Embed Size (px)
Citation preview

Alcohol consumption and risk of lymphoid and myeloidneoplasms: Results of the Netherlands cohort study
Mirjam M. Heinen1, Bas A. J. Verhage1, Leo J. Schouten1, R. Alexandra Goldbohm2, Harry C. Schouten3
and Piet A. van den Brandt1
1 School for Oncology and Developmental Biology (GROW), Department of Epidemiology, Maastricht University Medical Center, Maastricht, The Netherlands2 Department of Prevention and Health, TNO Quality of Life, Leiden, The Netherlands3 School for Oncology and Developmental Biology (GROW), Division of Hematology, Department of Internal Medicine, University Hospital Maastricht,
Maastricht, The Netherlands
Results from epidemiological studies suggest that alcohol drinkers have a decreased risk of lymphoid neoplasms, whereas
results for myeloid neoplasms are inconsistent. However, most of these studies have used retrospective data. We examined
prospectively whether alcohol consumption decreases the risk of both lymphoid and myeloid neoplasms, including most com-
mon subtypes. Moreover, we investigated whether this decreased risk is due to ethanol or other contents of specific alcoholic
beverages (i.e., beer, wine and liquor). The Netherlands cohort study consisted of 120,852 individuals who completed a base-
line questionnaire in 1986. After 17.3 years of follow-up, 1,375 cases of lymphoid and 245 cases of myeloid neoplasms with
complete exposure information were available for analysis. Compared with abstinence, we observed for plasma cell neoplasms
hazard rate ratios (HR) of 1.66 (95% confidence interval (CI), 1.21–2.29), 1.63 (95% CI, 1.17–2.27), 1.11 (95% CI, 0.75–1.64)
and 0.85 (95% CI, 0.51–1.42) with daily ethanol consumption of 0.1–<5, 5–<15, 15–<30 and �30 g, respectively. A similar
pattern was observed for chronic lymphocytic leukemia=small lymphocytic lymphoma. No associations were observed for other
subtypes and for myeloid neoplasms. When results were analyzed by beverage type, no clear associations were observed. In
conclusion, our study did not show an inverse association between alcohol consumption and lymphoid neoplasms. Also, no
inverse association was observed with myeloid neoplasms. If any association between alcohol consumption and lymphoid
neoplasms exists, our study suggests an increased risk rather than a decreased risk.
Hematologic malignancies, a heterogeneous group of neo-plasms arising in lymphoid and myeloid cells throughout thebody, account for 7.4% of cancers in males and 6.4% in
females worldwide.1 So far, little is known about the causesof hematologic malignancies. A few factors have beenlinked to lymphoid neoplasms, including age, gender,primary=inherited immune deficiencies, a number of virusesincluding the human immunodeficiency virus and severalautoimmune diseases.2 Also for myeloid neoplasms just fewetiologic factors have been identified so far, including age,gender, genetic abnormalities, family history and exposuresto radiation and benzene.3 There is some evidence indicatingthat distinguishing between subtypes of lymphoid and mye-loid neoplasms may reveal etiological heterogeneity4 and,therefore, further research including individual subtypes withsufficient numbers of these neoplasms is needed.
Most studies about alcohol consumption and risk of he-matologic malignancies concern non-Hodgkin lymphoma(NHL). Recently, a meta-analysis including 20 case-controlstudies, one pooled analysis of nine case-control studies andeight cohort studies showed a reduction in NHL risk in asso-ciation with higher alcohol intake.5 Compared with non-drinkers, the pooled relative risks (RRs) were 0.88 (95%confidence interval (CI), 0.81–0.96) for light drinking (�1drink per day) and 0.87 (95% CI, 0.79–0.95) for moderatedrinking (1–<4 drinks per day). When results were stratifiedby study design, no association was observed for lightdrinkers in cohort studies, whereas for moderate drinkers theRRs were similar in case-control (RR, 0.85; 95% CI, 0.74–
Key words: lymphoid neoplasms, myeloid neoplasms, alcoholic bev-
erages, ethanol, cohort study
Abbreviations: AML: acute myeloid leukemia; CI: confidence
interval; CLL=SLL: chronic lymphocytic leukemia=small lympho-
cytic lymphoma; DLBCL: diffuse large B-cell lymphoma; FFQ:
food-frequency questionnaire; FL: follicular lymphoma; HR: hazard
rate ratio; InterLymph: international lymphoma epidemiology con-
sortium; LL=WM: lymphoplasmacytic lymphoma=Waldenstr€om
macroglobulinemia; MM: multiple myeloma; NHL: non-Hodgkin
lymphoma; NLCS: Netherlands cohort study; PCN: plasma cell
neoplasms; RR: relative risk; WHO: world health organization
Additional Supporting Information may be found in the online
version of this article.
Grant sponsor: European Research Advisory Board (ERAB)
DOI: 10.1002/ijc.28175
History: Received 8 June 2012; Accepted 12 Feb 2013; Online 29
Mar 2013
Correspondence to: Bas A.J. Verhage (Ph.D.), Department of
Epidemiology, Maastricht University Medical Center, P.O. Box 616,
6200 MD Maastricht, The Netherlands. Fax: 131-43-388-4128,
Epidemiology
Int. J. Cancer: 133, 1701–1713 (2013) VC 2013 UICC
International Journal of Cancer
IJC

0.96) and cohort (RR, 0.89; 95% CI, 0.78–1.01) studies. Nosignificant differences were observed across common lym-phoma subtypes (i.e., DLBCL, follicular lymphoma [FL] andchronic lymphocytic leukemia=small lymphocytic lymphoma[CLL=SLL]).5 Of the studies investigating multiple myeloma(MM) in relation to alcohol, the majority observed nullresults in both case-control6–9 and cohort studies.10–13 Justfew epidemiological studies have investigated the relationbetween alcohol consumption and the incidence of myeloidneoplasms. In the NIH-AARP Diet and Health Study, noassociation was observed for acute myeloid leukemia (AML)risk, neither with total alcohol consumption nor with specificalcoholic beverages.14 Case-control studies investigating alco-hol consumption and AML risk have shown inconsistentresults, observing no association for alcohol consump-tion6,15,16 or observing increased risks.17,18
A decreased risk of lymphoid neoplasms associated withalcohol consumption is supported by experimental evidenceshowing that moderate alcohol consumption modulates theimmune system.19 Furthermore, moderate alcohol consump-tion has been shown to retard the growth of malignantlymphoid cells via inhibition of the mammalian target ofrapamycin.20
The inconsistent study findings observed in observationalstudies may be explained by methodological limitations,including low case numbers of specific subtypes (n<70),9,21,22
crude alcohol categorization,6,17,21 no data on the relationwith specific alcoholic beverages11,16,18 or retrospective assess-ment of alcohol consumption. The latter limitation poten-tially leads to (differential) misclassification of exposure. Toovercome these limitations, we investigated the relationbetween alcohol consumption and risk of lymphoid and mye-loid neoplasms, including the most common subtypes, in alarge prospective cohort study of men and women in theNetherlands. Specifically, we examined whether alcohol con-sumption decreases the risk of both lymphoid and myeloidneoplasms. Moreover, we investigated whether this inverseassociation is due to ethanol or other contents of specificalcoholic beverages, i.e., beer, wine and liquor.
Material and MethodsStudy population and cancer follow-up
The study design of the Netherlands Cohort Study (NLCS)has been reported in detail elsewhere.23 Briefly, the NLCSwas initiated in September 1986 and included 58,279 men
and 62,573 women aged 55–69 years at the beginning of thestudy, originating from 204 municipalities with computerizedpopulation registries. A self-administered questionnaire ondaily dietary habits, lifestyle factors and other potential riskfactors for cancer was completed at baseline.
For reasons of efficiency in questionnaire processing andfollow-up, the case-cohort approach24 was used. Incidentcases were derived from the entire cohort, whereas the per-son-years at risk were estimated from a random sample of5,000 subjects. This subcohort was chosen immediately afterbaseline and followed-up for vital status information. Theentire cohort is being monitored for cancer occurrence byannual record linkage to the Netherlands Cancer Registryand the Netherlands Pathology Registry.25,26 A total of 17.3years of follow-up (baseline to December 2003) was used forthe current analysis. Only one subcohort member was lost tofollow-up. The completeness of cancer follow-up was esti-mated to be >96%.27 All prevalent cancer cases at baselineother than skin cancer were excluded (n 5 226), leaving4,774 subcohort members (Supporting Information Fig. 1).
Histology is coded by the Netherlands Cancer Registryusing the International Classification of Diseases for Oncol-ogy (ICD-O).28 Cases were defined as participants with anincident, histologically verified diagnosis of a lymphoid neo-plasm (n 5 1,512) or a myeloid neoplasm (n 5 270). Usingthe histology codes provided by the cancer registries, we sub-divided the lymphoid neoplasms into categories based on thehierarchical groupings of the International Lymphoma Epide-miology Consortium (InterLymph) nested classification (Ta-ble 1).29 This classification is based on the World HealthOrganization (WHO) classification of tumors of hematopoi-etic and lymphoid tissues30 and the ICD-O, Third Edition.28
Regarding the myeloid neoplasms, we grouped these malig-nancies into categories defined by the WHO classification(Table 1).30 For cases that could not be assigned to a specificcategory (e.g., the “not otherwise specified (NOS)” categories),the summary of the pathology report (received from theNetherlands Pathology Registry) was inspected and, if possi-ble, an appropriate category was assigned. These included thefollowing percentages: 66.4% for NHL, B-cell, NOS; 55.6%for NHL, T-cell, NOS; 81.1% for NHL, unknown lineage;77.8% for lymphoid neoplasms, NOS and 100% for leukemia,NOS).
Subjects with incomplete or inconsistent dietary data andsubjects with incomplete alcohol data were excluded from
What’s new?
Recent epidemiological studies suggest that alcohol consumption may protect from hematological malignancies, especially
nonhodgkin lymphoma. In this large prospective study, the authors analyzed data from the Netherlands Cohort Study includ-
ing more than 1, 600 cases of lymphoid and myeloid neoplasms. No inverse correlation with alcohol consumption was found;
instead, the data suggest that alcohol consumption promotes hematological cancers. As this study includes a larger number
of cases as compared to previous studies, it contributes substantially to the growing, yet inconclusive evidence of an associa-
tion between alcohol consumption and lymphoid and myeloid neoplasms.
Epidemiology
1702 Alcohol and risk of lymphoid and myeloid neoplasms
Int. J. Cancer: 133, 1701–1713 (2013) VC 2013 UICC

Table 1. Number of lymphoid and myeloid neoplasms in the Netherlands Cohort Study on diet and cancer, 1986–2003
Epidemiology
Heinen et al. 1703
Int. J. Cancer: 133, 1701–1713 (2013) VC 2013 UICC

analysis. Details are given elsewhere.31 Alcohol data wereconsidered incomplete when all questions on consumptionfrequency of alcoholic beverages were left blank and twoquestions on alcohol consumption pattern did not indicatethat the subject was an abstainer. These two questions con-cerned alcohol intake during the past week and 5 years ago.Supporting Information Figure 1 shows the selection andexclusion steps that resulted in the final numbers of casesand subcohort members that were available for analysis. TheNLCS has been approved by the institutional review boardsof the TNO Nutrition and Food Research Institute (Zeist, theNetherlands) and Maastricht University (Maastricht, theNetherlands).
Questionnaire
The dietary section of the questionnaire was a 150-item semi-quantitative food-frequency questionnaire (FFQ), which con-centrated on the habitual consumption during the yearpreceding the start of the study. Alcohol consumption wasmeasured by six items: beer; red wine; white wine; sherry andother fortified wines; liqueur types containing on average16% ethanol; and (Dutch) gin, brandy and whiskey. The totalamount of mean daily ethanol intake was calculated usingthe Dutch food composition table.32 We defined low alcoholconsumption as drinking >0–�10 g day21 of ethanol; mod-erate consumption as drinking >10–<30 g day21, and highalcohol consumption as drinking �30 g day21. One questionin the questionnaire provided information on the subjects’drinking habits 5 years before baseline. Subjects could indi-cate for “beer” and “other alcoholic beverages” whether 5years before baseline, they drunk (a) more than; (b) equalamounts of; (c) less than at baseline or (d) never used thosebeverages.
The FFQ had been validated and tested for reproducibil-ity.31,33 For mean daily ethanol intake, the Spearman correla-tion coefficients between the 9-day diet record and thequestionnaire were 0.89 for all subjects and 0.85 for users ofalcoholic beverages.31 The absolute amount of ethanolreported in the questionnaire by users of alcoholic beverageswas, on average, 86% of that reported in the 9-day dietrecord.31
Statistical analysis
Cox proportional hazards models were used to estimate inci-dence hazard rate ratios (HRs) and corresponding 95% CIs.The total person-years at risk estimated from the subcohortwere used in the analyses.34 Standard errors were estimatedusing a robust covariance matrix estimator to account forincreased variance due to sampling from the cohort.35 Theproportional hazards assumption was tested using the scaledSchoenfeld residuals.36 In case the proportional hazardsassumption was violated with respect to alcohol consump-tion, we performed a test for interaction between alcoholconsumption and time, and we stratified the follow-up periodinto three periods (�5 years, >5–�10 years and >10 years)
to investigate further how risk estimates changed during fol-low-up. In the present study, the analysis was performed forlymphoid and myeloid neoplasms overall and for specificsubtypes with a sufficient number of incident cases (n � 70,as used in a previous analysis within the NLCS;37 Table 1).
All analyses were conducted for both sexes combined andseparately for men and women. Furthermore, interactions ona multiplicative scale between sex and alcohol consumptionwere tested for lymphoid and myeloid neoplasms. We wereunable to conduct stratified analyses on sex for most sub-types, due to low case numbers, especially among women.HRs were estimated for categories of ethanol intake, with theabstainers regarded as the reference group. Respondents whodrank alcohol beverages less than once a month were consid-ered an abstainer. Next to considering the total amount ofethanol intake, we examined three types of alcoholic bever-ages, i.e., beer, wine (red wine, white wine, sherry and otherfortified wines) and liquor (liqueurs, gin, brandy and whis-key), relative to the nondrinkers of beer, wine and liquor,respectively. Total ethanol intake was divided into five cate-gories: abstainers (0 g day21), 0.1–<5, 5–<15, 15–<30 and�30 g day21. For beer, wine and liquor, categories were anonuser and three-user categories: 0.1–<1, 1–<5 and �5glasses=week. On the basis of pilot study data, standard glasssizes were defined as 200 ml for beer, 105 ml for wine and45 ml for liquor, corresponding to 8, 10 and 13 g of ethanol,respectively.38
Variables examined as potential confounders includedBMI, height, energy intake, intake of vegetables, fruit, fat andprotein, level of education, nonoccupational physical activity,smoking, family history of hematologic malignancies, historyof chronic bowel irritation and rheumatoid arthritis. Thesevariables were regarded as confounders if they (a) were asso-ciated with lymphoid and myeloid neoplasms and with etha-nol intake and (b) changed the risk estimate by at least 10%.However, none of the potential confounding variables metthese criteria; therefore, we present only the results of age-and sex-adjusted models. Analyses for beer, wine and liquorwere adjusted for total ethanol intake (g day21), to evaluatethe effect of the beverage on the risk of lymphoid and mye-loid neoplasms independent of the beverage’s alcoholic con-tent. For each analysis, trends were evaluated with the Waldtest by assigning participants the median value for each levelof the categorical exposure variable among the subcohortmembers and this variable was entered as a continuous termin the Cox regression model. To evaluate whether the associ-ations between alcohol consumption and risk of lymphoidand myeloid neoplasms were linear, we examined nonpara-metric regression curves using restricted cubic splines usingdifferent numbers and positions of knots.39 Testing the needfor nonlinear terms in the models was done using the Waldv2 statistic. Participants with ethanol intake of 63 g day21 ormore (top 1% of subcohort members) were excluded fromthe cubic spline analysis to reduce the influence of extremevalues, as done in previous research.40
Epidemiology
1704 Alcohol and risk of lymphoid and myeloid neoplasms
Int. J. Cancer: 133, 1701–1713 (2013) VC 2013 UICC

Preclinical manifestations of hematologic malignanciesmay cause subjects to either quit drinking or to continuetheir drinking on a lower level.41 When using the baselinemeasurement of alcohol intake only, these individuals will becategorized as an abstainer or as a low level drinker. Thiswill result in an underestimated disease risk. In additionalanalyses, we investigated this into more depth using two dif-ferent approaches. First, we excluded the abstainers from theanalysis and used the moderate alcohol consumers (0.1–<5 gday21) as the reference group. This analysis, however, mightstill be contaminated by individuals who continued theirdrinking on a lower level. We therefore restricted furtheranalyses to alcohol drinkers who reported to have consumedequal amounts of alcohol 5 years before baseline comparedto baseline drinking habits, using as reference category theabstainers at baseline that reported to have also abstainedfrom alcohol 5 years before baseline. Hereafter, we refer tothis subgroup as stable alcohol users. Furthermore, earlycases (diagnosed within 2 years after baseline) were excludedin additional analyses. All analyses were performed using theSTATA statistical software package (Intercooled STATA, ver-sion 10; Stata Corporation, College Station, TX). All p valueswere based on two-sided tests and considered statistically sig-nificant if <0.05.
ResultsIn Table 2, baseline characteristics are presented for cases(overall and by subtype) and subcohort members. Most char-acteristics did not differ noticeably between cases and subco-hort members, but there were more men among cases thanamong subcohort members. Moreover, there were lessabstainers and more stable drinkers among lymphoplasma-cytic lymphoma=Waldenstr€om macroglobulinemia (LL=WM),CLL=SLL and plasma cell neoplasms (PCN; including MM)cases than among subcohort members. Also, there were moresubjects with a family history of hematologic malignanciesamong cases than among subcohort members, especiallyamong FL and AML cases.
For the risk of lymphoid neoplasms overall, we observed astatistically significantly increased risk for daily consumptionof 0.1–<5 and 5–<15 g of ethanol compared to abstainers(Table 3). HRs dropped to about 1, however, with higherethanol intake showing a p for trend of 0.06. A similar pat-tern was observed for two large lymphoma specific subtypes,CLL=SLL (p for trend 5 0.87) and PCN (p for trend 5 0.03;Table 3). When we excluded the PCN cases from the overallgroup of lymphoid neoplasms, the increased risks for lowalcohol consumption attenuated and were no longer signifi-cant (results not shown). No associations were observed withthe other lymphoma subtypes, although we observed a signif-icant inverse trend for DLBCL (p 5 0.03; Table 3). For mye-loid neoplasms and among AML cases, no associations wereobserved (Table 3). When the abstainers were excluded fromthe analyses and the moderate alcohol consumers (0.1–<5 gday21) were used as the reference group, the inverse trends
for the lymphoid neoplasms overall and the subtype PCNbecame even more significant (p for trend 5 0.004 and0.001, respectively). When restricting the analyses to the sub-group of stable alcohol users, results were similar to the over-all analyses (Table 3), although the significant p values fortrend for PCN and DLBCL became nonsignificant. The riskfor the LL=WM subgroup became statistically significant forthe highest ethanol intake category (�30 g day21), observingalmost a threefold increased risk (HR, 2.98; 95% CI, 1.19–7.49). This estimate was based on only 11 cases. PredictedHRs by use of a regression model with restricted cubic splinetransformation of ethanol intake is presented in Figure 1 forlymphoid neoplasms. No evidence for a nonlinear associationwas found for lymphoid neoplasms, showing no significantdeviation from linearity using the Wald test (p > 0.05). Formyeloid neoplasms, in the regression model with restrictedcubic spline transformation the proportional hazards assump-tion was violated for ethanol intake, showing a significantinteraction with time (p 5 0.002). Next, we stratified the fol-low-up period into three periods (data not shown). In thefirst and second part of the follow-up period, no significantdeviation from linearity was shown. During the third part offollow-up (>10 years), a significantly increased associationwas present with low ethanol intake (<15 g day21), afterwhich risk dropped to approximately unity. Also, the Waldtest showed a significant deviation from linearity (v2 5 6.76,p 5 0.03).
When the results were analyzed by alcoholic beveragetype after adjustment for total ethanol, we observed a signifi-cantly increased risk of LL=WM with consumption of 5 ormore glasses of wine per week (p for trend 5 0.05), whereasa significantly reduced risk was observed with wine intake forAML risk (p for trend 5 0.02). Regarding consumption ofliquor, a statistically significantly increased risk for PCN wasobserved with the highest intake category (HR, 1.64; 95% CI,1.21–2.41; p for trend 5 0.02). No clear associations wereobserved for the other lymphoma subtypes and myeloid neo-plasms with wine or with liquor intake. Also, for beer intake,no clear associations were observed.
When we stratified the analysis for lymphoid neoplasmsrisk and total ethanol intake by sex, results for men weresimilar to the overall results. Compared with abstinence, weobserved HRs of 1.32 (95% CI, 0.99–1.77), 1.38 (95% CI,1.04–1.82), 1.19 (95% CI, 0.89–1.59) and 0.97 (95% CI, 0.70–1.34; p for trend 5 0.10) for the intake of 0.1–<5, 5–<15,15–<30 and �30 g of ethanol per day among men, respec-tively. For women, the HRs were 1.18 (95% CI, 0.94–1.48),1.07 (95% CI, 0.81–1.41), 0.95 (95% CI, 0.66–1.37) and 0.90(95% CI, 0.50–1.62; p for trend 5 0.37) for the intake of 0.1–<5, 5–<15, 15–<30 and �30 g of ethanol per day, respec-tively. The test for interaction of ethanol intake and sex wasnot significant (p 5 0.76). For myeloid neoplasms, the find-ings stratified by sex were similar to the overall results show-ing no significant interaction between sex and ethanol intake(p > 0.05). Among men, findings for the analyses between
Epidemiology
Heinen et al. 1705
Int. J. Cancer: 133, 1701–1713 (2013) VC 2013 UICC

Table 2. Baseline characteristics (means or percent) of cases and subcohort members; Netherlands Cohort Study on diet and cancer, 1986–2003
Subcohort(n 5 4,308)
Lymphoidneoplasms
(n 5 1,375) DLBCL (n 5 265) FL (n 5 103)
Characteristic Mean (SD) % Mean (SD) % Mean (SD) % Mean (SD) %
Male sex 50.2 59.2 60.4 47.6
Age, y 61.4 (4.2) 61.9 (4.1) 61.9 (4.2) 61.4 (4.3)
Alcohol consumption
Abstainers 23.3 19.3 21.9 26.2
Ethanol, g day211 13.6 (15.1) 12.9 (14.2) 12.6 (15.6) 12.8 (13.0)
Beer, glasses=week1 2.2 (6.0) 1.9 (5.0) 2.3 (5.3) 0.9 (2.6)
Wine, glasses=week1 3.4 (5.5) 3.1 (5.3) 3.0 (5.4) 4.2 (6.6)
Liquor, glasses=week1 3.3 (5.8) 3.3 (5.5) 3.1 (5.9) 3.0 (4.9)
Stable drinkers2 58.0 63.3 61.8 68.4
Daily dietary intake
Energy, kcal 1,931 (516) 1,987 (512) 1,926 (488) 1,943 (525)
Total fat3, g 84.0 (16.0) 86.0 (15.6) 86.6 (14.2) 83.5 (17.1)
Total protein3, g 70.7 (12.1) 71.9 (12.3) 70.7 (11.3) 72.0 (13.0)
Vegetables, g 193.7 (83.1) 191.8 (78.3) 195.0 (78.0) 193.0 (67.0)
Fruit, g 175.0 (119.2) 179.8 (120.7) 165.8 (118.1) 181.2 (121.3)
Other characteristics
Current smoker 28.5 26.2 29.1 38.2
Years of smoking4 31.8 (12.3) 31.9 (12.4) 32.6 (12.4) 32.7 (11.3)
Height, cm 170.9 (8.5) 172.7 (8.5) 173.2 (9.1) 171.5 (8.6)
Body mass index, kg m22 25.0 (3.1) 25.0 (3.0) 24.9 (2.9) 25.0 (3.1)
Physical activity (nonoccupational), min day21
�30 21.1 22.3 26.1 21.4
>30–60 31.3 30.3 30.3 28.2
>60–90 20.8 19.6 16.1 16.5
>90 26.8 27.7 27.6 34.0
Family history of hematologic malignancies 2.8 4.3 4.5 6.8
History of chronic bowel irritation 3.2 3.8 1.9 1.9
History of rheumatoid arthritis 6.0 6.0 7.6 10.7
Level of education
Primary school or lower vocational school 50.5 46.9 51.7 49.0
Intermediate vocational school or high school 35.4 37.8 32.3 39.2
Higher vocational school or college 14.1 15.3 16.0 11.8
LL=WM(n 5 95)
CLL=SLL(n 5 231)
PCN(n 5 361)
Myeloidneoplasms(n 5 245)
AML(n 5 176)
Mean(SD) %
Mean(SD) %
Mean(SD) %
Mean(SD) %
Mean(SD) %
Male sex 63.2 67.1 52.6 63.3 62.5
Age, y 62.0 (4.0) 62.2 (4.0) 62.0 (4.0) 61.8 (4.3) 61.7 (4.3)
Alcohol consumption
Abstainers 13.7 15.2 16.9 20.4 22.2
Ethanol, g day211 16.2 (19.2) 14.0 (15.1) 10.7 (11.9) 14.5 (16.0) 13.6 (15.0)
Epidemiology
1706 Alcohol and risk of lymphoid and myeloid neoplasms
Int. J. Cancer: 133, 1701–1713 (2013) VC 2013 UICC

specific alcoholic beverages and both lymphoid and mye-loid neoplasms were similar to the overall results (data notshown). We did not run these analyses for women,because the proportional hazards assumption was violatedand because just few women consumed higher amounts ofthese specific drinks. Inclusion of confounding variables inthe Cox regression models yielded very similar results(data not shown). After excluding the first 2 years of fol-low-up, the results were not substantially different (datanot shown).
DiscussionOverall, we did not observe an inverse association betweenalcohol consumption and risk of both lymphoid and myeloidneoplasms. Compared with abstinence, we observed statisti-cally significant increased risks of CLL=SLL and PCN formoderate ethanol consumption. These increased risks were,however, no longer apparent with higher ethanol consump-tion. For LL=WM, we observed increased risks with higheralcohol intake, which became significant after restricting theanalyses to stable alcohol users. No clear associations were
Table 2. Baseline characteristics (means or percent) of cases and subcohort members; Netherlands Cohort Study on diet and cancer, 1986–2003 (Continued)
LL=WM(n 5 95)
CLL=SLL(n 5 231)
PCN(n 5 361)
Myeloidneoplasms(n 5 245)
AML(n 5 176)
Mean(SD) %
Mean(SD) %
Mean(SD) %
Mean(SD) %
Mean(SD) %
Beer, glasses=week1 3.0 (6.4) 2.4 (6.0) 1.4 (3.4) 2.5 (6.8) 2.6 (6.9)
Wine, glasses=week1 4.2 (5.9) 2.7 (4.8) 2.6 (4.8) 3.1 (6.5) 2.5 (4.9)
Liquor, glasses=week1 3.6 (6.4) 4.0 (6.8) 2.9 (4.5) 3.7 (5.9) 3.7 (5.7)
Stable drinkers2 62.2 62.2 62.0 59.0 56.2
Daily dietary intake
Energy, kcal 2,021 (514) 2,052 (526) 1,985 (513) 1,974 (505) 1,973 (525)
Total fat3, g 83.8 (14.0) 88.2 (17.1) 84.7 (15.8) 84.9 (15.8) 84.8 (15.8)
Total protein3, g 70.8 (11.4) 73.4 (12.5) 71.6 (13.0) 72.5 (11.6) 71.7 (11.8)
Vegetables, g 186.3 (64.3) 192.7 (83.8) 194.2 (81.9) 196.0 (80.3) 198.6 (84.5)
Fruit, g 183.0 (120.0) 174.0 (122.9) 193.6 (120.4) 182.1 (116.1) 184.2 (116.1)
Other characteristics
Current smoker 25.3 23.8 20.2 33.6 33.7
Years of smoking4 30.9 (12.6) 32.4 (12.2) 30.4 (12.4) 32.6 (13.5) 32.6 (13.6)
Height, cm 172.3 (7.8) 173.3 (7.6) 172.2 (8.4) 172.4 (8.7) 172.2 (8.6)
Body mass index, kg m22 25.4 (2.7) 24.9 (3.1) 25.2 (3.1) 25.3 (3.1) 25.5 (3.3)
Physical activity (nonoccupational), min day21
�30 27.4 24.5 19.1 19.3 19.0
>30–60 27.4 30.1 31.1 29.2 31.6
>60–90 19.0 21.4 21.6 25.1 25.9
>90 26.3 24.0 28.3 26.3 23.6
Family history of hematologic malignancies 3.2 4.8 3.9 5.7 6.3
History of chronic bowel irritation 4.2 2.6 5.3 4.1 4.0
History of rheumatoid arthritis 7.4 4.8 5.5 6.9 5.7
Level of education
Primary school or lower vocational school 41.1 47.0 50.6 48.6 48.6
Intermediate vocational school or high school 34.7 38.3 36.4 34.4 35.3
Higher vocational school or college 24.2 14.8 13.1 17.0 16.2
1Ethanol intake and consumption of beer, wine and liquor in alcohol users only. 2Stable drinkers were defined as those subjects reporting to haveconsumed equal amounts of total alcohol 5 years before baseline compared to baseline drinking habits.3Energy-adjusted intake.4Number of smok-ing years in ever smokers only.Abbreviations: AML, acute myeloid leukemia; CLL=SLL, chronic lymphocytic leukemia=small lymphocytic lymphoma; DLBCL, diffuse large B-cell lym-phoma; FL, follicular lymphoma; LL=WM, lymphoplasmacytic lymphoma=Waldenstr€om macroglobulinemia; PCN, plasma cell neoplasms.
Epidemiology
Heinen et al. 1707
Int. J. Cancer: 133, 1701–1713 (2013) VC 2013 UICC

Tab
le3
.A
ge
-a
nd
sex-
ad
just
ed
ha
zard
rate
rati
os
(HR
s)a
nd
95
%C
Ifo
rly
mp
ho
ida
nd
mye
loid
ne
op
lasm
sa
cco
rdin
gto
cate
go
rie
so
fe
tha
no
l(m
en
an
dw
om
en
);N
eth
erl
an
ds
Co
ho
rtS
tud
yo
nd
iet
an
dca
nce
r,1
98
6–
20
03
Lym
ph
oid
ne
op
lasm
sD
LBC
LFL
LL=
WM
Tota
le
tha
no
l(g
da
y21)
No
.o
fp
ers
on
-ye
ars
No
.o
fca
ses
HR
19
5%
CI
No
.o
fca
ses
HR
19
5%
CI
No
.o
fca
ses
HR
19
5%
CI
No
.o
fca
ses
HR
19
5%
CI
All
sub
ject
s2
Ab
sta
ine
rs3
14
,90
62
65
1.0
05
81
.00
27
1.0
01
31
.00
0.1
–<
51
8,9
36
41
71
.23
1.0
3–
1.4
78
81
.17
0.8
3–
1.6
62
90
.85
0.5
0–
1.4
43
11
.86
0.9
6–
3.6
0
5–<
15
14
,66
83
52
1.2
21
.01
–1
.47
59
0.9
00
.61
–1
.31
21
0.8
00
.44
–1
.43
20
1.3
90
.67
–2
.87
15
–<
30
10
,13
72
27
1.0
70
.87
–1
.32
40
0.8
20
.53
–1
.25
17
0.9
30
.49
–1
.77
17
1.6
00
.75
–3
.38
�3
05
79
81
14
0.9
00
.69
–1
.16
20
0.6
70
.39
–1
.15
90
.86
0.3
8–
1.9
41
42
.18
0.9
7–
4.8
8
Pfo
rtr
en
d0
.06
0.0
30
.89
0.2
3
Su
bg
rou
po
fst
ab
lea
lco
ho
lu
sers
4
Ab
sta
ine
rs5
11
,87
82
14
1.0
04
71
.00
20
1.0
01
11
.00
0.1
–<
51
1,0
77
24
81
.22
0.9
8–
1.5
05
61
.24
0.8
3–
1.8
71
60
.87
0.4
5–
1.6
81
71
.61
0.7
4–
3.4
9
5–<
15
90
53
22
51
.25
1.0
0–
1.5
63
50
.86
0.5
4–
1.3
71
61
.10
0.5
5–
2.2
11
41
.43
0.6
2–
3.2
9
15
–<
30
54
25
15
31
.39
1.0
8–
1.8
02
20
.89
0.5
1–
1.5
31
31
.54
0.7
1–
3.3
69
1.4
80
.60
–3
.69
�3
03
16
67
71
.17
0.8
5–
1.6
11
51
.00
0.5
3–
1.8
87
1.4
40
.56
–3
.69
11
2.9
81
.19
–7
.49
pfo
rtr
en
d0
.25
0.5
30
.20
0.0
5
CLL=
SLL
PC
NM
yelo
idn
eo
pla
sms
AM
L
No
.o
fca
ses
HR
19
5%
CI
No
.o
fca
ses
HR
19
5%
CI
No
.o
fca
ses
HR
19
5%
CI
No
.o
fca
ses
HR
19
5%
CI
All
sub
ject
s2
Ab
sta
ine
rs3
35
1.0
06
11
.00
50
1.0
03
91
.00
0.1
–<
56
51
.44
0.9
5–
2.2
01
28
1.6
61
.21
–2
.29
71
1.0
90
.75
–1
.58
56
1.1
00
.72
–1
.67
5–<
15
66
1.6
31
.07
–2
.48
10
11
.63
1.1
7–
2.2
76
01
.04
0.7
1–
1.5
33
60
.79
0.5
0–
1.2
6
15
–<
30
40
1.3
00
.81
–2
.09
49
1.1
10
.75
–1
.64
36
0.8
30
.53
–1
.30
25
0.7
40
.44
–1
.22
�3
02
51
.32
0.7
8–
2.2
62
20
.85
0.5
1–
1.4
22
81
.06
0.6
5–
1.7
42
00
.96
0.5
4–
1.7
0
pfo
rtr
en
d0
.87
0.0
30
.72
0.4
7
Epidemiology
1708 Alcohol and risk of lymphoid and myeloid neoplasms
Int. J. Cancer: 133, 1701–1713 (2013) VC 2013 UICC

observed for the other subtypes of lymphoma and for mye-loid neoplasms and AML. When results were analyzed byalcoholic beverage type, we observed a significantly increasedrisk between wine intake and LL=WM and between liquorintake and PCN. For AML, a reduced risk was observed withwine intake. No clear associations were observed for theother lymphoma subtypes, for myeloid neoplasms or withbeer intake.
Changes in our understanding of hematological malignan-cies have resulted in the evolution of several clinical andpathologic classification schemes over the last several decades.In 2007, the Pathology Working Group of the InterLymphhas developed a hierarchical scheme for the classification oflymphoid neoplasms and, in addition, provided a translationfrom previous classifications.29 This scheme will facilitatesubtype-specific analyses to the most detailed extent possible,based on the sample size and level of pathology informationavailable, which is critical for comparing subtypes-specificdata among epidemiological studies. In the current study,this hierarchical scheme was used. One of the main differen-ces with many other studies using other classifications, is thatin the current study PCN (including MM) is included in thegroup of lymphoid neoplasms, which most studies did notinclude6,8,10–12,42,43 The use of different classifications in pre-vious studies, mostly among case-control studies, makesmeaningful comparison of results between epidemiologicalstudies very difficult and might explain the observed differen-ces between case-control studies and between case-controland cohort studies.Ta
ble
3.
Ag
e-
an
dse
x-a
dju
ste
dh
aza
rdra
tera
tio
s(H
Rs)
an
d9
5%
CI
for
lym
ph
oid
an
dm
yelo
idn
eo
pla
sms
acc
ord
ing
toca
teg
ori
es
of
eth
an
ol
(me
na
nd
wo
me
n);
Ne
the
rla
nd
sC
oh
ort
Stu
dy
on
die
ta
nd
can
cer,
19
86
–2
00
3(C
on
tin
ue
d)
CLL=
SLL
PC
NM
yelo
idn
eo
pla
sms
AM
L
No
.o
fca
ses
HR
19
5%
CI
No
.o
fca
ses
HR
19
5%
CI
No
.o
fca
ses
HR
19
5%
CI
No
.o
fca
ses
HR
19
5%
CI
Su
bg
rou
po
fst
ab
lea
lco
ho
lu
sers
4
Ab
sta
ine
rs5
29
1.0
05
31
.00
36
1.0
02
81
.00
0.1
–<
53
71
.30
0.7
9–
2.1
37
61
.55
1.0
7–
2.2
43
71
.06
0.6
6–
1.7
02
70
.99
0.5
7–
1.7
0
5–<
15
38
1.4
00
.85
–2
.30
66
1.6
21
.09
–2
.38
38
1.2
00
.74
–1
.92
22
0.8
80
.50
–1
.55
15
––<
30
31
1.8
21
.07
–3
.11
30
1.2
50
.77
–2
.02
23
1.1
80
.68
–2
.04
15
0.9
60
.51
–1
.83
�3
01
61
.53
0.8
1–
2.8
71
40
.99
0.5
3–
1.8
61
71
.43
0.7
6–
2.6
71
31
.37
0.6
7–
2.8
1p
for
tre
nd
0.0
90
.52
0.2
80
.44
1A
dju
ste
dfo
ra
ge
(y)
an
dse
x.2S
ub
ject
sw
ith
ba
seli
ne
info
rma
tio
no
nto
tal
eth
an
ol
con
sum
pti
on
.3R
efe
ren
ceca
teg
ory
.4S
tab
led
rin
ke
rsw
ere
de
fin
ed
as
tho
sesu
bje
cts
rep
ort
ing
toh
ave
con
sum
ed
eq
ua
la
mo
un
tso
fto
tal
alc
oh
ol
5ye
ars
be
fore
ba
seli
ne
com
pa
red
tob
ase
lin
ed
rin
kin
gh
ab
its.
5R
efe
ren
ceca
teg
ory
:a
bst
ain
ers
at
ba
seli
ne
tha
tre
po
rte
dto
ha
vea
lso
ab
sta
ine
dfr
om
alc
oh
ol
five
yea
rsb
efo
reb
ase
lin
e.
Ab
bre
via
tio
ns:
AM
L,a
cute
mye
loid
leu
ke
mia
;C
LL=
SLL
,ch
ron
icly
mp
ho
cyti
cle
uk
em
ia=
sma
llly
mp
ho
cyti
cly
mp
ho
ma
;D
LBC
L,d
iffu
sela
rge
B-c
ell
lym
ph
om
a;
FL,
foll
icu
lar
lym
ph
om
a;
LL=
WM
,ly
mp
ho
-p
lasm
acy
tic
lym
ph
om
a=
Wa
lde
nst
r€ om
ma
cro
glo
bu
lin
em
ia;
PC
N,
pla
sma
cell
ne
op
lasm
s.
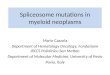
Figure 1. Hazard rate ratios (solid line) and 95% confidence inter-
vals (dashed lines) for lymphoid neoplasm as a function of ethanol
intake estimated by using restricted cubic spline models, the Neth-
erlands Cohort Study on Diet and Cancer, 1986–2003. Knots were
placed at percentiles 5, 35, 65 and 95 of ethanol intake (corre-
sponding to 0, 1.4, 9.7 and 36.8 g of ethanol per day). Partici-
pants with ethanol intake of 63 g day21 or more (top 1% of
subcohort members) were excluded from the analysis. Models are
adjusted for age and sex. The abstainers were regarded as the ref-
erence category. No significant deviation from linearity observed
using the Wald test (p > 0.05).
Epidemiology
Heinen et al. 1709
Int. J. Cancer: 133, 1701–1713 (2013) VC 2013 UICC

Table 4. Multivariable-adjusted hazard rate ratios (HRs) and 95% CI for lymphoid and myeloid neoplasms according to consumption of spe-cific alcoholic beverages (men and women); Netherlands Cohort Study on diet and cancer, 1986–2003
Lymphoid neoplasms DLBCL FL LL=WM
Alcoholicbeverage
No. ofperson-years
No. ofcases HR1 95% CI
No. ofcases HR1 95% CI
No. ofcases HR1 95% CI
No. ofcases HR1 95% CI
Beer (glasses=week)
No beer2 43,153 871 1.00 172 1.00 70 1.00 53 1.00
0.1–<1.0 6124 156 0.99 0.80–1.23 27 0.90 0.58–1.40 18 1.82 0.98–3.36 9 0.88 0.41–1.86
1.0–<5.0 8074 200 0.95 0.78–1.17 33 0.86 0.56–1.31 9 0.68 0.31–1.49 18 1.34 0.74–2.44
�5.0 7092 148 0.84 0.66–1.07 33 1.10 0.68–1.77 6 0.48 0.18–1.25 15 1.26 0.63–2.51
p for trend 0.19 0.47 0.07 0.50
Wine (glasses=week)
No wine2 29,875 611 1.00 129 1.00 42 1.00 30 1.00
0.1–<1.0 8202 212 1.22 0.99–1.50 32 0.86 0.56–1.33 19 2.36 1.20–4.64 20 2.36 1.20–4.64
1.0–<5.0 14,620 302 0.97 0.81–1.17 62 1.00 0.70–1.44 21 1.47 0.74–2.91 20 1.42 0.72–2.81
�5.0 11,748 250 1.15 0.93–1.43 42 1.10 0.70–1.72 21 1.81 0.86–3.81 25 2.46 1.17–5.20
p for trend 0.31 0.58 0.33 0.05
Liquor (glasses=week)
No. liquor2 32,998 605 1.00 137 1.00 51 1.00 35 1.00
0.1–<1.0 8896 202 1.15 0.94–1.41 28 0.66 0.42–1.02 19 1.61 0.87–2.99 22 2.08 1.12–3.87
1.0–<5.0 10,842 276 1.19 0.98–1.44 52 0.97 0.67–1.41 13 0.89 0.45–1.77 20 1.33 0.72–2.47
�5.0 11,709 292 1.21 0.97–1.50 48 0.90 0.57–1.43 20 1.20 0.59–2.46 18 0.74 0.38–1.44
p for trend 0.18 0.91 0.78 0.09
CLL=SLL PCN Myeloid neoplasms AML
No. ofcases HR1 95% CI
No. ofcases HR1 95% CI
No. ofcases HR1 95% CI
No. ofcases HR1 95% CI
Beer (glasses=week)
No. beer2 140 1.00 234 1.00 144 1.00 102 1.00
0.1–<1.0 25 0.81 0.51–1.28 44 1.13 0.79–1.63 28 1.10 0.70–1.75 17 1.05 0.59–1.87
1.0–<5.0 37 0.86 0.56–1.30 52 1.07 0.74–1.53 46 1.34 0.90–1.98 34 1.65 1.05–2.60
�5.0 29 0.77 0.47–1.26 31 0.84 0.54–1.31 27 0.91 0.56–1.47 23 1.37 0.79–2.38
p for trend 0.40 0.44 0.53 0.28
Wine (glasses=week)
No. wine2 113 1.00 152 1.00 122 1.00 92 1.00
0.1–<1.0 37 1.04 0.68–1.58 63 1.26 0.89–1.80 31 0.90 0.58–1.42 21 0.81 0.47–1.37
1.0–<5.0 43 0.63 0.43–0.94 91 1.02 0.75–1.40 59 0.95 0.66–1.36 45 1.00 0.67–1.51
�5.0 38 0.73 0.47–1.13 55 0.96 0.65–1.43 33 0.66 0.41–1.06 18 0.50 0.27–0.90
p for trend 0.19 0.64 0.09 0.02
Liquor (glasses=week)
No. liquor2 89 1.00 153 1.00 108 1.00 80 1.00
0.1–<1.0 29 1.04 0.66–1.65 59 1.18 0.83–1.68 31 1.03 0.65–1.63 19 0.85 0.48–1.50
1.0–<5.0 54 1.35 0.90–2.04 74 1.26 0.91–1.76 50 1.24 0.83–1.85 37 1.37 0.87–2.17
�5.0 59 1.33 0.84–2.12 75 1.64 1.12–2.41 56 1.26 0.81–1.99 40 1.47 0.86–2.51
p for trend 0.29 0.02 0.28 0.12
1Adjusted for age (y), sex and ethanol intake (abstainers; 0.1–<5; 5–<15; 15–<30; �30 g day21). 2Reference category.Abbreviations: AML, acute myeloid leukemia; CLL=SLL, chronic lymphocytic leukemia=small lymphocytic lymphoma; DLBCL, diffuse large B-cell lym-phoma; FL, follicular lymphoma; LL=WM, lymphoplasmacytic lymphoma=Waldenstr€om macroglobulinemia; PCN, plasma cell neoplasms.
Epidemiology
1710 Alcohol and risk of lymphoid and myeloid neoplasms
Int. J. Cancer: 133, 1701–1713 (2013) VC 2013 UICC

Some previous epidemiological cohort studies suggestedthat alcohol drinkers have a decreased risk of DLBCL13,42
and of CLL=SLL.44 On the other hand, other cohort studiesshowed no association for several lymphoma subtypes,including DLBCL,10 FL,10,13,42 CLL=SLL13,42 and MM.10–13
Regarding case-control studies, several studies including apooled analysis of nine case-control studies,43 showed adecreased risk of DLBCL,8,43 FL9,43 and MM7 with alcoholintake, whereas several others showed no association for sev-eral lymphoma subtypes, including DLBCL, FL, CLL=SLLand MM.6,8,9,15,22 To our knowledge, just few studiesobserved an increased risk. In the California teachers studycohort, any alcohol intake during the year before baseline sig-nificantly increased risk of CLL=SLL compared with non-drinking (RR, 2.14; 95% CI, 1.18–3.88 and RR, 1.93; 95% CI,1.03–3.63 for 0.1–<10 and �10 g day21, respectively).10
These studies observed a positive dose-response relation forincreased alcohol intake, rather than the pattern observed inthe present study. To our knowledge, no studies have yetinvestigated the association between LL=WM and alcoholconsumption.
Regarding the association between specific types of alco-holic beverages and lymphoma subtypes, no cohort studiesobserved significant increased risks with any type of alco-holic beverage as far as we know. A few case-controlsstudies did, including increased risks of CLL22 and FL21
for wine consumption and an increased risk of DLBCLwith hard liquor intake plus beer or wine.6 The few stud-ies that investigated the association between AML andwine consumption, observed either no association6,14,15 oran increased risk.17
Overall, some of our findings do not seem to be in linewith previous research. Also, due to the large number ofcomparisons that were made in the present study, somestatistical significant associations would be expected to arisedue to chance alone. Therefore, our results must beregarded with some caution, especially the results regardingspecific types of drinks. Further studies are needed to rep-licate our findings, preferably prospective studies with largecase numbers which are able to investigate the associationbetween alcohol intake, including specific alcoholic bever-ages, and specific subtypes of lymphoid and myeloidneoplasms.
Some of the heterogeneity among previous studies maypartly be due to the fact that case-control studies are proneto recall bias and selection bias.45 Because alcohol is a knownrisk factor for many diseases, cases may have underreportedalcohol intake in comparison to controls leading to recallbias. Also, reasons for nonparticipation may have differedbetween cases and controls and self-selection of systematicallydifferent controls may have taken place, which could haveled to spurious findings.
One of the limitations of this study is the use of a singlemeasure of dietary intake that may not have been representa-tive of the dietary habits of the study participants over the
course of follow-up. Since the late 80s, the prevalence ofdrinking habits among adults above 55 years of age have notchanged remarkably in the Netherlands.46 It is thereforeunlikely that this has influenced the results in the present pa-per. The FFQ was tested for reproducibility by Goldbohmet al.33 with repeated measurements at five annual intervalsin independent samples of the cohort. For alcohol, the esti-mated decrease of the correlation coefficient between baselineand repeated measurement amounted to 0.02 per year, indi-cating a rather stable measurement during the first 5 years offollow-up. Nevertheless, it is possible that our FFQ may nothave been representative of the drinking habits of the partici-pants during later follow-up. Another limitation is that thenumber of cases in some of the subgroups was low, leadingto limited power to explore the relation with alcohol intakein some subgroups and even precluding analyses for someother subgroups.
Strengths of this study include a high completeness offollow-up and the prospective design which avoids the pos-sibility of biased recall of alcohol consumption. Further-more, unlike most previous studies, we were able torestrict the analyses to stable alcohol drinkers. Excludingformer drinkers from the abstainers category is importantbecause some evidence suggests that former drinkers havean increased risk of developing lymphoid neoplasms.10
This might be due to prediagnostic symptoms of diseaseor other underlying health conditions. Therefore, not dis-tinguishing former drinkers from never drinkers couldresult in an artificial association between current alcoholconsumption and a reduced lymphoid neoplasms risk.However, restricting our analyses to these stable alcoholusers showed similar results compared to the overall resultsin which we included both abstainers and former drinkersin the abstainers category. Although, the period of 5 yearsmay not have been long enough to exclude all formerdrinkers from the abstainers group.
Our study did not show an inverse associationbetween alcohol consumption and lymphoid neoplasms aspreviously reported. Also, no inverse association wasobserved with myeloid neoplasms. If any associationbetween alcohol consumption and lymphoid neoplasmsexists, our study suggests an increased risk rather than adecreased risk.
AcknowledgementsThe authors are indebted to the participants of this studyand further wish to thank the cancer registries (IKA, IKL,IKMN, IKN, IKO, IKR, IKST, IKW, IKZ and VIKC), and theNetherlands nationwide registry of pathology (PALGA). Theyalso thank Dr. A. Volovics and Dr. A. Kester for statisticaladvice; S. van de Crommert, H. Brants, J. Nelissen, C. deZwart, M. Moll and A. Pisters for assistance; and H. vanMontfort, T. van Moergastel, L. van den Bosch, E. Dutman,R. Schmeitz, J. Berben and R. Meijer for programmingassistance.
Epidemiology
Heinen et al. 1711
Int. J. Cancer: 133, 1701–1713 (2013) VC 2013 UICC

References
1. Ferlay J, Shin HR, Bray F, et al. GLOBOCAN2008 v2.0, cancer incidence and mortalityworldwide: IARC CancerBase No. 10 [Internet].Lyon, France: International Agency for Researchon Cancer, 2010 [cited 2013 Feb 17]. Availableat: http:==globocan.iarc.fr.
2. Roman E, Smith AG. Epidemiology oflymphomas. Histopathology 2011;58:4–14.
3. Linet MS, Devesa SS, Morgan GJ. The leukemias.In: Schottenfeld D, Fraumeni JF, Jr., eds. Cancerepidemiology and prevention, 3rd edn. NewYork: Oxford University Press, 2006. 841–71.
4. Larsson SC, Wolk A. Body mass index and riskof non-Hodgkin’s and Hodgkin’s lymphoma: ameta-analysis of prospective studies. Eur J Cancer2011;47:2422–30.
5. Tramacere I, Pelucchi C, Bonifazi M, et al.Alcohol drinking and non-Hodgkin lymphomarisk: a systematic review and a meta-analysis.Ann Oncol 2012;23:2791–8.
6. Brown LM, Gibson R, Burmeister LF, et al.Alcohol consumption and risk of leukemia, non-Hodgkin’s lymphoma, and multiple myeloma.Leuk Res 1992;16:979–84.
7. Brown LM, Pottern LM, Silverman DT, et al.Multiple myeloma among Blacks and Whites inthe United States: role of cigarettes and alcoholicbeverages. Cancer Causes Control 1997;8:610–4.
8. Monnereau A, Orsi L, Troussard X, et al.Cigarette smoking, alcohol drinking, and risk oflymphoid neoplasms: results of a French case-control study. Cancer Causes Control2008;19:1147–60.
9. Nieters A, Deeg E, Becker N. Tobacco andalcohol consumption and risk of lymphoma:results of a population-based case-control studyin Germany. Int J Cancer 2006;118:422–30.
10. Chang ET, Clarke CA, Canchola AJ, et al.Alcohol consumption over time and risk oflymphoid malignancies in the california teachersstudy cohort. Am J Epidemiol 2010;172:1373–83.
11. Kanda J, Matsuo K, Inoue M, et al. Associationof alcohol intake with the risk of malignantlymphoma and plasma cell myeloma in Japanese:a population-based cohort study (Japan PublicHealth Center-based Prospective Study). CancerEpidemiol Biomarkers Prev 2010;19:429–34.
12. Klatsky AL, Li Y, Baer D, et al. Alcoholconsumption and risk of hematologicmalignancies. Ann Epidemiol 2009;19:746–53.
13. Troy JD, Hartge P, Weissfeld JL, et al.Associations between anthropometry, cigarettesmoking, alcohol consumption, and non-Hodgkinlymphoma in the prostate, lung, colorectal, andovarian cancer screening trial. Am J Epidemiol2010;171:1270–81.
14. Ma X, Park Y, Mayne ST, et al. Diet, lifestyle,and acute myeloid leukemia in the NIH-AARPcohort. Am J Epidemiol 2010;171:312–22.
15. Gorini G, Stagnaro E, Fontana V, et al. Alcoholconsumption and risk of leukemia: a multicentercase-control study. Leuk Res 2007;31:379–86.
16. Pogoda JM, Nichols PW, Preston-Martin S.Alcohol consumption and risk of adult-onsetacute myeloid leukemia: results from a Los
Angeles County case-control study. Leuk Res2004;28:927–31.
17. Li Y, Moysich KB, Baer MR, et al. Intakes ofselected food groups and beverages and adult acutemyeloid leukemia. Leuk Res 2006;30:1507–15.
18. Wakabayashi I, Sakamoto K, Masui H, et al. Acase-control study on risk factors for leukemia ina district of Japan. Intern Med 1994;33:198–203.
19. Diaz LE, Montero A, Gonzalez-Gross M, et al.Influence of alcohol consumption onimmunological status: a review. Eur J Clin Nutr2002;56 (Suppl 3):S50–S3.
20. Hagner PR, Mazan-Mamczarz K, Dai B, et al.Alcohol consumption and decreased risk of non-Hodgkin lymphoma: role of mTOR dysfunction.Blood 2009;113:5526–35.
21. Casey R, Piazzon-Fevre K, Raverdy N, et al.Case-control study of lymphoid neoplasm inthree French areas: description, alcohol andtobacco consumption. Eur J Cancer Prev2007;16:142–50.
22. Chang ET, Smedby KE, Zhang SM, et al. Alcoholintake and risk of non-Hodgkin lymphoma inmen and women. Cancer Causes Control2004;15:1067–76.
23. van den Brandt PA, Goldbohm RA, van ’t VeerP, et al. A large-scale prospective cohort study ondiet and cancer in The Netherlands. J ClinEpidemiol 1990;43:285–95.
24. Prentice RL. A case-cohort design forepidemiologic cohort studies and diseaseprevention trials. Biometrika 1986;73:1–11.
25. Casparie M, Tiebosch AT, Burger G, et al.Pathology databanking and biobanking in TheNetherlands, a central role for PALGA, thenationwide histopathology and cytopathologydata network and archive. Cell Oncol 2007;29:19–24.
26. van den Brandt PA, Schouten LJ, Goldbohm RA,et al. Development of a record linkage protocolfor use in the Dutch cancer registry forepidemiological research. Int J Epidemiol1990;19:553–8.
27. Goldbohm RA, van den Brandt PA, Dorant E.Estimation of the coverage of Dutchmunicipalities by cancer registries and PALGAbased on hospital discharge data. Tijdschr SocGezondheidsz 1994;72:80–84.
28. Fritz AG, Percy C, Jack A. Internationalclassification of diseases for oncology, 3rd edn.Geneva, Switzerland: World Health Organization,2000.
29. Morton LM, Turner JJ, Cerhan JR, et al.Proposed classification of lymphoid neoplasmsfor epidemiologic research from the PathologyWorking Group of the International LymphomaEpidemiology Consortium (InterLymph). Blood2007;110:695–708.
30. Jaffe ES, Harris NL, Stein H, et al. World HealthOrganization classification of tumours: pathologyand genetics of tumours of haematopoietic andlymphoid tissuesed. Lyon, France: IARC Press,2001.
31. Goldbohm RA, van den Brandt PA, Brants HA,et al. Validation of a dietary questionnaire used
in a large-scale prospective cohort study on dietand cancer. Eur J Clin Nutr 1994;48:253–65.
32. NEVO-tabel: Nederlands voedingsstoffenbestand1986–1987 (Nevo table: Dutch Food CompositionTable 1986–1987 [in Dutch]). The Hague, theNetherlands: Voorlichtingsbureau voor devoeding, 1986.
33. Goldbohm RA, van ’t Veer P, van den BrandtPA, et al. Reproducibility of a food frequencyquestionnaire and stability of dietary habitsdetermined from five annually repeatedmeasurements. Eur J Clin Nutr 1995;49:420–9.
34. Volovics A, van den Brandt PA. Methods for theanalysis of case-cohort studies. Biom J1997;39:195–214.
35. Lin DY, Wei LJ. The robust inference for theCox proportional hazards model. J Am Stat Assoc1989;84:1074–8.
36. Schoenfeld D. Partial residuals for theproportional hazards regression model.Biometrika 1982;69:239–41.
37. Pylypchuk RD, Schouten LJ, Goldbohm RA, et al.Body mass index, height, and risk of lymphaticmalignancies: a prospective cohort study. Am JEpidemiol 2009;170:297–307.
38. Brants HAM, den Breeijen H, Beschrijving enverantwoording van de codering van NEVO-codes, standaardporties e.d. (Description of andjustification for coding of the NEVO-codes,standardized serving sizes, etc. [in Dutch]).Institution CIVO—Toxicology and NutritionTNO, 1990.
39. Durrleman S, Simon R. Flexible regressionmodels with cubic splines. Stat Med 1989;8:551–61.
40. Lee JE, Hunter DJ, Spiegelman D, et al. Alcoholintake and renal cell cancer in a pooled analysisof 12 prospective studies. J Natl Cancer Inst2007;99:801–10.
41. Brewin TB. Alcohol intolerance in neoplasticdisease. Br Med J 1966;2:437–41.
42. Lim U, Morton LM, Subar AF, et al. Alcohol,smoking, and body size in relation to incidentHodgkin’s and non-Hodgkin’s lymphoma risk.Am J Epidemiol 2007;166:697–708.
43. Morton LM, Zheng T, Holford TR, et al. Alcoholconsumption and risk of non-Hodgkinlymphoma: a pooled analysis. Lancet Oncol2005;6:469–76.
44. Gapstur SM, Diver WR, McCullough ML, et al.Alcohol intake and the incidence of non-Hodgkinlymphoid neoplasms in the cancer preventionstudy II nutrition cohort. Am J Epidemiol2012;176:60–69.
45. Rothman KJ, Greenland S. Modern epidemiology,2nd edn. Philadelphia: Lippincott-RavenPublishers, 1998.
46. Statistics Netherlands. The Hague, theNetherlands: statistics on alcohol use in theNetherlands 1989–2000 [cited 2013 Feb 17].Available at: http:==statline.cbs.nl=StatWeb=publication=?DM5SLEN&PA57069ENG&D1574,82-83,96,104-105,118,126-127&D251-12&LA5EN&VW5T.
Epidemiology
1712 Alcohol and risk of lymphoid and myeloid neoplasms
Int. J. Cancer: 133, 1701–1713 (2013) VC 2013 UICC