Embed Size (px)
Citation preview

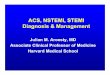
STEMI, NSTEMI and Cardiac Arrest Case presentation
Sam Dawkins, MD PhD Cedars-Sinai Heart Institute, Los Angeles, CA Controversies and Advances in the Treatment of Cardiovascular Disease Los Angeles, CA

Background
• 72 year old male
• Sudden onset shortness of breath with chest tightness
• Hypertension and hyperlipidemia
• No other significant past medical history

Background
• 72 year old male
• Sudden onset shortness of breath with chest tightness
• Hypertension and hyperlipidemia
• No other significant past medical history
• Ambulance transfer direct to cath lab
• On arrival
SaO2 88% on 15L
HR 105 sinus rhythm BP 110/55



Background
• 72 year old male
• Sudden onset shortness of breath with chest tightness
• Hypertension and hyperlipidemia
• No other significant past medical history
• Ambulance transfer direct to cath lab
• On arrival
SaO2 88% on 15L
HR 105 sinus rhythm BP 110/55

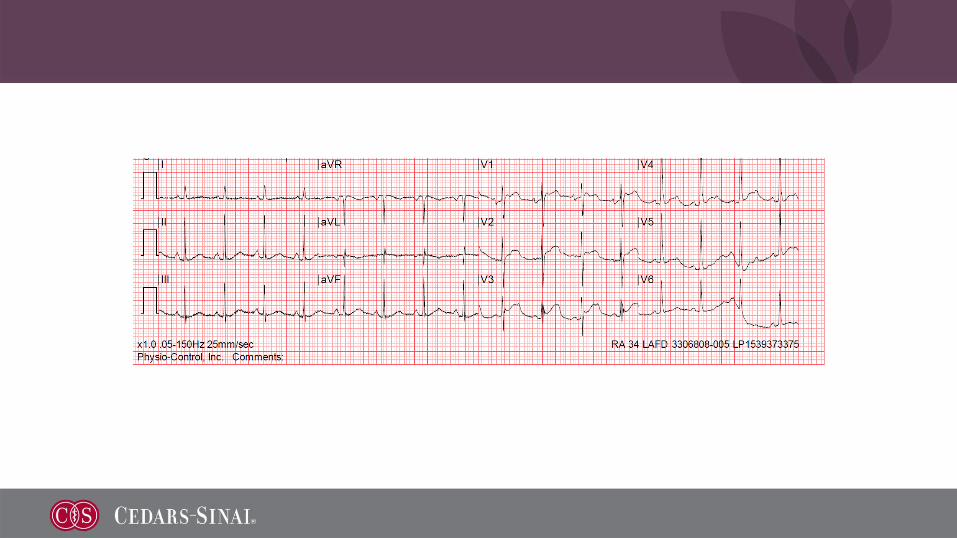
What is the strategy?
• PCI? Which vessel? Multivessel?
• Support – Impella, balloon pump?
• Anesthesia?
10
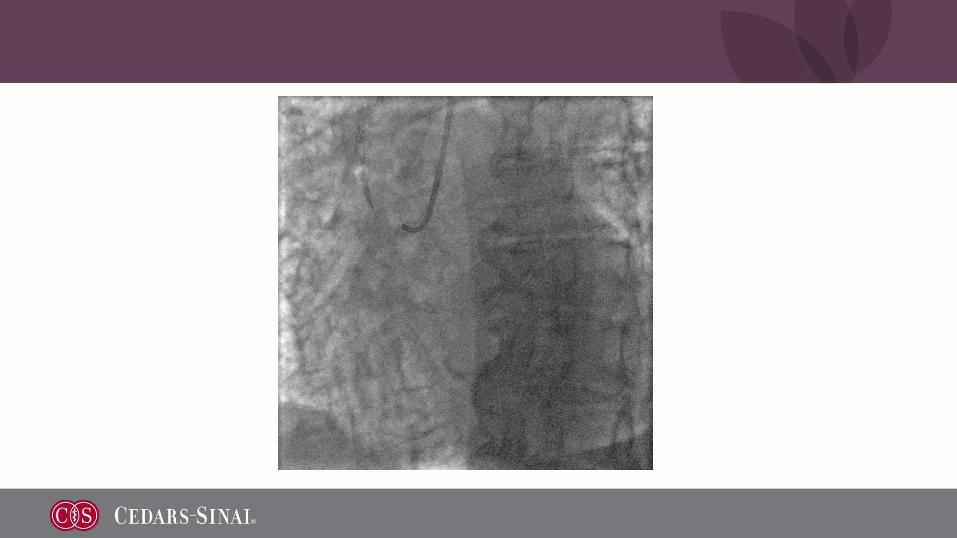
Procedure
• General anesthesia
• Intra-aortic balloon pump sited
• Balloon dilatation and PCI to mid circumflex with 3.0 x 12 drug eluting stent
• Guide wire to circumflex for guide stability
• Unable to cross proximal LAD lesion

11
Procedure
• General anesthesia
• Intra-aortic balloon pump sited
• Balloon dilatation and PCI to mid circumflex with 3.0 x 12 drug eluting stent
• Unable to cross proximal LAD lesion
• Eventually wired LAD with Fielder XT and Corsair backup

12
Procedure
• General anesthesia
• Intra-aortic balloon pump sited
• Balloon dilatation and PCI to mid circumflex with 3.0 x 12 drug eluting stent
• Unable to cross proximal LAD lesion
• Eventually wired LAD with Fielder XT and Corsair backup
• Intravascular ultrasound to confirm true lumen

13
Procedure
• General anesthesia
• Intra-aortic balloon pump sited
• Balloon dilatation and PCI to mid circumflex with 3.0 x 12 drug eluting stent
• Unable to cross proximal LAD lesion
• Eventually wired LAD with Fielder XT and Corsair backup
• Intravascular ultrasound to confirm true lumen
• Balloon dilatation of proximal LAD

14
Procedure
• General anesthesia
• Intra-aortic balloon pump sited
• Balloon dilatation and PCI to mid circumflex with 3.0 x 12 drug eluting stent
• Unable to cross proximal LAD lesion
• Eventually wired LAD with Fielder XT and Corsair backup
• Intravascular ultrasound to confirm true lumen
• Balloon dilatation of proximal LAD

15
Procedure
• General anesthesia
• Intra-aortic balloon pump sited
• Balloon dilatation and PCI to mid circumflex with 3.0 x 12 drug eluting stent
• Unable to cross proximal LAD lesion
• Eventually wired LAD with Fielder XT and Corsair backup
• Intravascular ultrasound to confirm true lumen
• Balloon dilatation of proximal LAD
• Drug eluting stent to proximal LAD

16
Procedure
• General anesthesia
• Intra-aortic balloon pump sited
• Balloon dilatation and PCI to mid circumflex with 3.0 x 12 drug eluting stent
• Unable to cross proximal LAD lesion
• Eventually wired LAD with Fielder XT and Corsair backup
• Intravascular ultrasound to confirm true lumen
• Balloon dilatation of proximal LAD
• Drug eluting stent to proximal LAD

17
What next?
• Stop and transfer to ICU?
• PCI to the right coronary artery?

18
Procedure
• Wire to distal vessel
• Balloon dilatation

19
Procedure
• Wire to distal vessel
• Balloon dilatation
• 3.0 x 28 drug eluting stent

20
Procedure
• Wire to distal vessel
• Balloon dilatation
• 3.0 x 28 drug eluting stent

21
Clinical Course
• Transferred to ICU
• TTE
Severe left ventricular impairment (EF 20%)
Anterior akinesis, hypokinesis elsewhere
No significant valvular pathology
• Balloon pump removed after 24 hours
• Failed attempt to extubate after 48 hours
• Falling blood pressure with pulmonary edema, requiring pressor support

22
Clinical Course
• Transferred to ICU
• TTE
Severe left ventricular impairment (EF 20%)
Anterior akinesis, hypokinesis elsewhere
No significant valvular pathology
• Balloon pump removed after 24 hours
• Failed attempt to extubate after 48 hours
• Falling blood pressure with pulmonary edema, requiring pressor support
• Extubated day 9
• Discharged day 29

23
Key points for discussion
• Use of circulatory support in STEMI
• Management of respiratory compromise in the cath lab
• Non-culprit PCI in STEMI / cardiogenic shock