Embed Size (px)
Citation preview

Case ReportMyeloid Neoplasms with t(512) and ETV6-ACSL6 Gene FusionPotential Mimickers of Myeloid Neoplasm with PDGFRBRearrangement Case Report with Imatinib Therapy and Reviewof the Literature
Javier De Luca-Johnson1 Jose I Ruades Ninfea2 Lauren Pearson1 Joanna Conant1
Ronald Bryant1 Neil A Zakai12 and Mary E Tang1
1Department of Pathology and Laboratory Medicine University of Vermont Medical Center 89 Beaumont AvenueCourtyard at Given S269 Burlington VT 05405 USA2Department of Medicine Division of Hematology and Oncology University of Vermont Medical Center89 Beaumont Avenue Given E-214-UVM363 Burlington VT 05405 USA
Correspondence should be addressed to Javier De Luca-Johnson javierdeluca-johnsonuvmhealthorg
Received 19 July 2016 Accepted 1 September 2016
Academic Editor Ting Fan Leung
Copyright copy 2016 Javier De Luca-Johnson et alThis is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
We report the second case of ETV6-ACSL6 associated myeloproliferative neoplasm that has received a full course of imatinibtherapy The patient was a 51-year-old previously healthy man who presented with three months of worsening dyspnea and wasfound to have a white count of 216000cmm of which 84 were eosinophil lineage Cytogenetic analysis revealed a t(512)(q31sim33p13) FISHwas negative for PDGFRB rearrangement but additional FISH testing demonstrated anACSL6 rearrangement ETV6-ACSL6 gene fusion is a rare abnormality that most often presents as amyeloproliferative-type disorder with prominent eosinophiliaor basophilia Review of the literature yielded a total of 11 previous casesThis gene fusion results in a t(512)(q31sim33p13) thatmimicsthe t(512) found in ETV6-PDGFRB neoplasms Identification of the fusion genes involved in t(512) in eosinophilia-associatedmyeloproliferative disorders is crucial to direct an effective treatment plan In particular while tyrosine kinase inhibitor therapyis effective in patients with PDGFRB rearrangement there is little information on imatinib efficacy in patients with ETV6-ACSL6gene fusion Our patient was found to be nonresponsive to imatinib therapy
1 Introduction
We report the second case of ETV6-ACSL6 associatedmyelo-proliferative neoplasm that has failed a complete course ofimatinib therapy and review the literature on this abnor-mality ETV6-ACSL6 fusion is a rare abnormality that isassociated withmyeloproliferative disorders myelodysplasiaor acute myeloid leukemia with eosinophilia or basophiliaThe ETV6-ACSL6 results in a t(512)(q31sim33p13) thatmimicsthe t(512) found in ETV6-PDGFRB neoplasms Identifica-tion of the fusion genes involved in t(512) in eosinophilia-associated myeloproliferative disorders is crucial to directan effective treatment plan Evidence has shown sustained
clinical response molecular remission and low toxicity pro-file with imatinib treatment in patients harboring PDGFRBrearrangement [1] but there is little information on imatinibefficacy in patients with ETV6-ACSL6 gene fusion
2 Case Report
21 Clinical and Pathologic Findings A51-year-old previouslyhealthy man presented to the emergency room with a three-month history of shortness of breath palpitations intermit-tent cough and unintentional 15-pound weight loss He wastreated by his primary care physician for asthma and environ-mental allergies but his symptoms failed to improve Physical
Hindawi Publishing CorporationCase Reports in MedicineVolume 2016 Article ID 8324791 4 pageshttpdxdoiorg10115520168324791
2 Case Reports in Medicine
(a) (b)
5
12
(c)
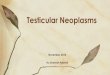
Figure 1 Myeloid neoplasm with t(512) and ETV6-ACSL6 gene fusion morphologic and cytogenetic features (a) Peripheral bloodwith a predominant population of eosinophil precursors large cells with mononuclear monolobated nuclei and abundant cytoplasmcontaining eosinophilic granules The predominant cell type is eosinophil myelocyte but there is a spectrum of forms including eosinophilmetamyelocytes eosinophils bands andmature eosinophils Promyelocytes andmyeloblasts are not observed (Wright stain 1000x) (b) Bonemarrow biopsy showing replacement of the marrow space by sheets of eosinophils and eosinophil precursors (hematoxylin and eosin 500x)(c) Partial karyogram demonstrating t(512)(q31p13) that was identified in 17 out of 20 cells cultured
examination was unremarkable except for tachycardia andhepatosplenomegaly Ultrasound of the abdomen showedhepatomegaly measuring 21 cm with normal echogenicityand an enlarged spleen measuring 18 times 13 times 8 cm Laboratorystudies revealed hemoglobin of 77 gmdL platelet count of84Kcmm and WBC of 216000cmm with 16 eosinophilsand 68 abnormal eosinophil precursors (Figure 1(a))
He was admitted to the hematology oncology serviceand scheduled for emergent bone marrow evaluation Thebone marrow biopsy demonstrated a markedly hypercellularbone marrow with extensive replacement of the marrowspace by sheets of eosinophils in various stages of maturationwith a predominance of mid-stage eosinophil forms withabnormal vacuolation hypogranulation hypolobation andnuclear-cytoplasmic asynchrony (Figure 1(b)) There was noincrease in blasts mast cells or fibrosis (CD34 tryptaseand reticulin resp) The residual myeloid elements weretoo few in number to evaluate for dysplasia Initial cyto-genetic analysis revealed a t(512)(q31sim33p13) in 17 of 20cells (Figure 1(c)) and a presumptive diagnosis of myeloidneoplasm with eosinophilia and translocation t(512) sug-gestive of PDGFRB rearrangement was made Confirmatorytesting for ETV6-PDGFRB gene fusion was negative usingboth a dual-fusion probe set and a PDGFRB break-apartprobe (Mayo Medical Laboratories) An ETV6 break-apartprobe confirmed an ETV6 rearrangement with a partnergene other than PDGFRB FISH for FIP1L1-PDGFRA andBCRABL1 were also negative In light of isolated reportsof eosinophilia with t(512) with ETV6-ACSL6 gene fusionadditional testing with an ACSL6 break-apart FISH probe(Empire Genomics LLC) was performed and demonstratedACSL6 rearrangement in 80 of cells
22 Clinical Course Soon after admission with the pre-sumptive diagnosis of myeloid neoplasmwith PDGFRB rear-rangement the patient was started on imatinib 200mgdayHydroxyurea 2 gm every 12 hours was added to rapidlyreduce the white blood cell count The patientrsquos WBC
White cell and platelet counts and transfusion requirements with medications
Day (after diagnosis)
Cou
nt (c
ells
per m
icro
liter
)
White cellsPlateletsRed cell TxPlatelet TxSolid = 2 units
ImatinibHydroxyureaInterferon
200
100
0
150100500
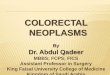
Figure 2 Summary of clinical courseThe ldquoSolid = 2 unitsrdquo refers tothe ldquoRed cell Txrdquo and the ldquoPlatelet Txrdquo If the red circle is solid thisindicates that 2 units of red cells were transfused If the green circleis solid this indicates that 2 units of platelets were transfused
hematocrit and platelet count decreased significantly butafter 10 days of treatment he required RBC and platelettransfusions so the hydroxyurea was discontinued After twoweeks he was discharged on imatinib and initially seemedto respond to therapy His white count reached a nadir of8000 and his presenting symptom of shortness of breathentirely resolved However by day 24 his white cell countrose to 130000Kcmm (Figure 2) and he was restartedon hydroxyurea The patient received imatinib 200mgdayfor four weeks and it was increased to 400mgday for anadditional week before the imatinib was discontinued due
Case Reports in Medicine 3
to lack of hematological response characterized by progres-sive leukocytosis (peak WBC count 139000cmm) anemia(hemoglobin 76 gmdL) and thrombocytopenia (plateletcount 18 Kcmm) The patient was subsequently treatedwith hydroxyurea prednisone and pegylated interferon alfaand after 8 weeks the patientrsquos WBC markedly decreasedand stabilized at 30000Kcmm However the eosinophiliapersisted and the patient required regular RBC and platelettransfusionsHe eventually elected to discontinue transfusionsupport andwas transitioned to hospice care where he passedaway nine months following his initial diagnosis
3 Discussion
Myeloid neoplasms with t(512) and ETV6-ACSL6 genefusion are rare poorly characterized hematologic neo-plasms with an aggressive clinical course characterizedby eosinophilic andor basophilic leukocytosis Literaturereview reveals 11 previous cases of myeloid neoplasmwith ETV6-ACSL6 gene fusion confirmed by either FISHRT-PCR or next-generation sequencing (NGS) with tar-geted RNA-seq [2ndash8] Several other cases of t(512) witheosinophilia or basophilia may represent additional casesbut confirmatory testing was not performed [5 9 10] Caseswith ETV6-ACSL6 gene fusion are clinically aggressive withmean survival from time of diagnosis of less than one year Asingle case demonstrated survival beyond one year [4] Otherimportant clinical features include male preponderance (9 of12 cases) and eosinophilic andor basophilic leukocytosis (12of 12 cases) All ages are affected with a range of 27ndash68 yearsand an average age of 47 years
Under current guidelines ETV6-ACSL6 neoplasms arenot classified as a unique disease entity Despite a unifyingmolecular alteration these patients present with a prominenteosinophilia or basophilia but may be classified as almostany myeloid neoplasm except chronic myeloid leukemiaOur case presented as chronic eosinophilic leukemia nototherwise specified (CEL-NOS) Among the 11 previouslypublished cases therewere three cases ofmyelodysplastic syn-drome two cases of acute myeloid leukemia and one of eachof atypical chronic myeloid leukemia polycythemia verapolycythemia veraacute myeloid leukemia overlap myelo-proliferative neoplasia not otherwise specified myelodys-plasticmyeloproliferative neoplasia overlap and CEL-NOS
The etiology of the eosinophilia in ETV6-ACSL6 is notwell understood ACSL6 encodes for acyl-CoA synthetaselong-chain family member 6 a protein that catalyzes forma-tion of acyl-CoA from fatty acids It plays a major role in fattyacid metabolism in the brain [11] and is expressed in brainfetal liver and bonemarrow and is highly conserved [2] It hasnot been associated with other neoplastic diseases [12] ETV6codes for a transcription factor that is commonly deleted ortranslocated inmyeloid and lymphoidmalignancies [7] It hasbeen implicated in leukemogenesis by generation of fusionproteins that modulate the activity of transcription factorsor kinases [3] Unlike BCR-ABL1 PDGFRA and PDGFRBthe ETV6-ACSL6 gene fusion does not result in a fusionprotein with constitutive tyrosine kinase activity Of the four
cases with molecular breakpoint analysis all four had fusionsinvolving the ETV6 region between exons 1 to 2 and thebreakpoints on ACSL6 were highly variable spanning fromthe 51015840 end of the gene to the 31015840 UTR Fusion transcripts weredetected in all four cases but did not result in a commontranscript making a fusion gene mechanism unlikely [2 3]
The 5q31 region has other genes associated witheosinophilia Telomeric to ACSL6 lies the cytokinegene cluster that includes interleukin- (IL-) 3 IL-5 andgranulocytemacrophage colony-stimulating factor (GM-CSF) These genes are the main cytokine mediators ofeosinophil proliferation and differentiation [13] Increasedexpression of IL-3 protein transcript has been documentedin two ETV6-ACSL6 cases and dysregulation of the IL-3gene due to a translocation event has been hypothesizedas a mechanism for eosinophilia [3 5] The 5q31ndash33 regionhas also been linked to familial eosinophilia (EOS) [14]Mutation screening of the IL-3 IL-5 and GM-CSF genes inEOS individuals found no mutations in these genes or in theIL-3GM-CSF enhancer region suggesting that EOS is notcaused by a mutation in these genes but by another gene inthis region [15] ACSL6 has not been investigated as a causeof EOS
Identification of the fusion genes involved in t(512) ineosinophilia-associated myeloproliferative disorders is cru-cial to direct an effective treatment plan While evidencehas shown sustained clinical response molecular remissionand low toxicity profile with imatinib treatment in patientsharboring PDGFRB rearrangement [1] there is no evidencefor imatinib efficacy in patients with ETV6-ACSL6 genefusion Our patient was treated with a full course of imatiniband was found to be nonresponsive Two other patients withETV6-ACSL6 gene fusion have been treated with imatiniband both were found to be nonresponsive The first patientreceived a short course of therapy [5] while the secondpatient received a full course (3 months) of therapy [8]Specific dosage information is lacking in the prior cases
Lack of response to imatinib is compatible with our cur-rent understanding of oncogenesis in ETV6-ACSL6 relatedtranslocation events and the lack of an obvious proteintarget for anti-tyrosine kinase therapy Notably second orthird generation tyrosine kinase inhibitors have not beenattempted to date and could be offered on an empiricbasis with intent on targeting downstream targets Patientspresenting with eosinophilia-associated myeloproliferativeneoplasm who lack overexpression of PDGFRA or PDGFRBhave been imatinib-responsive [6] emphasizing that it isreasonable to begin a therapeutic trial with tyrosine kinaseinhibitors in symptomatic patients pending further genefusion characterization
Additional therapeutic options in CEL-NOS includeMepolizumab an investigational anti-IL5 antibody that hasshown activity in patients with hypereosinophilic syndrome[16] Although ETV6-ACSL6 neoplasms usually lack IL-5 overexpression [3] there is potential for response toMepolizumab even when IL-5 is at physiologic levels [17]Alemtuzumab is an anti-CD52 monoclonal antibody thathas also been shown to produce hematological and clinical(no cytogenetic) responses in CEL-NOS but is reserved for
4 Case Reports in Medicine
patients with refractory disease because of significant adverseeffects [18] The role of bone marrow transplant has not yetbeen determined in CEL-NOS case reports have describedpromising results and currently this appears as the onlypossible curative option in CEL-NOS patients [19]
In the context of eosinophilic leukocytosis the findingof t(512) is highly suggestive of myeloid neoplasm withPDGFRB rearrangement However it is essential to confirmPDGFRB rearrangement in order to effectively direct treat-ment and predict prognosis Little is known about the patho-genesis and treatment of ETV6-ACSL6 associated neoplasmsOur case is the second to demonstrate no response to a fullcourse of imatinib therapy Further study may elucidate themechanism of disease and lead to effective therapy
Disclosure
This case was presented as an educational session (ldquoInterest-ing Case Studies in Hematopathologyrdquo) at the 2015 AnnualMeeting of the Association for Molecular Pathology inAustin Texas
Competing Interests
The authors declare that they have no conflict of interests
References
[1] MDavidN C P Cross S Burgstaller et al ldquoDurable responsesto imatinib in patients with PDGFRB fusion gene-positiveand BCR-ABL-negative chronic myeloproliferative disordersrdquoBlood vol 109 no 1 pp 61ndash64 2007
[2] F Yagasaki I Jinnai S Yoshida et al ldquoFusion of TELETV6to a novel ACS2 in myelodysplastic syndrome and acute myel-ogenous leukemia with t(512)(q31p13)rdquoGenes Chromosomes ampCancer vol 26 no 3 pp 192ndash202 1999
[3] J Cools N Mentens M D Odero et al ldquoEvidence forposition effects as a variant ETV6-mediated leukemogenicmechanism in myeloid leukemias with a t(412)(q11-q12p13) ort(512)(q31p13)rdquo Blood vol 99 no 5 pp 1776ndash1784 2002
[4] A Murati J Adelaıde V Gelsi-Boyer et al ldquot(512)(q23-31p13) with ETV6-ACSL6 gene fusion in polycythemia verardquoLeukemia vol 20 no 6 pp 1175ndash1178 2006
[5] Y Katsura K Suzukawa T Nanmoku et al ldquoMyelodysplasticsyndrome accompanied by basophilia and eosinophilia witht(512)(q31p13)rdquo Cancer Genetics and Cytogenetics vol 178 no1 pp 85ndash88 2007
[6] P Erben D Gosenca M C Muller et al ldquoScreening for diversePDGFRA or PDGFRB fusion genes is facilitated by genericquantitative reverse transcriptase polymerase chain reactionanalysisrdquo Haematologica vol 95 no 5 pp 738ndash744 2010
[7] C Haferlach U Bacher S Schnittger et al ldquoETV6 rearrange-ments are recurrent in myeloid malignancies and are frequentlyassociated with other genetic eventsrdquo Genes Chromosomes andCancer vol 51 no 4 pp 328ndash337 2012
[8] R J Su B A Jonas J Welborn J P Gregg and M ChenldquoChronic eosinophilic leukemia NOS with t(512)(q31p13)ETV6-ACSL6 gene fusion a novel variant of myeloid prolif-erative neoplasm with eosinophiliardquo Human Pathology CaseReports vol 5 pp 6ndash9 2016
[9] X Han L J Medeiros L V Abruzzo D Jones and P LinldquoChronic myeloproliferative diseases with the t(512)(q33p13)clonal evolution is associated with blast crisisrdquo American Jour-nal of Clinical Pathology vol 125 no 1 pp 49ndash56 2006
[10] G Tang L J Woods S A Wang et al ldquoChronic basophilicleukemia a rare form of chronic myeloproliferative neoplasmrdquoHuman Pathology vol 40 no 8 pp 1194ndash1199 2009
[11] K T Malhotra K Malhotra B H Lubin and F A KuypersldquoIdentification and molecular characterization of acyl-CoAsynthetase in human erythrocytes and erythroid precursorsrdquoBiochemical Journal vol 344 no 1 pp 135ndash143 1999
[12] The GeneCards Human Gene Database Weizmann Instituteof Science httpwwwgenecardsorgcgi-bincarddispplgene=acsl6
[13] S Esnault E A B Kelly Z-J Shen M W Johansson J SMalter and N N Jarjour ldquoIL-3 maintains activation of thep90S6KRPS6 pathway and increases translation in humaneosinophilsrdquo The Journal of Immunology vol 195 no 6 pp2529ndash2539 2015
[14] A Y Lin T B Nutman D Kaslow et al ldquoFamilial eosinophiliaclinical and laboratory results on a US Kindredrdquo AmericanJournal of Medical Genetics vol 76 no 3 pp 229ndash237 1998
[15] J D Rioux V A Stone M J Daly et al ldquoFamilial eosinophiliamaps to the cytokine gene cluster on human chromosomalregion 5q31-q33rdquoTheAmerican Journal of Human Genetics vol63 no 4 pp 1086ndash1094 1998
[16] P U Ogbogu B S Bochner J H Butterfield et al ldquoHyper-eosinophilic syndrome a multicenter retrospective analysisof clinical characteristics and response to therapyrdquo Journal ofAllergy and Clinical Immunology vol 124 no 6 pp 1319e3ndash1325e3 2009
[17] M E Rothenberg A D Klion F E Roufosse et al ldquoTreat-ment of patients with the hypereosinophilic syndrome withmepolizumabrdquo The New England Journal of Medicine vol 358no 12 pp 1215ndash1228 2008
[18] P Strati J Cortes S Faderl H Kantarjian and S VerstovsekldquoLong-term follow-up of patients with hypereosinophilic syn-drome treated with alemtuzumab an anti-CD52 antibodyrdquoClinical Lymphoma Myeloma and Leukemia vol 13 no 3 pp287ndash291 2013
[19] G Helbig A Soja A Bartkowska-Chrobok and S Kyrcz-Krzemien ldquoChronic eosinophilic leukemia-not otherwise spec-ified has a poor prognosis with unresponsiveness to con-ventional treatment and high risk of acute transformationrdquoAmerican Journal of Hematology vol 87 no 6 pp 643ndash6452012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Case Reports in Medicine
(a) (b)
5
12
(c)
Figure 1 Myeloid neoplasm with t(512) and ETV6-ACSL6 gene fusion morphologic and cytogenetic features (a) Peripheral bloodwith a predominant population of eosinophil precursors large cells with mononuclear monolobated nuclei and abundant cytoplasmcontaining eosinophilic granules The predominant cell type is eosinophil myelocyte but there is a spectrum of forms including eosinophilmetamyelocytes eosinophils bands andmature eosinophils Promyelocytes andmyeloblasts are not observed (Wright stain 1000x) (b) Bonemarrow biopsy showing replacement of the marrow space by sheets of eosinophils and eosinophil precursors (hematoxylin and eosin 500x)(c) Partial karyogram demonstrating t(512)(q31p13) that was identified in 17 out of 20 cells cultured
examination was unremarkable except for tachycardia andhepatosplenomegaly Ultrasound of the abdomen showedhepatomegaly measuring 21 cm with normal echogenicityand an enlarged spleen measuring 18 times 13 times 8 cm Laboratorystudies revealed hemoglobin of 77 gmdL platelet count of84Kcmm and WBC of 216000cmm with 16 eosinophilsand 68 abnormal eosinophil precursors (Figure 1(a))
He was admitted to the hematology oncology serviceand scheduled for emergent bone marrow evaluation Thebone marrow biopsy demonstrated a markedly hypercellularbone marrow with extensive replacement of the marrowspace by sheets of eosinophils in various stages of maturationwith a predominance of mid-stage eosinophil forms withabnormal vacuolation hypogranulation hypolobation andnuclear-cytoplasmic asynchrony (Figure 1(b)) There was noincrease in blasts mast cells or fibrosis (CD34 tryptaseand reticulin resp) The residual myeloid elements weretoo few in number to evaluate for dysplasia Initial cyto-genetic analysis revealed a t(512)(q31sim33p13) in 17 of 20cells (Figure 1(c)) and a presumptive diagnosis of myeloidneoplasm with eosinophilia and translocation t(512) sug-gestive of PDGFRB rearrangement was made Confirmatorytesting for ETV6-PDGFRB gene fusion was negative usingboth a dual-fusion probe set and a PDGFRB break-apartprobe (Mayo Medical Laboratories) An ETV6 break-apartprobe confirmed an ETV6 rearrangement with a partnergene other than PDGFRB FISH for FIP1L1-PDGFRA andBCRABL1 were also negative In light of isolated reportsof eosinophilia with t(512) with ETV6-ACSL6 gene fusionadditional testing with an ACSL6 break-apart FISH probe(Empire Genomics LLC) was performed and demonstratedACSL6 rearrangement in 80 of cells
22 Clinical Course Soon after admission with the pre-sumptive diagnosis of myeloid neoplasmwith PDGFRB rear-rangement the patient was started on imatinib 200mgdayHydroxyurea 2 gm every 12 hours was added to rapidlyreduce the white blood cell count The patientrsquos WBC
White cell and platelet counts and transfusion requirements with medications
Day (after diagnosis)
Cou
nt (c
ells
per m
icro
liter
)
White cellsPlateletsRed cell TxPlatelet TxSolid = 2 units
ImatinibHydroxyureaInterferon
200
100
0
150100500
Figure 2 Summary of clinical courseThe ldquoSolid = 2 unitsrdquo refers tothe ldquoRed cell Txrdquo and the ldquoPlatelet Txrdquo If the red circle is solid thisindicates that 2 units of red cells were transfused If the green circleis solid this indicates that 2 units of platelets were transfused
hematocrit and platelet count decreased significantly butafter 10 days of treatment he required RBC and platelettransfusions so the hydroxyurea was discontinued After twoweeks he was discharged on imatinib and initially seemedto respond to therapy His white count reached a nadir of8000 and his presenting symptom of shortness of breathentirely resolved However by day 24 his white cell countrose to 130000Kcmm (Figure 2) and he was restartedon hydroxyurea The patient received imatinib 200mgdayfor four weeks and it was increased to 400mgday for anadditional week before the imatinib was discontinued due
Case Reports in Medicine 3
to lack of hematological response characterized by progres-sive leukocytosis (peak WBC count 139000cmm) anemia(hemoglobin 76 gmdL) and thrombocytopenia (plateletcount 18 Kcmm) The patient was subsequently treatedwith hydroxyurea prednisone and pegylated interferon alfaand after 8 weeks the patientrsquos WBC markedly decreasedand stabilized at 30000Kcmm However the eosinophiliapersisted and the patient required regular RBC and platelettransfusionsHe eventually elected to discontinue transfusionsupport andwas transitioned to hospice care where he passedaway nine months following his initial diagnosis
3 Discussion
Myeloid neoplasms with t(512) and ETV6-ACSL6 genefusion are rare poorly characterized hematologic neo-plasms with an aggressive clinical course characterizedby eosinophilic andor basophilic leukocytosis Literaturereview reveals 11 previous cases of myeloid neoplasmwith ETV6-ACSL6 gene fusion confirmed by either FISHRT-PCR or next-generation sequencing (NGS) with tar-geted RNA-seq [2ndash8] Several other cases of t(512) witheosinophilia or basophilia may represent additional casesbut confirmatory testing was not performed [5 9 10] Caseswith ETV6-ACSL6 gene fusion are clinically aggressive withmean survival from time of diagnosis of less than one year Asingle case demonstrated survival beyond one year [4] Otherimportant clinical features include male preponderance (9 of12 cases) and eosinophilic andor basophilic leukocytosis (12of 12 cases) All ages are affected with a range of 27ndash68 yearsand an average age of 47 years
Under current guidelines ETV6-ACSL6 neoplasms arenot classified as a unique disease entity Despite a unifyingmolecular alteration these patients present with a prominenteosinophilia or basophilia but may be classified as almostany myeloid neoplasm except chronic myeloid leukemiaOur case presented as chronic eosinophilic leukemia nototherwise specified (CEL-NOS) Among the 11 previouslypublished cases therewere three cases ofmyelodysplastic syn-drome two cases of acute myeloid leukemia and one of eachof atypical chronic myeloid leukemia polycythemia verapolycythemia veraacute myeloid leukemia overlap myelo-proliferative neoplasia not otherwise specified myelodys-plasticmyeloproliferative neoplasia overlap and CEL-NOS
The etiology of the eosinophilia in ETV6-ACSL6 is notwell understood ACSL6 encodes for acyl-CoA synthetaselong-chain family member 6 a protein that catalyzes forma-tion of acyl-CoA from fatty acids It plays a major role in fattyacid metabolism in the brain [11] and is expressed in brainfetal liver and bonemarrow and is highly conserved [2] It hasnot been associated with other neoplastic diseases [12] ETV6codes for a transcription factor that is commonly deleted ortranslocated inmyeloid and lymphoidmalignancies [7] It hasbeen implicated in leukemogenesis by generation of fusionproteins that modulate the activity of transcription factorsor kinases [3] Unlike BCR-ABL1 PDGFRA and PDGFRBthe ETV6-ACSL6 gene fusion does not result in a fusionprotein with constitutive tyrosine kinase activity Of the four
cases with molecular breakpoint analysis all four had fusionsinvolving the ETV6 region between exons 1 to 2 and thebreakpoints on ACSL6 were highly variable spanning fromthe 51015840 end of the gene to the 31015840 UTR Fusion transcripts weredetected in all four cases but did not result in a commontranscript making a fusion gene mechanism unlikely [2 3]
The 5q31 region has other genes associated witheosinophilia Telomeric to ACSL6 lies the cytokinegene cluster that includes interleukin- (IL-) 3 IL-5 andgranulocytemacrophage colony-stimulating factor (GM-CSF) These genes are the main cytokine mediators ofeosinophil proliferation and differentiation [13] Increasedexpression of IL-3 protein transcript has been documentedin two ETV6-ACSL6 cases and dysregulation of the IL-3gene due to a translocation event has been hypothesizedas a mechanism for eosinophilia [3 5] The 5q31ndash33 regionhas also been linked to familial eosinophilia (EOS) [14]Mutation screening of the IL-3 IL-5 and GM-CSF genes inEOS individuals found no mutations in these genes or in theIL-3GM-CSF enhancer region suggesting that EOS is notcaused by a mutation in these genes but by another gene inthis region [15] ACSL6 has not been investigated as a causeof EOS
Identification of the fusion genes involved in t(512) ineosinophilia-associated myeloproliferative disorders is cru-cial to direct an effective treatment plan While evidencehas shown sustained clinical response molecular remissionand low toxicity profile with imatinib treatment in patientsharboring PDGFRB rearrangement [1] there is no evidencefor imatinib efficacy in patients with ETV6-ACSL6 genefusion Our patient was treated with a full course of imatiniband was found to be nonresponsive Two other patients withETV6-ACSL6 gene fusion have been treated with imatiniband both were found to be nonresponsive The first patientreceived a short course of therapy [5] while the secondpatient received a full course (3 months) of therapy [8]Specific dosage information is lacking in the prior cases
Lack of response to imatinib is compatible with our cur-rent understanding of oncogenesis in ETV6-ACSL6 relatedtranslocation events and the lack of an obvious proteintarget for anti-tyrosine kinase therapy Notably second orthird generation tyrosine kinase inhibitors have not beenattempted to date and could be offered on an empiricbasis with intent on targeting downstream targets Patientspresenting with eosinophilia-associated myeloproliferativeneoplasm who lack overexpression of PDGFRA or PDGFRBhave been imatinib-responsive [6] emphasizing that it isreasonable to begin a therapeutic trial with tyrosine kinaseinhibitors in symptomatic patients pending further genefusion characterization
Additional therapeutic options in CEL-NOS includeMepolizumab an investigational anti-IL5 antibody that hasshown activity in patients with hypereosinophilic syndrome[16] Although ETV6-ACSL6 neoplasms usually lack IL-5 overexpression [3] there is potential for response toMepolizumab even when IL-5 is at physiologic levels [17]Alemtuzumab is an anti-CD52 monoclonal antibody thathas also been shown to produce hematological and clinical(no cytogenetic) responses in CEL-NOS but is reserved for
4 Case Reports in Medicine
patients with refractory disease because of significant adverseeffects [18] The role of bone marrow transplant has not yetbeen determined in CEL-NOS case reports have describedpromising results and currently this appears as the onlypossible curative option in CEL-NOS patients [19]
In the context of eosinophilic leukocytosis the findingof t(512) is highly suggestive of myeloid neoplasm withPDGFRB rearrangement However it is essential to confirmPDGFRB rearrangement in order to effectively direct treat-ment and predict prognosis Little is known about the patho-genesis and treatment of ETV6-ACSL6 associated neoplasmsOur case is the second to demonstrate no response to a fullcourse of imatinib therapy Further study may elucidate themechanism of disease and lead to effective therapy
Disclosure
This case was presented as an educational session (ldquoInterest-ing Case Studies in Hematopathologyrdquo) at the 2015 AnnualMeeting of the Association for Molecular Pathology inAustin Texas
Competing Interests
The authors declare that they have no conflict of interests
References
[1] MDavidN C P Cross S Burgstaller et al ldquoDurable responsesto imatinib in patients with PDGFRB fusion gene-positiveand BCR-ABL-negative chronic myeloproliferative disordersrdquoBlood vol 109 no 1 pp 61ndash64 2007
[2] F Yagasaki I Jinnai S Yoshida et al ldquoFusion of TELETV6to a novel ACS2 in myelodysplastic syndrome and acute myel-ogenous leukemia with t(512)(q31p13)rdquoGenes Chromosomes ampCancer vol 26 no 3 pp 192ndash202 1999
[3] J Cools N Mentens M D Odero et al ldquoEvidence forposition effects as a variant ETV6-mediated leukemogenicmechanism in myeloid leukemias with a t(412)(q11-q12p13) ort(512)(q31p13)rdquo Blood vol 99 no 5 pp 1776ndash1784 2002
[4] A Murati J Adelaıde V Gelsi-Boyer et al ldquot(512)(q23-31p13) with ETV6-ACSL6 gene fusion in polycythemia verardquoLeukemia vol 20 no 6 pp 1175ndash1178 2006
[5] Y Katsura K Suzukawa T Nanmoku et al ldquoMyelodysplasticsyndrome accompanied by basophilia and eosinophilia witht(512)(q31p13)rdquo Cancer Genetics and Cytogenetics vol 178 no1 pp 85ndash88 2007
[6] P Erben D Gosenca M C Muller et al ldquoScreening for diversePDGFRA or PDGFRB fusion genes is facilitated by genericquantitative reverse transcriptase polymerase chain reactionanalysisrdquo Haematologica vol 95 no 5 pp 738ndash744 2010
[7] C Haferlach U Bacher S Schnittger et al ldquoETV6 rearrange-ments are recurrent in myeloid malignancies and are frequentlyassociated with other genetic eventsrdquo Genes Chromosomes andCancer vol 51 no 4 pp 328ndash337 2012
[8] R J Su B A Jonas J Welborn J P Gregg and M ChenldquoChronic eosinophilic leukemia NOS with t(512)(q31p13)ETV6-ACSL6 gene fusion a novel variant of myeloid prolif-erative neoplasm with eosinophiliardquo Human Pathology CaseReports vol 5 pp 6ndash9 2016
[9] X Han L J Medeiros L V Abruzzo D Jones and P LinldquoChronic myeloproliferative diseases with the t(512)(q33p13)clonal evolution is associated with blast crisisrdquo American Jour-nal of Clinical Pathology vol 125 no 1 pp 49ndash56 2006
[10] G Tang L J Woods S A Wang et al ldquoChronic basophilicleukemia a rare form of chronic myeloproliferative neoplasmrdquoHuman Pathology vol 40 no 8 pp 1194ndash1199 2009
[11] K T Malhotra K Malhotra B H Lubin and F A KuypersldquoIdentification and molecular characterization of acyl-CoAsynthetase in human erythrocytes and erythroid precursorsrdquoBiochemical Journal vol 344 no 1 pp 135ndash143 1999
[12] The GeneCards Human Gene Database Weizmann Instituteof Science httpwwwgenecardsorgcgi-bincarddispplgene=acsl6
[13] S Esnault E A B Kelly Z-J Shen M W Johansson J SMalter and N N Jarjour ldquoIL-3 maintains activation of thep90S6KRPS6 pathway and increases translation in humaneosinophilsrdquo The Journal of Immunology vol 195 no 6 pp2529ndash2539 2015
[14] A Y Lin T B Nutman D Kaslow et al ldquoFamilial eosinophiliaclinical and laboratory results on a US Kindredrdquo AmericanJournal of Medical Genetics vol 76 no 3 pp 229ndash237 1998
[15] J D Rioux V A Stone M J Daly et al ldquoFamilial eosinophiliamaps to the cytokine gene cluster on human chromosomalregion 5q31-q33rdquoTheAmerican Journal of Human Genetics vol63 no 4 pp 1086ndash1094 1998
[16] P U Ogbogu B S Bochner J H Butterfield et al ldquoHyper-eosinophilic syndrome a multicenter retrospective analysisof clinical characteristics and response to therapyrdquo Journal ofAllergy and Clinical Immunology vol 124 no 6 pp 1319e3ndash1325e3 2009
[17] M E Rothenberg A D Klion F E Roufosse et al ldquoTreat-ment of patients with the hypereosinophilic syndrome withmepolizumabrdquo The New England Journal of Medicine vol 358no 12 pp 1215ndash1228 2008
[18] P Strati J Cortes S Faderl H Kantarjian and S VerstovsekldquoLong-term follow-up of patients with hypereosinophilic syn-drome treated with alemtuzumab an anti-CD52 antibodyrdquoClinical Lymphoma Myeloma and Leukemia vol 13 no 3 pp287ndash291 2013
[19] G Helbig A Soja A Bartkowska-Chrobok and S Kyrcz-Krzemien ldquoChronic eosinophilic leukemia-not otherwise spec-ified has a poor prognosis with unresponsiveness to con-ventional treatment and high risk of acute transformationrdquoAmerican Journal of Hematology vol 87 no 6 pp 643ndash6452012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Case Reports in Medicine 3
to lack of hematological response characterized by progres-sive leukocytosis (peak WBC count 139000cmm) anemia(hemoglobin 76 gmdL) and thrombocytopenia (plateletcount 18 Kcmm) The patient was subsequently treatedwith hydroxyurea prednisone and pegylated interferon alfaand after 8 weeks the patientrsquos WBC markedly decreasedand stabilized at 30000Kcmm However the eosinophiliapersisted and the patient required regular RBC and platelettransfusionsHe eventually elected to discontinue transfusionsupport andwas transitioned to hospice care where he passedaway nine months following his initial diagnosis
3 Discussion
Myeloid neoplasms with t(512) and ETV6-ACSL6 genefusion are rare poorly characterized hematologic neo-plasms with an aggressive clinical course characterizedby eosinophilic andor basophilic leukocytosis Literaturereview reveals 11 previous cases of myeloid neoplasmwith ETV6-ACSL6 gene fusion confirmed by either FISHRT-PCR or next-generation sequencing (NGS) with tar-geted RNA-seq [2ndash8] Several other cases of t(512) witheosinophilia or basophilia may represent additional casesbut confirmatory testing was not performed [5 9 10] Caseswith ETV6-ACSL6 gene fusion are clinically aggressive withmean survival from time of diagnosis of less than one year Asingle case demonstrated survival beyond one year [4] Otherimportant clinical features include male preponderance (9 of12 cases) and eosinophilic andor basophilic leukocytosis (12of 12 cases) All ages are affected with a range of 27ndash68 yearsand an average age of 47 years
Under current guidelines ETV6-ACSL6 neoplasms arenot classified as a unique disease entity Despite a unifyingmolecular alteration these patients present with a prominenteosinophilia or basophilia but may be classified as almostany myeloid neoplasm except chronic myeloid leukemiaOur case presented as chronic eosinophilic leukemia nototherwise specified (CEL-NOS) Among the 11 previouslypublished cases therewere three cases ofmyelodysplastic syn-drome two cases of acute myeloid leukemia and one of eachof atypical chronic myeloid leukemia polycythemia verapolycythemia veraacute myeloid leukemia overlap myelo-proliferative neoplasia not otherwise specified myelodys-plasticmyeloproliferative neoplasia overlap and CEL-NOS
The etiology of the eosinophilia in ETV6-ACSL6 is notwell understood ACSL6 encodes for acyl-CoA synthetaselong-chain family member 6 a protein that catalyzes forma-tion of acyl-CoA from fatty acids It plays a major role in fattyacid metabolism in the brain [11] and is expressed in brainfetal liver and bonemarrow and is highly conserved [2] It hasnot been associated with other neoplastic diseases [12] ETV6codes for a transcription factor that is commonly deleted ortranslocated inmyeloid and lymphoidmalignancies [7] It hasbeen implicated in leukemogenesis by generation of fusionproteins that modulate the activity of transcription factorsor kinases [3] Unlike BCR-ABL1 PDGFRA and PDGFRBthe ETV6-ACSL6 gene fusion does not result in a fusionprotein with constitutive tyrosine kinase activity Of the four
cases with molecular breakpoint analysis all four had fusionsinvolving the ETV6 region between exons 1 to 2 and thebreakpoints on ACSL6 were highly variable spanning fromthe 51015840 end of the gene to the 31015840 UTR Fusion transcripts weredetected in all four cases but did not result in a commontranscript making a fusion gene mechanism unlikely [2 3]
The 5q31 region has other genes associated witheosinophilia Telomeric to ACSL6 lies the cytokinegene cluster that includes interleukin- (IL-) 3 IL-5 andgranulocytemacrophage colony-stimulating factor (GM-CSF) These genes are the main cytokine mediators ofeosinophil proliferation and differentiation [13] Increasedexpression of IL-3 protein transcript has been documentedin two ETV6-ACSL6 cases and dysregulation of the IL-3gene due to a translocation event has been hypothesizedas a mechanism for eosinophilia [3 5] The 5q31ndash33 regionhas also been linked to familial eosinophilia (EOS) [14]Mutation screening of the IL-3 IL-5 and GM-CSF genes inEOS individuals found no mutations in these genes or in theIL-3GM-CSF enhancer region suggesting that EOS is notcaused by a mutation in these genes but by another gene inthis region [15] ACSL6 has not been investigated as a causeof EOS
Identification of the fusion genes involved in t(512) ineosinophilia-associated myeloproliferative disorders is cru-cial to direct an effective treatment plan While evidencehas shown sustained clinical response molecular remissionand low toxicity profile with imatinib treatment in patientsharboring PDGFRB rearrangement [1] there is no evidencefor imatinib efficacy in patients with ETV6-ACSL6 genefusion Our patient was treated with a full course of imatiniband was found to be nonresponsive Two other patients withETV6-ACSL6 gene fusion have been treated with imatiniband both were found to be nonresponsive The first patientreceived a short course of therapy [5] while the secondpatient received a full course (3 months) of therapy [8]Specific dosage information is lacking in the prior cases
Lack of response to imatinib is compatible with our cur-rent understanding of oncogenesis in ETV6-ACSL6 relatedtranslocation events and the lack of an obvious proteintarget for anti-tyrosine kinase therapy Notably second orthird generation tyrosine kinase inhibitors have not beenattempted to date and could be offered on an empiricbasis with intent on targeting downstream targets Patientspresenting with eosinophilia-associated myeloproliferativeneoplasm who lack overexpression of PDGFRA or PDGFRBhave been imatinib-responsive [6] emphasizing that it isreasonable to begin a therapeutic trial with tyrosine kinaseinhibitors in symptomatic patients pending further genefusion characterization
Additional therapeutic options in CEL-NOS includeMepolizumab an investigational anti-IL5 antibody that hasshown activity in patients with hypereosinophilic syndrome[16] Although ETV6-ACSL6 neoplasms usually lack IL-5 overexpression [3] there is potential for response toMepolizumab even when IL-5 is at physiologic levels [17]Alemtuzumab is an anti-CD52 monoclonal antibody thathas also been shown to produce hematological and clinical(no cytogenetic) responses in CEL-NOS but is reserved for
4 Case Reports in Medicine
patients with refractory disease because of significant adverseeffects [18] The role of bone marrow transplant has not yetbeen determined in CEL-NOS case reports have describedpromising results and currently this appears as the onlypossible curative option in CEL-NOS patients [19]
In the context of eosinophilic leukocytosis the findingof t(512) is highly suggestive of myeloid neoplasm withPDGFRB rearrangement However it is essential to confirmPDGFRB rearrangement in order to effectively direct treat-ment and predict prognosis Little is known about the patho-genesis and treatment of ETV6-ACSL6 associated neoplasmsOur case is the second to demonstrate no response to a fullcourse of imatinib therapy Further study may elucidate themechanism of disease and lead to effective therapy
Disclosure
This case was presented as an educational session (ldquoInterest-ing Case Studies in Hematopathologyrdquo) at the 2015 AnnualMeeting of the Association for Molecular Pathology inAustin Texas
Competing Interests
The authors declare that they have no conflict of interests
References
[1] MDavidN C P Cross S Burgstaller et al ldquoDurable responsesto imatinib in patients with PDGFRB fusion gene-positiveand BCR-ABL-negative chronic myeloproliferative disordersrdquoBlood vol 109 no 1 pp 61ndash64 2007
[2] F Yagasaki I Jinnai S Yoshida et al ldquoFusion of TELETV6to a novel ACS2 in myelodysplastic syndrome and acute myel-ogenous leukemia with t(512)(q31p13)rdquoGenes Chromosomes ampCancer vol 26 no 3 pp 192ndash202 1999
[3] J Cools N Mentens M D Odero et al ldquoEvidence forposition effects as a variant ETV6-mediated leukemogenicmechanism in myeloid leukemias with a t(412)(q11-q12p13) ort(512)(q31p13)rdquo Blood vol 99 no 5 pp 1776ndash1784 2002
[4] A Murati J Adelaıde V Gelsi-Boyer et al ldquot(512)(q23-31p13) with ETV6-ACSL6 gene fusion in polycythemia verardquoLeukemia vol 20 no 6 pp 1175ndash1178 2006
[5] Y Katsura K Suzukawa T Nanmoku et al ldquoMyelodysplasticsyndrome accompanied by basophilia and eosinophilia witht(512)(q31p13)rdquo Cancer Genetics and Cytogenetics vol 178 no1 pp 85ndash88 2007
[6] P Erben D Gosenca M C Muller et al ldquoScreening for diversePDGFRA or PDGFRB fusion genes is facilitated by genericquantitative reverse transcriptase polymerase chain reactionanalysisrdquo Haematologica vol 95 no 5 pp 738ndash744 2010
[7] C Haferlach U Bacher S Schnittger et al ldquoETV6 rearrange-ments are recurrent in myeloid malignancies and are frequentlyassociated with other genetic eventsrdquo Genes Chromosomes andCancer vol 51 no 4 pp 328ndash337 2012
[8] R J Su B A Jonas J Welborn J P Gregg and M ChenldquoChronic eosinophilic leukemia NOS with t(512)(q31p13)ETV6-ACSL6 gene fusion a novel variant of myeloid prolif-erative neoplasm with eosinophiliardquo Human Pathology CaseReports vol 5 pp 6ndash9 2016
[9] X Han L J Medeiros L V Abruzzo D Jones and P LinldquoChronic myeloproliferative diseases with the t(512)(q33p13)clonal evolution is associated with blast crisisrdquo American Jour-nal of Clinical Pathology vol 125 no 1 pp 49ndash56 2006
[10] G Tang L J Woods S A Wang et al ldquoChronic basophilicleukemia a rare form of chronic myeloproliferative neoplasmrdquoHuman Pathology vol 40 no 8 pp 1194ndash1199 2009
[11] K T Malhotra K Malhotra B H Lubin and F A KuypersldquoIdentification and molecular characterization of acyl-CoAsynthetase in human erythrocytes and erythroid precursorsrdquoBiochemical Journal vol 344 no 1 pp 135ndash143 1999
[12] The GeneCards Human Gene Database Weizmann Instituteof Science httpwwwgenecardsorgcgi-bincarddispplgene=acsl6
[13] S Esnault E A B Kelly Z-J Shen M W Johansson J SMalter and N N Jarjour ldquoIL-3 maintains activation of thep90S6KRPS6 pathway and increases translation in humaneosinophilsrdquo The Journal of Immunology vol 195 no 6 pp2529ndash2539 2015
[14] A Y Lin T B Nutman D Kaslow et al ldquoFamilial eosinophiliaclinical and laboratory results on a US Kindredrdquo AmericanJournal of Medical Genetics vol 76 no 3 pp 229ndash237 1998
[15] J D Rioux V A Stone M J Daly et al ldquoFamilial eosinophiliamaps to the cytokine gene cluster on human chromosomalregion 5q31-q33rdquoTheAmerican Journal of Human Genetics vol63 no 4 pp 1086ndash1094 1998
[16] P U Ogbogu B S Bochner J H Butterfield et al ldquoHyper-eosinophilic syndrome a multicenter retrospective analysisof clinical characteristics and response to therapyrdquo Journal ofAllergy and Clinical Immunology vol 124 no 6 pp 1319e3ndash1325e3 2009
[17] M E Rothenberg A D Klion F E Roufosse et al ldquoTreat-ment of patients with the hypereosinophilic syndrome withmepolizumabrdquo The New England Journal of Medicine vol 358no 12 pp 1215ndash1228 2008
[18] P Strati J Cortes S Faderl H Kantarjian and S VerstovsekldquoLong-term follow-up of patients with hypereosinophilic syn-drome treated with alemtuzumab an anti-CD52 antibodyrdquoClinical Lymphoma Myeloma and Leukemia vol 13 no 3 pp287ndash291 2013
[19] G Helbig A Soja A Bartkowska-Chrobok and S Kyrcz-Krzemien ldquoChronic eosinophilic leukemia-not otherwise spec-ified has a poor prognosis with unresponsiveness to con-ventional treatment and high risk of acute transformationrdquoAmerican Journal of Hematology vol 87 no 6 pp 643ndash6452012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Case Reports in Medicine
patients with refractory disease because of significant adverseeffects [18] The role of bone marrow transplant has not yetbeen determined in CEL-NOS case reports have describedpromising results and currently this appears as the onlypossible curative option in CEL-NOS patients [19]
In the context of eosinophilic leukocytosis the findingof t(512) is highly suggestive of myeloid neoplasm withPDGFRB rearrangement However it is essential to confirmPDGFRB rearrangement in order to effectively direct treat-ment and predict prognosis Little is known about the patho-genesis and treatment of ETV6-ACSL6 associated neoplasmsOur case is the second to demonstrate no response to a fullcourse of imatinib therapy Further study may elucidate themechanism of disease and lead to effective therapy
Disclosure
This case was presented as an educational session (ldquoInterest-ing Case Studies in Hematopathologyrdquo) at the 2015 AnnualMeeting of the Association for Molecular Pathology inAustin Texas
Competing Interests
The authors declare that they have no conflict of interests
References
[1] MDavidN C P Cross S Burgstaller et al ldquoDurable responsesto imatinib in patients with PDGFRB fusion gene-positiveand BCR-ABL-negative chronic myeloproliferative disordersrdquoBlood vol 109 no 1 pp 61ndash64 2007
[2] F Yagasaki I Jinnai S Yoshida et al ldquoFusion of TELETV6to a novel ACS2 in myelodysplastic syndrome and acute myel-ogenous leukemia with t(512)(q31p13)rdquoGenes Chromosomes ampCancer vol 26 no 3 pp 192ndash202 1999
[3] J Cools N Mentens M D Odero et al ldquoEvidence forposition effects as a variant ETV6-mediated leukemogenicmechanism in myeloid leukemias with a t(412)(q11-q12p13) ort(512)(q31p13)rdquo Blood vol 99 no 5 pp 1776ndash1784 2002
[4] A Murati J Adelaıde V Gelsi-Boyer et al ldquot(512)(q23-31p13) with ETV6-ACSL6 gene fusion in polycythemia verardquoLeukemia vol 20 no 6 pp 1175ndash1178 2006
[5] Y Katsura K Suzukawa T Nanmoku et al ldquoMyelodysplasticsyndrome accompanied by basophilia and eosinophilia witht(512)(q31p13)rdquo Cancer Genetics and Cytogenetics vol 178 no1 pp 85ndash88 2007
[6] P Erben D Gosenca M C Muller et al ldquoScreening for diversePDGFRA or PDGFRB fusion genes is facilitated by genericquantitative reverse transcriptase polymerase chain reactionanalysisrdquo Haematologica vol 95 no 5 pp 738ndash744 2010
[7] C Haferlach U Bacher S Schnittger et al ldquoETV6 rearrange-ments are recurrent in myeloid malignancies and are frequentlyassociated with other genetic eventsrdquo Genes Chromosomes andCancer vol 51 no 4 pp 328ndash337 2012
[8] R J Su B A Jonas J Welborn J P Gregg and M ChenldquoChronic eosinophilic leukemia NOS with t(512)(q31p13)ETV6-ACSL6 gene fusion a novel variant of myeloid prolif-erative neoplasm with eosinophiliardquo Human Pathology CaseReports vol 5 pp 6ndash9 2016
[9] X Han L J Medeiros L V Abruzzo D Jones and P LinldquoChronic myeloproliferative diseases with the t(512)(q33p13)clonal evolution is associated with blast crisisrdquo American Jour-nal of Clinical Pathology vol 125 no 1 pp 49ndash56 2006
[10] G Tang L J Woods S A Wang et al ldquoChronic basophilicleukemia a rare form of chronic myeloproliferative neoplasmrdquoHuman Pathology vol 40 no 8 pp 1194ndash1199 2009
[11] K T Malhotra K Malhotra B H Lubin and F A KuypersldquoIdentification and molecular characterization of acyl-CoAsynthetase in human erythrocytes and erythroid precursorsrdquoBiochemical Journal vol 344 no 1 pp 135ndash143 1999
[12] The GeneCards Human Gene Database Weizmann Instituteof Science httpwwwgenecardsorgcgi-bincarddispplgene=acsl6
[13] S Esnault E A B Kelly Z-J Shen M W Johansson J SMalter and N N Jarjour ldquoIL-3 maintains activation of thep90S6KRPS6 pathway and increases translation in humaneosinophilsrdquo The Journal of Immunology vol 195 no 6 pp2529ndash2539 2015
[14] A Y Lin T B Nutman D Kaslow et al ldquoFamilial eosinophiliaclinical and laboratory results on a US Kindredrdquo AmericanJournal of Medical Genetics vol 76 no 3 pp 229ndash237 1998
[15] J D Rioux V A Stone M J Daly et al ldquoFamilial eosinophiliamaps to the cytokine gene cluster on human chromosomalregion 5q31-q33rdquoTheAmerican Journal of Human Genetics vol63 no 4 pp 1086ndash1094 1998
[16] P U Ogbogu B S Bochner J H Butterfield et al ldquoHyper-eosinophilic syndrome a multicenter retrospective analysisof clinical characteristics and response to therapyrdquo Journal ofAllergy and Clinical Immunology vol 124 no 6 pp 1319e3ndash1325e3 2009
[17] M E Rothenberg A D Klion F E Roufosse et al ldquoTreat-ment of patients with the hypereosinophilic syndrome withmepolizumabrdquo The New England Journal of Medicine vol 358no 12 pp 1215ndash1228 2008
[18] P Strati J Cortes S Faderl H Kantarjian and S VerstovsekldquoLong-term follow-up of patients with hypereosinophilic syn-drome treated with alemtuzumab an anti-CD52 antibodyrdquoClinical Lymphoma Myeloma and Leukemia vol 13 no 3 pp287ndash291 2013
[19] G Helbig A Soja A Bartkowska-Chrobok and S Kyrcz-Krzemien ldquoChronic eosinophilic leukemia-not otherwise spec-ified has a poor prognosis with unresponsiveness to con-ventional treatment and high risk of acute transformationrdquoAmerican Journal of Hematology vol 87 no 6 pp 643ndash6452012
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom