Embed Size (px)
Citation preview

Classification of LeprosyClassification of Leprosy
Classification of
Leprosy
WHO WHO ClassificationClassification
Clinical Clinical ClassificationClassification

WHO ClassificationWHO Classification ::
Two types: Purpose of treatment .
1. Paucibacillary Leprosy ( PB )
2. Multibacillary Leprosy ( MB )
Based on:
Number of skin lesions
Number of nerves involved

Skin Lesions :
Paucibacillary Paucibacillary
Leprosy ( PB )Leprosy ( PB )
1 to 5 lesions
Asymmetrical
Definite Loss of sensation
> 5 lesions
Towards Symmetrical
Loss of sensation
( May be / May not be )`
Nerve Lesions: Only 1 nerve involved 2 or more nerve involved
Multibacillary Multibacillary
Leprosy ( MB )Leprosy ( MB )
Clinical Classification :
Ridley and Joppling classified leprosy clinically into
the following :
1. Tuberculoid ( TT )
2. Borderline Tuberculoid ( BT )
3. Mid Borderline ( BB )
4. Borderline Lepromatous ( BL )
5. Lepromatous ( LL )
BB Leprosy is immunologically the least stable , and
therefore the rarest .
Pure Neural Leprosy :
In all forms of leprosy , at least one peripheral nerve is attacked by M. Leprae , though this may not have any clinical evidence .
Leprosy can involve nerves without any skin changes .
This unusual occurrence is called Pure Neural Leprosy .
Leprosy is a unique infectious disease, which exhibits a wide
spectrum of signs and symptoms .
These various signs and symptoms represent :
1. Patient’s ability to contain the bacilli
2. Bacillis’ ability to adapt as a human parasite
when the patient’s ability fails, he gets clinical form of
disease M. Leprae seldom kills its host .
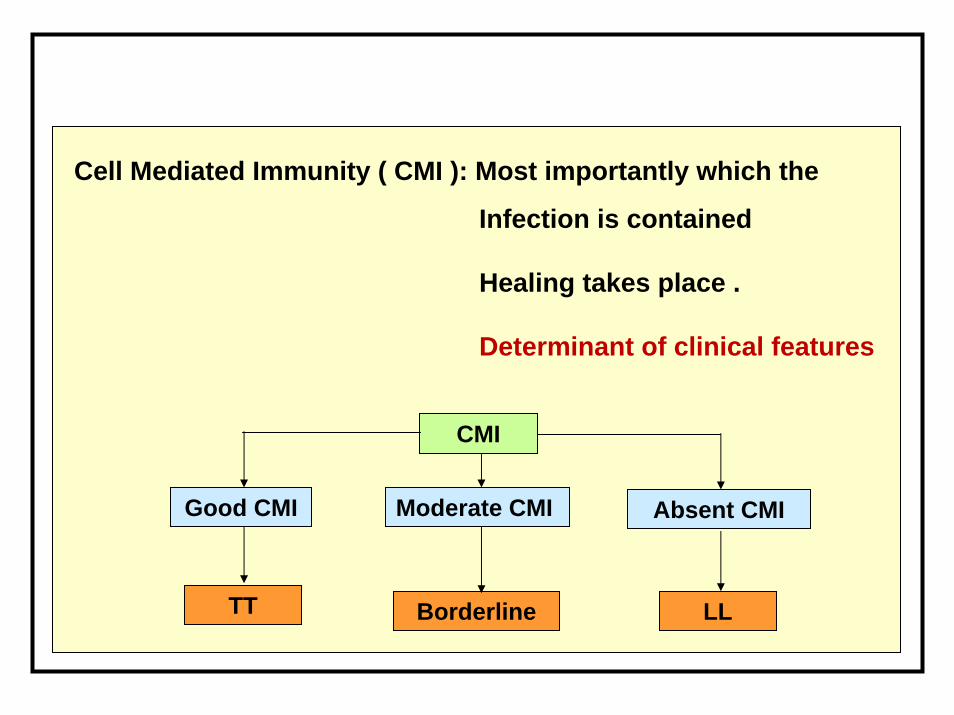
Cell Mediated Immunity ( CMI ): Most importantly which the
Infection is contained
Healing takes place .
Determinant of clinical features
CMI
Good CMI Moderate CMI Absent CMI
Borderline LLTT

CMI to M. Leprae is absent or suppressed : Lepromatous
Leprosy
Bacilli multiply and accumulate:.
If CMI is present : Tuberculoid Leprosy
Infection localized
Tends to heal.
Between these Extremes: Spectrum of Borderline leprosy,

Healthy Person
TT BT BB BL
PBPB MBMB
LL
Indeterminate Leprosy ( Sub clinical Stage
)M.leprae
Clinical Features
1-3 4 to Multiple Multiple Multiple Multiple
Patches with Anesthesia Patches without Anesthesia
Patches or plaques
Nodules
D.Infil.

Healthy Person
TT BT BB BL
PBPB MBMB
No.of Patches
Size of Patches
Border
Symmetry
LL
Indeterminate Leprosy (Sub clinical Stage )
MultipleMultiple4 to multiple1-3 Multiple
Anesthesia
SmallMedium to Small
BigBig Small
-+ / -+++++ -
Slightly ill -defined
Clear at some places
ClearClear Ill - Defined
SymmetricalAsymmetrical Symmetry starts SymmetricalAsymmetrical
M.leprae
Clinical Features

Treatment of Leprosy

Criteria for grouping
S. No. Characteristic PB (Pauci
bacillary)
MB (Multi
bacillary)
1 Skin lesions 1 – 5 lesions 6 and above
2 Peripheral nerve
involvement
No nerve / only
one nerve
More than one
nerve
3 Skin smear Negative at all
sites
Positive at any
site

Treatment of leprosy & std. regimen
•Cap Rifampicine: 10 mg/ kg body weight (bw)
•Cap Clofazimine: 1 mg /kg bw daily and 6 mg/kg bw for monthly dose
•Tab Dapsone: 2 mg /kg bw daily
PB Adult: For people with PB leprosy and 15 years of age or more
MB Adult: For people with MB leprosy and 15 years of age or more
PB child: For people with PB leprosy and 10‐14 years of age
MB child: For people with MB leprosy and 10‐14 years of age
• Safe, minimal side effects and increased patient compliance
• Kills the bacilli
• Stops progress of the disease
• Prevents further complications and reduces chances of relapse
• Renders LAP non‐infectious,
• Reduces transmission and spread of disease
• Reduces chances development of resistance
• Reduces duration of the treatment
• Available in blister pack; easy to dispense, store and take
Advantages of Multi Drug Therapy (MDT)
New case of leprosy: Person with signs of leprosy who have never received treatment before.
Other cases: Under NLEP all previously treated cases, who need further treatment are recorded as “other cases” including migrants
Relapse cases of PB/MB
Reentered for treatment (include defaulters) ‐ Previously treated cases, clinical assessment shows requirement of further treatment
Defaulter: PB 6 pulses in nine consecutive months MB 12 pulses in 18 consecutive months
Indications for prescribing MDT
Referred cases: Patient referred for completion of treatment \Carries a referral slip
Change in classification: Appearance of more lesions
Cases from outside the state & Temporary migration or cross border cases:
Indigenous case: Residing for more than six months likely to stay till completion of treatment,
Indications for prescribing MDT
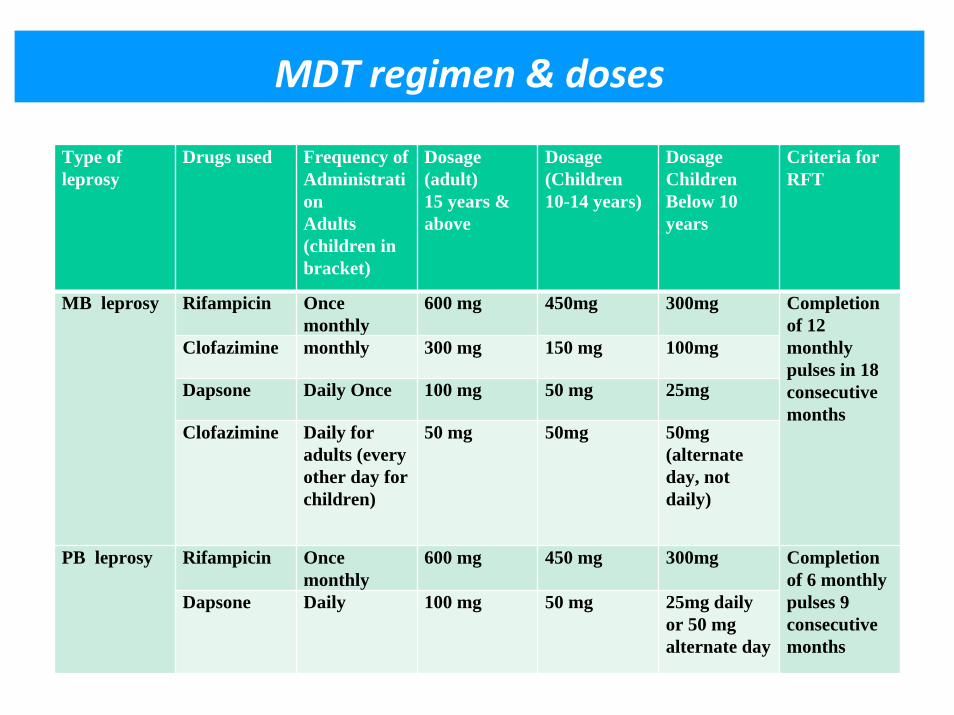
MDT regimen & doses
Type of leprosy
Drugs used Frequency ofAdministrationAdults (children in bracket)
Dosage(adult)15 years & above
Dosage(Children 10-14 years)
DosageChildren Below 10 years
Criteria forRFT
Rifampicin Once monthly
600 mg 450mg 300mg
Clofazimine monthly 300 mg 150 mg 100mg
Dapsone Daily Once 100 mg 50 mg 25mg
MB leprosy
Clofazimine Daily for adults (every other day for children)
50 mg 50mg 50mg (alternate day, not daily)
Completion of 12 monthly pulses in 18 consecutive months
Rifampicin Once monthly
600 mg 450 mg 300mgPB leprosy
Dapsone Daily 100 mg 50 mg 25mg daily or 50 mg alternate day
Completion of 6 monthly pulses 9 consecutive months


MDT Blister packs
First dose of the month
Daily dose from second day
First dose of the month
Doses for alternate day
Daily dose from second day

Before and after treatment

Before and after treatment
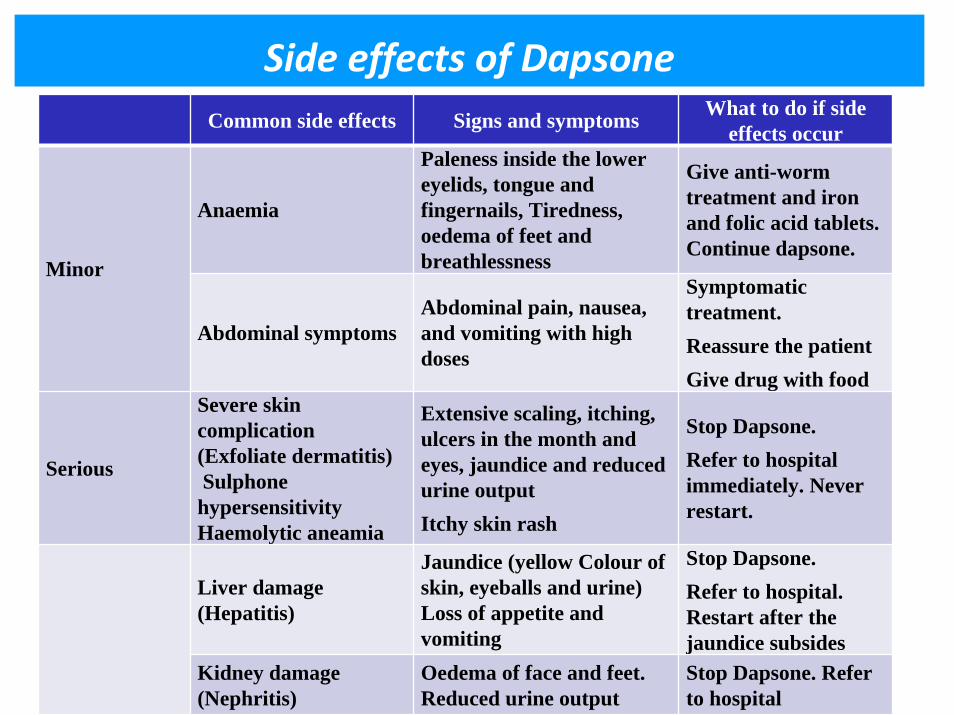
Side effects of DapsoneCommon side effects Signs and symptoms What to do if side
effects occur
Anaemia
Paleness inside the lower eyelids, tongue and fingernails, Tiredness, oedema of feet and breathlessness
Give anti-worm treatment and iron and folic acid tablets. Continue dapsone.
Minor
Abdominal symptomsAbdominal pain, nausea, and vomiting with high doses
Symptomatic treatment. Reassure the patientGive drug with food
Serious
Severe skin complication (Exfoliate dermatitis) Sulphone
hypersensitivity Haemolytic aneamia
Extensive scaling, itching, ulcers in the month and eyes, jaundice and reduced urine output Itchy skin rash
Stop Dapsone. Refer to hospital immediately. Never restart.
Liver damage (Hepatitis)
Jaundice (yellow Colour of skin, eyeballs and urine) Loss of appetite and vomiting
Stop Dapsone. Refer to hospital. Restart after the jaundice subsides
Kidney damage (Nephritis)
Oedema of face and feet. Reduced urine output
Stop Dapsone. Refer to hospital

Side effects of Rifampicin
Side effects Signs and symptoms What to do if side effects occur
Red discoloration of body fluids
Reddish coloration of urine, saliva and sweat
Reassure the patient and continue treatment
Flu like illness Fever, malaise and body ache
Symptomatic treatment
Minor adverse effects
Abdominal symptoms
Abdominal pain, nausea, and vomiting
Symptomatic treatment. Reassure the patientGive drug with food
Hepatitis (liver damage)
Jaundice (yellow colour of skin, eyeballs and urine). Loss of appetite and vomiting
Stop Rifampicin. Refer to hospital. Restart after the jaundice subsides.
Serious adverse effects
Allergy Skin rash or Shock, purpura, renal failure
Stop Rifampicin
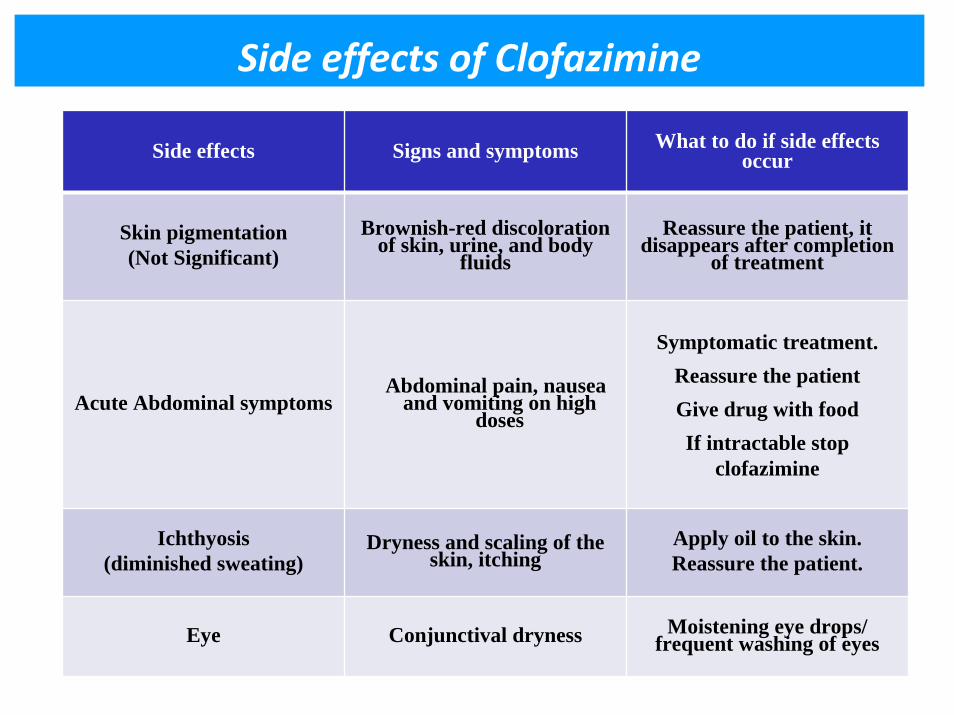
Side effects of Clofazimine
Side effects Signs and symptoms What to do if side effects occur
Skin pigmentation (Not Significant)
Brownish-red discoloration of skin, urine, and body
fluidsReassure the patient, it
disappears after completion of treatment
Acute Abdominal symptomsAbdominal pain, nausea
and vomiting on high doses
Symptomatic treatment. Reassure the patientGive drug with foodIf intractable stop
clofazimine
Ichthyosis(diminished sweating)
Dryness and scaling of the skin, itching
Apply oil to the skin. Reassure the patient.
Eye Conjunctival dryness Moistening eye drops/ frequent washing of eyes

Relapse of Leprosy: confirmed by laboratory.
Drop out cases: Discontinued MDT > 3 months in PB > 6 months in MB leprosy Active signs of leprosy.
Active disease persists / new signs developed within a year,
Suspicion of drug resistance
Criteria to restart course of MDT

Immediate referral: Impairment of visionRed painful eye, Infrequent blinking, Lag‐ophthalmos
Start MDT: if not taken previously
Manage conjunctivitis: frequent cleaning of eye Tropical antibiotic application Rest to the eye by padding.
Eyelashes: < 5 or > 5
Follow up treatment as advised
Self care: After acute phase is over. (Refer section on POD)
No perception of light’ (NPL): Incurably blind
Basic principles for management of ocular lesions