Embed Size (px)
Citation preview

©2011 MFMER | 3133089-1
Chronic Myeloid Leukemia and
Myeloproliferative Neoplasms in 2015
Rocky Mountain Blood Conference April 11, 2015
Ruben A. Mesa, MD Deputy Director, Mayo Clinic Cancer Center
Professor and Chair, Division of Hematology and Medical Oncology

Disclosures:
• Research/ Clinical Trial Funding:
• Incyte, CTI, Gilead, Genentech, Promedior, NS Pharma, Celgene, Pfizer
• Consultancy:
• Novartis, Shire, AOP

MPNs and CML in 2015 Shifting Targets, Goals, and Therapies
• Are the goals of CML therapy changing?
• Early MPNs – no longer just Hydroxyurea to consider
• Evolving options for Myelofibrosis

Disease Burden in CML: Shrinking the Iceberg

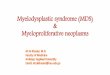
Effect of Early Molecular Response on Subsequent Response and Outcome
Branford S, et al, Leukemia 17(12), 2401-9, 2003 Marin D, et al, J Clin Oncol 30(3) 232-8, 2012 Hanfstein B, et al, Leukemia 26(9):2096-102, 2012
6
Months on Imatinib
% a
chie
vin
g M
MR
50
60
70
80
90
100
20
30
40
10
0
P<0.001 69%
100%
3 6 9 12 15 18 24 30 21 27
13%
>2 log reduction
1-2 log reduction
0-1 log reduction
0.0
0 1 2 3 4 5 6 7 8
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pro
ba
bil
ity
of
PF
S >10%
1-10% 1%
BCR-ABLIS
1%
1-10%
>10%
n
218
281 189
5Y-PFS
96%
92% 87%
p-value
n.s.
0.037
Years
Pro
ba
bil
ity
of
Su
rviv
al
Time From Onset of Imatinib Therapy (Yrs)
BCR-ABL/ABL< 9.84% 8-yr OS: 93.3%
BCR-ABL/ABL > 9.84% 8-yr OS: 56.9%
P < .001
1.0
0.8
0.6
0.4
0.2
0 0 1 3 4 5 8 7 6 2 Years

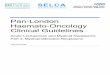
Addition of ‘CMR’ and Improvement in EFS, FFS
23 11 5 1 0 0 0
92 81 60 33 10 3 0
65 63 53 35 15 3 2
CCvR+MMR-
CCvR+MMR+CMR-
CCvR+MMR+CMR+
Number at risk
23 11 5 1 0 0 0
92 81 60 33 10 3 0
65 63 53 35 15 3 2
CCvR+MMR-
CCvR+MMR+CMR-
CCvR+MMR+CMR+
Number at risk
p = 0.00124
p < 0.0001
p < 0.0001
1.0
0.8
0.6
0.4
0.2
0.0
0 20 40 60 80 100 120 Follow-up (Months)
Eve
nt
Fre
e S
urv
iva
l
EFS
CCyR+MMR+CMR+
CCyR+MMR+CMR-
CCyR+MMR-
p = 0.0335
p < 0.0001
p < 0.0001
1.0
0.8
0.6
0.4
0.2
0.0
0 20 40 60 80 100 120 Follow-up (Months)
Fa
ilu
re F
ree
Su
rviv
al
FFS
CCyR+MMR+CMR+
CCyR+MMR+CMR-
CCyR+MMR-
EFS = event-free survival; FFS = failure-free survival. CMR Defined as undetectable BCR-ABL with a sensitivity of at least 4.7 logs on 2 consecutive analyses at least 2 months apart.
Etienne G et al. Haematologica 2014;99:458-464

©2011 MFMER | 3133089-8
Cortes et. al. ASH 2014
Final Results of Dasision Trial
Phase III Dasatinib vs. Imatinib

©2011 MFMER | 3133089-9
Lipton et. al. ASH 2014
Phase III Trial of Ponatnib Vs. Imatinib (EPIC)
CP-CML
45mg Ponatinib vs. 400mg Imatinib

Kantarjian, et al. Blood. 2012;119:1981-1987.
BCR-ABL1 TKI Associated Cardiovascular Adverse Effects
10
Cerebrovascular Disease
Coronary Heart Disease Myocardial Infarction
Pulmonary Arterial Hypertension
Venous Thrombosis Peripheral Arterial Disease
Cardiomyopathy Congestive Heart Failure
Morbidity and mortality; ? Effect on OS observations in front-line studies
? Delay/deferral of advantageous therapy both in front-line and salvage
Cardiomyocyte Injury?
Endothelial Dysfunction? Atherosclerosis?
Endothelial Dysfunction? Atherosclerosis?
Endothelial Dysfunction? Atherosclerosis?
Endothelial Dysfunction?
Platelet dysfunction? Prothrombotic state?
• Fatigue • Musculoskeletal Sx / Cramping • Exercise-Induced Symptoms
Other:

36mo: 61%
0
20
40
60
80
100
0 6 12 18 24 30 36 42
Su
rviv
al w
ith
ou
t M
MR
loss
%
Months since 2G-TKI discontinuation
12 mo: 61.1% (95% CI: 45.6-76.6)
Survival without loss of MMR: ~60% Success
Rea D, et al. Blood (ASH) 2012: Abstract 916
Rousselot P et al., J Clin Oncol. 2014 Feb 10;32(5):424-30
Ross DM et al. Blood. 2013 Jul 25;122(4):515-22
AUSTRALASIAN CML8
STOP 2G TKI A-STIM
Stable cCMR before stop Unstable cCMR before stop
Mo
lecu
lar
Re
lap
se-
Fre
e S
urv
iva
l (%
)
100
80
60
40
20
0 12 24 36 48 60 72 84
Time (months)
A-STIM

Paradise Lost, Regained?
Cumulative incidence of regained MR4.5 in A-STIM retreated pts after loss of MMR
Months
Perc
en
t C
MR
4.5
0 12 24 360
20
40
60
80
100
• Median time to regain deep molecular remission: 7.3 mo • One patient with CML>15y experienced lymphoid blast crisis 8.5 mo from regained
MMR after restarting imatinib
. Rousselot P et al., J Clin Oncol. 2014 Feb 10;32(5):424-30.
Pe
rce
nt
MR
4.5

What Should We Expect From MPN Therapy? Top 10 ways we better match therapy and patients
10. Understand that not all MPN patients are impacted the same
©2011 MFMER | 3133089-13

Assessing MPN Burden WHO Diagnosis Does Not Tell Whole Story
©2011 MFMER | 3133089-14
MPN Symptoms
• MF>PV>ET
• Multifactorial
• Some ET/PV > MF
• Cytoreductive rx
frequently not effective
Vascular Events
• PV/ET > MF
• Counts matter
• Can be
unrecognized
Progression
• PV/ET to MF
• PV/ET to AML
• MF to AML
• ? 2nd MDS
Cytopenias
• MF> ET/PV
• Anemia
• MF 75%
• TX Dep 25%
• TPN 30%
Splenomegaly
• MF> ET/PV
• Pain not always
a function of
size
Baseline Health AGE/ Medicines Comorbidities

What Should We Expect From MPN Therapy? Top 10 ways we better match therapy and patients
10. Understand that not all MPN patients are impacted the same
9. Understand the spectrum of symptoms MPN patients face
©2011 MFMER | 3133089-15

Evolution of MPN Symptom Assessment Tools
MF–SAF
2009
(19 items)
MF-SAF 2.0
(7 items 2011)
JCO 2012
Brief Fatigue
Inventory
(BFI) – 9 Items
Spleen Sx
4 Items
Constitutional Sx
5 Items
QOL 1 Item
Vascular and Ψ Sx
9 Items MPN–SAF
2011
(27 items)
Blood 2011
MPN-SAF TSS
(10 items 2012)
JCO 2013
MPN-SAF Languages
• English
• French
• German
• Spanish
• Dutch
• Swedish
• Italian
• Portuguese
• Mandarin
• Japanese
• Hebrew

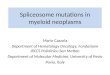
0%
20%
40%
60%
80%
100%
Wo
rst
fati
gue
(o
ne
-ite
m B
FI)
Earl
y sa
tiet
y
Ab
do
min
al d
isco
mfo
rt
Inac
tivi
ty
Co
nce
ntr
atio
n
Nig
ht
swe
ats
Itch
ing
Bo
ne
pai
n
Feve
r
We
igh
t lo
ss
ET (N=874)
PV (N=729)
MF (N=486)
MPN Total (N=2089)
Pre
vale
nce
of
Sym
pto
ms
(%)
Symptoms from 2089 MPN Patients Using the MPN-SAF TSS (MPN10)
MPN QOL - ISG

What Should We Expect From MPN Therapy? Top 10 ways we better match therapy and patients
10. Understand that not all MPN patients are impacted the same
9. Understand the spectrum of symptoms MPN patients face
8. Understand impact of symptom clusters, and gender effect on MPN patients
©2011 MFMER | 3133089-18

Quartile 1 (Q1): 0-24% Quartile 2 (Q2): 25-49%
Quartile 3 (Q3): 50-74% Quartile 4 (Q4): 75-
100%
Percentile MPN-SAF TSS
Q1
TSS <8
Q2
TSS 8 -17
Q3
TSS 18 - 31
Q4
TSS >32
MPN Symptom Burden by Quartiles 1858 MPN-SAF Respondents
Scherber et.al.
ASH 2013

ET (N=775)
PV (N=654)
MF (N=423)
Q1 – 30% Q2 – 26% Q3 – 24% Q4 – 20%
Q1 – 17% Q2 – 21% Q3 – 26% Q4 – 36%
Q1 – 25% Q2 – 23% Q3 – 26% Q4 – 26%
Parameter P value of Comparison
Age 0.24
Gender F>M <0.001
MPN Diagnosis <0.001
Subtype of MF 0.86
IPSET (ET Risk) 0.18
PV Risk (PV) 0.30
DIPSS (MF Risk) <0.001

©2014 MFMER | slide-21
Results
• Higher mean age than females (mean 60.7
yrs [SD 12.6] vs 59.3 yrs [SD 14.4]; p=0.02)
• Higher rate of requirement for red blood
cell transfusion (7% vs 5%, p=0.02)
• Higher mean white blood cell count (mean
9.5x109/L [SD 8.2 x109/L] vs mean 8.5 x109/L
[SD 6.1x109/L]; p=0.004)
• Lower rate of thrombocytopenia (8% vs 14%,
p<0.001).
• Higher TSS (adjusted mean 23.9 vs 20.6;
p<0.001)
• Higher symptom scores for 15/18 items
• Prominent symptoms: fatigue, bone pain,
abdominal discomfort, and microvascular
related
Females Males
Higher levels of fatigue
• Younger
• Lower red blood counts
• Lower transfusion rates
More Abdominal Symptoms
• Male=female abdominal thrombosis rates
Microvascular symptoms
• Previous reports show more macrovascular symptoms
Higher Symptom Scores
• Individual SS and TSS
• Male=female QOL score
Females demonstrate…

What Should We Expect From MPN Therapy? Top 10 ways we better match therapy and patients
10. Understand that not all MPN patients are impacted the same
9. Understand the spectrum of symptoms MPN patients face
8. Understand impact of symptom clusters, and gender effect on MPN patients
7. Understand the complex issue of MPN fatigue, and possible mood disorders
©2011 MFMER | 3133089-22

MPN “Fatigue” Project 2014 Collaborative Internet Based Trial with MPN Forum
©2011 MFMER | 3133089-23 ©2011 MFMER | 3133089-23
ANY MPN Patient • Survey online
• MPN Forum
• MPN Advocacy
• MPN Research
Foundation
• CMPD Ed
Foundation
Regis
ter/
Onlin
e C
onsent
Online 70 Item Survey
• Demographics
• MPN History
• MPN-SAF (MPN10)
• Brief fatigue inventory (BFI)
• Profile of mood states (POMS-Short)
• Patient Health Questionnaire (PHQ-2)
• Mental Health Inventory (MHI-5)
1788 MPN patients/ 1676 Eval.
ET 33%, PV 39%, MF 25%
68% Female, median age 59.
MPN10 Score average 28.4
(range 0-83)
Higher BFI, MPN-SAF,
MPN10 scores all correlated
with increased depressive
symptoms (p<0.0001)
23% high likelihood of depression
(≥ 3 on PHQ-2)
Prior diagnosis depression (32%),
anxiety (29%), stress (26%), grief
(15%)
22% on therapy for mood disorder
in last 6 months
Patients Psych Comorbidity MPN Correlation
Scherber R et al. 2014, ASH: abstract 3173

©2014 MFMER | slide-24
MPN Fatigue Project
• Three part project:
Evaluate
strategies to reduce fatigue burden
PHASE I
Determine strategy
efficacy and comorbidites
PHASE II
Home-based prospective
online trial to employ fatigue-related
interventions
PHASE III
N=1748 MPN pts (718 PV, 625 ET, 420 MF, 29 other)

©2014 MFMER | slide-25
Fatigue Project Strategies To Cope with Fatigue Related to MPN
BFI - Mean (SD), N YES
BFI - Mean (SD), N NO
Δ 95% CI P
Postponing non-essential activities
5.0 (2.1), 981 3.2 (2.3), 365 1.8 (1.6, 2.1) <.0001
Setting priorities 4.9 (2.1), 1015 3.3 (2.4), 353 1.6 (1.3, 1.9) <.0001
Medication psychostimulants 5.8 (2.0), 110 4.4 (2.3), 1253 1.4 (1.0, 1.8) <.0001
Antidepressants 5.5 (2.0), 320 4.2 (2.3), 1050 1.3 (1.1, 1.6) <.0001
Delegation 5.0 (2.2), 682 3.9 (2.4), 655 1.1 (0.8, 1.3) <.0001
Scheduling of activities to times of peak energy
4.9 (2.1), 827 3.8 (2.4), 528 1.1 (0.8, 1.3) <.0001
Naps 4.8 (2.3), 942 3.7 (2.3), 415 1.1 (0.8, 1.3) <.0001
Labor-saving devices 5.1 (2.1), 493 4.1 (2.4), 838 1 (0.8, 1.2) <.0001
Structured daily routines 5.0 (2.2), 706 4.0 (2.3), 635 1 (0.8, 1.2) <.0001
Socializing with family or friends 4.8 (2.2), 853 3.9 (2.5), 487 1 (0.7, 1.2) <.0001
Support groups 5.3 (2.1), 296 4.3 (2.3), 1066 1 (0.8, 1.3) <.0001
Pacing 4.9 (2.1), 772 4.0 (2.4), 580 0.9 (0.7, 1.2) <.0001
Reading 4.8 (2.2), 820 3.9 (2.4), 523 0.9 (0.6, 1.1) <.0001
Sleep therapy 5.3 (2.1), 117 4.4 (2.3), 1237 0.9 (0.5, 1.4) <.0001
Music 4.9 (2.2), 618 4.1 (2.3), 722 0.8 (0.5, 1.0) <.0001
Church or spiritual activities 4.9 (2.1), 485 4.2 (2.4), 841 0.8 (0.5, 1.0) <.0001
Nutrition 4.8 (2.2), 876 4.0 (2.4), 499 0.8 (0.5, 1.1) <.0001
Steroids 5.3 (2.0), 75 4.5 (2.3), 1282 0.8 (0.3, 1.4) 0.003
Meditation, quiet time, or cognitive re-framing
4.9 (2.2), 555 4.2 (2.4), 822 0.7 (0.4, 0.9) <.0001
New activities/ diversions 4.8 (2.3), 476 4.3 (2.3), 857 0.5 (0.2, 0.7) 0.0003
Relaxation, including yoga 4.7 (2.3), 572 4.3 (2.4), 821 0.4 (0.1, 0.6) 0.005
Walking/sitting in a natural environment
4.6 (2.2), 891 4.3 (2.5), 477 0.2 (-0.02, 0.5) 0.1
Gardening 4.6 (2.3), 585 4.4 (2.4), 788 0.1 (-0.1, 0.4) 0.3
Volunteer activities 4.5 (2.3), 430 4.5 (2.3), 937 0.1 (-0.2, 0.3) 0.7
Exercise 4.4 (2.3), 1009 4.7 (2.5), 377 -0.4 (-0.6, -0.1) 0.01
Postponing non-essential activities
Setting priorities
Medication Psychostimulants
Antidepressants
Exercise

MPN Patient Burden- Disease Impact 2014 Landmark Study
©2011 MFMER | 3133089-26 ©2011 MFMER | 3133089-26
ANY MPN Patient • Survey online
• MPN Forum
• MPN Advocacy
• MPN Research
Foundation
• CMPD Ed
Foundation
Regis
ter/
Onlin
e C
onsent
Online Survey
• Demographics
• MPN History
• MPN-SAF (MPN10)
• Impact on QoL
• Impact on Employment
• Impact on ADLs
• 813 MPN Patients
• MF (207)/ PV (380),
ET (226)
• INT/ High Risk
• MF (94%)
• PV (78%)
• ET (74%)
• ≥ 1 sick day in last month
• MF (33%), PV (23%),
ET (22%)
• ≥ 1 cancelled activity in last
month
• MF (46%), PV (35%),
• ET (34%)
• Anxious about their MPN
• MF (91%)
• PV (78%)
• ET (74%)
• MPN Symptoms decrease my
QoL
• MF (81%)
• PV (66%)
• ET (57%)
Patients Symptom Burden Impact
Mesa R et al. 2014, ASH: abstract 3183

What Should We Expect From MPN Therapy? Top 10 ways we better match therapy and patients
10. Understand that not all MPN patients are impacted the same
9. Understand the spectrum of symptoms MPN patients face
8. Understand impact of symptom clusters, and gender effect on MPN patients
7. Understand the complex issue of MPN fatigue, and possible mood disorders
6. Understand complex assessment of MPN “risk”, and comorbidities
©2011 MFMER | 3133089-27

Evolving MPN prognostic scales
Tefferi Leuk 2014
Passamonti Blood 2012
Passamonti Blood 2010
a 10% weight loss over prior 6 months, night sweats, unexplained fever.
IPSET
(ET—3 groups)
Survival
thrombosis risk
PV
Risk (4 groups)
Survival
leukemia rates
DIPSS
(PMF—4 groups)
Survival
Age, years ≥ 60 (2 pts) vs < 60 ≥ 67 (5 pts)
57-66 (2 pts), < 60 (0)
≥ 65 (1 pt) vs < 65
Leukocytes ≥ 11 (1 pt) vs
< 11 x 109/L
≥ 15 (1 point) vs
< 15 x 109/L
> 25 (1 pt) vs
≤ 25 x 109/L
Hemoglobin < 10 (2 pts) vs
≥ 10 g/dL
Constitutional
symptoms
Presenta (1pt) vs
absent
Blasts ≥ 1% (1pt) vs < 1%
Prior thrombosis Yes (1 point) vs No Yes (1 Point) vs No
Risk group point
cutoffs
0; 1-2; 3-4 pts 0; 1-2; 3; 4 pts 0; 1-2; 3-4; ≥ 4 pts
Monitoring MPNs

MIPSS: Molecular International Prognostic Score System
Weighted value
1.5
0.5
0.5
1.0
1.5
0.5
0.5
0.5
MULTIVARIATE ANALYSIS
Variables HR (95% CI) P
Age >60yrs 3.8 (2.60-5.51) <0.0001
Hb <100g/L 1.4 (1.01-1.99) 0.04
Constitutional Symptoms 1.5 .(1.13-2.16) 0.007
PLT <200x109/L 2.5 (1.77-3.42) <0.0001
Triple Negativity 3.9 (2.20-6.80) <0.0001
JAK2/MPL mutation 1.8 (1.11-2.90) 0.016
ASXL1 mutation 1.4 (1.06-1.99) 0.02
SRSF2 mutation 1.7 (1.08-2.58) 0.02
Vannucchi et. al. ASH 2014

Development of the MIPSS Score in the Learning Cohort
Int-1
Low Int-2
High
Risk category
Score % of pts
OS (y) HR
Low 0-0.5 27 26.4 1
Int-1 1-1.5 14 9.7 4.7
Int-2 2-3.5 46 6.4 9.9
High >4 13 1.9 36.5
P < .001
Vannucchi et. al. ASH 2014

IPSS - LOW IPSS - INT-1 IPSS - INT-2
P= .005
23.4y 17.7y 4.5y
Low 24.9y < Int-1 17.7y < Int-2 6.2y
> Low 15.3y > Int-1 8.1y > Int-2 1.9y
MIPSS
P= .040 P= < .001
*, IPSS Median Survival
* * *
Estimated
§
§
§
§
MIPSS Permits to Refine Prognostic Stratification Within the IPSS Categories
Vannucchi et. al. ASH 2014

FATIGUE Trial – Co-morbidities in 1676 MPN Patients
Scherber
et. al.
ASH 2014

What Should We Expect From MPN Therapy? Top 10 ways we better match therapy and patients
10. Understand that not all MPN patients are impacted the same
9. Understand the spectrum of symptoms MPN patients face
8. Understand impact of symptom clusters, and gender effect on MPN patients
7. Understand the complex issue of MPN fatigue, and possible mood disorders
6. Understand complex assessment of MPN “risk”, and comorbidities
5. Understand new response criteria, and need for their validation
©2011 MFMER | 3133089-33

©2011 MFMER | 3133089-34
Response Criteria for MPNs 2014 (All ≥ 12 Weeks) ET/PV – ELN (Barosi et. al. Blood 2013) MF – IWG-MRT (Tefferi et. al. Blood 2013)
ET
PV
MF
Complete
Remission
Partial
Remission
Clinical
Improvement Other
N.B. ET/PV – Progression is MF/MDS/ or AML
MF – Progression based on spleen growth or AML
• Resolve ET Signs
• ≥ 10 pt. MPN10
• Near normal counts
• No Prog. or Vascular
• BM rem & ≤Gr 1 MF
• Resolve ET Signs
• ≥ 10 pt. MPN10
• Near normal counts
• No Prog. or Vascular
Peripheral Blood
Granulocytes
• CR – Eradicated
mutation
• PR - ≥50% ,
≥ 20% baseline
• Resolve MF Signs
• Resolve MF sympts
• Near normal counts
• BM rem & ≤Gr 1 MF
Like MF CR but
• Hb (between 85 and
100 g/L)
• PLT (between 50-100
x 10(9)/L)
• Anemia (2g/dl or T.I.)
• Spleen (Based on BL)
• Symptoms (≥ 50%)
• Molecular (ET/PV
Criteria)
• Cytogenetic
• CR – Normal
• PR - ≥ 50%
• Resolve PV Signs
• ≥ 10 pt. MPN10
• Near normal counts
• No Prog. or Vascular
• BM rem & ≤Gr 1 MF
• Resolve PV Signs
• ≥ 10 pt. MPN10
• Near normal counts
• No Prog. or Vascular
Peripheral Blood
Granulocytes
• CR – Eradicated
mutation
• PR - ≥50% ,
≥ 20% baseline

©2011 MFMER | 3133089-35
“Clinically Meaningful” – What is Valid?
(Example – Spleen Reduction)
> 50% reduction of Palpable Length
IWG-MRT
2006
Blood 2006
> 35% Volume Reduction by MRI
COMFORT
1 & 2
NEJM 2012
> 10% Volume Reduction by MRI
- Better Survival and PGIC
Pooled
CI/CII
Blood 2013

What Should We Expect From MPN Therapy? Top 10 ways we better match therapy and patients
10. Understand that not all MPN patients are impacted the same
9. Understand the spectrum of symptoms MPN patients face
8. Understand impact of symptom clusters, and gender effect on MPN patients
7. Understand the complex issue of MPN fatigue, and possible mood disorders
6. Understand complex assessment of MPN “risk”, and comorbidities
5. Understand new response criteria, and need for their validation
4. Optimizing the timing and utilization of stem cell transplant
©2011 MFMER | 3133089-36

Stem Cell Transplant Use in MPNs
©2011 MFMER | 3133089-37
Baseline Assumptions/ Caveats
• SCT almost exclusively for MF/ MPN-BP
• In MF evolving risk/benefit analysis for use
“Problematic”
MF
& SCT
Eligible
Allo SCT
Question 1
Timing?
• Urgent
• Delayed
• Never
Question 2
Pre Transplant Therapy?
• JAK Inhibition?
• Cytoreduction?
• Iron chelation?
Question 3
Post Transplant Therapy?
• JAK Inhibition?
• Interferon?
• other?

What Should We Expect From MPN Therapy? Top 10 ways we better match therapy and patients
10. Understand that not all MPN patients are impacted the same
9. Understand the spectrum of symptoms MPN patients face
8. Understand impact of symptom clusters, and gender effect on MPN patients
7. Understand the complex issue of MPN fatigue, and possible mood disorders
6. Understand complex assessment of MPN “risk”, and comorbidities
5. Understand new response criteria, and need for their validation
4. Optimizing the timing and utilization of stem cell transplant
3. Optimizing the utilization of current available agents
©2011 MFMER | 3133089-38

Primary Commercially Available MPN Drugs 2015
ET
PV
MF
Hydroxyurea Interferon/
Peg -INF Anagrelide Ruxolitinib
XXX XX
XXX X X X
X
XX XX XXX
XX
X
EXPERIMENTAL – OFF LABEL – PHASE III DATA

Management of PV-ET
• ALL PV Patients
• Maintain HCT <45% Men, 42% Women
• Low Dose ASA
• Aggressive control of CV risk factors
• Cytoreduction
• High Risk or
• Intol to Phlebotomy, Increasing Spleen, Severe Sx
Plt >1500 x 10(9)/L, or prog WBC
• Medications • Hydroxyurea or Interferon alpha as Front line (or second)
• Busulfan, pipobroman, P-32 as second line
Barbui T, et. al. LeukemiaNET Consensus Guidelines. JCO 2011;29:761-770

Risk of the Primary End Point in prespecified subgroups
Barbui et. NEJM 2013

©2011 MFMER | 3133089-42
Interferons in MPNs – Evolving Footprint
Peginterferon alpha-2a
Pegasys (Roche/ Genentech)
Pegylated P Interferon alpha-2b
AOP 2014 P1101
(AOP/ Pharmessentia)
MPD – RC 112
PEG INF vs HU
(Front Line)
High Risk ET/PV NCT01258856
MPD-RC 111
PEG INF
(2nd Line)
High Risk ET/PV - SVT NCT01259817
PROUD - PV
AOP2014/P1101 vs HU
(Front Line)
High Risk PV NCT01949805

JAK Inhibitors and Status of Development Myelofibrosis as lead indications
0 1 2 3 4
AZD1280
XL019
CEP 701
Fedratininb (SAR302503)
INCB039110 (JAK1)
NS-018
BMS-911543
LY2784544
Momelotinib (CYT387)
Pacritinib (SB1518)
Ruxolitinib (FDA Approved)
©2011 MFMER | 3133089-43
No Longer in Development
For MPNs
* Now Testing
in PV
*
*
*
*

©2011 MFMER | 3133089-44
Ruxolitinib (Single Agent) in Myelofibrosis
COMFORT 1 COMFORT 2
Verstovsek, Mesa, Gotlib et. al. NEJM 2012;366(9):799-807
Harrison, Kiladjian, Kathrin et.al. NEJM 2012;366(9):787-798

©2011 MFMER | 3133089-45
Ruxolitinib (Single Agent) in Polycythemia Vera
BAT
Week 32
(Primary analysis)
Week 80
n = 110
n = 112
Crossover to
ruxolitinib
•Resistance to
or intolerance
of HU (modified
ELN criteria)
•Phlebotomy
requirement
•Splenomegaly
Pre-randomization
(Day −28 to Day −1)
Hct 40%-45%
Ra
nd
om
ize
d (
1:1
)
Extended
Treatment
Phase Ruxolitinib
10 mg BID
Week 208
Week 208
Vannucchi et. al. NEJM In Press
Compared to Best Alternative Therapy Ruxolitinib (post HU) in PV
1. Superior control of hematocrit
2. Superior reduction in splenomegaly
3. Superior reduction in PV related symptoms
4. Trend for less thrombotic events

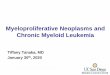
Change in Symptoms on RESPONSE Trial
in PV
46
Median Percentage Changes From Baseline at Week 32 in
Individual MPN-SAF Symptom Scores
−100.0 −99.5 −94.9 −93.9
−80.2
−65.9 −64.1 −61.1
−51.5 −49.6 −44.0 −41.8
−37.1
0.0
−4.4
3.9
−2.1
0.0 7.9
1.4 5.0
0.4
11.1
−4.2
16.7 10.9
15.7 17.2
-120
-100
-80
-60
-40
-20
0
20
40
Me
dia
n C
ha
ng
e F
rom
Ba
se
lin
e, %
Rux BAT
Impro
vem
ent
−120
−100
−80
−60
−40
−20
0
20
40
Mesa. et. al. ASH 2014

Proposed Algorithm of Therapy of ET/PV in 2015
Diagnosis of PV or ET
Front Line Cytoreduction HU, or HU vs INF Clinical Trial
JAK2 Inhibitor (Experimental Indication)
• Ruxolitinib
• Other Clinical Trial JAK2 Inhib
Consider Ruxolitinib (PV)/ ET ( 2nd line or Trial) or INF (Trial)/HU if not previously received
Assess Symptom Quartile
by MPN 10
Q1:TSS <8
Q2:TSS 8-17
Q3:TSS 18-31
Q4:TSS ≥32
Decide on need for concurrent cytoreduction based on Risk and Symptoms
YES NO
Monitor for symptom burden, vascular events,
progression
Worsening symptom burden Vascular event, progression Phlebotomy intolerance
Worsening symptom burden Vascular event, progression HU Resistance/ Intolerance
Assess MPN Risk Score (Table 1) & Assess MPN Symptoms (MPN 10)
Control of Hematocrit (<45%) in PV (? In ET) Low dose aspirin in appropriate patients

Diagnosis of MPN-MF (Primary, Post ET or Post PV Myelofibrosis)
Calculate DIPSS MF Score & Assess MPN Symptoms (MPN 10)
Low Risk Med S = 185m
Symptom Q1-Q2
Low Risk Med S <185m
Symptom Q3-Q4
Intermediate to High Risk Med S = 16m (H), 35m (Int 2), 78 (Int 1)
Assess role and timing of ALLO SCT (Donor, Risk, Candidate) ALLO – Urgent, Delayed, Never
Observation vs INF (Trial)
Possible Role Of JAK2 Inhib (Trial) or INF
(Trial)
Proceed to ALLO
(Possible JAK2 Inhib Prior)
(Trial)
N.B. Consider Rx for Prevention of
Vascular Events in Appropriate Patients (Aspirin & Cytoreduction)
JAK2 Inhibitors
• Ruxolitinib (Jakafi/Jakavi)
(Approved for MF)
• Clinical Trial JAK2 Inhib
Anemia Rx • Clinical Trials • IMID/ Androgens/ EPO • Splenectomy
Symptom Quartiles by MPN 10
Q1:TSS <8 Q3:TSS 18-31
Q2:TSS 8-17 Q4:TSS ≥32
Proposed Algorithm of Therapy of MPN-MF in 2015
Urgent ALLO
JAK2 Inhibitor* *Unless anemia/ cytopenias main
problem
Delayed/Never ALLO
Clinical Trials • Ruxo Combination • Non Ruxo JAK2 • New Targets
JAK2 Single Agent Failure Refractory Cytopenias

What Should We Expect From MPN Therapy? Top 10 ways we better match therapy and patients
10. Understand that not all MPN patients are impacted the same
9. Understand the spectrum of symptoms MPN patients face
8. Understand impact of symptom clusters, and gender effect on MPN patients
7. Understand the complex issue of MPN fatigue, and possible mood disorders
6. Understand complex assessment of MPN “risk”, and comorbidities
5. Understand new response criteria, and need for their validation
4. Optimizing the timing and utilization of stem cell transplant
3. Optimizing the utilization of current available agents
2. Thoughtful analysis of combination MPN therapeutic approaches
©2011 MFMER | 3133089-49

Myelofibrosis – Rx Opportunities
©2011 MFMER | 3133089-50 Time
Clinical Status
Dx of MF
MF on
JAK
Inhibitor
Spleen
MF Symptoms
Survival
Fibrosis
Anemia/
Thrombocytopenia
Molecular
Response

©2011 MFMER | 3133089-51
LANDSCAPE MPN Clinical Trials 2015
ET/PV Single Agent MF Combination MF
Rux Plus -
PEG INF vs HU
MPD-RC 112
NCT01258856
PEG INF (2nd Line)
NCT01259817
P1101 vs HU (PV)
AOP
NCT01949805
Ruxolitinib (PV)
Response 1,2
Relief Trials
Momelotinib
NCT01998828
Givinostat (HDAC)
NCT0190432
Pacritinib v BAT
(PERSIST1-PH III)
NCT01773187
Pacritinib v. BAT
(PERSIST2- PH III)
NCT02055781
Momelotinib v. Rux
(PH III)
NCT01969838
Momelotinib vs.
BAT (PH III)
NCT012101268
NS-018 (PH II)
NCT01423851
PRM-151
NCT01981850
Panobinostat
NCT01693601
NCT01433445
BKM 120 (Pi3K)
NCT01730248
LDE 225 (HH)
NCT01787552
Lenalidomide
NCT013575140
Pomalidomide
NCT01644110
Danazol
NCT01732445
Azacitidine
NCT01787487
Decitibine
NCT02076191
PF04449913 (Smo)
NCT02226172
Imetelstat

Different phenotypes in setting of JAK inhibition
Primary anemia phenotype
Proliferative phenotype
Good ruxolitinib response
Ruxolitinib response with anemia a problem
©2011 MFMER | 3133089-52
SPLN SX
Anemia/Cytope
nias
SPLN SX
Anemia/Cyt
openias
SPLN SX Anemia/C
ytopenias
SPLN SX
Anemia/Cyt
openias
SPLN SX
Anemia/Cyt
openias
SPLN SX
Anemia/Cytopen
ias

MPN Patient Supportive and Survivorship Care
Wellness
MPN
Post Therapy
Care MPN
Deficit/ Therapy Recovery
Care

What Should We Expect From MPN Therapy? Top 10 ways we better match therapy and patients
10. Understand that not all MPN patients are impacted the same
9. Understand the spectrum of symptoms MPN patients face
8. Understand impact of symptom clusters, and gender effect on MPN patients
7. Understand the complex issue of MPN fatigue, and possible mood disorders
6. Understand complex assessment of MPN “risk”, and comorbidities
5. Understand new response criteria, and need for their validation
4. Optimizing the timing and utilization of stem cell transplant
3. Optimizing the utilization of current available agents
2. Thoughtful analysis of combination MPN therapeutic approaches
1. Never lose the forest through the trees
©2011 MFMER | 3133089-54

Medicine Wheel of Health “Integrative Medicine”

Being a Blood Disease Survivor Top 10 List
10. Learn about your disease
9. Make friends with facing a similar challenge
8. Be your own best advocate
7. Capture what is discussed at doctors visits (friends/ recorder)
6. Take care of your caregiver
5. Take care of the rest of your health
4. Eat in a healthy way (most of the time)
3. Exercise
2. Live every moment
1. Focus on relationships
©2011 MFMER | 3133089-56

Quotes from Erma Bombeck Written as she was dying from Cancer
• If I had my life to live over I would…
• Have gone to bed when I was sick instead of pretending the earth would go into a holding pattern if I weren’t there for a day

I would have...
•Burned the pink candle sculpted like a rose before it melted in storage

I would have...
•Sat on the lawn with my grass stains

I would have...
•Talked less and listened more

I would have...
• Invited friends over to dinner even if the carpet was stained or the sofa faded

I would have...
•Shared more of the responsibility carried by my husband

I would have...
•Never have insisted the car windows be rolled up on a summer day because my hair had just been teased and sprayed

I would have...
•Don’t worry about who doesn’t like you, who has more or who is doing what. Instead, cherish the relationships we have with those who do love us.

I would have...
•Never have bought anything just because it was practical, wouldn’t show soil, or was guaranteed to last a lifetime

I would have...
• Instead of wishing away nine months of pregnancy, I’d have cherished every moment and realized that the wonderment growing inside me was the only chance in life to assist God in a miracle

I would have...
•Taken the time to listen to my grandfather ramble about his youth

I would have...
•Cried and laughed less while watching TV and more while watching life

I would have...
•But mostly, given another shot at life, I would seize every minute… look at it and really see it… live it and never give it back. Stop sweating the small stuff.

©2011 MFMER | 3133089-70


©2011 MFMER | 3133089-72
Acknowledgements Argentina
Ana Clara Kneese, MD
Federico Sackmann, MD
Australia
David M Ross MBBS, PhD
Cecily Forsyth
John Seymour, MBBS, PhD
Karen Hall, MD
Kate Burbury MD
Tam Constantine, MD
Canada
Lynda Foltz, MD
Vikas Gupta, MD
China
Hsin-An Hou, MD
Huan-Chau Lin,
MD Hung Chang, MD
Ming-Shen Dai, MD
Yuan-Bin Yu, MD
Yung-Chen Su, MD
Zhijian Xiao, MD
Denmark
Christen Lykkegaard Andersen, MD
Hans Hasselbalch, MD
France
Brigitte Dupriez, MD
Jean-Jacques Kiladjian, MD
Jean-Loup Demory MD
Magali Demilly, PhD
Germany
Heike L. Pahl, PhD
Ireland
Mary Francis McMullen, MD
Israel
Martin Ellis, MD
Italy
Alessandro M. Vannucchi, MD
Francesco Passamonti, MD
Giovanni Barosi, MD
Tiziano Barbui, MD
Netherlands
Harry Schouten, MD, PhD
Jan Jacques Michiels, MD
Karin Klauke, MD
Peter te Boekhorst, MD
Sonja Zweegman, MD PhD
Stephanie Slot, MD
Suzan Commandeur, MD
New Zealand
Hilary Blacklock, MD
Panama
Francis Guerra, MD
Singapore
Wee Joo Chng, MB ChB
Spain
Ana Kerguelen Fuentes, MD
Carlos Besses, MD
Francisco Cervantes, MD
Dolores Fernandez-Casados
Sweden
Andreasson Bjorn, MD
Elisabeth Ejerblad, MD
Gunnar Birgegard, MD
Jan Samuelsson, MD
Johanna Ablesson, MD
Peter Johansson, MD
UK
Anthony Green, MD
Claire N. Harrison, MD
Deepti Radia, MD
Uruguay
Pablo Muxi, MD
USA
Alison Moliterno, MD
Brady Stein, MD MHS
Casey O'Connell
Catriona Jamieson
Daniel Rubin, ND
Elizabth Hexner
Hala Simm
Jason Gotlib, MD
Jeff Sloan, PhD
Jessica Altman, MD
Joseph Prchal, MD
Kimberly Hickman
Martin Tallman, MD
Mike Boxer, MD
Olatoyosi Odenike, MD
Richard T Silver, MD
Ross Levine, MD
Soo Jin Kim
Srdan Verstovsek, MD

©2011 MFMER | 3133089-73
Thanks to MPN Patients, and their loved ones,
for Their Contributions to MPN Research
Courtesy of C. Harrison and UK MPN Patient