 2011)

12
48
16
Adju
ste
d H
R
10 30 100 300 1000 3000
ACR
Female
Male
Adjusted for traditional risk factors and eGFR spline
Reference at ACR=100
End Stage Renal Disease in CKD Cohorts
12
48
16
Adju
ste
d H
R
10 30 100 300 1000 3000
ACR
Female
Male
Adjusted for traditional risk factors and eGFR spline
Reference at ACR=100
End Stage Renal Disease in CKD Cohorts
12
48
16
32
Adju
ste
d H
R
15 30 45 60
eGFR, ml/min/1.73m2
Female
Male
Adjusted for traditional risk factors and logACR/PCR or dipstick
Reference at eGFR=50
End Stage Renal Disease in CKD Cohorts
12
48
16
32
Adju
ste
d H
R
15 30 45 60
eGFR, ml/min/1.73m2
Female
Male
Adjusted for traditional risk factors and logACR/PCR or dipstick
Reference at eGFR=50
End Stage Renal Disease in CKD Cohorts
A B
C D
Results: ESRD according to eGFR (A & B) and ACR (C & D) in
CKD cohorts. (male: red, female: blue)

Conclusion
Low eGFR and/or albuminuria are at least as potent risk factors for all-cause mortality, cardiovascular mortality and ESRD in women as they are in men.

Future CKD classification
NICE / NHS Clinical guideline no 73: National clinical guideline for the management of adults with chronic kidney disease in primary and secondary care. Sept. 24. 2008
ACR >30mg/mmol (macroalbuminuria)

Albuminuri eller Proteinuri?


Why has ACR been
recomended?
• Greater sensitivity and improved precision for
the detection of lower but clinically significant
levels of proteinuria compared to total protein.
• Albumin is the predominant protein in the vast
majority of proteinuric kidney disease.
• There is no constant numerical relationship
between albumin and totalprotein. At normal
levels of protein loss albumin is a minor
component
NICE

MARKERS OF INTEREST
Kreatinin, eGFR
K, fosfat,st bikarbonat, karbamid,Hb calcium
Urin stix, albumin/kreatinin ratio
(protein/kreatinin ratio)
KLINIKK

OPPSUMMERING
• Ved akutt nyresvikt: kreatinin, karbamid, elektrolytter, st bikarbonat og urinmengde
• Ved kronisk nyresvikt: kreatinin, eGFR, elektrolytter, karbamid, st bikarbonat, urin stix, alb/kreatinin ratio
•KLINIKK


www.edren.org
• SUMMARY
• of regular monitoring for low-risk patients with < 1g
protein/d (PRC=100, ACR=70)
• Every 6 months, extending to 12-24 months if all is
unchanged, check: Blood pressure Quantitate
proteinuria (PCR or ACR) Serum creatinine

Vanlige årsaker til normotensiv
iskemisk nyresvikt
Abuelo. N Engl J Med 2007;357:797-805

Behandling av akutt nyresvikt etter
ACEI eller Ang II receptor blokker
• Seponering
• ”Motgiften” er NaCl
• Hyperkalemi kan være livstruende
• Dialyse sjelden nødvendig (<10%)
• Ultralyd/Doppler nyrer og nyrearterier
• Angiografiberedskap
• Gjenoppta behandling?

Frostvæskeforgiftning
• Livstruende tilstand (100 ml)
• Diagnostikk forsinkes ofte
• Tidlig behandling, evt. på
mistanke
• Lab. diagnostikk
• Urinfunn og ultralyd

Frostvæskeforgiftning Behandling
• Akutt dialyse
• Korrigere acidose
• Blokkere metabolisme – Etanol 1-2 o/oo
– Fomepizol
• Dialyse evt. flere uker

Effective RAS blockade should be obtained by using sufficient high ACEi doses (often higher than standard recommendations)
or by adding an ARB so that a substantial reduction in proteinuria is achieved.
Test for s-creatinine and s-K increase after 1 and 3 weeks

























