Embed Size (px)
Citation preview

CDE Role in Redesigning Primary Care: Training
MAs in the CCM
Jan Wolfram RN, MN, CDE Shari Gioimo, Medical Assistant
Providence St. Peter Hospital, Olympia, WA August 3, 2007

2
PSPH Medical Assistants & Boldt Diabetes Center

3
CDE’s & Medical Assistants Work Within the CCM

4
Expanded Role of the Medical Assistant
• Data Registry Entry
• Goal Setting
• MA Patient Planned Visits
• Organized Patient Group Visits
• Referrals to Health Specialists (CDE’s)
• Initiate Standing Orders
• Provide FollowUp Phone Calls to Patients
• Foot Checks
• Immunizations
• DM Education Reinforcement

5
Dr. Devin Sawyer

6
Primary Care SelfManagement Goal Cycle

7
Considerations for the MA Curriculum
• American Association of Medical Assistants
• Western Washington Area Health Education Center
• Health Care Assistant Law in the State of Washington

8
More Considerations for the MA Curriculum
• Review of MA Focus Group Results
• Review of MA Curriculums from Local Technical Community Colleges
• Literature Search on MA Training for Diabetes Care
• Review of Published Diabetes Knowledge Surveys for Patients

9
Medical Assistant Learner Characteristics
Characteristics of MAs in Primary Care
• 18 Medical Assistants
• Most Caucasian
• Trained locally
• Significant Family Responsibilities

10
Rapid Cycle Improvement Process
Rapid Cycle Improvement Process
• MAs attended patient DM classes.
• MAs gave feedback.
• PPT slides for MA training edited.
• Classes revised

11
MA Curriculum Matrix
Reporting Conditions X X Goal Setting
X X X X Longterm Complications X X X X Acute Complications X Diabetes Treatments X X X X X Pathophysioloy of Diabetes X X X X X Age, Race, Gender Awareness
X X X X
Registry Data Entry
Telephone FollowUp
Planned Visits
Provider Visit
Group Visit

12
Applied Educational Theories
• Mezirow Transformational Learning – Experience – Reflection – Discussion
• Knowles Adult Learner – Independent Learner

13
Educational Methods
• Cognitive Methods: Lectures, Discussion, PPT slides
• Behavioral Methods: RolePlay, Phone Scripting, Computer Practice; Diaries for Food, Blood Glucose, & Exercise
• Kinetic Methods: SelfBlood Glucose Monitoring, Glucose Gel and Tablet Tasting, Injection of Normal Saline

14
Shari Gioimo, Medical Assistant
• Active Participant in the Diabetes Initiative
• National Consultant to Clinics Expanding the MA Role
• Certified Trainer in Chronic Disease Self Management

15
Clinical Life before the MA Expanded Role
• The MA traditionally “roomed” and “vitaled” the patient prior to the PCP visit
• The MA was dependent on the PCP direction
• The MAPatient Relationship was not well developed
• The MA role was to perform tasks and keep the office flow moving

16
Delivery System Design
• Individual “Planned Visits” with MA and Patients
• MA Organized Group Visits with PCP and Patients

17
Decision Support
• Standing Orders:
– Introduce the Idea of SelfManagement
– Laboratory (Tests A1c, etc.)
– Immunizations
– Foot Checks
– Referral to CDEs and specialists

18
SelfManagement Support
• Goal setting using the Transtheoretical Model
• Followup phone calls to “checkin”
• Goal Trotter’s Walking Club
• Newsletters

19
Clinical Information Systems
Data Input into CDEMS Registry
– SelfManagement Goals – A1c – Lab Results – Immunizations – Eye Exams – Smoking Cessations – Medications – Vital Signs

20
Interaction with the Community
• Consult with local CDE’s regarding questions on diabetes.
• Consult with other community agencies and programs such as the Food Bank, YMCA, and Senior Centers.

21
Health Systems Support
• MAs give administrative leaders and
doctors feedback.

22
Clinical Life After the MA Training • MAPatient relationship is better.
• MA patient care is more organized.
• MAs receive more respect from team members.
• MAs reinforce patient education.
• MA retention rate is higher.

23
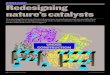
Percent of Patients with SelfManagement Goals
Percent of Patients with Documented SelfManagement Goals
6.8 9.2 12.6 12.4 12.0 11.3 11.2 12.4 10.4
18.8 16.7 19.0 20.6 18.6 19.4 19.2 20.1 21.5 21.6
24.7 25.9 25.5 27.1
36.7
46.9
57.2 58.5 61.5 61.2 62.7
66.7 68.6 72.6 73.8
76.9
0.0 10.0 20.0 30.0 40.0 50.0 60.0 70.0 80.0 90.0 100.0
perc
ent
Goal = 70%

24
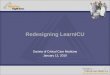
Quality of Patient SelfManagement Goals

25
Quality of SelfManagement Goals Over Time
Clinic SMG By Date
1.0
2.0
1.0 1.0 1.5
4.2 4.2 4.0
3.4
4.0 3.6
3.2
3.8
3.1
3.6 3.5
2.6 2.9
2.4 2.0 2.0 2.0
3.4
1.6 2.0 2.0
1.3
2.0 1.5
1.0 1.0
2.0
1.0 1.0
3.0
2.0
0
1
2
3
4
5
Mar01
May01
Jul01
Sep01
Nov01
Jan02
Mar02
May02
Jul02
Sep02
Nov02
Jan03
Mar03
May03
Jul03
Sep03
Nov03
Jan04
Mar04

26
Opportunities • The MA Curriculum A Work in Process
• CDE’s deliver MA training in local settings.
• Business expansion with referrals.
• Expand resource base for the CDE’s and the Family Medicine Teams.

28
PSPH Medical Assistants & Boldt Diabetes Center