Embed Size (px)
Citation preview

ANTEROLATERAL THIGH FLAP PEDICLE FOR INTERPOSITIONARTERY AND VEIN GRAFTS IN HEAD AND NECKRECONSTRUCTION: A CASE REPORT
BERNARDO BIANCHI, M.D., CHIARA COPELLI, M.D.,* SILVANO FERRARI, M.D., ANDREA FERRI, M.D., and ENRICO SESENNA, M.D.
The selection of receiving vessels is one of the most critical steps in ensuring a successful outcome in microvascular surgery. The use ofinterposition grafts in microsurgery offers the surgeon valuable options when the free flaps vascular pedicles are too short to be anasto-mosed directly to the recipient vessels. Here, we present a case in which artery and vein grafts were used in microsurgical reconstructionof an anterior maxillary defect with an iliac free flap. As donor vessels, we used the descending branch of the lateral circumflex femoral ar-tery and one of the two venae commitantes. The flap survived without major or minor complications. The anterolateral thigh flap pedicleallowed us to harvest safe, reliable grafts easily, with a suitable vessel length and diameter. VVC 2008 Wiley-Liss, Inc. Microsurgery 29:136–137, 2009.
With advances in microvascular surgery, free tissue
transfer is becoming the reconstructive option of choice
for many head and neck defects. One of the most critical
steps in ensuring a successful outcome is the selection of
safe, accessible vascular inflow and outflow sources capa-
ble of sustaining microvascular composite tissue-transfer
viability. Factors that may limit the surgeon’s options are
prior ipsilateral radical neck dissection, regional metasta-
sis, or atherosclerosis due to advanced age or preopera-
tive radiation therapy. Sometimes, the particular flap that
is selected has intrinsic restrictions in terms of the caliber
and length of the donor vessels. If the free flap vascular
pedicle is too short to be anastomosed to the recipient
vessels directly, a segmental graft is needed to bridge
this gap. Here, we present a case involving the use of a
simultaneous artery and vein graft performed in the
microsurgical reconstruction of an anterior maxillary
defect with an iliac free flap.
SURGICAL TECHNIQUE
A 65-year-old woman was admitted to our department
with an infiltrative T4 high-grade squamous cell carci-
noma of the anterior maxilla extending to the right nasal-
cheek skin.
The patient underwent combined surgery that con-
sisted of wide excision of the tumor mass and immediate
flap reconstruction. The surgical defect was reconstructed
through an iliac free flap. Because of the short pedicle,
the flap was anastomosed to the left facial vessels via a
vein and artery graft. As donor vessels, we used the de-
scending branch of the lateral circumflex femoral artery,
which arises from the deep femoral trunk, and one of the
two venae commitantes. The graft was harvested through
a 7-cm incision made on the proximal half of a line
drawn between the anterior superior iliac spine and the
superolateral border of the patella (see Fig. 1). Follow-
ing the technique used to identify the anterolateral thigh
flap pedicle, the rectus femoris muscle was identified
along with the intermuscular septum. Coursing obliquely
over the vastus lateralis muscle, the vascular pedicle
was seen and isolated (Fig. 2). An artery and vein seg-
ment 8 cm in length was harvested and anastomosed in
an end-to-end manner proximal to the flap artery and
vein, respectively, and distally to the facial artery and
vein in the left neck. The thigh incision was closed
directly.
The iliac crest flap survived well, without major or
minor postoperative complications at either the donor or
recipient site.
DISCUSSION
Despite recent advances, recipient vessel selection
remains one of the more critical steps in ensuring a suc-
cessful outcome in microvascular surgery. A short free
flap pedicle or a vessel-depleted neck may limit the
reconstructive options of head and neck defects.
The use of interposition grafts in microsurgery has
been reported in the presence of free flap vascular pedi-
cles too short to be anastomosed to the recipient vessels
directly.1–3 To achieve a tension-free vascular pedicle
that will accommodate the full range of motion of the
head and neck, vein grafts from the saphenous or ce-
phalic system are commonly considered the most versa-
tile and readily available.1–3 Nevertheless, they have
larger diameters than the iliac flap pedicle and the recipi-
ent vessels, which sometimes makes microanastomosis
Unita Operativa di Chirurgia Maxillo-Facciale, Dipartimento Testa-Collo,Ospedale Maggiore, Via Gramsci, 14-43100 Parma (Pr), Italy
*Correspondence to: Chiara Copelli, M.D., Unita Operativa di Chirurgia Max-illo-Facciale, Dipartimento Testa-Collo, Ospedale Maggiore, Via Gramsci,14-43100 Parma (Pr), Italy. E-mail: [email protected]
Received 27 June 2008; Accepted 9 August 2008
Published online 22 October 2008 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/micr.20566
VVC 2008 Wiley-Liss, Inc.

more difficult to perform. In the case described here, we
decided to use the descending branch of the lateral cir-
cumflex femoral artery and its two venae commitantes to
bridge the gap between the pedicle of an iliac crest free
flap and the neck vessels in reconstruction of an anterior
maxillary defect. Based on the cardiac literature, the pat-
ency rates of arterial conduits are far superior to those of
vein grafts.4,5 Moreover, some authors have reported that
high-flow vein grafts, such as the cephalic and saphenous,
have higher risks of acute thrombosis and hemorrhagic
complications due to hyperperfusion.6
The descending branch of the lateral circumflex femo-
ral artery has already been applied to vascular bypass
grafting by neuro- and cardiac surgeons.4,7 Its use for
coronary bypass has been associated with high rates of
patency and a low incidence of spasm.4
Following the technique used to identify the anterolat-
eral thigh flap pedicle, we harvested grafts with lengths
from 8 to 16 cm.8–10 The diameter of the artery can vary
from 1 to 2 mm and the two venae commitantes have
diameters slightly larger than the artery.8–10 The use of the
grafts allowed the full length and greatest caliber of the do-
nor artery to be used. We could take it closer to the source,
resulting in a larger lumen. The artery diameter was similar
to those of both the flap and facial artery. The presence of
two venae commitantes allowed the choice of the one with
the better diameter to reduce discrepancies between the do-
nor and recipient vessels. Furthermore, this allowed the
possibility of a second venous anastomosis, increasing the
venous outflow and reducing the risk of thrombosis.
The anterolateral thigh flap pedicle allowed us to eas-
ily harvest safe and reliable arterial and venous grafts of
suitable vessel length and diameter. In this way, we
obtained safe vascular inflow and outflow sources without
morbidity at either the donor or receiving site. In our
reconstruction of a maxillary defect with an iliac free
flap, the descending branch of the lateral circumflex fem-
oral artery and its two venae commitantes had good
matches with both the small vessels of the flap pedicle
and the larger recipient vessels of the neck.
Moreover, in comparison with grafts from the saphe-
nous or cephalic system, the method described here
resulted in only minor vessel mismatch and a reduction
of the risk of complications due to the surgical technique.
REFERENCES
1. Chang KP, Lee HC, Lai CS, Lin SD. Use of single saphenous inter-position vein graft for primary arterial circuit and secondary recipi-ent site in head and neck reconstruction: A case report. Head Neck2007;29:412–415.
2. Baker SR. Microsurgical Reconstruction of the Head and Neck.Hardcover; 1989. p 21.
3. Urken ML, Cheney ML, Sullivan MJ, Biller HF. Atlas of Regional andFree Flaps for Head and Neck Reconstruction. Hardcover; 1995. pp331–336.
4. Fabbrocini M, Fattouch K, Camporini G, DeMicheli G, Bertucci C, CioffiP, Mercogliano D. The descending branch of lateral femoral circumflex ar-tery in arterial CABG: Early midterm results. Ann Thorac Surg2003;75:1836–1841.
5. Suma H. Arterial grafts in coronary bypass surgery. Ann ThoracCardiovasc Surg 1999;5:141–145.
6. Friedman JA, Piepgras DG. Current neurosurgical indications for sa-phenous vein graft bypass. Neurosurg Focus 2003;14:e1.
7. Bas�kaya MK, Kiehn MW, Ahmed AS, Ates� O, Niemann DB. Alter-native vascular graft for extracranial-intracranial bypass surgery: De-scending branch of the lateral circumflex femoral artery. NeurosurgFocus 2008;24:E8.
8. Malhotra K, Lian TS, Chakradeo V. Vascular anatomy of anterolat-eral thigh flap. Laryngoscope 2008;118:589–592.
9. Chen CM, Chen CH, Lai CS, Lin SD, Huang IY, Shieh TY. Antero-lateral thigh flaps for reconstruction of head and neck defects. J OralMaxillofac Surg 2005;63:948–952.
10. Wei FC, Jain V, Celik N, Chen HC, Chuang DC, Lin CH. Have wefound an ideal soft-tissue flap? An experience with 672 anterolateral thighflaps. Plast Reconstr Surg 2002;109:2219–2226; Discussion 2227–2230.
Figure 1. A 7-cm incision made on the proximal half of a line drawn
between the anterior superior iliac spine and the superolateral bor-
der of the patella.
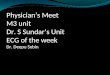
Figure 2. Identification of the lateral circumflex femoral artery (a)
and of the two venae commitantes (b) coursing obliquely over the
vastus lateralis muscle.
Use of Anterolateral Thigh Flap Pedicle 137
Microsurgery DOI 10.1002/micr