Embed Size (px)
Citation preview

Violence against children: Early recognition – early intervention
Early warningsystems
Risk assessment
Resilience research
Attachment research
Early childhoodintervention
Central issues:
IKK-News
German Youth Institute Deutsches Jugendinstitut e.V.
1–2/2005

2
Imprint
IKK-News 1–2/2005: Violence against children
ImprintPublisher and place of publication:
Informationszentrum Kindesmisshandlung/Kindesvernachlässigung (IKK)Deutsches Jugendinstitut e.V. Nockherstraße 2 D-81541 München Telephone: +49 (0)89 /62306-0 Homepage: www.dji.de
Legally responsible for editorial content: Prof. Dr. Thomas Rauschenbach
Editor: Beate Galm
Translated by: Anja Löbert, Dr. Timothy Wise
For copies, contact: Anet Holzwig +49(0)89 /62306-229 Fax: +49 (0)89 /62306-162 Email: [email protected] Internet: www.dji.de/ikk
Design: Susanne Topitsch, Nebe+Topitsch Design www.nebe-topitsch.de
Print: Offsetdruckerei Richard Rothe
IKK-News brochures are published at irregular intervals for a German-speaking readership. They can be obtained free of charge from the editors orordered directly online. The articles represent the opinion of their authors.Parts of this brochure may be reprinted with acknowledgement of source andsubmission of a specimen copy.

3IKK-News 1–2/2005: Violence against children
Contents
Violence against children: Early recognition – early intervention
Page 2 Imprint
Page 4 Preface Early prevention as a crucial step towards protecting children against violence and fostering their development
Page 6 Gregor Hensen:Social early warning systems in North Rhine-Westphalia – Early family intervention by means of obligatory forms of cooperation
Page 11 Dr. Heinz Kindler & Susanna Lillig: Early identification of families with increased risk of abuse or neglect
Page 15 Corina Wustmann: “As early as possible!” – Results of research into resilience
Page 21 Patricia M. Crittenden, Ph.D.: Preventive and Therapeutic Intervention in High-Risk Dyads: The Contribution of Attachment Theory and Research
Page 28 Prof. Dr. Gerhard J. Suess: STEEP™: Early intervention to promote resilience in at-risk childhoods
Page 32 Inge Beyersmann: A chance for psychosocially burdened mothers with babies and infants
Page 39 Ruth Wollwerth de Chuquisengo & Heike Kreß: Excessive crying during the first months of life and its treatment in the “Munich Consultation Hours for Crying Babies”
Page 45 Anke Laukemper: On-call family care by the youth office in Hamm as an example of early childhood intervention
Page 48 Project Announcement Prevention through early childhood intervention
Contents

4
Preface
IKK-News 1–2/2005: Violence against children
Dennis has his first day at school. Just afew days later the teacher notices hisaggressive behaviour. Only now does itcome to light that the little boy is suffer-ing as a result of various strains uponhim: experiences of violence, neglect, andthe denial of affection. In his case earlyprevention would have been an effectiveway to protect him against violence andto foster his development.
Parental violence against children is oftena result of a combination of psychosocialfactors: parents who themselves wereabused or neglected and experienced alack of empathetic affection; parents whonow tend to “solve” conflicts violently;parents who are facing numerous prob-lems and can scarcely fall back ontrusting relationships, supportive social net-works or prospects of life. Without ade-quate intervention both children andparents are going to suffer from the con-sequences of this strain, with the parentsbeing overtaxed by the task of raisingtheir offspring.
Early childhood intervention begins beforeunfavourable developments have a chanceto become fixed. Essential to this helpare early recognition and risk assessment.It is now necessary to extend this sectorin Germany and to go beyond the assess-ment of experts from individual institu-tions through the establishment of inter-disciplinary cooperation and early warn-ing systems. This increases the capabilityto react before the eruption of an acutecrisis and its serious repercussions.
According to the results of research intoattachment and resilience many approach-es to early prevention foster positiveinteractions between parents and theirchild or infant. Parents are being helpedto understand better the needs and sig-nals of their children, to assess theirstage of development more realistically,and to respond more appropriately to
their infant. For instance, this process canbe supported by video-assisted consulta-tions and suggestions regarding sensitiveinteraction while feeding, nappy-changingor playing. The development of defencemechanisms is aided by the secureattachment of the infant to at least oneperson it relates to most closely, a parentor some other central figure. Secureattachment can be seen as an importantshield that, in combination with otherprotective factors, serves as a cushionwhen problems occur.
The quality of the parent-child-relation-ship influences all sectors of child develop-ment. If the infant is neglected andsubjected to a permanent monotony ofstimuli, or if it is overwhelmed by inap-propriate stimuli, then not only its emo-tional and possibly physical developmentare affected, but also its cognitive growth.What is missing here is an age-appro-priate engagement with the child and itsnurturing during the stage of infancy – a time of crucial significance in regard tothe development of intellect and interests.
If families receive adequate support, theinfant is presented with a variety of pro-spects early on. However, families thatare subjected to a high level of psychoso-cial stress are especially difficult to reach.Structures of violence and neglect havepossibly pervaded them for many gen-erations. Patterns of interaction likely tolead to conflict, unstable relationships,and frequent relational breakdowns getrepeated. These experiences can recurand consolidate even in the context ofan aid system if appropriate forms ofintervention are missing and inadequateforms of help fail. Because of their lifehistory and living circumstances thosefamilies require extraordinary expertise.They rely on flexible, if necessary pro-active, offers geared towards the particu-larities of their lives. A precondition for a long-term, successful cooperation
between specialists and parents is thecreation of a sustainable relationship bet-ween them. However, the work towardssuch a relationship is time-consuming,and time is a rare resource in this hard-pressed era. Yet, the experience of astable, positive relationship is an essentialprerequisite in order to break successfullythe cycle of neglect and abuse. Further-more, an improvement of the situationcalls for multimodal, versatile, often verypractical support, for example withregard to the application for a washingmachine or to the organisation of thehousehold.
The efforts pay off: long-term studiessubstantiate the effectiveness of earlyprevention in high-risk families. One-offintervention, however, is hardly enough.Psychosocially burdened families mostlyneed long-term, continuous guidancethat fosters and consolidates positiveprocesses of development while takinginto consideration the current needs andresources for each case. This given, earlyprevention can be a first decisive steptowards providing the children concernedwith sustaining future prospects.
In this issue of IKK-News our authorsexplain methods of early risk assessment.They give an account of the results ofresearch into resilience and attachmentand introduce early childhood interventionfor a variety of target groups: for psycho-socially burdened families, as well as forparents whose children particularly taxtheir interaction competence, for instancethrough excessive screaming. In the lastarticle we discuss developments in thefield of child protection. (Further contribu-tions towards these subjects can befound in the IKK-News 2/2001 – only asgerman version. This issue can be ob-tained free of charge from the IKK and isalso available on the website of the IKKwww.dji.de/ikk as a PDF-file.)
Preface
Early prevention as a crucial step towardsprotecting children against violence andfostering their development

5IKK-News 1–2/2005: Violence against children
We would like to thank those who con-tributed through their various articles tothe information in this brochure. We welcome readers to offer any helpfulsuggestions.
Beate Galm
Literature
Ahnert, L. (2005): Entwicklungspsychologische Erfordernisse beider Gestaltung von Betreuungs- und Bildungs-angeboten im Kleinkind- und Vorschulalter. In: Sachverständigenkommission Zwölfter Kinder-und Jugendbericht (Hrsg.): Bildung, Betreuung und Erziehung von Kindernunter sechs Jahren. München: Deutsches Jugendinstitut, 9–54.
Crittenden, P. M. (2003): Frühe Förderung von Hochrisiko-Kindern: Der Beitrag von Bindungstheorie undBindungsforschung. In: Verein für Kommunalwissenschaften e.V. (Hrsg.): It Takes Two to Tango. Frühe Kindheit an derSchnittstelle zwischen Jugendhilfe undEntwicklungspsychologie. Berlin: Verein für Kommunalwissenschaften e.V.
Egeland, B., Jacobvitz, D., Sroufe, L. A. (1988):Breaking the Cycle of Abuse. In: Child Development, 59, 1080–1088.
Erickson, M. F., Kurz-Riemer, K. (1999): Infant, Toddlers, and Families.New York: Guilford Press.
Galm, B. (2004): Was ist im Kontakt mit Familien zu beachten,die Vernachlässigungsstrukturen aufweisen? In: Kindler, H., Lillig, S., Blüml, H., Werner, A.,Rummel, C. (Hrsg.): Handbuch Kindeswohlgefährdung nach § 1666 BGBund Allgemeiner Sozialer Dienst.Internetveröffentlichung des Deutschen Jugend-instituts.
Karoly, L. A., Greenwood, P. W., Everingham, S. S.,Houbé, J., Kilburn, M. R., Rydell, C. P., Sanders, M.,Chiesa, J. (1998): Investing in Our Children. What We Know andDon’t Know About the Costs and Benefits ofEarly Childhood Interventions. Santa Monica: Rand.
Kindler, H. (2005): Wie können Misshandlungs- und Vernach-lässigungsrisiken eingeschätzt werden? In: Kindler, H., Lillig, S., Blüml, H., Werner, A. (Hrsg.):Handbuch Kindeswohlgefährdung nach § 1666 BGBund Allgemeiner Sozialer Dienst (ASD).Internetveröffentlichung des Deutschen Jugend-instituts.
Niebank, K., Petermann, F. (2002): Grundlagen und Ergebnisse der Entwicklungs-psychopathologie. In: Petermann, F. (Hrsg.): Lehrbuch der Klinischen Kinderpsychologie und -psychotherapie. Göttingen: Hogrefe, 57–94.
Rutter, M. (1990): Psychosocial resilience and protectivemechanisms. In: Rolf, J., Masten, A. S., Cicchetti, D.,Nuechterlein, K. H., Weintraub, S. (Eds.): Risk and protective factors in the development ofpsychopathology. New York: Cambridge University Press, 181–214.
Schefold, W. (2004): Erziehungshilfen im gesellschaftlichen Kontext:Zur Entgrenzung der Kinder- und Jugendhilfe. In: Lenz, K., Schefold, W., Schröer, W. (Hrsg.):Entgrenzte Lebensbewältigung. Weinheim: Juventa, 159–237.
Shonkoff, J. P., Meisels, S. J. (Eds.) (2000): Handbook of early childhood intervention. Cambridge: Cambridge University Press.
Zenz, W. M., Bächer, K., Blum-Maurice, R. (Hrsg.)(2002): Die vergessenen Kinder. Köln: PapyRossa.
Preface

6
From research and practice
IKK-News 1–2/2005: Violence against children
Starting position
Growing up is a process conditionedby the environment in which it takesplace, by the people who accompany thisprocess, as well as by the abilities andpotentials the child acquires during eachformative phase. But a child’s develop-ment does not always proceed under idealconditions. Depending on their personalresources and the structures of disadvan-tage they are exposed to and on howchildren pass through the transitions intheir biography and under which circum-stances they grow up, dangers and riskscan evolve and solidify which have animpact on later stages of development.
Risks and dangers in the developmentof children and adolescents do not ariseovernight. They are often heralded earlyon. As a rule, child neglect does notresult from “extreme and unexpectedlyoccurring situations of emotionalpressure but evolve from the normalityof family constellations that blunder intothese stresses without the chance todevelop appropriate solutions in time.”(Schone, 2000, p.447) The current sys-tem of help and assistance operating in the German health sector and its fam-ily and youth welfare system maintains a broad spectrum of adequate servicesand offers. However, the early recognitionof high-risk situations often falls short ofsuccess. What is still missing are system-atic institutional procedures and coordi-nated intervention thresholds as a guide-line for action. For example, the problemof identification is normally carried outunder the jurisdiction of the GeneralSocial Service1 by the subjective assess-ment of a skilled employee (see Münderet al., 2000, p.165).
The various social institutions thatchildren and their families come intocontact with in their daily lives oftenoverlook or insufficiently perceive faintindications. They do not respond untilsignals point to grave problems or acutecrises. This late reaction is owed to thediverging interpretation of these signalsaccording to each institution and its
inner logic of action, because institutionsand their employees cannot or do notexchange experiences and observations withothers and because responsibilities areinsufficiently regulated or operate in avacuum. A further complication is thatfamilies that exhibit forms of childneglect or abuse are often socially isolated(see Ziegenhain et al., 2004, p.108).
If high-risk developments during theprocess of growing up are to be con-trolled at an early stage, even faint indi-cations need to be recognised and inspect-ed for their danger potential. In order totake early action in the true sense, thethreshold points at which a normal stateturns into a critical state need to berecognised. Often diverse and complexfactors influence the growing-up of chil-dren and, thus, the possibility of anyhigh-risk developments. Hence, a multi-tude of issues and observations need tobe watched and drawn on as indicators.
The recognition and assessment ofsignals and indications alone is notenough. The objective to counteract andeven to prevent precarious developmentscan only be achieved successfully if, onone hand, the institutions and people incharge are specified, and, on the otherhand, the appropriate institutions andagents involved act on the firm basis ofbinding mutual agreement.
Early identification and attention toproblem situations and developmentaldifficulties, for instance in the periodpreceding early learning support or othermeasures of higher intensity, requires anew binding character of the inter-insti-tutional cooperation. The final decisionregarding which institutions or servicesare suitable as points of contact for theconstitution of a social early warning sys-tem depends on both the existing on-sitestructures and the selected area of appli-cation. What are necessary are cross-insti-tutional analyses of the areas in whichcritical developments or support needs offamilies have become apparent or could
be assumed. The determination of amapped-out system of reference is ofcrucial significance for the success of anearly warning system: it is important,particularly with regard to the complexi-ties of familial situations and problemareas, to select a well-defined object areathat is transformable into manageablenetworks on a local level.
The pilot project “Social earlywarning systems in North Rhine-Westphalia”
With financial backing from the NorthRhine-Westphalian Ministry of FamilyAffairs a social early warning system pilotprogramme was developed and testedfrom September 2001 through 2004 insix locations (Bielefeld, Dortmund,Emmerich, Herne, Kreis Siegen-Wittgen-stein, and Society for the Prevention ofCruelty to Children – Division in Essen/NRW). During these three years theInstitut für Soziale Arbeit e.V. (Institutefor Social Work) was responsible for theacademic monitoring of the project.
With the aid of this pilot programmeapproaches and interdisciplinary formsof cooperation were developed whichserve the early identification of childrenand families at risk and, hence, preventthe consolidation of problems in goodtime. For this purpose, sensors and indi-cators were developed during the courseof the project which are intended toshow when the circumstances of childrenand their families can be classified ascritical and which responses are appro-priate to deal with such problems.
From the six pilot projects variousareas were selected in which, accordingto the participating institutions andagents, critical developments or needs forassistance in families have become appar-ent or could be assumed.
Gregor Hensen
Social early warning systems in North Rhine-Westphalia – Early family intervention by means of obligatory forms of cooperation
1 Allgemeiner Sozialer Dienst (ASD)Explanation on www.dji.de/asd

7
From research and practice
IKK-News 1–2/2005: Violence against children
Early warning system – Infant neglectIn cooperation with the Bielefeld chil-
dren’s and birth clinic, as well as the localSociety for the Prevention of Cruelty toChildren, families with infants could besuccessfully assisted in mastering the attimes critical first phase of life with the aidof voluntary godmothers. The project suc-ceeded because of the lasting and mutualcooperation of all institutions involved.
Early warning system – Neglect of living conditions
In Emmerich, too, critical social cir-cumstances were cause for action.During the course of the programmeseveral families who lived under unrea-sonable housing conditions could besupported in improving their situation.
Early warning system – Behavioural problems of children
The staff of the day-care centre forchildren in Herne is now equipped to recognise the first signs of behaviouralproblems and to plan together with theparents the next steps towards dealingwith them by a clearly defined protocol.
Early warning system – Biographicaltransition – kindergarten/primary school
The Dortmund project managed toattain improvement in children’s copingwith the transitional period from nurseryschool to primary school through the closecooperation of child day-care centres, pri-mary schools and youth welfare services.
Early warning system – Socio-economic trouble-spots
In the District of Siegen-Wittgensteinthe residential areas were made moretransparent for the staff of the regionalsocial services by means of a number oftechniques and methods. Hence, thecapacity for response was enhanced (e.g. in the development of services forfamilies that had, so far, not been reached).
Early warning system – Child neglectAmong other things the German
Society for the Prevention of Cruelty toChildren compiled a handbook alongwith and for the staff of a day-care centrein Essen-Mitte District. Here, contactpeople for the concerns of children,adolescents and families are specified,and “first steps” in dealing with initial
signs of child neglect are described (for a more thorough discussion of theindividual pilot locations see MGSFFNRW, 2005b).
The examples taken from the pilotphase illustrate the emergence of six earlywarning systems which are closely coupledto the problems, resources and modes ofcooperation of the individual commu-nity. They all are governed by the princi-ples of interdisciplinary cooperation,continuing development and transitiontowards more flexibility in existing formsof assistance, sensitisation of skilledemployees, and a neighbourhood-sensi-tive localisation of projects. Professionalrecommendations within the scope of different strands of discourse aroundprevention, participation, quality andneighbourhood-sensitivity all meet in theaims and objectives of a social earlywarning system.
In summary, a social early warningsystem for families can be understood asa necessary (and overdue) attempt tobring together different disciplines, pro-fessions, perceptions, and proceduresinto one coordinated and effective inter-action. A social early warning system isnot a new institution that defines servicesof its own. Its strength is rather in theconstructive joining together of existingauthorities within the community.
Theoretical background
The term “early warning systems” doesnot originate in the realm of the social.Instead, we are familiar with it in relationto technical systems (e.g. seismographswarn against earthquakes and smokedetectors alert us to fires). Even thoughexamples from the technical sphere dem-onstrate how early warning systems func-tion in a general sense (see Schatz, 2003),a direct transference to social circum-stances is not possible. When looking atsocial issues it is evident that one-dimen-sional measuring methods are insuffi-cient. Social early warning systems focuson the development of living conditionsin the social space families inhabit or onthe social situation of individual targetgroups and cohorts. The focal point ofall support and service eforts is the socialcircumstances and the interactions pro-ceeding therein between children, adoles-
cents and families. “Hence, ‘critical devel-opments’ of children and their familiesencompass different aspects of the chil-dren’s and parental lifestyle which areconsidered unreasonable and insufficientin the eye of social conventions and pro-fessional norms in a culture” (Wagenblass,2005, p.775, italics in original). Here,an implicit understanding of normalitybecomes a benchmark of perception andassessment. Therefore, a process of com-munication and coordination regardingthis matter and involving all relevantagents is fundamental to the implemen-tation of social early warning systems.
Social early warning systems are basedtherefore on the development of mutual-ly shared criteria of assessment of “normalstates” and their transitions which dependon professionally established standardsthat should result in obligatory responsesfrom the institutions. In addition to that,new approaches of an interdisciplinarynature will be developed regarding familieswhose problems might escalate into acrisis, and access will be sought to socialspaces that threaten to change and createsocial deprivation for families there.
In their practical implementation thesebasic theoretical ideas require the com-bination of several components – namelyskilled perception, clear notification, and consistent, coordinated action –within one overall system (see MGSFFNRW, 2005a and b).
How does an early warning system work?
A social early warning system is a closedchain of responses consisting of threebasic elements: identification, notification,and action. It is an agreement betweenspecialists in family support and in theadvisory services. The early warning systemcan refer either to a particular target group,to clearly specified problems in an indi-vidual case, or to a selected social space.
The capability afforded by the earlywarning system results from those clearlydefined stages through which the systemruns: on the identification of a danger-ous situation, an alert is given which isfollowed by action of a certain kind (see illustration 1). At this juncture thechoice of a reference system is of mar-ginal significance.

8
From research and practice
IKK-News 1–2/2005: Violence against children
Agree on threshold values
In order to recognise indications ofcritical developments it does not sufficemerely to identify deviances and potentialdangers within the context of an earlywarning system; they also need to beevaluated and filtered. This makes itnecessary to specify threshold values whosetransgression heralds the entrance intoa critical state and which is the basis for
the notification. Again, with regard tothese threshold values we cannot rely on“objective” reports. While it may bepossible to predict with some accuracythe amount of pressure a boiler is able towithstand before it bursts, such criticalvalues are much harder to pinpoint onthe social level (Jordan & Wagenblass,2002, p.178).
Illustration 2 shows the operation of a social early warning system using theanalogy of traffic lights. Many problemsand high-risk situations become apparentwhen the light switches, as it were, fromyellow to red, in other words only whenlatent problems have already become set and turned into acute crises, puttingthe child’s well-being at risk. It is then,normally, that intervention begins. A socialearly warning system, however, alreadydirects its scrutiny towards faintly per-ceptible signals at the stage of transitionfrom the normal state. In order to beable to substantiate the individual thresh-old values (from green to yellow, fromyellow to red) indicators need to be spec-ified which announce or initiate suchtransitions.
Specify indicators
Social systems are highly complex,controlled by multiple factors. Usuallythey are not made by a single criterionthat merely needs to be evaluated ormeasured. Therefore social early warningsystems need to be based on indicatorsthat can predict, with an (ideally) highprobability of success, events that are notdirectly measurable. An indicator is anauxiliary parameter that reflects an indi-rectly perceivable or measurable aspect ofa social phenomenon (Jordan, 2000,p.340). As an example, the income ofthe population can be drawn upon as anindicator of the “living standard”. Thisexample reveals the hypothetical natureof the relationship between the measuredindicator and the phenomenon of inter-est. An adequate system of social indica-tors is assigned the task of facilitatingsustainable and systematic monitoring ofsocial occurrences and problems (ibid.).
Specify threshold values
If we are to influence and counteractthe unfavourable developments duringthe process of child-raising at an earlierstage than previously, such faint signalsneed to be recognised and systematicallyinspected for their potential dangers.Early action can only be taken if weknow the threshold at which the normalstate is abandoned and a critical state canbe expected. However, few cases showonly one indication of a crisis or problem.Usually multiple and complex factorsaffect children’s growing-up and, thus, maycontribute to the possibility of a criticaldevelopment. Therefore it is necessary to consult a variety of aspects and factsof the case as indicators in order to get a clear picture and to be able to activatethe appropriate services.
Counteract risks
The mere recognition and assessmentof signals or indicators is not sufficientbecause the aim to counteract and evento prevent critical development can onlybe achieved if the responsible individualsor institutions are clearly specified, andthat these people will then act upon theirobservations. Among the involved agentsand services precise arrangements mustto be made concerning who is responsiblefor which task at what stage; in otherwords, a course of action will come intoexistence, the outcome of which will betangible help and assistance for the childor the family. This provided, then throughjoint efforts risks in child-raising can be prevented earlier and more effectively.
Establish an obligatory network
In the past, cooperation was often aproduct of coincidence or of the endeav-ours of individual specialists. A socialearly warning system, however, aims at a“system change” towards coordinatedcross-institutional cooperation and bind-ing agreements. This makes it necessaryto analyse at the outset in which branchesof work families’ risk developments andsupport needs have already come to thesurface, where they can be assumed, andwhich agents can make a contribution.
identification
notification
action
Submit explicit warning notice toresponsible institutions and agents
Consistent and prompt response of particular institution or jointly withother services
[
[
Illustration 1: Basic elements of a social early warning system
“normal state”
latent crisis or faint signals
acute crisis or solidification
[ threshold
[ threshold
Illustration 2: Phase model (see also MGSFF NRW, 2005a, p.7)
Identify potential dangers and developsensors; assess, verify and filter observations
9
From research and practice
IKK-News 1–2/2005: Violence against children
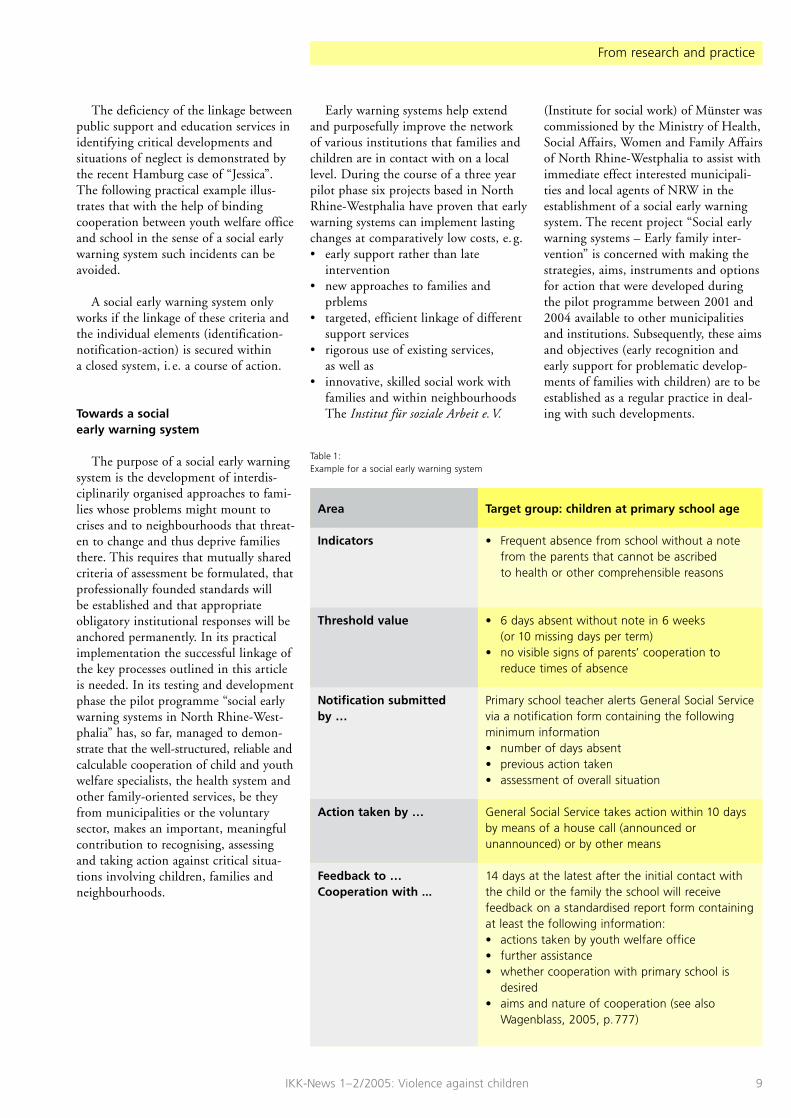
The deficiency of the linkage betweenpublic support and education services inidentifying critical developments andsituations of neglect is demonstrated bythe recent Hamburg case of “Jessica”.The following practical example illus-trates that with the help of bindingcooperation between youth welfare officeand school in the sense of a social earlywarning system such incidents can beavoided.
A social early warning system onlyworks if the linkage of these criteria andthe individual elements (identification-notification-action) is secured within a closed system, i. e. a course of action.
Towards a social early warning system
The purpose of a social early warningsystem is the development of interdis-ciplinarily organised approaches to fami-lies whose problems might mount tocrises and to neighbourhoods that threat-en to change and thus deprive familiesthere. This requires that mutually sharedcriteria of assessment be formulated, thatprofessionally founded standards will be established and that appropriateobligatory institutional responses will beanchored permanently. In its practicalimplementation the successful linkage ofthe key processes outlined in this articleis needed. In its testing and developmentphase the pilot programme “social earlywarning systems in North Rhine-West-phalia” has, so far, managed to demon-strate that the well-structured, reliable andcalculable cooperation of child and youthwelfare specialists, the health system andother family-oriented services, be theyfrom municipalities or the voluntarysector, makes an important, meaningfulcontribution to recognising, assessingand taking action against critical situa-tions involving children, families andneighbourhoods.
Early warning systems help extendand purposefully improve the network of various institutions that families andchildren are in contact with on a locallevel. During the course of a three yearpilot phase six projects based in NorthRhine-Westphalia have proven that earlywarning systems can implement lastingchanges at comparatively low costs, e. g.• early support rather than late
intervention• new approaches to families and
prblems• targeted, efficient linkage of different
support services• rigorous use of existing services,
as well as• innovative, skilled social work with
families and within neighbourhoodsThe Institut für soziale Arbeit e.V.
(Institute for social work) of Münster wascommissioned by the Ministry of Health,Social Affairs, Women and Family Affairsof North Rhine-Westphalia to assist withimmediate effect interested municipali-ties and local agents of NRW in theestablishment of a social early warningsystem. The recent project “Social earlywarning systems – Early family inter-vention” is concerned with making thestrategies, aims, instruments and optionsfor action that were developed duringthe pilot programme between 2001 and2004 available to other municipalitiesand institutions. Subsequently, these aimsand objectives (early recognition andearly support for problematic develop-ments of families with children) are to beestablished as a regular practice in deal-ing with such developments.
Target group: children at primary school age
• Frequent absence from school without a notefrom the parents that cannot be ascribed to health or other comprehensible reasons
• 6 days absent without note in 6 weeks (or 10 missing days per term)
• no visible signs of parents’ cooperation toreduce times of absence
Primary school teacher alerts General Social Servicevia a notification form containing the followingminimum information • number of days absent• previous action taken• assessment of overall situation
General Social Service takes action within 10 daysby means of a house call (announced orunannounced) or by other means
14 days at the latest after the initial contact withthe child or the family the school will receivefeedback on a standardised report form containingat least the following information:• actions taken by youth welfare office• further assistance• whether cooperation with primary school is
desired• aims and nature of cooperation (see also
Wagenblass, 2005, p.777)
Area
Indicators
Threshold value
Notification submitted by …
Action taken by …
Feedback to …Cooperation with ...
Table 1: Example for a social early warning system

10
From research and practice
IKK-News 1–2/2005: Violence against children
This objective is advocated by twoarguments in particular:1. The pilot projects demonstrated that
systematic identification of critical lifesituations of children, adolescents andfamilies within the scope of cross-institutionally agreed patterns of prob-lem assessment (definition of riskthresholds) results in earlier and easy-to-participate-in provision of support.Binding, reliable and “calculable” coop-eration among different service areasleads to an optimisation of supportprocesses and makes a significant con-tribution towards an accurate deploy-ment of resources.
2. Among other things, this model putsstronger emphasis on the findings ofinfant-attachment-research than otherapproaches to prevention in the fieldof social work with families andchildren. It therefore gains a qualita-tive advantage: the specialists’ scope of action is significantly enhanced bythese findings (e.g. “recognise biograph-ical transitions as ‘sensitive stages’ ”,“strengthen parent-child-attachment”,“intervene at an earlier stage”).
Contact
Gregor HensenPedagogue,Research associate
Institut für soziale Arbeit e.V. Studtstraße 20 D-48149 Münster
Telephone: +49 (0)251 /92536-0Email: [email protected]: www.soziales-fruehwarnsystem.de
Literature
Jordan, E. (2000): Sozialraum und Jugendhilfeplanung. In: Jordan, E., Schone, R. (Hrsg.): Handbuch Jugendhilfeplanung. Grundlagen,Bausteine, Materialien. Münster: Votum, 331–388.
Jordan, E., Wagenblass, S. (2002): Soziale Frühwarnsysteme. In: ISA-Jahrbuch zur Sozialen Arbeit. Münster: ISA – Institut für soziale Arbeit,175–195.
Ministerium für Gesundheit, Soziales, Frauen undFamilie des Landes Nordrhein-Westfalen (MGSFFNRW) (Hrsg.) (2005a): Soziale Frühwarnsysteme – Frühe Hilfen fürFamilien. Arbeitshilfe zum Aufbau und zurWeiterentwicklung lokaler sozialer Früh-warnsysteme. Münster: ISA – Institut für soziale Arbeit.
Ministerium für Gesundheit, Soziales, Frauen undFamilie des Landes Nordrhein-Westfalen (MGSFFNRW) (Hrsg.) (2005b): Soziale Frühwarnsysteme in NRW –Ergebnisse und Perspektiven einesModellprojekts. Münster: ISA – Institut für soziale Arbeit.
Münder, J., Mutke, B., Schone. R. (2000): Kindeswohl zwischen Jugendhilfe und Justiz.Professionelles Handeln in Kindeswohl-verfahren. Münster: Votum.
Schatz, R. (Hrsg.) (2003): Frühwarnsysteme. Fribourg: Innovatio.
Schone, R. (2000): Planung für Zielgruppen: Hilfen für Säuglingeund Kleinkinder in schwierigen Lebens-bedingungen. In: Jordan, E., Schone, R. (Hrsg.): Handbuch Jugendhilfeplanung. Grundlagen,Bausteine, Materialien. Münster: Votum, 442–460.
Wagenblass, S. (2005): Soziale Frühwarnsysteme – Frühe Hilfen fürKinder und Familien. In: Deegener G., Körner, W. (Hrsg.):Kindesmisshandlung und Vernachlässigung. Ein Handbuch. Göttingen: Hogrefe, 770–781.
Ziegenhain, U., Fries, M., Bütow, B., Derksen, B.(2004): Entwicklungspsychologische Beratung fürjunge Eltern. Grundlagen undHandlungskonzepte für die Jugendhilfe. Weinheim und München: Juventa.

11
From research and practice
IKK-News 1–2/2005: Violence against children
There is an international consensusthat abuse and neglect of children is asevere problem (Krug et al., 2002). Thefurther development of strategies todiagnose and to intervene when a child’swell-being is threatened was paramountnot only in the German youth welfarediscussion of recent years (Münder et al.,2000; Kindler et al., in print), but alsoin the international one (e.g. MacDo-nald, 2001; Munro, 2002). In the lightof the suffering associated with crueltyand neglect for both affected childrenand parents, there has been an ongoingdiscussion in several waves since the 1970sregarding the possibility of primaryprevention of abuse or neglect (on thehistory of the debate see Daro & Don-nelly, 2002; key contributions are forinstance Browne et al., 1988; Wolfe, 1991;Thompson, 1995; Guterman, 2001). To a certain extent universal measures ofprevention directed towards all parentswere tested (Sanders et al., 2003)
Attempts to realise such measureswere directed, for instance, to the intro-duction of a legal ban against corporalpunishment (e.g. Bussmann, 2003), aswell as better information about the dan-gers of shaking babies and infants (Diaset al., 2005). The thematic focus of theinternational debate, however, was onselective measures of prevention. In otherwords, measures aiming at families withheightened risk of abuse and neglect.Selective measures of prevention provideimportant advantages. First and foremostthey allow a concentration of existingresources and consequently more intensivemeasures of prevention in those areas ofsociety where they are most urgentlyneeded. Selective prevention measures,however, can only be effective under aseries of preconditions:• Firstly, crucial risk factors of abuse or
neglect need to be known • Secondly, these crucial risk factors
need actually to apply to a majority ofcruelty and neglect cases1
• Thirdly, relevant risk factors need tobe directly observable in practice and
• Fourthly, if the crucial risk factors arepresent, effective strategies of actionneed to be readily available which are
able to influence causal risk mecha-nisms behind the statistical risk factors
The article at hand will provide an over-view of the research towards the firstthree bullet points.
Risk factors of abuse or neglect in the general population
The number of surveys looking at riskfactors of abuse and neglect has increasedconsistently in the past 30 years (for twosystematic research reviews see Black et al.,2001; Schumacher et al., 2001). Particu-larly substantial for primary preventionare research projects that examine abroad spectrum of possible risk factorswithin the scope of representative samplesof newborns over longer periods. Thecredibility is further bolstered by findingsconfirmed in several studies conductedin different countries or ethnic-culturalgroups using different methods for iden-tifying abuse and neglect. However, sur-veys that meet these conditions com-pletely or at least for the most part arestill very rare (Brown et al., 1998; Side-botham et al., 2001, 2002; Wu et al.,2004). The most significant risk factorsextractable from this research are pover-ty, substance abuse, and a history ofsevere mental illness. If these risk factorsare seen only in isolation, the likelihoodof abuse or neglect by these parents is on average tripled and even quadrupled.For a number of further factors, such as juvenile motherhood or the necessityof taking care of several preschool agechildren at home, a doubled and even tri-pled risk of abuse or neglect was repeat-edly found. Because of the interaction ofsample size and intensity as well as thetime needed to investigate families, thebig studies mentioned so far are limitedto risk factors that are comparatively easyto identify. From in-depth long-termsurveys with smaller samples several otherhigh risk factors (with risk increased from3 to 6 times) are known, such as violencebetween partners, distinct feelings ofpowerlessness towards the child or a per-sonal history of abuse or neglect by aparent (Ertem et al., 2000; Kindler, in
print). Smaller surveys need to focus onsamples with an increased basic likeli-hood of abuse or neglect (e.g. familiesbelow the poverty line), in order toattain any results at all. This, of course,limits the possibility of generalising fromthese findings to the level of the overallpopulation.
As in other areas of risk research (e.g.Appleyard et al., 2005) a huge increasein danger with regard to the risk of abuseand neglect in the general populationwas registered if several risk factors coin-cided. In the survey conducted by Brownet al. (1998) this threshold occurred atthe convergence of more than three ap-plying risk factors. According to thestudy of Wu et al. (2004) slightly morethan 50 % of all known cases of abuse inthe first three years of life occurred inthe group of families with three or morerisk factors (13 % of the group of parentswith a new-born child). These numbersshould serve to demonstrate the poten-tial of early selective prevention.
Techniques of screening abuse andneglect risks
Based upon the results of studies intorisk factors and their cumulative statisti-cal effects an attempt was made at differ-ent places on an international level todevelop screening procedures for theidentification of families with a distinctlyincreased risk of abuse and neglect, inorder then to be able to offer the affectedmothers and fathers voluntary, preventa-tive support. An analysis of 19 preventionprogrammes against abuse and neglectshowed that the majority (14) focussed onrisk groups, while 5 programmes lookedonly at individual risk groups (such asjuvenile mothers), and the rest screeneda greater spectrum of possible risk factors
Dr. Heinz Kindler & Susanna Lillig
Early identification of families with increased risk of abuse or neglect
1 This cannot be taken for granted. The meta-bolism disorder phenylketonuria, for instance, inits untreated form constitutes a considerable riskfactor for mental impairment of children. At thesame time, only a small minority of childrenliable to mental impairment are exposed to thisrisk factor.

12
From research and practice
IKK-News 1–2/2005: Violence against children
(Guterman, 1999). Another recentlypublished evaluation of 43 selective pre-vention programmes (Geeraert et al.,2004) showed that 25 programmes haddrawn upon existing screening proce-dures, while the majority of the remain-ing programmes used self-developedmethods. Screening procedures workwell if• they identify reliably those cases that
later indeed exhibit abusive ornegligent behaviour (sensitivity) and
• they preferably classify families thatdo not exhibit this behaviour as low-risk families (specificity)
Presently there are about a dozen surveysthat have tested the predictive efficiencyof screening procedures (see Leventhal,1988; McCurdy, 1995; Peters & Barlow,2003; Nygren et al., 2004 for researchsurveys). The sensitivity of the examinedinstruments ranged from 30 to 100 %with a distinct emphasis above 80 %.The specificity data is slightly less favour-able, varying between 20 to 90 %, whilebeing more evenly distributed. The cen-tral tendency is around 80 %.
To illustrate this data a survey byMurphy et al. (1985) can be used, whichtested the explanatory power of a certaininstrument, the “Kempe Family StressInventory”. A sample of 600 pregnantwomen was interviewed with this instru-ment and then assigned to either a high-risk or a low-risk group. Later, whentheir children were one or two years old,the high-risk group families as well as a random sample of the families formerlyassigned to the low-risk group were re-examined based upon medical records ofwhether or not their children had mean-while been treated in relation to abuse orneglect. The sensitivity of the instrumentswas as high as 80 %; in other words, outof 25 cases with documented cruelty andneglect 20 had already been classified as high-risk during pregnancy. The speci-ficity was as high as 89 %, meaning outof 170 children that did not show anysign of abuse or neglect 152 had previ-ously been assigned to a low-risk group.
The available data on the sensitivityof screening procedures indicate that a high proportion of children that laterbecome victims of maltreatment couldhave been detected early for preventativemeasures. The data on specificity, how-ever, tells a different story. Because the
group of non-abusive and non-negligentparents is very sizable, even a specificityof 80 % and higher means that, in abso-lute numbers, many parents were wrong-ly classified as at-risk families. The sur-vey of Murphy et al. (1985) saw a rate of52 % of parents from the high-risk groupwhose children were later effectivelyexposed to abuse or neglect. The conclu-sion we draw from this is that screeningtechniques do not exclusively filter outchild abusers. Some of the so-calledatrisk parents would never, even withoutsupport, maltreat their children. Thatmeans these instruments need to be dealtwith responsibly and thoughtfully inorder to avoid an undue discrimination ofaffected and unaffected parents by bothspecialists and public. This is only aboutconfidently reaching such parents who,with a higher average likelihood thanothers, will encounter difficult or evendangerous situations with their children.
Which factors are considered by established screening tools?
As yet, there is no systematic and re-cent analysis of risk factors considered inestablished screening tools. We havetherefore opted to illustrate the chosenfactors and concrete modus operandiwith the help of two examples. The afore-mentioned “Kempe Family Stress Inven-tory” is a ten-item-scale whose assess-ment of “no problem”, “mild problem”and “severe problem” is based uponinterviews with mothers. There are a fewsuggestions regarding the conducting ofthe interview but no strictly standardisedform. The items to be evaluated com-prise the experience of abuse or neglectin the parents’ own childhood, social iso-lation of the parent, low self-esteem ordepression, potential for violent temperoutbursts, as well as unrealistic and rigidexpectations of child’s behaviour or de-velopment. After assessing the individualaspects a total score is created from all“mild problem” and “severe problem”responses. Ultimately, a final case assess-ment as high or low-risk is made basedupon a previously fixed criterion. A de-tailed description of the method and theavailable research can be found in Korf-macher (2000). Because the interviewcan take over an hour, several larger pre-vention programmes use a two-phase
technique that first selects various fami-lies through a quickly filled in list of riskfactors who are then interviewed usingthe “Kempe Family Stress Inventory”. If applicable they are then offered partici-pation in a prevention programme (e.g.Duggan et al., 2000). While the “KempeFamily Stress Inventory” originated inthe United States, a new screening toolwas developed only recently in Belgiumwhich is based on paediatric nurses visit-ing the homes of children after theirbirth in order to identify families thatneed to be offered special support (Grie-tens et al., 2004). This method comprises20 factors that will be assessed as appli-cable or non-applicable by a specialist.Some of these factors are aimed at a pos-sible social isolation of the mother (e.g.lack of support from the close partner,few and unfulfilling contacts outside fam-ily); others investigate the communica-tive capacities towards the visiting nurse(e.g. mother reveals little or very incom-plete information on her engagementwith the child). Further questions are con-cerned with the mother’s psychologicalfeatures (e.g. helplessness in stress situa-tions, recurring crises in the mother’s life).
Outlook
A number of recent meta-analyses (El-kan et al., 2000; MacLeod & Nelson,2000; Layzer et al., 2001; Geeraert et al.,2004; Sweet & Appelbaum, 2004; Bilukhaet al., 2005) have reconstructed the in-ternational research towards selective pri-mary prevention programmes againstchild abuse and neglect. They have showna fundamentally positive balance in theeffectiveness of several programmes andpresented us with useful perspectives forfurther development. The creation andapplication of meaningful screening toolshave contributed to this success. Ger-many has only just discovered the subjectof early prevention (e.g. Jordan et al.,2005), although German surveys, too,showed that a substantial number of prob-lem cases that required the taking intocare of a child could have been qualifiedas high-risk cases very early on (Kratzsch,in print). In Germany, revealing screeningmethods used regularly within the frame-work of pre-natal care, obstetrics, andpaediatrics could make a vital contribu-tion to the early identification of parents

13
From research and practice
IKK-News 1–2/2005: Violence against children
at risk of child abuse and to offeringthem early preventative services. A moresolid establishment of selective primaryprevention measures in Germany againstchild abuse and neglect would not onlycontribute to a readjustment of child andyouth welfare services desired by legisla-tors, but it would also promote improve-ment in child-raising abilities, inner-familial stimulation and the parent-child-relationship in a particularly vulnerableand burdened fraction of families (Kend-rick et al., 2000; Geeraert et al., 2004).
Contact
Dr. Heinz KindlerPsychologist
Deutsches Jugendinstitut e.V.PflegekinderhilfeNockherstraße 2 D-81541 München
Telephone: +49 (0)89 /62306-245 Email: [email protected]: www.dji.de/pkh
Susanna LilligPsychologist
IKK
Telephone: +49 (0)89 /62306-184Email: [email protected]: www.dji.de/ikk
Literature
Appleyard, K., Egeland, B., van Dulmen, M.,Sroufe, L. A. (2005): When more is not better: The role ofcumulative risk in child behaviour outcomes. In: Journal of Child Psychology and Psychiatry, 46,235–245.
Bilukha, O., Hahn, R. A., Crosby, A., Fullilove, M.T., Liberman, A., Moscicki, E., Snyder, S., Tuma, F.,Corso, P., Schofield, A., Briss, P. A., Task Force onCommunity Preventive Services (2005): The Effectiveness of Early Childhood HomeVisitation in Preventing Violence. In: American Journal of Preventive Medicine, 28,11–39.
Black, D. A., Heyman, R. E., Smith Slep, A. M.(2001): Risk factors for child physical abuse. In: Aggression and Violent Behavior, 6, 121–188.
Brown, J., Cohen, P., Johnson, J. G., Salzinger, S.(1998): A Longitudinal Analysis of Risk Factors forChild Maltreatment: Findings of a 17-YearProspective Study of Officially Recorded andSelf-Reported Child Abuse and Neglect. In: Child Abuse & Neglect, 22, 1065–1078.
Browne, K., Davies, C., Stratton, P. (1988): Early Prediction and Prevention of ChildAbuse. Chichester: Wiley.
Bussmann, K. (2003): Erste Auswirkungen des Gesetzes zur Äch-tung der Gewalt in der Erziehung. In: IKK-Nachrichten, Heft 1–2/2003, 1–4.
Daro, D., Donnelly, A. C. (2002): Charting the waves of prevention: two stepsforward, one step back. In: Child Abuse & Neglect, 26, 731–742.
Dias, M., Smith, K., deGuehery, K., Mazur, P., Li,V., Shaffer, M. L. (2005): Preventing Abusive Head Trauma amongInfants and Young Children: A Hospital-Based, Parent Education Program. In: Pediatrics, 115, 470–477.
Duggan, A., Winham, A., McFarlane, E., Fuddy,L., Rohde, C., Buchbinder, S., Sia, C. (2000): Hawaii’s Healthy Start Program of HomeVisiting for At-Risk-Families: Evaluation of Family Identification, FamilyEngagement, and Service Delivery. In: Pediatrics, 105, 250–259.
Elkan, R., Kendrick, D., Hewitt, M., Robinson, J.,Tolley, K., Blair, M., Dewey, M., Williams, D.,Brummell, K. (2000): The effectiveness of domicilliary healthvisiting: A systematic review of international studiesand a selective review of the Britishliterature. Health Technology Assessment, 4 (13).

14
From research and practice
IKK-News 1–2/2005: Violence against children
Ertem, I. O., Leventhal, J. M., Dobbs, S. (2000): Intergenerational continuity of child physicalabuse: How good is the evidence? In: The Lancet, 356, 814–819.
Geeraert, L., van den Noortgate, W., Grietens, H.,Onghena, P. (2004): The Effects of Early Prevention Programs forFamilies with Young Children at Risk for PhysicalChild Abuse and Neglect: A Meta-Analysis. In: Child Maltreatment, 9, 277–291.
Grietens, H., Geeraert, L., Hellinckx, W. (2004): A scale for home visiting nurses to identify risksof physical abuse and neglect among motherswith newborn infants. In: Child Abuse & Neglect, 28, 321–337.
Guterman, N. B. (2001): Stopping child maltreatment before it starts:Emerging horizons in early home visitationservices. Thousand Oaks: Sage.
Guterman, N. B. (1999): Enrollment Strategies in Early Home Visitation to Prevent Physical Child Abuse and Neglect andthe “Universal Versus Targeted” Debate: A Meta-Analysis of Population-Based andScreening-Based Programs. In: Child Abuse & Neglect, 23, 863–890.
Jordan, E., Schneider, K., Wagenblass S. (2005): Soziale Frühwarnsysteme in NRW – Ergebnisse und Perspektiven einesModellprojektes. Düsseldorf: Ministerium für Gesundheit, Soziales,Frauen und Familie des Landes Nordrhein-Westfalen.
Kendrick, D., Elkan, R., Hewitt, M., Dewey, M., Blair,M., Robinson, J., Williams, D., Brummell, K. (2000): Does home visiting improve parenting and thequality of the home environment? A systematic review and meta-analysis. In: Archives of Disease in Childhood, 82, 443–451.
Kindler, H. (im Druck): Wie können Misshandlungs- undVernachlässigungsrisiken eingeschätzt werden? In: Kindler, H., Lillig, S., Blüml, H., Werner, A. (Hrsg.):Handbuch Kindeswohlgefährdung nach § 1666 BGB und Allgemeiner Sozialer Dienst (ASD). München: DJI.
Kindler, H., Lillig, S., Blüml, H., Werner, A. (im Druck): Handbuch Kindeswohlgefährdung nach § 1666BGB und Allgemeiner Sozialer Dienst (ASD). München: DJI.
Korfmacher, J. (2000): The Kempe Family Stress Inventory: A Review. In: Child Abuse & Neglect, 24, 129–140.
Kratzsch, W. (im Druck): Früherkennung und Prävention bei Kindern aus psychosozialen Hochrisikofamilien: Wege und Vorgehensweise aus der Sicht einesKinderneurologischen Zentrums. In: Kinderärztliche Praxis.
Krug, E. G., Dahlberg, L. L., Mercy, J. A., Zwi, A. B.,Lozano, R. (2002): World Report on Violence and Health. Geneva: WHO.
Layzer, J. I., Goodson, B. D., Bernstein, L., Price, C.(2001): National Evaluation of Family Support Programs.Final Report Vol. A: The Meta-Analysis. Washington: DHHS.
Leventhal, J. M. (1988): Can Child Maltreatment be Predicted During thePerinatal Period: Evidence from LongitudinalCohort Studies? In: Journal of Reproductive and Infant Psychology, 6,139–161.
MacDonald, G. (2001): Effective Interventions for Child Abuse andNeglect. An Evidence-based Approach to Planning and Evaluating Interventions. Chichester: Wiley.
MacLeod, J., Nelson, G. (2000): Programs for the Promotion of Family Wellnessand the Prevention of Child Maltreatment: A Meta-Analytic Review. In: Child Abuse & Neglect, 24, 1127–1149.
McCurdy, K. (1995): Risk assessment in child abuse preventionprograms. In: Social Work Research, 19, 77–87.
Münder, J., Mutke, B., Schone, R. (2000): Kindeswohl zwischen Jugendhilfe und Justiz.Professionelles Handeln in Kindeswohlverfahren. Münster: Votum.
Munro, E. (2002): Effective child protection. Thousand Oaks: Sage.
Murphy, S., Orkow, B., Nicola, R. (1985): Prenatal Prediction of Child Abuse and Neglect:A Prospective Study. In: Child Abuse & Neglect, 9, 225–235.
Nygren, P., Nelson, H., Klein, J. (2004): Screening Children for Family Violence: A Reviewof the Evidence for the US Preventive ServicesTask Force. In: Annals of Family Medicine, 2, 161–169.
Peters, R., Barlow, J. (2003): Systematic Review of Instruments Designed toPredict Child Maltreatment During the Antenataland Postnatal Period. In: Child Abuse Review, 12, 416–439.
Sanders, M. R., Cann, W., Markie-Dadds, C. (2003): Why a Universal Population-Level Approach tothe Prevention of Child Abuse is essential. In: Child Abuse Review, 12, 145–154.
Schumacher, J. A., Smith Slep, A. M., Heyman, R. E.(2001): Risk factor for child neglect. In: Aggression and Violent Behavior, 6, 231–254.
Sidebotham, P., Golding, J., The ALSPAC StudyTeam (2001): Child Maltreatment in the “Children of thenineties”: A longitudinal study of parental riskfactors. In: Child Abuse & Neglect, 25, 1177–1200.
Sidebotham, P., Heron, J., Golding, J., The ALSPACStudy Team (2002): Child Maltreatment in the “Children of theNineties”: Deprivation, class, and socialnetworks in a UK sample. In: Child Abuse & Neglect, 26, 1243–1259.
Sweet, M. A., Appelbaum, M. I. (2004): Is Home Visiting an Effective Strategy? A Meta-Analytic Review of Home VisitingPrograms for Families with Young Children. In: Child Development, 75, 1435–1456.
Thompson, R. A. (1995): Preventing Child Maltreatment Through SocialSupport. A Critical Analysis. Thousand Oaks: Sage.
Wolfe, D. A. (1991): Preventing physical and emotional abuse ofchildren. New York: Guilford.
Wu, S. S., Ma, C.-X., Carter, R. L., Ariet, M., Feaver,E. A., Resnick, M. B., Roth, J. (2004): Risk factors for infant maltreatment. A popula-tion-based study. In: Child Abuse & Neglect, 28, 1253–1264.

15
From research and practice
IKK-News 1–2/2005: Violence against children
Time and again we encounter thephenomenon that despite the adversitiesof their environment and against all oddssome children develop astonishingly pos-itively and competently. The factors thatmake these children so “robust” and “re-sistant” and capable of mastering chal-lenging situations such as experiences ofviolence, poverty, parental unemploy-ment, or severe illness and how we canpromote their capacity for adversitymanagement are currently researched un-der the general term “resilience”.1 Theaim of resilience research is a better un-derstanding of the factors which pro-mote mental health and stability in chil-dren exposed to particular developmentalrisks. The resilience approach necessitatesa change of paradigm: away from thetraditional deficiency approaches towardsa competence- or resource-orientedapproach (see Wustmann, 2004a, 2004b,2005). With regard to prevention andintervention, this approach calls for ear-ly, long-lasting, and intensive support forall children in developing these impor-tant basic competencies beneficial incoping with adversity, but particularlyfor those children at risk. Early preven-tion approaches can indeed guard againstthe choice and solidification of unfavour-able coping mechanisms which makestress management in later developmen-tal stages more difficult. Well-developedresilience strategies, along with socialresources, contribute to an active, con-structive, and successful engagementwith the risk situation and, hence, reflecta central prevention goal of resilienceresearch. Early learning and formal edu-cation, both within and outside thefamily, can contribute significantly tothese objectives: they can focus early onthe promotion of such resilience factors,present children with effective opportu-nities to exert agency, such as how todeal with challenging situations, and im-part stability and security.
Development and features of the resilience concept
Many surveys in the early 1970s onrisks in children’s development enlight-ened researchers to the fact that there areimmense differences in how childrenreact to risk factors: on the one hand,there are those who develop behaviouraldisturbances, and on the other, thosewho “survive” and even thrive in the faceof difficult circumstances of life. Thefindings suggest that adversities and situ-ations of extreme risk need not inevi-tably lead to impaired child development,but that, indeed, some children have orcan develop an astonishing ability tobounce back in the face of negative influ-ences. Garmezy (1971) discovered in hisstudy of children with one mentally illparent (schizophrenia) that while theparent’s illness did present a risk for thechild’s development, 90 % of the childrendid not develop a mental disorder. For a long time this phenomenon of psycho-logical resilience was ignored in the re-search on child development: on one handthere was more interest in the causes ororigins of developmental disorders as wellas the individual risk factors; on the oth-er hand it appeared to be somewhat in-explicable and many scholars were hesitantto focus on the “positive” reactions (Rut-ter, 2000). These children were originallylabelled “invulnerable, invincible and in-destructible” (see e.g. Anthony, 1974;Werner & Smith, 1982) without furtherknowledge as to why and how they hadmanaged to adjust so effectively to theadverse situation. It was presumed thatthey are, indeed, so strong that they wouldunder no circumstances show psycholog-ical impairment. They were almost as-cribed mystical, super-human qualitiesreflected by book titles such as “Super-kids” (see e.g. Kauffman et al., 1979).
This concept of the so-called invulner-able children gained increasing popularityin the beginning of the 1980s. The reali-sations that some children are extraor-dinarily resilient to stressful circumstan-ces led to increased academic interest inorder to comprehend the developmentsof these children, which differed from
case to case, and particularly to investi-gate the personal qualities and social re-sources that helped them to cope so well.The consideration of such “protectivefactors” resulted in a remarkable expansionof risk research. In the course of morerecent findings the concept of the “abso-lute invulnerability” was soon refuted.Today resilience is characterised as follows:
Resilience is a dynamic process of adjustment and development
Resilience does not refer to an innatepersonality feature of a child, but de-scribes a capacity acquired during thecourse of child-environment-interaction(see e.g. Kumpfer, 1999; Luthar, Cicchet-ti & Becker, 2000; Rutter, 2000; Waller,2001). Resilience refers to a dynamic,transactional process between child andenvironment. What is significant is thebi-directional approach, in other words theinvolvement of both individual and envi-ronment in the development of resilientbehaviour. Early environmental factorshave a bearing on this process in so far aspositive, stabilising experiences early inlife fundamentally favour the develop-ment of coping mechanisms: a child whoproves equal to a challenging situationwill emerge strengthened from this expe-rience and, thus, create favourable pre-conditions to master future adversitiessuccessfully (Laucht, Schmidt & Esser,2000). Furthermore, the child participatesactively and constructively in the forma-tion of its environment. In a longitudi-nal study with the children of Kauai,Werner and Smith (2001) found that theresilient children and adolescents were ableto choose and create for themselves aprotective environment that sustained andstrengthened their capacities and skills.
Corina Wustmann
“As early as possible!” – Results of research into resilience
1 The term “resilience” stems from the Latin word “resilere” (to recoil) and generally refers to theability to cope successfully with the worst effectsof adversity (disaster, traumatic experience, failu-re, risk factors etc.) and the negative repercus-sions of stress. Thus, resilience can be understoodas children’s psychological invulnerability againstbiological, psychological and psychosocial deve-lopmental risks (Wustmann, 2004a, 2004b, 2005).

16
From research and practice
IKK-News 1–2/2005: Violence against children
Resilience is a variable qualityAccording to current research resilience
does not refer to some sort of a stableimmunity2 against negative events or men-tal disturbance, but rather to a constructthat varies with time and situations. Thecapacity to manage risk factors success-fully can change during the course of thechild’s development (Scheithauer, Nie-bank & Petermann, 2000), so that newvulnerabilities3 and resources can evolvethrough exposure to acute stress epi-sodes. In this respect, children can showstress-resilience at one stage of their lifewhile being considerably more vulnera-ble at a later period when exposed todifferent risk factors. There are stages ofheightened vulnerability during develop-ment, so-called critical periods, whenchildren are particularly delicate, for in-stance in times of social transition: thesetransitions are associated with a varietyof new tasks and, hence, make specialdemands on the adaptability of children,as in the crossing from Kindergarten to primary school. During this stage riskfactors can affect the psychosocial func-tioning of a child more than usual.Therefore resilience refers to a flexible,“elastic” defence mechanism (Bender &Lösel, 1998) attuned to the requirementsof the situation; it does not signify a“lifelong” ability according to the motto“once acquired, always there”.
Resilience is situation-specific and multidimensional
Resilience in one area of life cannotautomatically be transferred to all areasof life at large. As an example, childrensubjected to chronic parental conflict maybe resilient with regard to their perform-ance at school, but fail to be resilient insocial relationships. For this reason weno longer talk about universal, but onlysituational and domain-related resilience(Scheithauer et al., 2000). In order torender their terminology more preciselyand to avoid misapprehensions severalauthors have, thus, started to use morespecific terms such as “emotional resil-ience”, “academic/educational resilience”,“social resilience” or “behavioural resil-ience” (Luthar et al., 2000). Against thisbackdrop one of the problems of the re-silience concept becomes apparent: theenormous complexity of the researchobject involving very different methodo-logical approaches.
To summarise, resilience encompassesa highly complex conglomerate compris-ing features of the child and its environ-ment. The emergence of resilience isrooted in particular risk-alleviating, pro-tective factors both internal and externalto the child. People differ in their degreeof stress-affectedness because of theseinnate, learned, or elsewhere availableresources (Bender & Lösel, 1998). Today,resilience is looked at as a multidimen-sional, context-dependent and process-oriented phenomenon that is based upona multitude of interacting factors andcan, therefore, only be understood as amulti-causal development model.
Findings of empirical research
Despite the considerable differencesbetween the individual surveys withregard to risk factors and methodology(e.g. sample, choice of methods, exam-ined problem area and criteria for “suc-cessful” adjustment) many surprisinglyreach similar conclusions regarding factorscharacterising resilience or having a bear-ing on its emergence. Significant studiesto this end that should be highlighted arethe “Longitudinal Study of Kauai” byWerner & Smith (2001) – the pioneerstudy of resilience research conducted overa 40 year period, the “Mannheim Studyof Children at Risk” by Lauch et al.(2000), the “Bielefeld InvulnerabilityStudy” by Lösel and associates (e.g. Lösel& Bender, 1999) and the “RochesterChild Resilience Project” by Cowen et al.(1997).4 To summarise, the followingcrucial protective factors could be identi-fied in these surveys (see Wustmann,2004a, 2004b, 2005):
Personal resourcesAlready at infant age the resilient chil-
dren of the longitudinal study of Kauai(Werner & Smith, 2001) were character-ised by their primary caregivers as veryactive, affectionate, easy-to-handle andsociable.
They proved to be exceedingly adapt-able to new situations, hardly sufferedsleep dysfunction or eating difficultiesand could easily be calmed. In additionto that they had a high level of motiva-tion and were more sociable, emotionallymore balanced and more serene than
comparable non-resilient children. Thesefeatures present a direct contrast to so-called difficult temperaments (Thomas& Chess, 1980). Not only do childrenwith “difficult” temperaments have unfa-vourable developmental preconditionsdue to genetic makeup, they are also ingreater danger of being a victim of nega-tive, hostile feelings and of critical andpunishing upbringing. They can getcaught up relatively easily in a “viciouscircle” of mutually conditioning, nega-tive reactions. Children with so-calledeasy temperament (ibid.), however, elicitpositive responses with the caregiver,such as attention, affection, and socialsupport (Julius & Goetze, 2000).
The resilient children of the Kauailongitudinal study appeared in infancy tobe more self-reliant, self-confident andindependent compared to the non-resil-ient children of the same age and sex.They were more developed in both theircapacity for communication and move-ment, as well as being more integratedinto the social play of their age-group.On one hand they possessed sophisticatedself-help abilities (in conjunction with a striving for autonomy); on the otherhand they also were able to mobilise sup-port from others if this was seen as nec-essary. They were open to new experienceand curious. Closely related to this is thefact that most resilient children haddeveloped secure attachment behaviour:children with a secure attachment startexploring their environment early.According to Julius and Goetze (ibid.)“such explorative behaviour [should] in-crease the possibility of effective agency,which in turn strengthens the child’sautonomy” (p.297). Zimmerman et al.(2000) sum it up as follows: “A secureorganisation of attachment in the eyes ofdevelopmental psychopathology […] canbe seen as an important risk-alleviatingcondition, whereas insecure attachmentmust be seen as vulnerability.” Attach-ment security or insecurity do not equateto mental health or psychopathology;
2 From an anthropological point of view invulnera-bility is impossible: wounds or emotional dam-age are generally unavoidable (Grünke, 2003).
3 Vulnerability denotes the sensitivity and fragilityof a person to external (unfavourable) factors of influence. This person will exhibit an increasedsusceptibility to mental illness (Fingerle, 2000).
4 Further information on these studies can be found in Wustmann (2004a).

17
From research and practice
IKK-News 1–2/2005: Violence against children
attachment security is rather accompaniedby a better competence in coping withemotional stress, that is to say an effect-ive emotional regulation, and, hence,constitutes a good prerequisite of success-ful stress management” (p.310).5
By the age of ten the resilient childrenof the Kauai longitudinal study had bet-ter-developed problem solving skills and apositive self-concept. The resilient children’sapproach in problem solving situationswas less reactive and more proactive. Under their own initiative they assumedresponsibility in that situation and ac-tively sought a resolution: they did notwait until an outside person (an adult)removed the problem from them or ranfor support. While neither particularlytalented nor intellectually gifted, the resil-ient children made effective use of theirinnate resources and capacities. Theymanaged to concentrate well on their
homework and showed perseverance andtenacity that were above average (per-formance at school). Their good perform-ance in school in turn was a vital sourceof self-confirmation which helped com-pensate for the negative experienceswithin the context of the family (Bender& Lösel, 1998). In addition to that theresilient children possessed a strong senseof self-efficacy, a quality whose protectivecharacter lies in its motivation and theactive adversity management that it stim-ulates (Fingerly, Freytag & Julius, 1999):Those who do not expect their action tomake any difference will not bother evento try to change or risk something, butavoid the situation and assess him- orherself negatively. Those, however, whohave positive expectations regarding theirself-efficacy will apply it to new situationsand in difficulty will believe in them-selves. The sense of self-efficacy of these
resilient children encourages the develop-ment of confidence and trust in them-selves which ultimately correspondedwith greater self-confidence, positive self-assessment and more initiative.
Child-related factors• Positive temperament that arouses attention and social
support (flexible, active, frank)• First-born child• Female sex (in childhood)
Resilience factors• Sense of mastery• Sense of self-efficacy • Positive self-concept/good self-esteem• Sense of control/realistic attribution• Good social competencies: empathy/ability to make
contact and to cooperate/responsible conduct• active and flexible coping (e.g. the ability to mobilise
social support, the ability to relax)• an optimistic, confident attitude towards life
(sense of coherence)• Secure attachment behaviour• Talents, interests, hobbies
Personal resources
Within the family• at least one secure attachment figure who promotes
trust and autonomy• emotionally positive, supportive and structuring
child-rearing• cohesion, stability and constructive communication
within the family• close sibling attachment• supportive family network (relatives, friends, neighbours)
In educational institutions• Clear, transparent, consistent rules and structures• Appreciative climate (affection, respect and acceptance
towards the child)• High, but reasonable standard/positive encouragement
of the child’s willingness to make an effort• Constructive peer contacts and friendships• Promotion of fundamental competencies (resilience
factors)
In other aspects of the social environment• Competent and caring adults from outside the family,
who foster trust and a sense of belonging together andwho serve as positive role models (e.g. a grand parent, neighbours, friends, teachers)
• resources within the community (e.g. family education services, local services)
• presence of pro-social role models, norms and values inthe general society (social regard for children/upbrik-ging/family)
Social resources
5 However, despite these findings there are no surveys to date that explore the correlation bet-ween the two constructs resilience and attach-ment in a more detailed fashion.

18
From research and practice
IKK-News 1–2/2005: Violence against children
In adolescence (18 years of age) theresilient children of the Kauai study werecharacterised by a pronounced sense ofcontrol 6 and better social competencies.They acted more responsibly, more inde-pendently and in a more merit- andgoal-oriented way than their non-resilientpeers. They had better means of effectiveconflict management, had more trust intheir abilities, as well as the confidencethat things will turn out right (optimistic,confident attitude towards life). In addi-tion to that they exhibited empathy andcooperativeness towards other people.For instance, many had to assume respon-sibility for the nursing of a younger sib-ling, manage the household when theparents were ill or disabled, or take uppart-time jobs after school to contributeto the family income. The early assump-tion of responsibility for themselves andothers apparently favoured the develop-ment of an inner sense of control, self-efficacy and perseverance (Julius & Goetze,2000). These activities gave them achance to see the meaning and value oftheir own actions and the purpose oftheir existence (experience of meaningand structure in life). Antonovsky (1987)calls this cognitive, affective-motivationalfeature “sense of coherence”7: it is worthmaking an effort because of the firm con-viction that life and its tasks are assessedas meaningful.
Social resourcesDespite an enormous familial risk
burden most resilient children of theKauai study had a chance to construct aclose, positively emotional and stable rela-tionship with at least one primary caregiv-er who gave them consistent and compe-tent support and stimulation. This at-tachment figure engaged adequately andsensitively to the needs and signals of thechild. As a result of this continuous,dependable and affectionate relationshipthe majority of the children was able todevelop during infancy secure attach-ment patterns and trust. Closely asso-ciated with the bonds to the attachmentfigure are the characteristics of the rear-ing climate and the rearing style (Bender& Lösel, 1998). Most studies have shownan attachment pattern to prove mostprotective, namely one characterised byappreciation, respect and acceptancetowards the child, by secure and consist-ence rearing and by monitoring. Under
these positive conditions of parental behav-iour children can learn to deal with dif-ferent attitudes and viewpoints, to acceptboundaries, control their own behaviour,act independently, deal with success andfailure, make decisions, acknowledgetheir weaknesses and strengths, and tomobilise social support when necessary.Through the empathy of the attachmentfigure the child can experience security, a sense of belonging, tranquillity and con-fidence. Such an “authoritative rearingstyle” (Baumrind, 1989) can contribute tothe development of problem-orientedadversity management strategies, adjustedpsychosocial functioning, self-confidenceand a better sense of self-esteem.
Many resilient children of the Kauaistudy could also fall back on sources ofemotional and social support outside thefamily network. They were able to namemany teachers who gave them attention,stood up for them and who challengedthem. Not only did these supportive adultsfrom outside the family contribute to areduction of problem occurrence, theyalso served as role models for active andconstructive adversity management andpro-social behaviour.
Social relationships with attachmentfigures outside the family are of tremen-dous significance: on the one hand, theyprovide encouragement and support to-wards effective coping in an acute stresssituation, and on the other hand theyprovide alternative models of behaviourwhich are conducive to the future behav-iour of children in situations of adversity.
Perspectives of future resilienceresearch
In light of today’s research it does notsuffice merely to know the individualrisk-increasing and risk-alleviating factors;rather it is crucial to investigate the basicdynamic processes and mechanisms de-termining their effect (see e.g. Luthar &Cicchetti, 2000). We fail to understandthe phenomenon of resilience if we reduceit to a mere list of factors. With regardto this Rutter (2000) stressed, for in-stance, that the protective quality is notto be seen in the actual factor, that is inthe variable as such, but rather in theprotective “mechanism” it is based upon.Only by capturing this interaction canmore exact statements be made about the
conditions that lead either to a positiveor to a dysfunctional development.
In addition to that, risk or protectionfactors need to be seen in the light of thesocial context (see e.g. Glantz & Sloboda,1999; Waller, 2001). Depending on therisk situation often very different effectsoccur. In one case certain risk-enhancingor risk-alleviating factors can have nega-tive effects, while in another case they aremore positive. To give an example, thefactor “strict upbringing” presented aprotective shield for adolescents growingup in poverty, but not for those youthssubjected to familial risk conditions suchas parental psychopathology (Luthar &Cicchetti, 2000). Exactly what operatesas a protective factor depends on the over-all constellation of conditions surround-ing each individual. By merely looking atthe presence of a certain risk-alleviatingfactor without embedding its actualquality and effectiveness into the con-crete life situation, inaccurate prognoseswill be made resting upon a “mere bal-ance model” (which presumes resilienceto be based on the balance of risk-en-hancing and risk-alleviating factors).
Therefore, the paramount aim of fu-ture research into resilience is the devel-opment of a standardised, methodologi-cal framework that manages to reflectthe versatile, dynamic interrelations. Sofar the concept of resilience still featuresa number of methodological problemsand shortcomings, especially regardingthe absence of:• Standardised terminology,• Standardised methodology, e.g. re-
garding the understanding of resilientbehaviour or a successful, positive ad-justment and its consideration in theresearch design: some scholars defineit as the absence of psychologicaldisorders, others refer to certain com-
6 As an example they believed they could over-come their difficulties at school through theirown efforts. This belief was then linked withincreased activity, motivation and endeavour.Furthermore, the resilient children wereconvinced they could negotiate certain con-trollable problems and events; at the same timethey did not believe they could have an impacton de facto uncontrollable situations, such as an argument between their parents or thealcohol addiction of one parent (realistic senseof control).
7 According to Antonovsky a sense of coherencecomprises three dimensions: “comprehensi-bility”, “manageability” and “meaningfulness”.

19
From research and practice
IKK-News 1–2/2005: Violence against children
petencies linked with age-specific de-velopment, yet others see in it “sheersurvival” or they include all three cri-teria in their study8,
• A theory with explanatory, not merelydescriptive character.9
Conclusions
The knowledge of protective factors asidentified and (partly re-) introduced in-to the discussion by resilience research isof vital significance for the conceptionand the development of preventative andinterventional measures, as well as forprofessionals working in the educationalsector. This is for the reason that our aimis built upon “how” in our day-to-daynursing and education practice we can(further) strengthen and support children,so that they can handle stressful situa-tions and the challenges of every day life.In this connection, promotion of resil-ience primarily means to create, consoli-date and optimise those vital substruc-tures (personal and environmental resour-ces) that facilitate and motivate childrento advance by their own merit. Despitethe continuing methodological obscuri-ties and the accompanying controversiesin the discipline, the concept of resil-ience presents an enormously optimisticapproach: the focus is no longer on thedeficits and weaknesses of each child, buton its competences and coping resources.This perspective opens up the opportu-nity to overcome the long standing “re-pair-oriented” understanding of supportand to replace it by an approach thatseeks “self-correcting powers” which thenpresent the starting point for professionalagency (Freytag, 1999). It needs to beemphasised, however, that children cannotpermanently “make themselves resilient”.They require significant social help andsupport (Luthar & Cicchetti, 2000; Ga-briel, 2005). Otherwise, at that point,the resilience concept would degenerateto another “gratification approach”.
Contact
Corina WustmannPedagogue
Deutsches Jugendinstitut e.V.Nockherstraße 2 D-81541 München
Telephone: +49 (0)89 /62306-130 Email: [email protected]
8 Accordingly the findings of these surveys are heterogeneous. How “successful, positive” ad-justment is defined in the end is also subject tohistoric, cultural and evolutionary transformations.
9 A critical overview of the diverse attempts of adefinition and the methodical approaches is given by Kaplan (1999), Luthar & Cicchetti(2000) and Rutter (2000).

20
From research and practice
IKK-News 1–2/2005: Violence against children
Anthony, E. J. (1974): The syndrome of the psychologically invulnera-ble child. In: Anthony, E. J., Koupernik, C. (Eds.): The child in his family. Vol. 3. Children atpsychiatric risk. New York: Wiley, 529–545.
Antonovsky, A. (1987): Unraveling the mystery of health: How peoplemanage stress and stay well. San Francisco: Jossey-Bass.
Baumrind, D. (1989): Rearing competent children. In: Damon, W. (Ed.): Child development today andtomorrow. San Francisco: Jossey-Bass, 349–378.
Bender, D., Lösel, F. (1998): Protektive Faktoren der psychisch gesundenEntwicklung junger Menschen: Ein Beitrag zurKontroverse um saluto- und pathogenetischeAnsätze. In: Margraf, J., Siegrist, J., Neumer, S. (Hrsg.): Gesundheits- oder Krankheitstheorie? Saluto- vs.pathogenetische Ansätze im Gesundheitswesen. Berlin: Springer, 117–145.
Cowen, E. L. et al. (1997): Follow-up study of young stress-affected andstress-resilient urban children. In: Development and Psychopathology, 9,565–577.
Fingerle, M. (2000): Vulnerabilität. In: Borchert, J. (Hrsg.): Handbuch derSonderpädagogischen Psychologie. Göttingen: Hogrefe, 287–293.
Fingerle, M., Freytag, A., Julius, H. (1999): Ergebnisse der Resilienzforschung und ihreImplikationen für die (heil)pädagogischeGestaltung von schulischen Lern- undLebenswelten. In: Zeitschrift für Heilpädagogik, 50, 302–309.
Freytag, A. (1999): Kann das Resilienzparadigma integrierendeFunktion für die konzeptionelleWeiterentwicklung der Frühförderung über-nehmen? In: Opp, G., Fingerle, M., Freytag, A. (Hrsg.): Was Kinder stärkt: Erziehung zwischen Risiko undResilienz. München: Reinhardt, 166–169.
Gabriel, T. (2005): Resilienz – Kritik und Perspektiven. In: Zeitschrift für Pädagogik, 51, 207–217.
Garmezy, N. (1971): Vulnerability research and the issue of primaryprevention. In: American Journal of Orthopsychiatry, 41,101–116.
Glantz, M. D., Sloboda, Z. (1999): Analysis and reconceptualization of resilience. In: Glantz, M. D., Johnson, J. L. (Eds.): Resilience and development: Positive life adaptations. New York: Kluwer Academic/Plenum Publishers,109–126.
Grünke, M. (2003): Resilienzförderung bei Kindern und Jugendlichenin Schulen für Lernbehinderte. Lengerich: Pabst Science Publishers.
Julius, H., Goetze, H. (2000): Resilienz. In: Borchert, J. (Hrsg.): Handbuch der Sonderpädagogischen Psychologie.Göttingen: Hogrefe, 294–304.
Kauffman, C., Grunebaum, H., Cohler, B., Gamer, E.(1979): Superkids: Competent children of psychoticmothers.In: American Journal of Psychiatry, 136, 1398–1402.
Kaplan, H. B. (1999): Towards an understanding of resilience: A critical review of definitions and models. In: Glantz, M. D., Johnson, J. L. (Eds.): Resilience and development: Positive life adaptations. New York: Kluwer Academic/Plenum Publishers,17–83.
Kumpfer, K. L. (1999): Factors and processes contributing to resilience:The resilience framework. In: Glantz, M. D., Johnson, J. L. (Eds.): Resilience and development: Positive life adaptations. New York: Kluwer Academic/Plenum Publisher,179–224.
Laucht, M., Schmidt, M. H., Esser, G. (2000): Risiko- und Schutzfaktoren in der Entwicklungvon Kindern und Jugendlichen. In: Frühförderung interdisziplinär, 19, 97–108.
Lösel, F., Bender, D. (1999): Von generellen Schutzfaktoren zu differentiellenprotektiven Prozessen: Ergebnisse und Problemeder Resilienzforschung. In: Opp, G., Fingerle, M., Freytag, A. (Hrsg.): Was Kinder stärkt: Erziehung zwischen Risiko undResilienz. München: Reinhardt, 37–58.
Luthar, S. S., Cicchetti, D. (2000): The construct of resilience: Implications for inter-ventions and social policies. In: Development and Psychopathology, 12, 857–885.
Luthar, S. S., Cicchetti, D., Becker, B. (2000): The construct of resilience: A critical evaluationand guidelines for future work. In: Child Development, 71, 543–562.
Rutter, M. (2000): Resilience reconsidered: Conceptual considera-tions, empirical findings, and policy implications. In: Shonkoff, J. P., Meisels, S. J. (Eds.): Handbook of early childhood intervention. Cambridge: Cambridge University Press, 651–682.
Scheithauer, H., Niebank, K., Petermann, F. (2000): Biopsychosoziale Risiken in der Entwicklung:Das Risiko- und Schutzfaktorenkonzept ausentwicklungspsychopathologischer Sicht. In: Petermann, F., Niebank, K. Scheithauer, H. (Hrsg.): Risiken in der frühkindlichen Entwicklung:Entwicklungspsychopathologie der erstenLebensjahre. Göttingen: Hogrefe, 65–97.
Thomas, A., Chess, S. (1980): Temperament und Entwicklung. Stuttgart: Enke.
Waller, M. A. (2001): Resilience in ecosystemic context: Evolution ofthe concept. In: American Journal of Orthopsychiatry, 71,290–297.
Werner, E. E., Smith, R. S. (1982): Vulnerable but invincible: A study of resilientchildren. New York: McGraw-Hill.
Werner, E. E., Smith, R. S. (2001): Journeys from childhood to midlife: Risk, resilience, and recovery. Ithaca: Cornell University Press.
Wustmann, C. (2004a): Resilienz: Widerstandsfähigkeit von Kindern inTageseinrichtungen fördern. Weinheim: Beltz.
Wustmann, C. (2004b): Von den Stärken der Kinder ausgehen: Das Konzept der Resilienz und seineBedeutung für das pädagogische Handeln. In: Unsere Jugend, 56, 402–412.
Wustmann, C. (2005): Die Blickrichtung der neuerenResilienzforschung: Wie Kinder Lebensbelastungen bewältigen. In: Zeitschrift für Pädagogik, 51, 192–206.
Zimmermann, P., Suess, G. J., Scheuerer-Englisch,H., Grossmann, K. E. (2000): Der Einfluß der Eltern-Kind-Bindung auf dieEntwicklung psychischer Gesundheit. In: Petermann, F., Niebank, K., Scheithauer, H. (Hrsg.): Risiken in der frühkindlichen Entwicklung: Ent-wicklungspsychopathologie der ersten Lebensjahre. Göttingen: Hogrefe, 301–327.
Literature

21
From research and practice
IKK-News 1–2/2005: Violence against children
Everyone knows that prevention andearly intervention in cases of child mal-treatment can reduce parents’ and chil-dren’s suffering greatly and save moneyas well. But how should we intervene –and with whom? In this brief article, I consider these two issues from my 30years’ experience working in preventionand amelioration of mental retardation,abuse and neglect, and mental illness.
Infant attachment: Making cognitiveand affective meaning of experience
Parental behavior in cases of risk is usu-ally described in terms of what parentsdo that they shouldn’t do or fail to dothat they should do. I’m going to begindifferently – with parental intentionsand then ask how acting on those inten-tions produces unexpected and unfavor-able results.
Attachment theory is a theory aboutprotection from threat. Attachment be-havior is infants’ contribution to enablingcaregivers to protect and comfort them.Although mothers’ sensitive responsive-ness to infant signals is crucial to infants’safety and security, mothers don’t “natural-ly” know what babies want. Moreover,they have many other demands on theirattention and activity. Consequently it isup to babies to signal their needs. Patternsof attachment are infants’ strategies forshaping mothers’ behavior. When anadaptive strategy is used, mothers shouldbecome more competent and infants moresafe and comfortable. In some cases, how-ever, the threat is such that the infants’strategy can only accomplish part of this.In cases of risk, strategies can create dis-crepancies between appearance and reali-ty in which infants (or children) appearmore or less at risk than they actuallyare. These strategies are associated withrisk for physical abuse and neglect, sex-ual abuse, and psychological distress.
Attachment behavior (e.g., crying, look-ing, reaching, clinging, calling) attractsthe mother’s attention. Once she arrives,she picks up the baby and begins tryingout remedies for the problem. She ex-pects her baby to stop crying when sheprovides the needed solution.
But it’s not that simple. The way thatmothers do this has substantial impacton how their babies will learn to use theirminds. Some mothers think their babiesmust learn to wait, must learn that theyare not the only important thing in life.True enough! We all agree, but when?When should the baby learn that? Whencan babies learn that? Not in the firstmonths of life. Other mothers think theycan’t wait at all. Others vascillate betweenthese – depending upon how the motherfeels or who is guiding her at the moment(is her husband there? Her mother?)
Cognition and affect. Research has shown that for newborns
to learn contingencies, the contingenciesmust be nearly perfect. Baby cries, moth-er comes. Each time, every time- withoutintervening events. The more predictablyresponsive the mother is early on, the morequickly and firmly the infant learns therelation between his crying and mother’scoming. Predictable interpersonal con-tingencies are one way that infants – thatall people – feel connected. Babies whosemothers come quickly and predictablylearn sooner what to expect of themselvesand their mothers than babies whosemothers are less predictable.
But what should the mother do? Sure-ly we can’t expect that, without any priorexperience with this baby, she will knowalready what he or she needs. Motherseverywhere do the same thing: they pickthe baby up and put him against theirchest, on the left where their heartbeatcan be felt, and murmur soothing soundswhile stoking and rocking the babyrhythmically. This is the sensitive part ofAinsworth’s notion of “sensitive respon-siveness”; in Dan Stern’s terms, it is
“attunement.” Mothers bring their ownrhythms into accord with their babies’arousal and then help to modulate thebaby’s arousal from aroused crying tocalmly alert. When that occurs with reg-ularity, babies feel themselves in syn-chrony with another human. Shared sta-tes of arousal are the second way that ba-bies – and all humans – know that theyare together with another human.
Babies with sensitively responsivemothers learn two things. (1) Babies learnthat there are predicable contingenciesbetween events. Most important, theylearn that their behavior leads to, causes,their mothers’ response. I call this trans-formation of temporally ordered stimula-tion into implicit causal meanings “cogni-tion.” (2) When mothers attune theirresponse to the baby’s arousal and thenmodulate the arousal, babies learn thattheir feelings are understood and thatsharing feelings with another person leadsto comfort. This transformation is “affect.”Sensitively responsive mothers enabletheir babies to make cognitive and affec-tive meaning of experience.
Type B: Balance and secure. By three months of age, babies need
variability. Now they can wait. Call out,say you’re coming and the baby will wait– in eager anticipation of a certain eventoccurring at an uncertain moment. Theintense negative arousal of crying alone(a bad feeling) is transformed into ex-cited expectation (a good feeling) of soonbeing together. Cognitively and affective-ly, such favored babies make meaningout of life and relationships and, in theprocess, they learn what causes what,how to regulate their own feeling states,and how to communicate with otherhumans. Such a baby is on the way tobeing interpersonally secure and intra-psychically balanced with regard to affectand cognition.
Patricia M. Crittenden, Ph.D.
Preventive and therapeutic intervention in high-risk dyads: The contribution of attachment theory and research
Attachment and child maltreatment

22
From research and practice
IKK-News 1–2/2005: Violence against children
Type A: A preference for cognition. Some mothers are highly predictable,
but unattuned to their infants. In somecases, the mother rarely comes or comesafter such a delay that they baby hasalready given up hope. When she arrives,the infant is unable to find the contin-gency. Unsoothed crying escalates quick-ly until the baby is extremely distressed.Often mothers of these babies think,“He’s got to learn to control himself!”He does, but he can’t at this age. Or may-be their attention is preoccupied withother things and they just don’t registerthe baby’s need at all. Either way, the ba-by is left to cry until he exhausts himselfand falls asleep. What has this infantlearned? That there is predictably no re-sponse to his actions. That when he feelsdistressed, things get worse and worseand there is no relief except sleep. Othermothers respond promptly and consist-ently, but angrily. They speak sharply,touching and picking the baby up abrupt-ly or harshly. The baby feels worse, predict-ably worse. But if he cries more inten-sively- as he will – his mother gets moreupset. Their negative feelings will escalatein synchrony. A third group of motherscome promptly and predictably, but in-stead of soothing their babies, they smileand laugh – as if to deny the baby’s feel-ings. The baby cries more and the moth-er smiles harder, with sharp teeth dis-played in a face filled with fear.
All these babies learn about contin-gencies: they cause nothing, they irritateother people, they cause others to laughwhen they feel bad. They learn about af-fect as well. They learn that displayingaroused negative affect leads to more in-tense negative affect. By about threemonths of age, brain maturation enablesthem to inhibit behavior – and these ba-bies inhibit the expression of negative af-fect. Life gets better; they are less stressedand so are their caregivers.
Type C: A preference for affect. A third group of mothers responds to
their babies’ crying, but unpredictably.Sometimes they respond promptly, some-times after a delay, sometimes even beforethe baby has really signaled! Sometimesthey respond with comforting attune-ment, but often not. These babies are ona schedule of unpredictable, intermittentpositive reinforcement of negative affect.
Such a schedule maintains displays ofnegative affect for long periods of timeand at high intensity in spite of positivereinforcement of incompatible behavior,punishment, or attempts to extinguishthe behavior. These babies don’t knowhow to predictably affect the contingen-cies on their mothers’ behavior and theyfeel intensely badly about it. Cognitionfails them and affect overwhelms them.Their increasing arousal distresses theirmothers until parent and infant are joinedin their inability to regulate their feel-ings. They neither communicate recipro-cally, nor inhibit negative affect. Instead,they are filled with rapidly escalatingmixed negative feelings of anger, fear,and desire for comfort.
Child abuse and neglect. Type B babies are generally safe and
protected. So are most Type A and TypeC babies. Nevertheless, in extreme cases,Type A babies are harmed. Mothers whoseown concerns overwhelm them may notperceive their babies’ signals. Such moth-ers protect themselves and neglect basicneeds of their infants. Other mothers areover-vigilant and over-demanding, ex-pecting their babies to respond like olderchildren; they punish their children’sdemands severely, abusively. Mothers whofear distress and need everything happy,respond incongruently – and thus psycho-logically maltreat their infants. In infancy,there is little the children can do to pro-tect themselves except inhibit the nega-tive affect that leads nowhere and exhauststhem. Put another way, Type A babiesorganize around predictable contingen-cies and inhibit displays of negative af-fect that elicit undesirable outcomes romtheir mothers. Cognitive representationsorganize – or dispose – their behavior.
Mothers of Type C babies are mid-dling in sensitive responsiveness, fallingbetween the mothers of Types B and Ainfants. They are both too sensitive (alert-ing when there is no signal) and tooinsensitive (failing to alert when there isa signal) and also too responsive (over-reacting) and too unresponsive (givinglittle response). Their babies becomehighly aroused and feel bad; often this isexpressed somatically as problems witheating, sleeping, and attending. Althoughthey spend too little time in the comfortof interpersonal engagement (and sleep)
and too much time in distressed arousal,they are not usually maltreated. Theylearn to act on the basis dispositionalrepresentations (DRs) of how they feel.
A precarious transition: Me, you, and the rules
In the middle of the second year oflife, neurological maturation initiates amajor period of psychological change;toddlers use affect in a variety of commu-nicative ways that were not possible ininfancy. Concurrently physical maturationin locomotion increases toddlers’ expo-sure to danger. These changes coalesce inthe reorganization of toddlers’ strategies.
Type B: We can work it out. Once children can walk, the comfort-
ing relationships of infancy become hier-archical relationships in which parentsuse authority to restrict children and teachthem self-protective behavior. This pro-duces conflict between their desires andtheir parents’ protection. Type B toddlerstry to negotiate these differences, but withtheir limited access to language, they arevery dependent upon parents’ predictingand preventing struggles. The fewer therules, the clearer their function to protectchildren; the more predictably firm theparent is in confirming the rules, themore easily toddlers accept the rules. If,in addition, the parent prevents prob-lems (by removing forbidden objects ordistracting the child’s attention to safeactivities), the more clearly the child willunderstand the protective function of pa-rental authority. Many parents, however,can’t manage this and their children shiftfrom Type B in infancy to a more com-pelling (Type A) or persuasive (Type C)strategy in toddlerhood.
Type C: It’s about me! Some toddlers learn to manipulate
their parents’ feelings by turning protec-tive rules into personal battles. It’s aboutme! These toddlers exaggerate their dis-plays of feelings. Angry omnipotence isalternated with disarming displays oftender vulnerability. The displays shapeand mold their parents’ feelings. As a re-sult, parents are both coerced to do theirtoddler’s bidding and, mindful of theimportance of protecting their children,anxious to regain authority. To the extent

23
From research and practice
IKK-News 1–2/2005: Violence against children
that the parent forgets the protectivefunction of the rule and focuses on en-forcing authority, they enter the toddler’sdispute on the toddler’s terms. It’s aboutme! No, it is about me! The struggle be-gins and, once begun, few parents knowhow to resolve it. Their toddlers’ intensedisplays of affect leave them anxiouslyaroused and with few ways to regulateeither their own feelings or those of theirtoddlers. In moments of intense arousal,toddlers will sometimes be hurt by par-ents’ over-zealous punishment. Rates of physical punishment spike abruptly inthe middle of the second year of life – as do rates of injury from punishment(cf. Crittenden, 2004).
Other parents feel as anxiously arou-sed as their children. This leaves theirchildren feeling unsafe. When parentsbecome distressed, children fear lack ofcompetent protection. They agitate toelicit it, becoming perilously needy. Bothgroups of toddlers are now more at riskthan in infancy for maltreatment, in theforms of sudden and unpredictable attacksand negligent failure to enforce safetyprocedures. A different group of childrenis at risk for abuse. Their parents, howe-ver, being forced to be more responsive,look more normal than in infancy.
Type A: Internalizing others’ rules. Toddlers whose parents are extremely
neglectful, withdrawn, or depressed learnto combine inhibition of negative affectwith display of false positive affect thatattracts their parents’ attention in desira-ble ways. Their risk of being neglected isreduced by their role reversing, compul-sive caregiving strategy. Toddlers whoseparents are harshly punitive learn to doexactly as their parents desire, even be-fore it is requested; their compulsive com-pliance protects from the parents’ anger.Toddlers whose parents used incongru-ent positive affect learn to do the same;all appears happy while, in fact, there isno affective synchrony. For these tod-dlers, there is no chance of coercing theparent because, from the parent’s per-spective, it’s not about the child. Com-pulsive children refine the Type A strate-gy of infancy into a tool for eliciting at-tentive care from their parents, who nowappear less depressed, angry, or insensi-tively incongruent than when their tod-dlers were infants. With compulsive
strategies, Type A toddlers become less atrisk for maltreatment than in infancyand more at risk of certain kinds of psy-chological distress at later ages.
Preschool-aged children and the usesof language
In the third year of life, children be-come able to substituting language fornon-verbal affective communication.How this is managed is crucial for chil-dren’s ability to understand the sourcesof their own and other’s behavior as wellas for regulation of children’s safety.
Type B: When language communicates. Some children are given words that
accurately describe their feelings – evenwhen these are negative feelings thatexpress their frustration with their par-ents. Similarly, they are helped to tell thesimple episodes of their daily life – evenwhen these are unpleasant and builtaround uncertainty. Open and elaborat-ed verbal communication is typical ofType B children. Parents of such childrenare comfortable with mixed feelings andcomplex causation and are satisfied witha less than perfect reality.
Type A: Borrowed languge and perspectives. Type A children, especially the com-
pulsive Type A children, learn to use lan-guage to say how things should be, howmommy and daddy want life to be.When they tell episodes, their parentshelp them to see what really happened –as the parents’ desire it to be recalled.Type A preschoolers learn to tell episodesfrom the parents’ perspective; their ownperspectives fail to find expression inwords. The parents of compulsively care-giving children fear rejection by theirchildren and need soothing, reassuringstories of their children’s lives. Parents ofcompulsively compliant children fearmistakes; they need children who do theright thing. Parents of compulsively at-tentive and performing children believethat appearance is all that matters andthey strive to maintain the right appear-ance. In all cases, children inhibit expres-sion of negative affect, display positiveaffect and behavior that pleases parents,and tell the stories of their lives in bor-rowed parental language. Such childrenbecome safer, with more safely engaged
parents, but are at risk for losing accessto their own thoughts and feelings.
Type C: When words don’t work.Type C children, on the other hand,
diverge in two directions: constant chat-ter that keeps nothing discrete or clearand silence that hides what isn’t under-stood. In both cases, however, languagefails to communicate with clarity. Thechatter functions to keep parents focusedon the child while failing to clarify exact-ly why the child needs this attention orhow events are causally connected. Si-lence marks the place where neither thechild’s nor the parents’ perspective canbe tolerated. Parents of silent childrenoften have fearful secrets, either in theirown endangered past or in their mar-riage, from which they wish to protecttheir child. Unfortunately, instead ofprotecting children, all too often theyonly confuse the child about why thingshappen as they do. Ironically, too manyand too few words have similar effects:they exacerbate negative feelings and ob-scure the causal relations between parentand child. In an effort to ensure thatthey will be protected, some Type Cchildren abandon language as a strategictool and engage in provocative and risk-taking behavior
The school years: Why did I do that?
Up to about six years of age, childrenare refining their understanding of theeffects of (1) their behavior on othersand (2) their feelings on their behavior.This occurs in infancy in implicit, non-verbal ways (i. e., procedural and imagedmemory) and in toddlerhood is trans-formed into explicit, verbal information(i. e., semantic memory and connotativelanguage). Later, the experiences thatform the basis for these understandingsare encapsulated in episodes, togetherwith language that conveys the affect as-sociated with the experience (i. e., epi-sodic memory). That is, by age six, chil-dren have many ways of knowing, eachof which is a dispositional representation(DR) can influence their behavior.
To understand the relation betweenattachment and maltreatment in theschool years, one must focus on how chil-dren explain their own behavior. This is

24
From research and practice
IKK-News 1–2/2005: Violence against children
an integrative process that requires chil-dren to examine their own motivations,i. e., their DRs. When all the DRs sug-gest the same action, there is nothing toexamine. The crucial occasions are thosein which the various DRs motivate in-compatible responses. Which type of DRdoes a child rely on most often whenwhat he usually does, feels like doing,should do, and recalls doing are in con-flict? When children do what theyshould, in spite of not feeling like doingso, no one questions them – and the dis-crepancy among DRs is likely to go un-noticed by all. But when children dowhat adults think they should not do,they are asked, “Why did you do whatyou did when you knew you weren’t sup-posed to?!! Of course the answer is,“Because I felt like it and thought youwouldn’t find out.” But many parentswill punish a child who answers honestlylike that. So children learn to deceiveboth others and, more importantly, them-selves about their reasons for behaving as they did. They learn to spout parent-pleasing platitudes that, in fact, hadnothing to do with their behavior.
The irony, in both cases, is that theparents themselves rarely understand whythey are doing what they do, especiallywhen, as in cases of maltreatment, it hasbecome clear that they should not havedone it.
Prevention and intervention
If all of this is more or less accurate,what can we do to prevent or amelioraterisk to children and their parents? Fourconditions are relevant to selecting an in-tervention strategy: the development ofthe child, the child’s strategy, the parent’sstrategy, and the extent of the parents’integrative capacity.
Developmentally salient functions. The section above has addressed de-
velopment by showing that the focus ofthe parent-child relationship keepschanging and requiring new skills andattitudes from parents. Parents need tobe sensitive to infants’ competencies andresponsive to their perception of threat;they should be cognitively predictableand affectively empathic. That is, parentsfunction as attachment figures in chil-
dren’s ever-changing zone of proximaldevelopment (cf., Vygotsky). Toddlersneed protection within safe limits in ahierarchical relationship with parents thatfosters both competence and trust. Pre-school-aged children need help findingwords to express their feelings and ex-periences, especially those that are uncom-fortable or confusing. Young school-agedchildren need to explore their varied mo-tivations and the process by which onebecomes enacted behavior. Interventionshould address these developmental dif-ferences in how parent-child relation-ships function.
Child and parent self-protective strategies.Individuals’ self-protective strategies are
crucial to understand as well. The Type Acompulsive strategies are heavily skewedtoward cognitive, logical, reasoning, rule-based processes. Negative affect is mini-mized and sometimes transformed intofalse positive affect. The interventiontechniques employed should correct thisby emphasizing (1) the importance ofexperiencing feelings, especially negativefeelings, and (2) the flexibility and varia-tion that is possible even within a pre-dictable rule structure. Type C strategiesare organized around shifting, exagger-ated, and manipulative displays of nega-tive affect in a context of uncertain out-comes. Intervention should (1) reducethe emphasis on expression of feelings, (2) turn the focus towards other people’sperspectives, and (3) highlight the pre-dictable connections between events andoutcomes.
The point is quite simple: Type A andC are psychological opposites that mightrequire opposite interventions. Givingthe same intervention to a mixed groupsmight be helpful to those using onestrategy and harmful to those using itsopposite. For example, prescriptive orinformation-based approached might becounter-indicated for Type A parents asmight contingency-based behavioral tech-niques. On the other hand, Type C par-ents might experience greater negativearousal when imagery, somatic enactments,or episodic recall were emphasized – which,of course, might be very beneficial tech-niques to use with Type A parents.
Reflective integration. Imbedded in the developmental dis-
cussion above was the notion of an arrayof types of processing of informationfrom preconscious (implicit) to con-scious (explicit and verbal) to conscious-ly reflective (integrative). Parents differin the extent to which their behavior de-rives from these processes and the extentto which they can use reflective process-es. The more dependent a parent is uponimplicit processes and the less able toput motivations into words and considerdiscrepancies and conflict among moti-vations, the more intense and personallyfocused must be the intervention offeredto them. Indeed, one can suggest a gra-dient of interventions, each tied to par-ents’ ability to manage the transforma-tion of information to behavior.
Starting with the most competentparents, needing the least intervention,parent education in group settings is anappropriate preventive interventionwhen parents can use and integrate allsources of information, but lack specificinformation about young children. Giv-en the small, single-generation familiesthat exist today, parent education is rele-vant to the needs of many first-timemothers. Both the content and the groupcontext can enable mothers to enlargetheir repertoire of possible responses tothe babies while helping at-home moth-ers to feel less isolated.
Parents who are capable of integratinginformation, but who are stumped re-garding some particular problem, maybenefit from short-term counseling aroundthat problem. In this case, informationmay be offered, but more importantlythe counselor helps the parents to recon-sider the problem from new perspectivesuntil a new way forward is discovered.For counseling to be effective, however,parents must have access to both cogni-tive and affective information, be able tocommunicated effectively in words, andbe skilled and comfortable with critical,integrative reasoning processes.
When parents are relatively verbal,but not skilled with integrative processes,infant intervention may be appropriate.When this is done without the infant be-ing physically present, but with video-taped interactions of infant and parent,

25
From research and practice
IKK-News 1–2/2005: Violence against children
the parent can learn to (1) observe thebaby accurately, (2) explore their ownfeelings while watching themselves withtheir babies, and (3) reflect on what theysee and feel. Having other mothers pre-sent and engaged in the same process cangive each mother more practice, includ-ing less emotionally arousing practicethan with their own baby, as well as en-larging their repertoire of things to do(through observational learning). Havingthe babies are present will reduce the re-flective opportunity for the motherswhereas, if interactions are not video-taped, mothers skewed recall may distortthe reflective process.
When parents function primarily onthe basis of implicit information andespecially if they themselves have beenexposed to danger, either when they wereyoung or currently in their adult rela-tionships, adult psychotherapy (individual,marital, or family) for the parent mightbe needed. The focus of such psycho-therapy should be identifying the distor-tions in meaning attribution, bringing allforms of transformation to awareness(making them verbal and conscious), andlearning the process of integration of in-formation. Once that is managed (a long-term process in cases of severe distor-tions), the other forms of intervention(listed above) can be used productively.
Sensitive responsiveness. The point is that sensitive responsive-
ness in relationships is the topic of prevention and early intervention, is theprocess of intervention, and is the out-come as well. To be successful, treatmentmust function in the parents’ zone ofproximal development. When that includes learning to participate in openand reciprocal relationships in whichvulnerabilities can be expressed, ad-dressed, and protected, the interventionitself must become such a relationship.Thus, the more limited the parents’comfort in relationships (and the moreskewed their processing), the more important and extensive will be the ther-apeutic alliance required to enable change. A “one size fits all” interventionwill not only fail the most jeopardizedparent-infant relationships, it mightharm them. We need to select and focusour interventions will care, especially in cases of high risk (remembering that
some dyads that appear well functioninghave hidden problems). Good screening,thus, becomes an important part of in-tervention.
Interventions can be organized interms of sources of information (i. e.,cognitive and affective forms of procedur-al, imaged, semantic, connotative, andepisodic memory systems) and their de-gree of integration (i. e., preconscious,conscious and verbal, reflective and inte-grative. Selecting an intervention strategyrequires assessing both whether the par-ent has a Type A or C bias and also whichprocessing skills have been mastered.Offering an intervention that assumesless bias or greater skills than the indi-vidual has can do harm. For example,offering parent education to a not-yet ver-bal parent with a bias toward cognitiveprocessing can generate new rules andstandards that the child must meet. This,of course, is antithetical to sensitive re-sponsiveness. Similarly, offering a Type Cparent brief counseling around tantrum-ming may backfire if the parent’s exag-geration of feeling and minimization oftheir own contribution isn’t recognized.
Assessment. Assessment is the key to planning an
appropriate intervention. Of course, theassessment must be tied to the strategies,information processing, and integrativefunctioning offered here. A series of rele-vant assessments has been developed forthis purpose (as well as for research). TheCARE-Index is a brief screening toolsuitable from birth to about 30 months.The Strange Situation is a diagnostictool for 11-15 month old infants and tod-dlers, with the Preschool Assessment ofAttachment (PAA) extending the StrangeSituation procedure to about 5 years ofage. The School-age Assessment of At-tachment (SAA) uses verbal representa-tions in the context of content tied topreverbal behavioral DRs. The Transitionto Adulthood Attachment Interview(TAAI) and the Adult Attachment Inter-view (AAI) address the functioning ofolder individuals, including parents. Fordyads with infants and young childrenwho are at substantial risk, both adultand child should be assessed.
Treatment efficacy. The literature on treatment efficacy is
consistent in indicating that psychologi-cal treatment is effective in less than halfof cases and that the approach (psycho-dynamic, behavioral, cognitive, or familysystems) makes little difference in out-come. Cognitive therapy has producedthe most empirical data, but even so theresults suggest that high reduction insymptoms (about 70 %) immediately fol-lowing treatment yields much lowerlong-term success (approximately 35 %)at a year or more post-treatment.
Clearly far more work is needed tounderstand how best to apply the pleth-ora of available treatment approaches toparents and children. At a minimum,however, we should select interventionsthat (1) address parents’ needs and skillsand (2) carry little risk in increasing orcreating problems. That is, treatmentshould be sensitively responsive to theunique characteristics of each parent andshould be implemented in ways that re-duce the possibility of aggravating thesituation.
In addition, we should not fool our-selves into thinking that early interven-tion can inoculate families against futureproblems. Instead, we should promoteservices that (1) increase parents’ aware-ness of how they generate informationand select behavior and (2) foster reflect-ive, integrative processing. If that is ac-complished early on, simple periodicscreening can identify any on-going needfor anticipatory guidance, parent educa-tion tied to older children’s needs, orcounseling around specific problems.
The hypothesis offered here is that ifthe parents’ (a) use of biased and limitedsources of information and (b) failure toengage in reflective, integration is notaddressed early on, the family can be ex-pected to respond to each new develop-mental challenge in skewed ways thatrisk escalation of problems. In this case,the family and the treatment services arelikely to remain in frequent contactaround solving ever-changing crises.
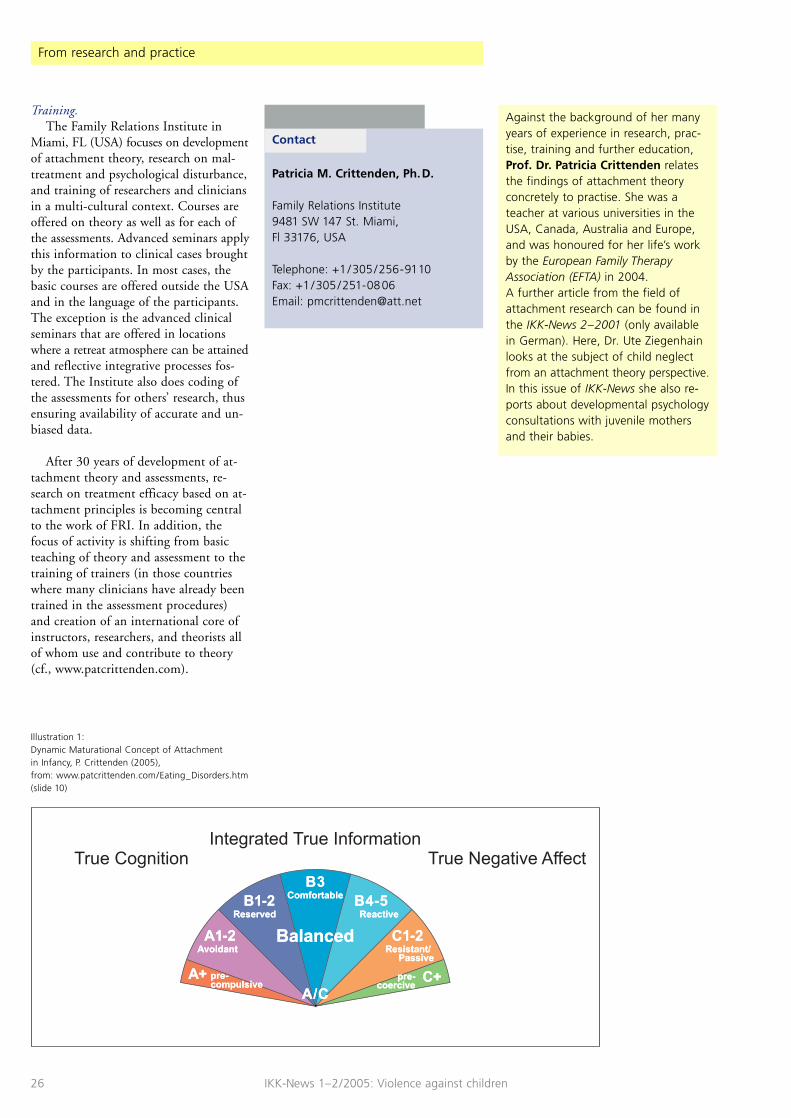
26
From research and practice
IKK-News 1–2/2005: Violence against children
Training. The Family Relations Institute in
Miami, FL (USA) focuses on developmentof attachment theory, research on mal-treatment and psychological disturbance,and training of researchers and cliniciansin a multi-cultural context. Courses areoffered on theory as well as for each ofthe assessments. Advanced seminars applythis information to clinical cases broughtby the participants. In most cases, thebasic courses are offered outside the USAand in the language of the participants.The exception is the advanced clinicalseminars that are offered in locationswhere a retreat atmosphere can be attainedand reflective integrative processes fos-tered. The Institute also does coding ofthe assessments for others’ research, thusensuring availability of accurate and un-biased data.
After 30 years of development of at-tachment theory and assessments, re-search on treatment efficacy based on at-tachment principles is becoming centralto the work of FRI. In addition, thefocus of activity is shifting from basicteaching of theory and assessment to thetraining of trainers (in those countrieswhere many clinicians have already beentrained in the assessment procedures)and creation of an international core ofinstructors, researchers, and theorists allof whom use and contribute to theory(cf., www.patcrittenden.com).
Against the background of her manyyears of experience in research, prac-tise, training and further education,Prof. Dr. Patricia Crittenden relatesthe findings of attachment theoryconcretely to practise. She was ateacher at various universities in theUSA, Canada, Australia and Europe,and was honoured for her life’s workby the European Family TherapyAssociation (EFTA) in 2004.A further article from the field ofattachment research can be found inthe IKK-News 2–2001 (only availablein German). Here, Dr. Ute Ziegenhainlooks at the subject of child neglectfrom an attachment theory perspective.In this issue of IKK-News she also re-ports about developmental psychologyconsultations with juvenile mothersand their babies.
Illustration 1:Dynamic Maturational Concept of Attachment in Infancy, P. Crittenden (2005),from: www.patcrittenden.com/Eating_Disorders.htm(slide 10)
Contact
Patricia M. Crittenden, Ph.D.
Family Relations Institute 9481 SW 147 St. Miami, Fl 33176, USA
Telephone: +1 /305 /256-9110 Fax: +1 /305 /251-0806 Email: [email protected]

27
From research and practice
IKK-News 1–2/2005: Violence against children
Literature
Ainsworth, M. D. S. (1979): Infant-mother attachment. In: American Psychologist, 34, 932–937.
Ainsworth, M. D. S., Blehar, M. C., Waters, E.,Wall, S. (1978): Patterns of Attachment: A psychological studyof the strange situation. Hillsdale, NJ: Erlbaum Associates.
Bowlby, J. (1980): Attachment and loss. Vol. III: Loss. New York: Basic Books.
Crittenden, P. M. (in press): Why do inadequate parents do what they do? In: Mayseless, O. (Ed.): Parenting representations: Theory, research, and cli-nical implications. Cambridge: Cambridge U. Press.
Crittenden, P. M. (2004): The origins of physical punishment: An ethological/attachment perspective on theuse of punishment by human parents. In: Donnelly, M., Strauss, M. A. (Eds.): Corporal Punishment of Children in TheoreticalPerspective. New Haven: Yale University Press.
Crittenden, P. M. (1999): Danger and development: The organization ofself-protective strategies. In: Vondra, J. I., Barnett, D. (Eds.): Atypical attachment in infancy and early childhoodamong children at developmental risk. Monographsof the Society for Research on Child Development,145–171.
Crittenden, P. M. (1995): Attachment and psychopathology. In: Goldberg, S., Muir, R., Kerr, J. (Eds.): John Bowlby’s attachment theory: Historical, clini-cal, and social significance. New York: The Analytic Press, 367–406.
Crittenden, P. M. (1992): Quality of attachment in the preschool years. In: Development and Psychopathology, 4, 209–241.
Damasio, A. R. (1994): Descartes’ error: emotion, reason, and thehuman brain. New York: Avon Books.
Fonagy, P., Target, M. (1997): Attachment and reflective function: Their rolein self-organization. In: Development and Psychopathology, 9, 679–700.
Gergely, G. (2001): The obscure object of desire: ,Nearly, but clear-ly not like me’: Contingency preference in nor-mal children versus children with autism. In: Bulletin of the Menninger Clinic, 65, 411–426.
Schacter, D. L., Tulving, E. (1994): What are the memory systems of 1994? In: Schacter, D. L., Tulving, E. (Eds.): Memory systems 1994. Cambridge, MA: Bradford, 1–38.
Stern, D. (1985): The interpersonal world of the infant. New York: Basic Books.
Vygotsky, L. S. (1987): The collected works of L. S. Vygotsky. R. W. Rieber, A. S. Carlton (Eds.), translated by N.Minick. New York: Plenum Press.
Young, J. E. (1999): Cognitive therapy for Personality Disorders: A schema-focused approach. Sarasota, FL: Professional Resource Exchange Inc.

28
From research and practice
IKK-News 1–2/2005: Violence against children
When talking about childhood, as astart we think of growing up in a certainera and under certain social circumstan-ces. We could pursue the question howchildhood today differs from childhoodin the past, for instance how many chil-dren experience parental separation anddivorce, and how many live in poverty.We would encounter statements aboutthe “individualisation of lives” and “plural-isation of lifestyles” (Federal Ministry of Family Affairs, Senior Citizens, Wom-en and Youth, 2001) and find out alongwith other experts that “growing up inour society has become riskier and moredangerous for children and adolescentsand that the task of upbringing for par-ents, too, has become more difficult”(Scheuerer-Englisch, 2005). It is there-fore self-evident that I limit my paper tochildren at risk. However, I am not go-ing to focus on the description of variousrisks, but rather on how different chil-dren manage them. By focusing oncourses of development we also avoid asplit between intrinsic and extrinsicworlds and look at the way they interactand which powers these transactions or-chestrate (Staudinger, 1999). Childreneither will tap new resources and avoid/successfully fend off dangers, or they willnot. But why? Why do some childrensuccessfully come through the very samecritical circumstances that others struggleso hard with? If we find answers to thisquestion, not only our understanding of general developmental processes andmechanisms broadens – the above men-tioned orchestrating powers – but, by the same token, it helps us to designeffective strategies with which we canmost optimally promote the course ofdevelopment of children at risk.
For a long time our knowledge aboutdevelopmental courses was limited to thefindings of retrospective surveys: whendisturbances occurred, explanations weresought by a review of the developmentand its formative characteristics to date.Such proceedings make developmentalrisks and deficits the focal point of atten-tion. Furthermore, with a retrospective
approach there is absolutely no opportu-nity to even come across developmentalrisks and dangers that were dealt with suc-cessfully or to probe the reasons behindthese. Therefore, in the 1970s longitu-dinal studies with high-risk samples werestarted, some of which continue up tothe present, providing information onwhy developmental courses can lead toan overall positive outcome despite adistinctively unfavourable environment.Among experts this phenomenon isreferred to as resilience (Masten, 2001).The findings allow the derivation ofseveral resilience-promoting strategieswhich will be represented with a focus onthe STEEP™ programme in what fol-lows. It needs to be said in advance thatSTEEP™ was conceived as a rigorouslypractical implementation of the results ofthe Minnesota-Parent-Child-Project(MPCP) – a research project aiming toinvestigate the origins of abuse and mal-treatment and therefore primarily a pro-gramme for the prevention of abuse andmaltreatment.
1. Resilience promoting strategies
Ann Masten (2001) summarises thevarious – empirically derived – ways ofpromoting resilience as: (1) risk-related,(2) resources-oriented, and finally (3)process-oriented strategies.
The first strategy encompasses allefforts to identify and to eliminate, or atleast minimise, the risks of child develop-ment. The protection and safeguardingof children from known dangers is soself-evident that perhaps the boundariesof such an approach are not sufficientlytaken into consideration. For a start,every society is overtaxed by the task of shielding its children from all knowndangers, because life is full with risks.Furthermore, risks affect different chil-dren differently, and not all risks areeasily recognisable. For a well-trainedcanoer, for instance, a challenging white-water rafting tour presents a calculablerisk, moreover, one that diminishes with
further training. This considered, itseems sensible not to keep children awayfrom all risks (e.g. marital arguments,traffic), but to help them cope with theserisks. Thereby they get practice in han-dling them, and similar circumstanceswill affect these children less and less, ifat all. However, we need to make a pointof highlighting the fact that there areadversities with which no child can copeand from which it needs to be protectedby all means (e.g. loyalty conflicts inparental quarrels, dangerous roads, notto mention abuse). With this in mind,however, our approach favours the supportof children in coping with risk and ad-versity, and disfavours their growing upunder the famous glass dome. We arecalling for a change of emphasis and re-orientation toward support and strength-ening of children for a successful man-agement of life’s risks.
The resource-oriented strategies of thesecond group summarise all the effortsthat strengthen both parents and childrenand contribute to their relaxation andrecreation, e.g. cafés, cinemas and clubsetc. for parents. These widely recognisedpositive strategies, however, need to be on constant offer, because their effectwill fizzle out just like the effect of arestorative weekend will.
This is a distinct difference from theprocess-oriented strategies of resiliencepromotion. As it were, the latter sows a seed corn in the soil of developmentalcourses which unfolds its effects longafter the end of the actual intervention.Such seed corns in the human develop-ment are represented by the followingprotective systems: regulation system,attachment system, coping-motivationsystem, as well as municipal, religious orspiritual defence systems, sensibly sup-
Prof. Dr. Gerhard J. Suess
STEEP™1
Early intervention to promote resilience in at-risk childhoods2
1 Steps Toward Effective and Enjoyable Parenting was developed by B. Egeland and M.F. Ericksonat the University of Minnesota.
2 Revised version of the paper “Nicht die Kindersind anders, sondern die Kindheiten” given at the symposium of the Bavarian branch of theGerman Society for the Prevention of Crueltytowards Children on 15 April 2005 in Würzburg.

29
From research and practice
IKK-News 1–2/2005: Violence against children
plementing the individual systemsthrough lived values and solidarity. Here,we are only going to elaborate the firstthree systems and of these particularlythe attachment system, because it is themost powerful defence system we know.
If a child learns to regulate its innerexcitement, emotions and behaviour inaccordance with the particular require-ments, it will benefit from that in the fu-ture when other adverse situations occur.The child’s overall development will bepositively affected by that. This is why itis so vital to support parents in timeswhen they have difficulties with the theirbabies not sleeping right through thenight, their crying or their feeding (Pa-pousek, 2004), because not only doesthis assistance foster the bonding be-tween mother and child, but it also helpsthe development of sufficient regulatorycapacities to the point of preventingattention deficit syndrome (ADS) or at-tention deficit hyperactivity disorder(ADHD). However, the blessing of self-regulatory properties is evident through-out the entire life. Individuals who canmanage the necessary level of ego-controlin order to accommodate every newchallenging situation usually also have anadvantage when it comes to optimisingdevelopmental opportunities.3
Very early in the first year of life infantshave several ways of experiencing their self-efficacy. Parents who respect their child’sautonomous personality with its own de-sires and needs will not carelessly disruptthe infant’s activities, but support theattainment of its own goals. They willonly intervene when the child by its ownefforts makes no progress, and they willdo so very subtly so that the child believesitself to be the originator of the accom-plished action. After countless experiencesof self-efficacy such children by the ageof two will exhibit more perseveranceand higher motivation when coping withtasks (Sroufe et al., 2005). These charac-teristics will continue to help the childsummon the right amount of energy andnecessary edge in order to master largertasks successfully. If need be, they will beable to give their very best, because theywill have learned to assess realisticallytheir abilities to deal with problems.That does not mean that a football teamso equipped will invariably turn a 0:2 into
a 3:2 and eventually win the match. Butwithout such coping-motivation capaci-ties such results would be even less likely.
The protective systems described upto this point overlap (while not beingcompletely congruent) with the last oneto be elaborated here: the attachmentsystem. Children with a secure attachmentrelationship with their parents usuallyhave good self-regulatory properties andgood coping-motivation competence.Basically, secure attachment means thatwithin a relationship that is experiencedas comforting, the children concerneddevelop inner working models whichrepresent the self as worthy of love, thecaregivers as psychologically availableand relationships in general as reliable andpositive – especially in times of personalinsecurity. As these children develop, thereliability they experienced in their firstrelationship will make them approachadults as a secure basis for their explora-tion of the environment as well as a havenof safety. These are the two sides to theparent-child-attachment. The aspect ofthe secure base supports children in theirprimary need to explore the environmentwhile the caregiver provides the requiredsafety and protectively watches over thechild’s activities, especially at a time whentheir own judgement of risks is still alittle undependable. Particularly at the ageof two, children expect their parents tocome to their aid from time to timewhen their own capacities are not enough,just as they want their parent to sharetheir happiness over achievements. Thatway they can test and extend their abili-ties – while risks are cushioned by a safetynet. If, indeed, unpredicted adversities orinner insecurities occur, children withsecure attachment relationships feel thatthey are welcome when they make bidsfor comfort and affection directed to therespective caregiver and that these bidsare reciprocated to the degree needed.Sometimes children just want to cuddleup to their parents and enjoy the feelingof being their source of happiness4 –that, too, is something children experi-ence when they have developed a secureattachment relationship with their parents.
The working models of the self whichare developed through such attachmentrelationships and relationships generallyare carried further into other social contextsand also apply to relationship networks
outside the family. They can be seen asshields safeguarding against life risks.Just like a fertile seed the attachmentsystem fosters the further course of devel-opment – even if only when its quality is good. Although attachment is a lifelongsubject, from the cradle to the grave, it is a particularly important function ofdevelopment in and around the first yearof life. While it stays somewhat in thebackground behind other tasks until kin-dergarten-age, it keeps its central meaninguntil puberty, even if so with lesseningsignificance. In adult age the meaning ofthe attachment system steps back strong-ly; however, it becomes more significantduring pregnancy and during criticalincidents in life. At an age when personalpowers increasingly wane, the attach-ment system gains in importance againand the closeness of confidants is sought.
However, the vital meaning of the at-tachment system in human developmentcannot only be described positively: if theexperiences made within it are negative,this central meaning will lead to equallysevere deformations and disorders andthe suffering associated with them. Thisis particularly the case with the so-calleddisorganised or disoriented attachmentproperties. Therefore it should be a prima-ry aim of early prevention to avoid theseforms of attachments and to promotesecure attachment qualities.
2. STEEP™ – a programme for the promotion of resilience based upon attachment theory
The course of attachment develop-ment and the mechanisms controlling itwere prospectively studied over a timeperiod of 30 years. The findings are com-plemented by retrospective studies thatdocumented the handing-down of attach-ment patterns across generations (Gross-mann & Grossmann, 2004; Sroufe et al.,2005). Attachment research among high-risk populations, as conducted very suc-cessfully by the University of Minnesotain the past 30 years involving 260 mother-
3 Block & Block (1980) were among the first to study the role of “ego-control” and “ego-resilience”for a successful organisation of behaviour. They have described them as the two fundamen-tal personality factors (Block, 1995).
4 These two sides of the parent-child-attachmentare very vividly illustrated by Marvin et al. (2003).

30
From research and practice
IKK-News 1–2/2005: Violence against children
child-couples living in poverty is especial-ly informative for all efforts to promoteresilience and to stop unfavourable cross-generational processes of handing down(for summary see Kißgen & Suess, 2005).
Based upon these findings about suc-cessful development despite the presenceof risk factors, Byron Egeland and Mar-tha F. Erickson from the University ofMinnesota developed the early inter-vention programme STEEP™ in 1987.It was then also introduced into practiseand tested for effectiveness with 154mothers (Erickson, 2002; Egeland, 2002;Suess & Hantel-Quitmann, 2004; Suess& Kißgen, 2005; Kißgen & Suess, inprint). Hence, STEEP™ represents a tech-nology particularly relevant for the day-to-day of social work; one for which notonly tremendous developmental costswere needed, but also one that imple-ments effectively and in a targeted waythe cumulative findings of attachmentresearch. Evidence of its effectiveness wasproven not only upon completion, butalso – in a longitudinal fashion – afteranother year had passed. This is an im-measurable asset not only in respect ofcost. The empirical findings, of course,did not always meet the expectations andled to modifications of the originalSTEEP™-model. One key modificationconcerned the duration: from the orig-inal duration of one year the STEEP™-programme was extended to two years andin the case of substance abuse even tothree years. STEEP™, in this sense, is adecidedly evidence-based interventionprogramme with profound empiricalbasis. Since its first implementation andevaluation the modified STEEP™-pro-gramme was used by selected institutions,partly in sponsorship of the University of Minnesota (Baby’s Space/Minneapolis).They all met the programme require-ments (St. David’s Child Developmentand Family Center/Minneapolis), hence,STEEP™ came under practical scrutinyafter the initial empirical evaluation.This also led to some alterations of theoriginal programme.
Now, the modified STEEP™-modelis to be tested for effectiveness in a furtherevaluation programme to be conductedin three metropolitan areas: Minneapolis,Hamburg and Berlin/Potsdam.5 It is tobe expected that this further test of effect-iveness will not only make for furtherrefinement, but will also provide summa-
rised and communicable experiencesabout the implementation requirementsin German-speaking regions.
Ideally, STEEP™ starts during preg-nancy and encourages realistic expecta-tions regarding the time ahead with thechild. What characterises the overallframe work are home visits with the par-ticipating mothers, group sessions with10-15 mothers each, as well as the use ofvideo taping to improve the relationshipwith the child. While the home visitsmainly focus on the nature of the moth-er’s engagement with her child, thegroup sessions provide the opportunityfor parents to develop skills necessary to create an indispensable social supportnetwork. In addition, they can benefitfrom the other parents’ positive transfor-mation processes. All aspects of STEEP™
are pervaded with an inner attitude basedupon principles of attachment theorywhich in addition to the relevant knowl-edge also comprises a decidedly respectfulengagement with the parents. The trans-formation process aimed at affects everyaspect of the parents’ lives and doubtless-ly involves a certain degree of emotionaldisturbance and anxiety. Here the facili-tator is to serve as a secure base andought to offer safety and secure footing.
For two reasons, then, STEEP™ can-not be learned through reading alone,but requires actual training by others6
that encompasses the eyes (observationtraining), as well as the brain (attachment-theoretical knowledge), as well as theheart (to reflect on their own relationshiphistory and how it influences their atti-tudes and parenting behaviour). Firstly,the cooperative and respectful engagementof facilitators with affected parents is an important objective which may also
necessitate changes in the advisors. Thiswill be done by self-observation and aprocess of intensive supervision. Secondly,the identification of successful mother-infant-interactions requires special train-ing in observation. If video taping is tobe used for the improvement of parent-infant-interactions, facilitators need anobjectifiable standard of what is aimed atin order to prevent both an endanger-ment of the child’s wellbeing and a de-mand for perfectionism. From an attach-ment-theoretical perspective parentsneed to be prepared for the deficienciesobtaining in all relationships and for theparticular dangers of perfectionism.Parents can be seen as well-prepared torear their children if they have the abilityto reflect critically on their relevantattachment relationships, including therepercussions on their children, and ifthey are capable of acknowledging sen-sitively the shortcomings of the relation-ship with their child and are able toapologise for them.
Attachment researchers are convincedof the bearing unconscious processeshave on child rearing and also of the ne-cessity of individualised programmes inorder to promote successful parent-infant-relationships. After all, it is not abstractexperts’ reports – programmes explainingvarious styles of child rearing – or ap-pealingly written parenting guide booksthat show the way to successful parent-hood, but only attention to the childand the signs it leaves to decipher. Theyrepresent a starting point of a parent-child journey to new horizons of experi-ence that is going to have a lasting effecton both and that will be a fertile seed forsocial systems. It is a central aspect ofSTEEP™ that parents are accompaniedon that journey during the first twoyears of their child’s life. Parents are sup-ported in “studying” the signals of theirinfants and to learn to see the world withtheir eyes. For this purpose psychothera-peutic measures are implemented aimingat the improvement of parent-child-interaction (Seeing is Believing) and at thereflection upon the parents’ childhoodexperiences (Looking back, Moving for-ward). In addition to that, knowledgebased upon developmental psychology is conveyed and the experience of a suc-cessful therapeutic relationship itself hashealing effects. Attachment models de-velop and preferably change in primary
der Hochschule für Angewandte WissenschaftenHamburg und der Fachhochschule Potsdam, gefördert durch das Bundesministerium für Bildung und Forschung

31
From research and practice
IKK-News 1–2/2005: Violence against children
attachment and in future meaningfulrelationships. From an attachment-theoryviewpoint, therefore, relationship-orient-ed intervention is required. In STEEP™,advisors employ as an instrument theirown relationship with the parents. Theyendeavour not only to be a secure base to the parents, but also to serve as a modelfor how to deal with personal shortcom-ings in an attachment-securing way. By that, parents are prepared for set backsand learn to deal with mistakes in a con-structive fashion. It is the particularintention of this advisory relationship toupset the parents’ expectations stemmingfrom insecure attachment models, so theycan learn to change them. The basis forthis is provided by the knowledge aboutthe mechanisms and the development-controlling functions these attachmentmodels are based upon. However, facilita-tors, too, need to look into their ownattachment models and histories.
Contact
Prof. Dr. Gerhard J. SuessHamburg University of Applied ScienceFaculty of Social Work and NursingSaarlandstraße 30D-22303 Hamburg
Telephone: +49 (0)179 /5838074Email: [email protected]
Literature
Block, J. H., Block, J. (1980): The role of ego-control and ego-resiliency inthe organization of behavior. In: Collins, W. A. (Ed.): The Minnesota Symposia onChild Psychology (13th). Hillsdale, N.J.: Lawrence Erlbaum Associates(Wiley), 39–101.
Block, J. (1995): A contrarian view of the five-factor approachto personality description. In: Psychological Bulletin, 117, 187–215.
Bundesministerium für Familie, Senioren, Frauenund Jugend (2001): Bericht über die Lebenssituation jungerMenschen und die Leistungen der Kinder- undJugendhilfe in Deutschland – Elfter Kinder- und Jugendbericht. Berlin: MuK.
Egeland, B. (2002): Ergebnisse einer Langzeitstudie an Hoch-Risiko-Familien – Implikationen für Präventionund Intervention. In: Brisch, K. H., Grossmann, K. E., Grossmann, K.,Köhler, L. (Hrsg.): Bindung und seelische Entwicklungswege. Stuttgart: Klett-Cotta.
Erickson, M. F. (2002): Bindungstheorie bei präventivenInterventionen. In: Brisch, K. H., Grossmann, K. E., Grossmann, K.,Köhler, L. (Hrsg.): Bindung und seelische Entwicklungswege. Stuttgart: Klett-Cotta.
Grossmann, K., Grossmann, K. E. (2004): Bindungen – das Gefüge psychischerSicherheit. Stuttgart: Klett-Cotta.
Kißgen, R., Suess, G. J. (2005): Bindung in Hoch-Risiko-Familien: Ergebnisseaus dem Minnesota Parent Child Projekt. Heft 1/Januar.
Kißgen, R., Suess, G. J. (im Druck): Bindungstheoretisch fundierte Intervention inHoch-Risiko-Familien am Beispiel des STEEP™-Programms. In: Frühförderung interdisziplinär, 24, 124–133.
Marvin, R. S., Cooper, G., Hoffmann, K., Powell, B.(2003): Das Projekt “Kreislauf der Sicherheit”:Bindungsgeleitete Intervention bei Eltern-Kind-Dyaden im Vorschulalter. In: Scheuerer-Englisch, H., Suess, G. J., Pfeifer, K.-W. P. (Hrsg.): Wege zur Sicherheit: Bindungswissen in Diagnostikund Intervention. Gießen: Psychosozial-Verlag, 25–50.
Masten, A. (2001): Resilienz in der Entwicklung: Wunder desAlltags. In: Röper, G., Hagen, C. v., Noam, G. G. (Hrsg.): Entwicklung und Risiko: Perspektiven einer klini-schen Entwicklungspsychologie. Stuttgart: Kohlhammer.
Papousek, M., Schieche, M., Wurmser, H. (2004): Regulationsstörungen der frühen Kindheit. Bern: Huber.
Scheuerer-Englisch, H. (2005): Brücken für Familien: Zur Verortung derErziehungsberatung in einer komplexen Welt. In: Informationen für Erziehungsberatungsstellen1/05, 12–19.
Sroufe, L. A., Egeland, B., Carlson, E., Collins, W. A. (2005): The Development of the Person: TheMinnesota Study of Risk and Adaptation fromBirth to Adulthood. New York: Guilford Publications.
Staudinger, U. M. (1999): Perspektiven der Resilienzforschung aus Sichtder Lebensspannen-Psychologie. In: Opp, G., Fingerle, M., Freytag, A. (Hrsg.): Was Kinder stärkt. München: Reinhardt.
Suess, G. J., Hantel-Quitmann, W. (2004): Bindungsbeziehungen in der Frühintervention. In: Ahnert, L. (Hrsg.): Frühe Bindung. Entstehung und Entwicklung. München: Reinhardt.
Suess, G. J., Kißgen, R. (2005): Frühe Hilfen zur Förderung der Resilienz aufdem Hintergrund der Bindungstheorie: Das STEEP™-Modell. In: Cierpka, M. (Hrsg.): Möglichkeiten der Gewaltprävention. Göttingen: Vandenhoeck & Ruprecht.
5 The German parts of the programme are financed by the Federal Ministry of Educationand Research and conducted by the HamburgUniversity of Applied Science (project manage-ment: Prof. Dr. Hantel-Quitmann & Prof. Dr. Suess;project coordination: Dipl.-Psych. Uta Bohlen) as well as the Potsdam University of AppliedScience (project management: Prof. Dr. LudwigKörner; project coordination: Dipl.-Psych. GabiKoch). The American part of the project is con-ducted by St. David’s (project management: Dr. Sue Fust) and financed by several sources.
6 www.steep-training.de; ZEPRA, telephone contact 040 /42875-7037,[email protected]

32
From research and practice
IKK-News 1–2/2005: Violence against children
The early counselling centre wasfounded as a district project in 1999 atthe Amt für Soziale Dienste Bremen(Department for Social Services) in orderto reach psychosocially burdened familieswith babies and infants as early as pos-sible. Its aims are the stabilisation of theparent-infant-relationship and the preven-tion of child abuse and neglect. Becauseof the increasing demand from parentsthus far, the early counselling centre’swork could be continued over a projectperiod of five years. This is partly thanksto a mother’s action group established in 2003 supported by citizens, paedia-tricians and social institutions. Becauseof the commitment of this group the earlycounselling centre’s future has beenensured by the authorities. Their work is currently evaluated by Prof. Dr. Frieseand her associates of the University of Bremen.
Through the interaction of parentingeducation, early childhood interventionand early advice, on-site prevention andintervention could be developed, withthe particular aim of reaching earlier par-ents who normally have little access tothese services. However, factors bearingupon the success of our work are thedegree and duration of the psychosocialstress and the emotional disturbance orthe illness of a parent. For the promotionof the psychological health of both chil-dren and their parents within the youthwelfare services social-therapeutic offersshould be available in order to enableyoung parents with extremely insecureattachment patterns and attachmentanxieties to have corrective experiences. Parents traumatised by violence andneglect do not normally consult a regis-tered therapist. They need a confidantand a secure attachment figure not onlyfor the current relationship with theirinfant, but also as a guidepost or a “bridge”– for instance to a therapy.
How do we work?
The counselling centre works in closecooperation with the adjacent Haus derFamilie (Family House) whose mother-child-sessions, family holiday courses,parenting education events, and playcircles are inviting and attractive to thefamilies. The interdisciplinary cooperationbetween teachers, the paediatrician, andthe psychologist has a particularly posi-tive effect when dealing with multi-prob-lem-families. We try to respond in ajoint effort to problems of parents withbabies and infants as early and unbureau-cratically as possible, and to strengthenprevention and child protection in asocio-economic trouble-spot. Many par-ents are aware of the fact that the Hausder Familie is a place where they can findsomething good for themselves and theirchildren and where they can expect sup-port with their family problems. Theearly counselling centre with its offer topromote the relationship between childand parents is a part of that. It integratesvarious concepts of counselling and ther-apy: advice based upon developmentalpsychology involving interactional diag-nosis, behavioural observations, guidancefor play, baby massage, family consul-tations, psychoanalytical therapy forcouples and families, body psychotherapy,and sand exercises. The parents’ percep-tible fears about involving themselveswith the centre can often be reduced bya supportive relationship, a multitude ofcontact opportunities for parents, as wellas the on-site support services for children.This involves not only the easy availa-bility of advisors and therapists as contacts,but also their transparent behaviour, thecommunication of their motivations andobjectives, as well as their easy engage-ment with the parents. This fosters thedevelopment of a trusting rapport withthe parents.
The central purpose in our work withpsychosocially stressed parents is thestimulation of communication betweenthem and their babies or infants and thesensitisation of the parents to the infant’ssignals. The awareness of successful inter-actions alerts the parents to the possibil-ity of a positive development of theirchild within their relationship. Video-assisted interaction-counselling, in partic-ular, gives the parents an impression ofhow crucial commitment and communi-cation are for development. For develop-mental advice purposes, these interac-tions illustrate for the parent the needs,signals and developmental tasks of thechild. Whether psychosocially burdenedparents engage in casual interactionduring nappy-changing, feeding, littlegames, and dialogues depends upon theadvisor’s communicative ability tostrengthen parents’ self-esteem and to showa positive response when parents decideto seek support. When a mother or par-ents feel accepted, they are more likely toovercome their inhibitions, their silence,and their barriers towards the child. Thejoint reflection of successful interactionsand individual developmental progressstrengthens the parents’ self-confidenceand interest in their children. A baby, for instance, that experiences its motheras more open, calm, and affectionate indialogue will, in turn, feel relaxed andmore interested in its environment. If amother during counselling experiencesher infant looking at her, smiling at her,and listening to her, this gives her a feel-ing of how important and meaningfulshe is to her baby. If she seeks and keepseye-contact and talks with her baby, a dia-logue can evolve. Thus, a mutual “lead-ing” and “going-along” can develop, withever richer interactions, if mother andchild as partners of the dyad impersonateone another and try to concentrate andhold the partner to themselves (Brazelton,994, p.151ff.). This “going-along” in acoordinated, playful rhythm has an en-couraging effect on both mother and baby,and is a vital contribution to the develop-ment of attachment (Brazelton, loc. cit.).
Inge Beyersmann
A chance for psychosocially burdened mothers with babies and infantsA report from the early counselling centre in Bremen-Hemelingen

33
From research and practice
IKK-News 1–2/2005: Violence against children
Parenting education sessions in an un-derstanding atmosphere, too, encouragepsychosocially stressed mothers to be-come involved.
An example: in an emotional turmoilan adolescent mother and her 15 monthold daughter burst into a parenting semi-nar on the subject “Dealing with defi-ance”. The father of the child, who wassupposed to baby-sit the daughter, stoodthe mother up. She therefore broughtthe child with her. She acts very insecurein the seminar and initially tries to strapher child – who is very lively – to thebuggy and pacify it. But by that sheachieves the opposite effect. The child be-comes defiant. Both mother and childraise their voices. In between, her mobilerings. She is embarrassed by all this andwants to leave the room. I try to enableher participation and tell her how I ap-preciate her effort to make her way overhere despite the disappointment. Noweverybody would have the opportunityto practice managing defiance. The otherparticipants are willing to do that andinvite the mother to stay. I ask her to sitin my vicinity and encourage her to relaxand let her baby play on the floor. Thechild calms down and gets interested inthe toy my colleague has brought it.While I speak, mother and daughterboth seek intensive eye-contact with me.Gradually the mother-child-interactionrelaxes and during the time of the semi-nar both find a space to cultivate theirrelationship in the presence of a third per-son. At the end of the session she repeat-edly expresses her thanks to the group.She is relieved that the fit of defiance didnot escalate – something that almost in-variably happens when she is alone withher child.
However, there are difficulties in ourwork, too. Our job to counteract risks inparent-child-relationships makes the par-ents fearful about contact with us advis-ors. The cooperation suffers because oftheir anxiety that their child will be takenaway. The fear, however, may also be themotor, for instance, to address the prob-lem of domestic violence and to look for new ways to find social security formother and child. Again and again wetry to convey to the parents that our pri-mary goals are the stabilisation of theparent-child-relationship and the infants’developmental support.
If parents fail to support sufficientlytheir child’s need for secure attachmentand autonomy and if they neglect theirresponsibility in the child’s development,the infant will need additional caregiversto offer support and social security.These will be provided by the case-man-agement of the outpatient social service.
Working methods such as guidance,counselling, early intervention, and psy-chotherapeutic sessions to help high-riskfamilies often merge into one anotherwhen we, along with the parents, wantto focus our attention on the successfuloutcome of positive parent-child-inter-actions. The facilitator as a secure attach-ment figure endeavours to adapt herselfto the needs of the parents in order toopen up the, as yet, awkward dialoguebetween parent and infant to both sides(child- and parent-centred) and to con-vey secure contact. As the parents experi-ence that they can have an impact andare able to counteract critical develop-ments, the rapport with their childrenand the counsellors changes. These correct-ive experiences are vital for the buildingof a trusting cooperation, particularly forparents who tend to distrust advice andparenting education services.
The reflection of our work within theteam of pedagogues allows us to ignitethe parents’ interest in the developmen-tal goals of their children in a concreteand close-to-their-needs fashion and inconcord with the life situation of theparents. The additional implementationof the early childhood intervention pro-gramme “Opstapje” (Dutch for step orstair) for at-risk families with two- tofour-year-old, somewhat developmentallydelayed children, for instance, showedthat their enthusiasm for play, as well astheir motor, cognitive, and social devel-opment was improved by the promotionof mother-infant-interaction and theemotional guidance of the mother. Afterdevelopmental guidance lasting one anda half years through the “Opstapje” earlychildhood intervention programme, thechildren managed to reach a normal state.The academic monitoring was conductedby the German Youth Institute of Munichin cooperation with the Universities ofErlangen and Bremen. All mothers appre-ciated the participation in the diagnosisand took pleasure in their children’s pro-
gress. When the inner-familial stress wasmoderated, their feeling for play wasenhanced. While their tendency towardisolation decreased, their need for be-longing grew.
We guide parents in order to workwith them towards brighter prospectswhich make their lives with little childrenseem worthwhile. The discovery of theirintuitive skills encourages them to makeuse of support service for themselves andtheir babies.
We advise parents characterised by deepinsecurity in dealing with their baby, oroffer early support with regulatory disor-ders such as excessive crying, sleeping,and eating disturbances (Papousek et al.,2004). It is especially important to givepsychosocially burdened parents a chanceto bring to life a positive image of theirchild and to widen their understandingabout the significance of the relationshipwith their child. Parents who carry withthem a negative image of themselvesfrom their own childhood and who ex-perienced only little understanding con-cerning their development need moretime and space to express their thoughtsand feelings about the child. This proc-ess can be very touching. Almost invaria-bly the parents desire that the child shouldbe better off one day than they them-selves are – even though other needs andfears often stand against that.
With our encouragement of playfulexchanges with the child when feedingand nappy-changing or through babymassage parents have the opportunity topractise sensitive interactions and todevelop secure attachment patterns. Thevideo-assisted interaction diagnosis en-ables them to modify their attitude andbehaviour towards the infant. Assistancein structuring their daily lives encouragesa rhythm suitable for the child andcontribute to the soothing comfort of thebaby and the relaxation of the parents.

34
From research and practice
IKK-News 1–2/2005: Violence against children
Psychotherapeutically orientated con-versations are mainly conducted withmothers who were exposed to violenceand pain in their childhood and who livein an outsider position with their fami-lies. We have become a contact point forthem, a place where they can open upand talk about their experiences of humil-iation and violence. The advisor becomesa “container” for their contradictoryemotions and often painful experiences.During this encounter, acute feelings of
disappointment and fury towards theirown parents, foster parents, the authori-ties, the partner or the child who does notact according to the mother’s will oftenbreak through impulsively. However, fearand a profound longing for harmoniousrelationships are perceptible. The oscil-lation between anger, distrust, resignationand longing puts a strain on the cooper-ation, but it is also what makes it “neces-sary”. We try to help the mothers attainaccess to their feelings and talk aboutthem rather than destructively act themout. In this process we endeavour to createfor the mother a positive mental image of the child. It is not easy to endure the
often fierce fits of fury, self-humiliation,dissociation, denial, and passivity ofmothers traumatised early in their lives.But if we succeed, they relax and starttalking about themselves in a more co-herent fashion. This also changes themother-child-relationship. The burden isremoved somewhat from the infant, whois able to experience itself as a separateentity from the mother when she isreferring to the counsellor as a referee.When the child senses the cessation of themother’s inner pressure and her threaten-ing silence or scolding, it feels less nervous,observes more attentively what is hap-pening around it, and starts to play moreactively. We then draw the mother’s atten-tion to that. Some value this with a senseof achievement and enjoy seeing thattheir child, too, “can play” and that theycan see the progress in their infant’s de-velopment.
Who comes to see us?
When henceforth we speak of parents,this refers mainly to mothers, since theyconsult our advice service more oftenthan fathers. We never or very rarely reachfathers of high-risk families with violenceproblems. Why is that?
I have addressed various fathers andmothers with this issue. Men’s responseswere such: “Upbringing is the respon-sibility of the woman.” – “This is aboutchild protection; that puts me off.” –“You don’t reveal your problems so readily.”The women expressed themselves on amore intimate level: “As a man you don’tlike to admit that you beat your wife un-less maybe you want to change.” –“They are embarrassed about the thingsthey do.” – “It is hard to change, andeven harder for a man to do so.” – “Mendon’t have any motivation to change” –“It’s scary to have to do without aggres-sions” – “You’re on virgin soil when youchange yourself; it’s scary, especially formen.” Overall the demand for counsel-ling, even among fathers, has increased,or they take up our suggestion to see usalong with the mother and child.
The word has gotten around amongmany parents that we provide supportfairly quickly when they have difficultiescalming their child, if it acts defiantly orunusually or when mothers feel at theend of their tether, especially in times of
Early childhood
intervention
Parental education
Parent and child
Arrangement ofpsychotherapy
Cooperation and
networkingConsultations
Psycho-therapeutically
orientatedconversations
Developmentalguidance
Illustration 1: Transitions in the spectrum of our work at the early counselling centre Bremen-Hemelingen

35
From research and practice
IKK-News 1–2/2005: Violence against children
trouble with their partner or family. It isthe desire for a harmonious relationshipwith their baby or for a lightening oftheir burden in periods of stress and riskof the parent-child-relationship that leadsparents to us. Mothers with babies andtoddlers mainly find their way to us inorder to discover a peaceful rhythm withtheir child, to comfort it appropriately,and to learn to “guide” it. Or they areseeking contact with a parent-baby-group,individual, couple, or family consulta-tions, or they want to collect informationon their child’s development.
The parenting school arranged by theHaus der Familie is an important com-plement.
The Mannheim longitudinal studygives evidence that a proper mother-infant-relationship has a protective effect and iscapable of preventing the occurrence ofdevelopmental disorders. Noticeable prob-lems at an early stage of the mother-in-fant relationship are a risk factor for boththe social-emotional and the cognitivedevelopment of the child. But the mentalhealth of the mother, too, depends onthe quality of their relationship (Lauchtet al., 2000). Psychosocially burdenedfamilies often show a cluster of risk factorswhich bear upon interactions and threat-en a healthy development of the child.
Risk featuresOne of the main risk factors of our
hard-to-reach parents is the trivialisationor denial of self-endangerment or theendangerment of their children. Thedevelopment of a small child is at risk ifa mother or both parents downplay theirsubstance addiction (e.g. drug abuse), if mothers tolerate repeated abuse by theirpartners, or if they allow themselves tobe blackmailed for their social and childbenefits. Many of our mothers frommultiple-problem-families display psycho-somatic illnesses such as anorexia, com-pulsive overeating, migraine, and otherstress symptoms. These often correspondwith restlessness, attention deficit, andthe bad physical state of the infants,which in turn burdens the already stres-sed parent-child-relationship.
Traumatic childhood experiences ofparents are a risk, often with profound re-percussions to the children. A mother whowas repeatedly frightened and harmed inher childhood and who never experienceda comforting and safeguarding parental
setting tends to try and somehow pro-cure comfort and relief for herself, ratherthan turning hopefully to someone else.She fears closeness and avoids attachment.The children get to feel this, too. Theymust do without physical closeness andthe satisfaction of their attachment needsassociated with it. They are left alonewith their feelings and thoughts (Brisch,2003). One moment the mother willcling to her child, the next moment sherejects it and neglects its needs, the sameway she was once neglected and abused.The disappointments of early attachmentoften get repeated in insecure partner-ships. The mother’s fear of being aban-doned, abused, and “going down” againalso affects their children. They, too, willdevelop insecure, ambivalent attachmentbehaviour. They find it hard to shed theimages of witnessing their mother beingbeaten and raped. Mrs. X says: “At first I used to be afraid when my mother wasbeaten up. When I made a scene, she usedto hit me. But I still wanted to help her.Then I started feeling hatred. I couldn’thelp her, and one of her partners eventried to get at me. In school everythingwent wrong. I couldn’t be bothered withit and ran away. Now, I thought, shemight be pleased about my baby. But noluck. If I didn’t have a child, I wouldn’tcome here. I want everybody to knowwhat kind of mother I’ve got.” This youngmother is now financially exploited bythe father of her child. In her disappoint-ment and rage she beat her baby. Nowshe is trying to escape the vicious cycleof passing on her experiences of violence.
A mother who fails to protect herselfand lives under anxious tensions, en-dangers her child’s protection and alsoloses developmental continuity for herselfand her infant. Unconsciously her childis used as a “cohesive agent” and expectedto relieve the mother’s tension. The fearof the child being taken away is also mo-tivated by the mother’s fear that she willbe an abandoned nonentity once more.
There are typical patterns of reactionthat develop as coping-mechanisms inresponse to early traumatisation, when ahuman being’s psychological and bio-logical capacities are overtaxed and are notcushioned by caring support. These com-prise unconscious re-enactment of situ-ations similar to the trauma, numbnessand dissociation, defence mechanismscharacterised by struggle and flight, as
well as victim-perpetrator-reflexes thatfrustrate the desire for change and coping.
Another risk factor is long-term un-employment. It alters the experience oftime, attitude, hope and resilience. If work is missing as a structural elementof the day, in many families “time getsout of kilter”. This, too, causes stress andhas a bearing upon psychological well-being, personal relationships, planningand mutual agreements. Hence, long-termunemployment and the parents’ lack ofprospects cast a dark shadow over the de-velopment on their child.
Tightrope walk in preventive workwith psychosocially stressed mothersand their babies
Parents who were neglected, abused,or maltreated as children have developedunder these conditions of deprivationcertain defence mechanisms in order toregulate fears and their relationship withtheir environment. Rigid distinctions in “good-and-bad”, denial, projection, regression and somatisation work as defences, but hamper cooperation. Mat-ters are further complicated by the factthat psychosocially burdened familiesusually have to deal with several parallelproblems and therefore are under enor-mous pressure.
Stoléru and Morales-Huet (1994) de-scribe in their preventative and therapeuticwork with multiple-problem-families withbabies and infants an early unconsciousdefence mechanism against relationshipsexpressed by assault, resulting from frus-tration and traumatisation suffered in theparents’ childhood. Such an assault canbe evident in the aggression meeting theadvances of facilitators and therapists,and as transference, can be understood asan offence against the mother or otherprimary attachment figures. Absence, tardiness, cancellation of appointments,and perceptible hostility gnaw at the re-lationship between client and advisor.However, these also guard the individualagainst the subconsciously anticipatedattack which overwhelmed it as a childwithout protection.
This early dynamic of defence mecha-nisms contributes significantly to socialisolation.

36
From research and practice
IKK-News 1–2/2005: Violence against children
Loss of social inclusion reinforces feel-ings of stress, shame, inferiority, andguilt. What also plays a part is envy ofthose who have it better or feelings ofrivalry towards one’s child, who dares toexpress its needs. Because of the emo-tional dependency of a partner and theentanglement with one’s origins, theparents’ intuitive skills vanish more andmore. It is not uncommon that thetension in hard-to-reach families is analo-gous to a pressure cooker. It is released inconflictual and violent relationships be-tween the partners and between parentsand children, a constellation underwhich, from our experience, mainly themothers and their children suffer.
How do we respond to situationswhen the child, other attachment figures,or we ourselves as facilitators get caughtup in a vortex of dissociation, projec-tions, and negative attributions of theparents and when their frustrationthreshold is very low?
We cannot help multiple-problem-families effectively without understand-ing the fierce processes of defence andprojection. But we are not able to resolvethem either. For this, long-term therapyis required. However, for parents thisseems hardly comprehensible as a solutionbecause they tend to attribute their mis-ery to some external reality, for instancedebt, too small a flat, and unemploy-ment. What we can do, however, is tobring the increase of defence mechanismsto a halt, and direct the process towardswhat they can perceive and change intheir relationship with their partner andchild. For the parents to experience thatwe are able to endure their fierce feelingsand defensive responses can make for anew connection. This is evident in that alarge proportion of our psychosociallyburdened mothers arrive punctually andregularly for the agreed appointments, andthat they consult our support on a long-term basis in order to take care of theirown social security and that of their chil-dren. However, if a mother’s internal andexternal stresses dominate, a sensitiveand stable engagement with the child isat risk. Frequently, the history of a trau-matic childhood is continued in the chil-dren. A severely traumatised mother’scapability to offer her child a protectedspace for its development is very limited.She needs a sustainable network for
herself and her infant in which the de-velopment of the autonomy of both canthrive. It needs to be clarified for indi-vidual cases whether an interdisciplinarylinkage of medical, therapeutic, or social-pedagogical support on an outpatientbasis or whether an inpatient mother-child-therapy is necessary (Lüders & Deneke,2001). If the mother learns to confide insecure attachment figures and to accepthelp for herself and her child, the qualityof the mother-child-relationship and thechild’s development can improve. But formothers with severe personality disordersthe barriers against trusting other peopleare high, and even higher against psycho-therapy. However, in our day-to-day workwe find it is possible to encourage indi-vidual mothers to seek psychotherapy.With this help they managed to improvethe perception of their child’s signals andto engage more sensitively with them.
Regrettably, the possibilities of findingan inpatient or outpatient place in therapyare highly limited.
What helps?
The primary fear of mothers in ourcounselling service whose children areexposed to the risk of neglect, abuse andmaltreatment is that their children willbe taken away from them, not the possi-ble violation and neglect of the child orthe mother. We incorporate this fear andtry to relate it to the mothers’ personalhistory, her experiences of separation andloss, and her fear of abandonment inorder to motivate them to improve theircurrent living situation by giving theirchildren sufficient footing and protection.In cooperation with the Haus der Familiewe try to detect what is beneficial for themother and what her strengths are, inorder to boost her self-confidence and topromote child-oriented activities. We al-ways prioritise on a strengthening of themother-child-relationship and endeavourto focus the mother on the perception of the infant’s needs. The naming of riskand protection factors, in conjunctionwith helping the parents to realise theirdevelopmental tasks in small steps, canhave a liberating effect and open up anew door with clearer ideas about oneselfand the thriving of the child. It is impor-tant that parents develop a self-propelleddesire to understand their children better
and that they feel they can change thecommunication and the engagement withtheir child for the better. The boundariesof effective counselling are reached if theparents’ possibilities for a more sensitiveway of communicating with their childare so drastically limited by their psycho-social stress that a relaxed being-togetherand an ego-strengthening behaviour areimpossible. It needs to be clarified, then,whether mother and child need moreintensive attention in conjunction withpsychotherapy for the mother or whethermother-child-psychotherapy is advisable.
These considerations illustrate thatwork with multiple-problem-families needsan interdisciplinary network in order toimprove the living conditions of babiesand infants. For the help agenda, a jointdecision needs to be made regardingwhich risk factors are just about tolerablefor the child and how protection and de-velopmental promotion for the child andits family can be realised. This also in-volves easily accessible therapeutic supportfor parents.
Our experiences show that the supportfor parents with enormous psychosocialstresses can be effective, if• they can find a self-propelled desire
for professional help for themselvesand their children,
• they take care of their social securityin cooperation with professional facilitators and other parents (aspectof self-help, e.g. in mother sessions),
• they perceive what their child isdoing, experiencing, and feeling, andhave the ability to specify it linguis-tically,
• they support the development of thechild’s autonomy,
• they specify ideas about developmentand recognise as well as reflect upontheir projections onto the child,
• they find a way out of the chaos andentanglement within the family andmanage to organise a supportive wayof living together with their children,
• they ultimately make corrective, posi-tive experiences through the interac-tion of social support, early assistance,parenting education, and develop-mental counselling services and takemore pleasure in their child.

37
From research and practice
IKK-News 1–2/2005: Violence against children
A vital prerequisite in the cooperationwith traumatised and very insecurelyattached parents is the willingness to en-gage with the parents and to enable themto experience relaxation and “holding”.Children and parents alike rely on aspace where they can address and learnto endure their emotions and innertensions, but also where they can developcreativity and new initiatives. In dealingwith early, recurring traumatisation a supportive disposition which is gearedtowards developmental support, resourcedevelopment and late-maturation ishelpful (Naumann-Lenzen, 2003).
Example of a successful case of con-sultation: When Mrs. Z. came to see uswith her 10-month-old baby, the infantwas remarkably quiet. It did not seek orhold eye-contact, almost constantly dis-played a smile which, upon closer obser-vation, proved to be more of a defensivegrin. I was concerned about the avoid-ance of eye contact and the child’s lackof vocalisation as well as the mother’squietness and inhibition. She classifiedher child as easy-care. When I asked herhow she could tell, she said: “ThankGod it hardly ever cried, it was happy inthe playpen … it didn’t notice when we(father and mother) got high in thekitchen.” Gradually it became apparentthat both parents were nearly alwaysunder the influence of cannabis, and thattheir baby was nearly always put away inthe pen. It learned to regulate itself andto do without the loving affection of itsparents. It was only taken out for feedingand nappy-changing. The relationshipbetween mother and child seemed frozen.There was hardly any eye contact, nosocial smile, no positive excitement, noreaching out of the little arms, no oral ormanual exploration of toys. The babysought neither the mother’s closeness norours, but avoided eye contact, smiles,and physical approaches. Selma Fraibergdescribes this avoidance and paralysis asan early pathological defence response to helplessness and anxiety (2003). At theage of one year the child of our clientdisplayed good motor skills, but was re-markably withdrawn and disconnectedfrom the mother. It was hard for us, too,to reach the child. When it hurt itself it did not actively seek comfort and pro-tection. We addressed the risk to the child’swell-being and the necessity of addiction
rehabilitation. The mother was con-cerned by the prospect of her child beingtaken away from her and after severalmonths managed to do without drugs. It is still awkward for her to communicateplayfully with her baby, but she willinglyaccepts all support offers of the earlycounselling centre and tries to make pro-ductive use of them. Meanwhile, sheceased to trivialise her addiction and rec-ognised her child’s avoidance behaviouras a consequence of her lack of affection.Eventually, painful feelings arose in herthat her child did not turn towards her,did not listen to her, and ran away. Aftermother-child-therapy, instigated by us,that lasted several months, mother andchild displayed a better mutual relation-ship, the mother became more active, isable to fondle her child, and to talk withit more. The indicators of an early at-tachment disorder are still not entirelyrepaired. But the mother has managed toremain free of her dependence upondrugs and is coming to terms with hertraumatic childhood. She is about to startan outpatient therapy. While initially thechild was her “agenda” (in the words ofthe mother), she has now developedfuture prospects for herself. She is pleasedto see that, now, her child accepts herattempts to comfort it and listens to her.
Outlook
The work in the early counselling cen-tre shows that in high-stress situationstraumatised and psychosocially stressedmothers, too, are seeking early supportwith their babies and infants. This processreveals the necessity of long-term guidancein order for the mothers to have new,corrective experiences for themselves andwith their child. The youth welfare serviceis particularly adept at gaining the con-fidence of at-risk families with insecureattachment patterns and arranging forthem to have access to further support ser-vices and therapies. These families needpsychotherapeutic help in order to workthrough traumas and other stressful lifeevents, because otherwise these will leadto an increase of violence in the parent-child-relationship and obstruct the wayto new, constructive coping-strategies.
The findings of early interventionprogrammes for at-risk families give evi-dence that preventative and early applied,long-term training in sensitive interac-tion between parents and child in con-junction with psychotherapeutic sessionscan strengthen secure attachment, thelatter being an important shield againststressors and deviant development of thechild. Traumatised parents with babiesand infants can be reached more effective-ly with the cooperation of the institutionsresponsible for developmental guidance,counselling, early childhood intervention,and psychotherapy. Social-pedagogicalservices and high-quality day-nurseriesshould be extended in order to enhancethe chances for integration for childrenfrom socially stressed families. It is ouraim to foster a secure attachment of thesechildren and to stabilise a positive par-ent-child-relationship. Seen against thebackground of the emotionally demand-ing childhood of many of these parents,involving the discontinuation of relation-ships, as well as experiences of abuse andneglect, it is understandable that notonly time and patience are required, butalso the willingness to attend to theseparents. Quite like a baby or infant theyrely on positive, affectionate reciprocitywhich will be available to them on along-term basis.
AcknowledgementThe work in the early counselling centre
could not have been accomplished withoutmy colleagues in both the counselling centreand the Haus der Familie. I would like tothank everybody for that.

38
From research and practice
IKK-News 1–2/2005: Violence against children
Contact
Inge BeyersmannEarly counselling centreHaus der Familie – HemelingenHinter den Ellern 13D-28309 Bremen
Telephone: +49 (0)421 /498836-0
Literature
Beyersmann, I. (2003): Beratung für psychosozial belastete Familienmit Säuglingen und Kleinkindern – Chancen und Grenzen interdisziplinärerZusammenarbeit. In: Verein für Kommunalwissenschaften e.V.(Hrsg.): It takes two to tango. Frühe Kindheit an derSchnittstelle zwischen Jugendhilfe undEntwicklungspsychologie. Berlin: Verein für Kommunalwissenschaften e.V.,136–152.
Beyersmann, I. (2000): Beratung für Eltern mit Säuglingen undKleinkindern in einem sozialen Brennpunktim Rahmen von Netzwerkstrukturen. In: Frühförderung interdisziplinär, 19, 10–22.
Brazelton, T. B., Cramer, B. G., (1994): Die frühe Bindung. Stuttgart: Klett-Cotta.
Brisch, K. H., Hellbrügge, T. (2003): Bindung und Trauma. Stuttgart: Klett-Cotta.
Fraiberg, S. (2003): Pathologische Schutz- und Abwehrreaktionenin der frühen Kindheit. In: Praxis der Kinderpsychologie undKinderpsychiatrie, 52, 560–577.
Laucht, M., Esser, G., Schmidt, M. H. (2000): Längsschnittforschung zur Entwicklungs-epidemiologie psychischer Störungen:Zielsetzung, Konzeption und zentraleErgebnisse der MannheimerRisikokinderstudie. In: Zeitschrift für Klinische Psychologie undPsychotherapie, 29, 246–262.
Lüders, B., Deneke, C. (2001): Präventive Arbeit mit Müttern und ihrenBabys im tagesklinischen Setting. In: Praxis der Kinderpsychologie undKinderpsychiatrie, 50, 552–559.
Naumann-Lenzen, M. (2003): Frühe, wiederholte Traumatisierung,Bindungsdesorganisation undEntwicklungspsychopathologie. In: Praxis der Kinderpsychologie undKinderpsychiatrie, 52, 595–619.
Papousek, M., Schieche, M., Wurmser, H. (2004): Regulationsstörungen in der frühen Kindheit. Bern: Huber.
Stoléru, S., Morales-Huet, M. (1994): Prävention bei subproletarischen Familien. In: Psyche, 48, 1123 –1153.
Early childhood intervention pro-gramme “Step by step – opstapje”
“‘Step by step – opstapje’ is a two-year, prevention-oriented early child-hood intervention programme forchildren between the age of 2 and 4from psychosocially burdened familieswhich is organised as a home-visit-programme. The intention of this out-reach service is to support child-raisingin families who cannot be reached by the classical “drop-in structures” of child-raising and family support.The overall conceptual orientation of the programme is geared towardsempowerment understood as the utilisation and extension of existingresources, as well as the strengthen-ing the personal responsibility of the families. The linchpin of the pro-gramme is the improvement and in-tensification of the mother- or father-child-interaction.”
For further information:
Alexandra SannPsychologist
Deutsches Jugendinstitut e.V.Nockherstraße 2 D-81541 München
Telephone: +49 (0)89 /62306-323 Email: [email protected]: www.dji.de/opstapje

39
From research and practice
IKK-News 1–2/2005: Violence against children
Introduction
A baby’s excessive crying during thefirst months of life presents for the affect-ed parents enormous stress and insecuri-ty. In pre-verbal communication whimper-ing, crying, and screaming are seen assignals essential to life which express thebaby’s feelings. What are the reasons, then,if a baby keeps crying despite its needshaving been satisfied? What are the con-sequences of excessive crying for the fam-ily as a whole? Based upon clinical ex-periences during the “Consultation Hoursfor Crying Babies” in the children’scentre of Munich and the accompanyingacademic evaluation we have come tounderstand that excessive crying presentsa risk for a healthy development of theparent-child-relationship, and can, in somecases, lead to abuse and neglect.
Symptoms
According to international consensusthe distinction for academic purposesbetween normal and excessive crying isbased upon Wessel’s “rule of three”(1954). Wessel described the excessivelycrying baby as “an otherwise healthy,well-fed baby with fits of irritation, whim-pering, or crying that last more thanthree hours a day, on more than threedays a week for more than three weeks”.
However, clinical diagnosis needsmore than a criterion based solely uponthe duration of crying and whimpering.
We are dealing with an utterly com-plex phenomenon reflecting difficultieson the levels of the infant, the parents,and their interaction.
Core symptoms of the child are uncon-trollable crying without recognisablereason and long stretches of mysteriousrestlessness and whimpering. These babiescannot be calmed by regular pacificationstrategies. Carrying the baby around,usually holding it in ever changing posi-tions, will only have a brief calming effect.Many of the babies are noticeably suscep-tible to visual stimuli; they observe their
environment with widely opened eyes,and do not seem to be able to switch off.Thus, the parents “learn” from their babyto keep coming up with new distractions,because restlessness and crying come toan end temporarily by virtue of intensive,constantly changing stimulation. However,this stimulation will not create genuinetranquillity in the child, so that the cryingresumes once the stimulation ceases.During the day the babies seem to bebarely and only for short periods able togo to sleep; they seem to fight against it.Around late afternoon and evening un-rest and crying noticeably increase, untilthe children fall into a relatively soundsleep around midnight.
The mothers of excessively crying babiesare usually on duty around the clock try-ing to make her infant happy. Still thebaby seems to confirm, by its incessantunrest and whimpering, that the parentsare failing. In addition to this, some ofthe excessively crying babies do not snuggleup, but push themselves away, as thoughthey are seeking to avoid the mother’scloseness. Besides feelings of helplessness,exhaustion, and desperation in the lightof the alarming cries and their experienceof powerlessness, many parents also feelrage, aggression, and negative attitudestowards their child – emotions they areshocked by and which have an unsettlingeffect on their self-esteem (Papousek &Hofacker, 1995; St. James-Roberts et al.,1995). Usually, unless severe psychosocialand biographical strains exist, the parentsmanage to keep a check on aggressivefantasies and impulses, so that child abuseor neglect can be avoided.
Diagnosis
To designate this complex appearanceinvolving irregularities on the level of thechild, the parents, and the interaction, thephrase early childhood regulatory disorderwith excessive crying is used. If cryingpersists over the first three months of life,this is called persistent excessive crying(Papousek & Hofacker, 1995).
From a systemic point of view the baby and its regulatory problems cannotbe looked at in isolation, and neither canthe overtaxed mother who does notmanage to calm her child. Thus, the termdiagnostic triad is more precise, becauseaside from the child-related aspect ofincessant crying and problems regardingthe sleep-wake-regulation, it also cap-tures the parental aspect of exhaustionand psychosocial stress, as well as theaspect of interaction which often fails orescalates (Papousek, 2004).
Prevalence
The prevalence of excessive cryingduring the first trimester is between 16and 29 per cent in representative samplesof various western industrial countries(Lehtonen, 1994; St. James-Roberts &Halil, 1991). The differences are mainlya result of diverging criteria for distinction,survey instruments, and the point oftime at which the data collection was con-ducted. The only retrospective epide-miological study thus far conducted inGermany stated a prevalence of 21 per cent(excessive crying during the first tri-mester). 8.3 per cent of mothers statedthat the crying persisted beyond thethird month of life, thus, among nearly40 per cent of excessively crying babies(Wurmser et al., 2001).
Although it is generally assumed thatfirst-borns and male newborns displayincreased crying problems, this assump-tion failed to be confirmed in two largestudies (Lehtonen, 1994; St. James-Roberts & Halil, 1991). However, thereis a cluster among siblings and twinswhich indicates an influence of geneticand environmental factors. According to most academic surveys, the age of themother, the level of parental education,and socio-economic status have no im-pact (Lehtonen, 1994).
Ruth Wollwerth de Chuquisengo & Heike Kreß
Excessive crying during the first months of life and its treatment in the “Munich Consultation Hours for Crying Babies”

40
From research and practice
IKK-News 1–2/2005: Violence against children
Causes and conditional factors
Often paediatric and neuro-paediatricdisorders or illnesses are among the causingfactors of excessive crying1: they can bethe sole causes, but often they are part of a more complex configuration of caus-es. In the case of those babies referred tothe consultations by paediatricians, acuteillnesses associated with increased crying(such as inflammation of the middle ear,inflammation of the urinary tract, gastro-enteritis, fractures etc.) could be ruledout as well as malnutrition caused by toolittle food on offer (Ziegler et al., 2004).
Only in 5 per cent of cases are gastro-enterological illnesses (intolerance to lactoseor cow milk protein, gastroesophagealreflux) the sole reason for excessive crying(Lehtonen et al., 2000; Miller & Barr, 1991).
Furthermore, Biedermann (2000) postulates a hypomobile dysfunction ofthe cervical spine as a possible cause forexcessive crying. However, according to awide-ranging double-blind study, generalmanual-therapeutic treatment for allexcessively crying children fails to showthe desired effect of stopping the crying(Olafsdottir et al., 2001).
In contrast to a control group the clin-ical group of the babies introduced in the“Consultation Hours for Crying Babies”stands out for its increased number ofneurological irregularities (asymmetries,regulatory disorders of the tonus, faintdisorder of the central coordinationincluding posture deficit and occasionalhypomobile dysfunction of the spine).Commonly, these irregularities improvedwith physiotherapy, manual therapy, orwith parental instruction on how tohandle their children. Frequent holdingand lack of experience in abdominal orsupine positioning on a firm mat appearsto lead to a slight delay of motor devel-opment which is usually quickly madeup for if appropriate measures are taken(Ziegler et al., 2004).
But paediatric disorders are by far notthe only symptoms explaining excessivecrying. Other revealing insights followfrom investigations of the crying habits ofall babies during the first three months.Representative samples of healthy babiesshowed that the duration of whimperingand crying is generally increased duringthat period and that the individual differ-ences of the daily degree of crying are
very high (Barr, 1990). The average whim-pering and crying duration goes up untilthe sixth week of life and then decreasescontinuously until the twelfth week. Thatthis crying curve is tied very closely tothe postnatal stage of development wasevident in a study of premature babieswho had the same phase-typical durationof whimpering and crying – but with regardto the corrected age (Barr et al., 1996).
Excessively crying babies display thesame curve in their daily crying patterns.The increased crying usually starts in the first or second week of life; it peaksaround the sixth week and graduallyabates at the end of the third monthwhen the first bio-psycho-social phase ofdevelopment begins (Papousek, 2004).Thus, these babies represent the extremeend of normal individual differences.
The first trimester is a phase of intensephysiological adaptation processes duringwhich the baby depends to a high degreeupon the regulatory support of its care-givers (Papousek & Papousek, 1990).Central developmental topics during thatstage are the regulation and the cyclicalalternation of behavioural states (activesleep, quiet sleep, quiet-alert waking state).The regulation of these behavioural sta-tes is closely related to the basic adaptiveregulatory system which controls theactivation and relaxation processes duringthe reception and processing of environ-mental stimuli (Papousek, 2004).
Babies with well-developed self-regula-tion have an early ability to maintain a quiet-alert waking state; they display a balanced excitability of all senses, are ableto let go if they get tired, can calm them-selves by sucking their hands, and go tosleep without difficulties. Excessivelycrying babies, however, have tremendousproblems regulating themselves; they on-ly manage to stay in a quiet-alert statefor a very short time, are frequently over-excited, do not manage to calm them-selves down, appear to fight against fall-ing asleep, and ultimately do not fallasleep (Ziegler et al., 2004).
Both the study of non-clinical samplesof excessively crying babies and the resultsof the clinical sample from the “Consul-tation Hours for Crying Babies” point toan overall duration of sleep that is onehour shorter than normal (Kirjavainen etal., 2001; St. James-Roberts et al., 1997;Schaumann, 2003).
Excessive crying on one hand and in-consolability, lack of self-relaxation andability to fall asleep on the other can beinterpreted as an indication of a dis-turbed balance between activating andinhibiting processes. This complicatesthe regulation of the waking states asmuch as the transitions between wakingand sleeping.
Various causal factors are discussed asthe reasons of this disturbed balance.
The constitutional variability of new-born children can be genetic or acquiredin the prenatal period. With respect tonearly all features of temperament, exces-sively crying infants come off significant-ly less favourably than their peers with-out crying difficulties (St. James-Robertset al., 1998a; Papousek & von Hofacker,1995; 1998). However, it is not possibleto draw reliable conclusions regardingthe constituent factors, because of theconfounding of temperament and relativeimmaturity especially during the firsttrimester. The decisive factor is the long-term stability of the temperament fea-tures beyond this developmental phase(Wurmser, 2004).
Except for an increased occurrence of pre-term labour (involving treatmentwith tocolytics) and nicotine abuse inthe clinical group there are no furtherdifferences evident with regard to organicpre- or perinatal risk factors (Papousek& Hofacker, 1998; Ziegler et al., 2004).However, there is a significantly higherpressure with respect to prenatal risk factors such as stress, fears, partnershipconflicts, depression, and primarily un-wanted pregnancy.
These prenatal burdens present a riskto the child’s development in two respects:by influencing, possibly directly, theconstitutional preconditions of the infant’sself-regulation, and by impairing theprimary caregiver’s resources. The correla-tion between prenatal psychosocial stressand increased irritability of the newbornis repeatedly documented in researchliterature (Mulder et al., 2002; Murray& Cooper, 1997; Rautava et al., 1993).
The still widespread assumption thatexcessive crying is primarily caused byparental failure can be refuted by researchfindings which show that the responsive-ness and the communicative capacity of
1 Explanations of these paediatric irregularities canbe found in Ziegler et al., 2004.

41
From research and practice
IKK-News 1–2/2005: Violence against children
mothers with excessively crying babiesand their peers in a control group do notdiffer (St. James-Roberts et al., 1998b;Papousek & Hofacker, 1996). However,in the process of calming and comfortingthe child a dysfunctional parent-child-interaction is evident, which is explicableby the mutually negative influencing ofparents and child.
Development-dynamics model of the emergence and continuation of excessive crying
A significant feature of the infant’s self-regulation during the first months is thedependency upon parents’ regulatorysupport which needs to be finely attunedto the child’s needs.
To what extent this is successful is oftendecided by the crying and its repercus-sions. Crying as an alarm signal inducesstress to the social environment (heart-pounding, increased blood pressure,sweating, psychological excitement), atthe same time, though, it induces intuitive-ly-attuned calming behaviour (physicalcontact while holding, soothingly rhyth-mic stimulation, descending melodies) as well as a strong motivation to identifyand remedy the cause for the crying. In response the baby nestles to the moth-er, the crying ceases and the baby calmsdown. Along with that mother or fatherwill calm down, because they feel con-firmed in their parental abilities by thebaby’s positive feedback and because theyhave experienced a moment of intimatecloseness with their baby, a moment of“positive reciprocity”.
Inconsolable crying, often coupledwith motor unrest, stiffening on themother’s arm or temporary complete in-accessibility, creates feelings of failure,powerlessness and depression in the par-ent and damages self-esteem. If it comesto feelings of powerlessness during a stateof arousal and alarm, almost all parentsdevelop aggression and powerless rageagainst their own baby. These are impuls-es which raise feelings of guilt and makeparents increasingly vulnerable. Ulti-mately, the intensity of the roused emo-tions is the breeding-ground for the pos-sible revival of latent conflict with thepartner or their own parents, as well asthe revitalisation of memories and affects,feelings of abandonment and childhood
pains. The effects become especiallyproblematic when the parental compe-tencies are persistently inhibited by inse-curities, depressions, and exhaustion.Consequently, the in any case dysregulat-ed baby has to do without the intuitivesupport of its parents. Initially, this leadsto a dysfunction in the context of calm-ing; increasingly, however, other day-to-day interaction patterns are negativelyaffected which are perpetuated by negativemutual influence or usher in vicious cir-cles of reciprocal escalation.
These vicious circles of negative reci-procity primarily emerge when parentsare exposed to cumulative psychosocialstress. In the clinical sample of the“Consultation Hour for Crying Babies”an increased post-partum manifestationof couple conflicts, conflicts with theorigin family, a troubled childhood, andsocial isolation of the mother could befound. 96 per cent of all mothers dis-played a syndrome of exhaustion or ofbeing over-taxed, and 33.5 per cent post-natal depression. A further 16 per centshowed indications of a neurotic relation-ship disorder, and 6.4 per cent showed apersonality disorder (Ziegler et al., 2004).
See illustration on next page
Possible risks of crying babies
Because of the unfavourable conditionsthat the baby suffering from regulatorydisorder brings with it, parents of thesechildren face considerably more stressthan parents of normally regulated babies.Hence, a regulatorily disturbed babymakes greater demands on the naturalchild-rearing competence. Depending onthe parents’ past (personal childhoodexperiences of abuse or neglect), missingresources (relief opportunities, partner-ship), risk factors (juvenile parents, con-sumption of drugs, socio-economic fac-tors), and psychological illnesses (depres-sion, borderline disorder, psychopath-ologies) this child-raising competencemay already be restricted or taxed, and itis additionally challenged by excessivelycrying babies.
Thus, on one hand insufficient parentalcompetence can bear negatively upon the child’s behaviour, and on the otherhand the parents’ competence will be fur-ther damaged by the infant’s increasingly
rejecting and withdrawn social behaviour(avoidance of eye contact, absence of so-cial smiles, restricted vocalisation).
The possible consequences of earlyregulatory disorders range from interac-tion disorders, progression disorders,attachment disorders, deprivation, andendangerment of personality develop-ment to severe forms of abuse, possiblyeven the child’s death.
For instance, several research reportspoint to the fact that babies with regu-latory disorders run an above averagerisk of endangerment to their well-being(Kindler, 2004).
The so-called shaken baby syndromerepresents a particularly dangerous formof abuse. The infant is highly vulnerablebecause of the premature development of the muscular system around the neckin comparison to the weight of the headand the brain structure in early childhood(immaturity of the brain, greater widthof the inner and outer cerebral fluidinterspaces). If the baby is grabbed by thearms or the body and ferociously shakenor thrown heavily, head-first, against asoft surface, “the infant’s head can be ex-posed to centrifugal or rotary force sostrong that they lead to several injuries,such as tears in the blood vessels or nervesin the skull or contusions in the brain asa consequence of a collision with theskull capsule” (Kindler, 2004). The diag-nosis is made more difficult because itmay not come to external bruises. About15 per cent of shaken infants die, circa50 per cent survive with remaining, par-tially severe disabilities, and about 35 percent of shaken infants do not exhibit neg-ative repercussions (studies of 20 chil-dren by Ludwig & Warmann in Thyenet al., 1991). On one hand, this is partic-ularly problematic because infants disabledby a shaking-trauma again make higherdemands on the parents’ (in any case miss-ing) rearing abilities and on the otherhand because the risk of abuse remains.In more than 50 per cent of shaken in-fants the fathers or partners of the moth-ers were the perpetrators. The factorsthat all these cases shared were a missingattachment to the child, ignorance aboutthe vulnerability of the infant, an inter-pretation of the child’s behaviour as inappro-priately hostile, as well as the perpetrators’impaired check upon his/her impulses(Kindler, 2004).

42
From research and practice
IKK-News 1–2/2005: Violence against children
Illustration 1: Consequences of excessive crying for the parents(modified according to Papousek & Hofacker, 1995)
Illustration 2: Development-dynamics, communication-based model(modified according to Papousek & Papousek, 1990)
Concepts of counselling and therapyused in the consultations in Munich
In cooperation with psychologists andpaediatricians the Consultation Hoursfor Crying Babies in Munich involve aloosely structured interview in order tofind out about the anamnesis of the infantand to detect stress factors and resourcesof the family. The paediatric and neuro-paediatric examination is conducted dur-ing a quiet waking phase of the baby; init, both the child’s development and itsregulatory skills and problems are assessed.
Psychological and physical relief of the parents
A first important step in working withstressed families is to take seriously theparents and their anxieties, guilt feelingsand aggressions and to be there for them.
Mothers particularly, because of weeksof sleep deprivation and daily stress, areso exhausted and overtaxed that opportu-nities for relief need to be created. Alongwith the parents we work out a way inwhich resources inside and outside thefamily can be used for relief and support.
Developmental counselling
Based upon the assumption that ex-cessive crying during the first trimester isan expression of dysregulated sleep-wake-organisation involving hypersensitivityand sleep deficit, we always offer com-prehensive developmental counsellingwith respect to crying, sleep-wake-regula-tion, and strategies for calming.
Communication therapy
Communication therapy is concernedwith the reciprocal understanding of par-ents and infant in the context of crying,calming efforts, and putting to sleep.Along with the parents we examine justwhat needs the baby expresses with itswhimpering and crying. If pain, hungeror boredom can be ruled out as causes,and the baby shows signs of sleepiness andhypersensitivity, or if it was two hourssince the last sleep-phase – as is the casemost of the time – we offer parents oursupport in the usually very difficult falling-

43
From research and practice
IKK-News 1–2/2005: Violence against children
asleep phase of their baby. In the contextof the therapeutic setting the parentscommonly succeed in getting their childto sleep; at home, left to their own de-vices, they find it harder. In this case weoffer the possibility of home visits by a social education worker who specialisesin regulatory disorders.
As a positive counterbalance to thesemany hours of whimpering and crying,another aim of the communication ther-apy is to create moments which areequally fulfilling for both parents and ba-by. Within the protected, therapeuticenvironment the parents are sensitised tothe short phases in which their babydisplays good regulatory capacities andinterest in its surroundings, and they areencouraged to use them for relaxed inter-actions. These phases of “positive reciproc-ity”, even though they may be of shortduration, present a vital step out of thevicious circle of excessive crying and itslong phases of “negative reciprocity”.
Parent-baby-psychotherapy
Excessive crying can trigger intensefeelings and episodic memories of pastrelationships which may eclipse anddistort the perception of the real baby.For instance, the crying may be inter-preted as an act of aggression, as intention-al screaming, or as an expression ofobsession, in which case it will provokeinappropriate responses. In some parents,deeply rooted feelings of abandonmentand anxiety are triggered. It is the ambi-tion of the psychotherapeutic work tofacilitate the parents’ undistorted percep-tion of the baby and its needs.
Duration of treatment and success
The evaluation of 218 children broughtto the consultations with a syndrome of excessive crying shows successful treat-ment in 92.6 per cent of the cases. By the end of the treatment 6.5 per centhad improved slightly, and 0.9 per centnot at all. On average, only four appoint-ments were necessary for a successfulintervention.
Summary
With its high prevalence, excessivecrying is one of the most wide spread dis-orders in early infancy. An accumulationof risk factors on the part of both theparents and the infant impairs the child’sself-regulatory skills and/or the parents’competence, as a result of which the par-ent-infant-communication is derailed.The manifestations of inconsolablecrying and its consequences for the youngfamily can take on dramatic forms to thepoint of abuse and severe neglect. How-ever, additional factors need to be presentin the parents’ lives if violence towardthe child is actually to occur. These areparticularly traumatic experiences oftheir own and reduced impulse control.It is questionable that these families canbe reached by the Consultation Hoursfor Crying Babies, since experienceshows that contacting such an institutionpresents too high a barrier for sociallydeprived and multi-problem-families. To fill this gap, midwives, paediatricians,and children’s clinics, among others,need to be vigilant with regard to at-riskfamilies.
Commonly, excessive crying is a tem-porary disorder which rapidly respondsto treatment and counselling. However,if it occurs in the context of multiplepsychosocial stresses and limited resources,it can persist and, in the long run, canlead to more profound disorders of com-munication, relationships, and behaviourduring infancy.
Therapy for excessive crying focuseson parent-child-communication and in-volves organic and psychosocial risk fac-tors on the part of both the parents andthe child. This makes it an importantand promising approach for preventionwith regard to subsequent relationshipand behavioural disorders.
Kontakt
Ruth Wollwerth de Chuquisengo Psychologist
Heike Kreß Social Education Worker
Ambulanz für SchreibabysKinderzentrum MünchenHeiglhofstraße 63D-81377 München
Telephone: +49 (0)89 /71009-330
44
From research and practice
IKK-News 1–2/2005: Violence against children
Literature
Barr, R. G. (1990): The normal crying curve: What do we reallyknow? In: Developmental Medicine and Child Neurology,32, 356–362.
Barr, R. G., Chen, S., Hopkins, B., Westra, T. (1996): Crying patterns in preterm infants. In: Developmental Medicine and Child Neurology,38, 345–355.
Biedermann, H. (2000): KISS-Kinder. In: Harms, T. (Hrsg): Auf die Welt gekommen. Berlin: Leutner.
Jacubeit, T. (2001): Misshandlung und Vernachlässigung imSäuglings- und Kleinkindalter. In: Schlippe, A. v., Lösche, G. et al. (Hrsg.): Frühkindliche Lebenswelten undErziehungsberatung: die Chancen des Anfangs. Münster: Votum.
Keefe, M. R. (Ed.): New evidence on unexplained early infantcrying: its origins, nature and management. Johnson & Johnson Pediatric Institute Round TableSeries. New Jersey: Skillman, 133–148.
Kindler, H. (2004): Was ist unter Schütteltrauma zu verstehen? In: Kindler, H., Lillig, S., Blüml, H. (Hrsg.): Handbuch Kindeswohlgefährdung nach § 1666BGB und Allgemeiner Sozialer Dienst (ASD): Internetveröffentlichung des DeutschenJugendinstituts.
Kirjavainen, J., Kirjavainen, T., Huhtala, V.,Lehtonen, L., Korvenranta, H., Kero, P. (2001): Infants with colic have a normal sleepstructure at two and seven months of age. In: Journal of Pediatrics, 138, 218–223.
Lehtonen, L. (1994): Infantile colic. Annalesunniversitatis Turkunensis, Sarja–Ser. D.,Medicaodontologica, 151.
Lehtonen, L., Gormally, S., Barr, R. G. (2000): Clinical pies for etiology and outcome ininfants presenting with early increased crying. In: Barr, R. G, Hopkins, B., Green, J. A. (Eds.): Crying as a sign, a symptom and a signal. London: Mac Keith Press, 67–95.
Miller, A. R., Barr, R. G. (1991): Infantile colic: Is it a gut issue? In: Pediatric Clinics of North America, 38,1407–1423.
Mulder, E. J. H., Robles de Medina, P. G., Huizink, A.C., Van den Bergh, B. R. H., Buitelaar, J. K., Visser, G.H. A. (2002): Prenatal maternal stress: Effects on pregnancyand the unborn child. In: Early Human Development, 70, 3–14.
Murray, L., Cooper, P. J. (1997): The role of infant and maternal factors in post-partum depression, mother-infant interactionsand infant outcomes. In: Murray, L., Cooper, P. J. (Eds.): Postpartum depression and child development. New York, London: The Guilford Press, 111–135.
Olafsdottir, E., Forshei, S., Fluge, G., Markestad, T.(2001): Randomised controlled trial of infantile colic tre-ated with chiropractic spinal manipulation. In: Archives of Disease in Childhood, 84, 138–141.
Papousek, M., Papousek, H. (1990): Excessive infant crying and intuitive parentalcare: buffering support and its failures in parent-infant interaction. In: Early Child Development and Care, 65, 117–126.
Papousek, M., Hofacker, N. v. (1995): Persistent crying and parenting: Search for abutterfly in a dynamic system. In: Early Development and Parenting, 4, 209–224.
Papousek M., Hofacker, N. v. (1996): Infantile colic, state regulation and interactionwith parents: a systems approach. In: Bornstein, M. H., Genevro J. (Eds.): Child development and behavioral pediatrics: towardunderstanding children and health. Hillsdale N. J.: Lawrence Erlbaum.
Papousek M., Hofacker, N. v. (1998): Persistent crying in early infancy: a non trivialcondition of risk for the developing mother-infant relationship. In: Child Care Health Development, 24, 395–424.
Papousek, M. (2004): Regulationsstörungen der frühen Kindheit:Klinische Evidenz für ein neues diagnostischesKonzept. In: Papousek, M., Schieche, M., Wurmser, H. (Hrsg.): Regulationsstörungen der frühen Kindheit. Bern: Huber.
Rautava, P., Helenius, H., Lehtonen, L. (1993): Psychosocial predisposing factors for infantilecolic. In: British Medical Journal, 307, 600–604.
Schaumann, A. (2003): Exzessives Schreien und Schlaf-Wach-Regulationim ersten Lebenshalbjahr. Dissertation. München: LMU München, Medizinische Fakultät.
St. James-Roberts, I., Halil, T. (1991): Infant crying patterns in the first year: Normal community and clinical findings. In: Journal of Child Psychology and Psychiatry, 32,951–968.
St. James-Roberts, I., Hurry, J., Bowyer, J, Barr, R.G. (1995): Supplementary carrying compared with adviceto increase responsive parenting as inter-ventions to prevent persistent crying. In: Pediatrics, 95, 381–388.
St. James-Roberts, I., Conroy, S., Hurry, J. (1997): Links between infant crying and sleep-wakingat 6 week of age. In: Early Human Development, 48, 143–152.
St. James-Roberts, I., Conroy, S., Wilsher, C.(1998a): Stability and outcome of persistent infantcrying. In: Infant Behaviour and Development, 21,411–435.
St. James-Roberts, I., Conroy, S., Wilsher, C.(1998b): Links between maternal care and persistantinfant crying in the early months. In: Child Care Health and Development, 24,353–376.
Thyen, U., Tegtmeyer, F. K. (1991): Das Schütteltrauma des Säuglings – eine besondere Form der Kindesmisshandlung. In: Monatsschrift Kinderheilkunde, 139, 292–296.
Wessel, M. A., Cobb, J. C., Jackson, E. B., Harris,G. S., Detwiler, A. C. (1954): Paroxismal fussing in infancy, sometimes calledcolic. In: Pediatrics, 14, 421–434.
Wurmser, H., Laubereau, B., Hermann, M.,Papousek, M., Kries, R. v. (2001): Excessive infant crying: Often not confined tothe first 3 months of age. In: Early Human Development, 64, 1–6.
Wurmser, H. (2004): Langzeitrisiken persistierenden exzessivenSäuglingsschreiens. In: Papousek, M., Schieche, M., Wurmser, H. (Hrsg.): Regulationsstörungen der frühen Kindheit. Bern: Huber.
Ziegler, M., Wollwerth de Chuquisengo, R.,Papousek, M. (2004): Exzessives Schreien im frühen Säuglingsalter. In: Papousek, M., Schieche, M., Wurmser, H.(Hrsg.): Regulationsstörungen der frühen Kindheit. Bern: Huber.

45
From research and practice
IKK-News 1–2/2005: Violence against children
The service of the FBB as part of thefoster care and adoption services of theyouth office in Hamm was founded in1996 because of the realisation that babiesand infants are overtaxed by being in thecare of youth service institutions, e. g. by the shift work and the changeover ofcaregivers involved. Furthermore, therewas a need for a less costly form of carefor children in crisis situations (Baier-Baran & Laukemper, 2001).
The temporary placement of a childin an FBB during a crisis offers an earlyopportunity for diagnosis and clarificationof prospects within the scope of youthsupport. This is conducive to the pro-tection of the child as well as to the clarifi-cation of the appropriate help measures,be it the return to the biological parents,the arrangement of a full-time adoptivehome, or placement in a suitable insti-tutional home. The specialist personnelof the FBB in Hamm are working in a child-centred fashion. The organisationof support and the cooperation with thebiological parents are in the hands of theGeneral Social Service2.
The target group of the FBB at theyouth office in Hamm is commonly in-fants up to an age of 2.5 years. Themajority of the children accepted since1996 have a family background in whichthey were either neglected or abused byone or both parents.
The age-group up to three especiallyneeds the continuity the family frame-work provides with the particular close-ness, undivided attention, and exclu-siveness it offers.
Long experience showed the impor-tance of an appropriate selection processand the qualification of the care familiesfor the challenging and responsible taskof the FBB (Blüml et al., 2002).
Already at the stage of interviewingfamilies it becomes apparent that manyget interested in the work of the FBBout of a desire to “do something good”.To some women this type of professional
occupation presents an opportunity tocombine their role as mother and house-wife with a new challenge while at thesame time allowing them to remainavailable to their own growing children.
However, what we seek are personali-ties (families or individuals) with peda-gogical training or far-reaching child-rearing experience who see their occupa-tion at the FBB as a professional task,and who meet a specific requirementprofile as well as specific eligibility char-acteristics. Their family history shouldshow stable and sustainable relationships.They should have sufficient living space.The main caregiver should not performan out-of-house occupation. The bio-logical children of the family/individualshould be older than ten years. The care-givers working for the FBB should be avail-able for short-notice fostering of a child.
The following personality traits arerequired: stable personality of one’s own;flexibility and resilience; capacity to dealwith criticism and conflict; willingnessto engage in a consultation and develop-ment process; empathy for the state ofmind of the FBB children; ability to setboundaries and to objectify; toleranceand open-mindedness towards differentframes of reference and ideas about life;preparedness to cooperate with the bio-logical parents and institutions; prepared-ness to participate in further trainingand supervision.
Exemption criteria for the FBB are:personal desire for children; children ofone’s own under the age 10; adoptedchildren living in the home3; profession-al employment of the main caregiver;factors relating to family or personality.
Because the adoption of a child with-in the framework of the FBB is a hugeturning point in the family system andgives rise to considerable transitions inthe family dynamics, a successive, gradualintroduction to the task is necessary.Thus, it is the comprehensive duty of thecare centre “to consistently establish a
balance in the tension between the pri-vateness as a family and the openness as a care system that the youth office asksfor. This task requires a special form ofexpertise, not to act as “employees” but as“private persons” on behalf of the public”(Blüml et al., 2002).
The selection process spans a lengthytime period and takes place in the formof individual as well as family interviews,home visits, and a discussion in groupa session (preparation seminar).
If the applicants match the admissioncriteria, they will then learn about the“everyday world” of the infants to be caredfor and the requirements resulting fromthat regarding the FBB. The training usesa variety of methods for qualification.
Alongside the theoretical backgroundand knowledge4 detailed case studies are considered with the aim of arousingthe applicants’ dismay, which enablesthem to engage more realistically withthe enormous experiences of violencethese children encountered.
Through self-awareness gained withthe help of life review therapy (“What didI need as a child that I did not receive?”),family constellation (Where within thefamily is there space for an “alien” child?),and role plays (“You accompany the childto a visit with the abusive parents – howdoes that affect you?”) etc. the applicantsget an opportunity to find out whetherthey feel equal to the task. Life experiencesof their own that were associated withexpectations, loss, and grief are focusedon, and serve the purpose of bringing
Anke Laukemper
On-call family care1 by the youth office in Hamm as an example of early childhood interventionWhat has proven its worth in practical work? What needs to be considered?
1 Familiäre Bereitschaftsbetreuung (henceforth referred to as FBB)
2 Allgemeiner Sozialer Dienst3 Experiences with younger biological children as
well as foster or adopted children in the FBBshowed that the adoption of a particularly needyinfant can start a non-absorbable dynamic wit-hin the family (e.g. feelings of competition orthe memory of traumatic experiences and fearsof being returned one day) that has negativeconsequences for the foster child.
4 Facts about topics such as child neglect, as wellas physical, psychological and sexual child abuse.

46
From research and practice
IKK-News 1–2/2005: Violence against children
the applicants closer to the upcomingchanges as well as enabling them, asidefrom cognitive engagement, to empathiseemotionally with the emotional state ofthe children in the FBB.
After an appropriate time intervalfollowing the preparation seminar, anevaluation interview is conducted duringwhich the knowledge gained is exchangedand reflected between applicants andexperts of the FBB.
If the applicants decide to act as anon-call foster family, it will come to acooperation if the specialists are convincedthat the applicants, during the training,attained a realistic judgement of theirown resources and the task expected ofthem, and if they are prepared to engagein a permanent learning process.
Experience shows clearly how vitalclose professional guidance of the familiesis at this stage, since the children to beplaced are challenging in a special waydue to their prior experience of abuse,neglect and sexual violence.
It is only during the concrete work thatthe on-call foster family gets a sense ofthe actual misery of these children and,despite all the (theoretical) training, facesnot only emotional dismay, but manynew questions to be answered. This is a particularly demanding situation sincecompetent decision-making and respon-sibility are expected of them. Here, expertsare needed who are available to the fam-ily for advice in order to explain the in-itially incomprehensible behaviour of thechildren from the infant’s point of view.Experience, time, and strong nerves arerequired in order to understand the chil-dren and to ask oneself unflaggingly:what is the infant trying to tell me withits behaviour? A philosophical attitude is very useful, too, as is shown by the caseof Jacqueline. After visiting her biologic-al parents with the on-call foster familythe three year old girl refused to eat forseveral days. The foster mother was veryconcerned and tried repeatedly to en-courage the child to eat. During the ad-vice consultations it was rememberedthat the biological mother had exclaimedwith a raised index finger during thatvisit: “Make sure you eat well, you hearme!”, so that a correlation could be as-sumed between this threat and the girl’sdisturbed eating habit. After the fostermother told Jacqueline understandingly
that she, too, would lose her appetite aft-er such a threat, Jacqueline’s eating habitsnormalised. The little girl felt acknowl-edged and understood in her misery anddid not have to continue calling atten-tion to it by irregular eating behaviour.
Talking about the infant’s perspectivein the training sessions also proves veryeffective for a better understanding of these children. Thus, there are regularpresentations of a psychologist who,among others, works as a consultant fordomestic relations court cases, as anattachment expert, and as a diagnosticianfor traumatised children. Issues such asabuse, neglect, addiction, attachment,separation etc. are considered throughthe eyes of the child. For instance, howdoes a mother’s alcohol consumptionduring pregnancy affect the infant? How does the child experience a drunkand violent father? How does it experi-ence a mother on drugs?
What are the feelings that emerge insuch situations? How does the childexperience the separation of parents whohardly cared for it? How can the indi-vidual attachment relationships of thechild be characterised? How does the childexperience the separation from the on-call foster family?
From our own case studies hypothesesare then drawn about the inner experienceand behaviour of the children on thebasis of general theoretical knowledge –a procedure which results in a sensitisationtowards the behavioural patterns and abetter understanding of the children, andwhich has a positive effect on decision-making and responsibility of the care-givers. It is only when the foster motherrecognises that a child which, as an ex-ample, has a sudden fierce “fit of defiance”in a bakery and, for no apparent reason,screams: “You never give me anything toeat” is experiencing a “transference situa-tion” (Nienstedt & Westermann, 1990)that she will understand that this behav-iour is directed towards the biologicalmother, not the foster mother. This willprevent her from feeling personally hurt(“What are you talking about? That’s nottrue!”) and enable her to resolve the situ-ation empathetically and understanding-ly: “Yes, it’s sad if you are hungry andaren’t given any food.”
Practical exercises such as “How do I talk to the child” promote the sensitivityin dealing with the infants and help thecaregivers to gain more security in theirdaily engagement with the toddler. Insteadof repeatedly asking the child why it didthis or the other, the foster parents learnto formulate “hypotheses”, to “thinkaloud” and to develop a “therapeutic-understanding” rather than an “educative-sanctioning” stance: “Oh, I believe Kevinalways hides my shoes because he’s afraidI will leave the flat without him.”
Along with the growing understand-ing of the children’s irregularities the fos-ter parents develop the competence fordetailed day to day observation which isan important foundation for the furtherorganisation of intervention (Cappen-berg, 2004).
In addition to the counselling offeredregarding the work with the child, care-givers need the environment of thesupervision to talk regularly about theirworries and problems in their role as on-call foster parents (e.g. their own limita-tions), outside of the control of the youthoffice. Experience shows that, whenworking by a “laymen-model” – i. e. withnon-professionals – it is often seen as agreat challenge for foster parents to openup to subjects concerning their personalityand to make the connection betweentheir understanding of their role and theirwork with the children.
Experience also shows that despitetraining and intensive guidance there is a potential for “surprises” on account ofdiverse uncontrollable factors: thus, forinstance, when, after having fostered fivechildren, a long-term foster mother hasthe desire to keep the sixth one as a per-manent foster child, or when marriagesthought to be stable fall into a crisis
Using the example of the On-CallFamily Care (Familiäre Bereitschafts-betreuung, FBB) in Hamm, AnkeLaukemper explains a form of imple-menting this service. A more basicdescription of the FBB, its purposeand its embedding in the children andyouth welfare system can be read inthe IKK-News 2/2001 (only in germanversion).

47
From research and practice
IKK-News 1–2/2005: Violence against children
because of the permanent high pressureinvolved in fostering children, or whenbiological children develop problems in school.
One reason for the enormous pressureis the long-lasting court procedures.Although, in theory, the duration of aninfant’s stay within an on-call foster fam-ily is limited to six months, in practicetheir placement usually extends over ayear or longer. This even applies to casesin which the youth office has alreadydetermined the future of a child withinthe abovementioned period, and is irre-sponsible with respect to the child’s age.
Infants at this age want and need toget attached in order to develop in ahealthy way. However, this attachment isimpossible in an interim situation, becausehere the children keep receiving the sig-nal that they are not going to stay in thisfamily.5 With attachment-theoreticalconsiderations in mind (Bowlby, 2001)the continuance in an on-call foster fam-ily is only maintainable for a short period.As soon as the child exhibits readinessand need for parental objects6, adequateaction needs to be taken (e.g. arrange-ment of a proper foster family).
Proceedings are further delayed whencommissioned expert reports on the fam-ily psychology are not produced withinthe agreed time. A prompt and profession-al workflow is urgently needed! It would be instrumental if judges, law-yers, and guardians ad litem were psycho-logically trained and, in addition to legalprocedures, had the psychological processof child development in mind.
Contact
City of Hamm Youth OfficeFoster Care Service/Adoption Service
Hilmar JankeTelephone: +49 (0)2381/176260
Karin Baier-BaranTelephone: +49 (0)2381/176309
Literature
Baier-Baran, K., Laukemper, A. (2001): Familiäre Bereitschaftsbetreuung. In: Der Oberbürgermeister der Stadt Hamm,Jugendamt/Pflegekinderdienst. FBB-Konzeption. Hamm.
Blüml, H., Helming, E., Lillig, S., Schattner, H. etal. (2000): Psychologische Aspekte von Bindung undTrennung, Risiko- und Schutzfaktoren sowiebiographisch orientierte Arbeitsansätze inder familiären Bereitschaftsbetreuung. In: Zusammenfassung der 6. und 7.Regionaltagungen. München.
Blüml, H., Helming, E., Lillig, S., Schattner, H. etal. (2002): Familiäre Bereitschaftsbetreuung.Abschlussbericht der wissenschaftlichenBegleitung des bundesweiten Modellprojektszur FBB. Stuttgart: Kohlhammer.
Bowlby, J. (2001): Frühe Bindung und kindliche Entwicklung. München: Reinhardt.
Cappenberg, M. (2004): Besuchskontakte vor dem Hintergrund derBindungstheorie: Möglichkeiten und Grenzendieser Theorie, zum Verständnis der Situationvon Pflegekindern beizutragen. In: Stiftung zum Wohl des Pflegekindes (Hrsg.): 3. Jahrbuch des Pflegekinderwesens. Idstein: Schulz-Kirchner Verlag.
Nienstedt, M., Westermann, A. (1990): Pflegekinder. Psychologische Beiträge zurSozialisation von Kindern in Ersatzfamilien. Münster: Votum.
5 Blüml et al., 2000, p.17: “Processing trauma canonly succeed in secure attachment relationships,in other words, not during the interim that theon-call foster family presents.”
6 Nienstedt & Westermann, 1990, p.34: If a childdoes “not allow the mother to care for it, stiffens upon a touch, turns the eyes away whenapproached, or aggressively seeks escape, it is not ready for a relationship or a placement,because the individualised connection with a potential parental object would still be toobeset by fear.”

48 IKK-News 1–2/2005: Violence against children
Project announcement
Prof. Dr. Christian Pfeiffer, Dr. Daniela Hosser, Anna Maier-Pfeiffer, Dr. Tanja Jungmann
Prevention through early childhoodinterventionPilot programme for the preventionof illness, poverty and delinquency of children from socially deprivedfamilies
1. Abbreviated information: main ambition of the pilot projectand its accompanying research
The results of recent research makeevident that severe illnesses as well aspronounced behavioural problems orcriminal careers in adulthood frequentlygo back to the first years in childhood.With regard to illnesses this was recentlypointed out by a longitudinal study of17,000 US-Americans (Felitti, 2002). It showed that psychosocially burdeningexperiences in infancy remain highly ef-fective risk factors even 50 years later.They increase considerably the likeli-hood of severe alcohol abuse, nicotine ordrug addiction, and contribute remarka-bly to subsequent organic illnesses. Thecauses of such pressures can be foundeven further in the past if the mother’spregnancy was characterised by substanceabuse, alcohol consumption, smoking,and malnutrition. Still, government andsociety usually do not intervene untilmore acute problems force action. At thesame time we know from evaluatingmeasures of treatment and interventionthat the later one reacts against illnessesand negative behaviour, the harder theyare to correct. Interventions which startat a very early stage while aiming athigh-risk families whose children are inspecial danger of developing massivehealth problems and of drifting to thesocial margins without the aid of earlychildhood intervention have proven to beparticularly effective and cost-saving.
We have taken initiative together withthe former Minister of Social Affairs ofLower Saxony, Dr. Ursula von der Leyen:for the first time new ways of earlychildhood intervention for children fromsocially disadvantaged families are going
to be tested in Germany within the scopeof a broad-based model experiment. The project is going to start in Hanoverand the surrounding cities Celle, Garbsen,Langenhagen, and Lehrte in spring 2006.The ambition is to offer comprehensivesupport to young families living undermost demanding conditions, especiallysingle mothers with low-income and lowlevel formal education. Preferably fromthe fifth month of pregnancy these youngwomen will be visited at home by familymidwives who will endeavour to encour-age a healthy life style and constructivebirth preparations. After childbirth familyassistants will come by to advise andsupport parents in raising their child, aswell as in their own education and job-seeking. Furthermore, the children willbe systematically promoted in well-managed nurseries and specially designedkindergarten-programmes until theyenrol in school.
Projects of this kind have proven asuccessful path toward lasting preventionof illnesses, criminality, and poverty inthe USA. The first successes of this inter-vention targeted towards preschool-age-groups were evident in their scholasticsuccess. By the age of 15 they had fewerarrests and criminal convictions, smokedand drank less and more rarely had drugproblems than children from the iden-tically composed control group. Themothers also benefited: more often em-ployment could be arranged for them,they more rarely were dependent on socialbenefits, and they had fewer drug andalcohol problems.
Carefully conducted cost-benefit anal-yses show that despite the considerablecosts of such early childhood interventionprogrammes, those measures were alreadypaying off while they were in process.The unsupported children caused farhigher health expenses, and their parentsmore often relied on social benefits.With advancing age the expense differen-tial between both groups only widened:already by the age of 20 every dollar in-vested in the early childhood interventionprogramme saved four dollars in subse-quent consequential costs (Olds et al.,2004). One of these projects – the PerryPreschool Project conducted in Ypsilanti(Michigan, USA) – allows researchers to benefit from 40 years of cost-benefit
analyses (Schweinhart, in print). Onlythis comparison makes it clear that themain effect of early childhood interven-tion is to be expected in adulthood.While the Ypsilanti control group gener-ated high expenses through imprison-ment, drug therapy, hospitalisation, ordependency on social benefits, the groupof 40 year olds supported by early child-hood intervention was dominated bypeople who were employed, paid taxes,had children, and coped well. This paysoff: for every dollar invested in earlychildhood intervention in the 1960s,society gained back 16.6 dollars duringthe course of 34 years.
It is obvious that these findings shouldprompt us to test this successful projecton the basis of a model experiment herein Germany. The enormous costs in-volved can only be justified, of course, if academic monitoring runs alongside theproject. This is the only way to clarifywhether the described programme of earlychildhood intervention has an equallypositive effect in Germany, a country witha comparatively good social welfare sys-tem, as in the USA. It is the only way toexamine in detail what contributes to the success of early intervention and whichmeasures are not to be recommended.Therefore, we are planning comprehensiveacademic monitoring comprising threeaspects. The implementation research isto clarify whether the project can beimplemented as planned, whether thetarget group is reached, and which modi-fications the original concept needs inorder for the project objectives to beattained. The project-efficiency-evaluationlooks into the question whether and towhat extent the project achieves the de-sired results and successes with childrenand their parents, and how the document-ed effects can be explained. The cost-benefits analysis investigates the econom-ic effects of the model test by means of acomparative data analysis of the financialburden generated by the early interven-tion programme, and the costs emergingfrom both groups of children and par-ents during the course of the years. TheKriminologisches Forschungsinstitut Nieder-sachsen e.V. (Criminological ResearchCentre of Lower Saxony) is responsiblefor the first two segments of the academicmonitoring; the cost-benefits analysis is conducted by private lecturer Dr. Peter
Project announcement

49IKK-News 1–2/2005: Violence against children
Lutz, who holds Chair IV of PublicEconomics at the University of Hanover.The costs involved are covered by theHanover-based TUI-Foundation.
2. Project aims of the planned model experiment
Early intervention for socially stressedfamilies has the following four aims:
2.1. Healthy living during pregnancyDuring pregnancy, the health and
psychological stability of the prospectivemother are going to be promoted. Thisinvolves the endeavour to encourage apreferably nicotine-free and alcohol-freelife style, as well as the support in day-to-day issues of life management and theavoidance of severe psychosocial stress.Furthermore, we are aiming at a strongerinvolvement of the father in birth prepa-ration. The ambition, at this stage, is thebirth of a healthy child with a regularbirth weight, to whose well-being bothmother and father feel a commitment.
2.2. Early childhood interventionFirstly, after birth, the emotional at-
tachment between mother and child, andpreferably that between father and child,too, is going to be fostered. We want towork towards healthy nutrition and lovingnurturing of the baby. As the childgrows, we are concerned to support itsphysical, linguistic, and cognitive develop-ment, so that its personality, capacities,and physical maturation can unfold optimally, and the risk of very stressfulillnesses or behavioural irregularities (e.g. ADHD) can be reduced or avoided.
2.3. Promotion of parental child-rearingcompetence and labour integration
A further significant task of the pro-ject is to strengthen the mothers and,where appropriate, the fathers. On onehand, this concerns their child-rearingcompetence. Both are going to be en-couraged to attune positively to theirrole as a parent; this means to accept theburdens associated with the task, to learncorrect parental behaviour, and to dis-cover the joys of parenthood. The neces-sary working knowledge and experiencesfor this are going to be conveyed. On theother hand, we are trying to help the so-cially marginalised mothers (and fathers)
out of their dependency upon social wel-fare in which they are usually caught up.The offer of nursery or day-mother-ser-vices as well as subsequent kindergartenattendance should encourage them to usethe opportunity of full-time child-nurseryto gradually get back on their own twofeet. They will be supported in complet-ing their aborted school education orvocational training, in finding employ-ment, and in earning a regular income.The American experiences make ushopeful that this goal can be achieved formany people over here. We are assumingthat the goal of strengthening the occu-pational and social position of the mother(and, if applicable, the father) will havepositive repercussions on the engagementwith her child.
2.4. Budget savings for municipalities,state, and health insurance funds
Finally, a further ambition of the mod-el experiment it is to reduce noticeablythose expenses that very frequently occurwith high-risk families. This concernsthe health insurance costs during child-hood as much as the high expenses thatare generated by juvenile delinquency,drug addiction, street children, and schooldrop-outs. The early childhood interven-tion project strives for a lasting reductionof the costs to the health insurancesystem, municipalities, councils, and theLänder involved with such negative devel-opment. The American projects havedemonstrated the possible successes ofthis. The pilot project should facilitatethe examination of the question whethersuch an effect is to be expected in Ger-many, a country which, in comparison tothe USA, has a better social welfarestructure. The cost-benefits analyses arenot only going to comprise financial bur-den generated by the supported childrenin contrast to the unsupported, identical-ly composed control group, but alsothose generated for both groups of parents(social benefits, unemployment benefitsetc.). Finally, the efficiency of this supportneeds to be taken into account (e.g. thetax revenue for municipalities and thefederal state resulting from the labourincome of the parents and their childrengrowing up to be employees themselves).
Contact
Criminological Research Center ofLower SaxonyLützerodestraße 9D-30161 Hannover
Telephone: +49 (0)511 /348360Fax: +49 (0)511 /3483610Email: [email protected]
Project announcement

50 IKK-News 1–2/2005: Violence against children
Literature
Bastian, H. G. (2000): Musikerziehung und ihre Wirkung. EineLangzeitstudie an Berliner Grundschulen. Mainz: Schott.
Christiakis, D. A., Zimmerman, F. J., DiGiuseppe, D.L., McCarty, C. A. (2004): Early television exposure and subsequentattentional problems in children. In: Pediatrics, 113, 708–713.
Comby, D. S., Culross, P. L., Behrman, R. E. (1999):Home visiting. Recent program evaluations –analysis and recommendations. In: The Future of Children, 9, 4–24.
Cierpka, M. (2002): FAUSTLOS – ein Curriculum für sozial-emotio-nales Lernen im Kindergarten. Heidelberg: Heidelberger Präventionszentrum.
Dietz, W. H., Gortmaker, S. L. (1985): Do we fatten our children at the television set?Obesity and television viewing in children andadolescents. In: Pediatrics, 75, 807–812.
Elliot, D. (2004): Blueprints. Modellvorlagen zurGewaltprävention. In: DVJJ (Hrsg.): Sonderdruck zum 26. Deutschen Jugendgerichtstag. Hannover: DVJJ.
Huizink, A. C., Robles de Medina, P., Mulder, E. J.H., Visser, G. H. A., Buitelaar, J. K. (2003): Stress during pregnancy is associated withdevelopmental outcome in infancy. In: Journal of Child Psychology and Psychiatry, 44,810–818.
Hüther, G. (1998): Biologie der Angst. Göttingen: Vandenhoeck & Ruprecht.
Hüther, G. (1999): Die Evolution der Liebe. Göttingen: Vandenhoeck & Ruprecht.
Hüther, G. (2002): Die Folgen traumatischer Kindheits-erfahrungen für die weitere Hirnentwicklung.[www.agsp.de/html/a34.html]
Korsten-Reck, U., Kromeyer-Hauschild, K., Korsten,K., Bjarnason-Wehrens, B., Dickhuth, H. H., Berg,A. (2004): Bedeutung des Freizeit- und Ernährungs-verhaltens und der Spezialanamnese in derTherapie der Adipositas bei Kindern. In: Perfusion, 17, 458–464.
Kuschel, A., Hahlweg, K., Miller, Y., Bertram, H.,Heinrichs, N., Saßmann, H. (2003): Universelle Prävention kindlicherVerhaltensstörungen – das Triple P-Programm. In: Lehmkuhl, U. (Hrsg.): Aggressives Verhalten bei Kindern und Jugendlichen.Ursachen, Prävention, Behandlung. Göttingen: Vandenhoeck & Ruprecht, 175–182.
Kuschel, A., Heinrichs, N., Hahlweg, K. (im Druck): Prävention im Vorschulalter. In: Gasteiger Klicpera, B., Julius, H. (Hrsg.): Förderschwerpunkt soziale und emotionale Entwick-lung. Handbuch der Pädagogik und Psychologie beiBehinderungen. Göttingen: Hogrefe.
Lösel, F., Beelman, A., Jaursch, S., Stemmler, M. (2004): Soziale Kompetenz für Kinder und Familien.Ergebnisse der Erlangen-NürnbergerEntwicklungs- und Präventionsstudie. Pressebericht.
Olds, D., Henderson, C. R., Cole, R., Eckenrode, J.,Kitzman, H., Luckey, D., Pettitt, L., Sidora, K., Morris,P., Powers, J. (1998): Long-term effects of Nurse Home Visitation onchildren’s criminal and antisocial behavior. In: The Journal of the American Medical Association,280, 1238–1244.
Olds, D., Henderson, C. R., Kitzman, H., Eckenrode,J. J., Cole, R. E., Tatelbaum, R. C. (1999): Prenatal and infancy home visitation by nurses.Recent findings. In: The Future of Children, 9, 44–63.
Olds, D. L., Kitzman, H., Cole, R., Robinson, J.,Sidora, K., Luckey, D. W., Henderson, C. R., Hanks,C., Bondy, J., Holmberg, J. (2004): Effects of Nurse Home-Visiting on maternal lifecourse and child development. Age 6 follow-upresults of a randomized trial. In: Pediatrics, 114, 1550–1559.
Opstapje – Schritt für Schritt (Hrsg.), Manstetten, M.,Sann, A., Thrum, K. (2004): Opstapje – Schritt für Schritt. Ein innovativesFörderprogramm für 2-jährige Kinder aus sozialbenachteiligten Familien. Vorstellung desModellprogramms und der wissenschaftlichenBegleitung. München: Deutsches Jugendinstitut e.V.
Patry, J.-L., Perrez, M. (2000): Theorie-Praxis-Probleme und die Evaluation vonInterventionsprogrammen. In: Hager, W., Patry, J.-L., Brezig, H. (Hrsg.): Evaluation psychologischer Interventionsmaßnahmen.Göttingen: Huber, 19–40.
Reynolds, A. J. (2000): The State of early intervention. In: Reynolds, A.: Success in early intervention. TheChicago child parent centers. Lincoln, NE: University of Nebraska Press.
Scheithauer, H., Barquero, B. (2005): Papilio. Primärprävention von Verhaltens-problemen und Förderung sozial-emotionalerKompetenz im Kindergarten. Ein Beitrag zurentwicklungsorientierten Sucht- und Gewalt-prävention. Erste Ergebnisse (Kurzfassung) zurEvaluation des Projekts. (www.papilio.de/download/papilio-ergebnisse.pdf )
Schick, A., Cierpka, M. (2004): “FAUSTLOS” – Ein Gewaltpräventions-Curriculum für Grundschulen undKindergärten. In: Melzer, W., Schwind, H.-D. (Hrsg.): Gewaltprävention in der Schule. Baden-Baden: Nomos, 54–66.
Schiffer, K., Ennemoser, M., Schneider, W. (2002): Die Beziehung zwischen dem Fernsehkonsumund der Entwicklung von Sprach- und Lese-kompetenzen im Grundschulalter in Abhängig-keit von der Intelligenz. In: Zeitschrift für Medienpsychologie, 14, 2–13.
Schweinhart, L. J., Barnes, H. V., Weikart, D. P.(1993): Significant benefits. The High/Scope PerryPreschool Study through age 27. Ypsilanti, MI: High/Scope Press.
Schweinhart, L. J. (Eds.) (im Druck): Lifetime effects. The High/Scope PerryPreschool Study through age 40. Ypsilanti, MI: High/Scope Press. [www.highscope.org/Research/PerryProject/PerryAge40SumWeb.pdf ]
Zierau, J., Gonzáles-C., I.-M. (2005): Modellprojekt Aufsuchende Familienhilfe fürjunge Mütter – Netzwerk Familienhebammen.Ergebnisse der Evaluation. Bericht 104.05. Hannover: IES an der Universität Hannover.
Zimmerman, F. J., Glew, G. M., Christiakis, D. A.,Katon, W. (2005): Early cognitive stimulation, emotional support,and television watching as predictors of subse-quent bullying among grade-school children. In: Archives of Pediatrics & Adolescent Medicine,159, 384–388.
Project announcement

51IKK-News 1–2/2005: Violence against children

52 IKK-News 1–2/2005: Violence against children
is a federal interdisciplinary information,advice and network centre supporting theprimary, secondary and tertiary preventionof cruelty and neglect to children. Being a national as well as an internationaljunction between research, practice andpolitics, it promotes the transparency andthe productive teamwork between thevarious fields.
We – your IKK team – access a variety of information and we mutually connectimportant practical experiences withresearch results. Aiming at the develop-ment of demand-oriented preventionwork to protect children from violence,we initiate innovative actions based on extensive interdisciplinary knowledge. We support qualified practical work andencourage practice-oriented researchapproaches.
The information centre is part of theGerman Youth Institute and is financedby the Ministry of Family Affairs, SeniorCitizens, Women and Youth.
The IKKThe following offer concerns all individuals and professional groupscontributing directly or indirectly to the prevention of child abuseor neglect. You may take advantage of it free of charge.
Information about
• Institutions, establishments, (model-)projects, programs• Seminars, events, advanced training and qualification courses• Consultants, experts• Multiprofessional networks• Research results, research methods• Professional literature
Scientific advice at
• Development of innovative needs-based approaches and programs
• Conception of (model-)projects• Development of professional standards and quality features• Development of innovative research approaches• General professional requests
Networking
• Selective networking• Ongoing co-operation with specialized units, institutions
and organisations• Support of interdisciplinary networks
IKK-Homepage
• Literature database• Project database “PraxiPro-IKK” – practical projects
with the aim of preventing violence against children• International calendar of events• Address table of institutions and organisations
Events like
• Conferences• Workshops• Advanced training• Meetings for experts
Publication of
• IKK-News• Professional articles• Expertises• Commented bibliographies• Readers• Handbooks
Our offer
For any questions pleasedo not hesitate to contact us.
Scientific staff
Regine DerrTelephone : +49 (0)89 /62306-285 Email: [email protected]
Beate GalmTelephone: +49 (0)89 /62306-238 Email: [email protected]
Sabine HerzigTelephone : +49 (0)89 /62306-102 Email: [email protected]
Susanna LilligTelephone : +49 (0)89 /62306-184 Email: [email protected]
Literature data baseHelga MenneTelephone : +49 (0)89 /62306-105 Email: [email protected]
OrganisationAnet HolzwigTelephone : +49 (0)89 /62306-229 Email: [email protected]
IKK team
www.dji.de/ikk





























