Embed Size (px)
Citation preview

Current and future options in the
treatment of Uveal Melanoma
Sophie Piperno-Neumann
Institut Curie, Paris, France
27 April 2017

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013
Uveal Melanoma: the disease
and the challenges
Institut Curie SPN, 27 APR 2017
■ Rare tumor: 6 new cases per million per year - up to 50% of patients develop metastases in 2-3 years - via hematogenous spread - liver is the predominant site of relapse in > 80%patients
■ The metastatic risk is the major challenge in UM
BSC systemic immuno/chemotherapy liver surgery OS 2-6 mo 6-12 mo 10-24 mo <25% resectable pts ■ No treatment in the metastatic setting has improved survival No adjuvant treatment capable to prevent (micro)metastases
■ Risk factors for metastasis - Tumor diameter, ciliary body or extraocular spread, epithelioid cell type - Cytogenetics : Monosomy 3 - Genomics (aCGH, FISH, MLPA): Chr 3 chr 8 status are independent variables for metastasis - Gene Expression Profiling : Class 1-low risk/class 2-high risk
Prescher 1996, Onken 2004, Damato 2009, Cassoux 2013

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013
Early detection of metastases
Institut Curie, SPN, 27 APR 2017
■ Retrospective study in 2241 patients (Desjardins, 2006): 5-yr MFS 81% and 5-yr OS 78% (mFU: 6 yrs)
■ International recommendations: 6 monthly liver US for all patients N risk Fu modalities metastatic rate Hicks (1998) 245 all US, Chest Xray, LFTs 22% Eskelin (1999) 390 all US, LFTs 16% COMS (2004) 2320 all LFTs 24%
→No impact on outcome (survival , R0 liver resection rate)
■ NICE 2015 Uveal Melanoma UK National Guidelines (http://melanomafocus.com/) 7 th TNM staging system Prognostic biopsy Multidisciplinary team prognostication and surveillance “Patients judged at high-risk of developing metastases should have 6-monthly life-long surveillance incorporating a clinical review, nurse specialist support and liver-specific imaging by a non-ionising modality. Liver function tests alone are an inadequate tool for surveillance. »
■ High risk patients surveillance
Definition of high risk? no consensus: clinical vs genomic vs GEP? Best imaging modalities? Optimal interval and duration of screening?

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013
Early detection of metastases
Institut Curie, SPN, 27 APR 2017
Marshall et al, BJO 2013 Piperno-Neumann et al, JFO 2015
Primary endpoint
Surveillance methods
detection of asymptomatic liver mets with MRI LFTs and biannual liver MRI
R0 liver resection rate
LFTs and biannual liver MRI
Period Number of patients
2000-2010 188/279 screened
2006-2009 100 /102
High risk definition 5-yr MFS<50% using the Liverpool prognosticator tool on line
large tumors (LTD>15mm or thickness>8mm) or extrascleral extension or M3
Detection of mets before symptoms LFTs MRI
- 92%
- 98%
Genomic risk 97% M3 29% M3 28% M3+8g
Median Follow up (months) Median Metastasis-Free Survival Median OS
29 18 34
49 30 59
Metastatic pts Eligible for liver surgery
90 (48%) 38 (42%)
60 (60%) 25 (42%)
R0 Liver surgery Med OS of R0 pts /metastatic pts (months)
12 (13%) 24/ 12
8 (13%) 40 /14

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
First randomized study 1988-1995 Institut Curie
348 High risk pts
Thickness>5 mm and/or diameter>10 mm
Observation versus DTIC 250 mg/m2 D1-D5 D29, 6 cycles
Endpoints: Overall survival (OS)
Metastasis-Free Survival (MFS)
■ Desjardins et al, 1998 med FU 3 yrs 5-yr OS 70% 68% obs vs 72 % DTIC
■ Piperno-Neumann, 2006 med FU 12.6 yrs
10-yr OS 57% 53% obs vs 62 % DTIC
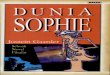
■ March 2007 : Kaplan Meier survival curves in 137 pts with LTD>15 mm
5-yr OS 44% 33% obs vs 55% DTIC
Adjuvant DTIC versus observation for high-risk patients: long-term results
0.0
0.2
0.4
0.6
0.8
1.0
months
percent
OVERALL SURVIVAL & TREATMENT ARM
observationDTIC
0 24 48 72 96 120 144 168 192 216
p=0.05
LTD>15 mm

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
■ Multicentre Randomized Phase III study (EudraCT 2008-005691-27)
■ Adjuvant Fotemustine, 6 cycles, 100 mg/m2 IV 1 h versus observation
■ Primary Objective: Metastasis Free Survival rate
■ Secondary Objectives: Overall Survival, Safety (NCI-CTC v3), quality of life (QLQ- C30)
■ UM patients with high-risk of metastasis, defined by:
Clinical criteria: LTD ≥ 15 mm with extra scleral extension and/or retinal detachment or LTD ≥ 18 mm AND/ OR Genomic high risk signature (aCGH +/-LOH): Monosomy 3 or partial deletion of 3p associated with 8 gain
■ Statistics To improve the 5-Y MFS rate from 50% w/o adjuvant treatment to 70 % with Fotemustine, 302 patients have to be recruited, 99 events are needed to observe the expected benefit with a
type I error of 5% and a power of 95 %. Annual IDMC: no safety concern Interim analysis for futility after 50% of the required target events have been observed
■ Planned treatment period: 20 weeks Follow up period: 3 years (LFTs/3 mo, liver MRI or CT/6 mo, whole body CT/12 mo)
FOTEADJ Study

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
FOTEADJ Study
• Futility analysis: 224 first ® patients (11feb 2016) median FU: 27 months, 2-year MFS: 70.6 %, no chance to observe any significant statistical difference at the end of the study
• IDMC recommendations: - stop randomization - amend the study : « interventional surveillance » in high-risk patients (April 2016) - final analysis: Q1 2017
• FOTEADJ: First adjuvant randomized phase III trial based on genomic analysis. FNA biopsies should precise the rate of genomic high risk in small tumors.
FINAL RESULTS :
ASCO, Melanoma Oral Session, June 4 2017

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013
On going Adjuvant studies
Institut Curie, SPN, 27 APR 2017
Treatment Status Status/Results ClinicalTrials.gov identifier
-Cisplatin, sunitinib, and tamoxifen San Diego
Ph II, 50 clinical high risk pts, May 2007-Dec 2012
unknown no results available
NCT00489944
-Dacarbazine and IFNα2b Cleveland
38 pts, M3 and/or 8q Nov 2009- Mar 2017
active, not recruiting no results available
NCT01100528
-Sunitinib vs valproic acid Thomas Jefferson Univ
R Ph II, class 2 or M3+8q 90 pts, Nov 2014- Feb 2019
recruiting NCT02068586
-Crizotinib MSKCC/Columbia
Ph II, 30 class 2 high risk pts Mar 2015-Aug 2019
recruiting NCT02223819
-Dendritic cells +autologous tumor RNA vaccination University Hospital Erlangen
Ph III, 200 high risk pts (M3) vs observation June 2014-June 2020
recruiting NCT01983748
-mRNA (encoding gp100 and/or tyrosinase)-transfected DC vaccination Radboud University
Ph I/II, recruiting 30 HLA-A2 positive pts M3 June 2009- Apr 2016
terminated (slow accrual)
NCT00929019

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
Effectiveness of Treatments for Metastatic Uveal Melanoma JAMES J. AUGSBURGER, ZÉLIA M. CORRÊA, AND ADEEL H. SHAIKH(Am J Ophthalmol 2009;148:119–127)
▶ 80 identified publications between Jan 1, 1980 and June 30, 2008
12 (15.0%) review articles without original information
2 (2.5%) review articles combined with case reports
22 (27.5%) case reports
16 (20.0%) retrospective descriptive case series reports
3 (3.75%) pilot studies of a novel intervention
2 (2.5%) prospective phase I clinical trials
8 (10.0%) prospective phase I/II clinical trials
15 (18.75%) prospective phase II clinical trials
▶ 25 (30%) prospectives studies
None of these articles reported a randomized phase III clinical trial.
Metastatic UM: published peer-review data

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
Loco-regional: surgery chemo- or immuno-embolization isolated hepatic perfusion intra-arterial hepatic chemotherapy
Systemic: chemotherapy targeted agents immunotherapy
Treatment options for MUM

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
SURGERY-Retrospective series
n R0 resection Median survival (mo)
All pts/ R0 pts
Salmon (1998) 75 20 (27%) 9 22
Rivoire (2005) 63 14 (22%) 15 25
Mariani (2009) 255 76 (29%) 14 27
► Prognostic factors: DFI>24 mo, nb lesions ≤4, no miliary
▶ No prospective comparative study - Optimal preoperative staging?
>2/3 of pts do have more extensive hepatic or extrahepatic disease
- Radiofrequency ablation indications?
- Multimodality cytoreductive strategy?

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
Regional treatment: Hepatic transarterial chemoembolization (TACE)
►
Embolization of the hepatic artery with polyvinyl sponge and cisplatin (2 case reports) C.Humberto Carrasco et al. JAMA 255: 3152-54 1986
drug n Response rate (%) Median survival (mo)
Mavligit 1988 CDDP 30 46% 11
Patel 2005 BCNU 24 21% (1CR+4PR) 5
Vogl 2006 MMC 12 25% (3PR+5SD) 21
Sharma 2008 CDDP/DOX/MMC 20 0% (13 SD) 9

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
Regional treatment: Isolated hepatic perfusion(LPAM)
► Non randomized studies Limited number of patients Treatment-related toxicities are frequent and can be severe Progression of extra hepatic sites despite control of liver metastasis
►Ph III trial comparing IHP with BAC underway (NCT01785316)
n Response Rate (%) Median survival (mo)
Alexander 2000 22 59 11
Alexander 2003 29 62 12
Van Iersel 2008 12 33 12
Van Etten 2009 8 37 11
Olofsson 2014 34 68 24

• Device designed to administer high-dose chemotherapy to the liver while reducing systemic exposure
• Percutaneous Alternative to IHP • 3 procedural steps: Isolation, chemosaturation, filtration • Marketed as Delcath Hepatic CHEMOSAT® Delivery System (device only) in EU/
Investigational drug/device combination product regulated as a drug in the U.S.
Liver Isolated Via Double Balloon Catheter In IVC
Melphalan Infused Directly Into Liver Via Catheter In Hepatic Artery
Blood Exiting The Liver Filtered By Proprietary Extra-corporeal Filters

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
Regional treatment: Percutaneous hepatic perfusion with melphalan (PHP-Mel)► Randomized Phase III study: Chemosaturation-PHP
versus Best Alternative Care (BAC)
▶ Primary Endpoint: hepatic Progression Free Survival(hPFS) Cross-Over of BAC patients at hepatic progression
▶ Secondary Endpoints: Response rate & Duration of Response; Overall Survival;
Safety & Tolerability
▶ Stratification: Cutaneous versus Ocular
▶ Lead Center: National Cancer Institute (NIH), JF Pingpank
▶ Melphalan dose = 3.0 mg/kg
▶ 93 patients: 89% ocular, 41% extrahepatic disease Prior tts:
systemic (chemo- or immunotherapy) 20%
regional (chemo- or radiembolisation, surgery) 9%
▶AE related to bone marrow suppression, 4 deaths attributed to PHP-Mel Hughes et al, Ann Surg Oncol 2016

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
FOCUS: A Randomized, Controlled, Phase 3 Study to Evaluate the Efficacy, Safety and Pharmacokinetics of Melphalan/PHP Treatment in Patients with Hepatic-Dominant Ocular Melanoma vs BAC
.
Parameter FOCUS Study
Conducted 2016-2019
Population Metastatic Ocular Melanoma , mets ≤ 50% tumor burden in the liver
N 240
# of Sites 30 (12 in US; 18 in Western EU)
Primary Endpoint OS
Secondary endpoints PFS, ORR (determined by Investigator)
Exploratory endpoints PFS, ORR, hPFS, hORR (determined by IRC) QoL, PK (sparse and pop), exposure and SAEs
Randomization Cross-over
1:1 No
BAC options DTIC, Ipi, Pembro, TACE
Stratification 1.) Liver burden 2.) Choice of BAC tx prior to randomization
Filters New design built in-house (up to 95% efficiency)

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
Regional treatment: Immunoembolization
LAK cells Keilholz 1994 n=5 no response GM-CSF Sato, 2008 n=34 mOS 14 mo High-Dose Immunoembolization: GM-CSF < 1500 ug versus > 1500 ug versus CE with BCNU
N=53 median OS HDE 20.4 mo LDE 13 mo CE 9.8 mo
Yamamoto et al, Radiology, 252:290-8, 2009
Radioembolization - Yttrium-90 microspheres: (90Y) pure-beta emitter, tissue penetration of 2.5 mm , max range: 1.1 cm
- Pretreated patients series : 9 pts: 1 CR, 6 PR , 1-yr OS: 80% (Kennedy et al., 2009) 20 pts: clinical benefit in 62% , mOS: 10 mo (Gonsalves et al., 2011) 13 pts: 8PR and 2 SD, mOS: 7 mo (Klingenstein et al., 2013)
- On going trials in combination with sorafenib (NCT01893099) or ipilimumab (NCT01730157)

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
Systemic chemotherapyn Response rate
(%)Median PFS (months)
Median OS (months)
Single agent Dacarbazine, Fotemustine, Cisplatin
Temozolomide Bedikian 2004
>50
14
0-19%
0
?
1,8
4-9
-
BOLD-Interferonα Kivela 2003
20 6-14% 1,9 12
Dacarbazine-Treosulfan O’Neill 2006
15 0+2 SD 3 9
Treosulfan-Gemcitabine Schmittel 2005
14: T<3g/m2 19: T>3,5
0+4SD 1PR+10SD
- -
6 9
Treosulfan+/-Gemcitabine Schmittel 2006
24 Treo 24 Treo+G
0+3SD 1PR+7 SD
2 3 p=0.08
- -
Paclitaxel Homsi 2010
22 1PR+7 SD - 9,8

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
Intra arterial chemotherapy-FotemustinRetrospective series n Response rate (%) Median survival (mo)
Leyvraz 1997 31 40 14
Becker 2000 + IL2/IFN 23 22 12
Egerer 2001 7 28 24
Siegel 2006 16 28 22
Peters 2006 101 36 15
Hepatic intra-arterial versus intravenous fotemustine in patients with liver metastases from uveal melanoma (EORTC 18021): a multicentric randomized trial N=171 (2005-2011), mFU: 1,6 yr Stop for futility OS analysis RR : 10,5 vs 2,4% (pS) mPFS:4,5 vs 3,5 mo (pS) mOS: 14,6 vs 13,8 mo (pNS)
S. Leyvraz, S. Piperno-Neumann, S. Suciu, et al, Annals of Oncology 25: 742–746, 2014

Biological potential targets in uveal melanoma
Increased expression
BCL2 (100%)
Cyclin D1 (60%)
HDM2 (100%)
P21 (20%)
pERK (70%)
pAKT (50%)
α5b1(50%)
αvb3 (20%)
MMP-2 (50%)
MMP-9 (50%)
FGF-2 (90%)
VEGF (25%)
E-Cadherin
cMET (86%)
IGFR-1(73%)
cKIT (64%)
Decreased expression
INK4A (30%)
PERP (50%)
GNAQ

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
KIT and antiangiogenic agents
Drug Patients # Response # mPFS/OS months
Remarks/Reference
Imatinib 800 (KIT-inh) 600
13 12
1 SD 1 SD
-/10.8 -/6.8
Penel, 2008 Hofmann, 2009
Sunitinib (PDGFR,VEGFR
and c-KIT inh)
20
Suni vs DTIC 74
1PR, 12 SD
0 vs 8%
4/8
2.8/6.4vs 3.9/ 8.7
Mahipal, 2012
Sacco, ASCO 2013 (stop for futility)
Sorafenib-CarboTXL
(Raf, VEGFR, PDGFR, c-KIT and Flt-3 inh)
24 9 SD 4/11 Bathia, 2012
Bevacizumab (VEGFi)
35 8 SD 3/12 Piperno-Neumann, 2016
Aflibercept (VEGF-Trap)
10 5 SD 5.7/19 Tarhini, 2011 (toxicity)

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
c-MET pathway ► MET signaling stimulates cell growth, invasion and metastasis in many cancer types. Upregulation of MET is a consequence of GNAQ/11 activating mutation present in 80% UM.
► UM models Role of c-Met overexpression and its ligand HGF (Hepatocyte Growth Facto ) in cell migration/metastasis
Crizotinib (ALK and c-MET TKI) - inhibits phospho-Met in vitro - reduces onset of metastasis but seems not sufficient to decrease tumor growth in xenografts (Surriga, 2013)
►Early trials Cabozantinib (MET and VEGF inh) 11 SD/23 MUM pts mPFS/OS: 5/12 mo (Daud, ASCO 13)
→Ph II vs DTIC ongoing (NCT01835145), stop for toxicity

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
GNAQ/11 downstream targets ► GNAQ/11 mutations leads to a cascade activation of phospholipase C, that ends up to a PKC-dependant MEK/ERK/MAPK cascade and PI3K-AKT activation - No small molecules targeting directly the activated domain like BRAF in CM, but rationale for targeting downstream pathways, including MEK and PKC.
► AEB071 (sotrastaurin, Novartis) -Potent, selective oral inhibitor of the classical (α, β), and novel (δ, ε, η, θ) isoforms of PKC, which causes selective growth inhibition through preclinical targeting of PKC/ERK1/2 and PKC/NF-kB pathways (Wu et al., 2012) - Preclinical data : efficacy in 100% mutated UM cell lines (Bastian et al.)

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
Recent trials with MEK/PKC inhibitors
Drug Patients # Response # mPFS/OS months
Remarks/Reference
Trametinib (MEK1/2 inh)
16 (part of Ph I)
8 SD (2mo) 4SD (4 mo)
1.8/- Falchook, 2012
Selumetinib (MEK1/2 inh)
120 Selu vs DTIC
ORR: 14 vs 0% SD: 50 vs 23%
PFS: 4 vs1,7 OS: 11.8 vs 9.1 Carvajal, 2014
AEB071 (sotrastaurin, PKCi)
141 Ph I/II
PR 2% SD 50%
PFS: 3,8 Piperno-Neumann, ASCO 2014
AEB071+Binimetinib (MEK162)
Ph Ib/II (n=38)
May 2015:early termination (combo toxicity)
SUMIT trial Selumetinib+DTIC vs placebo +DTIC
n=129 ® Ph III
(3:1)
3,1 vs 0% PFS: 2,8 vs 1,8 Carvajal, SMR 2015
Trametinib vs Trame+GSK2141795
(AKTi)
Target n=80 ® Ph II
(1:1) US only
ORR: Trametinib: 1/18
(6%) Tram + AKTi: 1/21
(5%)
PFS: 3,925 vs 3,9
Arm B accrual halted Toxicity of the combo led to
frequent dose reductions

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013
On going trials in MUM
Institut Curie, SPN, 27 APR 2017
Treatment Status Status/Results ClinicalTrials.gov identifier
-Selumetinib +Paclitaxel Ph II, 50 pts May 2007-Dec 2012
recruiting EUDRACT: 2014-004437-22
-LXS196 (PKCi 2nd generation) Ph I-II , 100 pts FeB 2016- Dec 2017
recruiting NCT02601378
-Glembatumumab (Antibody-Drug Conjugate CR011)
Ph II, 34 pts Jan 2015- Feb 2017
recruiting NCT02363283
-AEB071 + BYL719 (PI3Ki) Ph Ib, 50 pts Nov 2014-Dec 2018
recruiting NCT02273219
-Cabozantinib vs DTIC ® Ph II, 69 pts June 2013-Nov 2017
Active, not recruiting NCT01835145
-Vorinostat (HDAC i) Ph II, 40 pts Apr 2012- Nov 2017
not recruiting NCT01587352

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
Immunotherapy in Metastatic Uveal Melanoma
Drug Patients # Response # mPFS/OS months
Remarks/Reference
Ipilimumab CTLA4 mab
Retrospective
Prospective
13 39 22 82
53
2 SD 1CR+1PR
1PR 1irPR+24irSD
16 SD
-/8 -/9,6
2,9/5,2 3,6/6
2,8/6,8
Danielli, 2012 Luke, 2013
Telderman, 2013 Maio, 2013
Zimmer, 2015
Tremelimumab
+ IFN α
11
8
0
1 CR, 4 SD
2,9/12,8
-
Joshua, 2015 (stop for futility)
Tarhini, 2011
Nivolumab Pembrolizumab PD-1 inhibitors
8 8
1SD 1CR+2PR 3/-
Weber, 2013 Kottschade, 2016
Adoptive T-cell therapy
(autologous TILs)21
ongoing1 CR+ 6PR - Chandran, 2017

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27APR 2017
- Eye: immune-privileged site, could be responsive to T cell-based immunotherapy
-PDL1 expression in primary UM: 89% PDL1+, 39% high expression (p=40) (Zoroquiain, ARVO 2015)
- Ipilimumab results: <5% objective responses - Nivolumab/Pembrolizumab case reports: 3/7 OR in Kottschade report; 7/8 PD in Weber study concerning ▶ NOT an indication to rush all patients onto antiPD1therapy outside trials
- Ongoing studies - Pool existing data: clinicopath predictive of response (Tsai et al, ASCO 2015) retrospective and prospective study in France: imMUno - Phase 2 Pembrolizumab (NCT02359851) - Phase 2 Nivolumab+ Ipilimumab (NCT01585194) and GEM1402 (NCT02626962) ▶ Need translational correlates: PDL1, serial immunophenotyping of tumors, genomic analyses
UM and immunotherapy

Institut Curie - nom de l’émetteur - Titre de la présentation 03 juin 2013Institut Curie, SPN, 27 APR 2017
- Lack of systemic treatment with OS advantage in UM
- Better understanding of the biology and key signaling pathways
● Identification of deregulated pathways/mutations: driver mutations by WES and RNAseq, epigenetic map of UM models and tumor samples, pathways downstream of GNAQ/GNA11 ● Understanding of UM tropism for the liver and its microenvironment ● Development of relevant metastatic models (i.e. cell lines and PDX) ● Drug sensitivity/efficacy preclinical assays
- Prospective trials based on identification of molecular targets validated in preclinical models
- International collaboration needed International Rare Cancer Initiative (2010): NCRN,CR-UK, NCI, EORTC H2020 grant (2016) EURACAN (2017) : European network for rare adult tumors
Conclusion / Key Messages