Embed Size (px)
DESCRIPTION
Cognitive Differences in Dementia Patients With Autopsy-Verified
Citation preview

DOI 10121201WNL000016598789198652005642069-2073 Neurology
M L Kraybill E B Larson D W Tsuang et al AD Lewy body pathology or both
Cognitive differences in dementia patients with autopsy-verified
This information is current as of June 27 2005
httpwwwneurologyorgcontent64122069fullhtmllocated on the World Wide Web at
The online version of this article along with updated information and services is
0028-3878 Online ISSN 1526-632Xsince 1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN
reg is the official journal of the American Academy of Neurology Published continuouslyNeurology
Cognitive differences in dementiapatients with autopsy-verified AD
Lewy body pathology or bothML Kraybill BA EB Larson MD DW Tsuang MSc MD L Teri PhD WC McCormick MD
JD Bowen MD WA Kukull PhD JB Leverenz MD and MM Cherrier PhD
AbstractmdashObjective To examine the neuropsychological profile of dementia patients from a community-based autopsysample of dementia comparing Alzheimer disease (AD) Lewy body pathology (LBP) alone and LBP with coexistent AD(ADLBP) Methods The authors reviewed 135 subjects from a community-based study of dementia for whom autopsy andbrain tissue was available Diagnostic groups were determined according to standard neuropathologic methods andcriteria and the presence of LBs was determined using -synuclein immunostaining Neuropathologically defined diag-nostic groups of AD ADLBP and LBP were examined for differences on neuropsychological test performance at the timeof initial study enrollment Results There were 48 patients with AD alone 65 with LB and AD pathology (ADLBP) and22 with LBP alone (LBP alone) There were no significant differences between groups demographically or on performanceof enrollment Mini-Mental State Examination (MMSE) or Dementia Rating Scale (DRS) AD patients performed worsethan the LBP patients on memory measures (Fuld Object Memory Evaluation Delayed Recall Wechsler Memory ScaleLogical Memory Immediate and Delayed Recall p 005) and a naming task (Consortium to Establish a Registry forAlzheimerrsquos Disease Naming p 005) LBP patients were more impaired than AD patients on executive function (TrailMaking Test Part B p 005) and attention tasks (Wechsler Adult Intelligence ScalendashRevised Digit Span p 005)Decline in MMSE and DRS scores over time were greatest in the patients with ADLBP Conclusions In a community-based sample of older medically complicated patients with dementia there are neuropsychological differences betweendementia subtypes at the time of diagnosis In particular patients with Alzheimer disease (AD) alone and ADLewy bodypathology (LBP) had more severe memory impairment than patients with LBP LBP alone was associated with moresevere executive dysfunction Patients with ADLBP had the most rapid rate of cognitive decline
NEUROLOGY 2005642069ndash2073
It has been suggested that dementia with Lewy bod-ies (LBs) is the second most common form of demen-tia in old age1 The high frequency and extent ofLB-associated pathology in dementia patients has re-cently been confirmed and extended by the use of-synuclein (ASN) immunohistochemistry and sam-pling of regions such as the amygdala2-4 Howeverdespite improved techniques in neuropathologicallyconfirming the presence of LB and associated ASNpathology clinically differentiating between patientswith only LB pathology (LBP alone) Alzheimer dis-ease (AD) alone or AD with LB (ADLBP) remainschallenging This is clinically relevant as there isevidence that these patients may differ in terms ofresponse to medications and prognosis56 In additionit is important to improve the diagnostic accuracy forclinical studies of the LB-associated dementias
Previous studies examining the neuropsychologi-cal characteristics of the LB-associated dementiashave noted that these patients generally demon-
strate more severe impairments in visuoconstructiveand visuospatial abilities working memory atten-tion language initiation and ldquoexecutiverdquo functionswith some evidence of relatively preserved episodicmemory when compared with AD17-15 Howeverthere have been major methodologic problems withthese studies such as using cases without autopsyconfirmation or without the use of ASN and extrani-gral staining Also most studies have not differenti-ated LBP alone from ADLBP In general thesestudies have used patients from highly selected re-search samples which may significantly bias resultsand may not be generalizable to the usually olderand more medically complicated dementia patient inthe general medical community
To address some of these issues we examined theneuropsychological characteristics of patients from alarge community-based sample of older adults withcognitive complaints16 This study examined onlyautopsy-confirmed cases from this sample and uti-
From the Mental Illness Research Education and Clinical Center (Drs Tsuang Leverenz and Cherrier ML Kraybill) Veterans Administration PugetSound Health Care System Seattle and Departments of Medicine (Drs Larson and McCormick) Psychiatry and Behavioral Sciences (Drs TsuangLeverenz and Cherrier) Psychosocial and Community Health (Dr Teri) Neurology (Drs Bowen and Leverenz) and Epidemiology (Dr Kukull) University ofWashington SeattleThe Alzheimerrsquos Disease Patient Registry was supported in part by a grant from the National Institute on Aging (UO1-AG06781)Received September 6 2004 Accepted in final form March 7 2005Address correspondence and reprint requests to Dr MM Cherrier S-116 MIRECC VAPSHCS 1660 S Columbian Way Seattle WA 98108 e-mailcherrieruwashingtonedu
Copyright copy 2005 by AAN Enterprises Inc 2069
lized ASN immunostaining to systematically identifyLBP change We divided cases into three diagnosticgroups (AD LBP alone ADLBP)
Methods Subjects were part of the University of WashingtonGroup Health Cooperative Alzheimerrsquos Disease Patient Registrywhich is a population-based registry of incident dementia cases16
In brief 1028 patients with clinical history of memory and cogni-tive complaints or documented impairments were enrolled from1987 to 1996 Patients underwent a complete standardized diag-nostic workup and neuropsychological evaluation followed by aconsensus diagnosis using National Institute of Neurological andCommunication Disorders and StrokeAlzheimerrsquos Disease andRelated Disorders Association17 and Diagnostic and StatisticalManual for Mental Disorders (3rd rev ed)18 criteria for AD anddementia Patients received annual follow-up consisting of a phys-ical examination and abbreviated neuropsychological evaluationnamely Mini-Mental State Examination (MMSE) and DementiaRating Scale (DRS) To date 291 subjects from this sample havecome to autopsy Of these autopsied cases 135 cases met criteriafor inclusion in the current study One hundred thirty-two caseswere excluded based on insufficient neuropsychological data inad-equate tissue limited AD pathology or advanced dementia atintake
Tests administered at the time of entry included the followingDRS19 Wechsler Memory ScalendashRevised (WMS-R) Logical Mem-ory and Visual Reproduction Subtests20 Fuld Object MemoryEvaluation21 Wechsler Adult Intelligence Scale-Revised (WAIS-R)Digit Span20 WAIS-R Comprehension Subtest20 WAIS-R Proverbitems from Comprehension Subtest20 WAIS-R SimilaritiesSubtest20 WAIS-R Block Design Subtest20 Trail Making Test22
Consortium to Establish a Registry of Alzheimerrsquos Disease(CERAD) Test Battery Naming Subtest23 and MMSE24
Neuropathologic evaluation was performed on specific brainregions including frontal temporal parietal and calcarine cortexcingulate gyrus substantia innominata basal ganglia claustruminsula amygdaloid nucleus hypothalamus hippocampus andparahippocampus midbrain pons medulla and cerebellumBraak staging25 was based on a modified Bielshowsky stain Eval-uation of LBP included hematoxylin and eosin staining in thesubstantia nigra and immunohistochemical staining for ASN (LB509 Zymed San Francisco CA) in the amygdala and substantianigra A blinded assessment (blind to diagnosis Braak stagingand ASN immunostaining in other regions) of ASN-immunostainedsections was performed for the presence or absence of intraneuro-nal ASN-immunopositive inclusions and neurites
Participants were categorized into the following diagnosticgroups AD (Braak stage IV or higher and plaque scores consistentwith CERAD definite AD) ADLBP (AD as above with ASN-positive inclusions in either the amygdala or the substantianigra) LBP alone (Braak stage III or less and ASN-positive inclu-sions in either the amygdala or the substantia nigra) This crite-rion for setting a cut-off score of Braak stage IV for clinically
relevant AD is based on a previous description of neuropathologyin cognitively normal elderly subjects26 Others have suggestedthat the amygdala is the most sensitive region for identifying ASNLB pathology2327 and in this study some subjects in the ADLBPgroup were found to have LB inclusions only in the amygdala andnot in the brainstem (amygdala-only ADLBP) Currently theclinical and pathophysiologic importance of AD with LBP re-stricted to the amygdala alone is unclear (without other brain-stem limbic or neocortical LBP) Therefore in addition to thegroup membership as described above an additional analysis wasperformed with the amygdala-only ADLBP patients excludedfrom the ADLBP group Following neuropathologic diagnosissubsequent analyses were performed on neuropsychological dataobtained at intake Because these diagnostic groups are definedneuropathologically and because this study was started before theconsensus criteria for dementia with LBs clinical data about fluc-tuation parkinsonian features and visual hallucinations were notadequately generated and were not available to analyze Patientswithout AD or LBP were not included in this study and patientswith an MMSE score of 14 at their initial evaluation were ex-cluded to select a population of subjects not already in the latestages of a dementing illness To examine the change in patientsrsquocognitive function over time final MMSE and DRS scores weresubtracted from their initial (entry) scores and divided by years ofobservation Yearly follow-up data from other neuropsychologicaltests were not available for analysis
Results Between-group comparisons for education ageat onset and MMSE and DRS scores at entry to the study(average of 1 year after onset of memory problems) re-vealed no significant differences between groups (table 1)A multivariate analysis of variance (ANOVA) with groups(AD ADLBP and LBP) as the between factor and tests(DRS WMS Logical Memory and Visual ReproductionFuld Object Memory Evaluation WAIS-R Digit SpanWAIR-R Comprehension WAIS-R Similarities WAIS-RBlock Design WAIS-R Proverbs Trail Making TestCERAD Naming and MMSE) as dependent factors wassignificant (F[5 22] 465 p 005) To ensure a largersample size subsequent ANOVAS were performed for eachindividual test
Table 2 displays the means and SE of intake neuropsy-chological test results and change in DRS and MMSE bydiagnostic group AD patients performed worse than LBPpatients on memory measures (Fuld Object Memory De-layed Recall F[190] 404 p 005 WMS Logical Mem-ory Delayed Recall F[212] 1224 p 005) and a verbaltask (CERAD Naming F[2126] 545 p 005) LBPpatients were more impaired than AD patients on an exec-
Table 1 Demographics
AD n 48 ADLBP n 65 LBP n 22 Total n 135
Age at onset mean 7747 734 7477 659 7645 534 7599 675
Sex MF 1830 2441 166 5877
Intake MMSE 2060 387 2068 372 2073 381 2066 376
Education
HS 13 (027) 13 (020) 4 (018) 30 (022)
HS 7 (015) 26 (040) 5 (023) 38 (028)
HS 27 (056) 26 (040) 13 (059) 66 (049)
Duration of disease 603 262 681 252 565 223 616 250
Braak stage 469 059 488 057 214 077 436 116
Sex frequency of male and female patients intake MMSE initial Mini-Mental State Examination score out of 30 HS less thanhigh school HS high school or equivalent HS greater than high school duration of disease age at death minus age of onsetBraak stage mean stage of neurofibrillary tangles
2070 NEUROLOGY 64 June (2 of 2) 2005
utive function task (Trails B Time F[231] 603 p 005) and an attention task (WAIS-R Digit Span F[195] 826 p 005) (see table 2)
A comparison of MMSE and DRS scores over time re-vealed a difference between groups (DRS F[297] 369
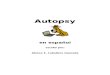
p 005 MMSE F[2116] 344 p 005) with ADLBPpatients demonstrating the greatest degree of change fol-lowed by AD patients and then LBP (figure) The groupsdid not differ in terms of their duration of disease definedas the amount of time that elapsed between age at onset
Table 2 Means and standard errors of intake neuropsychological test results by diagnostic group
AD(Mean SE)
ADLBP(Mean SE)
LBP(Mean SE) p Value
Attention
DRS Attention 344 03 346 03 343 04 089
Trail Making Test Part A 987 112 1003 89 1140 139 067
WAIS-R Digit Span 91 04 82 04 72 05 001
Language
CERAD Naming 69 04 61 03 79 04 001
Memory
DRS Memory 151 06 151 06 175 11 008
Fuld Object Memory Retrieval 176 14 191 14 202 20 056
Fuld Object Memory Del Recall 36 03 43 04 49 05 005
WMS Logical Memory Immediate 31 03 32 03 53 07 000
WMS Logical Memory Delayed 05 01 08 02 24 05 000
WMS Visual Reproduction Immediate 20 03 13 02 16 04 012
WMS Visual Reproduction Delayed 05 02 02 01 03 01 048
Visuo-constructional
DRS Construction 48 02 48 02 47 03 089
WAIS-R Block Design 74 05 72 05 65 05 059
Executive Function
DRS InitiationPerseveration 261 09 267 08 244 13 035
DRS Conceptualization 338 09 331 06 333 11 079
Trail Making Test Part B 1687 181 1838 148 2975 451 001
WAIS-R Comprehension 86 05 86 04 82 06 087
WAIS-R Proverbs 19 03 21 03 12 03 017
WAIS-R Similarities 99 04 88 04 89 06 011
Other
DRS Total 1147 21 1142 18 1142 27 099
MMSE Total 206 06 207 05 207 08 099
Rate of Decline (DRS) points per year 96 15 153 19 88 17 003
Rate of Decline (MMSE) points per year 35 04 50 05 34 07 004dagger
p Values A one-way ANOVA for group difference
dagger This finding is reduced to a statistical trend (p 007) with removal of patients in the ADLBP group who have Lewy body pathologyrestricted to the Amygdala (N 17)
DRS attention subscale 37 points possible Trail Making Test Part A total time in seconds to complete trails test A WAIS-RDigit Span subscale age corrected scaled score CERAD Naming 10 item naming task DRS-Memory subscale 25 points possibleFuld Object Memory Retrieval 50 points possible Fuld Object Memory Delayed Recall 10 points possible WMS-Logical Mem-ory Immediate 50 points possible WMS-Logical Memory Delayed 50 points possible WMS-Visual Reproduction Immediate 41points possible WMS-Visual Reproduction Delayed 41 points possible DRS Construction subscale 6 points possible WAIS-RBlock Design subscale age corrected scaled score DRS-InitiationPerseveration subscale age corrected scaled score DRS-Conceptualization subscale age corrected scaled score Trail Making Test Part B total time in seconds to complete trails BWAIS-R Comprehension subscale age corrected scaled score WAIS-R Comprehension subscale age corrected scaled score WAIS-RSimilarities subscale age corrected scaled score WAIS-R Proverb items taken from comprehension subscale age corrected scaledscore DRS-Total total score of the DRS out of 144 Rate of Decline (DRS) average points per year of decline Rate of Decline(MMSE) average points per year of decline
AD Alzheimer disease LBP Lewy body pathology DRS Dementia Rating Scale WAIS-R Wechsler Adult Intelligence-ScaleRevised CERAD Consortium to Establish a Registry of AD WMS Wechsler Memory Scale MMSE Mini-Mental StateExamination
June (2 of 2) 2005 NEUROLOGY 64 2071
and age at death so it is unlikely that cognitive changeover time was affected by survival rates (p 0315) Al-though we recognize that rate of decline may not have atruly linear progression and may be influenced by factorssuch as education age at diagnosis duration of disease atfirst testing etc this simple calculation of change per yearseems to reflect a more rapid change in general cognitivefunction over time
Because the clinical and pathophysiologic importance ofamygdala-only LB pathology is currently unclear we ex-cluded these cases from our analysis ADLBP patientswith LB inclusions restricted to the amygdala (n 17)were removed from the ADLBP group and ANOVAS asdescribed above were repeated These results were essen-
tially unchanged from those described above (and as notedin figure and table 2) with the exception of MMSE changeover time which was only approaching significance (p 007) To examine whether concomitant diseases or vascu-lar dementia contributed to the findings of unique cogni-tive deficits between groups we reviewed neuropathologyreports and counted the total number of additional find-ings for each subject (eg infarcts lacunes hemorrhageetc) A comparison of this count (a score of 1 for eachadditional event) between groups was not significant
Discussion We used only autopsy-confirmed casesfrom a community-based sample of dementia andused ASN immunohistochemistry and extranigralsampling The number of cases in each group waslarge and the LB-associated dementias were dividedby the presence or absence of significant coexistentAD pathologic change Our results indicate that pa-tients with LBP alone evidence relatively less severeimpairments than patients with AD and ADLBP onmeasures of verbal memory and confrontation nam-ing when mild to moderately demented These find-ings were not due to differences of demographicssuch as age at onset and education or dementia se-verity as the initial MMSE and DRS scores were notsignificantly different between dementia subgroupsConsistent with previous findings patients withLBP alone performed worse than those with AD andADLBP on measures of executive function (Trails B)and attention (WAIS-R Digit Span) Part A of theTrail Making Test did not differ among groupswhich suggests that LBP patients were more im-paired in terms of divided attention and not simplyperforming the task more slowly owing to motorimpairments
Other studies have failed to find cognitive differ-ences between LBP and AD patients at an early dis-ease stage28 LBP patients with high Braak stageratings have been shown to be less likely to expressthe clinical features of LBP29 Thus clinical recogni-tion and differentiation of LBP vs AD can be diffi-cult Consistent with these findings our study alsofound that patients with ADLBP did not differ sig-nificantly from AD patients on any of the neuropsy-chological measures used It is possible that becauseboth groups share a high degree of overlap with re-gard to AD pathology clinical symptoms and cogni-tive differences should they exist may be too subtleto detect with current methods
In terms of cognitive decline patients with ADLBP clearly stood out as having the greatest degreeof change in both the DRS and the MMSE per yearEven when the analysis excluded the patients in theADLBP group where LB inclusions were found onlyin the amygdala there was a significant change inthe DRS per year A greater degree of change incognitive function over time in the ADLBP groupcould be explained as the result of two concomitantdisease processes or that ASN pathology is a markerfor a more aggressive form of AD Other groups havedescribed a rapidly progressive course for patients
Figure (A) Repeated follow-up change in cognitive testingscores (Dementia Rating Scale [DRS]) Change in DRSscores over time Decline (pointsyear) was calculated bysubtracting final scores from initial scores and dividing bythe number of years the patient was followed Patientswith Alzheimer disease (AD)Lewy body pathology (LBP)had a significantly greater rate of decline (p 005) thanboth AD and LBP patients p 005 (B) Repeatedfollow-up change in cognitive testing scores (Mini-MentalState Examination [MMSE]) Change in MMSE scoresover time Decline (pointsyear) was calculated by sub-tracting final scores from initial scores and dividing bythe number of years the patient was followed ADLBP pa-tients had a significantly greater rate of decline (p 005)than both AD and LBP patients p 005 daggerThis findingis reduced to p 007 with the removal of patients in theADLBP group who have LBP restricted to the amygdala
2072 NEUROLOGY 64 June (2 of 2) 2005
with ADLBP830 Our study confirms that finding butemphasizes that it is only the AD cases with LB thathave this more rapid loss of cognitive function re-gardless of the localization of LBP In fact thosecases with LBP alone had the least amount ofchange over time on the MMSE and DRS
It has been suggested that early diagnosis of LBDand differentiation from AD may have therapeuticimplications in terms of avoiding neuroleptic medica-tions5 and the use of cholinesterase inhibitors hasbeen recommended6 Our study provides additionalsupport for the previously described symptoms cog-nitive impairments and functional disabilities thatspecifically characterize LBP and provides furtherevidence for some initial cognitive differences amongthe groups Our study sample is community basedand patients were not excluded based on other dis-ease processes Thus this sample may better repre-sent dementia in the general medical community
Limitations of this study may include selectionbias between patients who elected to participate inthe initial evaluation as well as for those who con-sented for autopsy It is unknown whether these dif-ferences are systematic
References1 McKeith IG Galasko D Kosaka K et al Consensus guidelines for the
clinical and pathologic diagnosis of dementia with Lewy bodies (DLB)report of the Consortium on DLB International Workshop Neurology1996471113ndash1124
2 Hamilton RL Lewy bodies in Alzheimerrsquos disease a neuropathologicalreview of 145 cases using alpha-synuclein immunohistochemistryBrain Pathol 200010378ndash384
3 Lippa CF Fujiwara H Mann DM et al Lewy bodies contain alteredalpha-synuclein in brains of many familial Alzheimerrsquos disease patientswith mutations in presenilin and amyloid precursor protein genesAm J Pathol 19981531365ndash1370
4 Lippa CF Schmidt ML Lee VM Trojanowski JQ Antibodies to alpha-synuclein detect Lewy bodies in many Downrsquos syndrome brains withAlzheimerrsquos disease Ann Neurol 199945353ndash357
5 McKeith I Fairbairn A Perry R Thompson P Perry E Neurolepticsensitivity in patients with senile dementia of Lewy body type BrMed J 1992305673ndash678
6 McKeith I Del Ser T Spano P et al Efficacy of rivastigmine in demen-tia with Lewy bodies a randomised double-blind placebo-controlledinternational study Lancet 20003562031ndash2036
7 Ferman TJ Smith GE Boeve BF et al DLB fluctuations specificfeatures that reliably differentiate DLB from AD and normal agingNeurology 200462181ndash187
8 Heyman A Fillenbaum GG Gearing M et al Comparison of Lewy bodyvariant of Alzheimerrsquos disease with pure Alzheimerrsquos disease Consor-
tium to Establish a Registry for Alzheimerrsquos Disease part XIX Neurol-ogy 1999521839ndash1844
9 Ballard C OrsquoBrien J Gray A et al Attention and fluctuating attentionin patients with dementia with Lewy bodies and Alzheimer diseaseArch Neurol 200158977ndash982
10 Larner AJ MMSE subscores and the diagnosis of dementia with Lewybodies Int J Geriatr Psychiatry 200318855ndash856
11 Noe E Marder K Bell KL Jacobs DM Manly JJ Stern Y Comparisonof dementia with Lewy bodies to Alzheimerrsquos disease and Parkinsonrsquosdisease with dementia Mov Disord 20041960ndash67
12 Pasquier F Early diagnosis of dementia neuropsychology J Neurol19992466ndash15
13 Salmon DP Galasko D Hansen LA et al Neuropsychological deficitsassociated with diffuse Lewy body disease Brain Cogn 199631148ndash165
14 Collerton D Burn D McKeith I OrsquoBrien J Systematic review andmeta-analysis show that dementia with Lewy bodies is a visualndashperceptual and attentionalndashexecutive dementia Dement Geriatr CognDisord 200316229ndash237
15 Hansen L Salmon D Galasko D et al The Lewy body variant ofAlzheimerrsquos disease a clinical and pathologic entity Neurology 1990401ndash8
16 Larson E Kukull W Teri L et al The University of Washington Alz-heimerrsquos Disease Patient Registry (ADPR) 1987ndash1988 Aging 19902404ndash408
17 McKhann G Drachman D Folstein M Katzman R Price D Stadlan EClinical diagnosis of Alzheimerrsquos disease report of the NINCDS-ADRDA Work Group under the auspices of Department of Health andHuman Services Task Force on Alzheimerrsquos Disease Neurology 198434939ndash944
18 American Psychiatric Association Diagnostic and statistical manual ofmental disorders 3rd ed rev Washington DC American PsychiatricPress 1987
19 Mattis S Dementia Rating Scale Odessa FL Psychological Assess-ment Resources 1988
20 Wechsler D Wechsler Adult Intelligence Scale-rRevised manual NewYork Psychological Corp 1981
21 Fuld PA Fuld ObjectndashMemory Evaluation Chicago IL Stoetling 197722 Reitan R Validity of the Trail-Making Test as an indicator of organic
brain damage Percept Mot Skills 198519199ndash20623 Welsh KA Butters N Mohs RC et al The Consortium to Establish a
Registry in Alzheimerrsquos Disease (CERAD) Part V A normative study ofthe neuropsychological battery Neurology 199444609ndash614
24 Folstein MF Folstein SE McHugh PR Mini-Mental State a practicalmethod for grading the cognitive state of patients for the clinicianJ Psychiatr Res 197512189ndash198
25 Braak H Braak E Neuropathological stageing of Alzheimer-relatedchanges Acta Neuropathol 199182239ndash259
26 Knopman DS Parisi JE Salviati A et al Neuropathology of cognitivelynormal elderly J Neuropathol Exp Neurol 2003621087ndash1095
27 Marui W Iseki E Nakai T et al Progression and staging of Lewypathology in brains from patients with dementia with Lewy bodiesJ Neurol Sci 2002195153ndash159
28 Mormont E Laurier-Grymonprez L Baisset-Mouly C Pasquier F Theprofile of memory disturbance in early Lewy body dementia differs fromthat in Alzheimerrsquos disease Rev Neurol (Paris) 2003159762ndash766
29 Merdes AR Hansen LA Jeste DV et al Influence of Alzheimer pathol-ogy on clinical diagnostic accuracy in dementia with Lewy bodies Neu-rology 2003601586ndash1590
30 Olichney JM Galasko D Salmon DP et al Cognitive decline is fasterin Lewy body variant than in Alzheimerrsquos disease Neurology 199851351ndash357
June (2 of 2) 2005 NEUROLOGY 64 2073
DOI 10121201WNL000016598789198652005642069-2073 Neurology
M L Kraybill E B Larson D W Tsuang et al pathology or both
Cognitive differences in dementia patients with autopsy-verified AD Lewy body
This information is current as of June 27 2005
ServicesUpdated Information amp
httpwwwneurologyorgcontent64122069fullhtmlincluding high resolution figures can be found at
References
1httpwwwneurologyorgcontent64122069fullhtmlref-list-at This article cites 25 articles 8 of which you can access for free
Citations
icleshttpwwwneurologyorgcontent64122069fullhtmlotherartThis article has been cited by 11 HighWire-hosted articles
Subspecialty Collections
odieshttpwwwneurologyorgcgicollectiondementia_with_lewy_bDementia with Lewy bodies
httpwwwneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
ehaviorhttpwwwneurologyorgcgicollectionall_neuropsychology_bAll NeuropsychologyBehaviorfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

Cognitive differences in dementiapatients with autopsy-verified AD
Lewy body pathology or bothML Kraybill BA EB Larson MD DW Tsuang MSc MD L Teri PhD WC McCormick MD
JD Bowen MD WA Kukull PhD JB Leverenz MD and MM Cherrier PhD
AbstractmdashObjective To examine the neuropsychological profile of dementia patients from a community-based autopsysample of dementia comparing Alzheimer disease (AD) Lewy body pathology (LBP) alone and LBP with coexistent AD(ADLBP) Methods The authors reviewed 135 subjects from a community-based study of dementia for whom autopsy andbrain tissue was available Diagnostic groups were determined according to standard neuropathologic methods andcriteria and the presence of LBs was determined using -synuclein immunostaining Neuropathologically defined diag-nostic groups of AD ADLBP and LBP were examined for differences on neuropsychological test performance at the timeof initial study enrollment Results There were 48 patients with AD alone 65 with LB and AD pathology (ADLBP) and22 with LBP alone (LBP alone) There were no significant differences between groups demographically or on performanceof enrollment Mini-Mental State Examination (MMSE) or Dementia Rating Scale (DRS) AD patients performed worsethan the LBP patients on memory measures (Fuld Object Memory Evaluation Delayed Recall Wechsler Memory ScaleLogical Memory Immediate and Delayed Recall p 005) and a naming task (Consortium to Establish a Registry forAlzheimerrsquos Disease Naming p 005) LBP patients were more impaired than AD patients on executive function (TrailMaking Test Part B p 005) and attention tasks (Wechsler Adult Intelligence ScalendashRevised Digit Span p 005)Decline in MMSE and DRS scores over time were greatest in the patients with ADLBP Conclusions In a community-based sample of older medically complicated patients with dementia there are neuropsychological differences betweendementia subtypes at the time of diagnosis In particular patients with Alzheimer disease (AD) alone and ADLewy bodypathology (LBP) had more severe memory impairment than patients with LBP LBP alone was associated with moresevere executive dysfunction Patients with ADLBP had the most rapid rate of cognitive decline
NEUROLOGY 2005642069ndash2073
It has been suggested that dementia with Lewy bod-ies (LBs) is the second most common form of demen-tia in old age1 The high frequency and extent ofLB-associated pathology in dementia patients has re-cently been confirmed and extended by the use of-synuclein (ASN) immunohistochemistry and sam-pling of regions such as the amygdala2-4 Howeverdespite improved techniques in neuropathologicallyconfirming the presence of LB and associated ASNpathology clinically differentiating between patientswith only LB pathology (LBP alone) Alzheimer dis-ease (AD) alone or AD with LB (ADLBP) remainschallenging This is clinically relevant as there isevidence that these patients may differ in terms ofresponse to medications and prognosis56 In additionit is important to improve the diagnostic accuracy forclinical studies of the LB-associated dementias
Previous studies examining the neuropsychologi-cal characteristics of the LB-associated dementiashave noted that these patients generally demon-
strate more severe impairments in visuoconstructiveand visuospatial abilities working memory atten-tion language initiation and ldquoexecutiverdquo functionswith some evidence of relatively preserved episodicmemory when compared with AD17-15 Howeverthere have been major methodologic problems withthese studies such as using cases without autopsyconfirmation or without the use of ASN and extrani-gral staining Also most studies have not differenti-ated LBP alone from ADLBP In general thesestudies have used patients from highly selected re-search samples which may significantly bias resultsand may not be generalizable to the usually olderand more medically complicated dementia patient inthe general medical community
To address some of these issues we examined theneuropsychological characteristics of patients from alarge community-based sample of older adults withcognitive complaints16 This study examined onlyautopsy-confirmed cases from this sample and uti-
From the Mental Illness Research Education and Clinical Center (Drs Tsuang Leverenz and Cherrier ML Kraybill) Veterans Administration PugetSound Health Care System Seattle and Departments of Medicine (Drs Larson and McCormick) Psychiatry and Behavioral Sciences (Drs TsuangLeverenz and Cherrier) Psychosocial and Community Health (Dr Teri) Neurology (Drs Bowen and Leverenz) and Epidemiology (Dr Kukull) University ofWashington SeattleThe Alzheimerrsquos Disease Patient Registry was supported in part by a grant from the National Institute on Aging (UO1-AG06781)Received September 6 2004 Accepted in final form March 7 2005Address correspondence and reprint requests to Dr MM Cherrier S-116 MIRECC VAPSHCS 1660 S Columbian Way Seattle WA 98108 e-mailcherrieruwashingtonedu
Copyright copy 2005 by AAN Enterprises Inc 2069
lized ASN immunostaining to systematically identifyLBP change We divided cases into three diagnosticgroups (AD LBP alone ADLBP)
Methods Subjects were part of the University of WashingtonGroup Health Cooperative Alzheimerrsquos Disease Patient Registrywhich is a population-based registry of incident dementia cases16
In brief 1028 patients with clinical history of memory and cogni-tive complaints or documented impairments were enrolled from1987 to 1996 Patients underwent a complete standardized diag-nostic workup and neuropsychological evaluation followed by aconsensus diagnosis using National Institute of Neurological andCommunication Disorders and StrokeAlzheimerrsquos Disease andRelated Disorders Association17 and Diagnostic and StatisticalManual for Mental Disorders (3rd rev ed)18 criteria for AD anddementia Patients received annual follow-up consisting of a phys-ical examination and abbreviated neuropsychological evaluationnamely Mini-Mental State Examination (MMSE) and DementiaRating Scale (DRS) To date 291 subjects from this sample havecome to autopsy Of these autopsied cases 135 cases met criteriafor inclusion in the current study One hundred thirty-two caseswere excluded based on insufficient neuropsychological data inad-equate tissue limited AD pathology or advanced dementia atintake
Tests administered at the time of entry included the followingDRS19 Wechsler Memory ScalendashRevised (WMS-R) Logical Mem-ory and Visual Reproduction Subtests20 Fuld Object MemoryEvaluation21 Wechsler Adult Intelligence Scale-Revised (WAIS-R)Digit Span20 WAIS-R Comprehension Subtest20 WAIS-R Proverbitems from Comprehension Subtest20 WAIS-R SimilaritiesSubtest20 WAIS-R Block Design Subtest20 Trail Making Test22
Consortium to Establish a Registry of Alzheimerrsquos Disease(CERAD) Test Battery Naming Subtest23 and MMSE24
Neuropathologic evaluation was performed on specific brainregions including frontal temporal parietal and calcarine cortexcingulate gyrus substantia innominata basal ganglia claustruminsula amygdaloid nucleus hypothalamus hippocampus andparahippocampus midbrain pons medulla and cerebellumBraak staging25 was based on a modified Bielshowsky stain Eval-uation of LBP included hematoxylin and eosin staining in thesubstantia nigra and immunohistochemical staining for ASN (LB509 Zymed San Francisco CA) in the amygdala and substantianigra A blinded assessment (blind to diagnosis Braak stagingand ASN immunostaining in other regions) of ASN-immunostainedsections was performed for the presence or absence of intraneuro-nal ASN-immunopositive inclusions and neurites
Participants were categorized into the following diagnosticgroups AD (Braak stage IV or higher and plaque scores consistentwith CERAD definite AD) ADLBP (AD as above with ASN-positive inclusions in either the amygdala or the substantianigra) LBP alone (Braak stage III or less and ASN-positive inclu-sions in either the amygdala or the substantia nigra) This crite-rion for setting a cut-off score of Braak stage IV for clinically
relevant AD is based on a previous description of neuropathologyin cognitively normal elderly subjects26 Others have suggestedthat the amygdala is the most sensitive region for identifying ASNLB pathology2327 and in this study some subjects in the ADLBPgroup were found to have LB inclusions only in the amygdala andnot in the brainstem (amygdala-only ADLBP) Currently theclinical and pathophysiologic importance of AD with LBP re-stricted to the amygdala alone is unclear (without other brain-stem limbic or neocortical LBP) Therefore in addition to thegroup membership as described above an additional analysis wasperformed with the amygdala-only ADLBP patients excludedfrom the ADLBP group Following neuropathologic diagnosissubsequent analyses were performed on neuropsychological dataobtained at intake Because these diagnostic groups are definedneuropathologically and because this study was started before theconsensus criteria for dementia with LBs clinical data about fluc-tuation parkinsonian features and visual hallucinations were notadequately generated and were not available to analyze Patientswithout AD or LBP were not included in this study and patientswith an MMSE score of 14 at their initial evaluation were ex-cluded to select a population of subjects not already in the latestages of a dementing illness To examine the change in patientsrsquocognitive function over time final MMSE and DRS scores weresubtracted from their initial (entry) scores and divided by years ofobservation Yearly follow-up data from other neuropsychologicaltests were not available for analysis
Results Between-group comparisons for education ageat onset and MMSE and DRS scores at entry to the study(average of 1 year after onset of memory problems) re-vealed no significant differences between groups (table 1)A multivariate analysis of variance (ANOVA) with groups(AD ADLBP and LBP) as the between factor and tests(DRS WMS Logical Memory and Visual ReproductionFuld Object Memory Evaluation WAIS-R Digit SpanWAIR-R Comprehension WAIS-R Similarities WAIS-RBlock Design WAIS-R Proverbs Trail Making TestCERAD Naming and MMSE) as dependent factors wassignificant (F[5 22] 465 p 005) To ensure a largersample size subsequent ANOVAS were performed for eachindividual test
Table 2 displays the means and SE of intake neuropsy-chological test results and change in DRS and MMSE bydiagnostic group AD patients performed worse than LBPpatients on memory measures (Fuld Object Memory De-layed Recall F[190] 404 p 005 WMS Logical Mem-ory Delayed Recall F[212] 1224 p 005) and a verbaltask (CERAD Naming F[2126] 545 p 005) LBPpatients were more impaired than AD patients on an exec-
Table 1 Demographics
AD n 48 ADLBP n 65 LBP n 22 Total n 135
Age at onset mean 7747 734 7477 659 7645 534 7599 675
Sex MF 1830 2441 166 5877
Intake MMSE 2060 387 2068 372 2073 381 2066 376
Education
HS 13 (027) 13 (020) 4 (018) 30 (022)
HS 7 (015) 26 (040) 5 (023) 38 (028)
HS 27 (056) 26 (040) 13 (059) 66 (049)
Duration of disease 603 262 681 252 565 223 616 250
Braak stage 469 059 488 057 214 077 436 116
Sex frequency of male and female patients intake MMSE initial Mini-Mental State Examination score out of 30 HS less thanhigh school HS high school or equivalent HS greater than high school duration of disease age at death minus age of onsetBraak stage mean stage of neurofibrillary tangles
2070 NEUROLOGY 64 June (2 of 2) 2005
utive function task (Trails B Time F[231] 603 p 005) and an attention task (WAIS-R Digit Span F[195] 826 p 005) (see table 2)
A comparison of MMSE and DRS scores over time re-vealed a difference between groups (DRS F[297] 369
p 005 MMSE F[2116] 344 p 005) with ADLBPpatients demonstrating the greatest degree of change fol-lowed by AD patients and then LBP (figure) The groupsdid not differ in terms of their duration of disease definedas the amount of time that elapsed between age at onset
Table 2 Means and standard errors of intake neuropsychological test results by diagnostic group
AD(Mean SE)
ADLBP(Mean SE)
LBP(Mean SE) p Value
Attention
DRS Attention 344 03 346 03 343 04 089
Trail Making Test Part A 987 112 1003 89 1140 139 067
WAIS-R Digit Span 91 04 82 04 72 05 001
Language
CERAD Naming 69 04 61 03 79 04 001
Memory
DRS Memory 151 06 151 06 175 11 008
Fuld Object Memory Retrieval 176 14 191 14 202 20 056
Fuld Object Memory Del Recall 36 03 43 04 49 05 005
WMS Logical Memory Immediate 31 03 32 03 53 07 000
WMS Logical Memory Delayed 05 01 08 02 24 05 000
WMS Visual Reproduction Immediate 20 03 13 02 16 04 012
WMS Visual Reproduction Delayed 05 02 02 01 03 01 048
Visuo-constructional
DRS Construction 48 02 48 02 47 03 089
WAIS-R Block Design 74 05 72 05 65 05 059
Executive Function
DRS InitiationPerseveration 261 09 267 08 244 13 035
DRS Conceptualization 338 09 331 06 333 11 079
Trail Making Test Part B 1687 181 1838 148 2975 451 001
WAIS-R Comprehension 86 05 86 04 82 06 087
WAIS-R Proverbs 19 03 21 03 12 03 017
WAIS-R Similarities 99 04 88 04 89 06 011
Other
DRS Total 1147 21 1142 18 1142 27 099
MMSE Total 206 06 207 05 207 08 099
Rate of Decline (DRS) points per year 96 15 153 19 88 17 003
Rate of Decline (MMSE) points per year 35 04 50 05 34 07 004dagger
p Values A one-way ANOVA for group difference
dagger This finding is reduced to a statistical trend (p 007) with removal of patients in the ADLBP group who have Lewy body pathologyrestricted to the Amygdala (N 17)
DRS attention subscale 37 points possible Trail Making Test Part A total time in seconds to complete trails test A WAIS-RDigit Span subscale age corrected scaled score CERAD Naming 10 item naming task DRS-Memory subscale 25 points possibleFuld Object Memory Retrieval 50 points possible Fuld Object Memory Delayed Recall 10 points possible WMS-Logical Mem-ory Immediate 50 points possible WMS-Logical Memory Delayed 50 points possible WMS-Visual Reproduction Immediate 41points possible WMS-Visual Reproduction Delayed 41 points possible DRS Construction subscale 6 points possible WAIS-RBlock Design subscale age corrected scaled score DRS-InitiationPerseveration subscale age corrected scaled score DRS-Conceptualization subscale age corrected scaled score Trail Making Test Part B total time in seconds to complete trails BWAIS-R Comprehension subscale age corrected scaled score WAIS-R Comprehension subscale age corrected scaled score WAIS-RSimilarities subscale age corrected scaled score WAIS-R Proverb items taken from comprehension subscale age corrected scaledscore DRS-Total total score of the DRS out of 144 Rate of Decline (DRS) average points per year of decline Rate of Decline(MMSE) average points per year of decline
AD Alzheimer disease LBP Lewy body pathology DRS Dementia Rating Scale WAIS-R Wechsler Adult Intelligence-ScaleRevised CERAD Consortium to Establish a Registry of AD WMS Wechsler Memory Scale MMSE Mini-Mental StateExamination
June (2 of 2) 2005 NEUROLOGY 64 2071
and age at death so it is unlikely that cognitive changeover time was affected by survival rates (p 0315) Al-though we recognize that rate of decline may not have atruly linear progression and may be influenced by factorssuch as education age at diagnosis duration of disease atfirst testing etc this simple calculation of change per yearseems to reflect a more rapid change in general cognitivefunction over time
Because the clinical and pathophysiologic importance ofamygdala-only LB pathology is currently unclear we ex-cluded these cases from our analysis ADLBP patientswith LB inclusions restricted to the amygdala (n 17)were removed from the ADLBP group and ANOVAS asdescribed above were repeated These results were essen-
tially unchanged from those described above (and as notedin figure and table 2) with the exception of MMSE changeover time which was only approaching significance (p 007) To examine whether concomitant diseases or vascu-lar dementia contributed to the findings of unique cogni-tive deficits between groups we reviewed neuropathologyreports and counted the total number of additional find-ings for each subject (eg infarcts lacunes hemorrhageetc) A comparison of this count (a score of 1 for eachadditional event) between groups was not significant
Discussion We used only autopsy-confirmed casesfrom a community-based sample of dementia andused ASN immunohistochemistry and extranigralsampling The number of cases in each group waslarge and the LB-associated dementias were dividedby the presence or absence of significant coexistentAD pathologic change Our results indicate that pa-tients with LBP alone evidence relatively less severeimpairments than patients with AD and ADLBP onmeasures of verbal memory and confrontation nam-ing when mild to moderately demented These find-ings were not due to differences of demographicssuch as age at onset and education or dementia se-verity as the initial MMSE and DRS scores were notsignificantly different between dementia subgroupsConsistent with previous findings patients withLBP alone performed worse than those with AD andADLBP on measures of executive function (Trails B)and attention (WAIS-R Digit Span) Part A of theTrail Making Test did not differ among groupswhich suggests that LBP patients were more im-paired in terms of divided attention and not simplyperforming the task more slowly owing to motorimpairments
Other studies have failed to find cognitive differ-ences between LBP and AD patients at an early dis-ease stage28 LBP patients with high Braak stageratings have been shown to be less likely to expressthe clinical features of LBP29 Thus clinical recogni-tion and differentiation of LBP vs AD can be diffi-cult Consistent with these findings our study alsofound that patients with ADLBP did not differ sig-nificantly from AD patients on any of the neuropsy-chological measures used It is possible that becauseboth groups share a high degree of overlap with re-gard to AD pathology clinical symptoms and cogni-tive differences should they exist may be too subtleto detect with current methods
In terms of cognitive decline patients with ADLBP clearly stood out as having the greatest degreeof change in both the DRS and the MMSE per yearEven when the analysis excluded the patients in theADLBP group where LB inclusions were found onlyin the amygdala there was a significant change inthe DRS per year A greater degree of change incognitive function over time in the ADLBP groupcould be explained as the result of two concomitantdisease processes or that ASN pathology is a markerfor a more aggressive form of AD Other groups havedescribed a rapidly progressive course for patients
Figure (A) Repeated follow-up change in cognitive testingscores (Dementia Rating Scale [DRS]) Change in DRSscores over time Decline (pointsyear) was calculated bysubtracting final scores from initial scores and dividing bythe number of years the patient was followed Patientswith Alzheimer disease (AD)Lewy body pathology (LBP)had a significantly greater rate of decline (p 005) thanboth AD and LBP patients p 005 (B) Repeatedfollow-up change in cognitive testing scores (Mini-MentalState Examination [MMSE]) Change in MMSE scoresover time Decline (pointsyear) was calculated by sub-tracting final scores from initial scores and dividing bythe number of years the patient was followed ADLBP pa-tients had a significantly greater rate of decline (p 005)than both AD and LBP patients p 005 daggerThis findingis reduced to p 007 with the removal of patients in theADLBP group who have LBP restricted to the amygdala
2072 NEUROLOGY 64 June (2 of 2) 2005
with ADLBP830 Our study confirms that finding butemphasizes that it is only the AD cases with LB thathave this more rapid loss of cognitive function re-gardless of the localization of LBP In fact thosecases with LBP alone had the least amount ofchange over time on the MMSE and DRS
It has been suggested that early diagnosis of LBDand differentiation from AD may have therapeuticimplications in terms of avoiding neuroleptic medica-tions5 and the use of cholinesterase inhibitors hasbeen recommended6 Our study provides additionalsupport for the previously described symptoms cog-nitive impairments and functional disabilities thatspecifically characterize LBP and provides furtherevidence for some initial cognitive differences amongthe groups Our study sample is community basedand patients were not excluded based on other dis-ease processes Thus this sample may better repre-sent dementia in the general medical community
Limitations of this study may include selectionbias between patients who elected to participate inthe initial evaluation as well as for those who con-sented for autopsy It is unknown whether these dif-ferences are systematic
References1 McKeith IG Galasko D Kosaka K et al Consensus guidelines for the
clinical and pathologic diagnosis of dementia with Lewy bodies (DLB)report of the Consortium on DLB International Workshop Neurology1996471113ndash1124
2 Hamilton RL Lewy bodies in Alzheimerrsquos disease a neuropathologicalreview of 145 cases using alpha-synuclein immunohistochemistryBrain Pathol 200010378ndash384
3 Lippa CF Fujiwara H Mann DM et al Lewy bodies contain alteredalpha-synuclein in brains of many familial Alzheimerrsquos disease patientswith mutations in presenilin and amyloid precursor protein genesAm J Pathol 19981531365ndash1370
4 Lippa CF Schmidt ML Lee VM Trojanowski JQ Antibodies to alpha-synuclein detect Lewy bodies in many Downrsquos syndrome brains withAlzheimerrsquos disease Ann Neurol 199945353ndash357
5 McKeith I Fairbairn A Perry R Thompson P Perry E Neurolepticsensitivity in patients with senile dementia of Lewy body type BrMed J 1992305673ndash678
6 McKeith I Del Ser T Spano P et al Efficacy of rivastigmine in demen-tia with Lewy bodies a randomised double-blind placebo-controlledinternational study Lancet 20003562031ndash2036
7 Ferman TJ Smith GE Boeve BF et al DLB fluctuations specificfeatures that reliably differentiate DLB from AD and normal agingNeurology 200462181ndash187
8 Heyman A Fillenbaum GG Gearing M et al Comparison of Lewy bodyvariant of Alzheimerrsquos disease with pure Alzheimerrsquos disease Consor-
tium to Establish a Registry for Alzheimerrsquos Disease part XIX Neurol-ogy 1999521839ndash1844
9 Ballard C OrsquoBrien J Gray A et al Attention and fluctuating attentionin patients with dementia with Lewy bodies and Alzheimer diseaseArch Neurol 200158977ndash982
10 Larner AJ MMSE subscores and the diagnosis of dementia with Lewybodies Int J Geriatr Psychiatry 200318855ndash856
11 Noe E Marder K Bell KL Jacobs DM Manly JJ Stern Y Comparisonof dementia with Lewy bodies to Alzheimerrsquos disease and Parkinsonrsquosdisease with dementia Mov Disord 20041960ndash67
12 Pasquier F Early diagnosis of dementia neuropsychology J Neurol19992466ndash15
13 Salmon DP Galasko D Hansen LA et al Neuropsychological deficitsassociated with diffuse Lewy body disease Brain Cogn 199631148ndash165
14 Collerton D Burn D McKeith I OrsquoBrien J Systematic review andmeta-analysis show that dementia with Lewy bodies is a visualndashperceptual and attentionalndashexecutive dementia Dement Geriatr CognDisord 200316229ndash237
15 Hansen L Salmon D Galasko D et al The Lewy body variant ofAlzheimerrsquos disease a clinical and pathologic entity Neurology 1990401ndash8
16 Larson E Kukull W Teri L et al The University of Washington Alz-heimerrsquos Disease Patient Registry (ADPR) 1987ndash1988 Aging 19902404ndash408
17 McKhann G Drachman D Folstein M Katzman R Price D Stadlan EClinical diagnosis of Alzheimerrsquos disease report of the NINCDS-ADRDA Work Group under the auspices of Department of Health andHuman Services Task Force on Alzheimerrsquos Disease Neurology 198434939ndash944
18 American Psychiatric Association Diagnostic and statistical manual ofmental disorders 3rd ed rev Washington DC American PsychiatricPress 1987
19 Mattis S Dementia Rating Scale Odessa FL Psychological Assess-ment Resources 1988
20 Wechsler D Wechsler Adult Intelligence Scale-rRevised manual NewYork Psychological Corp 1981
21 Fuld PA Fuld ObjectndashMemory Evaluation Chicago IL Stoetling 197722 Reitan R Validity of the Trail-Making Test as an indicator of organic
brain damage Percept Mot Skills 198519199ndash20623 Welsh KA Butters N Mohs RC et al The Consortium to Establish a
Registry in Alzheimerrsquos Disease (CERAD) Part V A normative study ofthe neuropsychological battery Neurology 199444609ndash614
24 Folstein MF Folstein SE McHugh PR Mini-Mental State a practicalmethod for grading the cognitive state of patients for the clinicianJ Psychiatr Res 197512189ndash198
25 Braak H Braak E Neuropathological stageing of Alzheimer-relatedchanges Acta Neuropathol 199182239ndash259
26 Knopman DS Parisi JE Salviati A et al Neuropathology of cognitivelynormal elderly J Neuropathol Exp Neurol 2003621087ndash1095
27 Marui W Iseki E Nakai T et al Progression and staging of Lewypathology in brains from patients with dementia with Lewy bodiesJ Neurol Sci 2002195153ndash159
28 Mormont E Laurier-Grymonprez L Baisset-Mouly C Pasquier F Theprofile of memory disturbance in early Lewy body dementia differs fromthat in Alzheimerrsquos disease Rev Neurol (Paris) 2003159762ndash766
29 Merdes AR Hansen LA Jeste DV et al Influence of Alzheimer pathol-ogy on clinical diagnostic accuracy in dementia with Lewy bodies Neu-rology 2003601586ndash1590
30 Olichney JM Galasko D Salmon DP et al Cognitive decline is fasterin Lewy body variant than in Alzheimerrsquos disease Neurology 199851351ndash357
June (2 of 2) 2005 NEUROLOGY 64 2073
DOI 10121201WNL000016598789198652005642069-2073 Neurology
M L Kraybill E B Larson D W Tsuang et al pathology or both
Cognitive differences in dementia patients with autopsy-verified AD Lewy body
This information is current as of June 27 2005
ServicesUpdated Information amp
httpwwwneurologyorgcontent64122069fullhtmlincluding high resolution figures can be found at
References
1httpwwwneurologyorgcontent64122069fullhtmlref-list-at This article cites 25 articles 8 of which you can access for free
Citations
icleshttpwwwneurologyorgcontent64122069fullhtmlotherartThis article has been cited by 11 HighWire-hosted articles
Subspecialty Collections
odieshttpwwwneurologyorgcgicollectiondementia_with_lewy_bDementia with Lewy bodies
httpwwwneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
ehaviorhttpwwwneurologyorgcgicollectionall_neuropsychology_bAll NeuropsychologyBehaviorfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

lized ASN immunostaining to systematically identifyLBP change We divided cases into three diagnosticgroups (AD LBP alone ADLBP)
Methods Subjects were part of the University of WashingtonGroup Health Cooperative Alzheimerrsquos Disease Patient Registrywhich is a population-based registry of incident dementia cases16
In brief 1028 patients with clinical history of memory and cogni-tive complaints or documented impairments were enrolled from1987 to 1996 Patients underwent a complete standardized diag-nostic workup and neuropsychological evaluation followed by aconsensus diagnosis using National Institute of Neurological andCommunication Disorders and StrokeAlzheimerrsquos Disease andRelated Disorders Association17 and Diagnostic and StatisticalManual for Mental Disorders (3rd rev ed)18 criteria for AD anddementia Patients received annual follow-up consisting of a phys-ical examination and abbreviated neuropsychological evaluationnamely Mini-Mental State Examination (MMSE) and DementiaRating Scale (DRS) To date 291 subjects from this sample havecome to autopsy Of these autopsied cases 135 cases met criteriafor inclusion in the current study One hundred thirty-two caseswere excluded based on insufficient neuropsychological data inad-equate tissue limited AD pathology or advanced dementia atintake
Tests administered at the time of entry included the followingDRS19 Wechsler Memory ScalendashRevised (WMS-R) Logical Mem-ory and Visual Reproduction Subtests20 Fuld Object MemoryEvaluation21 Wechsler Adult Intelligence Scale-Revised (WAIS-R)Digit Span20 WAIS-R Comprehension Subtest20 WAIS-R Proverbitems from Comprehension Subtest20 WAIS-R SimilaritiesSubtest20 WAIS-R Block Design Subtest20 Trail Making Test22
Consortium to Establish a Registry of Alzheimerrsquos Disease(CERAD) Test Battery Naming Subtest23 and MMSE24
Neuropathologic evaluation was performed on specific brainregions including frontal temporal parietal and calcarine cortexcingulate gyrus substantia innominata basal ganglia claustruminsula amygdaloid nucleus hypothalamus hippocampus andparahippocampus midbrain pons medulla and cerebellumBraak staging25 was based on a modified Bielshowsky stain Eval-uation of LBP included hematoxylin and eosin staining in thesubstantia nigra and immunohistochemical staining for ASN (LB509 Zymed San Francisco CA) in the amygdala and substantianigra A blinded assessment (blind to diagnosis Braak stagingand ASN immunostaining in other regions) of ASN-immunostainedsections was performed for the presence or absence of intraneuro-nal ASN-immunopositive inclusions and neurites
Participants were categorized into the following diagnosticgroups AD (Braak stage IV or higher and plaque scores consistentwith CERAD definite AD) ADLBP (AD as above with ASN-positive inclusions in either the amygdala or the substantianigra) LBP alone (Braak stage III or less and ASN-positive inclu-sions in either the amygdala or the substantia nigra) This crite-rion for setting a cut-off score of Braak stage IV for clinically
relevant AD is based on a previous description of neuropathologyin cognitively normal elderly subjects26 Others have suggestedthat the amygdala is the most sensitive region for identifying ASNLB pathology2327 and in this study some subjects in the ADLBPgroup were found to have LB inclusions only in the amygdala andnot in the brainstem (amygdala-only ADLBP) Currently theclinical and pathophysiologic importance of AD with LBP re-stricted to the amygdala alone is unclear (without other brain-stem limbic or neocortical LBP) Therefore in addition to thegroup membership as described above an additional analysis wasperformed with the amygdala-only ADLBP patients excludedfrom the ADLBP group Following neuropathologic diagnosissubsequent analyses were performed on neuropsychological dataobtained at intake Because these diagnostic groups are definedneuropathologically and because this study was started before theconsensus criteria for dementia with LBs clinical data about fluc-tuation parkinsonian features and visual hallucinations were notadequately generated and were not available to analyze Patientswithout AD or LBP were not included in this study and patientswith an MMSE score of 14 at their initial evaluation were ex-cluded to select a population of subjects not already in the latestages of a dementing illness To examine the change in patientsrsquocognitive function over time final MMSE and DRS scores weresubtracted from their initial (entry) scores and divided by years ofobservation Yearly follow-up data from other neuropsychologicaltests were not available for analysis
Results Between-group comparisons for education ageat onset and MMSE and DRS scores at entry to the study(average of 1 year after onset of memory problems) re-vealed no significant differences between groups (table 1)A multivariate analysis of variance (ANOVA) with groups(AD ADLBP and LBP) as the between factor and tests(DRS WMS Logical Memory and Visual ReproductionFuld Object Memory Evaluation WAIS-R Digit SpanWAIR-R Comprehension WAIS-R Similarities WAIS-RBlock Design WAIS-R Proverbs Trail Making TestCERAD Naming and MMSE) as dependent factors wassignificant (F[5 22] 465 p 005) To ensure a largersample size subsequent ANOVAS were performed for eachindividual test
Table 2 displays the means and SE of intake neuropsy-chological test results and change in DRS and MMSE bydiagnostic group AD patients performed worse than LBPpatients on memory measures (Fuld Object Memory De-layed Recall F[190] 404 p 005 WMS Logical Mem-ory Delayed Recall F[212] 1224 p 005) and a verbaltask (CERAD Naming F[2126] 545 p 005) LBPpatients were more impaired than AD patients on an exec-
Table 1 Demographics
AD n 48 ADLBP n 65 LBP n 22 Total n 135
Age at onset mean 7747 734 7477 659 7645 534 7599 675
Sex MF 1830 2441 166 5877
Intake MMSE 2060 387 2068 372 2073 381 2066 376
Education
HS 13 (027) 13 (020) 4 (018) 30 (022)
HS 7 (015) 26 (040) 5 (023) 38 (028)
HS 27 (056) 26 (040) 13 (059) 66 (049)
Duration of disease 603 262 681 252 565 223 616 250
Braak stage 469 059 488 057 214 077 436 116
Sex frequency of male and female patients intake MMSE initial Mini-Mental State Examination score out of 30 HS less thanhigh school HS high school or equivalent HS greater than high school duration of disease age at death minus age of onsetBraak stage mean stage of neurofibrillary tangles
2070 NEUROLOGY 64 June (2 of 2) 2005
utive function task (Trails B Time F[231] 603 p 005) and an attention task (WAIS-R Digit Span F[195] 826 p 005) (see table 2)
A comparison of MMSE and DRS scores over time re-vealed a difference between groups (DRS F[297] 369
p 005 MMSE F[2116] 344 p 005) with ADLBPpatients demonstrating the greatest degree of change fol-lowed by AD patients and then LBP (figure) The groupsdid not differ in terms of their duration of disease definedas the amount of time that elapsed between age at onset
Table 2 Means and standard errors of intake neuropsychological test results by diagnostic group
AD(Mean SE)
ADLBP(Mean SE)
LBP(Mean SE) p Value
Attention
DRS Attention 344 03 346 03 343 04 089
Trail Making Test Part A 987 112 1003 89 1140 139 067
WAIS-R Digit Span 91 04 82 04 72 05 001
Language
CERAD Naming 69 04 61 03 79 04 001
Memory
DRS Memory 151 06 151 06 175 11 008
Fuld Object Memory Retrieval 176 14 191 14 202 20 056
Fuld Object Memory Del Recall 36 03 43 04 49 05 005
WMS Logical Memory Immediate 31 03 32 03 53 07 000
WMS Logical Memory Delayed 05 01 08 02 24 05 000
WMS Visual Reproduction Immediate 20 03 13 02 16 04 012
WMS Visual Reproduction Delayed 05 02 02 01 03 01 048
Visuo-constructional
DRS Construction 48 02 48 02 47 03 089
WAIS-R Block Design 74 05 72 05 65 05 059
Executive Function
DRS InitiationPerseveration 261 09 267 08 244 13 035
DRS Conceptualization 338 09 331 06 333 11 079
Trail Making Test Part B 1687 181 1838 148 2975 451 001
WAIS-R Comprehension 86 05 86 04 82 06 087
WAIS-R Proverbs 19 03 21 03 12 03 017
WAIS-R Similarities 99 04 88 04 89 06 011
Other
DRS Total 1147 21 1142 18 1142 27 099
MMSE Total 206 06 207 05 207 08 099
Rate of Decline (DRS) points per year 96 15 153 19 88 17 003
Rate of Decline (MMSE) points per year 35 04 50 05 34 07 004dagger
p Values A one-way ANOVA for group difference
dagger This finding is reduced to a statistical trend (p 007) with removal of patients in the ADLBP group who have Lewy body pathologyrestricted to the Amygdala (N 17)
DRS attention subscale 37 points possible Trail Making Test Part A total time in seconds to complete trails test A WAIS-RDigit Span subscale age corrected scaled score CERAD Naming 10 item naming task DRS-Memory subscale 25 points possibleFuld Object Memory Retrieval 50 points possible Fuld Object Memory Delayed Recall 10 points possible WMS-Logical Mem-ory Immediate 50 points possible WMS-Logical Memory Delayed 50 points possible WMS-Visual Reproduction Immediate 41points possible WMS-Visual Reproduction Delayed 41 points possible DRS Construction subscale 6 points possible WAIS-RBlock Design subscale age corrected scaled score DRS-InitiationPerseveration subscale age corrected scaled score DRS-Conceptualization subscale age corrected scaled score Trail Making Test Part B total time in seconds to complete trails BWAIS-R Comprehension subscale age corrected scaled score WAIS-R Comprehension subscale age corrected scaled score WAIS-RSimilarities subscale age corrected scaled score WAIS-R Proverb items taken from comprehension subscale age corrected scaledscore DRS-Total total score of the DRS out of 144 Rate of Decline (DRS) average points per year of decline Rate of Decline(MMSE) average points per year of decline
AD Alzheimer disease LBP Lewy body pathology DRS Dementia Rating Scale WAIS-R Wechsler Adult Intelligence-ScaleRevised CERAD Consortium to Establish a Registry of AD WMS Wechsler Memory Scale MMSE Mini-Mental StateExamination
June (2 of 2) 2005 NEUROLOGY 64 2071
and age at death so it is unlikely that cognitive changeover time was affected by survival rates (p 0315) Al-though we recognize that rate of decline may not have atruly linear progression and may be influenced by factorssuch as education age at diagnosis duration of disease atfirst testing etc this simple calculation of change per yearseems to reflect a more rapid change in general cognitivefunction over time
Because the clinical and pathophysiologic importance ofamygdala-only LB pathology is currently unclear we ex-cluded these cases from our analysis ADLBP patientswith LB inclusions restricted to the amygdala (n 17)were removed from the ADLBP group and ANOVAS asdescribed above were repeated These results were essen-
tially unchanged from those described above (and as notedin figure and table 2) with the exception of MMSE changeover time which was only approaching significance (p 007) To examine whether concomitant diseases or vascu-lar dementia contributed to the findings of unique cogni-tive deficits between groups we reviewed neuropathologyreports and counted the total number of additional find-ings for each subject (eg infarcts lacunes hemorrhageetc) A comparison of this count (a score of 1 for eachadditional event) between groups was not significant
Discussion We used only autopsy-confirmed casesfrom a community-based sample of dementia andused ASN immunohistochemistry and extranigralsampling The number of cases in each group waslarge and the LB-associated dementias were dividedby the presence or absence of significant coexistentAD pathologic change Our results indicate that pa-tients with LBP alone evidence relatively less severeimpairments than patients with AD and ADLBP onmeasures of verbal memory and confrontation nam-ing when mild to moderately demented These find-ings were not due to differences of demographicssuch as age at onset and education or dementia se-verity as the initial MMSE and DRS scores were notsignificantly different between dementia subgroupsConsistent with previous findings patients withLBP alone performed worse than those with AD andADLBP on measures of executive function (Trails B)and attention (WAIS-R Digit Span) Part A of theTrail Making Test did not differ among groupswhich suggests that LBP patients were more im-paired in terms of divided attention and not simplyperforming the task more slowly owing to motorimpairments
Other studies have failed to find cognitive differ-ences between LBP and AD patients at an early dis-ease stage28 LBP patients with high Braak stageratings have been shown to be less likely to expressthe clinical features of LBP29 Thus clinical recogni-tion and differentiation of LBP vs AD can be diffi-cult Consistent with these findings our study alsofound that patients with ADLBP did not differ sig-nificantly from AD patients on any of the neuropsy-chological measures used It is possible that becauseboth groups share a high degree of overlap with re-gard to AD pathology clinical symptoms and cogni-tive differences should they exist may be too subtleto detect with current methods
In terms of cognitive decline patients with ADLBP clearly stood out as having the greatest degreeof change in both the DRS and the MMSE per yearEven when the analysis excluded the patients in theADLBP group where LB inclusions were found onlyin the amygdala there was a significant change inthe DRS per year A greater degree of change incognitive function over time in the ADLBP groupcould be explained as the result of two concomitantdisease processes or that ASN pathology is a markerfor a more aggressive form of AD Other groups havedescribed a rapidly progressive course for patients
Figure (A) Repeated follow-up change in cognitive testingscores (Dementia Rating Scale [DRS]) Change in DRSscores over time Decline (pointsyear) was calculated bysubtracting final scores from initial scores and dividing bythe number of years the patient was followed Patientswith Alzheimer disease (AD)Lewy body pathology (LBP)had a significantly greater rate of decline (p 005) thanboth AD and LBP patients p 005 (B) Repeatedfollow-up change in cognitive testing scores (Mini-MentalState Examination [MMSE]) Change in MMSE scoresover time Decline (pointsyear) was calculated by sub-tracting final scores from initial scores and dividing bythe number of years the patient was followed ADLBP pa-tients had a significantly greater rate of decline (p 005)than both AD and LBP patients p 005 daggerThis findingis reduced to p 007 with the removal of patients in theADLBP group who have LBP restricted to the amygdala
2072 NEUROLOGY 64 June (2 of 2) 2005
with ADLBP830 Our study confirms that finding butemphasizes that it is only the AD cases with LB thathave this more rapid loss of cognitive function re-gardless of the localization of LBP In fact thosecases with LBP alone had the least amount ofchange over time on the MMSE and DRS
It has been suggested that early diagnosis of LBDand differentiation from AD may have therapeuticimplications in terms of avoiding neuroleptic medica-tions5 and the use of cholinesterase inhibitors hasbeen recommended6 Our study provides additionalsupport for the previously described symptoms cog-nitive impairments and functional disabilities thatspecifically characterize LBP and provides furtherevidence for some initial cognitive differences amongthe groups Our study sample is community basedand patients were not excluded based on other dis-ease processes Thus this sample may better repre-sent dementia in the general medical community
Limitations of this study may include selectionbias between patients who elected to participate inthe initial evaluation as well as for those who con-sented for autopsy It is unknown whether these dif-ferences are systematic
References1 McKeith IG Galasko D Kosaka K et al Consensus guidelines for the
clinical and pathologic diagnosis of dementia with Lewy bodies (DLB)report of the Consortium on DLB International Workshop Neurology1996471113ndash1124
2 Hamilton RL Lewy bodies in Alzheimerrsquos disease a neuropathologicalreview of 145 cases using alpha-synuclein immunohistochemistryBrain Pathol 200010378ndash384
3 Lippa CF Fujiwara H Mann DM et al Lewy bodies contain alteredalpha-synuclein in brains of many familial Alzheimerrsquos disease patientswith mutations in presenilin and amyloid precursor protein genesAm J Pathol 19981531365ndash1370
4 Lippa CF Schmidt ML Lee VM Trojanowski JQ Antibodies to alpha-synuclein detect Lewy bodies in many Downrsquos syndrome brains withAlzheimerrsquos disease Ann Neurol 199945353ndash357
5 McKeith I Fairbairn A Perry R Thompson P Perry E Neurolepticsensitivity in patients with senile dementia of Lewy body type BrMed J 1992305673ndash678
6 McKeith I Del Ser T Spano P et al Efficacy of rivastigmine in demen-tia with Lewy bodies a randomised double-blind placebo-controlledinternational study Lancet 20003562031ndash2036
7 Ferman TJ Smith GE Boeve BF et al DLB fluctuations specificfeatures that reliably differentiate DLB from AD and normal agingNeurology 200462181ndash187
8 Heyman A Fillenbaum GG Gearing M et al Comparison of Lewy bodyvariant of Alzheimerrsquos disease with pure Alzheimerrsquos disease Consor-
tium to Establish a Registry for Alzheimerrsquos Disease part XIX Neurol-ogy 1999521839ndash1844
9 Ballard C OrsquoBrien J Gray A et al Attention and fluctuating attentionin patients with dementia with Lewy bodies and Alzheimer diseaseArch Neurol 200158977ndash982
10 Larner AJ MMSE subscores and the diagnosis of dementia with Lewybodies Int J Geriatr Psychiatry 200318855ndash856
11 Noe E Marder K Bell KL Jacobs DM Manly JJ Stern Y Comparisonof dementia with Lewy bodies to Alzheimerrsquos disease and Parkinsonrsquosdisease with dementia Mov Disord 20041960ndash67
12 Pasquier F Early diagnosis of dementia neuropsychology J Neurol19992466ndash15
13 Salmon DP Galasko D Hansen LA et al Neuropsychological deficitsassociated with diffuse Lewy body disease Brain Cogn 199631148ndash165
14 Collerton D Burn D McKeith I OrsquoBrien J Systematic review andmeta-analysis show that dementia with Lewy bodies is a visualndashperceptual and attentionalndashexecutive dementia Dement Geriatr CognDisord 200316229ndash237
15 Hansen L Salmon D Galasko D et al The Lewy body variant ofAlzheimerrsquos disease a clinical and pathologic entity Neurology 1990401ndash8
16 Larson E Kukull W Teri L et al The University of Washington Alz-heimerrsquos Disease Patient Registry (ADPR) 1987ndash1988 Aging 19902404ndash408
17 McKhann G Drachman D Folstein M Katzman R Price D Stadlan EClinical diagnosis of Alzheimerrsquos disease report of the NINCDS-ADRDA Work Group under the auspices of Department of Health andHuman Services Task Force on Alzheimerrsquos Disease Neurology 198434939ndash944
18 American Psychiatric Association Diagnostic and statistical manual ofmental disorders 3rd ed rev Washington DC American PsychiatricPress 1987
19 Mattis S Dementia Rating Scale Odessa FL Psychological Assess-ment Resources 1988
20 Wechsler D Wechsler Adult Intelligence Scale-rRevised manual NewYork Psychological Corp 1981
21 Fuld PA Fuld ObjectndashMemory Evaluation Chicago IL Stoetling 197722 Reitan R Validity of the Trail-Making Test as an indicator of organic
brain damage Percept Mot Skills 198519199ndash20623 Welsh KA Butters N Mohs RC et al The Consortium to Establish a
Registry in Alzheimerrsquos Disease (CERAD) Part V A normative study ofthe neuropsychological battery Neurology 199444609ndash614
24 Folstein MF Folstein SE McHugh PR Mini-Mental State a practicalmethod for grading the cognitive state of patients for the clinicianJ Psychiatr Res 197512189ndash198
25 Braak H Braak E Neuropathological stageing of Alzheimer-relatedchanges Acta Neuropathol 199182239ndash259
26 Knopman DS Parisi JE Salviati A et al Neuropathology of cognitivelynormal elderly J Neuropathol Exp Neurol 2003621087ndash1095
27 Marui W Iseki E Nakai T et al Progression and staging of Lewypathology in brains from patients with dementia with Lewy bodiesJ Neurol Sci 2002195153ndash159
28 Mormont E Laurier-Grymonprez L Baisset-Mouly C Pasquier F Theprofile of memory disturbance in early Lewy body dementia differs fromthat in Alzheimerrsquos disease Rev Neurol (Paris) 2003159762ndash766
29 Merdes AR Hansen LA Jeste DV et al Influence of Alzheimer pathol-ogy on clinical diagnostic accuracy in dementia with Lewy bodies Neu-rology 2003601586ndash1590
30 Olichney JM Galasko D Salmon DP et al Cognitive decline is fasterin Lewy body variant than in Alzheimerrsquos disease Neurology 199851351ndash357
June (2 of 2) 2005 NEUROLOGY 64 2073
DOI 10121201WNL000016598789198652005642069-2073 Neurology
M L Kraybill E B Larson D W Tsuang et al pathology or both
Cognitive differences in dementia patients with autopsy-verified AD Lewy body
This information is current as of June 27 2005
ServicesUpdated Information amp
httpwwwneurologyorgcontent64122069fullhtmlincluding high resolution figures can be found at
References
1httpwwwneurologyorgcontent64122069fullhtmlref-list-at This article cites 25 articles 8 of which you can access for free
Citations
icleshttpwwwneurologyorgcontent64122069fullhtmlotherartThis article has been cited by 11 HighWire-hosted articles
Subspecialty Collections
odieshttpwwwneurologyorgcgicollectiondementia_with_lewy_bDementia with Lewy bodies
httpwwwneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
ehaviorhttpwwwneurologyorgcgicollectionall_neuropsychology_bAll NeuropsychologyBehaviorfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

utive function task (Trails B Time F[231] 603 p 005) and an attention task (WAIS-R Digit Span F[195] 826 p 005) (see table 2)
A comparison of MMSE and DRS scores over time re-vealed a difference between groups (DRS F[297] 369
p 005 MMSE F[2116] 344 p 005) with ADLBPpatients demonstrating the greatest degree of change fol-lowed by AD patients and then LBP (figure) The groupsdid not differ in terms of their duration of disease definedas the amount of time that elapsed between age at onset
Table 2 Means and standard errors of intake neuropsychological test results by diagnostic group
AD(Mean SE)
ADLBP(Mean SE)
LBP(Mean SE) p Value
Attention
DRS Attention 344 03 346 03 343 04 089
Trail Making Test Part A 987 112 1003 89 1140 139 067
WAIS-R Digit Span 91 04 82 04 72 05 001
Language
CERAD Naming 69 04 61 03 79 04 001
Memory
DRS Memory 151 06 151 06 175 11 008
Fuld Object Memory Retrieval 176 14 191 14 202 20 056
Fuld Object Memory Del Recall 36 03 43 04 49 05 005
WMS Logical Memory Immediate 31 03 32 03 53 07 000
WMS Logical Memory Delayed 05 01 08 02 24 05 000
WMS Visual Reproduction Immediate 20 03 13 02 16 04 012
WMS Visual Reproduction Delayed 05 02 02 01 03 01 048
Visuo-constructional
DRS Construction 48 02 48 02 47 03 089
WAIS-R Block Design 74 05 72 05 65 05 059
Executive Function
DRS InitiationPerseveration 261 09 267 08 244 13 035
DRS Conceptualization 338 09 331 06 333 11 079
Trail Making Test Part B 1687 181 1838 148 2975 451 001
WAIS-R Comprehension 86 05 86 04 82 06 087
WAIS-R Proverbs 19 03 21 03 12 03 017
WAIS-R Similarities 99 04 88 04 89 06 011
Other
DRS Total 1147 21 1142 18 1142 27 099
MMSE Total 206 06 207 05 207 08 099
Rate of Decline (DRS) points per year 96 15 153 19 88 17 003
Rate of Decline (MMSE) points per year 35 04 50 05 34 07 004dagger
p Values A one-way ANOVA for group difference
dagger This finding is reduced to a statistical trend (p 007) with removal of patients in the ADLBP group who have Lewy body pathologyrestricted to the Amygdala (N 17)
DRS attention subscale 37 points possible Trail Making Test Part A total time in seconds to complete trails test A WAIS-RDigit Span subscale age corrected scaled score CERAD Naming 10 item naming task DRS-Memory subscale 25 points possibleFuld Object Memory Retrieval 50 points possible Fuld Object Memory Delayed Recall 10 points possible WMS-Logical Mem-ory Immediate 50 points possible WMS-Logical Memory Delayed 50 points possible WMS-Visual Reproduction Immediate 41points possible WMS-Visual Reproduction Delayed 41 points possible DRS Construction subscale 6 points possible WAIS-RBlock Design subscale age corrected scaled score DRS-InitiationPerseveration subscale age corrected scaled score DRS-Conceptualization subscale age corrected scaled score Trail Making Test Part B total time in seconds to complete trails BWAIS-R Comprehension subscale age corrected scaled score WAIS-R Comprehension subscale age corrected scaled score WAIS-RSimilarities subscale age corrected scaled score WAIS-R Proverb items taken from comprehension subscale age corrected scaledscore DRS-Total total score of the DRS out of 144 Rate of Decline (DRS) average points per year of decline Rate of Decline(MMSE) average points per year of decline
AD Alzheimer disease LBP Lewy body pathology DRS Dementia Rating Scale WAIS-R Wechsler Adult Intelligence-ScaleRevised CERAD Consortium to Establish a Registry of AD WMS Wechsler Memory Scale MMSE Mini-Mental StateExamination
June (2 of 2) 2005 NEUROLOGY 64 2071
and age at death so it is unlikely that cognitive changeover time was affected by survival rates (p 0315) Al-though we recognize that rate of decline may not have atruly linear progression and may be influenced by factorssuch as education age at diagnosis duration of disease atfirst testing etc this simple calculation of change per yearseems to reflect a more rapid change in general cognitivefunction over time
Because the clinical and pathophysiologic importance ofamygdala-only LB pathology is currently unclear we ex-cluded these cases from our analysis ADLBP patientswith LB inclusions restricted to the amygdala (n 17)were removed from the ADLBP group and ANOVAS asdescribed above were repeated These results were essen-
tially unchanged from those described above (and as notedin figure and table 2) with the exception of MMSE changeover time which was only approaching significance (p 007) To examine whether concomitant diseases or vascu-lar dementia contributed to the findings of unique cogni-tive deficits between groups we reviewed neuropathologyreports and counted the total number of additional find-ings for each subject (eg infarcts lacunes hemorrhageetc) A comparison of this count (a score of 1 for eachadditional event) between groups was not significant
Discussion We used only autopsy-confirmed casesfrom a community-based sample of dementia andused ASN immunohistochemistry and extranigralsampling The number of cases in each group waslarge and the LB-associated dementias were dividedby the presence or absence of significant coexistentAD pathologic change Our results indicate that pa-tients with LBP alone evidence relatively less severeimpairments than patients with AD and ADLBP onmeasures of verbal memory and confrontation nam-ing when mild to moderately demented These find-ings were not due to differences of demographicssuch as age at onset and education or dementia se-verity as the initial MMSE and DRS scores were notsignificantly different between dementia subgroupsConsistent with previous findings patients withLBP alone performed worse than those with AD andADLBP on measures of executive function (Trails B)and attention (WAIS-R Digit Span) Part A of theTrail Making Test did not differ among groupswhich suggests that LBP patients were more im-paired in terms of divided attention and not simplyperforming the task more slowly owing to motorimpairments
Other studies have failed to find cognitive differ-ences between LBP and AD patients at an early dis-ease stage28 LBP patients with high Braak stageratings have been shown to be less likely to expressthe clinical features of LBP29 Thus clinical recogni-tion and differentiation of LBP vs AD can be diffi-cult Consistent with these findings our study alsofound that patients with ADLBP did not differ sig-nificantly from AD patients on any of the neuropsy-chological measures used It is possible that becauseboth groups share a high degree of overlap with re-gard to AD pathology clinical symptoms and cogni-tive differences should they exist may be too subtleto detect with current methods
In terms of cognitive decline patients with ADLBP clearly stood out as having the greatest degreeof change in both the DRS and the MMSE per yearEven when the analysis excluded the patients in theADLBP group where LB inclusions were found onlyin the amygdala there was a significant change inthe DRS per year A greater degree of change incognitive function over time in the ADLBP groupcould be explained as the result of two concomitantdisease processes or that ASN pathology is a markerfor a more aggressive form of AD Other groups havedescribed a rapidly progressive course for patients
Figure (A) Repeated follow-up change in cognitive testingscores (Dementia Rating Scale [DRS]) Change in DRSscores over time Decline (pointsyear) was calculated bysubtracting final scores from initial scores and dividing bythe number of years the patient was followed Patientswith Alzheimer disease (AD)Lewy body pathology (LBP)had a significantly greater rate of decline (p 005) thanboth AD and LBP patients p 005 (B) Repeatedfollow-up change in cognitive testing scores (Mini-MentalState Examination [MMSE]) Change in MMSE scoresover time Decline (pointsyear) was calculated by sub-tracting final scores from initial scores and dividing bythe number of years the patient was followed ADLBP pa-tients had a significantly greater rate of decline (p 005)than both AD and LBP patients p 005 daggerThis findingis reduced to p 007 with the removal of patients in theADLBP group who have LBP restricted to the amygdala
2072 NEUROLOGY 64 June (2 of 2) 2005
with ADLBP830 Our study confirms that finding butemphasizes that it is only the AD cases with LB thathave this more rapid loss of cognitive function re-gardless of the localization of LBP In fact thosecases with LBP alone had the least amount ofchange over time on the MMSE and DRS
It has been suggested that early diagnosis of LBDand differentiation from AD may have therapeuticimplications in terms of avoiding neuroleptic medica-tions5 and the use of cholinesterase inhibitors hasbeen recommended6 Our study provides additionalsupport for the previously described symptoms cog-nitive impairments and functional disabilities thatspecifically characterize LBP and provides furtherevidence for some initial cognitive differences amongthe groups Our study sample is community basedand patients were not excluded based on other dis-ease processes Thus this sample may better repre-sent dementia in the general medical community
Limitations of this study may include selectionbias between patients who elected to participate inthe initial evaluation as well as for those who con-sented for autopsy It is unknown whether these dif-ferences are systematic
References1 McKeith IG Galasko D Kosaka K et al Consensus guidelines for the
clinical and pathologic diagnosis of dementia with Lewy bodies (DLB)report of the Consortium on DLB International Workshop Neurology1996471113ndash1124
2 Hamilton RL Lewy bodies in Alzheimerrsquos disease a neuropathologicalreview of 145 cases using alpha-synuclein immunohistochemistryBrain Pathol 200010378ndash384
3 Lippa CF Fujiwara H Mann DM et al Lewy bodies contain alteredalpha-synuclein in brains of many familial Alzheimerrsquos disease patientswith mutations in presenilin and amyloid precursor protein genesAm J Pathol 19981531365ndash1370
4 Lippa CF Schmidt ML Lee VM Trojanowski JQ Antibodies to alpha-synuclein detect Lewy bodies in many Downrsquos syndrome brains withAlzheimerrsquos disease Ann Neurol 199945353ndash357
5 McKeith I Fairbairn A Perry R Thompson P Perry E Neurolepticsensitivity in patients with senile dementia of Lewy body type BrMed J 1992305673ndash678
6 McKeith I Del Ser T Spano P et al Efficacy of rivastigmine in demen-tia with Lewy bodies a randomised double-blind placebo-controlledinternational study Lancet 20003562031ndash2036
7 Ferman TJ Smith GE Boeve BF et al DLB fluctuations specificfeatures that reliably differentiate DLB from AD and normal agingNeurology 200462181ndash187
8 Heyman A Fillenbaum GG Gearing M et al Comparison of Lewy bodyvariant of Alzheimerrsquos disease with pure Alzheimerrsquos disease Consor-
tium to Establish a Registry for Alzheimerrsquos Disease part XIX Neurol-ogy 1999521839ndash1844
9 Ballard C OrsquoBrien J Gray A et al Attention and fluctuating attentionin patients with dementia with Lewy bodies and Alzheimer diseaseArch Neurol 200158977ndash982
10 Larner AJ MMSE subscores and the diagnosis of dementia with Lewybodies Int J Geriatr Psychiatry 200318855ndash856
11 Noe E Marder K Bell KL Jacobs DM Manly JJ Stern Y Comparisonof dementia with Lewy bodies to Alzheimerrsquos disease and Parkinsonrsquosdisease with dementia Mov Disord 20041960ndash67
12 Pasquier F Early diagnosis of dementia neuropsychology J Neurol19992466ndash15
13 Salmon DP Galasko D Hansen LA et al Neuropsychological deficitsassociated with diffuse Lewy body disease Brain Cogn 199631148ndash165
14 Collerton D Burn D McKeith I OrsquoBrien J Systematic review andmeta-analysis show that dementia with Lewy bodies is a visualndashperceptual and attentionalndashexecutive dementia Dement Geriatr CognDisord 200316229ndash237
15 Hansen L Salmon D Galasko D et al The Lewy body variant ofAlzheimerrsquos disease a clinical and pathologic entity Neurology 1990401ndash8
16 Larson E Kukull W Teri L et al The University of Washington Alz-heimerrsquos Disease Patient Registry (ADPR) 1987ndash1988 Aging 19902404ndash408
17 McKhann G Drachman D Folstein M Katzman R Price D Stadlan EClinical diagnosis of Alzheimerrsquos disease report of the NINCDS-ADRDA Work Group under the auspices of Department of Health andHuman Services Task Force on Alzheimerrsquos Disease Neurology 198434939ndash944
18 American Psychiatric Association Diagnostic and statistical manual ofmental disorders 3rd ed rev Washington DC American PsychiatricPress 1987
19 Mattis S Dementia Rating Scale Odessa FL Psychological Assess-ment Resources 1988
20 Wechsler D Wechsler Adult Intelligence Scale-rRevised manual NewYork Psychological Corp 1981
21 Fuld PA Fuld ObjectndashMemory Evaluation Chicago IL Stoetling 197722 Reitan R Validity of the Trail-Making Test as an indicator of organic
brain damage Percept Mot Skills 198519199ndash20623 Welsh KA Butters N Mohs RC et al The Consortium to Establish a
Registry in Alzheimerrsquos Disease (CERAD) Part V A normative study ofthe neuropsychological battery Neurology 199444609ndash614
24 Folstein MF Folstein SE McHugh PR Mini-Mental State a practicalmethod for grading the cognitive state of patients for the clinicianJ Psychiatr Res 197512189ndash198
25 Braak H Braak E Neuropathological stageing of Alzheimer-relatedchanges Acta Neuropathol 199182239ndash259
26 Knopman DS Parisi JE Salviati A et al Neuropathology of cognitivelynormal elderly J Neuropathol Exp Neurol 2003621087ndash1095
27 Marui W Iseki E Nakai T et al Progression and staging of Lewypathology in brains from patients with dementia with Lewy bodiesJ Neurol Sci 2002195153ndash159
28 Mormont E Laurier-Grymonprez L Baisset-Mouly C Pasquier F Theprofile of memory disturbance in early Lewy body dementia differs fromthat in Alzheimerrsquos disease Rev Neurol (Paris) 2003159762ndash766
29 Merdes AR Hansen LA Jeste DV et al Influence of Alzheimer pathol-ogy on clinical diagnostic accuracy in dementia with Lewy bodies Neu-rology 2003601586ndash1590
30 Olichney JM Galasko D Salmon DP et al Cognitive decline is fasterin Lewy body variant than in Alzheimerrsquos disease Neurology 199851351ndash357
June (2 of 2) 2005 NEUROLOGY 64 2073
DOI 10121201WNL000016598789198652005642069-2073 Neurology
M L Kraybill E B Larson D W Tsuang et al pathology or both
Cognitive differences in dementia patients with autopsy-verified AD Lewy body
This information is current as of June 27 2005
ServicesUpdated Information amp
httpwwwneurologyorgcontent64122069fullhtmlincluding high resolution figures can be found at
References
1httpwwwneurologyorgcontent64122069fullhtmlref-list-at This article cites 25 articles 8 of which you can access for free
Citations
icleshttpwwwneurologyorgcontent64122069fullhtmlotherartThis article has been cited by 11 HighWire-hosted articles
Subspecialty Collections
odieshttpwwwneurologyorgcgicollectiondementia_with_lewy_bDementia with Lewy bodies
httpwwwneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
ehaviorhttpwwwneurologyorgcgicollectionall_neuropsychology_bAll NeuropsychologyBehaviorfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

and age at death so it is unlikely that cognitive changeover time was affected by survival rates (p 0315) Al-though we recognize that rate of decline may not have atruly linear progression and may be influenced by factorssuch as education age at diagnosis duration of disease atfirst testing etc this simple calculation of change per yearseems to reflect a more rapid change in general cognitivefunction over time
Because the clinical and pathophysiologic importance ofamygdala-only LB pathology is currently unclear we ex-cluded these cases from our analysis ADLBP patientswith LB inclusions restricted to the amygdala (n 17)were removed from the ADLBP group and ANOVAS asdescribed above were repeated These results were essen-
tially unchanged from those described above (and as notedin figure and table 2) with the exception of MMSE changeover time which was only approaching significance (p 007) To examine whether concomitant diseases or vascu-lar dementia contributed to the findings of unique cogni-tive deficits between groups we reviewed neuropathologyreports and counted the total number of additional find-ings for each subject (eg infarcts lacunes hemorrhageetc) A comparison of this count (a score of 1 for eachadditional event) between groups was not significant
Discussion We used only autopsy-confirmed casesfrom a community-based sample of dementia andused ASN immunohistochemistry and extranigralsampling The number of cases in each group waslarge and the LB-associated dementias were dividedby the presence or absence of significant coexistentAD pathologic change Our results indicate that pa-tients with LBP alone evidence relatively less severeimpairments than patients with AD and ADLBP onmeasures of verbal memory and confrontation nam-ing when mild to moderately demented These find-ings were not due to differences of demographicssuch as age at onset and education or dementia se-verity as the initial MMSE and DRS scores were notsignificantly different between dementia subgroupsConsistent with previous findings patients withLBP alone performed worse than those with AD andADLBP on measures of executive function (Trails B)and attention (WAIS-R Digit Span) Part A of theTrail Making Test did not differ among groupswhich suggests that LBP patients were more im-paired in terms of divided attention and not simplyperforming the task more slowly owing to motorimpairments
Other studies have failed to find cognitive differ-ences between LBP and AD patients at an early dis-ease stage28 LBP patients with high Braak stageratings have been shown to be less likely to expressthe clinical features of LBP29 Thus clinical recogni-tion and differentiation of LBP vs AD can be diffi-cult Consistent with these findings our study alsofound that patients with ADLBP did not differ sig-nificantly from AD patients on any of the neuropsy-chological measures used It is possible that becauseboth groups share a high degree of overlap with re-gard to AD pathology clinical symptoms and cogni-tive differences should they exist may be too subtleto detect with current methods
In terms of cognitive decline patients with ADLBP clearly stood out as having the greatest degreeof change in both the DRS and the MMSE per yearEven when the analysis excluded the patients in theADLBP group where LB inclusions were found onlyin the amygdala there was a significant change inthe DRS per year A greater degree of change incognitive function over time in the ADLBP groupcould be explained as the result of two concomitantdisease processes or that ASN pathology is a markerfor a more aggressive form of AD Other groups havedescribed a rapidly progressive course for patients
Figure (A) Repeated follow-up change in cognitive testingscores (Dementia Rating Scale [DRS]) Change in DRSscores over time Decline (pointsyear) was calculated bysubtracting final scores from initial scores and dividing bythe number of years the patient was followed Patientswith Alzheimer disease (AD)Lewy body pathology (LBP)had a significantly greater rate of decline (p 005) thanboth AD and LBP patients p 005 (B) Repeatedfollow-up change in cognitive testing scores (Mini-MentalState Examination [MMSE]) Change in MMSE scoresover time Decline (pointsyear) was calculated by sub-tracting final scores from initial scores and dividing bythe number of years the patient was followed ADLBP pa-tients had a significantly greater rate of decline (p 005)than both AD and LBP patients p 005 daggerThis findingis reduced to p 007 with the removal of patients in theADLBP group who have LBP restricted to the amygdala
2072 NEUROLOGY 64 June (2 of 2) 2005
with ADLBP830 Our study confirms that finding butemphasizes that it is only the AD cases with LB thathave this more rapid loss of cognitive function re-gardless of the localization of LBP In fact thosecases with LBP alone had the least amount ofchange over time on the MMSE and DRS
It has been suggested that early diagnosis of LBDand differentiation from AD may have therapeuticimplications in terms of avoiding neuroleptic medica-tions5 and the use of cholinesterase inhibitors hasbeen recommended6 Our study provides additionalsupport for the previously described symptoms cog-nitive impairments and functional disabilities thatspecifically characterize LBP and provides furtherevidence for some initial cognitive differences amongthe groups Our study sample is community basedand patients were not excluded based on other dis-ease processes Thus this sample may better repre-sent dementia in the general medical community
Limitations of this study may include selectionbias between patients who elected to participate inthe initial evaluation as well as for those who con-sented for autopsy It is unknown whether these dif-ferences are systematic
References1 McKeith IG Galasko D Kosaka K et al Consensus guidelines for the
clinical and pathologic diagnosis of dementia with Lewy bodies (DLB)report of the Consortium on DLB International Workshop Neurology1996471113ndash1124
2 Hamilton RL Lewy bodies in Alzheimerrsquos disease a neuropathologicalreview of 145 cases using alpha-synuclein immunohistochemistryBrain Pathol 200010378ndash384
3 Lippa CF Fujiwara H Mann DM et al Lewy bodies contain alteredalpha-synuclein in brains of many familial Alzheimerrsquos disease patientswith mutations in presenilin and amyloid precursor protein genesAm J Pathol 19981531365ndash1370
4 Lippa CF Schmidt ML Lee VM Trojanowski JQ Antibodies to alpha-synuclein detect Lewy bodies in many Downrsquos syndrome brains withAlzheimerrsquos disease Ann Neurol 199945353ndash357
5 McKeith I Fairbairn A Perry R Thompson P Perry E Neurolepticsensitivity in patients with senile dementia of Lewy body type BrMed J 1992305673ndash678
6 McKeith I Del Ser T Spano P et al Efficacy of rivastigmine in demen-tia with Lewy bodies a randomised double-blind placebo-controlledinternational study Lancet 20003562031ndash2036
7 Ferman TJ Smith GE Boeve BF et al DLB fluctuations specificfeatures that reliably differentiate DLB from AD and normal agingNeurology 200462181ndash187
8 Heyman A Fillenbaum GG Gearing M et al Comparison of Lewy bodyvariant of Alzheimerrsquos disease with pure Alzheimerrsquos disease Consor-
tium to Establish a Registry for Alzheimerrsquos Disease part XIX Neurol-ogy 1999521839ndash1844
9 Ballard C OrsquoBrien J Gray A et al Attention and fluctuating attentionin patients with dementia with Lewy bodies and Alzheimer diseaseArch Neurol 200158977ndash982
10 Larner AJ MMSE subscores and the diagnosis of dementia with Lewybodies Int J Geriatr Psychiatry 200318855ndash856
11 Noe E Marder K Bell KL Jacobs DM Manly JJ Stern Y Comparisonof dementia with Lewy bodies to Alzheimerrsquos disease and Parkinsonrsquosdisease with dementia Mov Disord 20041960ndash67
12 Pasquier F Early diagnosis of dementia neuropsychology J Neurol19992466ndash15
13 Salmon DP Galasko D Hansen LA et al Neuropsychological deficitsassociated with diffuse Lewy body disease Brain Cogn 199631148ndash165
14 Collerton D Burn D McKeith I OrsquoBrien J Systematic review andmeta-analysis show that dementia with Lewy bodies is a visualndashperceptual and attentionalndashexecutive dementia Dement Geriatr CognDisord 200316229ndash237
15 Hansen L Salmon D Galasko D et al The Lewy body variant ofAlzheimerrsquos disease a clinical and pathologic entity Neurology 1990401ndash8
16 Larson E Kukull W Teri L et al The University of Washington Alz-heimerrsquos Disease Patient Registry (ADPR) 1987ndash1988 Aging 19902404ndash408
17 McKhann G Drachman D Folstein M Katzman R Price D Stadlan EClinical diagnosis of Alzheimerrsquos disease report of the NINCDS-ADRDA Work Group under the auspices of Department of Health andHuman Services Task Force on Alzheimerrsquos Disease Neurology 198434939ndash944
18 American Psychiatric Association Diagnostic and statistical manual ofmental disorders 3rd ed rev Washington DC American PsychiatricPress 1987
19 Mattis S Dementia Rating Scale Odessa FL Psychological Assess-ment Resources 1988
20 Wechsler D Wechsler Adult Intelligence Scale-rRevised manual NewYork Psychological Corp 1981
21 Fuld PA Fuld ObjectndashMemory Evaluation Chicago IL Stoetling 197722 Reitan R Validity of the Trail-Making Test as an indicator of organic
brain damage Percept Mot Skills 198519199ndash20623 Welsh KA Butters N Mohs RC et al The Consortium to Establish a
Registry in Alzheimerrsquos Disease (CERAD) Part V A normative study ofthe neuropsychological battery Neurology 199444609ndash614
24 Folstein MF Folstein SE McHugh PR Mini-Mental State a practicalmethod for grading the cognitive state of patients for the clinicianJ Psychiatr Res 197512189ndash198
25 Braak H Braak E Neuropathological stageing of Alzheimer-relatedchanges Acta Neuropathol 199182239ndash259
26 Knopman DS Parisi JE Salviati A et al Neuropathology of cognitivelynormal elderly J Neuropathol Exp Neurol 2003621087ndash1095
27 Marui W Iseki E Nakai T et al Progression and staging of Lewypathology in brains from patients with dementia with Lewy bodiesJ Neurol Sci 2002195153ndash159
28 Mormont E Laurier-Grymonprez L Baisset-Mouly C Pasquier F Theprofile of memory disturbance in early Lewy body dementia differs fromthat in Alzheimerrsquos disease Rev Neurol (Paris) 2003159762ndash766
29 Merdes AR Hansen LA Jeste DV et al Influence of Alzheimer pathol-ogy on clinical diagnostic accuracy in dementia with Lewy bodies Neu-rology 2003601586ndash1590
30 Olichney JM Galasko D Salmon DP et al Cognitive decline is fasterin Lewy body variant than in Alzheimerrsquos disease Neurology 199851351ndash357
June (2 of 2) 2005 NEUROLOGY 64 2073
DOI 10121201WNL000016598789198652005642069-2073 Neurology
M L Kraybill E B Larson D W Tsuang et al pathology or both
Cognitive differences in dementia patients with autopsy-verified AD Lewy body
This information is current as of June 27 2005
ServicesUpdated Information amp
httpwwwneurologyorgcontent64122069fullhtmlincluding high resolution figures can be found at
References
1httpwwwneurologyorgcontent64122069fullhtmlref-list-at This article cites 25 articles 8 of which you can access for free
Citations
icleshttpwwwneurologyorgcontent64122069fullhtmlotherartThis article has been cited by 11 HighWire-hosted articles
Subspecialty Collections
odieshttpwwwneurologyorgcgicollectiondementia_with_lewy_bDementia with Lewy bodies
httpwwwneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
ehaviorhttpwwwneurologyorgcgicollectionall_neuropsychology_bAll NeuropsychologyBehaviorfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

with ADLBP830 Our study confirms that finding butemphasizes that it is only the AD cases with LB thathave this more rapid loss of cognitive function re-gardless of the localization of LBP In fact thosecases with LBP alone had the least amount ofchange over time on the MMSE and DRS
It has been suggested that early diagnosis of LBDand differentiation from AD may have therapeuticimplications in terms of avoiding neuroleptic medica-tions5 and the use of cholinesterase inhibitors hasbeen recommended6 Our study provides additionalsupport for the previously described symptoms cog-nitive impairments and functional disabilities thatspecifically characterize LBP and provides furtherevidence for some initial cognitive differences amongthe groups Our study sample is community basedand patients were not excluded based on other dis-ease processes Thus this sample may better repre-sent dementia in the general medical community
Limitations of this study may include selectionbias between patients who elected to participate inthe initial evaluation as well as for those who con-sented for autopsy It is unknown whether these dif-ferences are systematic
References1 McKeith IG Galasko D Kosaka K et al Consensus guidelines for the
clinical and pathologic diagnosis of dementia with Lewy bodies (DLB)report of the Consortium on DLB International Workshop Neurology1996471113ndash1124
2 Hamilton RL Lewy bodies in Alzheimerrsquos disease a neuropathologicalreview of 145 cases using alpha-synuclein immunohistochemistryBrain Pathol 200010378ndash384
3 Lippa CF Fujiwara H Mann DM et al Lewy bodies contain alteredalpha-synuclein in brains of many familial Alzheimerrsquos disease patientswith mutations in presenilin and amyloid precursor protein genesAm J Pathol 19981531365ndash1370
4 Lippa CF Schmidt ML Lee VM Trojanowski JQ Antibodies to alpha-synuclein detect Lewy bodies in many Downrsquos syndrome brains withAlzheimerrsquos disease Ann Neurol 199945353ndash357
5 McKeith I Fairbairn A Perry R Thompson P Perry E Neurolepticsensitivity in patients with senile dementia of Lewy body type BrMed J 1992305673ndash678
6 McKeith I Del Ser T Spano P et al Efficacy of rivastigmine in demen-tia with Lewy bodies a randomised double-blind placebo-controlledinternational study Lancet 20003562031ndash2036
7 Ferman TJ Smith GE Boeve BF et al DLB fluctuations specificfeatures that reliably differentiate DLB from AD and normal agingNeurology 200462181ndash187
8 Heyman A Fillenbaum GG Gearing M et al Comparison of Lewy bodyvariant of Alzheimerrsquos disease with pure Alzheimerrsquos disease Consor-
tium to Establish a Registry for Alzheimerrsquos Disease part XIX Neurol-ogy 1999521839ndash1844
9 Ballard C OrsquoBrien J Gray A et al Attention and fluctuating attentionin patients with dementia with Lewy bodies and Alzheimer diseaseArch Neurol 200158977ndash982
10 Larner AJ MMSE subscores and the diagnosis of dementia with Lewybodies Int J Geriatr Psychiatry 200318855ndash856
11 Noe E Marder K Bell KL Jacobs DM Manly JJ Stern Y Comparisonof dementia with Lewy bodies to Alzheimerrsquos disease and Parkinsonrsquosdisease with dementia Mov Disord 20041960ndash67
12 Pasquier F Early diagnosis of dementia neuropsychology J Neurol19992466ndash15
13 Salmon DP Galasko D Hansen LA et al Neuropsychological deficitsassociated with diffuse Lewy body disease Brain Cogn 199631148ndash165
14 Collerton D Burn D McKeith I OrsquoBrien J Systematic review andmeta-analysis show that dementia with Lewy bodies is a visualndashperceptual and attentionalndashexecutive dementia Dement Geriatr CognDisord 200316229ndash237
15 Hansen L Salmon D Galasko D et al The Lewy body variant ofAlzheimerrsquos disease a clinical and pathologic entity Neurology 1990401ndash8
16 Larson E Kukull W Teri L et al The University of Washington Alz-heimerrsquos Disease Patient Registry (ADPR) 1987ndash1988 Aging 19902404ndash408
17 McKhann G Drachman D Folstein M Katzman R Price D Stadlan EClinical diagnosis of Alzheimerrsquos disease report of the NINCDS-ADRDA Work Group under the auspices of Department of Health andHuman Services Task Force on Alzheimerrsquos Disease Neurology 198434939ndash944
18 American Psychiatric Association Diagnostic and statistical manual ofmental disorders 3rd ed rev Washington DC American PsychiatricPress 1987
19 Mattis S Dementia Rating Scale Odessa FL Psychological Assess-ment Resources 1988
20 Wechsler D Wechsler Adult Intelligence Scale-rRevised manual NewYork Psychological Corp 1981
21 Fuld PA Fuld ObjectndashMemory Evaluation Chicago IL Stoetling 197722 Reitan R Validity of the Trail-Making Test as an indicator of organic
brain damage Percept Mot Skills 198519199ndash20623 Welsh KA Butters N Mohs RC et al The Consortium to Establish a
Registry in Alzheimerrsquos Disease (CERAD) Part V A normative study ofthe neuropsychological battery Neurology 199444609ndash614
24 Folstein MF Folstein SE McHugh PR Mini-Mental State a practicalmethod for grading the cognitive state of patients for the clinicianJ Psychiatr Res 197512189ndash198
25 Braak H Braak E Neuropathological stageing of Alzheimer-relatedchanges Acta Neuropathol 199182239ndash259
26 Knopman DS Parisi JE Salviati A et al Neuropathology of cognitivelynormal elderly J Neuropathol Exp Neurol 2003621087ndash1095
27 Marui W Iseki E Nakai T et al Progression and staging of Lewypathology in brains from patients with dementia with Lewy bodiesJ Neurol Sci 2002195153ndash159
28 Mormont E Laurier-Grymonprez L Baisset-Mouly C Pasquier F Theprofile of memory disturbance in early Lewy body dementia differs fromthat in Alzheimerrsquos disease Rev Neurol (Paris) 2003159762ndash766
29 Merdes AR Hansen LA Jeste DV et al Influence of Alzheimer pathol-ogy on clinical diagnostic accuracy in dementia with Lewy bodies Neu-rology 2003601586ndash1590
30 Olichney JM Galasko D Salmon DP et al Cognitive decline is fasterin Lewy body variant than in Alzheimerrsquos disease Neurology 199851351ndash357
June (2 of 2) 2005 NEUROLOGY 64 2073
DOI 10121201WNL000016598789198652005642069-2073 Neurology
M L Kraybill E B Larson D W Tsuang et al pathology or both
Cognitive differences in dementia patients with autopsy-verified AD Lewy body
This information is current as of June 27 2005
ServicesUpdated Information amp
httpwwwneurologyorgcontent64122069fullhtmlincluding high resolution figures can be found at
References
1httpwwwneurologyorgcontent64122069fullhtmlref-list-at This article cites 25 articles 8 of which you can access for free
Citations
icleshttpwwwneurologyorgcontent64122069fullhtmlotherartThis article has been cited by 11 HighWire-hosted articles
Subspecialty Collections
odieshttpwwwneurologyorgcgicollectiondementia_with_lewy_bDementia with Lewy bodies
httpwwwneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
ehaviorhttpwwwneurologyorgcgicollectionall_neuropsychology_bAll NeuropsychologyBehaviorfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online

DOI 10121201WNL000016598789198652005642069-2073 Neurology
M L Kraybill E B Larson D W Tsuang et al pathology or both
Cognitive differences in dementia patients with autopsy-verified AD Lewy body
This information is current as of June 27 2005
ServicesUpdated Information amp
httpwwwneurologyorgcontent64122069fullhtmlincluding high resolution figures can be found at
References
1httpwwwneurologyorgcontent64122069fullhtmlref-list-at This article cites 25 articles 8 of which you can access for free
Citations
icleshttpwwwneurologyorgcontent64122069fullhtmlotherartThis article has been cited by 11 HighWire-hosted articles
Subspecialty Collections
odieshttpwwwneurologyorgcgicollectiondementia_with_lewy_bDementia with Lewy bodies
httpwwwneurologyorgcgicollectionalzheimers_diseaseAlzheimers disease
ehaviorhttpwwwneurologyorgcgicollectionall_neuropsychology_bAll NeuropsychologyBehaviorfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpwwwneurologyorgmiscaboutxhtmlpermissionsor in its entirety can be found online atInformation about reproducing this article in parts (figurestables)
Reprints
httpwwwneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online