Embed Size (px)
Citation preview

ACS differentiation: With or without ST- elevation
STEMI NSTEMI UAP

Myocardial Nekrosis
• Starts 30-45min after occlusion• 90min: 40-50% nekrotized• 6 hrs: nekrosis often complete
• However collaterals can modify time-course• Occlusion can be subtotal/fluctuating• Protective agents ?
AHA Textbook of Advanced Cardiac Life Support, 1999Courtesy Dr. Lars Aaberge, Oslo
Primary PCIPrimary PCI
••preferred treatment if performed by preferred treatment if performed by experienced team <90min after first experienced team <90min after first medical contactmedical contact
••indicated for patients in shock and those indicated for patients in shock and those with contraindications to fibrinolytic with contraindications to fibrinolytic therapytherapy

• Treatment before PPCI– ASA 300 mg– Clopidogrel 300-600 mg– Unfractioned heparin 5000 - (70 IE/kg) < 70 år
• Treatment during PPCI– Heparin 100 IE/kg bolus or Enoxaparin 30 mg iv + 1 mg/kg sc– Ev. Abciximab bolus, reduce Hep 70 IE/kg
• Treatment after PPCI– Evt Abciximab infusion 12 hrs– ASA + Clopidogrel 75 mg x 1
P(rimary)PCI
Courtesy Dr. Lars Aaberge, Oslo

Reperfusion therapyReperfusion therapy
Reperfusion therapy is indicated in all Reperfusion therapy is indicated in all patients with history of chest patients with history of chest pain/discomfort of <12h and associated pain/discomfort of <12h and associated with ST-segment elevation or (presumed) with ST-segment elevation or (presumed) new bundle-branch block on the ECGnew bundle-branch block on the ECG

ThrombolysisThrombolysis
Within the first 3 hours after onset of Within the first 3 hours after onset of chest pain fibrinolysis is a viabale chest pain fibrinolysis is a viabale alternative.alternative.
Within the first 3 hours of chest pain Within the first 3 hours of chest pain primary PCI and fibrinolysis are equally primary PCI and fibrinolysis are equally effective in reducing infarct size and effective in reducing infarct size and mortality.mortality.

Kontraindikationer mot trombolys
· Tidigare intracerebral blödning · Inom 2 månader efter övriga stroke eller cerebrovaskulära händelser · Känt intrakraniellt neoplasm · Pågående invärtes blödning (inkluderar icke menstruation)

– ASA 300 mg– Clopidogrel 300-600 mg– One-dose rTPA (tenecteplase) + Enoxaparin 30
mg iv + 1 mg/kg sc
– Morphin - Oxgen – Nitrates - Betablokker
Pre-hospital Thrombolysis
Resuce PCIResuce PCI
after failed thrombolysis in patients with after failed thrombolysis in patients with large infarcts large infarcts

ReperfusionReperfusion
50 % av ST höjningen går i regress 90 min 50 % av ST höjningen går i regress 90 min efter start av trombolys.efter start av trombolys.
Om ej reperfusion efter trombolys, Om ej reperfusion efter trombolys, ställningstagande till rescue PTCAställningstagande till rescue PTCA




STEMISTEMI
NSTEMINSTEMI

KITKIT
KoagulationKoagulationIschemiIschemiTrombocyterTrombocyter
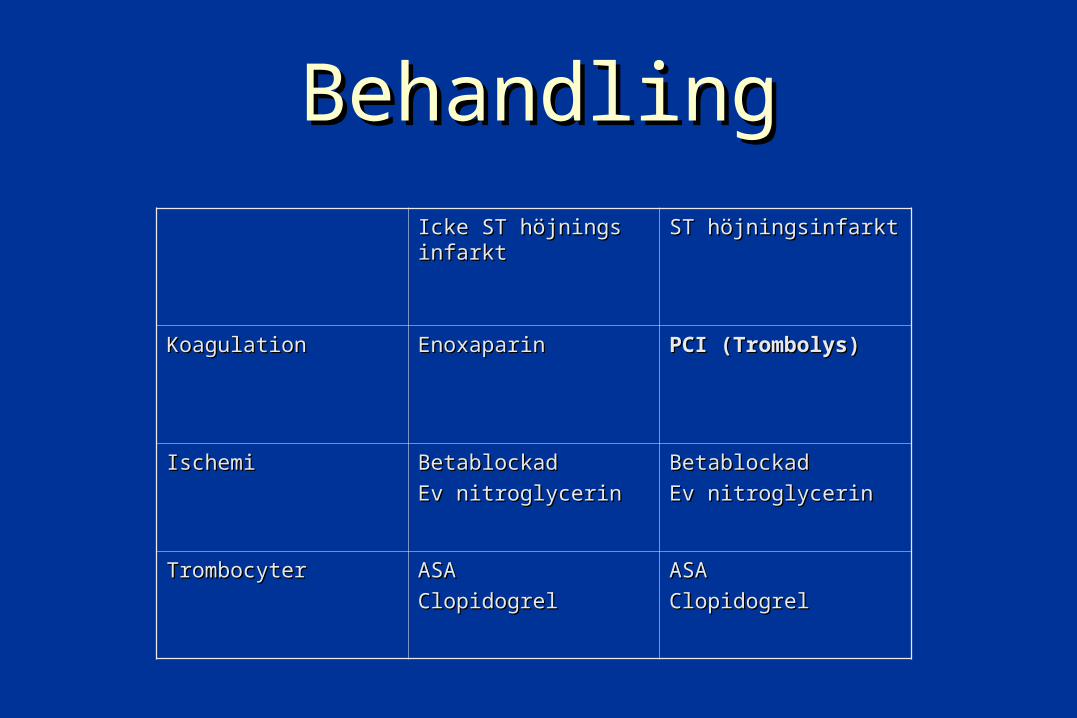
BehandlingBehandling
Icke ST höjnings Icke ST höjnings infarktinfarkt
ST höjningsinfarktST höjningsinfarkt
KoagulationKoagulation EnoxaparinEnoxaparin PCI (Trombolys)PCI (Trombolys)
IschemiIschemi BetablockadBetablockad
Ev nitroglycerinEv nitroglycerinBetablockadBetablockad
Ev nitroglycerinEv nitroglycerin
TrombocyterTrombocyter ASAASA
ClopidogrelClopidogrelASAASA
ClopidogrelClopidogrel


Antithrombotic Trialists’ Collaboration: Evidence Supports Low Dose ASA (75–150mg)1
1. Antithrombotic Trialists’ Collaboration. BMJ 2002; 324: 71–86.
ASA dose % odds reduction
500–1500 mg daily
160–325 mg daily
75–150 mg daily
< 75 mg daily
Any ASA dose 23% ±2
(p < 0.0001)
1.00.50.0 1.5 2.0
Control betterASA better

1. The CURE Study Investigators. Eur Heart J 2000; 21:2033–41
CURE-trial
Double-blind treatment up to 12 months
ASA 75–325 mg od
Clopidogrel75mg od
(n = 6,259)
Placebo1 tab od
(n = 6,303)
ASA 75–325 mg od
Day
1
6 m
onth
vis
it9
mon
th v
isit
12 m
onth
or fi
nal v
isit
Clopid
ogrel
300m
g load
ing
dose
3 m
onth
vis
it
Dis
char
ge v
isit
1 m
onth
vis
it
Patients withACS
(unstable angina or non-Q-wave
MI)
Plac
ebo
load
ing
dose
R = randomisation
n = 12,562
28 countries
R
NON-STEMI

CURE: early and long-term benefits of clopidogrel1
1. The CURE Trial Investigators. N Engl J Med 2001; 345:494–502
0.00
0.02
0.04
0.06
0.08
0.10
0.12
0.14
0 3 6 9 12Months of follow-up
Cu
mu
lati
ve h
azar
d r
ate Placebo*
(n = 6,303)
Clopidogrel* (n = 6,259)
20% relativerisk reduction
p = 0.00009
Cumulative events(MI, stroke or cardiovascular death)
*On top of standard therapy (including ASA)

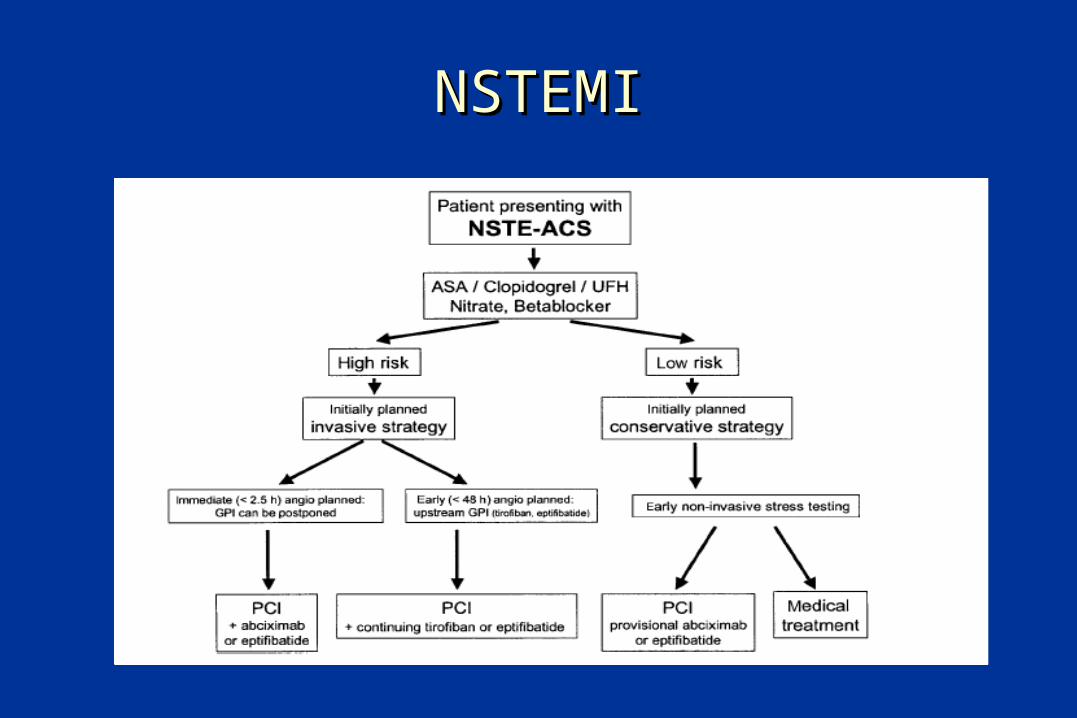
Revascularization in NSTEMI/UAP

• Risk stratification– High (GPIIb/IIIa and fast PCI)– Intermediate (neg trop, delayed invasive dx)– Low (elective invasive dx or search for ischemia)
• Basistreatment– ASA 300 mg, 75-160 mg– Clopidogrel 300 mg 75 mg for 9-12mths– LMWH (Enoxaparin/Dalteparin)
– (Betablokker, Nitrates, Statins)
UAP / NSTEMI - Treatment
Courtesy Dr. Lars Aaberge, Oslo

• Treatment prior to PCI– ASA 300 mg 75 x1– Clopidogrel 300-600 mg 75x1– Enoxaparin / Dalteparin sc
• Treatment during PCI– Heparin 100 IE/kg bolus or Enoxaparin 30 mg iv + 1
mg/kg sc (ACT 250-350)– Possible: GPIIb/IIIa (reduce Hep to 70 IE/kg, ACT<250)
• Treatment post PCI– ASA + Clopidogrel 75 mg x 1 – (GP IIb/IIIa)
UAP/NSTEMI

Cholesterol

0
50
40
30
20
10
0
0.5
LRCCARE
POSCH
WOS4S
LIPID
AFCAPS
1.0 1.5 2.0 2.5
HPS
Adapted from:
LRC, JAMA 1984;251:351-364 Downs JR et al., JAMA 1998;279:1615-1622
LIPID Study Group, N Engl J Med 1998;339:1349-57 Shepherd J et al., N Engl J Med 1995;333:1301-7
Sacks FM et al., N Engl J Med 1996;335:1001-9 Buchwald H et al., N Engl J Med 1990;323:946-955
4S Group, Lancet 1994;344:1383-89 HPS Collaborative Group, Lancet 2002;360:7-22
Reduction in cholesterol (mmol/l)
Reduct
ion in c
ard
iovasc
ula
r events
(%
)
Relationship between reduction of cholesterol and decrease of cardiovascular events in various trials
1 mmol LDL- 21% CHD-