Embed Size (px)
Citation preview

Myeloproliferative Neoplasms and
Chronic Myeloid Leukemia
Tiffany Tanaka, MD
January 30th, 2020


MPNs: Clonal disorders of hematopoiesis characterized
by proliferation of ≥1 lineage of mature myeloid cells
• Essential thrombocythemia (ET)
• Polycythemia vera (PV)
• Primary myelofibrosis (PMF)
• Chronic myeloid leukemia (CML)
• Chronic neutrophilic leukemia, Mastocytosis, Chronic
eosinophilic leukemia
WHO 2016
Arber et al. Blood 2016;127: 2391

ESSENTIAL THROMBOCYTHEMIA
(ET)

A 54 year old woman is referred for a platelet count of 1130 x
109/L. Her WBC is 7.8 x 109/L and Hb is 13 g/dL.
She reports chronic fatigue and depression. She has no
abnormal bleeding or bruising.
There is no splenomegaly on exam.
Mutation profiling identifies a CALR mutation in exon 9
(c.1154_1155insTTGTC, p.K385fs*47).
Patient 1

Patient 2
A 76 year old woman with dementia presents with headache,
lightheadedness and is found to have a platelet count 4100 x
109/L.
She recently moved to San Diego to be closer to family. Her
prior hematologist had her on aspirin, hydroxyurea and
anagrelide. Her family is unclear if she was taking these. She
reportedly has a JAK2 V617F mutation.

Patient 3
A 34 year old woman presents for second opinion. She was
diagnosed with JAK2-mutated ET at Kaiser SD following a recent
pregnancy. She is taking aspirin 81 mg daily.
Her CBC: Plt 1030 x 109/L, Hb 13.2 g/dL, Hct 43.3, WBC 9.7
She wishes to become pregnant again in the next 1-2 years.

Primary:
Thrombocytosis
Secondary (“Reactive”):
• Infection
• Inflammation
• Acute blood loss
• Trauma
• Surgery
• Splenectomy
• Malignancy
“Clonal” – acquired
mutation
• Somatic mutations:
• JAK2 V617 (50-60%)
• CALR (20-30%)
• MPL (5-10%)
• Other less common
mutations: ASXL1, EZH2,
TET2, IDH1/IDH2, SRSF2,
SF3B1

WHO 2016: 4 major or 3 major + 1 minor
Major:
1. Platelet count ≥450 x 109/L
2. Bone marrow showing increased/enlarged and mature
megakaryocytes with hyperlobulated nuclei; +/- minor fibrosis
3. Not meeting WHO criteria for other myeloid neoplasm (CML,
PV, PMF, MDS)
4. Presence of JAK2, CALR or MPL mutation
Minor:
1. Presence of another clonal marker
2. Absence of evidence for reactive thrombocytosis
Essential Thrombocythemia (ET)
Arber et al. Blood 2016;127: 2391

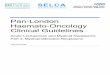
ET Peripheral Smear (Patient 2)

ET Bone Marrow Morphology
ASH Image Bank (Elizabeth Courville; 9/22/15)

• Rare, 1-2.5 patients per 100,000 people
• Female to male ratio 2:1
• Median age at diagnosis is 60 years
- 20% of patients are <40 years
• Higher incidence in Blacks over Whites, Hispanics, Asians
ET Demographics
Srour et al. Br J Haematol 2016; 174: 382

MPN Clinical Features
PV
Geyer HL, Mesa RA. Blood 2014;124:3529-3537.
ET MF

ET Risk Stratification
If PLT >1500 X 109/L:Screen for acquired von Willebrand before instituting ASA
Very Low-Risk
Disease
Low-Risk
Disease
Intermediate-Risk
Disease
High-Risk
Disease
• No history of
thrombosis
• Age ≤60
• JAK2 wild-type
• No history of
thrombosis
• Age ≤60
• JAK2-mutated
• No history of
thrombosis
• Age >60
• JAK2 wild-type
• History of
thrombosis
or
• Age >60
• JAK2-mutated
• CV risk factors:
Aspirin daily
• No CV risk:
Observation
• CV risk factors:
Consider aspirin
2x daily
• No CV risk:
Aspirin daily
• Aspirin daily +/-
hydroxyurea
• If CV risk,
consider aspirin
2x daily
• Arterial
thrombosis:
hydroxyurea +
aspirin daily
• Venous
thrombosis:
hydroxyurea +
anticoagulation

• Thrombohemorrhagic
- 15-year cumulative risk is 10-25%
- Highest with JAK2 mutation
• Progression to myelofibrosis
- 15-year cumulative risk is 10%
- Higher with type 1 CALR over JAK2 mutation
• Leukemic transformation
- 15-year cumulative risk is 3%
ET Complications
Arber et al. Blood 2016;127: 2391

Back to our Clinic Patients…

Very low-risk CALR-mutated ET
A 54 year old woman is referred for a platelet count of 1130 x
109/L. Her WBC is 7.8 x 109/L and Hb is 13 g/dL.
She reports chronic fatigue and depression. She has no
abnormal bleeding or bruising.
There is no splenomegaly on exam.
Mutation profiling identifies a CALR mutation in exon 9
(c.1154_1155insTTGTC, p.K385fs*47).
Patient 1


Very low-risk CALR-mutated ET
• Bone marrow biopsy consistent with ET (increased
megakaryocytes in clusters), no increased blasts, no fibrosis
• Re-connected with her prior psychiatrist
• On surveillance every 6 months
Patient 1

Patient 2
High-risk JAK2-mutated ET
A 76 year old woman with dementia presents with headache,
lightheadedness and is found to have platelet count 4 x 109/L.
She recently moved to San Diego to be closer to family. Her
prior hematologist had her on aspirin, hydroxyurea and
anagrelide. Her family is unclear if she was taking these. She
reportedly has a JAK2 V617F mutation.

Patient 2
Thrombo-
cytapheresis
Thrombo-
cytapheresis
Hydroxyurea +
Ruxolitinib + ASA

Patient 3
Low-risk JAK2-mutated ET, planned pregnancy
A 34 year old woman presents for second opinion. She was
diagnosed with JAK2-mutated ET at Kaiser SD following a recent
pregnancy. She is taking aspirin 81 mg daily.
Her CBC: Plt 1030 x 109/L, Hb 13.2 g/dL, Hct 43.3, WBC 9.7
She wishes to become pregnant again in the next 1-2 years.

MPN and Pregnancy
NCCN Guidelines
Low Risk High Risk
• Low dose ASA (50-100 mg
daily)
• Maintain Hct<45%, in PV
patients
If any are present:
- Microcirculatory disturbances
or 2+ hereditary thrombophilic
factors
- Severe complications with
prior pregnancy
- Platelet count >1M
- Age >35 years
• Consider cytoreduction
• Low dose ASA +/- LMWH,
prophylactic dose

MPN and Pregnancy
Griesshammer et al. Expert Review Hematol 2018; 11:697

Patient 3
Pegasys
45 mcg qwk Pegasys
60 mcg qwk Pegasys
75 mcg qwk

POLYCYTHEMIA VERA(PV)

A 63 year old woman presents with Hb 17.9 g/dL, WBC 11.1 x
109/L and platelet 530 x 109/L.
She reports diffuse itching that is more pronounced after
showering. She has no other symptoms or history of thrombosis.
Her spleen size is normal.
JAK2 V617F mutation is detected. Serum epo level is low.
Patient 1

A 53 year old man is referred by GU Oncology for Hb 18 g/dL.
He has a history of RCC treated with partial nephrectomy in
2013, Hb was 18.2 g/dL at time of diagnosis (!). His RCC is in
remission.
He takes testosterone for androgen insufficiency diagnosed
outside UCSD. Off of testosterone, he feels fatigued and cannot
exercise as vigorously.
Patient 2

Primary Polycythemia:
Polycythemia
Secondary Polycythemia:
• EPO-producing
neoplasms (RCC, HCC,
pheo) or renal lesions
(cysts, RAS,
hydronephrosis)
• Hypoxemia from COPD, R-
to-L cardiac shunts, OSA,
obesity, high altitude, RBC
defects (CO poisoning,
methemoglobinemia)
• Misc: Androgens or anabolic
steroids, diuretics, blood
doping
“Clonal” – somatic or
inherited mutation
• Somatic mutations:
• JAK2 V617F (96%)
• JAK2 exon 12 (2-3%)
• CALR in minority
• Germline mutations:
• EPO receptor gene
• VHL gene mutation
• HIF2-alpha
• Etc.

WHO 2016: 3 major or 1st 2 major + all minor
Major:
1. Hb >16.5 g/dL (men) or >16.0 g/dL (women)
2. Bone marrow hypercellularity with prominent erythroid,
granulocytic, megakaryocytic proliferation
3. JAK2 V617F or JAK2 exon 12 mutation
Minor:
1. Bone marrow trilineage expansion
2. Subnormal EPO level
3. Endogenous erythroid colony growth
Polycythemia Vera (PV) Diagnosis
Arber et al. Blood 2016;127: 2391Megakaryocyte hyperplasia,
clumping, nuclear hyperlobation

PV Risk Stratification
Very Low-Risk
Disease
Low-Risk
Disease
Intermediate-Risk
Disease
High-Risk
Disease
• No history of
thrombosis
• Age ≤60
• JAK2 wild-type
• No history of
thrombosis
• Age ≤60
• JAK2-mutated
• No history of
thrombosis
• Age >60
• JAK2 wild-type
• History of
thrombosis
or
• Age >60
• JAK2-mutated

For all:
• Monitor for new thrombosis or bleeding
• Monitor for disease progression (MF/AML)
• Manage cardiovascular risk factors
Low Risk:
• Aspirin (81-100 mg daily)
• Cytoreduction to maintain Hct <45%
High Risk:
• Aspirin (81-100 mg daily)
• Cytoreduction to maintain Hct <45%
• Hydroxyurea +/- phlebotomy, interferon
• Anticoagulation if indicated
PV Treatment
nccn.gov

PV Treatment
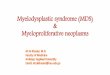
Marchioli et al. N Engl J Med 2013; 368: 22-33
Why target Hct <45%?
Randomized phase 3 trial (n=365) found:
• Lower rate of cardiovascular events
• Lower rate of thrombosis

Back to the clinic!

High-risk JAK2-mutated PV
A 63 year old woman presents with Hb 17.9 g/dL, WBC 11.1 x
109/L and platelet 530 x 109/L.
She reports diffuse itching that is more pronounced after
showering. She has no other symptoms or history of thrombosis.
Her spleen size is normal.
JAK2 V617F mutation is detected. Serum epo level is low.
Patient 1

Patient 1Therapeutic
phlebotomy,
hydroxyurea
500 mg daily
Therapeutic
phlebotomy
stopped
Hematocrit
WBC
count

Testosterone-Induced Erythrocytosis
A 53 year old man is referred by GU Oncology for Hb 18 g/dL.
He has a history of RCC treated with partial nephrectomy in
2013, Hb was 18.2 g/dL at time of diagnosis (!). His RCC is in
remission.
He takes testosterone for androgen insufficiency diagnosed
outside UCSD. Off of testosterone, he feels fatigued and cannot
exercise as vigorously.
Patient 2

Patient 3
RCC
Diagnosis
Partial
Nephrectomy
Testosterone
?

Secondary Erythrocytosis – Treatment
Bhasin et al, J Clin Endocrinol Metab 2010; 95: 2536
The Endocrine Society, Clinical Practice Guidelines
• Recommends against testosterone if Hct >50%
• Monitor Hb/Hct at baseline and every 3-6 months while on
testosterone
• If Hct trends >54%, hold testosterone and evaluate for other
causes (OSA), resume at lower dose

http://transhealth.ucsf.edu/protocols

MYELOFIBROSIS
Hit the road,
JAK (STAT)!

A 76 year old woman presents to the ED with diarrhea and
leukocytosis is noted (WBC 71.9 x 109/L). Hb is 12.9 g/dL and
platelet count is 437 x 109/L.
CT abdomen/pelvis done in the ED shows a splenomegaly
(20.8 cm).
She reports fatigue and dizzy spells, causing her to quit karate
and Zoomba classes recently.
BCR-ABL1 p210 is negative.
JAK2 V617F mutation is noted.
Patient 1

A 67 year old woman presents to transfer care. She was
diagnosed with ET in the 1990s and was observed. Over time,
she developed thrombocytopenia and RBC macrocytosis. A
bone marrow biopsy was repeated 12/2017 and this showed
WHO grade 2/3 MF.
She is asymptomatic – she is not too active, but walks her 2
dogs daily with no problem.
Her spleen size is normal.
Patient 2

Myelofibrosis
Peripheral Smear: Bone Marrow:

Myelofibrosis Diagnosis
WHO 2016: 3 major + at least 1 minor
Major:
1. Bone marrow megakaryocytic proliferation and atypia with
collagen or reticulin fibrosis ≥grade 2
2. Not meeting WHO criteria for other myeloid neoplasm
3. Presence of JAK2, CALR or MPL mutation, or another
clonal marker, or absence of reactive fibrosis
Minor:
1. Anemia
2. Leukocytosis >11 x 109/L
3. Palpable spleen
4. Increased serum LDH
5. Leukoerythroblastosis

Myelofibrosis Risk Stratification
D-IPSS Scoring: # of points
• Age >65 years 1
• Constitutional symptoms 1
• Hb <10 g/dL 2
• WBC count >25 x 109/L 1
• Peripheral blood blasts >1% 1
Risk group: # of factors Median Surival (yrs)
• Low 0 Not reached
• Intermediate-1 1-2 14.2
• Intermediate-2 3-4 4
• High 5-6 1.5
Passamonti F et al. Blood 2010; 115: 1703-1708

Myelofibrosis Risk Stratification
Gangat et al. J Clin Oncol 2011; 29: 392

Myelofibrosis Treatment
Mesa & Stein. ASH-SAP 6.


Back to the clinic!

DIPSS Int-2 PMF (also Int-2 by DIPSS-Plus)
A 76 year old woman presents to the ED with diarrhea and
leukocytosis is noted (WBC 71.9 x 109/L). Hb is 12.9 g/dL and
platelet count is 437 x 109/L. CT abdomen/pelvis done in the ED
shows a splenomegaly (20.8 cm). JAK2 V617F mutation is
noted.
Bone marrow biopsy shows a hypercellular marrow with large
megakaryocytes with “staghorn” nuclei, marked fibrosis (WHO
grade 3/3) by reticulin staining.
Patient 1

Patient 1

Patient 1
Platelet count
WBC count
Rux 20 mg BID
Rux 15 mg BID

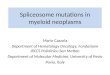
Ruxolitinib in MF
Verstovsek et al. New Engl J Med 2012; 366: 799-807
COMFORT-I randomized phase 3 trial
• Ruxolitinib vs. placebo
• Primary endpoint: 35% SVR at 24 wk
• 41.9% with SVR in rux group
• 45.9% with decreased Sx in rux group

Harrison et al. New Engl J Med 2012; 366: 787-798
Ruxolitinib in MF
COMFORT-II randomized phase 3 trial
• Ruxolitinib vs. best available therapy
• Primary endpoint: 35% SVR at 48 wk
• 28% with SVR in rux group
- Median time to response 12 wk
- 80% had response at median follow up 12 mo
• Improvement in QOL and Sx in rux group

DIPSS Int-1 PMF (also Int-1 by DIPSS-Plus)
A 67 year old woman presents to transfer care. She was
diagnosed with ET in the 1990s and was observed. Over time,
she developed thrombocytopenia and RBC macrocytosis. A
bone marrow biopsy was repeated 12/2017 and this showed
WHO grade 2/3 MF with normal cytogenetics.
She is asymptomatic – she is not too active, but walks her 2
dogs daily with no problem.
Her spleen size is normal.
Patient 2

Allogeneic HSCT
IWG-MRT and ELN Consensus Recommendations:
• Int-2 or higher risk disease and age <70 yr
• Int-1, PRBC dependent, PB blast >2%, adverse cytogenetics
• Int-1, ASXL1-mutated and/or triple negative
Kroger et al. Leukemia 2015; 29: 2126
Pre-transplant Management:
Iron chelation in severely iron overloaded patients
Ruxolitinib if splenomegaly or symptomatic
Splenectomy/Splenic irradiation generally not done

Patient 2


Other JAK inhibitors
Mascarenhas et al. JAMA Oncology 2018; 4: 652
Harrison et al. Lancet Haematol 2017; 4: e317
Mesa et al. J Clin Oncol 2017; 35: 3844
Verstovsek et al. Leukemia 2017; 31: 393
Pacritinib
(JAK2/FLT3)
PERSIST (vs BAT,
including rux): improved
SVR, TI and included
plt<100
Bleeding, cardiac
events; clinical hold in
2016
Fedratinib
(JAK2)
JAKARTA (vs placebo):
improved SVR 40-50%
at both doses
Wernicke
encephalopathy (?);
nausea, diarrhea
Momelotinib
(JAK1/2)
SIMPLIFY (vs. rux): non-
inferior; best responses
in CALR+/ASXL1-
Increased neuropathy,
infection rate
NS-018 Phase I data
INCB039110 Phase II – modest SVR

Beyond JAK
Thalidomide +
prednisone
ORR 28% (2 small
series, n=36)
Paresthesias,
diarrhea,
neutropenia, DVT
Lenalidomide +
prednisone
ORR 30% for anemia,
42% for splenomegaly
(phase 2, n=40)
Frequent gr 3-4
cytopenias
AURKAi Alisertib – increased
GATA1, safety data
Neutropenia,
thrombocytopenia
PI3K Everolimus ORR 23% Feedback up Akt?
FTi Tipifarnib 33% spleen RR Myelosuppression
HDACi Panobinostat + rux…
HMA 23% response, 5 mo Myelosuppresion

CHRONIC MYELOID LEUKEMIA (CML)

Patient
A 71 year old man with chronic-phase CML is seen for
reevaluation of his disease. He has been taking imatinib since
2006 and achieved a complete molecular response within 12
months of therapy.
He experienced nausea and diarrhea intermittently on imatinib
that has now become persistent, causing hypophosphatemia
requiring supplementation and imodium. Scheduled Zofran with
meals did not improve his symptoms adequately.

Patient
BCR-ABL1 p210
WBC

Pathophysiology
ALL CML CML variant

Pathophysiology
Deininger et al. Blood 2000

• Detection of the Ph chromosome or its products, BCR-
ABL1 fusion mRNA or protein, through:
o Cytogenetic analysis,
o Fluorescence in situ hybridization (FISH), or
o Reverse transcription polymerase chain reaction (RT-PCR)
• Peripheral blasts <10%
• Neutrophilic leukocytosis with immaturity, basophilia and/or
eosinophilia, thrombocytosis
• Bone marrow biopsy is needed
Diagnosis
Arber et al. Blood 2016

Diagnosis
Cytogenetic Analysis:
Ch 9 Ch 22
FISH for BCR-ABL1:
FISH false positive rate 3% →
RT-PCR preferred for disease
monitoring

• 1-2 per 100,000 people
• 15% of newly diagnosed adult leukemias
• Slight male predominance (M:F = 1.3:1)
• Median age of 67 years
• Risk factors: Radiation (?)
Epidemiology

Clinical Features
Peripheral Smear: Bone Marrow:

• 50% are asymptomatic
• 90-95% present in chronic phase (CML-CP)
o Constitutional Sx; Sx related to anemia, splenomegaly
o Rare Sx – bleeding, thrombosis, gout, priapism, PUD
o Leukostasis is rare
• Accelerated phase (CML-AP)
o Fever, bone pain, night sweats
o Progressive splenomegaly, infarction
• Blast phase (CML-BP)
o Extramedullary disease
Clinical Features

CML History of Treatment
Kantarjian et al. Clin Cancer Res. 2004

CML Treatment Overview
Kantarjian et al. Clin Cancer Res. 2004
Front-line therapy decision making:
• CML risk category
• Comorbidities
• Concurrent medications
• Patient preference, cost
Available therapies:
• Front line: imatinib, dasatinib, nilotinib
• If intolerance, resistance, or loss of response → switch to
another TKI, consider mutational profile
o Next line: bosutinib, ponatinib for T315I
mutation

TKI Therapy
Druker Blood 2008; 112: 4808-4817

Unique TKI Toxicities
Imatinib Dasatinib Nilotinib Bosutinib
• Cytopenias
• Nausea, vomiting
• Fatigue
• Edema (leg,
periorbital)
• Myalgias
• Hypophos, low
BMD
• Cytopenias
• Pleural effusions
• Pulmonary
hypertension
• Platelet
dysfunction
• Hyperglycemia
• Hyperlipidemia
• Prolonged QTc
• CV events
reported (MI,
CVA, PVD)
• Nausea, vomiting
• Diarrhea
• Transaminitis
• Rash
• Front-line
• Cardiotoxicity is
rare
• Front- or 2nd-line
• Less susceptible
to kinase domain
mutations
• Front- or 2nd-line
• Structural
derivative of
imatinib but 30x
more potent
• Not yet approved
for front-line, but
promising phase
3 results

TKI Response Milestones
Time Optimal Warning Failure
3 months • MCyR (Ph+
metaphases
≤35%), and/or
• BCR-ABL1 ≤10%
• Ph+ metaphases
35-95%
• BCR-ABL1 >10%
• No CHR
• Ph+ metaphases
>95%
6 months • CCyR (Ph+
metaphases 0%)
• BCR-ABL1 <1%
• Ph+ metaphases
1-35%
• BCR-ABL1 1-
10%
• Ph+ metaphases
>35%
• BCR-ABL1 >10%
12 months • MMR (BCR-
ABL1 ≤0.1%)
• BCR-ABL1 0.1-
1%
• Ph+ metaphases
>0%
• BCR-ABL1 >1%
>12 months • MMR (BCR-
ABL1 ≤0.1%)
• Additional
cytogenetic
abnormalities in
Ph- cells
• Loss of CHR,
CCyR, MMR;
kinase domain
mutations

TKI Response Milestones

Loss of TKI Response
• Repeat bone marrow biopsy
• Test CML cells for BCR-ABL1 kinase domain mutations
• Selection of 2nd or 3rd line TKI:
o CML disease phase
o Mutation profile
o Patient’s comorbidities
Mutation TKI Recommendation
Y253H, E255K/V or F359V/C/I Dasatinib
F317 L/V/I/C, T315A or V299L Nilotinib
E255K/V, F317L/V/I/C, F359V/C/I,
T315A or Y253H
Bosutinib
T315I Ponatinib, Omacetaxine, allo-HSCT,
clinical trial

• MPNs are stem-cell derived clonal disorders characterized
by proliferation of mature, myeloid lineage cells
• Ph-negative MPNs are progressive diseases with
transformative potential (AML, myelofibrosis)
• Common clinical manifestations include:
- Abnormal proliferation of hematopoietic cells
- Constitutional symptoms
- Hepatomegaly, splenomegaly
- Thromboses
Take Home Points