Embed Size (px)
Citation preview

A VIPER IN THE
COURTYARDLA ILA ABUZAID , MD
ENDOCR INOLOGY FELLOW

•NO DISCOLSURES

OBJECTIVES:
• Recognize signs and symptoms of
hyperthyroidism
• Develop a differential diagnosis for a patient
with chronic diarrhea (secretory)
• Describe anchoring heuristic/premature
closure

CASE PRESENTATION
• A 55 year old man presents to the hospital multiple times in
two months for uncontrolled watery diarrhea.
• Onset: 5 months, on-off
• Non-bloody
• Associated with nausea and vomiting
• No abdominal pain
• Patient had lost 20 pounds/6 months

MEDICAL HISTORY
• OSA on CPAP
• Grave’s disease
• TSH < 0.02 Free T4 1.37
• Radioactive iodine uptake scan: 24-hour uptake of 53%
• Diarrhea was attributed to hyperthyroidism from Grave’s
disease.
• He was started on methimazole 10 mg daily.

• Past surgical history:
• Right total hip
arthroplasty
• Medications:
• Methimazole
• Immodium
• Family History:
• Father with DM
• Social History:
• Lives with wife
• No smoking
• Occasional alcohol
• No illicit drug use

RECURRENT ADMISSIONS
• Despite optimal anti-diarrheal therapy and methimazole, he
continued to have watery diarrhea, causing acute kidney injury
and severe hypokalemia, and required several inpatient
admissions for intravenous fluid resuscitation.

FIRST ADMISSION: (JAN 3-4TH, 2016)
• Diarrhea, nausea and vomiting
• C. diff: negative
• TSH <0.02 Free T4 1.32
• Managed with IV fluids and loperamide.
• Diarrhea was thought to be due to viral gastroenteritis +
hyperthyroidism

SECOND ADMISSION: (FEB 4-7TH, 2016)
• Had been holding methimazole for a week for RIA
• Diarrhea, nausea and vomiting
• C. diff: negative
• TSH <0.02 Free T4 1.61 Potassium
2.8
• Improved quickly with IV fluids and loperamide.
Methimazole restarted.

THIRD ADMISSION (FEB 16-19TH, 2016)
• Again, watery diarrhea associated with nausea and vomiting.
• TSH <0.02 Free T4 1.44 Potassium 2.5
• On methimazole.
1. Free T4 is 1.44
2. He is ON Methimazole
3. Hyperthyroidism doesn’t usually
cause watery diarrhea but
rather hyper defecation

WORK UP FOR SECRETORY DIARRHEA
• Stool studies for
Clostridium difficile
and other infectious
organisms (including
ova and parasites):
negative.
• HIV and hepatitis
serologies: negative.
• Celiac antibody:
negative.
• Autoimmune workup:
non-revealing.

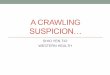
Fig 1. Coronal (left) and Axial (right) views on CT of abdomen/pelvis showed a
large mass in pancreatic body, measuring 8 x 6 cm.

• Plasma
metanephrines: not
elevated
• Gastrin level: normal
• Vasoactive intestinal
peptide level: 1065
ng/mL (normal < 75
ng/mL)
VIPoma

Fig 2. Octreotide scan showing localized lesion in the pancreas.

VIPOMAS
• Rare endocrine tumors that secrete vasoactive intestinal
peptide (VIP), causing secretory diarrhea.
• Age of onset: 30-50.
• Prevalence is 1 in 10 million per year.
• Pancreatic in origin in 95% of cases
• The secretory diarrhea is high volume (700 ml/day-3 L/day).
• Less than 5% of patients will have multiple endocrine
neoplasia syndrome type 1 (MEN 1), 3P’s
PTH 52 pg/mL
Normal Calcium
Prolactin 14.9 ng/mL

VIPOMAS
• Elevated VIP levels over 75 pg/ml raises suspicion for
VIPoma, and should be further worked up with an imaging
(either a CT or MRI) to localize as well as stage the tumor.
• Most VIPomas are greater than 3 cm. Sensitivity of a CT scan
to detect a VIPoma larger than 3 cm in size is close to 100%.
• Octreotide scan localizes tumor metastases outside the
abdominal wall. Tissue biopsy is rarely needed if hormonal
and imaging findings are unequivocal.

VIPOMAS
• Median survival for VIPoma is 96 months.
• More than half of patients have metastases at the time of
diagnosis, which makes a worse prognosis.
• Long term follow-up is done with serial VIP levels and cross-
sectional imaging studies.

MANAGEMENT
• Somatostatin analogs (e.g octreotide). Octreotide has been shown to reduce the frequency and amount of diarrhea, and improve quality of life.
• Anti-diarrheal agents and repletion of electrolytes.
• Surgical resection of the tumor is indicated if the tumor is localized to pancreas or has limited hepatic involvement.
• Advanced disease: hepatic artery chemoembolization or ablation.

CASE OUTCOME
• Patient was discharged from hospital after his diarrhea was well-controlled with octreotide, and his electrolytes were adequately replaced.
• After 1 week of therapy with octreotide, his diarrhea continues to improve, with 3-4 formed to loose stools per day.
• Staging:
• TNM classification from the American Joint Committee on Cancer (AJCC)= T2N0M0 = stage IB

CASE OUTCOME
• Underwent central pancreatectomy with removal of 12 * 12 cm encapulated tumor in the neck of the pancreas.
• Normal Portal and peripancreatic LNs.
Currently following with surgical oncology for serial
imaging/labs.

CONCLUSIONS
• Hyperthyroidism usually causes hyper defecation rather than
watery diarrhea.
• VIPomas are rare neuroendocrine tumors, require high index
of suspicion.
• Anchoring heuristic: Settling on a diagnosis early in the
diagnostic process despite data that refute the diagnosis or
support another diagnosis (premature closure).