Embed Size (px)
Citation preview

Curiosare tra le raccomandazioni delle nuove
linee guida sull’ipertensione arteriosa
Stefano Taddei Dipartimento di Medicina Clinica e Sperimentale
Università di Pisa

2013 ESH/ESC Hypertension Guidelines
2003 Guidelines
2007 Guidelines
2009 Reappraisal ESH
2013 Guidelines
J Hypertens 2013;31:1281-1357
Eur Heart J 2013 June 14
Blood Pressure 2013 June 15
Historical Perspective

Table of contents
2013 ESH/ESC Hypertension Guidelines
1. Introduction
2. Epidemiological aspects
3. Diagnostic evaluation
4. Treatment approach
5. Treatment strategies
6. Treatment strategies in special conditions
7. Treatment of associated risk factors
8. Follow-up
9. Improvement of blood pressure control in hypertension
10. Hypertension disease management
11. Gaps in evidence and need for future trials
Appendix 1
Appendix 2
Acknowledgements
References
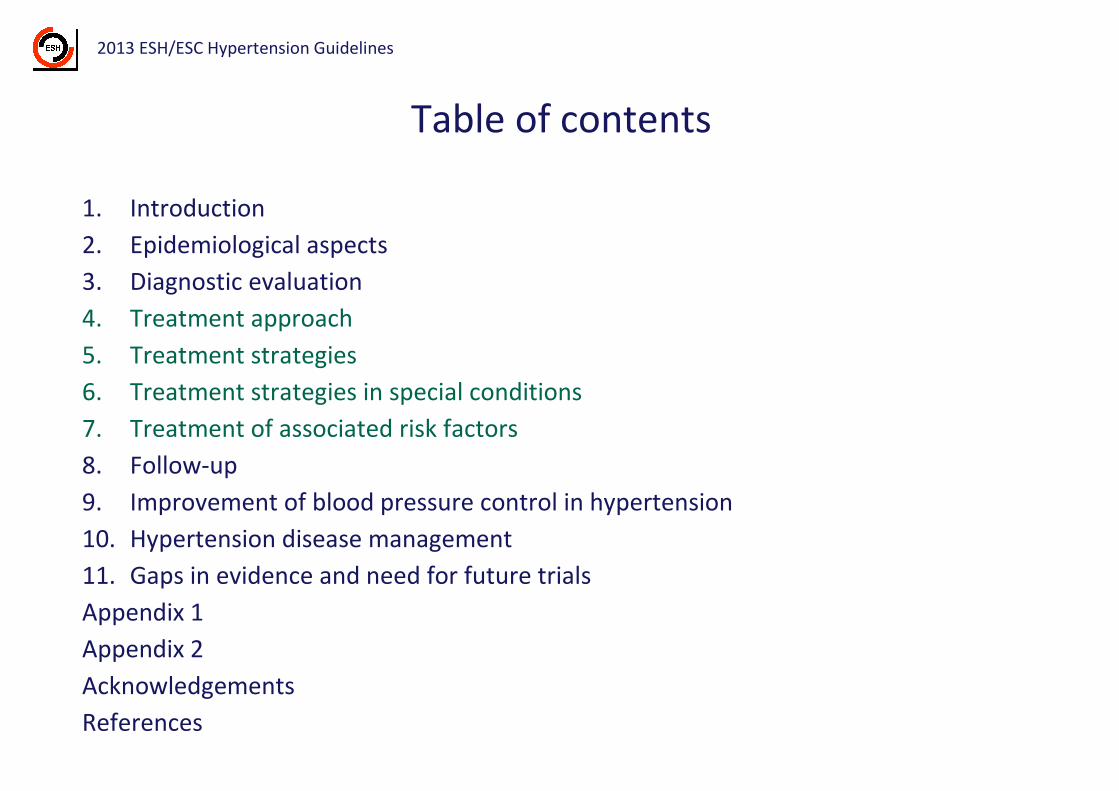
Table of contents
2013 ESH/ESC Hypertension Guidelines
1. Introduction
2. Epidemiological aspects
3. Diagnostic evaluation
4. Treatment approach
5. Treatment strategies
6. Treatment strategies in special conditions
7. Treatment of associated risk factors
8. Follow-up
9. Improvement of blood pressure control in hypertension
10. Hypertension disease management
11. Gaps in evidence and need for future trials
Appendix 1
Appendix 2
Acknowledgements
References

2007 ESH/ESC Hypertension Guidelines
Threshold BP
Target BP
General hypertensive
population
≥ 140/90 mmHg
< 140/90 mmHg
High / very high CV risk
(DM / CVD / CKD)
≥ 130/80 mmHg
< 130/80 mmHg
BP threshold / targets flexible according to CV risk level
142
137
149
138
150
146
140
130
148
130
100
110
120
130
140
150
160
Achieved SBP in “Uncomplicated” HypertensionS
BP
(m
mH
g)
OS HDFP AUS MRC FEV
BP ∆Benefit
Zanchetti, Grassi, Mancia J Hypert 2009; 27: 923 - Mancia et al., J Hypert 2009; 27: 2121
%
130
110
100
120
140
150
160

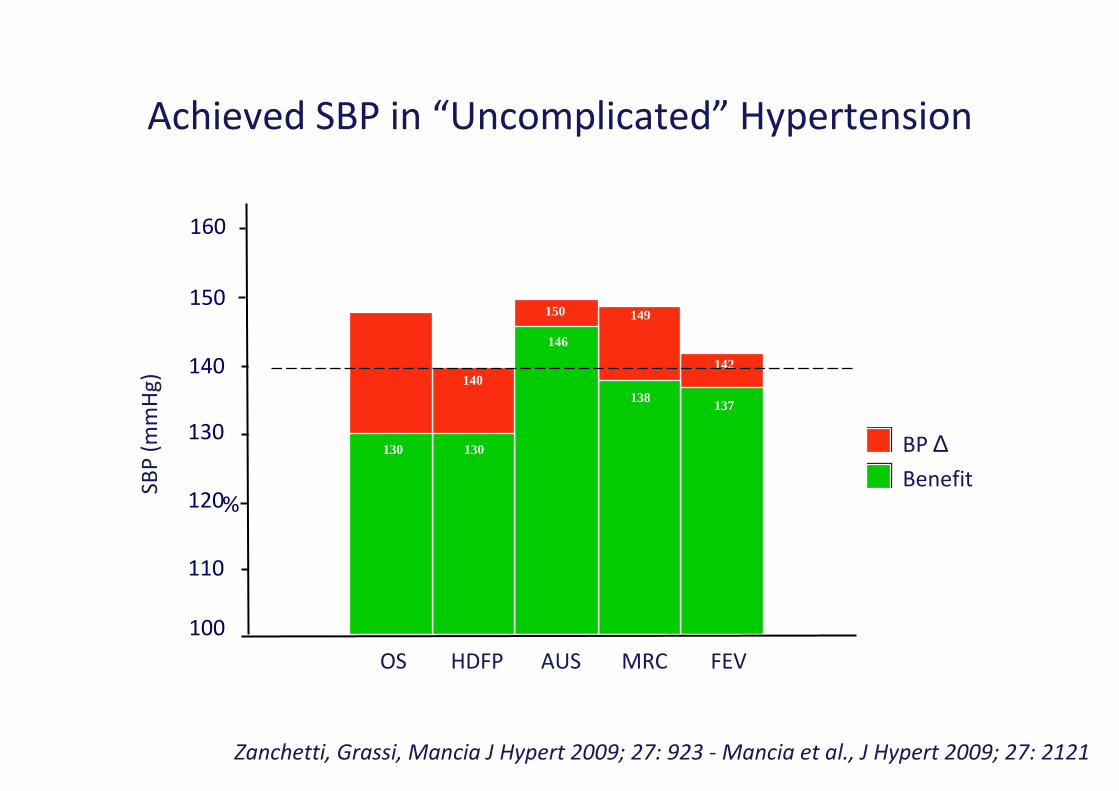
Achieved SBP in Trials
Zanchetti, Grassi, Mancia, J Hypertens 2009; 27: 923-934, Mancia et al., J Hypertens 2009; 27: 2121
133
119
141
143
140
128132
134134
153
139
144145145
110
120
130
140
150
160
170
Diabetes
HOT
SHEP
UKPDS S. Eur ADV ABCD
RENHOPEAM
IDNT
ACRD
NAV
preDM
Benefit No benefit
SB
P (
mm
Hg
)
Active treatment
PROG
HT NT
IDNT

Achieved SBP in Trials
Zanchetti, Grassi, Mancia, J Hypertens 2009; 27: 923-934, Mancia et al., J Hypertens 2009; 27: 2121
133
119
141
143
140
128132
134134
153
139
144145145
110
120
130
140
150
160
170
129
124
130
122
136
124
128
135136
150
132
143
100
110
120
130
140
150
160
Diabetes Previous CVD
PATS
PROG
ACC
PROF
HOPE
EU
CAM-AM PREV
ACT
CAM-EN
PEATR
Stroke CHD
HOT
SHEP
UKPDS S. Eur ADV ABCD
RENHOPEAM
IDNT
SB
P (
mm
Hg
)ACRD
NAV
preDM
Benefit No benefit
SB
P (
mm
Hg
)
Benefit No benefit Benefit No benefit
Active treatment
Active treatment
PROG
HT NT
IDNT

Target SBP < 130 mmHg at high / very high CV risk
2013 ESH/ESC Hypertension Guidelines
• No clear / consistent evidence of CV event reduction also by
subgroup / post-hoc data analysis
• No beneficial effects on risk of ESRD in nephropathic patients
• Although mainly based on post-hoc approach, suspicion of a possible
J curve phenomenon
Blood pressure goals in hypertension
2013 ESH/ESC Hypertension Guidelines2013 ESH/ESC Hypertension Guidelines
• A SBP < 140 mmHg recommended/considered, regardless the level of
risk
• Low/moderate risk (IB)
• Diabetes (IA)
• Diabetic/nondiabetic CKD (IIaB)
• Patients with CHD/previous stroke or TIA (IIaB)
• A DBP < 90 mmHg recommended

Elderly patients
(> 65 - < 80 Years)

Elderly patients
(> 65 - < 80 Years)
Per quali livelli di pressione arteriosa è
raccomandato iniziare il trattamento?

Recruitment BP criteria Mean BP at randomization
Trial SBP
(mmHg)
DBP
(mmHg)
SBP
(mmHg)
DBP
(mmHg)
EWPHE 160-239 or 90-119 183 101
Coope/warrende
r
>170 or >105 196 99
SHEP >160 and <90 170 77
STOP-1 >180 or >105 195 94
MRC-elerly 160-209 and <115 185 91
Syst-Eur 160-219 and <95 174 85
Syst-China 160-219 and <95 171 86
SCOPE* 160-179 or 90-99 166 90
HYVET 160-179 and <110 173 91
YATOS >160 and <120 171 89
*In SCOPE 50% of patients pretreated with low dose thiazides
Zanchetti, Grassi, Mancia, J Hypertens 2009; 27: 923-934
BP at randomization in antihypertensive treatment trials in th elderly

2013 ESH/ESC Hypertension Guidelines
Elderly patients with SBP < 160 mmHg represent a
relevant number in trials showing beneficial effects of
antihypertensive drug treatment

Elderly hypertensive patients
2013 ESH/ESC Hypertension Guidelines
In ELDERLY HYPERTENSIVE PATIENTS drug treatment
• is recommended when SBP ≥ 160 mmHg
• may be considered (in those aged < 80 years) if SBP 140-
159 mmHg, provided treatment is well tolerated
Evidence
Class Level
I A
IIb C

Elderly patients
(> 65 - < 80 Years)
Quali livelli di pressione arteriosa è
raccomandato raggiungere con il
trattamento?

Achieved SBP in Trials
18559a M Zanchetti, Grassi, Mancia, J Hypertens 2009; 27: 923-934, Mancia et al., J Hypertens 2009; 27: 2121
138
145144
151151
156
167
143
162
150
120
130
140
150
160
170
180
190
ElderlyS
BP
(m
mH
g)
EW SHEP MRC S. China SCOPE
CW STOP S. Eur HYVET
JATOS
Benefit No benefit
Active treatment

Incidence of Morbidity / Mortality in HYVETN
o.
of
eve
nts
pe
r 1
00
pa
tie
nts
Total mortality
Fatal stroke
Heart failure
All stroke
0 1 2 3 4
Follow-up (yr)
0 1 2 3 4
Follow-up (yr)
0
1
2
3
4
5
6
7
8
0
1
2
3
4
5
0
10
20
30
1
2
3
4
5
6
7
Placebo
173/91 → 160/84 (mmHg)
Active treatment
173/91 → 144/78 (mmHg)
-30%-39%
-21%-64%p < 0.0001 p = 0.019
p = 0.055 p = 0.046
Goal SBP < 150 mmHg
HYVET - Beckett, NEJM 2008; 358: 10

Target BP in the elderly
2013 ESH/ESC Hypertension Guidelines
• In elderly pts (>65 ys of age) there is solid evidence to recommend
reducing SBP to 150-140 mmHg (IA)
• This is the case also in individuals older than 80 ys, provided they are
in good physical/mental conditions
• Any evidence in favour of lower BP targets?

BP targets in the elderly
2013 ESH/ESC Hypertension Guidelines
“In fit elderly pts <80 ys old a SBP TARGET <140mmHg may be
considered if treatment is well tolerated”
Evidence
Class Level
IIb CC

Choice of antihypertensive drugs -
Conclusions from 2013 (and 2003 and 2007) Guidelines
2013 ESH/ESC Hypertension Guidelines
• The main benefits of antihypertensive treatment are due to lowering BP “per se” and
are largely independent of the drug employed
• Although meta-analyses occasionally claim superiority of one class for some
outcomes this largely depends on selection bias of trials. The largest meta-analyses
do not show clinically relevant between-class differences

Choice of antihypertensive drugs -
Conclusions from 2013 (and 2003 and 2007) Guidelines
2013 ESH/ESC Hypertension Guidelines
• The main benefits of antihypertensive treatment are due to lowering BP “per se” and
are largely independent of the drug employed
• Although meta-analyses occasionally claim superiority of one class for some
outcomes this largely depends on selection bias of trials. The largest meta-analyses
do not show clinically relevant between-class differences
• Current Guidelines reconfirm that the following drugs classes are all suitable for
initiation and maintenance of antihypertensive treatment either as monotherapy or
in some combinations with each other (IA)
• Diuretics (thiazides / chlorthalidone / indapamide)
• Beta-blockers
• Calcium antagonists
• ACE-inhibitors
• Angiotensin receptor blockers
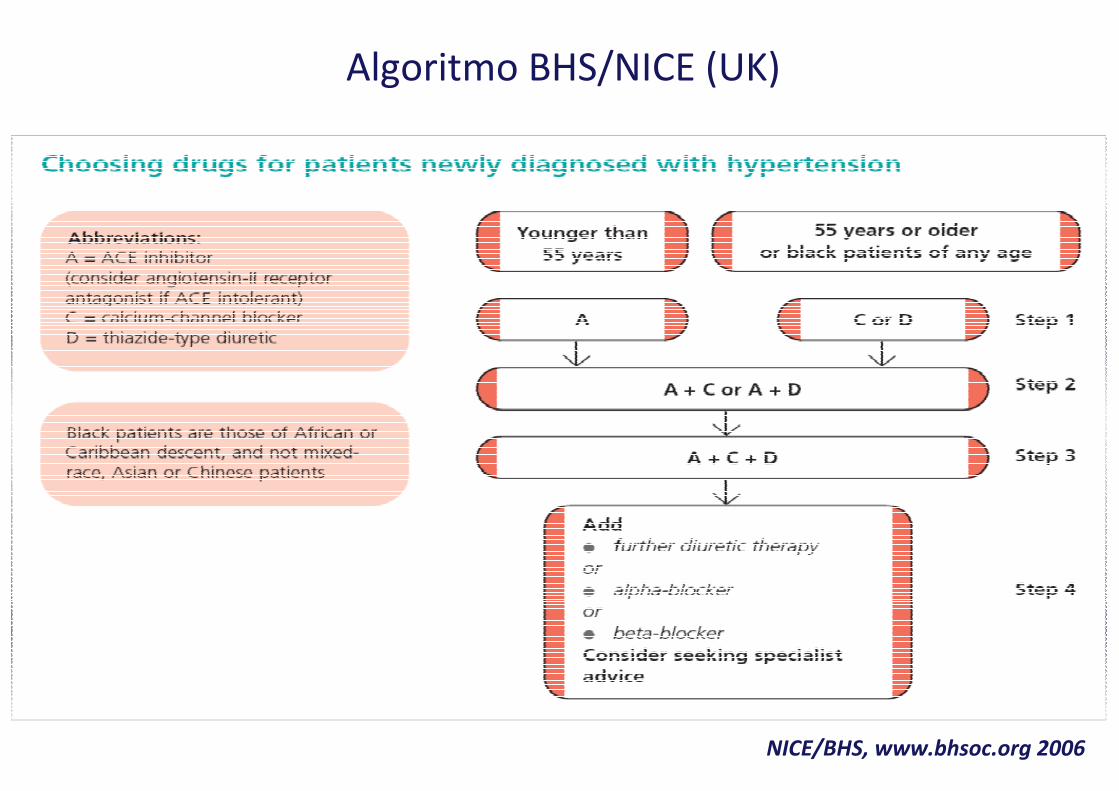
Algoritmo BHS/NICE (UK)
NICE/BHS, www.bhsoc.org 2006
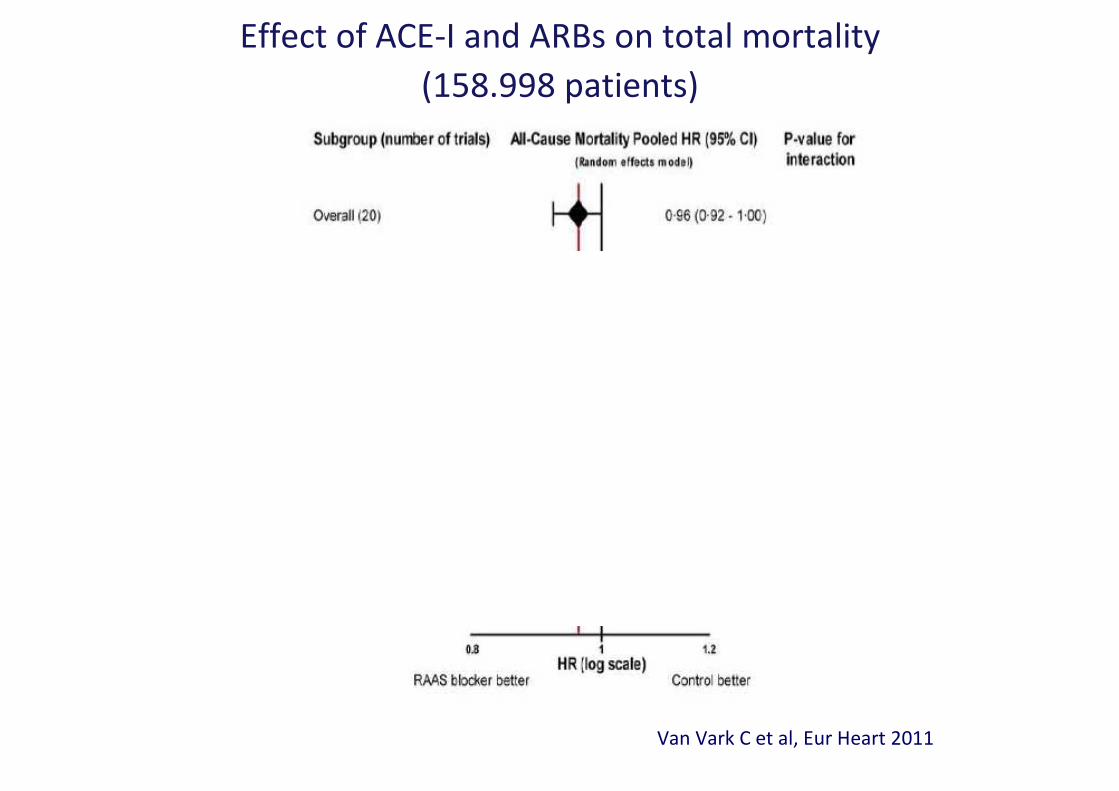
Van Vark C et al, Eur Heart 2011
Effect of ACE-I and ARBs on total mortality
(158.998 patients)
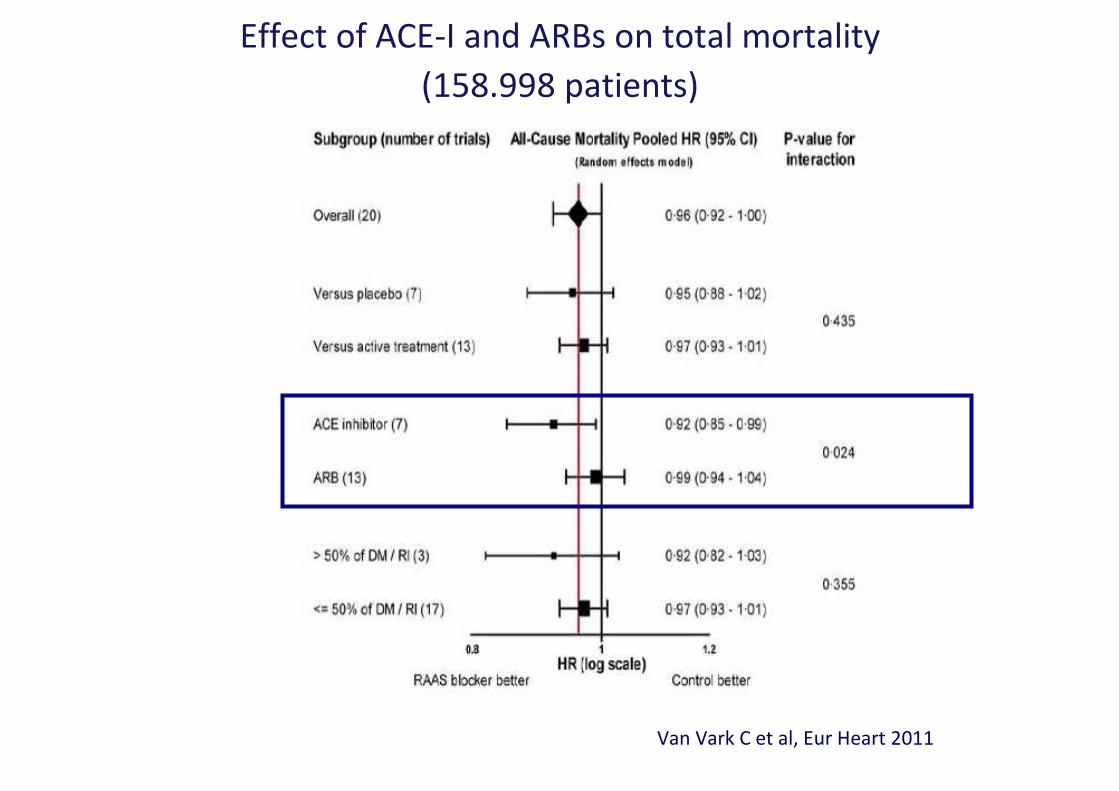
Van Vark C et al, Eur Heart 2011
Effect of ACE-I and ARBs on total mortality
(158.998 patients)

Effect of ACE-Is or ARBs on outcomes
(108.212 patients)
Composite outcome
%
0,11
0,7
0,5
0,9
Cardiovascular death
%
0,11
0,7
0,5
0,9
Myocardial infarction
%
0,11
0,7
0,5
0,9
New heart failure onset
%
0,11
0,7
0,5
0,9
All-cause death
%
0,11
0,7
0,5
0,9
Stroke
%
0,11
0,7
0,5
0,9*
** *
*
New diabetes onset
%
0,11
0,7
0,5
0,9
*
** *
Savarese G et al, JACC 2013
ACE-Is
ARBs
outcome significantly reduced as compared to placebo*

Composite outcome
%
0,11
0,7
0,5
0,9
Cardiovascular death
%
0,11
0,7
0,5
0,9
Myocardial infarction
%
0,11
0,7
0,5
0,9
New heart failure onset
%
0,11
0,7
0,5
0,9
All-cause death
%
0,11
0,7
0,5
0,9
Stroke
%
0,11
0,7
0,5
0,9*
** *
*
New diabetes onset
%
0,11
0,7
0,5
0,9
*
** *
Savarese G et al, JACC 2013
ACE-Is
ARBs
outcome significantly reduced as compared to placebo*
Effect of ACE-Is or ARBs on outcomes
(108.212 patients)


Drugs to be preferred in specific conditions
2013 ESH/ESC Hypertension Guidelines
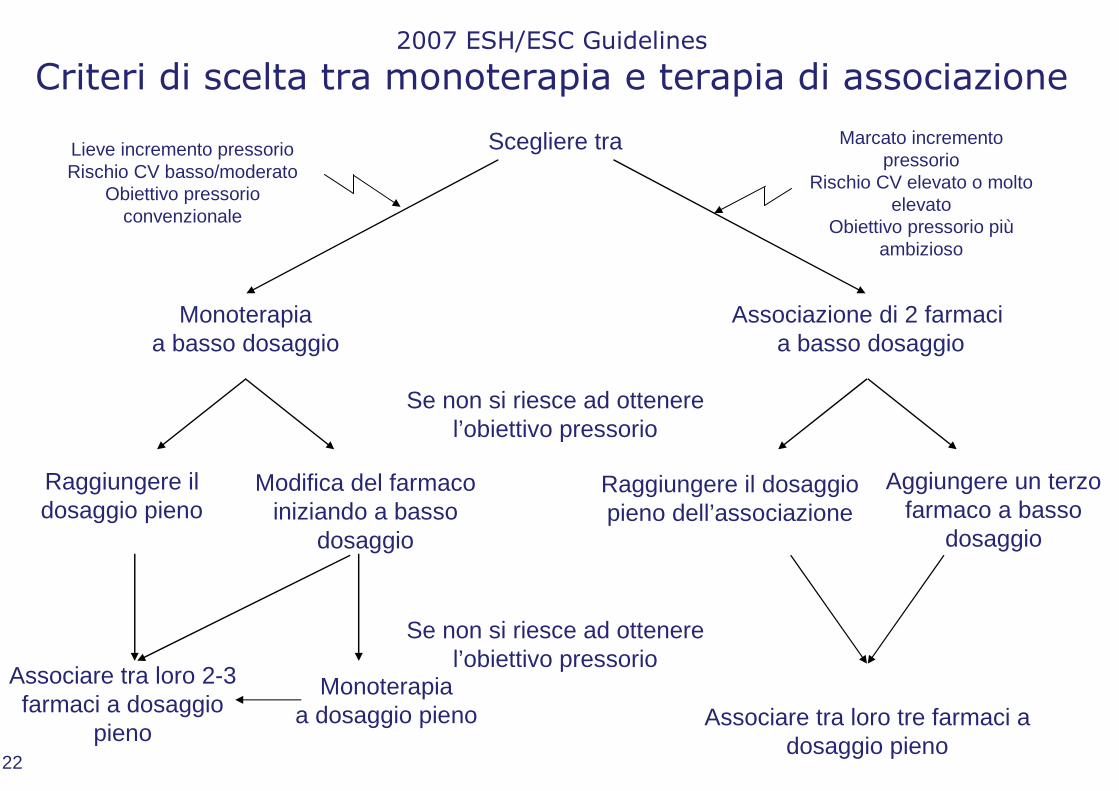
2007 ESH/ESC Guidelines
Criteri di scelta tra monoterapia e terapia di associazione
Scegliere tra
Se non si riesce ad ottenerel’obiettivo pressorio
Se non si riesce ad ottenerel’obiettivo pressorio
Monoterapia a basso dosaggio
Associazione di 2 farmaci a basso dosaggio
Associare tra loro tre farmaci a dosaggio pieno
Raggiungere il dosaggio pieno
Modifica del farmaco iniziando a basso
dosaggio
Raggiungere il dosaggio pieno dell’associazione
Aggiungere un terzo farmaco a basso
dosaggio
Associare tra loro 2-3 farmaci a dosaggio
pieno
Monoterapia a dosaggio pieno
Lieve incremento pressorioRischio CV basso/moderato
Obiettivo pressorio convenzionale
Marcato incremento pressorio
Rischio CV elevato o molto elevato
Obiettivo pressorio piùambizioso
22

2007 ESH/ESC Guidelines
Criteri di scelta tra monoterapia e terapia di associazione
Scegliere tra
Se non si riesce ad ottenerel’obiettivo pressorio
Se non si riesce ad ottenerel’obiettivo pressorio
Monoterapia a basso dosaggio
Associazione di 2 farmaci a basso dosaggio
Associare tra loro tre farmaci a dosaggio pieno
Raggiungere il dosaggio pieno
Modifica del farmaco iniziando a basso
dosaggio
Raggiungere il dosaggio pieno dell’associazione
Aggiungere un terzo farmaco a basso
dosaggio
Associare tra loro 2-3 farmaci a dosaggio
pieno
Monoterapia a dosaggio pieno
Lieve incremento pressorioRischio CV basso/moderato
Obiettivo pressorio convenzionale
Marcato incremento pressorio
Rischio CV elevato o molto elevato
Obiettivo pressorio piùambizioso

Associazioni “omeopatiche”
Ramipril 2.5 mg / HTCZ 12.5 mg
Perindopril 2.5 mg / Indapamide 0.625
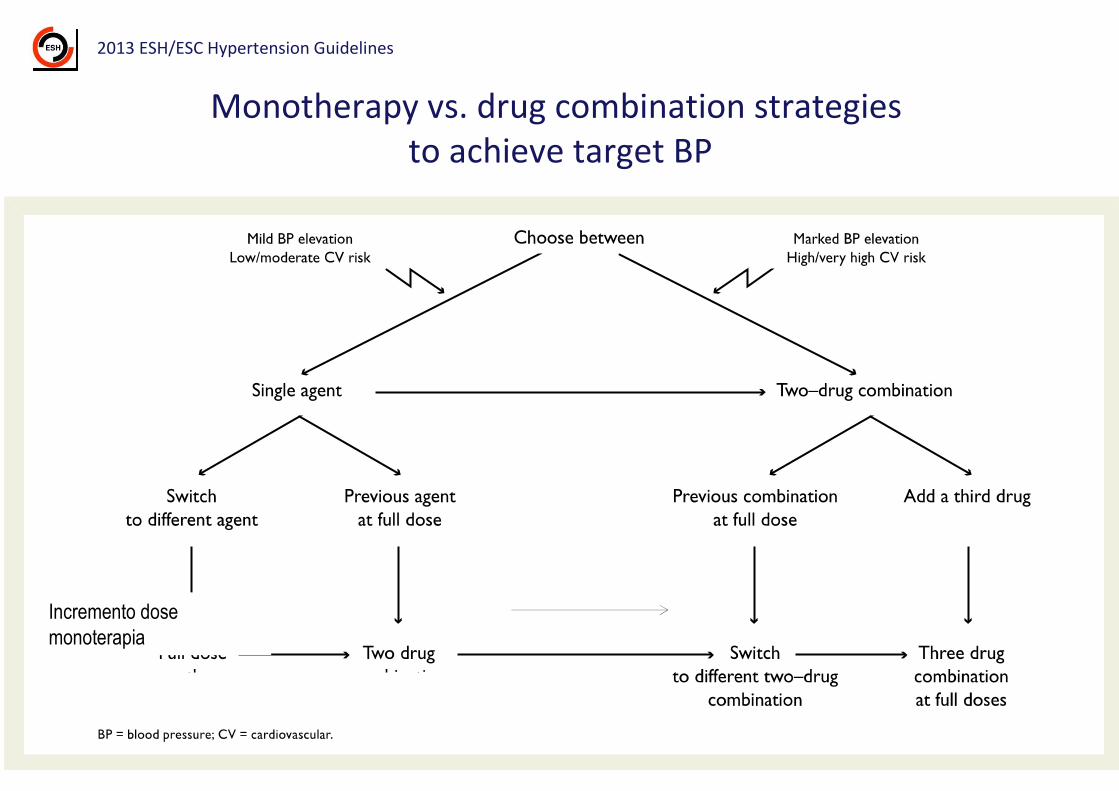
Incremento dose
monoterapia
Monotherapy vs. drug combination strategies
to achieve target BP
2013 ESH/ESC Hypertension Guidelines

Possible combinations of antihypertensive drug classes
2013 ESH/ESC Hypertension Guidelines
Only dihydropyridines to be combined with β-blockers (except for verapamil or diltiazem for rate control in AF)
Thiazides + β-blockers increase risk of new onset DM
ACEI + ARB combination discouraged (IIIA)
Green/continuous: preferred
Green/dashed: useful (with some limitations)
Black/dashed: possible but less well tested
Red/continuous: not recommended

Meccanismi d’ azione dei farmaci antipertensivi
Diuretici
Calcio antagonisti
Alfa-antagonistiSRA
ACE-inibitori
AT-1 antagonisti
Beta-bloccanti
Vasodilatatori SNSACE-inibitori
AT-1 antagonisti
Beta-bloccanti
Simpatomodulatori

VALUE: Disegno dello Studio
Titolazione secondo target pressorio (<140/90 mmHg)
Mese 0.5 0 1 2 3 4 6 * 72
A 10 mg +
HCTZ 25 mg
A 5 mg
A 10 mg +
HCTZ 12.5 mg
A 10 mg
V 80 mg
V 160 mg
V 160 mg +
HCTZ 12.5 mg
V 160 mg +
HCTZ 25 mg
Terapia a base di
Amlodipina
V 160 mg +
HCTZ 25 mg + Agg. “libera"
A 10 mg +
HCTZ 25 mg + Agg. “libera"
Terapia a base di
Valsartan
ScreeningRandomizzazione Fine della fase di
aggiustamento posologico
Randomizzazione
(Pazienti già in
trattamento 92%)
*Visite ai pazienti ogni 6 mesi per 6–72 mesi.
Julius S et al. Lancet. 2004
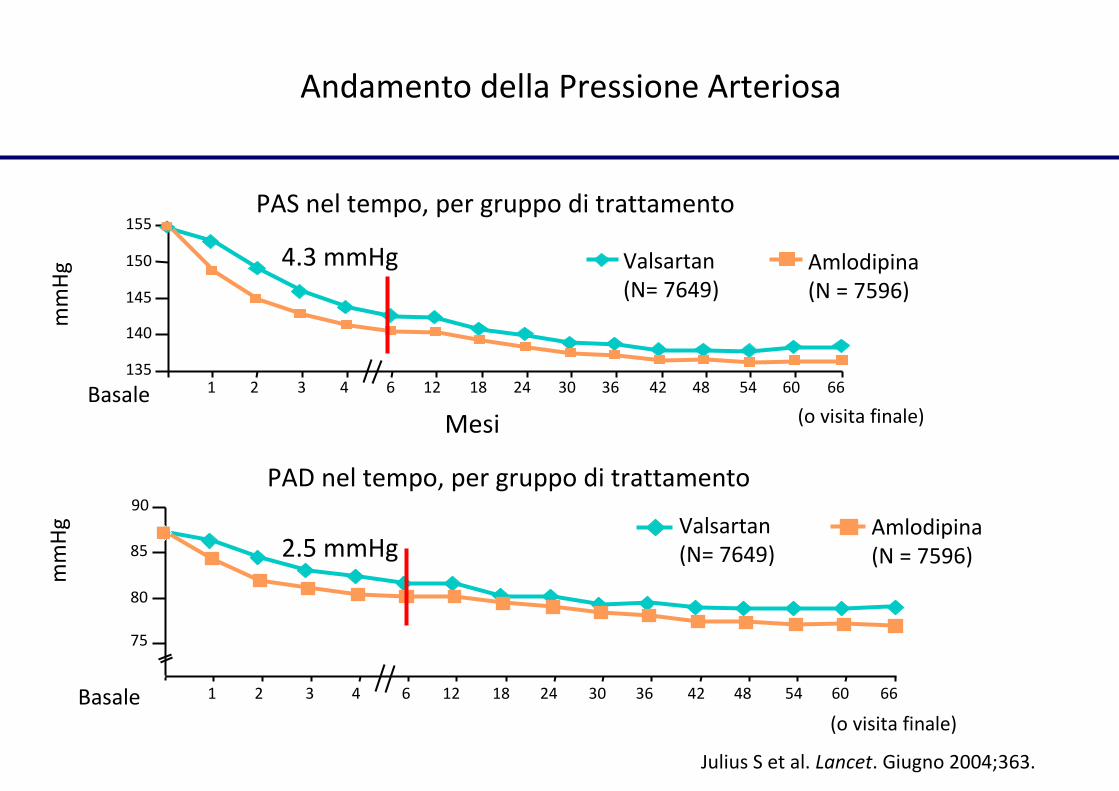
Andamento della Pressione Arteriosa
Valsartan
(N= 7649)
Amlodipina
(N = 7596)
135
140
145
150
155
mm
Hg
Mesi (o visita finale)
PAS nel tempo, per gruppo di trattamento
Basale 1 24 482 3 4 6 12 18 30 36 42 54 60 66
Julius S et al. Lancet. Giugno 2004;363.
Valsartan
(N= 7649)
Amlodipina
(N = 7596)
mm
Hg
(o visita finale)
PAD nel tempo, per gruppo di trattamento
Basale 1 24 482 3 4 6 12 18 30 36 42 54 60 66
75
85
80
90
4.3 mmHg
2.5 mmHg

100
105
110
115
120
PA
me
dia
Placebo Nifedipina Clortalidone Nifedipina+
Clortalidone
107.3±1.2
108.9±0.9108.4±1.1
117.5±1.5
****
*
* p <0.05 vs placebo
Assenza di effetto additivo tra i
Calcio-Antagonisti e i Diuretici
Salvetti et al, J Hypertens 1989

ALLHAT Study
Farmaco
Clortalidone
Amlodipina
Lisinopril
Associazione
Atenololo
Atenololo
Atenololo
Razionale
Razionale
Non razionale
Nello studio ALLHAT il controllo della PA è stato inferiore nel braccio trattato con lisinopril!

RAS Blocker plus CA or Diuretic (D) in ACCOMPLISH
2013 ESH/ESC Hypertension Guidelines
• Only trial comparing two combinations in all patients
• ACEI+D inferior to ACEI+CA despite no BP difference
• Replication desirable because trials on CA-based vs D-based therapy
have never shown a CA superiority
• Further information on which patients benefit more from one or the
other treatment extremely important
Applicazione delle Linee Guida nella
pratica clinica quotidiana
1. Le Linee Guida sono un discreto strumento culturale (un “text book” sull’
ipertensione)
2. La gestione del paziente deve però essere affidata alle qualità cliniche
del medico che sono determinate dalla sapiente unione di: cultura,
esperienza e buon senso.