Clinical Oncology Assignment
Directions: Divide the following anatomical areas amongst your
group members and complete the following assignment. For groups
with 4 members you may choose 2 primary tumors in the same area
(head and neck, chest, or pelvis) but they should not be the same
tumor site.
•Primary Head and Neck with lymph nodes
•Primary Lung/Mediastinum or Breast/chest wall with lymph
nodes
•Primary Pelvis (any tumor found below L4-L5) with lymph
nodes
Find a case in your clinic that you have worked on, or are
working on, to research and answer the corresponding questions
(Note: this can be a case that your clinical instructor is planning
or planned but you observed/participated). Please include any
references and helpful screenshots to describe your rationale and
to explain the treatment plan design and process.
Questions:
1. How was this patient positioned for simulation? What
positioning devices/accessories were used, how and why? (5
points)
The patient was simulated head first, supine, with a wing board
and a 4-inch pillow under their knees. The legs were straight with
an O-ring on the feet to keep them stabilized. The arms were up,
and a half body vacuum lock bag was utilized for reproducible
setup. The arms were up so the preaortic region was not blocked
during treatment.
2. Discuss the target dose as defined by your physician and the
rationale behind the total dose and fractionation regimen. Include
any references or current research to help answer the question. (5
points)
The target dose was for this patient was 45 Gy to be delivered
in 1.8 Gy fractions and a total of 25 fractions. This was a stage
IIIC1 endometrioid adenocarcinoma of the uterus. The uterus was
removed along with nodes of the external and internal iliac
although the resident thinks they may have removed a common iliac
node. There was no involvement of the surrounding organs (cervix,
ovaries, or fallopian tubes). The left and right internal and
external iliac was positive for disease and were removed. The
resident did not believe there was any gross disease left and was
comfortable not delivering a dose to 50 Gy, administering any type
of boost and there was no need for Brachytherapy. The patient will
begin chemo in coordination with the radiation treatment. At the
physician’s discretion, radiation treatment for the entire pelvis
and preaortic field can be 45 Gy in 25 fractions or 50.4 Gy in 30
fractions per ROTG 12031.
3. What specific avoidance structures were contoured? Include a
screen shot of your contoured target and organs at risk. Create and
embed a table of OAR tolerance doses based on your physician
prescription and include any associated QUANTEC values. List the
contraindications if tolerance doses were to be exceeded. (20
points)
The high priority organs at risk as defined by the treatment
plan which is aligned with ROTG 12031 is as follows. The
constraints from the physician are below, all plans at my clinic
are checked by Mobius with their defined objectives.
OAR
QUANTEC Value2,3
Physician
Contraindications
Rectum
V75<15%
V30 Gy < 60%
Grade 3+. Bleeding, diarrhea.
Bladder
V65<50%
V45 Gy < 40%
Grade 3+. Cystitis
Femur L/R
Femoral Heads: V50 , 5% (RTOG)
V30 < 15%
Fracture
Bone Marrow
TD 5/5 30 Gy (2/3)
V10 < 90%, V20 < 75%
Temporary decrease in number of stem cells.
Spinal Cord
Max Dose 50 Gy
V50 Gy < .01cc
Myelopathy
Cauda Equina
Max Dose 60 GY (Emani)
V50 Gy < .01cc
Neurotoxicity
Kidney L/R
Mean < 15-18 Gy, V12 < 55%
Dmean < 15 Gy, V12 Gy < 50%, If mean to one kidney > 18
Gy dose to remaining V6 Gy < 30%.
Clinical dysfunction. Nephritis
Small Bowel
V45<195cc
Bowel Bag V52 < 1cc*
*Constraint over target*
V40 < 30%
Grade 3 +. Perforation/fistula.
Below is a 3-view screen shot of all contoured structure for
this plan.
The full list of structures contoured for this treatment plan
include:
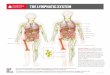
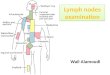
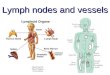
4. Identify any involved lymph nodes in your treatment region.
Embed a screen shot of the nodal regions with corresponding labels.
(15 points)
The lymph nodes in the pelvic region are highlighted well by the
following screen shot.
From the planning system, here is a coronal view showing the
pelvic vessel contour that has a margin of .7 cm.
5. Use your IMAIOS
Subscription: http://www.imaios.com/en (Links to an
external site.)Links to an external site. and other anatomy
references to describe the anatomical “boundaries” (physical
limits) of the area treated. (examples: hard palate, nasal
choanae). Embed a diagram and/or screen shot of your CT data to
point out the boundaries. (20 points)
Standard pelvic regions include:1
Superior Border: A transverse line between L4 and L5
Inferior Border: Transverse line below the lowest extent of the
obturator foramen
Lateral Border: 2 cm lateral to widest true bony pelvic
diameter.
With this case involving lymph nodes, the superior border
extends to the top of L3 to include the bottom region of the
preaortic nodes and includes the S3 vertebrae posteriorly. The
inferior border of the obturator foramen remains the same and the
field was to include at least 3 cm of the vagina.
6. Describe, in detail, the radiation treatment technique used
to treat this anatomical region. (20 points)
Examples: Technique type (VMAT, IMRT, Conformal), VMAT-Number of
arcs, their direction, collimator rotations, number of degrees.
Beam angles, couch rotations, field design, wedges, use of split
fields, etc. Include all specific setup information to describe
your process. Include any screen shots to help describe your
plan design.
The treatment was delivered using a Siemens Helical Tomography
(HT) machine delivering 1.8 Gy in 25 fractions with MU’s equaling
6,523. The number of gantry rotations were 23.6 for a duration of
474.5 seconds. The couch speed was .05374 cm/second and traveled
25.5 centimeters. The final prescription was 96% of the PTV
receives at least 45 Gy.
Typically, 5 cm jaws are used to reduce treatment time, but it
proved too difficult to meet the constraints, so it was switched to
2.5 cm jaws. Priorities (importance) were adjusted for the organs
at risk to meet the constraints issued by the physician. The bowel
bag, rectum, bone marrow and bladder were all given high priorities
compared to the other structures. The bladder and bowel bag proved
to be the most difficult constraints, the PTV that was targeted
encompassed 23% of the bladder but the constraint was eventually
met. You can see the priority of 50 versus 10 to the other
structures (PTV is a 500)
The use of an inner and outer ring structures was utilized to
“drive” dosages to regions of tight boundaries and to create
uniformity of dose to the PTV. The rings also prevent leakage dose
to surrounding tissue. The inner ring was created for 30 Gy and
over while the outer ring was for 30 Gy and under.
7. Include a final DVH of your treatment plan with appropriate
labels and discuss your ability to meet the target and OAR
tolerance guidelines. (15 Points)
As mentioned earlier, the final prescription was 96% of the PTV
receives at least 45 Gy. All of the constraints were met except for
the bowel bag which received a dose of 40 Gy of slightly more than
the 30% constraint but only went over by a few percent. The large
area the PTV covered and the large size of the bowel bag made it
extremely difficult to overcome the constraint. The physician knew
this would be an issue and created the constraint of a max dose to
the bowel bag of 53 Gy that took priority over coverage to the
target. The max dose for the bowel bag in this plan was 47.83 Gy.
The organs at risk results are below.
OAR
Physician Constraints
DVH Results
Rectum
V30 Gy < 60%
30 Gy to 34%
Bladder
V45 Gy < 40%
40 Gy to 32.5%
Femur L/R
V30 < 15%
30 Gy < 5%
Bone Marrow
V10 < 90%, V20 < 75%
10 Gy to 85%
20 Gy to 75%
Spinal Cord
V50 Gy < .01cc
Max Dose 34 Gy
Cauda Equina
V50 Gy < .01cc
Max Dose 42.5%
Kidney L/R
Dmean < 15 Gy, V12 Gy < 50%, If mean to one kidney > 18
Gy dose to remaining V6 Gy < 30%.
12 Gy to 17%
Small Bowel
Bowel Bag V52 < 1cc*
*Constraint over target*
V40 < 30%
Max Dose 47.83 Gy
40 Gy to 32.7%
References:
1. Klopp A, Yeung A, et al. RTOG 1203: A RANDOMIZED PHASE III
STUDY OF STANDARD VS. IMRT PELVIC RADIATION FOR POST-OPERATIVE
TREATMENT OF ENDOMETRIAL AND CERVICAL CANCER (TIME-C). Published
3/16/15. Accessed 03-1-19.
2.Radiation Oncology/Toxicity/QUANTEC. Wikibooks.
https://en.wikibooks.org/wiki/Radiation_Oncology/Toxicity/QUANTEC.
Accessed March 2nd 2019.