Embed Size (px)
Citation preview

IJCRI – International Journal of Case Reports and Images, Vol. 3 No. 8, August 201 2. ISSN – [0976-31 98]
IJCRI 201 2;3(8):34–38.www.ijcasereportsandimages.com
Aggressive osteoblastoma of ilium: Diagnosed on FNACLubna Khan, MK Gupta, PK Singh, Asha Agarwal
ABSTRACTIntroduction: Aggressive osteoblastoma is a raretumor which has a higher growth potential thanconventional osteoblastomas and high risk ofrecurrence. Case Report: An aggressiveosteoblastoma of ilium diagnosed on cytologywhich had three recurrences. Osteolytic lesionof hemate bone occurred in a 23yearoldpatient. Tumor was excised and diagnosed asosteoblastoma on histopathology. First recurrencewas managed with excision and implantation ofrods, and bony chips from right iliac bone.Second recurrence was similarly managed byimplantation of bony chips from the other iliacbone. Below elbow amputation was performedfollowing third recurrence. After eleven monthsfrom the last surgery patient developed swellingof iliac bone and pulmonary metastasis.Conclustion: The case highlights the biologicaldiversity of aggressive osteoblastoma and itspotential for implantation at the site of surgeryand distant metastasis. The case illustrates thedifficulties which may be encountered indifferentiating between benign and malignantform of osteoblastoma, and between aggressiveosteoblastoma and osteosarcoma.
Keywords: Aggressive Osteoblastoma,Osteosarcoma, Fine needle aspiration cytology.*********
Khan L, Gupta MK, Singh PK, Agarwal A. Aggressiveosteoblastoma of ilium: Diagnosed on FNAC.International Journal of Case Reports and Images2012;3(8):34–38.*********
doi:10.5348/ijcri201208163CR10
INTRODUCTIONOsteoblastoma is an uncommon primary neoplasmof the bone. It has clinical and histologicalmanifestations similar to those of osteoid osteoma;therefore, some consider the two tumors to be variantsof the same disease, with osteoblastoma representing agiant osteoid osteoma. However, an aggressive type ofosteoblastoma has been recognized, making therelationship less clear.There is continuing debate in the literature regardingrecurrent aggressive osteoblastic lesions with epithelioidosteoblasts, as to whether these represent benign,locally aggressive lesions [1] or osteosarcomas [2].Aggressive osteoblastoma has unpredictable clinicalcourse. A case of aggressive osteoblastoma is presentedwhich had three recurrences along with implantation oftumor at surgical site and pulmonary metastasis over aperiod of 3 years and 4 months.
CASE REPORTA 23yearold male, presented with mild pain at thedorsum of hand around wrist joint. Thereafter graduallyincreasing 2x2 cm, hard, non mobile and non tenderswelling appeared around the same region over a period
CASE REPORT OPEN ACCESS
Lubna Khan1 , MK Gupta2, PK Singh3, Asha Agarwal3
Affi l iations: 1MD, (PATH), Assistant Professor, Dept. ofPathology, GSVM Medical College, Kanpur, U.P, India;2MD, (PATH), Ex- Junior Resident, Dept. of Pathology,GSVM Medical College, Kanpur, U.P, India; 3MD, (PATH),Professor, Dept. of Pathology, GSVM Medical College,Kanpur, U.P, India.Corresponding Author: Lubna Khan, Warden House, U.GGirls Hostel, GSVM Medical College Campus, Kanpur-208002, , Uttar Pradesh (U.P), India; Ph:0091 993671 2330; E-mail : lkhan1@rediffmail .com
Received: 1 6 June 2011Accepted: 1 3 Apri l 201 2Published: 01 August 201 2
Khan et al. 34

IJCRI – International Journal of Case Reports and Images, Vol. 3 No. 8, August 201 2. ISSN – [0976-31 98]
IJCRI 201 2;3(8):34–38.www.ijcasereportsandimages.com Khan et al. 35
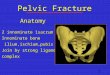
of 2 months. On Xray osteolytic lesion of hemate bonewas detected. Excisional biopsy was performed and itwas diagnosed as osteoblastoma on histopathology.After 11 months 2x3 cm, hard, fixed non tender tumorrecurred for which patient was reoperated and rodswere implanted along with bony chips taken from rightiliac bone. Unfortunately, 2x3 cm hard fixed nontendertumor again recurred after a year for which patient wasreoperated and rods were implanted along with bonychips which were now taken from left iliac bone. Lesionwas diagnosed as osteoblastoma with active osteoblasticactivity on histopathological investigation.Third recurrence of tumor (4x4 cm) occurred afterfive months and level of alkaline phosphatase wasraised (343 IU/L). Below left elbow joint amputationwas performed. Patient was lost in the follow up. After 1year 2 months, patient again reported in the outpatientdepartment with 6x5 cm swelling in right iliac regionwhich had developed over a period of three months.Retrospective history suggested asymptomatic period of11 months followed by development of a small swellingin right iliac region (Figures 1 and 2). Level of alkalinephosphatase had increased further (840 IU/L) during 1year. The digital pulmonary skiagram showed multipleround radiopaque shadows in the upper lobes of boththe lungs suggestive of metastasis. Fine needle aspirationcytology (FNAC) was done from right iliac swelling.On FNAC highly cellular smears consisting of ovalosteoblastic cells with eccentric nuclei and denseeosinophilic cytoplasm were obtained. Some of thesecells had characteristics ‘hof’—a feature of activatedosteoblasts. Multinucleated giant cells were abundant inthe smears with occasional mitotic figures (Figure 3).Atypical mitosis and nuclear pleomorphism wasevident. Cytomorphologic features, size more than 4 cmand frequent recurrence of previous lesions favored thediagnosis of aggressive osteoblastoma, which was laterconfirmed by histopathological examination.
DISCUSSIONOsteoblastoma is a benign lesion, which isdifferentiated from osteoid osteoma by the large size ofthe nidus (> 1.5 cm), the absence of surroundingreactive new bone formation and lack of intense pain[3]. Microscopically, osteoblastoma is well demarcatedfrom the surrounding bone and is composed ofhaphazardly deposited trabeculae of woven bonerimmed by osteoblasts and scattered osteoclasts withinrichly vascular stroma. Cytomorphologically, theosteoblasts in conventional tumors are ovoid or roundwith eccentric nuclei and moderate amount ofeosinophilic cytoplasm. Mitoses are uncommon andnecrosis is usally absent [4]. Aggressive osteoblastomais very rare tumor that is considered as borderlinebetween benign osteoblastomas and osteosarcomas [5].They have a higher growth potential than conventionalosteoblastomas and are typically more than 4 cm in sizewith high risk of recurrence [5]. They are distinguishedmicroscopically from the ordinary osteoblasts because
of the presence of wider or more irregular trabecula,which is bordered by epithelioid appearing osteoblasts,by the focal lack of a trabecular pattern of the osteoidproliferation [1]. Aspirates from aggressive osteoblastomaare highly cellular and the osteoblasts are two to threetimes larger than the conventional osteoblasts and haveabundant eosinophilic cytoplasm with vesicular nucleiand prominent nuclei (epithelioid osteoblasts) [4]. Thepresence of epithelioid osteoblasts is the maindifferentiating point between conventional osteoblastomaand aggressive osteoblastoma [5] (Table 1).
Figure 1: Clinical photograph: Swelling of right ilium.
Figure 2: XRay showing lytic lesion of right iliac bone.

IJCRI – International Journal of Case Reports and Images, Vol. 3 No. 8, August 201 2. ISSN – [0976-31 98]
IJCRI 201 2;3(8):34–38.www.ijcasereportsandimages.com Khan et al. 36
Table 1: Differentiation between osteoblastoma and aggressive osteoblastoma.
The complex presentation of this case presented twodiagnostic dilemmas. One was whether to consider thistumor as aggressive osteoblastoma or as low grade/welldifferentiated osteosarcoma. Morphologic features,involvement of short and flat bones, long duration ofillness and diagnosis of osteoblastoma in hemate bonewere in favor of diagnosis of aggressive osteoblastoma.Aggressive osteoblastoma is differentiated from
conventional osteosarcoma due to low mitotic rate andthe absence of the following features: lacelike osteoid,permeation of surrounding intertrabecular spaces andatypical mitoses [6]. Aspirates from osteosarcoma arehighly cellular. Osteosarcoma cells are spindled, oval,rounded, or pleomorphic, and show high degree ofcellular atypia. Intracellular and/or extracellular osteiodmay be present [5] (Table 2).
Second problem was to establish whether the tumordeveloped de novo, or was it a metastasis ofosteoblastoma, or weather it developed due toimplantation during surgery. The implantation theorywas given weightage due to the development of tumor inthe iliac bone following sampling for bone chips.The histopathological study of biopsy from right iliacregion showed abundant osteoid with numerous emptyas well as nucleated osteocytic lacunae separated by lacyosteoid matrix. The osteoid had numerous blotchy areasof calcification and a few entrapped dysplasticosteoblastic as well as spindle shaped cells (Figure 4).A small island of proliferating osteoblasts, showing well
Figure 3: FNAC: Osteoblasts with characteristic ‘hof’ andmultinucleate osteoclastic giant cell (H&E, x500).Figure 4: Section showing abundant osteoid with proliferationof immature plump osteoblasts and areas of calcification.(H&E, x250).
Table 2: Difference between aggressive osteoblastoma and lowgrade / well differentiated osteosarcoma.

IJCRI – International Journal of Case Reports and Images, Vol. 3 No. 8, August 201 2. ISSN – [0976-31 98]
IJCRI 201 2;3(8):34–38.www.ijcasereportsandimages.com Khan et al. 37
defined darkly stained nucleus and abundant deeplyeosinophilic cytoplasm was seen at the periphery.Another small area showed proliferating spindle shapedfibroblastic type cells with aggressive appearing nuclei.Occasional multinucleated osteoclastic giant cells as wellas a few small bi and tri nucleated giant cells were alsoappreciated. These findings favored the diagnosis ofaggressive osteoblastoma.Mark et al. [7] have reported two cases of aggressiveosteoblastoma exhibiting diverse biological behavior.One was in iliac bone of 15 years old male patient. Thepatient died despite curettage, extensive chemotherapy,and radiotherapy. On autopsy distant metastases weredetected. The other case was in femur of 12 years oldfemale patient. Amputation was recommendedfollowing recurrence, but the patient declined andradiation therapy was given. Patient survived up to next14 years on radiotherapy [7]. Two unusual cases havebeen reported in maxillary bone. Both the cases wereinitially diagnosed as osteoblastoma, but later it wassuggested as a malignant transformation ofosteoblastoma into osteosarcoma [8]. One case has beenreported in calcaneum of a 29yearold female, whichwas initially diagnosed as benign osteoblastoma butafter recurrence, revised diagnosis of aggressiveosteoblastoma was established on histology [9].Osteoblastoma with conversion to osteosarcoma shouldbe considered as a separate tumor entity distinguishedfrom genuine osteosarcoma [10]. However, it is verydifficult to differentiate between aggressiveosteoblastoma and low grade/well differentiatedosteosarcoma [11] both radiologically and histologically.The presence of epithelioid osteoblasts, trabecularosteoid, prominent osteoclastic activity, absence ofcartilage, well demarcated woven bonehost boneinterface and low mitotic activity are some of thehistological criteria to differentiate it fromosteosarcoma.
CONCLUSIONThese cases highlight the biological diversity ofosteoblastoma like lesions and illustrate the difficultieswhich may be encountered in attempting to differentiatebetween benign and malignant forms of osteoblastomaand between aggressive osteoblastoma andosteosarcoma.
*********Author ContributionsLubna Khan – Substantial contributions to conceptionand design, Acquisition of data, Analysis andinterpretation of data, Drafting the article and revising itcritically for important intellectual content, Finalapproval of the version to be publishedMK Gupta – Substantial contributions to acquisition ofdata,analysis and interpretation of data, Drafting thearticle, Final approval of the version to be published
PK Singh – Substantial contributions to conception anddesign, Analysis and interpretation of data, Revising itcritically for important intellectual content, Finalapproval of the version to be publishedAsha Agarwal – Substantial contributions to conceptionand design, Analysis and interpretation of data;Revising the article critically for important intellectualcontent, Final approval of the version to be publishedGuarantorThe corresponding author is the guarantor ofsubmission.Conflict of InterestAuthors declare no conflict of interest.Copyright© Lubna Khan et al. 2012; This article is distributedunder the terms of Creative Commons attribution 3.0License which permits unrestricted use, distributionand reproduction in any means provided the originalauthors and original publisher are properly credited.(Please see www.ijcasereportsandimages.com/copyrightpolicy.php for more information.)
REFERENCES1. W Dorfman HD, Weiss SW. Borderline osteoblastictumors: problems in the differential diagnosis ofaggressive osteoblastoma and low gradeosteosarcoma. Semin Diagn Pathol 1984;1:21534.2. Bertoni F, Unni KK, McLeod RA, Dahlin DC.Osteosarcoma resembling osteoblastoma. Cancer1981;11:41626.3. Dahlin DC, Johnson EW. Giant osteoid osteoma. JBone Joint Surg 1954;36A:55972.4. Nielsen GP, Layfield LJ, Rosenberg AE. Noeplasticand tumor like lesions of bone. In: Silverberg SGDeLellis RA, Frable W J LiVolsi VA, Wick MR, Ed.Silverberg’s principles and practices of surgicalpathology and cytopathology. 4th ed. China:Churchill Livingstone, Elsevier; 2006. 725.5. Koss Leopold G. Koss’ Diagnostic cytology & itshistopathologic bases. 5th ed. Philadelphia:Lippincott Williams & Wilkins, 2006:134348.6. Schajowicz F, Lemos C. Malignant osteoblastoma. JBone Joint Surg (Br) 1976: 58; 202211.7. Mark L. Mitchell, Lauren V. Ackerman. Metastaticand pseudomalignant osteoblastoma: a report of twounusual cases. Skeletal Radiology 1986 March;15(3).8. Hiroshi Ueno, Eiichiro Ariji, Takemasa Tanaka.Imaging features of maxillary osteoblastoma and itsmalignant transformation. Skeletal RadiologySpringer Berlin / Heidelberg (Online) 1994 Oct ;23(7) :14322161.9. Miyayama H, Sakamoto K, Ide M, et al. Aggressiveosteoblastoma of the calcaneus. Cancer 1993;71:346353.10. Kunze E, Enderle A, Radig K, SchneiderStock R.Aggressive osteoblastoma with focal malignanttransformation and development of pulmonary

IJCRI – International Journal of Case Reports and Images, Vol. 3 No. 8, August 201 2. ISSN – [0976-31 98]
IJCRI 201 2;3(8):34–38.www.ijcasereportsandimages.com Khan et al. 38
metastases. A case report with a review ofliteratureGen Diagn Pathol. 1996 May; 141(56):37792.11. Mirra JM. Bone In: “Surgical Pathology” Ed. WFCoulson JB. Philadelphia: Lippincott Co 1988:1356471.