Embed Size (px)
Citation preview

Ariel Weissman, MD IVF Unit, Dep. Ob/Gyn, Wolfson Medical Center, Holon Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv
Israel
Best stimulation protocol for freeze all cycles

No conflict of interest to declare!

• Change of practice (routine)
• PGD/PGT-A (PGS)
• Fertility preservation (medical)
• Elective fertility preservation (EFP)
• Oocyte donors (fresh/banking)
Indications for elective cycle segmentation – freeze all

Key players in controlled ovarian stimulation (COS) for freeze all:
May be different compared to fresh cycles All should be taken into consideration Little is known….
• Size of the cohort • Timing the start of COS • Regimen of pituitary suppression used • Type of gonadotropins given • Monitoring during COS • Type and dose of ovulatory trigger

Goal of COS for freeze-all cycle
• To retrieve the optimal (maximal?) number of oocytes
• That can be safely retrieved

Factors affecting the success of freeze-all cycles
• Size of the cohort
• Timing the start of COS
• Regimen of pituitary suppression used
• Type of gonadotropins given
• Monitoring during COS
• Type and dose of ovulatory trigger

Success of IVF is clearly dependent on the size and quality of the oocyte cohort
Does the size of the cohort affect oocyte quality?


Figure 11
Frequency of chromosome abnormalities in human blastocysts analyzed by NGS
Munne S. Forty Years of IVF. Fertil Steril 2018.
n > 100,000 embryos.
Cooper Genomics data, with mosaics not reported
(<40% classified as normal and ≥40% as abnormal)

Advantages of the development of very large follicular cohorts
Shapiro and Yding Andersen, Fertil Steril 2015
• Having multiple embryos for cryopreservation • Greater opportunity for pregnancy in subsequent FET cycles • Reduce the chance of the patient ever needing another cycle of
ovarian stimulation, even if a large family is desired • Increase the chance of having euploid embryos or genetically normal embryos for PGT-A and PGD • Enhanced ability to obtain sufficient numbers of eggs for: Egg-sharing Egg-banking Embryo donation

Drawbacks of the development of very large follicular cohorts • Concomitant high E2 and P levels
• Theoretical concerns and unknown risks associated with these extremes • May elicit mechanical, physiologic, and hormonally initiated complications
The incidence of thromboembolic events Magnusson et al., Hum Repord 2018

Figure 2
Reproductive BioMedicine Online 2017 34, 345-353DOI: (10.1016/j.rbmo.2017.01.010)
Rates of live birth and ovarian hyperstimulation syndrome with increasing oocyte yield
Based on Society for Assisted Reproductive Technology (SART) data from 2008–2010
Steward et al., Fertil Steril 2014

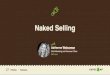
Figure 1
Cumulative and fresh LBRs according to the number of oocytes retrieved Light blue bars: fresh live birth probability; Dark blue bars: cumulative live birth probability; Gray line: freeze-all rate.

2007-2013 overall survival : 92.7% (38,087/ 42,152) oocytes
How many eggs for a baby?
Cobo et al., Fertil Steril 2015

Survival and clinical outcomes in patients aged ≤35 and ≥36 at time of vitrification
Patients (n) Cycles (n) Survival rate (%)
OPR/ET n(%) LBR/patient n (%)
≤35 32 41 94.6 21/39 (53.9) 16/32 (50)
≥36 105 150 82.4 27/118 (22.9) 24/105 (22.9)
Total 137 191 85.2 48/157 (30.5) 40/137 (29.2)
Cobo et al., Fertil Steril 2016
• 1468 patients had 14,415 (6.7) oocytes vitrified • Mean age 37.2 years • 137 returned to use their oocytes


• A model to determine the proportion of mature oocytes that fertilize and then form blastocysts
as a function of age, using women with presumably normal ovarian reserve
• Age-specific probabilities of euploidy were estimated from 14 500 PGS embryo results
• Assuming survival of thawed oocytes at 95% for women <36 y and for egg donors,
and 85% for women ≥36 y, and 60% live birth rate per transferred euploid blastocyst,
probabilities of having at least one, two or three live birth(s) were calculated.

The probability of having a live birth with a given number of mature oocytes:
The probability that one mature oocyte will become a blastocyst [p(blast)] for any given patient age (years, y):
For example, patients each having eight mature oocytes, would be predicted to have, on average blastocysts 34 years - 3 37 years – 2 42 Years - one
Goldman et al., Hum Reprod 2017

Live birth predictions by age and number of mature oocytes retrieved
Each curve shows the percent likelihood that a patient of a given age will have at least one live birth
according to Equation 2, based on the number of mature oocytes retrieved and frozen.

• More usable/euploid blastocysts with larger cohorts • Higher cumulative live birth rates with larger cohorts
A cohort of ~20 oocytes would be a balance between safety and efficacy Age should guide the target for the final number of oocytes
Conclusion: Size of the cohort
Embryonic aneuploidy rates do not differ: • In natural cycles/mild stimulation/intense stimulation Data do not support a causative role for gonadotropin stimulation in embryonic aneuploidy

Factors affecting the success of freeze-all cycles
• Size of the cohort
• Timing the stimulation start
• Regimen of pituitary suppression used
• Type of gonadotropins given
• Monitoring during COS
• Type and dose of ovulatory trigger

Morphologic and endocrinologic changes associated with two waves (a–c)
and three waves (d–f) of follicle development during the human menstrual cycle
Ovarian antral folliculogenesis during the human menstrual cycle
.91-73: 18;2012 Hum Reprod Update. et al., Baerwald




Conventional group
Late follicular phase group
Luteal phase group
n 50 50 50
Stimulation duration (days)*
8.9±1.4 11.4±3.1 10.9±3.4
hMG daily dose (IU)* 149.2±14.6 159.9±11.9 169.4±28.1
E2 level on COS start (pg/mL)*
39.9±21.2 154.4±120.3 141.1±94.9
Oocytes retrieved (n) 6.6±3.8 5.9±4.3 5.9±4.2
MII oocytes (n) 5.7±3.6 5.2±3.7 5.2±3.9
Cleaved embryos (n) 4.8±3.0 4.0±2.9 4.0±3.0
Cryopreserved embryos (n) 2.5±2.0 2.1±2.2 2.5±2.5
Cancellation rate (%) 10 22 16
Patients with FET 33 27 30
No of transferred embryos (mean)
1.8 1.7 1.7
Ongoing PR (%) 16/41 (39) 13/33 (39.4) 12/36 (33.3)

The paradigm that COS should start at the early follicular phase may not be true for freeze all cycles
• The effects of elevated P4 levels on oocyte quality and developmental competence • The effects of random start COS on embryo quality and implantation potential • The short and long term effects of random start COS on neonatal outcome
Random start could be a viable option that should be further explored…
Conclusion: Timing the stimulation start

Factors affecting the success of freeze-all cycles
• Size of the cohort
• Timing the stimulation start
• Regimen of pituitary suppression used
• Type of gonadotropins given
• Monitoring during COS
• Type and dose of ovulatory trigger

Severe OHSS Ongoing pregnancy/Live birth rate
No. of
RCTs
OR= 0.43
95% CI 0.33-0.57
OR= 0.86
95% CI 0.69-1.08
45 Al-Inany et al. Cochrane Colab. 2011
Long Agonists vs. GnRH Antagonists: meta-analysis of RCTs:
Antagonist Agonist
vs.

Weighted mean difference for the number of retrieved oocytes.
Heterogeneity: τ2 = 2.91; χ2 = 20.49; df = 6 (P=.002); I2 = 71%.
Test for overall effect: Z = 0.70 (P=.48).

Risk ratio for recipient ongoing pregnancy rate per randomized donor (studies with 1:1 donor-recipient ratio).
Heterogeneity: χ2 = 1.64; df = 4 (P=.80); I2 = 0. Test for overall effect: Z = 1.57 (P=.12).

• Retrospective study
• 2817 embryos from 400 couples undergoing oocyte donation
• GnRH antagonist + GnRH agonist trigger (n = 2101)
• GnRH agonist + hCG trigger (n = 716)
• No significant differences in morphokinetic characteristics
• No significant differences in implantation, clinical pregnancy and miscarriage rates

Conclusion: regimen of pituitary suppression used
GnRH antagonists offer: • Similar oocyte number and live birth rates • Improved safety compared with the long GnRH-a protocol GnRH antagonist regimens should be preferably used

Factors affecting the success of freeze-all cycles
• Size of the cohort
• Timing the stimulation start
• Regimen of pituitary suppression used
• Type of gonadotropins given
• Monitoring during COS
• Type and dose of ovulatory trigger

Type of gonadotropin used
• To date there seems to be no clear benefit obtained by combining LH and FSH in unselected normogonadotrophic patients
Kolibianakis et al., Hum Repord Update 2006 Mochtar et al., Cochrane Database Syst Rev 2007
• The physiologic role of LH during the follicular phase of a natural cycle is unquestionable • Its impact during a COS cycle remains controversial

LH supplementation in a donor oocyte program
Group I: 225 IU r-hFSH + GnRH antagonist (n=20) Group II: 225 IU r-hFSH + 75 IU r-hLH + GnRH antagonist (n=22)
Acevedo et al., Fertil Steril 2004

LH supplementation in a donor oocyte program
Acevedo et al., Fertil Steril 2004
r-hFSH r-hFSH+r-hLH P value
R-hFSH (IU) 1807±97 1738±407 NS
E2 on hCG day (pg/mL)
989.6±597 1596±988 NS
Follicles (hCG day) 14.2±2/6 12.3±6.4 NS
Fert. rate (%) 71 83 <0.05
MII oocytes (%) 71 80 <0.05
G1 embryos (%) 3 17 <0.05
Pregnancy/ET (%) 43 57 NS
Biochem preg (%) 28 10 <0.05
CPR (%) 30 51 NS
IR 15 35 <0.05

Recombinant hLH supplementation appears to be beneficial in two subgroups of patients: 1) women with adequate prestimulation ovarian reserve parameters and an unexpected hyporesponse to r-hFSH monotherapy 2) women 36–39 years of age. No evidence that r-hLH is beneficial in young (<35 y) normoresponders cotreated with the use of a GnRH antagonist.

0
3/15
6/15
9/15
12/15
FSH FSH+LH
Which gonadotropins to use?
Respondents: • Brussels • Edinburgh • Hamburg • Istanbul • London • Madrid • New York • New Jersey • New Delhi • New Haven • Paris • Tel Aviv • Thessaloniki
Personal communication

Factors affecting the success of freeze-all cycles
• Size of the cohort
• Timing the stimulation start
• Regimen of pituitary suppression used
• Type of gonadotropins given
• Monitoring during COS
• Type and dose of ovulatory trigger

Monitoring during COS
• Progesterone
• Estradiol

ORs for pregnancy achievement in women with PE when
compared with those without PE
Venetis et al. Hum. Reprod. Update 2013;19:433-457

Odds ratios for achievement of pregnancy in women undergoing
(a)FET and (b) oocyte donation after a fresh cycle
with or without progesterone elevation
Venetis et al. Hum. Reprod. Update 2013;19:433-457
No effect for progesterone elevation in frozen-thawed ET cycles and in cycles with donated oocytes

Poor responders
High responders
Intermediate responders
PLoS ONE 9(6): e100011. doi:10.1371/journal.pone.0100011

N= 986 N= 4236

Supraphysiological estradiol levels and embryo quality in oocyte donation cycles
Pena et al., Hum Reprod 2002
Peak E2 (pg/mL) <1500 1500-3000 >3000
A B C
n 79 141 110
Oocytes retrieved 10±0.5 16.2±0.5** 26.2±0.8**§
2pn embryos 5.9±0.3 9.5±0.4** 15.5±0.6**§
Fert rate (%) 60 59 59
Avr. embryo score 27.1±1.2 30.2±0.8** 31.5±0.8**
Embryos cryopreserved
1.1±0.2 3.3±0.3** 6.4±0.5**§
Implantation rate (%) 17.4 19.3 24.5*
CPR/ET (%) 38.0 41.2 47.7
Ongoing/del/ET (%) 33.8 34.6 44
* p<0.05 vs. group I ** p<0.005 vs group I § p <0.005 vs group II

Supraphysiological estradiol levels and embryo quality in oocyte donation cycles
Pena et al., Hum Reprod 2002
Sustained supraphysiological E2 levels do not adversely affect the quality of developing oocytes and embryos

Monitoring during COS
• Progesterone: Late follicular phase P elevation Might be a problem….
• Estradiol: High late follicular phase E2 levels Not a problem…

Factors affecting the success of freeze-all cycles
• Size of the cohort
• Timing the stimulation start
• Regimen of pituitary suppression used
• Type of gonadotropins given
• Monitoring during COS
• Type and dose of ovulatory trigger

Types of ovulatory triggers currently in use
• hCG
• GnRH agonist trigger
• Dual trigger (hCG+agonist)

Youssef et al., 2014, Issue 10
GnRH agonist versus HCG for oocyte triggering in antagonist ART cycles
OHSS risk

GnRH agonist versus hCG for oocyte triggering in antagonist ART cycles
Youssef et al., 2014, Issue 10
Ongoing pregnancy rate

Types of GnRH-a for ovulation triggering:
• Triptorelin SC 0.1-0.4 mg
Bodri et al., Fertil Steril 2009
Hernandez et al., Fertil Steril 2009
Papanikolaou et al., Fetil Steril 2011
• Buserelin SC 0.5 mg
Humaidan et al., Hum Reprod 2005
Humaidan et al., Fertil Steril 2010
• Intranasal buserelin 0.2 mg
Pirard et al., Hum Reprod 2006
• Leuprolide acetate (LA) SC 1- 4 mg
Engmann et al., Fertil Steril 2008
Castillo et al., RBM Online 2010
Chang et al., Fertil Steril 2016
Pereira et al., RBM online 2017
• Intranasal Nafarelin acetate

GnRH agonist trigger in Asian oocyte donors: a dose-finding study
63-356:105Feb;2016 Fertil Steril.TN et al., Vuong The primary end point: number of MII oocytes

GnRH agonist trigger in Asian oocyte donors: a dose-finding study
Reproductive outcome in recipients
63-356:105Feb;2016 Fertil Steril.TN et al., Vuong
Group A Decapeptyl 0.2mg
Group B Decapeptyl 0.3mg
Group C Decapeptyl 0.4mg
P
n 20 21 20
No. of ET 2.6±0.5 2.8±0.4 2.7±0.5 NS
CPR (%) 60 47.6 45 NS
Ongoing PR (%) 55 38.1 35 NS
IR (%) 33.3 26.1 17.5 NS

Summary: Dose finding studies for the GnRH agonist trigger
• A dose of 0.2 mg of triptorelin seems highly effective
• No dose finding studies available for other GnRH-a

Dual trigger GnRH-agonist and a standard dosage of hCG
Significantly higher proportion of mature oocytes in patients with a previous history of >25% immature oocytes Griffin et al., Fertil Steril 2014
Lin et al., Fertil Steril 2013
In normal responders GnRH-antagonist IVF cycles: • More oocytes MII oocytes • Significantly improved implantation, CPR and LBR • Improved endometrial receptivity?
N=187 n=191
for the FSH surge at the time of final oocyte maturationbiological role Potential

Dual trigger with GnRHa and varying doses of hCG increases the blastulation rate amongst high responders
Werner et al., ASRM 2014
The addition of GnRH-a to hCG when triggering high responders increases usable blastocyst yield.

Dual trigger versus low-dose hCG for patients with high peak E2
Melnick et al., ASRM 2014
Higher oocyte yield up to the age of 42Y
CPR/ET CPR/cycle Oocytes n CPR/ET CPR/cycle Oocytes n Age
54.7 50.1 18.1±9 131 55.9 54.5 *13.5±5.9 355 <35
63 48.7 16±7.8 76 52 47.2 *12.7±5.4 197 35-37
63.2 50 14.8±7.2 72 43.4 39.5 *12±5.3 182 38-40
43.3 37.1 16. ±6.3 35 40.5 38.6 *12±4.8 88 41-42
29.1 26.9 12.7±4.6 26 26.8 24.6 11±5 61 >42
3300 IU hCG 1500 IU hCG+ LA 2 mg

Dual trigger
Potential clinical role for the FSH surge at the time of final oocyte maturation: • Higher proportion of mature oocytes • Higher usable blastocyst yield • Improved implantation, CPR and LBR? • Improved endometrial receptivity?
Disadvantages of the dual trigger • Increased risk for OHSS • Inconvenience • Increased cost

Criteria for GnRH agonist trigger administration
247 patients undergoing IVF after pituitary down-regulation with GnRH agonists Divided into three groups: Group I (n= 79): hCG was administered when the mean diameter of the leading follicle ≥18 mm, at least two other follicles were 14 mm in diameter, and serum E2 levels were consistent with the number of follicles observed on ultrasound. Group II (n= 84) : hCG was administered 1 day later Group III (n 84) : hCG was administered 2 days later
No significant advantage in the precise timing of hCG administration was observed
Tan et al., Fertil Steril 1992

Criteria for GnRH agonist trigger administration 413 patients undergoing IVF with fixed GnRH antagonist protocol divided into two groups:
Group I (n= 208): received 10,000 IU of hCG as soon as at least three follicles were ≥ 17 mm (early-hCG group)
Group II (n= 205) : 2 days later after this criterion was met (late-hCG group)
Kolibianakis et al., Fertil Steril 2004
P value Late-hCG group Early-hCG group
NS 12.4±0.5 11.2±0.5 No. of oocytes
NS 57.3±1.7 56.6±1.9 Fertilization rate
NS 2.0±0.1 2±0.1 No. ET
0.027 25 35.6 Ongoing PR/OPU (%)
0.024 27.7 39.2 Ongoing PR/ET (%)
0.009 15.1 22.6 Ongoing IR (%)
Prolongation of the follicular phase in patients stimulated with rec-FSH and GnRH antagonists for IVF: • Does not affect oocyte or embryo quality • Is associated with a significantly lower ongoing pregnancy rate.

Criteria for GnRH agonist trigger administration

Criteria for GnRH agonist trigger administration
Should we use the same triggering criteria as for fresh GnRH antagonist cycles?
Currently unknown (no data available)

Factors affecting the success of freeze-all cycles: Summary and (my) best estimate
• Size of the cohort Age-related (~20 oocytes) • Regimen of pituitary suppression used GnRH antagonist • Type of gonadotropins given FSH (LH for unexpected hyporesonders and patients >35?) • Monitoring during COS E2 not so important P may be important • Type and dose of ovulatory trigger GnRH agonist (Dual?) • Trigger criteria? Unknown