Embed Size (px)
Citation preview

ARTHROSCOPICALLV ASSISTED POSTERIOReRUCIATE LIGAMENT RECONSTRUCTION:
A SURGICAL ATLAS
The technique orientation of Operative Techniques inSports Medicille lends itself well to the presentation of posterior cruciate ligament (PCL) reconstruction in a coloratlas format. This brief section demonstrates with colorillustrations the technical details of arthroscopically assisted PCL reconstruction followed by radiographs thatdemonstrate fixation options. Many of the details included in the following illustrations reflect a summation
of techniques presented by the various contributors inthis issue. By presenting this in an atlas format, it is theguest editor's intent to provide the reader with a quickreference guide using uniform color illustrations that canbe used for teaching purposes.
Daniel E. Cooper, MDGuest Editor
Operative Techniques in Sports Medicine, Vol 1, No 2 (April), 1993: pp 125·128 125

/
/
/
'lI.
,'/ .j/ // ,/ ,/, /
Auto oUS fa 1 I ri1 /Patellar Pa I r • ,I s /
Te d Te / ,/'I
~/.
/ "/ //
,//
Moni tor # 1
I
Surgeon #2
Surgeon #1
Mon itor 1t2
Fig 1. Setup for arthroscoplcally assisted posterior cruclateligament (PCL) reconstruction. The primary surgeon is labeled no. 1, and the assisting surgeon is labeled no. 2. Thisdrawing depicts a right knee PCl reconstruction. The end ofthe table may be extended and a bolster used tor flexion.Alternately, the end of the table may be dropped and thethigh placed in a thigh holder.
Scope n1 Scope 112
Fig 3. Artistic representation of prepared grafts tor PCl reconstruction. According to a recent survey by Bach, autologous patellar tendon is the most commonly used graft. Allograft patellar tendon and Achilles tendon are also commonly used grafts. Although it Is Ideal to use autologoustissue, the disadvantages of potential short length and increased morbidity can affect the surgeon's decision regarding use autologous patellar tendon graft. Both allograft patellar tendon and allograft Achilles tendon allow for increasing the diameter of the graft by tUbularizing the graft, asdemonstrated in the diagram. Additionally, the bone plugson the tibial side may be left somewhat longer than with anautologous graft. This enhances incorporation. The allograftAchilles tendon Is passed through bone tunnels more easilythan patellar tendon bone-tendon-bone grafts. However, thismay be offset by less ideal fixation.
Scope # 1-
Scope 112
Scope ;11
o
cope 112
cope #1
Scope 2
Rig t Leg
Fig 2. Scope no. 1 depicts the anterolateral portal, which isthe primary arthroscopic portal for a PCl reconstruction.Scope no. 2 demonstrates the posterior medial portal, whichIs used as an accessory arthroscope portal and working portal. The inserts depict the arthroscopic anatomy in the setting of a torn PCL. Initially, 30° arthroscopes are usedthrough each portal for visualization. Use of a motorizedshaver Is employed through an anterior medial portal to clearthe synovlum from around the PCl to facilitate visualizationthrough both arthroscopes.
Fig 4. After debridement of the PCl remnants with the motorized shaver, an angled curette and angled periosteal elevator are used to debride the PCl Insertion on the tibia. ThisIs visualized through both portals to demonstrate adequatedebridement of the soft tissue for proper tunnel placement.
ope 1
70
cope 2 -
cope 1Scope "2
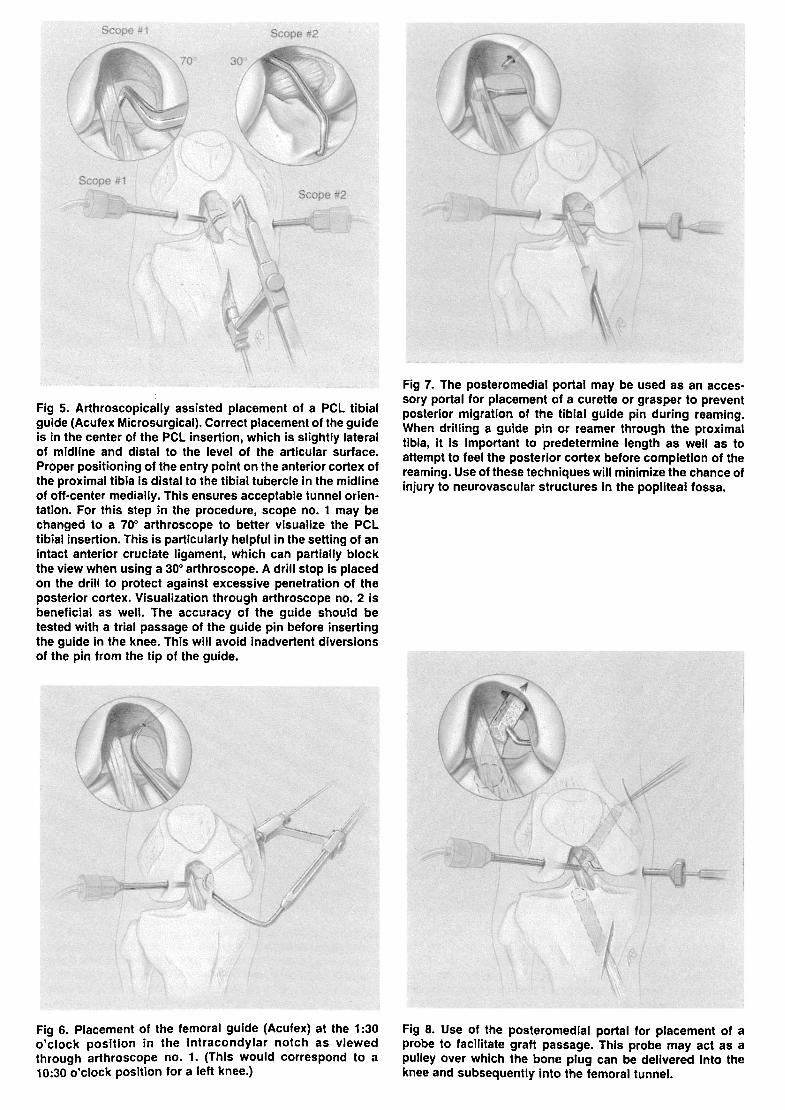
Fig 5. Arthroscopically assisted placement of a PCl tibialguide (Acufex Microsurgical). Correct placement of the guideis in the center of the PCl insertion, which is slightly lateralof midline and distal to the level of the articular surface.Proper positioning of the entry point on the anterior cortex ofthe proximal tibia is distal to the tibial tubercle in the midlineof ott-center medially. This ensures acceptable tunnel orientation. For this step in the procedure, scope no. 1 may bechanged to a 70° arthroscope to better visualize the PCltibial insertion. This is particularly helpful in the setting of anintact anterior cruclate ligament, which can partially blockthe view when using a 30° arthroscope. A drill stop is placedon the drill to protect against excessive penetration of theposterior cortex. Visualization through arthroscope no. 2 isbeneficial as well. The accuracy of the guide should betested with a trial passage of the guide pin before insertingthe guide in the knee. This will avoid inadvertent diversionsof the pin from the tip of the guide.
Fig 7. The posteromedial portal may be used as an accessory portal for placement of a curette or grasper to preventposterior migration of the tibial guide pin during reaming.When drilling a guide pin or reamer through the proximaltibia, it Is important to predetermine length as well as toattempt to feel the posterior cortex before completion of thereaming. Use of these techniques will minimize the chance ofinjury to neurovascular structures in the popliteal fossa.
-
Fig 6. Placement of the femoral guide (Acufex) at the 1:30o'clock position in the Intracondylar notch as viewedthrough arthroscope no. 1. (This would correspond to a10:30 o'clock position for a left knee.)
Fig 8. Use of the posteromedial portal for placement of aprobe to facilitate graft passage. This probe may act as apulley over which the bone plug can be delivered Into theknee and subsequently into the femoral tunnel.
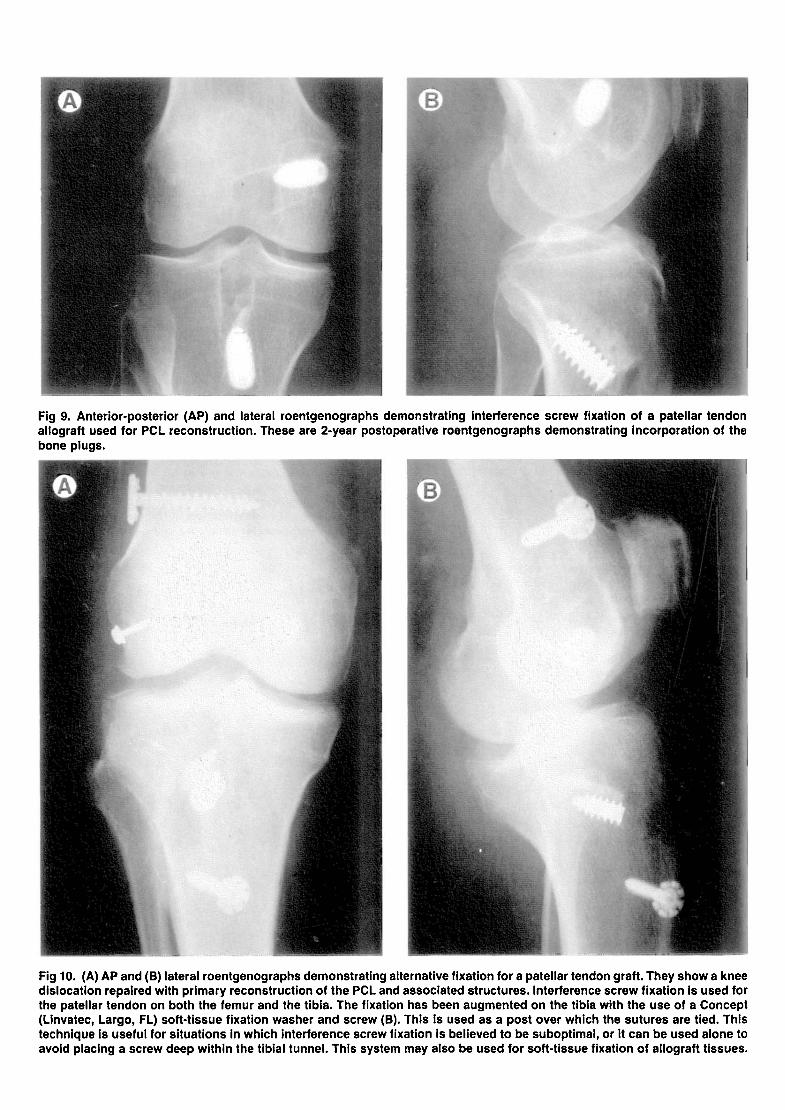
Fig 9. Anterior-posterior (AP) and lateral roentgenographs demonstrating interference screw fixation of a patellar tendonallograft used for PCL reconstruction. These are 2-year postoperative roentgenographs demonstrating incorporation of thebone plugs.
Fig 10. (A) AP and (B) lateral roentgenographs demonstrating alternative fixation for a patellar tendon graft. They show a kneedislocation repaired with primary reconstruction of the PCL and associated structures. Interference screw fixation Is used forthe patellar tendon on both the femur and the tibia. The fixation has been augmented on the tibia with the use of a Concept(Linvatec, Largo, FL) soft-tissue fixation washer and screw (B). This Is used as a post over which the sutures are tied. Thistechnique Is useful for situations In which interference screw fixation Is believed to be suboptimal, or it can be used alone toavoid placing a screw deep within the tibial tunnel. This system may also be used for soft-tissue fixation of allograft tissues.




























