Embed Size (px)
Citation preview

I. INTRODUCTION
The most important thing in illness is never to lose heart.
~Nikolai Lenin
There is nothing more terrifying in life than facing an illness; especially if that illness
inflicts a very young person who did not even experience life yet. That very young
person inflicted with an illness may not see the effects of her illness in her life, but her
loved ones will. What is very essential with a person afflicted with an illness is her
support system. It necessary for the support system to have a positive attitude in facing
an illness with the patient. It is believed that positive thinking can do great effects on the
part of the patient. People who are more optimistic when faced with an illness tend to
have more faith in cure. It gives enlightenment to the persons involved that the illness
will be treated.
Maintaining a positive attitude is needed more when faced with a very rare
disease. One such rare disease is having a pancreatic endocrine tumor. Pancreatic
endocrine tumors (PETs) are also called islet tumors or islet cell tumors; however,
because the cell of origin of most is unknown, the general PET is preferred. PETs
frequently are classified as functional or nonfunctional depending on whether a clinical
syndrome resulting from the autonomously released hormone is present (gastrinoma,
insulinoma, glucagonoma, VIPoma, somatostatinoma, GRFoma, ACTHoma).
Nonfunctional PETs frequently release hormones and peptides (pancreatic polypeptide,
neurotensin, α- and β-subunits of human chorionic gonadotropin, neuron-specific
enolase, chromogranin A and breakdown products) that cause no distinct clinical
syndromes (Goldman and Ausiello, 2008, p. 1482).
Islet cell tumors are either sporadic and can occur in association with other
known genetic syndromes, such as multiple endocrine neoplasia type1. Sporadic tumors
1

occur at any age but most commonly are detected between 40 to 69 years of age. The
diagnosis can be confirmed by obtaining tissue during surgical resection or by needle
biopsy (Goldman and Ausiello, 2008, p. 1765).
A more specific type of pancreatic endocrine tumor is VIPoma. VIPoma (also known as
pancreatic cholera) is characterized by profuse watery diarrhea, marked fecal loss of
potassium and bicarbonate, hypokalemia, and low or absent gastric acid secretion
(Greenspan and Baxter, 1994, p. 565). Inappropriate secretion of vasoactive intestinal
polypeptide (VIP) by vipomas causes the watery diarrhea, hypokalemia, and
achlorhydria (WDHA) syndrome, also called Verner-Morrison syndrome. Although VIP is
the most likely mediator of the WDHA syndrome, other hormone-like substances such as
the peptide histidine methionine may also be involved (Flethcer, 2007, p. 1129). Death
may result from renal failure or cardiac arrest caused by volume depletion and acidosis
(Ferry, 2008).
In the adult, the vast majority of vipomas are of pancreatic origin. Exceptions are
some rare VIP-producing pheochromocytomas and intestinal endocrine tumors
(Flethcer, 2007, p. 1129). Pancreatic vipomas are usually solitary large tumors (mean
size 4-5 cm). These tumors are usually not multiple, 50-75% are in the pancreatic tail,
and 37 to 68% have hepatic metastasis at diagnosis (Kasper, et. al., 2005). In children
<10 years, WDHA syndromes have been reported in association with VIP-secreting
ganglioneuromas and ganglioneuorblastomas, which are less malignant and account for
10% of VIPomas in adults (Kasper, et. al., 2005). The WDHA syndrome has also been
attributed to islet hyperplasia. These reports are difficult to interpret because, in the
normal adult human pancreas, VIP is only present in autonomic nerves but not in islet
cells (Flethcer, 2007, p. 1129).
2

VIPomas are very rare cancers. Each year very few new cases of VIPoma are
reported (0.05 to 0.2 cases per million adults). Even fewer cases in children are
reported. VIPomas are the third most common neuroendocrine tumor of the pancreas
(15%), after insulinomas (50%) and gastrinomas (30%). When VIPomas occur in adults,
they appear most commonly between the ages of 40 and 50 years (Ferry, 2008).
The diagnosis requires the demonstration of an elevated plasma VIP level and
the presence of large-volume diarrhea (Kasper, et. al., 2005).
The most important initial treatment is to correct their dehydration, hypokalemia,
and electrolye losses with fluid and electrolyte replacement. If a tumor has been
identified, complete surgical excision is the primary form of treatment. If the tumor
cannot be removed completely, surgical debulking may have palliative benefit. In one
series, surgical excision of the primary pancreatic tumor relieved all symptoms in 17
patients (27%) (Vinik, 2006). Because 37 to 68% of VIPomas have metastatic disease in
the liver at presentation, a significant number of patients cannot be cured surgically. In
these patients, long-acting somatostatin analogues such as octreotide or lanreotide are
the drugs of choice (Kasper, et. al., 2005). Other drugs reported to be helpful in small
number of patients include prednisone (60 to 100 mg/d), clonidine, indomethacin,
phenothiazines, loperamide, lidamidine, lithium, propranolo, and metoclopramide.
Treatment of advance disease with embolization, chemoembolization,and chemotherapy
may also be helpful (Kasper, et. al., 2005).
An article by David, et. al. entitled “Multi-visceral resection of pancreatic VIPoma in a
patient with sinistral portal hypertension” shows a patient who have undergone multiple
resection of the pancreas with flying colors. A 46 year old women presented with
abdominal pain and diarrhea. A three-dimensional (3-D) pancreas protocol computed
tomography scan revealed an 18 × 12 cm pancreatic VIPoma abutting the liver,
3

stomach, spleen, left adrenal, colon that also invaded the distal duodenum – proximal
jejunum at the ligament of Treitz in association with sinistral portal hypertension.
Following preoperative proximal splenic artery embolization, the patient with underwent
successful en bloc resection of the locally advanced VIPoma in conjunction with a
diaphragmatic resection, total gastrectomy, splenectomy, left adrenalectomy, as well as
small and large bowel resection. The estimated blood loss was 500 ml. All margins were
negative (R0 resection). The patient is alive and disease-free. This case illustrates the
role of aggressive resection of pancreatic neuroendocrine tumors and highlights several
key technical points that allowed for successful resection.
This type of aggressive treatment is only possible under advanced medical
equipment and highly skilled surgeons. The treatment has shown a great improvement
on the patient who have undergone the surgery. However, patients have different
reactions to surgery and it is not assured that if the surgery was successful in one
patient, it would also be successful in another patient. Special precautions should be
made in administering this type of treatment to other patients.
The study “Amelioration of Symptoms and Reduction of VIP Levels after Hepatic Artery
Chemoembolization in a Patient with Sandostatin Resistant VIPoma” by Shaib, et. al.
report a successful treatment of VIPoma with hepatic chemoembolization of a metastatic
hepatic lesion evidenced by a reduction of VIP levels and resolutions of symptoms in a
patient with pancreatic VIPoma unresponsive to increased doses of an octreotide
analog.
This is another treatment alternative to clients with VIPoma who are not
responsive to the octreotide. It is done by injecting a chemotherapeutic drug directly into
the blood vessel feeding a cancerous tumor and an embolic agent is placed inside the
blood vessel feeding the tumor trapping the chemotherapy in the tumor. This treatment
4

is effective and durable as a treatment modality for patients with metastatic VIPomas (or
other neuroendocrine tumors) who are clinically symptomatic from the effects of
hormone hypersecretion. It is applied as a palliative technique in symptomatic patients
with unresectable hepatic metastasis. This is a less invasive treatment rather than
undergoing surgery. It provides high successful rates to patients who have undergone
this procedure.
Nowadays, lifespan of humans continuously decreases as time passes by. Many
individuals are suffering diseases due to lack of consciousness on how they can avoid
acquiring such diseases. However, some diseases occur sporadically and are very rare.
One very rare disease is VIPoma.
The study was chosen because it was the first time of the nurse researcher to
encounter this illness. She was interested in the pathophysiology and management of
clients with VIPoma. Such knowledge can be use to formulate health teachings that
could be rendered to clients hence may help them in the management of such condition.
Moreover, with the increased in information, people will know how to approach this very
rare disease.
A case of VIPoma is very rare and as a nurse, it is also very rare to handle such
case. For a disease process that entails proper understanding, to handle such case is a
superb opportunity to fully understand the physiology of the disease process, and thus
knowing the cause of the client’s VIPoma. Furthermore, the knowledge about the
pathophysiology and the treatment regimen for these diseases can help her become an
effective nurse. By being equipped with such knowledge, the researcher can be assured
that she can properly execute her functions whenever in the future she encounters
another case of a client with VIPoma.
5

Lastly, curiosity is one of the main reasons why the researcher chose such case.
This study is to boost and broaden her awareness and understanding on how such kind
of condition arise and how does it affect the clients especially their physical wellness.
Through research and studies, the researcher will be able to discover more about some
scheme and method that she can apply and adapt to clients with VIPoma. More facts
and information can be learned through continuous study and reading books and
magazines related to health care. Being a health care provider is not an easy task; it is a
continuous study and discovering new trends about different approach in helping clients
to cope up with their illnesses. And as a member of the health care team, it is only
necessary to be a patient advocate and participate in the medical management of clients
with VIPoma.
6

A. OBJECTIVES
1. Nurse-centered
General Objectives:
After completion of the study, the nurse researcher shall be able to:
Establish a good working relationship to the client and her family.
Encourage participation and compliance from the client and her family.
Perform comprehensive assessment.
Explain the medical management.
Provide appropriate interventions.
Understand the concept of Vipoma.
Determine the treatment for VIPoma.
Specific Objectives:
After completion of the study, the nurse researcher shall be able to:
Explain purpose of the case study and its importance to the client/ family.
Gain the client’s/ family’s trust regarding health matters.
Monitor and recorded vital signs.
Perform initial physical assessment needed.
Perform comprehensive assessment with regards to the signs and
symptoms of the disease.
Obtain necessary information like demographic data, family history,
personal history, socio-economic, cultural information from the family.
Gather the past and present health history of the client.
Identify the present medical management of the patient and diagnostic
and laboratory procedure done to the client
7

Identify abnormal diagnostic findings that are significant to the
identification of the disease condition.
Provide information about the disease process, present signs and
symptoms, its management, and its complications.
Formulate nursing care plans to manage the existing problems of the
patient.
Encourage client/ family to participate in formulating the nursing care
plans.
Provide health teachings with the family regarding prevention of illness
and promotion of wellness and health.
Render the appropriate interventions for patients with Vipoma.
Emphasize the importance of health teachings given and compliance to
treatment regimen.
Determine and understand the etiology, risk factors, assessment findings,
manifestations, pathophysiology, and treatment regimen of Vipoma.
Identify the cause of Asthma of the client in the study.
Present the nursing care plans to the client/ family.
Explain the necessary interventions and their rationales.
Involve the client/ family during the implementation phase of the care
plans.
Evaluate the interventions made in comparison to the objectives set by
the nurse and client/ family.
Monitor the hydration status of the client continuously.
Monitor the progress of the client.
Monitor the intake and output of the client.
Prevent injury and complications of Vipoma.
8
Encouraged continuous support of the client at home.
Reassure regarding the characteristic of the course of the disease, with
emphasis on the importance of long-term care, needs to be provided to
parents and the client.
Emphasize the dietary restrictions and needs of the client.
2. Client-centered
General Objectives:
After completion of the study, the nurse researcher shall be able to:
Establish and maintain rapport with the nurse researcher throughout the
nurse-patient interactions.
Participate in the study.
Understand the interventions and management.
Comply with the treatment management.
Specific Objectives:
After completion of the study, the nurse researcher shall be able to:
Express approval and cooperation with the treatment regimen.
Understand the importance of adherence for continuous treatment
regimen of the client.
Participate in the assessment phase and provide the needed information
of the nurse researcher.
Provide the needed information to the nurse researcher.
Participate and impart views on the nursing care plans.
Participate in the implementation of the nurse researcher.
9
Understand intervention and management such as compliance to
medications, diet, exercise and lifestyle given by the nurse researcher.
Verbalize current health problems that the client does not know how to
manage.
Verbalize understanding of health teachings regarding prevention of
illness and promotion of wellness and health.
Verbalize understanding of the information regarding the disease
process, signs and symptoms, management and complications.
Comply with the prescribed management, diet, and medications.
Identify and demonstrate behaviors that could prevent complications.
Manifest increased activity tolerance and good hydration status.
Demonstrate ways on how to prevent dehydration.
Identify the medications given after discharge, the route, the time and the
amount that should be taken.
Recognize measures to promote normal activities of daily living.
II. NURSING ASSESSMENT
A. Personal History
10
1. Demographic Data
Vipsy, a 2 year-old single female, was born on January 30, 2008 via normal
spontaneous delivery in a private hospital in the City of San Fernando. She is the only
child of Daddy Vips and Mommy Vips. She is a natural born Filipino citizen. Vipsy is
currently residing in Camachiles, Dau Mabalacat, Pampanga. She is the first child of
Mommy and Daddy Vips. Mommy Vips was 16 years old when she got pregnant with
Vipsy and Daddy Vips was 20 years old then. The parents of Vipsy are not married.
They had Vipsy after having a relationship of six months and they were separated by the
parents of Mommy Vipsy.
Vipsy had persistent loose watery stools and loss of appetite which prompted her
mother to seek medical advice and her mother was advised to admit Vipsy. She was
admitted at a private hospital in Angeles City last March 24, 2010 5:20 PM with an
admitting diagnosis of To Consider Vipoma. After five days of confinement, Vipsy was
discharged in the institution last March 28, 2010 at 3 o’clock in the afternoon with the
final diagnosis of Vipoma.
2. Socio-Economic and Cultural Factors.
In the Philippines, the family is a complex network of relatives by blood and affinity.
Affinity may come through marriage or Catholic rituals like god parenting newly baptized
children or newly married couples or even living under the common law.
The Vips family is classified under the extended type of family. Vipsy lives with
Mommy Vips, the mother of Mommy Vips (Grandma Vips), Grandma Vips’ (Sister Vips)
sister and the two siblings of Mommy Vips. Before December 2009, Grandma Vips was
in Iraq and she was working in a laundry shop which makes Sister Vips as the
companion of Mommy Vips, her siblings and Vispy. Mommy Vips is separated from
Daddy Vips. Mommy Vips is 18 years old while Daddy Vips is 22 years old. According to
11

the Grandma Vips, she did not like Daddy Vips that is why they separated Mommy Vips
and Daddy Vips. Vipsy is the first born child of Mommy Vips and Daddy Vips. Grandpa
Vips is not living with them as of the moment. He works in Lakuna and he goes home at
least once a week. Mommy Vips has two siblings. Vipsy Boy is 16 years old and Vipsy
Girl is 14 years old.
The Vips Family suffices their needs with the income of Grandma Vips and Grandpa
Vips since Mommy Vips is still a high school student. Grandpa Vips is a personal driver
of the vice mayor in Lakuna. He works six days a week which gives him time to go home
on Sundays. Sometimes, he does not have time to go home during Sundays. His salary
is around Php 20,000.00. Grandma Vips works in Iraq as an employee in a laundry
shop. She has been working abroad for almost four years. Her salary is around Php
30,000.00 per month. Grandma Vips only went home last December 2009 because her
granddaughter is sick and Mommy Vips needs her mother to help her in taking care of
Vipsy.
With the income of Php 50,000.00 per month, they allot Php 4,000 for their daily
food expenditure, Php 2,000 for their electric bill, Php 600 for their water bill. Their
groceries account to Php 7,000, Php 3,000 for the transportation of Vipsy Boy and Vipsy
Girl. Vipsy Boy and Vipsy Girl are fetched by a school service. They also allot Php
7,000.00 for the allowance of Mommy Vips, Vipsy Boy and Vipsy Girl dividied into Php
3,000 for the allowance of Mommy Vips, Php 2,000.00 each for Vipsy Boy and Vipsy
Girl. Mommy Vipsy’s allowance is Php 150/ day while Vipsy Boy and Vipsy Girl’s
allowance each is Php 100/day each. Also, Php 2,000.00 is spent on the milk of Vipsy.
Their total monthly expenditure is Php 25,600.00. The rest of their budget is saved for
their tuition fees and for their extra expenditures.
12

As to their economic status, the Vips’ family is considered not poor because their
monthly budget is Php 50,000.00 and when divided into 4 is Php `12,500. And according
to the basis given by NEDA wherein there are two categories of economic status: poor
and not poor. Families who have Php 2,768.60/month/ individual and higher fall under
Not Poor category, and those below the standard amount falls under Poor citizens.
Therefore, the Vips’ family financial assets are adequate as compared to their
expenditures. As shown on the breakdown of their expenses, they allotted budget for
health emergencies. However, their previous monthly budget has been lessened
because Grandma Vips went home from her work from Iraq. Consequently, Grandma
Vips stated that her stay here in the Philippines is only temporary and she will come
back to Iraq this year.
Vipsy does not go to school yet. Sister Vips and Mommy Vips teach her how to
talk, count and sing. She can sing her ABCs and can count up to 10. Vipsy is talkative
according to Mommy Vips; however, she still cannot complete a sentence.
The Vips Family is affiliated with the Roman Catholic. They see to it that they
attend mass every Sundays. Vipsy is baptized as a Catholic when she was 3 months
old. The Vips family prays the rosary at least once a month usually every first Fridays of
the month.
As Filipinos, we are very much concerned when it comes to superstitious or
cultural beliefs. They believe in superstitions. They believe that one should not clean the
house at night because it brings bad luck. When Vipsy was only months old, Sister Vips
puts a touch of lipstick on the forehead of Vipsy to prevent “asug”. They also believe in
herbolarios. They sought a herbolario when Vipsy’s diarrhea was consistent for almost 2
13

weeks. “Tawas” was made by the herbolario and interpreted that Vipsy’s stomach is full
of gas. They sought a herbolario because Vipsy’s diarrhea did not stop. However, their
first consultation whenever an illness is present is with their private physician. They only
consult a herbolario if the signs and symptoms of illness are consistent. They also
believe in “nuno” and “tawas” and in offering sacrifices, such as eggs and chicken, to the
“punso”. The family also believes in “ambon” and “pasma”. Whenever Vipsy goes out at
night, Mommy Vips see to it that she wears a cap or Vipsy’s head is covered to prevent
“ambon”. Mommy Vips believe that “ambon” can cause cough and cold. Grandma Vips
does not allow her family members to take a bath if they are tired and after ironing the
clothes. They also self-medicate when one of their members gets sick. They use
Biogesic, Carbocisteine, Solmux and Nafarin for fever, cough and colds. They also do
tepid-sponge bath for members with fever.
Vipsy usually wakes up at around 6 AM. She would have her breakfast then she
would start watching Barney or Dora on the television. She eats Cerelac in the morning
and she still bottle feeds every 3 to 4 hours. She usually consumes 2 to 3 oz of milk
every time she bottle feeds. At 12 noon, she would have her lunch. She eats half cup of
rice with different viands every day. Her favorite viand is fried chicken. Sister Vips
usually cooks Tinola, Sinigang, Caldereta, and Fish. Vipsy is not very particular when it
comes to her food. She usually eats what is served. However, she could not consume
her full meal. She usually consumes ¾ of her meal and she would just be given her milk.
After eating, she would play or watch television. At 2 PM, Sister Vips bathes Vipsy then
puts her to sleep thereafter. She would sleep for three to four hours. When she wakes
up, Mommy Vips would play with her daughter while Sister Vips is cooking dinner. At
6:30 PM, they would have their dinner. After dinner, Mommy Vips would give Vipsy
bananas or apples as her dessert. Vipsy’s sleeping time is usually 9 PM to 10 PM. She
14

would usually watch television with her mother or her mother would teach her the ABCs.
Before Vispy’s sleeping time, she would be given milk and water after her feeding and
would go to sleep.
The environmental condition plays a significant role in the development and health of the
family members. The Vips Family lives in Camachiles Dau, Mabalacat, Pampanga. Their
house is located in an urban area in Pampanga.
They own their home and as described by Mommy Vips, their house is concrete,
made up of cement, from wall to wall, roof is made from galvanized iron sheet and
ceiling is fixed with plywood. Their house measures approximately 300 m2. They have a
two-storey house. Their house has three bedrooms, one master bedroom for Grandma
and Grandpa Vips, one for Mommy Vips, Vipsy Girl and Vipsy and the other room is
Vipsy Boy. Their home has a sala, dining room, and kitchen with two windows each
room and two bathrooms. Mommy Vips mentioned that they have good ventilation since
their home is surrounded by plants.
According to Mommy Vips, they have a closed drainage system. The source of
their water is through the jetmatic. Their source of electricity is from a private
corporation. They buy their drinking water from water refilling stations. They have
different appliances like television, refrigerator, electric fans for each room, DVD player,
and a gas range.
In their living room, a set of sofa, and television, an electric fan, and different
room designs like picture frames and figurines would be found. Every room has 2
windows measuring approximately 2x2 meters, where the light and air pass at day time.
It is covered with a curtain but they usually tie it at daytime. There are no other
obstructions other than that for the light and air to pass through. In the bedrooms, they
only have one window in each bedroom.
15

Their kitchen is situated at the right side of the dining room with a round glass
table and six chairs. They have their own utensils, which they use when eating and
cooking. They cook by using stove and LPG tank. They use fluorescent bulbs.
Their home is near a supermarket. There is also a church that is a jeepney ride
away from their home. They have a car. However, since Grandpa Vips is the only one in
their family who knows how to drive, they only use their car when he is present. They
use jeepneys and tricycles as their means of transportation. They use cellphones as a
mean of communication.
B. Pediatric History
Growth and Development
1. Erik Erikson
Stage 1: Trust vs. Mistrust
The development task for infants is learning trust versus mistrust. Infants whose
needs are met when those needs arise, whose discomforts are quickly removed, who
are cuddled, played with , and talked to, come to view the world as a safe place and
people as helpful and dependable. However, when their care is inconsistent, inadequate,
or rejecting, it fosters a basic mistrust: infants become fearful and suspicious of the world
and of people (Pillitteri, 2007, p. 815).
According to Mommy Vips, Vipsy’s needs were always met in a consistent
manner. They would feed her every two to three hours. They would cuddle her whenever
she cries. Mommy Vips have a schedule of when to feed Vipsy, her nap time, her play
time, and the time of her bath. During her infancy years, Vipsy always smiles whenever
someone other than her caregivers plays with her. She developed stranger anxiety when
16
she was about 9 months old. By that time, only her caregivers are able to cuddle her;
otherwise, she would cry and look for her caregivers.
Stage 2: Autonomy vs. Shame and Doubt
Autonomy builds on children’s new motor and mental abilities. Children take
pride in new accomplishments and want to do everything independently, whether it is
pulling the wrapper off a piece of candy, selecting a vitamin tablet out of the bottle,
flushing the toilet, or replying, “No!” (Pillitteri, 2007, p. 816).
Vipsy as observed by the researcher love to say the word “ayaw”. When asked to
state her name, she would reply “ayaw”. According to Mommy Vips, “ayaw” is her
favorite word. As stated by her mother, Vipsy can already tell her mother that she would
like to pee. Vipsy would say “wiwi” so that she can go to the comfort room. After that,
she always flushes the toilet without the help of her mother. Vipsy at this age loves to do
things independently such as eating her bubble gum. She would open the wrapper by
herself and throw the bubble gum by herself.
2. Sigmund Freud
Oral Phase
Freud termed the infant period the “oral phase” because infants are so interested
in oral stimulation or pleasure during this time. According to this theory, infants suck for
enjoyment or relief of tension, as well as nourishment (Pillitteri, 2007, p. 814).
When Vipsy was in her infancy stage, she loves to put everything in her mouth
according to Mommy Vipsy. Whatever object she touches, she would put in her mouth to
play with. She has her teething toys which she used always. Caregivers usually provide
her with a pacifier. If Vipsy has no pacifier, she would thumb suck and usually fall
asleep.
17

Anal Phase
Freud described the toddler period as the “anal phase” because during this time,
children’s interests focus on the anal region as they begin toilet training. Elimination
takes place on new importance for them. Children find pleasure in both the retention of
feces and defecation. This anal interest is part of toddlers’ self-discover, a way of
exerting independence (Pillitteri, 2007, p. 814).
Vipsy can only tell her mother that she is about to urinate by saying the word
“wiwi”. However, she still cannot control her defecation because of her illness.
3. Jean Piaget
Sensorimotor Stage (Coordination of secondary reactions)
Sensorimotor intelligence is practical intelligence, because words and symbols for
thinking and problem solving are not yet available at this early stage. At the beginning of
infancy, babies relate to the world through their sense, using only reflex behavior. As
infants progress through this stage (which includes the schemas of primary and
secondary circular reactions and coorination of secondary reactions), they learn the
basic concept that people are separate entities from objects. In the primary circular
return, infants repeat what they tend to enjoy such as sucking. There is repetition of
behavior. The secondary circular return refers to activities that are separated from the
child’s body. Infants learn that objects in the environment are permanent and continue to
exist even when out of sight. During the final phase (coordination of secondary
reactions), infants begin to demonstrate a goal directed behavior. After noticing that
hitting a mobile makes it move, infants then reach for and hit a music box nearby, in this
way actively seeking new experiences (Pillitteri, 2007p. 818).
18
During this stage, Vipsy discovered permanence. She knows that when her
mother disappears, her mother would come back again. When her mother is out of sight,
she would cry continuously because she knows that her mother is present even if she is
out of Vipsy’s sight. She also has a toy that has a button. If that button is pressed, the
toy would vibrate and make sounds. When Vipsy’s mother presses the button, the toy
would vibrate and make sounds; when the toy stopped, the baby pressed the button
again to make it vibrate again and again. Vipsy also loves to play peek-a-boo with her
caregivers during her infancy years.
Tertiary Circular Reaction
The toddler period is one of transition as children complete the final stages of the
sensorimotor period as tertiary circular reaction and begin to develop some cognitive
skills of the preoperative period, such as symbolic thought and ego-centric thinking. In
the tertiary reaction schema, children use trial and error to discover new characteristics
of objects and events. The child is able to experiment to discover new properties of
objects and events. Child uses memory and imitation to act.
According to Mommy Vips, Vipsy can count from one to ten and can sing her
ABCs with the guidance of her caregivers. Vipsy also loves watching Barney and she
can sing with the songs being played. As observed, Vipsy loves to eat bubble gum.
When she eats bubble gum, she only chews it for one minute and throws it. Then she
would get another gum, chew it for one minute and discard it again. She loves to talk
with her caregivers, however, she still babbles and she cannot complete a sentence.
19
C. Family-Health Illness History
Legend:
20
VIPSY2 y/o
Vipsy Boy16 y/o
Grandma Vips49 y/o
Vipsy Girl
14 y/o
89 y/o 2008DM
GrandpaVips (HPN)
47 y/o
Mommy Vips
18 y/o
2008Old age
66 y/oHPNDM
Daddy Vips20 y/o
Female
Male
Deceased
Client
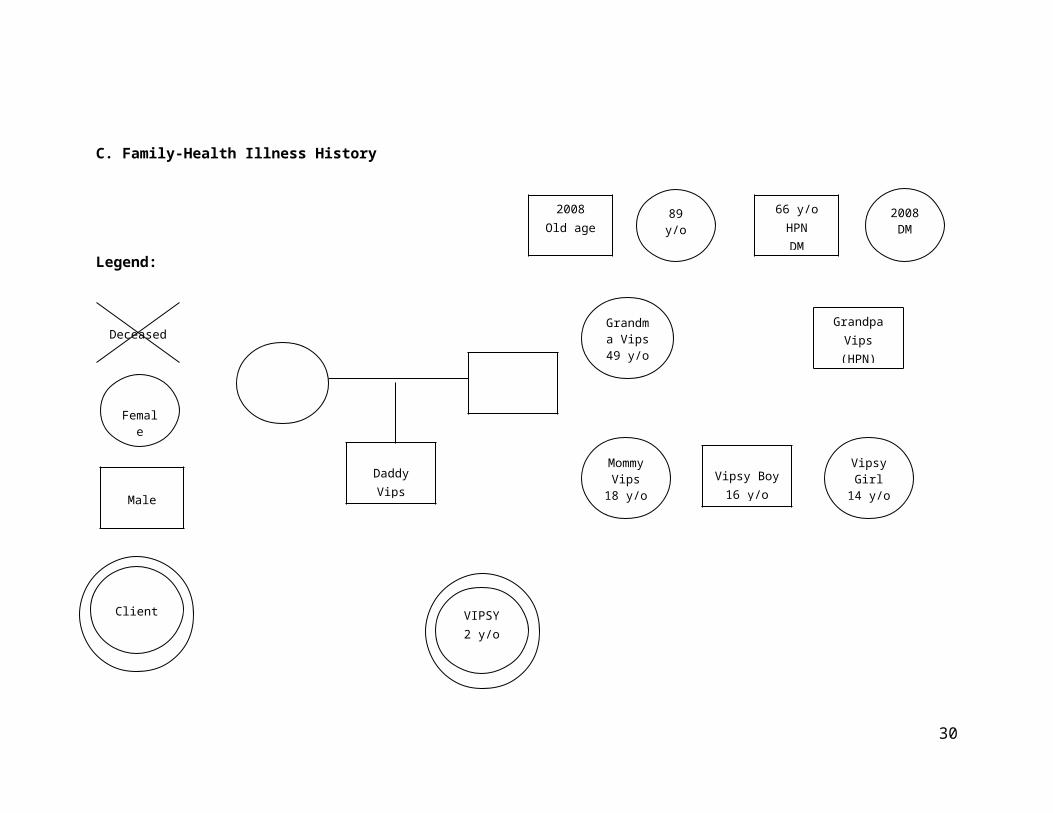
The diagram shows the family health history of Vipsy. Family health history taking is very
crucial in determining hereditary factors that contributed to the disease of the client. The
information came from Grandma Vips’ narration.
Vipsy have a history of Diabetes Mellitus and Hypertension. Grandpa Vips has
hypertension. Grandma Vips have no diagnosed illness. The father of Grandma Vips
died last 2008 and the death was due to old age. The mother of Grandma Vips is still
alive with no diagnosed illness. On Grandpa Vips’ side, her mother died also last 2008
due to complications of Diabetes Mellitus. Grandpa Vips’ father is diagnosed to have
Hypertension and Diabetes Mellitus. Mommy Vips have no known disease as well as
Daddy Vips. The siblings of Mommy Vips are not diagnosed of any illness.
*Family history of Daddy Vips was not included because Grandma Vips does not want to
talk about the father of Vipsy since they are not married and Mommy Vips got pregnant
with Vipsy when she was only 16 years old. Also, Mommy Vips is not familiar with the
family health-illness history of Daddy Vips.
D. History of Past Illness
Vipsy is diagnosed to have a Glucose-6-Phosphate Dehydrogenase deficiency.
She had her newborn screening after she was born in a private hospital in the City of
San Fernando. Mommy Vips wants to confirm the diagnosis so they went to Manila to
have a second opinion regarding her diagnosis. After testing, it was confirmed that Vipsy
has G6PD. Mommy Vips was given education regarding the diet and food restrictions
with regards to clients with G6PD. Vipsy occasionally has fever, cough and colds. She
had two medical consultations with regards to her fever, cough and colds and she was
prescribed to have Paracetamol and Loviscol and Salinase for her cough and colds.
Mommy Vips religiously followed the prescribed medications for Vipsy.
21

E. History of Present Illness
The history of present illness of the client was discussed by Grandma Vips.
According to her, Vipsy’s first episode of diarrhea started last Novermber 2009. She had
watery stools three to four times per day. At the onset of her diarrhea, they immediately
consulted her private physician and she was prescribed to take OMX, Zinnat, Pediachlor
and Chlorocare. The physician diagnosed her to have an Acute Gastroenteritis
Medications were given to Vipsy then her signs and symptoms would subside for one
week. After that week, she would have episodes of diarrhea again. Consultation is done
and same medications were given. Grandma Vips stated that they have been consulting
their private physician almost every week. Mommy Vips mentioned that her diarrhea
started when Vipsy started to eat solid foods. She was bottle fed for more than one year
before solid foods were introduced. Before, she did not have any episodes of diarrhea
until she began to eat solid foods.
By the third week of December 2009, she had three watery loose stools and no
other signs and symptoms noted. They consulted her private physician and Vipsy was
diagnosed with Acute Gastroenteritis again. She was prescribed with Erceflora and
Hidrasec. After one week, Vipsy continues to have two to three watery stools per day,
hence, consult to a private physican and was advised to continue taking Erceflora and
Hidrasec. The week after her last consult, Vipsy was still having two to three watery
loose stools. They consulted her private physician again and she was given an
additional antibiotic. By the second week of January 2010, Mommy Vips noticed that
Vipsy’s abdomen is distended; they consulted her private physician and ordered for
Vipsy to have an ultrasound of her abdomen. Vipsy’s ultrasound revealed Hydrops of her
Gallbladder. However, no surgery was done since the surgeon was not available. On the
third week of January 2010, Vipsy’s signs and symptoms persisted and was given
22

Pediachlor by her private physician. The day after her consultation she was advised to
have a repeat abdominal ultrasound. The result was the same as the first ultrasound
which reveals Hydrops of the gallbladder. Her signs and symptoms persisted hence her
admission in a private institution last January 21, 2010 with a chief complaint of
abdominal enlargement.
Her admission last January 21, 2010 was her first confinement. She was
admitted from January 21, 2010 with an admitting diagnosis of Hydrops of Gallbladder,
Electrolyte Imbalance and glucose-6-phosphate dehydrogenase deficiency and was
discharged last February 15, 2010 with a final diagnosis of Vasoactive Intestinal Tumor.
During her confinement, she was given Ampicillin IV, Gentamicin IV, Hidrasec sachet,
Clarithromycin syrup, Paracetamol suppository, Metronidazole IV, Unasyn IV, Aeknil IV,
Vitamin K IV, Famotidine IV, Amikacin IV, Nutrillin and Pedzinc + C syrup as her
medications. Antibiotics, Antipyretic, Antidiarrheal and Vitamins were given during her
confinement. Total parenteral nutrition was also administered because Vipsy was kept
on NPO for almost two weeks. Nasogastric tube was also inserted to decompress her
stomach due to the findings from her abdominal x-ray and CT scan. The nasogastric
tube remained in place for almost two weeks. Abdominal x-ray was done which had an
impression of Mild Adynamic Ileus. The abdominal x-ray also showed that there is an
increase in the number of small and large that shows moderate gaseous distention and
multiple air-fluid levels are seen. Chest X-ray was also done with a result which revealed
Atelectasis or pneumonia left retrocardiac area. Ultrasound of the gallbladder was also
done. Results demonstrated that Vipsy has a normal sized gallbladder with sludge ball,
negative for cholecystits and non-dilated biliary tree. Computed Tomography of the chest
was also done to have more clear visualization of the lungs. The CT scan of the chest
revealed that there is a calcified soft tissue mass, left posterior T8-T12 paravertebral
area, primary consideration is posterior mediastinal teratoma. There was an incidental
23

note of moderate gaseous distention of intestine; either due to ileus or obstruction and
the lungs is negative for neither pulmonary infiltrates nor pleural effusion. On February 4,
2010, Vipsy had undergone operation. The procedure was Exploratory Laparotomy
Transabdonminal Biospy (transdiaphragmatic), Laddi Procedure with Appendectomy
and Cholecystectomy. The tumor incised was located in the left paravertebral area
behind the posterior lips of the diaphragm. The tumor was solid, fixed, and hard in
character. The Histopathology Diagnosis of tumor revealed a posterior mediastinal mass
ganglioneuroma. The microscopic description of the tumor stated no nuclear atypia,
mitosis or malignant changes is seen in the tumor. Vipsy’s potassium levels were also
monitored. She was hypokalemic upon admission with a result of 1.94 mmol/L and she
was infused with postassium chloride in her intravenous solution. Sodium results were
determined which revealed low levels (133.7 mmol/L). Ionized Calcium and Chloride
levels were also determined and the results were within normal range. Bicarbonate
determination was done through arterial blood gas test which revealed a low
Bicarbonate level. Fasting and random blood sugar were determined and they were
within normal limits. According to Grandma Vips, serum Vasoactive Intestinal Peptide
was also determined and the results was VIP serum was >400. It was done on an OPD
basis in Manila.
After one month (March 24, 2010), Vipsy was admitted in the same institution
with a chief complaint of loose bowel movement. Four days prior to admission, Vipsy
had colds of watery discharge associated with low grade fever and soft stool (three times
per day) and she was given Paracetamol and Pediatapp by her mother. Two days prior
to admission, they consulted her attending physician and was given Chlorocare.
According to her attending physician, her weight the week after her admission was 12
kg. Few hours prior to admission, Vipsy had loss of appetite, profuse sweating, and
weakness associated with one soft watery stool which prompted her physician to admit
24

her in a private institution. She was then discharged after five days of confinement last
March 28, 2010.
F. Physical Examination
March 24, 2010 (Lifted from the Chart)
Vital Signs:
Temperature: 36.5 oC
Pulse Rate: 100 bpm
Respiratory Rate: 24 cpm
Physical Assessment
General Survey: Anicteric sclera, pale palpebral conjunctiva
Chest & Lungs: symmetrical lung expansion, clear breath sounds
Cardiovascular: Adynamnic Precordium, normal rate regular rhythm
Abdomen: Globular; LBS, soft, (+) slightly tympanic
Extremities: full and equal pulses, (-) edema
Nutritional Status
Age: 26 months (2 years, 1 month, 6 days)
Weight: 11.8 kgs
According to the FNRI table, Vipsy’s weight is within the normal range.
First Nurse- client Interaction (March 24, 2010)
25

General Appearance
The client was awake, cyring and irritable with an ongoing IVF of #1 D5 0.3 NaCl
500 cc x 44-45 ugtts/ min at 400 cc level infusing well on the left hand, with pale nail
beds, pale palpebral conjunctiva, pale lips, appears weak, and slightly sleepy, (-)
vomiting, with good skin turgor, (+) loss of appetite, with 3 episodes of watery loose
stools.
Vital Signs:
Temperature: 36.7 oC
Pulse Rate: 112 bpm
Respiratory Rate: 26 cpm
Physical Assessment
The Integument
Skin: Fair complexion, uniform in color, (+) Pallor noted; (-) cyanosis
Hair: Evenly distributed short, thin, straight hair. Body hair are evenly distributed
Nails: pale pink nail beds; Short and clean finger nails, capillary refill of 2
seconds, (-) clubbing
The Head
Skull and Face: Head is normocephalic and has a smooth contour. Facial
features are symmetrical with symmetrical facial movements.
Eyes: Hair at the eyebrows is evenly distributed with skin intact. Eyebrows are
symmetrically aligned and equal in movement. Eyelashes are equally distributed
and slightly curled outside. Eyelids have intact skin with no discharge and
discoloration. The eyelids close and open symmetrically. With a normal blinking
reflex and bilateral blinking. The palpebral conjunctiva is shiny and pale. There
26

is no edema or tenderness over the lacrimal gland. Pupils equally round and
reactive to light accommodation. Sclera is anicteric.
Ears: Color same as facial skin, symmetrical and aligned with the outer canthus
of the eye. The auricles are mobile, firm and not tender. Pinna recoils after it is
folded. She was able to hear normal voice tones.
Nose and Sinuses: Nose is symmetrical, uniform in color, (-) nasal flaring. There
is no presence of tenderness and lesions. Clear watery discharge from both
nares. The nasal septum is intact and in midline. The maxillary and frontal
sinuses are not tender.
Mouth: The lips are pale pink in color. With two upper incisor, two lower incisor,
2 upper lateral incisor, and one upper molar teeth, pinkish gums. The tongue is in
central position, pinkish in color, with thin whitish coating, no lesions. It moves
freely without any tenderness. Uvula is positioned in the midline of soft palate,
tonsils are pink, not inflamed with no discharge. With the presence of gag reflex.
Neck
Head centered, coordinated, smooth movements, no palpable lymph nodes. The
thyroid gland is not visible on inspection and ascends during swallowing. No difficulty
in swallowing. No hoarseness of voice.
Chest
Symmetric, skin intact with uniform temperature. Clear breath sounds,
symmetrical chest expansion.
Cardiovascular and Peripheral Vascular Systems
27

Heart: There were no pulsations, with symmetric pulse volumes of the carotid
artery; there is also absence of sound (bruit) heard on auscultation. The jugular
veins are not visible in a semi-fowler’s position.
Peripheral Vascular System: There is a presence of symmetric pulse volume
with full pulsations. No presence of edema.
Abdomen
Abdomen with uniform color, unblemished skin on the right upper part. No
evidence of enlargement of the liver or spleen and symmetric in contour.
Symmetrical movements caused by respirations. Have tympani sound over the
stomach and dull on the liver and spleen. Flabby, soft and nontender; with a surgical
scar on umbilical area, rounded abdomen.
Musculoskeletal
Muscles are equal in size on both sides of the body. There are no tremors, firm,
and smooth coordinated movements with equal strength on each body side. No
presence of deformities.
Extremities: No edema. Full and equal pulses.
Second Nurse-client Interaction (March 25, 2010)
28

General Appearance
The client was on bed awake on a sitting position, with an ongoing IVF of #4 D5
0.3 NaCl 72.5 cc + KCl 1.5 cc = 74 cc every 2 hours at 50 cc level via soluset infusing
well on the left hand, with pale nail beds, pale palpebral conjunctiva, pale lips, (-)
weakness, (-) vomiting, with good skin turgor, with fair appetite, with 3 episodes of
scanty loose stools, and (+) productive cough. She was not irritable and she smiled
at the nurse researcher
Vital Signs:
Temperature: 37.6 oC
Pulse Rate: 124 bpm
Respiratory Rate: 28 cpm
Physical Assessment
The Integument
Skin: Fair complexion, uniform in color, (+) Pallor noted; (-) cyanosis
Hair: Evenly distributed short, thin, straight hair. Body hair are evenly distributed
Nails: pale pink nail beds; Short and clean finger nails, capillary refill of 2
seconds, (-) clubbing
The Head
Skull and Face: Head is normocephalic and has a smooth contour. Facial
features are symmetrical with symmetrical facial movements.
Eyes: Hair at the eyebrows is evenly distributed with skin intact. Eyebrows are
symmetrically aligned and equal in movement. Eyelashes are equally distributed
and slightly curled outside. Eyelids have intact skin with no discharge and
29
discoloration. The eyelids close and open symmetrically. With a normal blinking
reflex and bilateral blinking. The palpebral conjunctiva is shiny and pale. There
is no edema or tenderness over the lacrimal gland. Pupils equally round and
reactive to light accommodation. Sclera is anicteric.
Ears: Color same as facial skin, symmetrical and aligned with the outer canthus
of the eye. The auricles are mobile, firm and not tender. Pinna recoils after it is
folded. She was able to hear normal voice tones.
Nose and Sinuses: Nose is symmetrical, uniform in color, (-) nasal flaring. There
is no presence of tenderness and lesions. Clear watery discharge from both
nares. The nasal septum is intact and in midline. The maxillary and frontal
sinuses are not tender.
Mouth: The lips are pale pink in color. With two upper incisor, two lower incisor,
2 upper lateral incisor, and one upper molar teeth, pinkish gums. The tongue is in
central position, pinkish in color, with thin whitish coating, no lesions. It moves
freely without any tenderness. Uvula is positioned in the midline of soft palate,
tonsils are pink, not inflamed with no discharge. With the presence of gag reflex.
Neck
Head centered, coordinated, smooth movements, no palpable lymph nodes. No
difficulty in swallowing. No hoarseness of voice.
Chest
Symmetric, skin intact with uniform temperature. Clear breath sounds,
symmetrical chest expansion. (+) productive cough.
Cardiovascular and Peripheral Vascular Systems
30

Heart: There were no pulsations, with symmetric pulse volumes of the carotid
artery; there is also absence of sound (bruit) heard on auscultation. The jugular
veins are not visible in a semi-fowler’s position.
Peripheral Vascular System: There is a presence of symmetric pulse volume
with full pulsations. No presence of edema.
Abdomen
Abdomen with uniform color, unblemished skin on the right upper part. No
evidence of enlargement of the liver or spleen and symmetric in contour.
Symmetrical movements caused by respirations. Have tympani sound over the
stomach and dull on the liver and spleen. Flabby, soft and nontender; with a surgical
scar on umbilical area, rounded abdomen.
Musculoskeletal
Muscles are equal in size on both sides of the body. There are no tremors, firm,
and smooth coordinated movements. No presence of deformities.
Extremities: No edema. Full and equal pulses.
31

Third Nurse-client Interaction (March 27, 2010)
General Appearance
The client on bed asleep on a supine position, with an ongoing IVF of # 38 D5
0.3 NaCl 72.5 cc + KCl 1.5 cc = 74 cc every 2 hours at 70 cc level via soluset infusing
well on the left hand, with pinkish nail beds, pinkish palpebral conjunctiva, pinkish lips, (-)
weakness, (-) vomiting, with good skin turgor, with fair appetite, with 2 episodes of
scanty loose stools.
Vital Signs:
Temperature: 36.6 oC
Pulse Rate: 110 bpm
Respiratory Rate: 30 cpm
Physical Assessment
The Integument
Skin: Fair complexion, uniform in color, (-) cyanosis
Hair: Evenly distributed short, thin, straight hair. Body hair are evenly distributed
Nails: pinkish pink nail beds; Short and clean finger nails, capillary refill of 2
seconds, (-) clubbing
The Head
Skull and Face: Head is normocephalic and has a smooth contour. Facial
features are symmetrical with symmetrical facial movements.
Eyes: Hair at the eyebrows is evenly distributed with skin intact. Eyebrows are
symmetrically aligned and equal in movement. Eyelashes are equally distributed
and slightly curled outside. Eyelids have intact skin with no discharge and
32

discoloration. The eyelids close and open symmetrically. With a normal blinking
reflex and bilateral blinking. The conjunctiva is shiny and pinkish. There is no
edema or tenderness over the lacrimal gland. Pupils equally round and reactive
to light accommodation. Sclera is anicteric.
Ears: Color same as facial skin, symmetrical and aligned with the outer canthus
of the eye. The auricles are mobile, firm and not tender. Pinna recoils after it is
folded. She was able to hear normal voice tones.
Nose and Sinuses: Nose is symmetrical, uniform in color, (-) nasal flaring. There
is no presence of tenderness and lesions. The nasal septum is intact and in
midline. The maxillary and frontal sinuses are not tender.
Mouth: The pinkish lips in color. With two upper incisor, two lower incisor, 2
upper lateral incisor, and one upper molar teeth, pinkish gums. The tongue is in
central position, pinkish in color, with thin whitish coating, no lesions. It moves
freely without any tenderness. Uvula is positioned in the midline of soft palate,
tonsils are pink, not inflamed with no discharge. With the presence of gag reflex.
Neck
Head centered, coordinated, smooth movements, no palpable lymph nodes. No
difficulty in swallowing. No hoarseness of voice.
Chest
Symmetric, skin intact with uniform temperature. Clear breath sounds,
symmetrical chest expansion. (+) productive cough
33

Cardiovascular and Peripheral Vascular Systems
Heart: There were no pulsations, with symmetric pulse volumes of the carotid
artery; there is also absence of sound (bruit) heard on auscultation. The jugular
veins are not visible in a semi-fowler’s position.
Peripheral Vascular System: There is a presence of symmetric pulse volume
with full pulsations. No presence of edema.
Abdomen
Abdomen with uniform color, unblemished skin on the right upper part. No
evidence of enlargement of the liver or spleen and symmetric in contour.
Symmetrical movements caused by respirations. Have tympani sound over the
stomach and dull on the liver and spleen. Flabby, soft and nontender; with a surgical
scar on umbilical area, rounded abdomen.
Musculoskeletal
Muscles are equal in size on both sides of the body. There are no tremors, firm,
and smooth coordinated movement. No presence of deformities.
Extremities: No edema. Full and equal pulses.
34

G. DIAGNOSTIC AND LABORATORY FINDINGS
Laboratory
Procedure
Date
ordered/
Date
results in
Indication or Purpose Results Normal Values Analysis and interpretation of results
CBC
The CBC and differential count are a series of tests of the peripheral blood that provide a tremendous amount of information
about the hematologic system and many other organ systems. They are inexpensively, easily, and rapidly performed as
screening test.
Hematocrit
DO: 03/
24/10
Results in:
03/ 24/ 10
To aid diagnosis of
anemia, or abnormal
states of hydration
0.40 0.31 – 0.43
The client has a normal hematocrit count. She
has a good hydration status. The client does
not have anemia.
HemoglobinTo measure the severity
of anemia
128 110 – 160 g/LHemoglobin level is normal indicating the
absence of anemia.
Leukocytes
count
To determine infection or
inflammation
4.2 5 – 15.5 x 103 g/L
The leukocyte count is decreased which
indicates a presence of viral infection that may
be the cause of the client’s cough and colds.
Neutorphils To help diagnose 0.36 0.25 – 0.43 The client has normal neutorphil level. The

specific types of illnesses
that affect the immune
system
client has no inflammation.
Lymphocytes
Plays an important role
in the immunity, they are
the one responsible for
the activities of the
immune system.
To assess and monitor
genetic and acquired
immuno deficiency
states.
0.55 0.20 – 0.65
The client has normal lymphocyte level. This
indicates that the client is not
immunocompromised.
Monocytes
To help diagnose an
illness such as infection
or inflammatory disease
0.07 0.00 – 0.05
The levels are increased. This indicates the
presence of infection as in conjunction with the
decrease in leukocyte count.
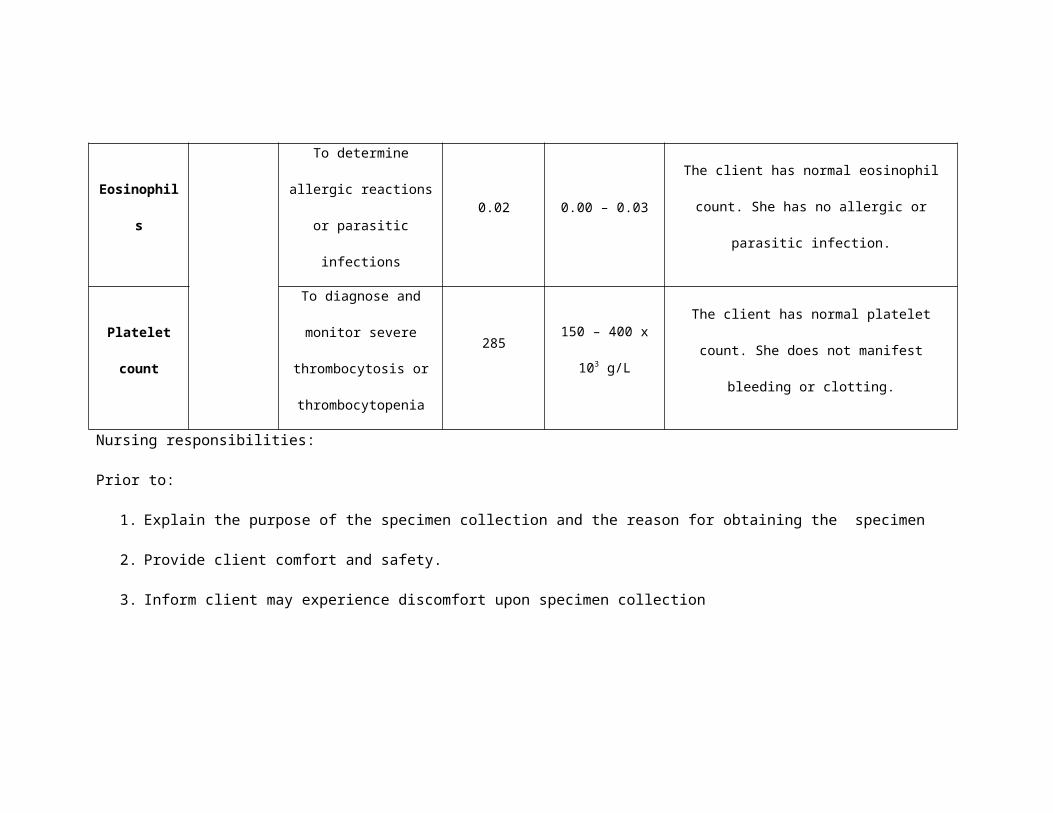
Eosinophils To determine allergic
reactions or parasitic
0.02 0.00 – 0.03 The client has normal eosinophil count. She

infections has no allergic or parasitic infection.
Platelet
count
To diagnose and monitor
severe thrombocytosis or
thrombocytopenia
285150 – 400 x 103
g/L
The client has normal platelet count. She does
not manifest bleeding or clotting.
Nursing responsibilities:
Prior to:
1. Explain the purpose of the specimen collection and the reason for obtaining the specimen
2. Provide client comfort and safety.
3. Inform client may experience discomfort upon specimen collection
4. Obtain history of the patient’s gastrointestinal, hematopoeitic, immune and respiratory system, as well as results of previously
performed tests, patient’s complaints, including a list of known allergy.
5. Obtain a list of medications the patient is taking including herbs, nutritional supplements and nutraceuticals. The requesting
practitioner and laboratory should be advice if the patient regularly uses these products so that their effects can be taken into
consideration when reviewing results.
6. There are no food or medical, fluid restrictions unless by medical directions.
During:

1. Avoid hemolysis.
2. List on the laboratory slip any drugs that may affect test results.
3. Direct the patient to breathe normally and to avoid unnecessary movements.
After:
1. Apply pressure to the venipuncture site.
2. Document the procedure done.
3. Label and transport the specimen to the laboratory promptly.
4. Report abnormal lab findings to the health care professional in a timely manner consistent with the severity of the abnormal
results and observe venipuncture site for bleeding or hematoma formation. Apply pressure bandage
5. Evaluate test results in relation to the patient’s symptoms and other test performed.

Laboratory
Procedure
Date ordered/
Date results inIndication or Purpose
Result
sNormal Values Analysis and interpretation of results
BLOOD
CHEMISTRY
A number of other tests may be performed on blood serum. These are often referred to as the blood chemistry. It provides
valuable diagnostic cues.
Potassium
DO: 03/ 24/10
Results in: 03/
24/ 10
To evaluate clinical signs of
potassium excess
(hyperkalemia) or potassium
depletion (hypokalemia) 2.68
3.50 – 5.50
mmoL/L
The client has hypokalemia. Due to the
excessive production of VIP, there is also
excessive stimulation of intestinal
secretions and intestinal motility. This
leads to frequent secretory watery
diarrhea of the client wherein potassium is
lost further.
DO: 03/ 24/10
Results in: 03/
25/ 10 (6 AM)
2.04
The client’s potassium level decreased.
Potassium is lost in her stool due the
effects of excessive amount of VIP
produced by the ganglioneuroma. The
intravenous fluids did not increase her
potassium level.
DO: 03/ 25/10 2.34 The client’s potassium level increased

Results in: 03/
25/ 10 (3 PM)
due to the incorporation of potassium in
the intravenous fluid. However, the client
still has watery stools that cause excretion
of potassium in the stool caused by
VIPoma.
DO: 03/ 25/10
Results in: 03/
26/ 10 (6 AM)
2.89
The potassium level increased indicating
that the client is responding well to the
intravenous therapy prescribed to her.
Her intravenous fluid is incorporated with
potassium chloride. Still with the presence
of VIPoma, potassium is being secreted
continuously through her stool.
DO: 03/ 26/10
Results in: 03/
26/ 10 (2 PM)
3.49
The level of the client’s potassium is near
the normal level showing improvement in
her condition.
DO: 03/ 26/10
Results in: 03/
27/ 10 (6 AM)
3.47 The potassium level slightly decreased
since the client had four episodes of loose
watery stools from the night before
extraction. Potassium is lost through her

stool from the effect of excessive
vasoactive intestinal peptide.
DO: 03/ 27/10
Results in: 03/
28/ 10 (6 AM)
3.18
The client’s potassium level decreased
despite the presence of potassium
chloride in her intravenous fluid since she
had 3 episodes of loose watery stool from
the previous day. Potassium was
secreted from the stool because of the
effect of cAMP which was stimulated by
the excessive amounts of vasoactive
intestinal peptide.
DO: 03/ 28/10
Results in: 03/
28/ 10 (2 PM)
3.49
The client’s potassium level is near the
normal level. She responded well to the
intravenous treatment and with her intake
of kalium durule.
Sodium DO: 03/ 25/10
Results in: 03/
25/ 10 (3 PM)
To evaluate fluid-electrolyte
and acid-base balance and
excretion of sodium from the
136.3 135 – 150
mmoL/L
The client has normal sodium level. The
client did not excrete sodium through her

stool stool.
Chloride
DO: 03/ 25/10
Results in: 03/
25/ 10 (3 PM)
To detect acid-base
imbalance (acidosis or
alkalosis) and to aid
evaluation of fluid status and
extracellular cation-anion
balance
106.198 - 107
mmoL/L
The client has normal chloride level. She
does not manifest hypochlorhydria which
is also a manifestation of vipoma.
Nursing Considerations:
Prior to
1. Explain the purpose of the specimen collection and the reason for obtaining the specimen
2. Obtain history of the patient’s complains, including a list of known allergy.
3. Provide client comfort and safety.
4. Inform client may experience discomfort upon specimen collection
5. Obtain a list of medications the patient is taking including herbs, nutritional supplements and nutraceuticals. The requesting
practitioner and laboratory should be advice if the patient regularly uses these products so that their effects can be taken into
consideration when reviewing results.
During
1. Ensure that the patient has complied with the dietary preparations and other pre-fasting restrictions.

2. Direct the patient to breathe normally and to avoid unnecessary movements.
3. Observe standard precautions.
After
1. Report abnormal laboratory findings to the health care professional in a timely manner consistent with the severity of the
abnormal results
2. Observe venipuncture site for bleeding or hematoma formation. Apply pressure bandage.
3. Instruct the client to resume usual diet as directed by the health care practitioner.
4. Evaluate test results in relation to the patient’s symptoms and other test performed.
Laboratory
Procedure
Date
ordered/
Date
Indication or Purpose Results Normal
Values
Analysis and interpretation of results

results in
Urinalysis
Color
DO: 03/
24/10
Results in:
03/ 25/ 10
To determine color of urine Light yellowYellow to light
orange
The client has normal appearance of
urine. She does not manifest
concentrated urine which may indicate as
dehydration which can be a result of
secretory diarrhea from VIPoma.
AppearanceTo determine presence of
crystalsClear Clear No crystals are present in the urine.
pHTo determine the acid/ base
balance of the patient.6.5 4.6 – 8.0
The client has normal urine pH. Metabolic
acidosis is not present.
Specific Gravity
Indicates the concentration of
urine and reflects the client’s
hydration status as well as
renal function.
1.010 1.005-1.030The result is within the normal range. The
client is not dehydrated.
SugarTo determine presence of
sugar in the urineNegative Negative
Sugar and albumin are not present in the
urine and it indicates normal functioning
of the kidneys and absence of
hyperglycemia which can be manifested
Albumin To detect protenuria Negative Negative

by presence of sugar in the urine.
Pus cells
To indicate presence
bacteria; to determine
presence of infection
1-3/ HPFNone
Pus cells are present in small amount
which indicates presence of bacteria in
the urine.
Red Cells To detect hematuria 1-3/ HPF < 2/ HPF
The client has a slight presence of
microscopic RBC in her urine. This
indicates the presence of microscopic
hematuria.
Epithelial cellsTo detect infection
RareNone
Results indicate that bacteria are present
in the urine.Bacteria Few
Nursing Responsibilities:
Prior to:
1. Explain that this analysis helps to diagnose renal or urinary tract disease and to evaluate overall body function.
2. Inform the relative that the patient need not restrict food and fluids.
3. Notify the laboratory and physician of medications the patient is taking that may affect laboratory results; they may need to be
restricted.
During:
1. Do perineal hygiene.

2. Place the weebag.
3. Handle the specimen container gently to avoid spillage
After:
1. Submit sample to lab with lab order for proper screening
2. Document the procedure done.
Laboratory
Procedure
Date
ordered/
Date
results in
Indication or Purpose ResultsNormal
ValuesAnalysis and interpretation of results

Stool
Examination/
Fecalysis
DO: 03/
24/10
Results in:
03/ 27/ 10
The examination of feces
provides important information
that aids in the differential
diagnosis of various
gastrointestinal disorders.
Fecal studies may also be used
for microbiologic studies,
chemical determination, and
parasitic examinations.
To determine cause of diarrhea.
Color: Brown Brown The client has normal color of feces.
Consistency:
watery
Soft and
well formed
The client has an abnormal consistency of
feces. This is due to the effects of
excessive vasoactive intestinal peptide
which stimulates overproduction of cAMP
and cause intestinal motility which cause
passing out of watery stool.
Result: No
intestinal
parasites seen
No
intestinal
parasites
seen
The feces does not contain and intestinal
parasites. No infection is seen.
Nursing responsibilities:
Prior to:
1. Explain the purpose of the study and how it is done.
2. Prepare all the materials to be used.
During:
1. Observe universal precautions in collecting a stool specimen.
2. Collect stool specimens in a clean container that has a fitted cover.

3. Do not mix urine and toilet paper with the stool specimen.
After:
1. Correctly label and deliver stool specimens to the laboratory within 30 minutes after collection. If you are unable to deliver the
specimen within 30 minutes, it may be refrigerated for up to 2 hours.
2. Note that no special care is required following the procedure
3. Document the procedure done.
Diagnostic
Procedure
Date ordered/
Date results inIndication or Purpose Results Impression
Analysis and interpretation of
results
Chest X-ray
Posterior-
DO: 03/ 26/10
Results in: 03/
The chest x-ray film is
important in a complete
Compared with chest
taken 2-6-10, present
The rest of the
visualized lung
The results show an abnormal
mass in the left retrocardiac area.

Anterior-
Lateral (PAL)
view
26/ 10
evaluation of the
pulmonary and cardiac
systems.
It was used as a
comparison with the chest
x-ray taken when the client
was admitted in the same
institution last February
2010.
study shows
unchanged status of
mass-like opacity with
lobulated margins
measuring
approximately 48.3 (L)
x 31.8 (trans) mm in
left retrocardiac area.
Rule out posterior
meidastinal mass.
Suggest CT scan for
further evaluation.
fields are
clear.
Heart and
great vessels
in normal size
and
configuration.
Other chest
structures are
unremarkable.
This is in conjunction with the
diagnostic done from the first
confinement of Vipsy such as CT
scan, biopsy and x-ray which
indicates the presence of
ganglioneuroma.
The client has no pneumonia.
Nursing responsibilities:
Prior to:
3. Make sure the patient has signed and appropriate consent form.
4. Explain the purpose of the study and how it is done.

5. Explain who will perform the test and where it will be done.
6. Tell the relatives that fasting is not required and the test takes less than 5 minutes.
7. Instruct relatives to remove clothing to the waist and to put on an x-ray gown.
8. Inform the relatives to remove all metal objects (e.g., necklace) so that they do not block visualization of part of the chest.
9. Tell the relatives that the patient will be ask to take a deep breath and hold it while the film the x-ray films are taken.
10. Instruct relatives to have the patient’s ovaries covered, using a lead shield to prevent radiation-induced abnormalitites.
During:
4. After the patient is correctly positioned, tell him or her to take a deep breath and hold it until the x-ray films are taken.
5. Note that x-ray films are taken by a radiologic technologist in several minutes.
6. Inform the relatives that no discomfort is associated with chest radiography.
After:
4. Note that no special care is required following the procedure
5. Document the procedure done.

Diagnostic
Procedure
Date ordered/
Date results inIndication or Purpose Results Analysis and interpretation of results
15-Lead ECG
DO: 03/ 25/10
Results in: 03/
25/ 10
Electrocardiography graphically
records the electrical current
generated by the heart and
measured by electrodes connected
to an amplifier and strip chart
recorder.
To identify conduction abnormalities
and cardiac arrhythmias
T wave
flattening on
Lead II;
Presence of
U wave on
Leads V4,
V5, V6
Presence of abnormal T wave flattening
and presence of U wave indicates the
presence of hypokalemia. Hypokalemia
causes prolonged myocardial
repolarization function. Hypokalemia
developed due to the secretory effects of
vasoactive intestinal peptide. Cardiac
dysrhythmias are not present.
Nursing responsibilities:
Prior to:
1. Explain the procedure to the patient and relatives.
2. Tell the relatives that no food or fluid restriction is necessary.
3. Explain to the relatives the need of the patient to lie still, relax and breathe normally during the procedure.
4. Explain that the test is painless and takes 5 to 10 minutes.
5. Explain the purpose of the study and how it is done.

6. Explain who will perform the test and where it will be done.
During:
1. Place the patient in a supine or semi-Fowler’s position.
2. Expose the chest, ankles, and wrists.
3. The skin areas designated for electrode placement are prepared by using alcohol swabs or sandpaper to remove skin oil or
debris.
4. Pads with special gel are applied to ensure electrical conduction between skin and electrodes.
5. Place electrodes on the inner aspect of the writs, on the medial aspect of the lower legs, and on the chest.
6. After all the electrodes are in place, connect the lead wires.
7. Press the start button and input any required information.
8. Make sure that all leads are represented in the tracing. If not, determine which electrode has come loose, reattach it, and
restart the tracing.
9. All recording and other nearby electrical equipment should be properly grounded.
10. Make sure that electrodes are firmly attached.
After:
1. Disconnect the equipment, remove the electrodes, and remove the gel with a moist cloth towel.
2. Note that no special care is required following the procedure and document the procedure done.

III. ANATOMY AND PHYSIOLOGY
THE DIGESTIVE SYSTEM
The digestive system
consists of the digestive
tract, a tube extending
from the mouth to the
anus, plus the associated
organs, which secrete
fluids into the digestive
tract. The digestive tract
consists of the oral
cavity, pharynx, esophagus, stomach, small intestine, large intestine, and anus.
Accessory glands are associated with the digestive tract. The salivary glands empty into
the oral cavity, and the liver and pancreas are connected to the small intestine. Inside
digestive tract is a lining called the mucosa. In the mouth, stomach, and small intestine,
the mucosa contains tiny glands that produce juices to help digest food.
Oral Cavity. The oral cavity is bounded by the lips and cheeks and contains the teeth
and tongue. This is the site where food is mechanically digested through mastication.
Mastication breaks large food particles into many small ones and increases efficiency of
digestion. Salivary glands are also found in the oral cavity. The salivary glands secrete
saliva that begins the process of chemical digestion.
Pharynx. The pharynx connects the mouth with the esophagus, consists of three parts:
the nasopharynx, orophayrnx, and laryngopharynx.
Esophagus. It extends from the pharynx to the stomach. It transports foods from the
pharynx and stomach.it contains upper and lower esophageal sphincter that regulates
movement of food into and out of the mouth.
Stomach. It is an enlarged segment of the digestive tract in the left superior part of the
abdomen. It is divided into the fundus(most superior part) and body(largest part). It has
2 openings: cardiac opening (opening from the esophagus to the stomach) and pyloric
opening (opening from the stomach to the small intestine) surrounded by a ring of
smooth muscle (pyloric sphincter). The wall of the stomach consists of three muscle
layers: longitudinal, circular, and oblique. It consists of gastric glands that produce
mucus, HCl, pepsin, gastrin, and intrinsic factor.
Small intestine. It is divided into the duodenum, jejunum, and ileum. It has circular folds,
villi, and microvilli that greatly increase the surface area of the intestinal lining. Goblet
cells and duodenal glands produce mucus.
Liver and Pancreas. The liver consists of four lobes. It receives blood from the hepatic
artery and the hepatic portal vein. Bile leaves the liver through the hepatic duct system.
The pancreas is an endocrine organ and an exocrine gland. Its endocrine function is to
control blood nutrient levels. Its exocrine function is to produce bicarbonate ions and
digestive enzymes.
Large intestine. The cecum forms a blind sac at the junction of the small and large
intestines. The appendix is a blind sac off the cecum. The colon consists of ascending,

transverse, descending, and sigmoid portions. The rectum is a straight tube that ends at
the anal canal.
The functions of the digestive system are to take in and break down food, absorb
digested molecules, provide nutrients and eliminate wastes.
Digestion involves the mixing of food, its movement through the digestive tract, and the
chemical breakdown of the large molecules of food into smaller molecules. Digestion
begins in the mouth, when we chew and swallow, and is completed in the small
intestine. The chemical process varies somewhat for different kinds of food.
After mastication, food is swallowed. Deglutition or swallowing can be divided into
voluntary phase (bolus is formed and it is pushed by the tongue into the oropharynx),
pharyngeal phase (the soft palate is elevated and closes the passage between the
nasopharynx and the oropharynx and the food is received by the pharynx causing the
epiglottis to cover the opening of the larynx) and esophageal phase (food is moved from
the pharynx to the stomach through peristaltic waves. The action of peristalsis looks like
an ocean wave moving through the muscle. The muscle of the organ produces a
narrowing and then propels the narrowed portion slowly down the length of the organ.
At the junction of the esophagus and stomach, there is a ringlike valve closing the
passage between the two organs. However, as the food approaches the closed ring,
the surrounding muscles relax and allow the food to pass.
The food then enters the stomach, which has three mechanical tasks to do. First, the
stomach must store the swallowed food and liquid. This requires the muscle of the
upper part of the stomach to relax and accept large volumes of swallowed material. The
second job is to mix up the food, liquid, and digestive juice produced by the stomach.
The lower part of the stomach mixes these materials by its muscle action. The third task
of the stomach is to empty its contents slowly into the small intestine.
Two solid organs, the liver and the pancreas, produce digestive juices that reach the
intestine through small tubes. In addition, parts of other organ systems (for instance,
nerves and blood) play a major role in the digestive system.
Several factors affect emptying of the stomach, including the nature of the food (mainly
its fat and protein content) and the degree of muscle action of the emptying stomach
and the next organ to receive the contents (the small intestine). As the food is digested
in the small intestine and dissolved into the juices from the pancreas, liver, and
intestine, the contents of the intestine are mixed and pushed forward to allow further
digestion.
Finally, all of the digested nutrients are absorbed through the intestinal walls. The waste
products of this process include undigested parts of the food, known as fiber, and older
cells that have been shed from the mucosa. These materials are propelled into the
colon, where they remain, usually for a day or two, until the feces are expelled by a
bowel movement.
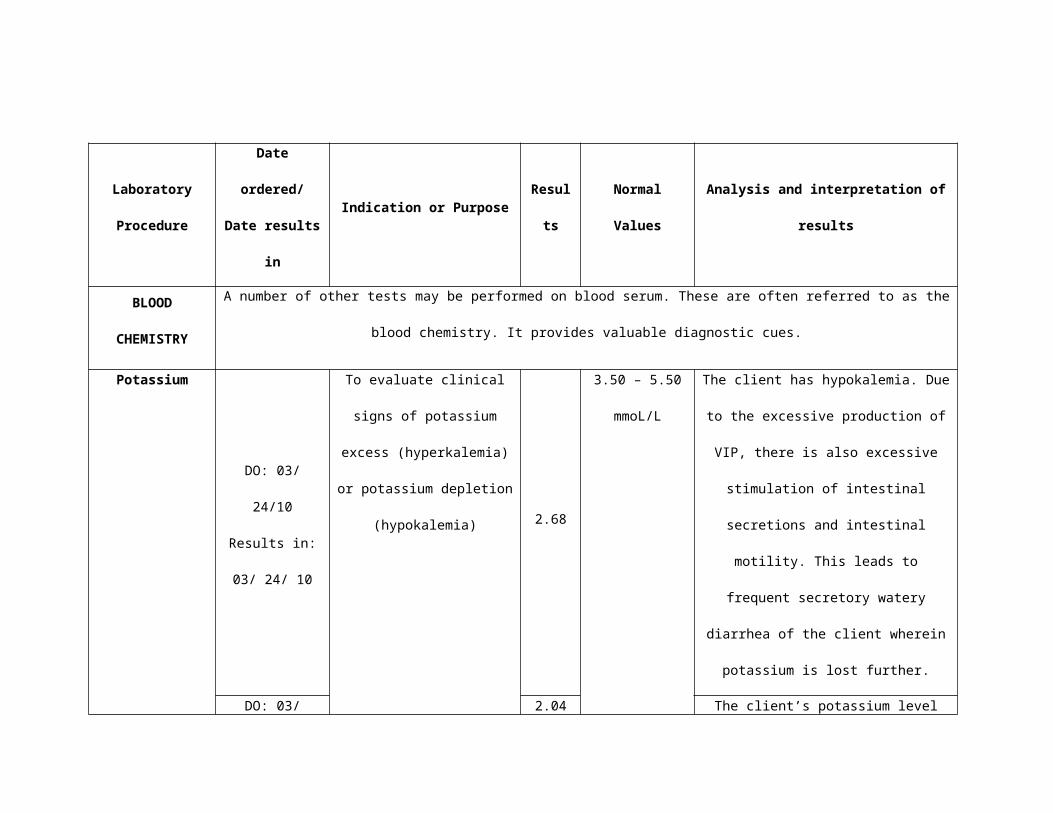
The Pancreas
The secretions of the pancreas, called pancreatic juice, include various enzymes,
including pancreatic amylase (digestion of starch), trypsin, carboxypepiydase, and
chymotrypsin (proteases), as well as pancreatic lipase (digestion of fats). Sodium
bicarbonate is also produced, making the pancreatic juice alkaline. An alkaline
solution neutralizes the HCl in the chyme and provides an optimal environment for
the action of these enzymes.
Pancreatic juice is produced in clusters of exocrine cells called acini. The
remaining cells in the pancreas (about 1 percent of the total) also form clusters (islets of
Langerhans). These are the endocrine cells that produce the hormones insulin,
glucagon, somatostatin, and pancreatic polypeptide.
Pancreatic
juice collects in
small ducts that
merge to form
two large
ducts. The main
pancreatic
duct (duct of
Wirsung)
exits the
pancreas
and merges with the common bile duct from the liver and gallbladder. This combined
duct, called the hepatopancreatic ampulla (ampulla of Vater), then enters the duodenum.
A smaller, second duct that exits the pancreas, the accessory pancreatic duct (duct of
Santorini), joins the duodenum directly.

Pancreatic Islets Form the Endocrine Pancreas
The islets of Langerhans are scattered throughout the organ and consist of richly
vascularized globular masses of cells. Six distinct cell types are correlated with
specific hormones.
Alpha cells synthesize glucagon and are located in the outer rim of the islets.
They constitute 15 to 20% of the total islet cell population. Glucagon induces
glycogenolysis and gluconeogenesis in the liver, thereby raising the blood
glucose level. Its secretion is stimulated by hypoglycemia and by the ingestion of
a low-carbohydrate, high-protein meal. By virtue of these responses, glucagon,
together with insulin, serves to maintain fuel homeostatis.
Beta cells produce insulin and constitute 60 to 70% of all islet cells. By electron
microscopy, cellular insulin is resolved into characteristic polygonal and
rhomboidal crystals enclosed in secretory vesicles. The major obligatory stimulus
for insulin secretion is the binding of glucose to receptors on the surface of the
beta cell.
Delta cells are subdivided into D and D1 types, secreting somatostatin and
vasoactive intestinal polypeptide (VIP), respectively. They are fewer in number
and slightly larger than alpha cells and, like them, tend to be localized at the
periphery of the islets. Delta cells are situated between the alpha and beta cells,
so that the three cell types are often contiguous. Pancreatic somatostatin, a
peptide identical to the one in the hypothalamus, inhibits the pituitary release of
growth hormone. Somatostatin also inhibits secretion by alpha, beta, and D1
cells, acinar cells of the exocrine pancreas, and certain hormone-secreting cells
in the gastrointestinal tract. Coupled with the topographical cell-cell relations

noted above, these hormonal interactions suggest that somatostatin plays a
regulatory role in glucose homeostatis.
D1 cells are smaller than other islet cell types and are rare in the islets of normal
human pancreas. Its hormone, VIP, also has been localized in ganglion cells and
nerve fibers of the pancreas, gut, and brain. In a manner similar to that of
glucagon, VIP induces glycogenolysis and hyperglycemia and regulated ion and
water secretion by epithelial cells of the gastrointestinal tract.
Pancreatic polypeptide-secreting cells are located primarily in the islets of the
head of the pancreas and synthesize a polypeptide that appears to have variable
and opposed functions. These include stimulation of the secretion of enzymes
from the gastric mucosa and inhibition of a number of functions, such as smooth
muscle contraction in the intestine and gallbladder, production of gastric acid,
and secretion by the exocrine pancreas and biliary system.
Enterochromaffin cells are rare components of the islet cell population in the
head of the pancreas. They synthesize serotonin and peptide motilin, a hormone
that stimulates motility of gastric smooth muscle and increases the tone of the
sphincter at the gastoesophageal junction (Rubin, 2005).

IV. THE PATIENT AND HER ILLNESS
Produce excessive amounts of VIP: ↑ serum
VIP
Tumor in adrenal areaNeuroblastic tumors
GanglioneuromaGanglioneuroblastomaNeurofibroma
Dilation of blood vessels
Vasodilatory hypotension
Severe hypotension
Non-modifiable Risk Factors Gender: M 1: F3 (Adults); M1:F1 (Children) MEN Family History; Somatic mutations of MEN1 gene Age: 40-50 years old
Secretion of calcitrophic peptide
Neuroendocrine islet cell tumor of the pancreas
Primordial neural crest cells
CNS
Coincidental MEN accompanied by
hyperparathyroidism
↑ Blood flow to the corpora cavernosa
Priapism in males
Penile erection
Hypercalcemia
A. Pathophysiology (Book-based) Schematic Diagram
Idiopathic
GIT CV GUT
Profound glycogenolytic effect
S/sx of DM
Steatorrhea
↑ Glucose intolerance
Hyperglycemia
LipolysisRegulation of neuronal activity, differentiation,
and survival in SNS
Embryologic endoderm
VIPoma
Paravertebral mass on chest radiograph
Malignant
Benign
Hepatomegaly
Metastasis commonly in the liver

Facial flushing
Abdominal distention; bloating;
Abdominal pain
Massive secretion of water and
electrolytes (Na, K, Mg, Cl)
Stimulation of cAMP
Secretroy, non-fasting, large
volume diarrhea (dilute tea in appearance)
Bronchial smooth muscle contraction
Colonic dilatation
Dilation of intestinal smooth
muscle & peripheral blood
vessel
Stimulate bicarbonate
secretion
Gallbladder Intestine
↑ Intestinal motility
Dilation of gallbladder
Hypochlorhydria/ achlorhydria
A
Relaxation of lower esophageal sphincter,
gastric fundus, anal sphicter
Stimulate alkaline pancreatic juice
secretion
GIT
Inhibits secretion by exocrine
pancreas and biliary system
Inhibits smooth muscle contraction
Inhibits histamine release &
pentagastrin-stimulated acid
secretion
Vasodilatory effect
Renal failure
Retention of Cl by kidneys
Bicarbonate wasting
Hyperchloremic metabolic acidosis
Hypomagnesemia Tetany
Hypochlorhydria/ achlorhydria;
hypercalcemia
Electrolyte imbalance
Hypokalemia
Large distended
gallbladder
Gallbladder relaxation

Cardiac arrest
Dehydration & weight loss; poor
skin turgor
↑ Conduction of nerve impulses
Fatigue, paresthesia, hyporeflexia,
irritability
Ventricular fibrillation
Hypokalemia
↑ Resting membrane potential
↓ K gradient b/w ICF & plasma
Reabsorb water and Na in kidney; K is
eliminated
↑ Excitability
Anorexia, abdominal distention,
constipation
Slowed smooth muscle contraction
↑ In transmembrane
potential
A
Hypotension & slow peak
pulse
↓ Myocardial contraction
↑ Cellular excitability
Dysrythmia
Depressed & prolonged ST segment, depressed
& inverted T wave, prominent U wave
Prolonged myocardial
repolarization function
Severe hypokalemia
Shallow respirations,
shortness of breath, apnea
Respiratory arrest
Deterioration of respiratory muscular
contractionMuscle
weakness & leg cramps, nephrosis
Tachycardia
Progression of hypokalemia
Vomiting, ileus, urinary retention
Extreme smooth muscle slowing
Dysphasia, confusion, depression,
convulsions, areflexia, coma
Altered nerve conduction
Paralysis
Inhibits the kidney to concentrate urine
Polyuria, nocturia, ↓ plasma osmolality
Baroreceptors stimulate SNS
ADH & aldosterone secretion
↑ Na levels in blood
Increase peripheral vasoconstriction
Osmoreceptors triggers thirst mechanism
Progression of hypokalemia
Progression of hypokalemia
Movement of fluid from the periphery to
the circulation
Excess fluid loss & volume depletion
Slowed skeletal muscle
contraction

Synthesis of the Disease (Book-based)
1. General Description of Vipoma
Vipomas are endocrine tumors that secrete excessive amounts of VIP, which causes a
distinct syndrome characterized by large-volume of watery diarrhea, hypokalemia, and
dehydration. This syndrome is also called Verner-Morrison syndrome, pancreatic
cholera, or WDHA syndrome fro watery diarrhea, hypokalemia, and achlorhydria, which
some patients develop. The mean age of patients is 49 years; however, it can occur in
children. (Kasper, et. al., 2005).
VIPomas in adults are usually neuroendocrine islet cell tumors of the pancreas
that produce high amounts of VIP. Other secreted hormones may include secreted
gastrin and pancreatic polypeptide (Ferry, 2008). The cells in pancreatic endocrine
neoplasms are termed amine precursor uptake and decarboxylation (APUD) cells
because they have a high amine content, are capable of amine precursor uptake, and
contain an amino acid decarboxylase. It is believed that these cells develop from
embryologic endoderm (Ong, 2009).
In children and adolescents, VIP is produced mainly by ganglioneuromas,
ganglioneuroblastomas, neurofibromas, or other tumors in the adrenal area (most
common location) (Ferry, 2008). Neuroblastic tumors are derived from primordial neural
crest cells (Kumar, et. al., 2010).
VIP is a 28-amino-acid peptide that is an important neurotransmitter ubiquitously
present in the central nervous system (ie, hypothalamus, hippocampus, cortex).,
respiratory system, urogenital tracts, and gastrointestinal tract. Its known actions include
stimulation of small-intestinal chloride secretion and effects on smooth-muscle
contractility, inhibition of acid secretion, and vasodilatory effects which explain most
features of the clinical syndrome (Kasper, et. al., 2005). Vasoactive intestinal peptide
(VIP) is a peptide hormone with a number of important functions in the regulation of

neuronal activity, differentiation, and survival, particularly in the sympathetic nervous
system. It probably functions as a neuroacrine agent, and its presence in neurons with
processes extending to mucosal cells, smooth muscle, and blood vessels suggests that
VIP affects local secretion, motility, and blood flow (Greenspan and Gardner, 2001).
The most important physiologic actions of VIP in the gastrointestinal tract are
relaxation of vascular and nonvascular smooth muscles specifically relaxation of the
lower esophageal sphincter, receptive relaxation of gastric fundus, relxation of the anal
sphincter, and relaxation of gallbladder. VIP inhibits pentagastrin and histamine-
stimulated gastric acid and pepsin secretion. It stimulates lipolysis, glycogenolysis, and
secretion by the small intestine and pancreas. It stimulates pancreatic bicarbonate
secretion (Greenspan and Gardner, 2001). These effects work together to increase
motility (Bergram RA, 2010). VIP is a potent stimulator of adenosine 3',5'-cyclic
phosphate (cAMP) production by the gut. Thus, overproduction leads to massive
secretion of water and electrolytes, mainly potassium (Ferry, 2008). The action of VIP is
mediated by stimulatory G proteins and activation of adenylyl cyclase Additionally, VIP
increases gut blood flow and is one of the many factors responsible for penile erection.
This causes priapism in males (Greenspan and Gardner, 2001).
The principal symptoms are large-volume diarrhea (100%) severe enough to
cuase hypokalemia (80 to 100%), dehydration (83%), hypochlorhydria (54 to 76%), and
flushing (20%). The diarrhea is secretory in nature, persists during fasting, and is almost
always >1 L/d and >3 L/d in 70% (Greenspan and Baxter, 1994). The diarrhea is caused
by the effects of excessive VIP to increase the motility (Bergram RA, 2010) and the
overproduction of cAMP that leads to massive secretion of water and electrolytes (Ferry,
2008). Steatorrhea (16%) is caused by lipolysis, and the increased stool volume is due
to increased excretion of sodium and potassium, which with the anions, account for the
osmolality of the stool (Kasper, et. al., 2005). Clients frequently have hyperglycemia (25

– 50%) due to the profound glycogenolytic effect of high portal vein VIP on the liver
(Vinik, 2004) and hypercalcemia (25 – 50%). The cause of hypercalcemia is not clear,
but it may relate to dehydration, electrolyte imbalance due to diarrhea, coincidental MEN
accompanied by hyperparathyroidism, or secretion by the tumor of calcitrophic peptide.
Hypomagnesemia also results secondary to diarrhea which is manifested by tetany. The
vasodilatory effects of VIP cause gallbladder distention, facial flushing, dilation of blood
vessels in the cardiovascular system which causes vasodilatory hypotension, and
dilation of intestinal smooth muscle. Dilation of intestinal muscle causes colonic
dilatation which manifests abdominal distention, bloating, and abdominal pain. Severe
metabolic acidosis may be present due to severe bicarbonate wasting (Vinik, 2004).
When excess bicarbonate is lost from the body, the kidneys retain chloride causing
hyperchloremic metabolic acidosis (Black and Hawks, 2005). Death may result from
renal failure or cardiac arrest caused by volume depletion and acidosis (Ferry, 2008).
Approximately 60-80% of VIPomas are malignant and have metastasized at the time of
diagnosis. Metastasis occurs most frequently in the liver, but it may also occur in the
lymph nodes, lung, or kidneys (Tung, 2008).
With dehydration, ADH and aldosterone secretion increase to reabsorb water
and sodium in the kidney. The baroreceptors sense low blood pressure, and the
sympathetic nervous system is stimulated to increase peripheral vasoconstriction and
the heart rate. Vasoconstriction moves fluids from the periphery (legs, gastrointestinal
tract) into circulation. Increasing sodium levels in the blood is also sensed by the
osmoreceptors in the hypothalamus, which triggers thirst mechanism (Black and Hawks,
2005). Aldosterone secretion aggravates hypokalemia since it excretes potassium
(Seeley, et. al., 2007).
The remaining sysmptoms associated with VIPomas are secondary to
hypokalemia (Ong, 2004). When plasma potassium levels decrease, a decrease in

potassium gradient occurs between ICF and the plasma. The decreased gradient
causes the resting membrane potential to increase, thus increasing excitability.
Therefore, cell membranes are more responsive to stimuli. In hypokalemia, muscle
contraction is slowed. Slowed smooth muscle contraction leads to early GI
manifestations, which include anorexia, abdominal distention, and constipation. Slowed
skeletal muscle contract results in muscle weakness and leg cramps. Increased
conduction of nerve impulses secondary to an increase in the transmembrane potential
leads to neurologic manifestations of fatigue, paresthesias, hyporeflexia, and irritability
(Black and Hawks, 2005).
With severe hypokalemia, ECG changes may occur. The depressed and
prolonged ST segment, depressed and inverted T wave, and prominent U wave are due
to the prolongation of myocardial repolarization. Dysrhythmias are common because of
increased cellular excitability. Hypokalemia also leads to a decrease in myocardial
contraction, which is manifested as hypotension and a slow, weakened pulse. Potassium
levels of less than 2.5 mEq/L increase the risk of ventricular fibrillation and cardiac
arrest. Pulmonary manifestations of shallow respirations, shortness of breath, and
apnea, culminating in respiratory arrest, are also from progressive deterioration of
respiratory muscular contraction (Black and Hawks, 2005).
The progressive neurologic consequences of altered nerve conduction are
manifested as dysphasia, confusion, depression, convulsion, areflexia, and coma.
Extreme smooth muscle slowing leads to vomiting and ileus as well as urinary retention.
Skeletal muscle weakness may progress to paralysis. Hypokalemia also inhibits the
ability of the kidney to concentrate urine, which leads to polyuria, nocturia, and a
decreased plasma osmolality (Black and Hawks, 2005).
2. Non-modifiable/ Modifiable Factors (Book-Based)
Non-modifiable Factors
Idiopathic. The etiology of sporadic pancreatic endocrine tumors in largely unknown.
Risk factors have not been identified, but carcinogens may be involved, because
pancreatic endocrine neoplasms can be induced in rats treated with streptozotocin in
combination with nicotinamide. (Fletcher, 2007).
Family history of Multiple Endocrine Neoplasia Type 1. A family history of Multiple
Endocrine Neoplasia type 1 and similar syndromes can also increase one’s risk
(http://www.knowcancer.com/oncology/vipoma/). Multiple Endocrine Neoplasia Type
1hyperfunctioning tumors in all 4parathyroid glands, pancreatic islets (eg, gastrinoma,
insulinoma, glucagonoma, vasoactive intestinal peptide tumor [VIPoma], pancreatic
polypeptide–producing tumor [PPoma]), and the anterior pituitary (eg, prolactinoma,
somatotropinoma, corticotropinoma, nonfunctioning tumors) (Ferry, 2008).
Somatic point mutations on chromosome 11 of the MEN1 gene have been
discovered in sporadic VIPomas and VIPoma cases associated with MEN type 1 (Ferry,
2008).
Age: When VIPomas occur in adults, they appear most commonly between the ages of
40 and 50 years and they usually develop in the pancreas. In children, VIPomas more
commonly arise in or near the adrenal gland
(http://www.novartisoncology.us/education/diseases-conditions/oncology/vip-tumors.jsp).

Gender: Male-to-female ratio in children is approximately 1:1, compared with 1:3 in
adults (Ferry, 2008).
3. Signs and Symptoms (Book-Based)
Increased Serum VIP test. Increased due to secretions of excessive amounts of
VIP by the endocrine tumor. Determined during periods of ongoing diarrhea, the
level of serum VIP in clients with Verner-Morrison syndrome ranges from 225-
1850 pg/mL. The normal serum VIP level is less than 170 pg/mL (Ong, 2008).
Hypokalemia. VIP is a potent stimulator of adenosine 3’,5’-cyclic phosphate
(cAMP) production by the gut. Thus, overproduction leads to massive excretion
of water and electrolytes, mainly potassium.
Hypercalcemia. May relate to dehydration, electrolyte disturbances secondary to
diarrhea, coincidental MEN accompanied by hyperparathyroidism, or secretion
by the tumor of a calcitrophic peptide.
Hypomagnesemia. Caused by the massive secretion of water and electrolytes
from the stimulation of adenosine 3’,5’-cyclic phosphate (cAMP) production by
VIP.
Tetany. A manifestation of hypomagnesemia.
Severe hypotension. VIP causes vasodilatory effects throughout the body. In
the cardiovascular system, it causes dilation of blood vessels thereby leading to
vasodilatory hypotenstion. Excessive amounts of VIP causes further vasodilatory
hypotension which results to severe hypotension.
Hyperglycemia and signs and symptoms of DM. Excessive amounts of VIP
causes profound glycogenolytic effect of high portal vein VIP on the liver causing
hyperglycemia, increasing glucose tolerance and the development of signs and
symptoms of Diabetes Mellitus.

Hypochlorhydria/ achlorhydria. Hypochlorhydria results from the direct gastric
acid inhibitory effect of VIP. VIP inhibits histamine release and pentagastrin-
stimulated acid secretion. Also, hypochlorhydria results from excessive secretion
of water and electrolytes due to stimulation of adenosine 3’,5’-cyclic phosphate
(cAMP) production by VIP.
Colonic dilatation. The vasodilatory effect of VIP causes dilation of intestinal
smooth muscle and peripheral blood vessel thus causing colonic dilatation.
Abdominal distention, bloating, abdominal pain. Because of dilation of
intestinal smooth muscle , colonic dilatation occurs which causes abdominal
distention, bloating, and abdominal pain.
Secretroy, non-fasting, large volume diarrhea (dilute tea in appearance).
VIP causes dilation of intestinal smooth muscle, inhibits smooth muscle
contraction of the gallbladder and intestine, inhibits secretion by exocrine
pancreas and biliary system, ihnhibits histamine release and pentagastrin-
stimulated acid secretion, and stimulate alkaline pancreatic juice secretion to
increase intestinal motility. Increase in intestinal motility and excessive
stimulation of cAMP which causes massive secretion of water and electrolytes.
Both intestinal motility and massive secretion of water and electrolytes cause the
secretory diarrhea in VIPoma.
Dehydration & weight loss; poor skin turgor. Due to secretory large volume
diarrhea brought by the effects of excessive amouts of VIP, the body losses body
fluids and leads to volume depletion.
Thirst. Excess fluid loss triggers ADH and aldosterone secretion to reabsorb
water and sodium in the kidney. Thereby increasing sodium levels in the blood
and in turn trigger the osmoreceptors to stimulate thirst.

Tachycardia. The baroreceptors sense low blood pressure, and the smypahtetic
nervous system is stimulated to increase peripheral vasoconstriction and heart
rate.
Fatigue, paresthesia, hyporeflexia, irritability. Increased conduction of nerve
impulses secondary to an increase in the transmembrane potential leads to
neurologic manifestations of fatigue, paresthesias, hyporeflexia, and irritability.
Dysphasia, confusion, depression, convulsions, areflexia, coma. The
progressive neurologic consequences of altered nerve conduction are
manifested as dysphasia, confusion, depression, convulsion, areflexia, and
coma.
Muscle weakness & leg cramps, nephrosis. Slowed skeletal muscle contract
results in muscle weakness and leg cramps.
Paralysis. Skeletal muscle weakness worsens resulting to paralysis.
Anorexia, abdominal distention, constipation. Hypokalemia causes slowed
muscular contraction among the smooth muscles of the gastrointestinal tract.
Vomiting, ileus, urinary retention. Due to progression of hypokalemia, there is
an extreme muscle slowing of the smooth muscle contraction.
Polyuria, nocturia, ↓ plasma osmolality. Hypokalemia also inhibits the ability of
the kidney to concentrate urine, which leads to polyuria, nocturia, and a
decreased plasma osmolality.
Shallow respirations, shortness of breath, apnea. Pulmonary manifestations
of shallow respirations, shortness of breath, and apnea, culminating in respiratory
arrest, are also from progressive deterioration of respiratory muscular
contraction.
Depressed & prolonged ST segment, depressed & inverted T wave,
prominent U wave. Due to the prolongation of myocardial repolarization.

Hypotension & slow peak pulse. Hypokalemia also leads to a decrease in
myocardial contraction, which is manifested as hypotension and a slow,
weakened pulse.
Dysrythmia & Ventricular fibrillation. Dysrhythmias are common because of
increased cellular excitability. Potassium levels of less than 2.5 mEq/L increase
the risk of ventricular fibrillation and cardiac arrest.
Large distended gallbladder. Develop from the vasodilatory effects of
vasoactive intestinal peptide in the gallbladder.
Steatorrhea. It is caused by lipolysis effect of vasoactive intestinal peptide.
Chest radiography may reveal a paravertebral mass (Ferry, 2008).
Hepatomegaly may be detected if liver metastasis has occurred (Tung, 2008).

B. Pathophysiology (Client-Centered)
Produce excessive amounts of VIP: ↑ serum
VIP
Schematic Diagram
GIT
VIPoma
Mass like opacity with lobulated margins in left retrocardiac area on CXR
(03.26.10).
Benign
Ganglioneuroma on biopsy (02.04.10)
Primordial neural crest cells
Non-modifiable Risk Factors Gender: Female Idiopathic

Abdominal enlargement (01.21.10).
Abdominal pain (03.26 - 27.10).
Slightly tympanic abdomen upon
percussion (03.24.10).Massive secretion
of water and electrolytes (Na, K,
Mg, Cl)
Stimulation of cAMP
Watery diarrhea: 3-4x/ day (03.24
to 28. 10); Watery consistency on
stool examination (03.27.10)
Bronchial smooth muscle contraction
Dilation of intestinal smooth
muscle & peripheral blood
vessel
Stimulate bicarbonate
secretionGallbladder relaxation
Gallbladder Intestine
↑ Intestinal motility
A
Relaxation of lower esophageal sphincter,
gastric fundus, anal sphicter
Stimulate alkaline pancreatic juice
secretion
GIT
Inhibits secretion by exocrine
pancreas and biliary system
Inhibits smooth muscle contraction
Inhibits histamine release &
pentagastrin-stimulated acid
secretion
Vasodilatory effect
Decreased bicarbonate (16.4) in ABG (01.30.10).
Bicarbonate wasting
Hyponatremia: 133.7 (02.03.07).
Electrolyte imbalance
Hypokalemia (03.24 to 28. 10). Decreased urine
potassium: 21.9 mmol/L (02.05.10).
Hydrops of gallbladder on abdominal UTZ
(01.20.10).
Dilation of gallbladder
Large distended
gallbladderModerate gaseous
distention of intestine on CT
scan of the chest (02.01.10).
Colonic dilatation

Hyperthermia (03.26.10).
Weight loss (03.24.10).
Hypokalemia
↑ Resting membrane potential
↓ K gradient b/w ICF & plasma
Reabsorb water and Na in kidney; K is
eliminated
↑ Excitability
Loss of appetite
(03.24.10).
Slowed smooth muscle contraction
Slowed skeletal muscle
contraction
A
Presence of T-wave flattening on lead 2, U wave on Leads V4, V5, V6 on ECG ((03.25.10).
Prolonged myocardial
repolarization function
Severe hypokalemia
Appears weak (03.24.10).
Pale palpebral conjunctiva, lips,
nail beds (03.24.10).
Mild adynamic ileus from abdominal x-
ray (01.25.10).
Extreme smooth muscle slowing
Baroreceptors stimulate SNS
ADH & aldosterone secretion
↑ Na levels in blood
Increase peripheral vasoconstriction
Osmoreceptors triggers thirst
(03.24.10).mechanism
Progression of hypokalemia
Movement of fluid from the periphery to
the circulation
Excess fluid loss & volume depletion

Synthesis of the Disease (Client-centered)
1. General Description of Vipoma
Vipomas are endocrine tumors that secrete excessive amounts of VIP, which causes a
distinct syndrome characterized by large-volume of watery diarrhea, hypokalemia, and
dehydration. The etiology of VIPoma is not known. Male-to-female ratio in children is
approximately 1:1. This ration gives equal incidence of VIPoma in males and females.
In the case of Vipsy, VIP is produced mainly by the ganglioneuroma present in
the left paravertebral area behind the posterior lips of the diaphragm. Ganglioneuroma is
a neuroblastic tumor derived from primordial neural crest cells.
The presence of ganglioneuroma causes secretion of excessive amounts of VIP
which causes the WDHA syndrome. The main system affected by VIPoma is the
digestive system. With an increased serum levels of vasoactive intestinal polypeptide,
it’s normal action is exaggerated. Vasointestinal polypeptide increases the intestinal
motility of the digestive system by (1) vasodilation of intestinal smooth muscle,
gallbladder and peripheral blood vessel, (2) inhibiting the smooth muscle contraction of
gallbladder and intesitines, (3) inhibits secretion by exocrine pancreas and biliary
system, (4) inhibits histamine release and pentagastrin acid stimulated acid secretion,
and (5) stimulates alkaline pancreatic juice secretion. VIP also causes excessive
stimulation of of adenosine 3',5'-cyclic phosphate (cAMP) production which causes
massive secretion of water and electrolytes. Both an increase in intestinal motility and
massive secretion of water and electrolytes cause the watery diarrhea of the client.
There is excess fluid and volume depletion causing stimulation of barorecptors to
increase peripheral circulation by moving fluid from the periphery to the circulation.
Volume depletion also caused dehydration and weight loss. With volume depletion,
antidiuretic hormone and aldosterone secretion is secreted to reabsorb water and
sodium in the kidney to compensate to the excess fluid loss causing increase in sodium

levels in the blood which causes the osmoreceptors to trigger thirst. Aldosterone also
contributes to elimination of potassium in the body.
Due to excessive secretion of electrolytes, hyponatremia and hypokalemia
developed. Hypokalemia causes a decrease in potassium gradient occurs between ICF
and the plasma. The decreased gradient causes the resting membrane potential to
increase, thus increasing excitability. Therefore, cell membranes are more responsive to
stimuli. In hypokalemia, muscle contraction is slowed. Slowed smooth muscle
contraction leads loss of appetite. Progression of hypokalemia causes extreme muscle
slowing leading to ileus. Slowed skeletal muscle contract results in muscle weakness.
With severe hypokalemia (2.04), ECG changes occurred. Prolongation of myocardial
repolarization caused a presence of T-wave and U-wave on the ECG.
2. Non-modifiable/ Modifiable Factors (Client-centered)
Non-modifiable Factors
Idiopathic. The exact cause is not known. There is no family health history of
malignancy which cannot be attributed to a possible occurrence of MEN among the
family members.
Gender: Vipsy is a female and she has an equal chance with a male to develop the
sporadic endocrine tumor.
3. Signs and Symptoms (Client-centered)
Increase in serum VIP >400. Increase in serum VIP is due to the presence of
ganglioneuroma, a tumor that secretes excessive amounts of vasoactive
intestinal polypeptide in the blood, located on the left paravertebral area behind

the posterior lips of the diaphragm. The serum VIP levels of Vipsy was >400 pg/
mL.
Hydrops of gallbladder on abdominal UTZ (01.20.10). Excessive amounts of
vasoactive intestinal polypeptide causes excessive action of VIP. A known action
of VIP is its vasodilatory effect which causes over distention of the gallbladder.
Also, VIP inhibits smooth muscle contraction of the gallbladder leading to
galldbladder relaxation. Both over distention and relaxation of gallbladder caused
Hydrops of the gallbladder.
Abdominal enlargement (01.21.10); Abdominal pain (03.26 - 27.10). Because
of the vasodilatory effect of VIP, there is too much dilation of the intestinal
smooth muscle causing distention of the intestine. Also, development of hydrops
of the gallbladder caused the abdominal enlargement.
Mild adynamic ileus from abdominal x-ray (01.25.10). Excessive amounts of
VIP lead to the watery diarrhea of the client and massive loss of electrolytes
specifically potassium. Hypokalemia causes a slowed smooth muscle contraction
in the gastrointestinal wall causing a decrease in peristalsis.
Decreased bicarbonate (16.4) in ABG (01.30.10). Increase in VIP causes
excessive stimulation of the alkaline pancreatic juice secretion. This causes
stimulation of bicarbonate secretion causing bicarbonate wasting. Bicarbonate
wasting also is due to massive secretion of electrolytes through the stool which
causes a decreased in bicarbonate levels.
Moderate gaseous distention of intestine on CT scan of the chest
(02.01.10). This is due to the dilation of the intestinal smooth muscle by the
vasoactive intestinal polypeptide.
Hyponatremia: 133.7 (02.03.07). The stimulation of cAMP by VIP results in
massive secretion of water and electrolytes through the gastrointestinal system.

Ganglioneuroma on biopsy: benign (02.04.10). The cause of the development
of ganglioneuroma is idiopathic.
Decreased urine potassium: 21.9 mmol/L (02.05.10). Excessive amounts of
circulating VIP results to massive secretion of electrolytes specifically potassium.
Hypokalemia develops due to excessive secretion of potassium and no
replacement is done which also cause a decrease in urine potassium level.
Watery diarrhea: 3-4x/ day (03.24 to 28. 10); Watery consistency on stool
examination (03.27.10). This is due to the increase in intestinal motility and
stimulation of cAMP by the vasoactive intestinal polypeptide.
Weight loss (03.24.10). Because of frequent loss of fluids through the stools,
there is decrease in circulating blood volume which can be easily measured by
the weight of the client. A decrease in weight indicates excess fluid loss.
Thirst (03.24.10). Excess fluid loss triggers ADH and aldosterone secretion to
reabsorb water and sodium in the kidney. Thereby increasing sodium levels in
the blood and in turn trigger the osmoreceptors to stimulate thirst.
Pale palpebral conjunctiva, lips, nail beds (03.24.10). Decrease in circulating
blood volume causes an increase in peripheral vasoconstriction. This effect
moves fluid from the periphery into the circulation.
Loss of appetite (03.24.10). Hypokalemia causes slowed muscular contraction
among the smooth muscles of the gastrointestinal tract.
Slightly tympanic abdomen upon percussion (03.24.10). Due to the
vasodilatory effects of vipoma which causes the intestinal walls to dilate.
Appears weak (03.24.10). Hypokalemia causes a slowed skeletal smooth
muscle contraction. Hypokalemia is due to the secretory watery diarrhea effect of
excessive amounts of vasoactive intestinal peptide in the serum.

Hypokalemia (03.24 to 28. 10). VIP is a potent stimulator of adenosine 3’,5’-
cyclic phosphate (cAMP) production by the gut. Thus, overproduction leads to
massive excretion of water and electrolytes, mainly potassium. The client had
three to four watery stools per day causing an excessive loss of potassium in the
stool.
Presence of T-wave flattening on lead 2, U wave on Leads V4, V5, V6 on
ECG ((03.25.10). Due to the prolongation of myocardial repolarization caused by
decreased in potassium levels of the client.
Hyperthermia (03.26.10). Frequent watery diarrhea from the effect of excessive
vasoactive intestinal peptide causes depletion in the fluid volume which causes
dehydration.
Mass like opacity with lobulated margins in left retrocardiac area on Chest
x-ray (03.26.10). Indicates the presence of a tumor which is in congruence with
the previous chest x-ray done on her first hospitalization.

V. THE PATIENT AND HER CARE
A. MEDICAL MANAGEMENT
a. IVFs, BT, NGT Feeding, Nebulization, TPN, Oxygen Therapy, etc.
Medical Management
Treatment
Date Ordered
Date (s) Performed
Date changed/ D/C
General DescriptionIndication (s) or Purpose
(s)
Client’s response to
treatment
D5 0.33 NaCl 500 cc x 44-
45 µgtts/min for 8 hours
DO: 03/ 24/10
DP: 03/ 24/ 10
DC: 03/ 24/ 10
D5 is a nutrient solution,
which contains some form
of carbohydrate (dextrose)
and water. 0.3 NaCl is a
hypotonic solution used to
provide free water and
treat cellular dehydration.
Water from D5 is supplied
for fluid requirements and
carbohydrate for calories
and energy. It also
prevents dehydration and
ketosis. 0.3 NaCl promotes
diuresis. Promotes waste
elimination by the kidneys.
The client had good
hydration status. The client
has normal urine output.D5 0.33 NaCl 500 cc x 69
µgtts/min for 6 hours
DO: 03/ 24/10
DP: 03/ 24/ 10
DC: 03/ 24/ 10
D5 IMB 500 cc x 36-37
µgtts/min
DO: 03/ 24/10
DP: 03/ 25/ 10
DC: 03/ 25/ 10
It is a hypertonic solution.
Hypertonic solutions draw
fluid out of the intracellular
and interstitial
To expand vascular
volume lost from diarrhea.
The client maintained a
good hydration status,
however, potassium levels
did not increase.

compartments into the
vascular compartment
expanding vascular
volumes.
D5 0.33 NaCl 71.2 cc
+ KCl 2.3 cc = 74 cc to run
for 2 hours
DO: 03/ 25/10
DP: 03/ 25/ 10 (8 AM)
DC: 03/ 25/ 10
D5 is a nutrient solution,
which contains some form
of carbohydrate (dextrose)
and water. 0.3 NaCl is a
hypotonic solution used to
provide free water and
treat cellular dehydration.
To prevent dehydration
and to increase potassium
levels.
The client’s hydration
status was maintained.
The client’s potassium
level increased.
DO: 03/ 25/10
DP: 03/ 25/ 10 (5:05 PM)
DC: 03/ 25/ 10
D5 0.33 NaCl 72.5 cc
+ KCl 1.5 cc = 74 cc to run
every 2 hours
DO: 03/ 25/10
DP: 03/ 25/ 10 (8 AM)
DC: 03/ 25/ 10
DO: 03/ 25/10
DP: 03/ 25/ 10 (7:30 PM)
DC: 03/ 25/ 10

Nursing Considerations:
Prior to:
1. Prepare the equipment
6. Check Doctor’s order
7. Acquaint the patient with the requirement and need of
IV transfusion
8. Select a suitable vein to permit easier access to a
vessel
9. Select a appropriate needle suitable for type and
location of infusion
10. Clean the area of insertion
11. Use strict aseptic technique
12. Identify the client
13. Assess vital signs for baseline data
14. Assess skin turgor, allergy to tape
15. Check the status or veins to determine appropriate
venipuncture site
During:
1. Use the smallest gauge needle possible.
2. Check for patency of the tubing
3. Spike the solution container
4. Cleanse the fluid to be given, make sure it is the same
with the prescribed fluid.
5. Partially fill the drip chamber gently with solution.
6. Select a suitable vein for venipuncture
7. Dilate the vein
8. Put on clean gloves and clean the venipuncture site.
9. Check for line and infusion integrity
After:
1. Label the IVF (name, date started, number)
2. Ensure appropriate infusion flow.
3. Regulate flow rate as ordered

4. Adjust the rate of fluids appropriate to the needs f the
patient as ordered. If there is any question with the flow
rate ordered, check with the physician who gave the
order.
5. Monitor IV flow and patient’s response
6. Monitor patient for evidence of IV infiltrations
7. Check for presence of air in the tubing, if air is present,
remove immediately
8. Check for the patency of the line always.
9. Check for IV insertion for phlebitis frequently
10. Document relevant data.

b. Drugs
Name of Drug
Date
Ordered
Date Taken/
Given
Date
Changed/
D/C
Route of
Administration
Dosage and
Frequency of
administration
General Action
Functional
Classification
Mechanism of Action
Indication(s)
Client’s
response to
the
medication
with actual
side effect
Nursing responsibilities
Generic Name:
Racecadotril
Brand Name:
Hidrasec
DO: 03/ 24/
10
DG: 03/ 24/
10
DC: 03/ 26/
10
Hidrasec 10 mg/
sachet, 2 sachet
three times a
day
General Action:
Antidiarrheal
Functional Classification:
Antidiarrheal
Mechanism of Action:
Racecadotril is an
inhibitor of
enkephalinase, the
Adjunct to oral
or parenteral
rehydration in
treatment of
acute watery
diarrhea in
infants and
children
The client’s
stool was still
watery until
discharge
however, it
contains small
amounts of soft
stool and the
amount was
decreased. The
1.May be taken with or without
food.
2.Monitor for signs and symptoms
of side effects.
3.Store below 30oC.

enzyme responsible for
breaking down
enkephalins. It is a
selective but reversible
inhibitor and protects
endogenous enkephalins
which are physiologically
active in the digestive
tract.
frequency of
stool fluctuates
since Vipsy
does not like
the taste of
Hidrasec.
Generic Name:
Ampicillin
Brand Name:
Ampicin
DO: 03/ 24/
10
DG: 03/ 24/
10
IV, 500 mg/ vial,
300 mg SIVP
every 6 hours
ANST
General Action:
Anti-infective
Functional Classification:
Penicillin
Mechanism of Action:
Inhibits cell-wall synthesis
during bacterial
For treatment of
infection.
Infection was
treated.
Assessment:
1. Assess client’s condition before
starting therapy and regularly
thereafter to monitor drug’s
effectiveness.
2. Be alert for advers reactions
and drug interactions.

multiplication.
Evaluation:
1. Evaluate the effectiveness of
drug and client’s respond to
therapy.
Generic Name:
Carbocisteine
Brand Name:
Solmux Syrup
DO: 03/ 25/
10
DG: 03/ 25/
10
½ tsp PO three
times a day
General Action:
Cough and cold
Preparations
Functional Classification:
Mucolytic
Mechanism of Action:
Carbocisteine, a
derivative of
acetylcysteine, is a
mucoregulating agent.
Its major action is
thought to be on the
metabolism of mucus-
Relief of cough
associated with
excessive and
tenacious
sputum or
phlegm
The client was
relieved from
cough.
1. Store at temperature not
exceeding 30oC.
2. Should be administered with
food.

producting cells. The
mucus produced under
the influence of
carbocisteine has an
increased content of
the less viscous
sialomucin and a
reduced content of the
highly viscious
fucomucin. Sialomucins
influence the
rheological properties
of mucus and may also,
through the inhibition
of kinins reduce or
prevent bronchial
inflammation and
bronchospasm.
Generic Name: DO: 03/ 26/ PO, 1.2 ml every General Action: Relief of fever Vipsy’s fever 1. Take and record temperature

Paracetamol
Brand Name:
Tempra drops
10
DG: 03/ 26/
10
4 hours as
needed for fever
Analgesics (Non-opioid)
and Antipyretics
Mechanism of Action:
Tempra is
acetaminophen
(paracetamol), a safe and
effective analgesic-
antipyretic. It is a not
salicylate. It contains no
phenacetin or caffeine. It
has no effect on
prothrombin
time. Tempra is
particularly valuable for
use in patients who do
not tolerate aspirin well
because it is less likely to
was decreased
from 37.7 to
36.3.
2. Administer with food or full
glass of water
3. Can be taken with food or an
empty stomach
4. Monitor for patient’s
temperature
5. Advise patient to increase oral
fluid intake

cause GI distress.
Generic Name:
Dicycloverine
Hydrochloride
Brand Name:
Relestal
DO: 03/ 27/
10
DG: 03/ 27/
10
PO, 2.5 ml every
8 hours
General Action:
Antispasmodic
Functional Classification:
Anticholinergic
Mechanism of Action:
Dicycloverine HCl acts
as a nonselective
smooth muscle relaxant
by: 1) A specific
anticholinergic effect at
the acetylcholine-
receptor sites; and 2)
Acting directly on the
bradykini- and
For the
treatment of
functional
disturbances of
gastrointestinal
motility
eg, irritable
bowel
syndrome and
renal and
biliary colic
The client did
not complain of
stomach pain
after the
administration
of Relestal.
1. May be taken with or without
food.
2. Keep patient in a cool
environment. Fever and heat
stroke due to decreased sweating
may be experienced in the
presence of high environmental
temperature.

histamine- induced
spasm. Dicycloverine
has little or no effect on
gastric secretion.
Generic Name:
Potassium Chloride
Brand Name:
Kalium Durule
DO: 03/ 25/
10
DG: 03/ 25/
10
DC: 03/ 28/
10
Incorporation of
potassium
chloride in IVF
to run in infusion
General Action:
Potassium
Functional Classification:
Electrolyte, mineral
replacement
Mechanism of Action:
Needed for adequate
transmission of nerve
impulses and cardiac
contraction, renal
function, intracellular ion
For hypokalemia The client’s
potassium level
decreased from
3.47 to 3.18
indicating that
the dosage is
not enough.
The client’s
potassium level
increased from
3.18 to 3.49.
Assess:
1. ECG for peaking T waves,
lowered R, depressed RST,
prolonged P-R interval, widening
QRS complex, hyperkalemia; drug
should be reduced or discontinued.
2. I&O ration; watch for decreased
urinary output; notify prescriber
immediately.
3. Cardiac status: rate, rhythm.
Administer:
PO route
1. Do not break, crush, or chew
enteric products.
DO: 03/ 27/
10
DG: 03/ 27/
10
DC: 03/ 28/
10
PO, 750 mg/
tab, 1 tab once a
day
DO: 03/ 28/
10
PO, 750 mg/
tab, 1 tab BID

DG: 03/ 28/
10maintenance. 2. With or after meals.
IV route
1. Through large-bore needle to
decrease vein inflammation; check
for extravasation
2. In large vein, avoiding scalp Nursing Responsibilities:
Prior to:
1. Check the written medication order for completeness. It should include the drug name, dosage, frequency, and duration of the
therapy.
2. Check if IV in.
3. Check to see if there are any special circumstances surrounding administration of the dose to the patient.

4. Be certain that you know the expected action, safe dosage range, special instructions for administration and adverse effects
associated with drug orders.
5. Prepare the necessary equipment.
6. Wash your hands.
7. Check the label on the medications three times before administering any drug.
8. Prepare the dosage as ordered.
9. Explain the procedure to the patient. The action of the drug and its side effects.
During:
10. Identify the patient.
11. Identify if the patient expresses any doubt about the medication; always recheck the order, drug label and dosage on the
medication card.
12. For oral meds do special regulation and precaution to avoid or prevent aspiration.
After:
13. Following administration, be certain that the patient is comfortable, then immediately record the procedure.
14. Instruct the patient to report signs of superinfection and allergy.
15. Inspect IV insertion sites for sign of phlebitis.

16. Document and assess the patient's reaction to the given drug.

c. Diet
Type of Diet
Date ordered
Date started
Date Changed
General Description Indication(s) or Purpose(s)Specific foods
taken
Client’s
Response &/ or
reaction to the
diet
Pediasure and
include two
bananas daily
DO: 03/ 24/ 10
DS: 03/ 24/ 10 Pediasure is a
Fat/carbohydrates/proteins/miner
als/vitamins combination used a
general nutrient.
Bananas have very benefitial
nutritional properties. They are
a good source of vitamin C, B6
and A. Bananas have a high
content of carbohydrates and
fiber, while they are low in
protein levels and fat free.
For childn 1-10 yr who could
physically & mentally benefit from
improved nutrition including picky
eaters, catch-up growth,
prematurity, malnutrition,
hypermetabolism, growth failure,
GI disorders, neurologic disorder
& congenital abnormalities. As a
nutritional supplement for childn
w/ failure to thrive, pre/post
surgery, severe injury, cancer,
recovery from illness or when a
lactose-free nutritional supplement
Banana,
cerelac,
pediasure,
rice
The client
tolerate the diet
well and her
potassium
increased.

They are also rich in
potassium.
is needed.
The client has an illness that
causes hypokalemia and she is
still recuperating from her previous
surgery.
Nursing Responsibilities:
Prior to:
1. Check the doctor’s order for the type of diet prescribed
2. Explain the importance of the diet given.
3. Explain the importance of compliance to the diet given.
4. Inform dietary department on the patient’s diet
5. Identify the right client
6. Update patient significant others of the patient diet change
During:
1. Give appropriate foods to the patient.
2. Enumerate the foods that the patient may or may not take.
3. Emphasize strict compliance to diet

4. Reiterate diet frequently
5. Monitor intake and output
After:
1. Document the patient’s tolerance to the diet given.

B. NURSING MANAGEMENT
1. Nursing Care Plans
Problem # 1: Fluid Volume Deficit Related To Active Fluid Losses As Evidenced By Diarrhea Secondary To Vipoma
AssessmentNursing
Diagnosis
Scientific
ExplanationObjectives Interventions Rationale
Expected
Outcome
S: Ø
O:
Patient
manifested:
Weight loss
from 12 kg to
11.8 kg
3-4 watery
stools per day
Pale
palpebral
conjunctive,
Fluid
Volume
Deficit
Related To
Active Fluid
Losses As
Evidenced
By Diarrhea
Secondary
To Vipoma
Presence of the
ganglioneuroma
produces excessive
amounts of
vasoactive intestinal
polypeptide in the
body. Excessive
amounts of VIP
causes a profound
action of VIP
causing an increase
in intestinal motility
and massive
Short term:
After 8 hours
of nursing
interventions,
the patient
will be able to
have a
decrease in
stool
episode.
Long term:
After days of
1.Established rapport
2.Monitor v/s especially
blood pressure and pulse
3.Monitor and document
vital signs.
1.To gain trust and
cooperation of so and
patient
2.Variations help identify
fluctuating intravascular
volumes.
3.Sinus tachycardia may
occur with hypovolemia to
maintain an effective
cardiac output. Usually
the pulse is weak, and
may be irregular if
electrolyte imbalance also
Short term:
The patient shall
have a decrease
in stool episode.
Long term:
The patient shall
have improved
fluid volume at a
functional level
as evidenced by
an increase in
weight.

lips and nail
beds
Increased
thirst
Hyperthermi
a
Appears
weak
The patient
may manifest:
Tachycardia
Elevated
hematocrit
levels
Decreased
skin turgor
Decreased
secretion of fluids
and electrolytes in
the gastrointestinal
tract causing fluid
losses which can
lead to dehydration
and hypokalemia.
nursing
interventions,
the patient
will improve
fluid volume
at a
functional
level as
evidenced by
an increase
in weight.
4.Monitor temperature.
5.Obtain patient history to
ascertain the probable
cause of the fluid
disturbance.
6.Assess or instruct patient
to monitor weight daily and
consistently, with same
scale, and preferably at the
same time of day.
occurs. Hypotension is
evident in hypovolemia.
4.Febrile states decrease
body fluids through
perspiration and
increased respiration.
5.This can help to guide
interventions. Causes
may include acute trauma
and bleeding, reduced
fluid intake from changes
in cognition, large amount
of drainage post-surgery,
or persistent diarrhea.
6.This facilitates accurate
measurement and follows
trends.

urine output
Increased
urine
concentration
7.Assess fluid losses,
sources, amounts and
effects, urinary output,
vomiting, diarrhea.
8.Increase fluid intake
9.Encourage patient to
drink prescribed fluid
amounts. If oral fluids are
tolerated, provide oral fluids
patient prefers. Place at
bedside within easy reach.
Provide fresh water and a
straw. Be creative in
selecting fluid sources (e.g.,
flavored gelatin, frozen
juice bars, sports drink).
7.Provides information
about body fluid losses
and depletion which can
lead to serious
consequences in the
child.
8.To replace the fluid
losses
9.Oral fluid replacement
is indicated for mild fluid
deficit.

10. Assess intake and
output accurately compare
to losses q 2-8 for I&O
determination and balance.
11. Provide oral hygiene.
12. Teach interventions to
prevent future episodes of
inadequate intake.
13. Provide oral rehydration
therapy (i.e. Pedialyte,
rehydralyte) as ordered
14. Administer parenteral
fluids as ordered. Anticipate
10. Determines loses
related to fluid deficit and
potential for dehydration.
11. This promotes
interest in drinking.
12. Patients need to
understand the
importance of drinking
extra fluid during bouts of
diarrhea, fever, and other
conditions causing fluid
deficits.
13. Promotes fluid and
electrolyte replacement
and prevent dehydration

the need for an IV fluid
challenge with immediate
infusion of fluids for patients
with abnormal vital signs.
15. Administer antidiarrheal
medications
and electrolyte deficits
14. Provide fluid
replacement and maintain
hydration
15. Decreases the
diarrheal episode of the
client
Problem # 2: Diarrhea related to Increase Intestinal Motility Secondary to VIPoma

AssessmentNursing
Diagnosis
Scientific
ExplanationObjectives Nursing Interventions Rationale
Expected
Outcome
S: Ø
O:
Patient
manifested:
Passage of
three to four
watery, loose
stools per day
Weakness
Pale
palpebral
conjunctiva
Pale lips and
nail beds
Watery
consistency of
Diarrhea
related to
Increase
Intestinal
Motility
Secondary
To
VIPoma
The presence of
excessive amounts
of VIP produced by
the
ganglioneuroma
exaggerates the
physiology of VIP
in the
gastrointestinal
tract causing a
further increase in
intestinal motility
and secretion of
fluids and
electrolytes
through the GIT
causing watery
Short-term:
After 5 hours
nursing
interventions,
client’s stool
consistency
will change
from loose to
semi-solid
state.
Long-Term:
After 2 days
nursing
interventions,
1. Establish rapport
2. Assess normal pattern
of bowel elimination and
characteristics of stool
3. Assess abdominal
distention, palpation and
bowel sounds for
increases in auscultation
4. Assess for temperature
elevation, irritability,
lethargy, anorexia
5. Assess for fluid loss
with a light weight loss, dry
1. To gain trust and
promote participation
2. Provides information
about baseline parameters
for comparison and reason
for changes
3. Indicates a distended
bowel with fluid for hyper
motility of bowel which
reduces the amount of
material that is absorbed by
the bowel mucosa
4. To provide information
about signs and symptoms
associated with diarrhea
5. Indicates possible
dehydration associated with
ST:
The client shall
have a change
in stool
consistency
from loose to
semi-solid
state.
LT:
The client shall
have
reestablished
and maintained
a normal

stool on
fecalysis
diarrhea. client’s bowel
functioning
will
reestablish
and maintain
a normal
pattern.
skin and mucous
membranes, poor skin
turgor
6. Evaluate diet history
7. Review food
preparation and discuss
proper food refrigeration
and handling of foods to
SO
8. Check for history of the
following:
GI diseases
9. Encourage continuation
or reinforce the child’s
regular diet as soon as
possible
10. Change diaper
fluid loss
6. To assess the cause
related to environmental
factors
7. To promote wellness
and prevent contamination
and spoiling
8. To detect cause of
diarrhea
9. Regular diet provides
adequate nutrients
10. To prevent skin
pattern of
bowel
functioning.

frequently as needed
11. Wash the perineal
area with warm water after
each diarrhea episode
12. Encourage increase
oral fluid intake
13. Encourage boiling of
drinking water
14. Expose buttocks to air
and apply skin protective
ointment to buttocks
15. Instruct parents for
signs and symptoms of
dehydration or changes in
characteristics of diarrhea
to report them to physician
breakdown and lessen
discomfort
11. To protect skin from
excretions and secretions
that are irritating and cause
excoriation and skin
breakdown
12. To replace fluid losses
and electrolytes
13. To kill microbes present
in water
14. To keep area dry and to
prevent irritation or skin
breakdown
15. To provide immediate
prevention of sever
complication of acidosis

16. Teach caregiver the
importance of fluid
replacement during
diarrheal episodes.
17. Administer
antidiarrheal medications
as ordered
18. Give medications as
ordered
16. Fluids prevent
dehydration.
17. To decrease GI motility
and minimize fluid losses
18. To treat infectious
process
Problem # 3: Hyperthermia related to dehydration
AssessmentNursing
Diagnosis
Scientific
ExplanationObjectives Nursing Interventions Rationale
Expected
Outcome

S: Ø
O:
Patient
manifested:
Warm to
touch skin
Weakness
Pallor
Temperature
of 37.7 oC
3-4 watery
stools per day
Patient may
manifest:
Exhibits
chills
Exhibits
Hyperthermia
related to
dehydration
Because of
excessive fluid
losses from the
inflated effects of
VIP, the body’s
fluid is not
adequate enough
to hydrate the
body causing an
increase in
temperature.
Short-term:
After 5 hours
of nursing
interventions,
the client’s
temperature
will lower of
decrease
from 37.7 oC
to a normal
range of 36.5
oC to 37.4 oC.
Long-Term:
After 2 days
nursing
interventions,
1. Establish rapport
2. Monitor vital signs
especially temperature
3. Provide tepid sponge
bath
4. Provide loose slight
fitting clothes
5. Assess for fluid loss
with a light weight loss,
dry skin and mucous
membranes, poor skin
turgor
6. Keep back dry
7. Promote adequate rest
8. Increase caloric intake
1. To gain trust and
promote participation
2. Used as a baseline data
3. To lower body
temperature
4. To provide conduction
of heat and comfort
5. Indicates possible
dehydration associated
with fluid loss
6. To provide comfort and
alleviate the condition
7. To reduce metabolic
demands and consumption
8. To meet body’s
Short-term:
The client shall
have lowered
or decreased in
temperature
from 37.7 oC to
a normal range
of 36.5 oC to
37.4 oC.
Long-Term:
The client shall
be free from
signs of
hyperthermia
or will not have
increase body

diaphoresis
Tachypnea
Tachycardia
the client will
be free from
signs of
hyperthermia
or will not
have increase
body
temperature.
9. Administer
replacement fluids and
electrolytes
10. Administer
antipyretics as ordered
metabolic needs
9. Serves as a support to
the client’s circulating
volume and tissue
perfusion
10. To decrease
tempereature
temperature.
Problem # 4: Acute Pain related to Colonic Dilatation
AssessmentNursing
Diagnosis
Scientific
ExplanationObjectives Nursing Interventions Rationale
Expected
Outcome
S: “Tiyan, Acute With the intense Short-term: 1. Establish rapport 1. To gain trust and Short-term:

tiyan”, patient
verbalized.
O:
Patient
manifested:
Protective
behavior on
the abdominal
area
Tympanic
abdomen upon
percussion
Facial mask
Crying
The patient
may manifest:
Sleep
Pain
related to
Colonic
Dilatation
action of VIP in the
gastrointestinal
tract, it causes
overdistention of
the smooth
muscles in the
intestines. This
leads to colonic
dilatation. With
colonic dilatation,
the nerve endings
are irritated
causing abdominal
pain.
After 5 hours
nursing
interventions,
the patient’s
pain will be
relieved as
evidence by
absence of
crying and
guarding
behavior.
Long-Term:
After 2 days
nursing
interventions,
2. Assess pain
characteristics:
a. Quality (e.g.,
sharp, burning,
shooting)
b. Severity (scale of 1
to 10, with 10 being
the most severe).
Other methods such
as a visual analog
scale or descriptive
scales can be used
to identify extent of
pain.
c. Location
(anatomical
promote participation
2. Serves as baseline
data
The patient’s
pain shall be
relieved as
evidence by
absence of
crying and
guarding
behavior.
Long-Term:
The patient
shall not
experience
pain.

disturbance
Autonomic
responses
the patient
will not
experience
pain.
description)
d. Onset (gradual or
sudden)
e. Duration (how
long; intermittent or
continuous)
f. Precipitating or
relieving factors
3. Observe or monitor
signs and symptoms
associated with pain,
such as BP, heart rate,
temperature, color and
moisture of skin,
restlessness, and ability
to focus.
4. Assess for probable
3. Nonverbal cues may
determine severity of
pain. Attention to
associated signs may
help the nurse in
evaluating pain.
4. Different etiological

cause of pain.
5. Assess caregiver’s
knowledge of or
preference for the array
of pain-relief strategies
available.
6. Evaluate patient’s
factors respond better to
different therapies.
5. Some caregiver may
be unaware of the
effectiveness of
nonpharmacological
methods and may be
willing to try them, either
with or instead of
traditional analgesic
medications. Often a
combination of therapies
(e.g., mild analgesics
with distraction or heat)
may prove most
effective.
6. It is important to help
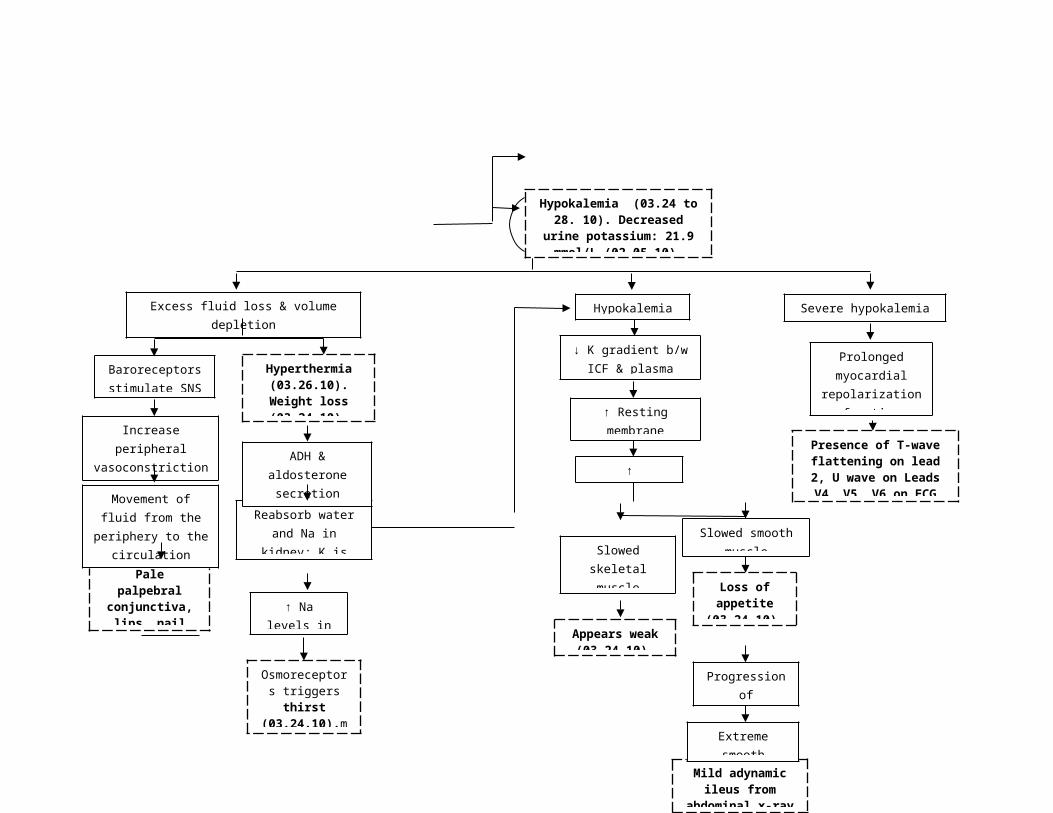
response to pain and
medications or
therapeutics aimed at
abolishing or relieving
pain.
7. Respond immediately
to complaint of pain.
8. Eliminate additional
stressors or sources of
patients express as
factually as possible (i.e.,
without the effect of
mood, emotion, or
anxiety) the effect of pain
relief measures.
7. Prompt responses to
complaints may result in
decreased anxiety in the
patient. Demonstrated
concern for patient’s
welfare and comfort
fosters the development
of a trusting relationship.
8. Patients may
experience an
exaggeration in pain or a

discomfort whenever
possible.
9. Provide rest periods
to facilitate comfort,
sleep, and relaxation.
10. Give analgesics as
decreased ability to
tolerate painful stimuli if
environmental,
intrapersonal, or
intrapsychic factors are
further stressing them.
9. The patient’s
experiences of pain may
become exaggerated as
the result of fatigue A
quiet environment, a
darkened room, and a
disconnected phone are
all measures geared
toward facilitating rest.
10. Pain medications are
absorbed and

ordered, evaluating
effectiveness and
observing for any signs
and symptoms of
untoward effects.
metabolized differently
by patients, so their
effectiveness must be
evaluated from patient to
patient. Analgesics may
cause side effects that
range from mild to life-
threatening.
Problem # 5: Risk for Injury Related To Muscle Weakness Secondary To Hypokalemia
AssessmentNursing
Diagnosis
Scientific
ExplanationObjectives Interventions Rationale
Expected
Outcome
S: Ø
O:
Patient
manifested:
Weight loss
from 12 kg to
11.8 kg
3-4 watery
stools per day
Pale
palpebral
conjunctive, lips
and nail beds
Appears weak
Hypokalemia
Loss of
appetite
Risk For
Injury
Related To
Muscle
Weakness
Secondary
To
Hypokalemia
Excessive
secretion of VIP
from the
ganglioneuroma
causes an
increase in
intestinal motility
and massive
secretion of fluids
and electrolytes
due to the
stimulation of
cAMP. With the
increase in
intestinal motility
and massive
secretion of
electrolytes, loose
watery diarrhea
Short term:
After four
hours of
nursing
interventions,
the patient
will be at
reduced risk
of injury.
Long term:
>After three
days of
nursing
interventions,
the patient
will be free
from injury.
1.Established rapport
2.Monitor and record vital
signs
3.Increased fluid intake
4.Employ safety and
seizure precautions such
as raising side rails and
keeping the bed in a low
position with padded side
rails.
5.Place nonslippery shoes
on the client and assist her
when walking.
6.Discuss to the relatives
the need for assistance of
the patient with her
1.To gain relative and
patient’s trust and
cooperation
2.For baseline
measurement
3.To minimize
dehydration
4.To reduce the risk of
injury.
5.This prevents slipping
of the client and prevent
fall.
6.The relatives must
understand the disease
process and they should
Short term:
The patient shall
have a reduced
risk of injury.
Long term:
The patient shall
be free from
injury.
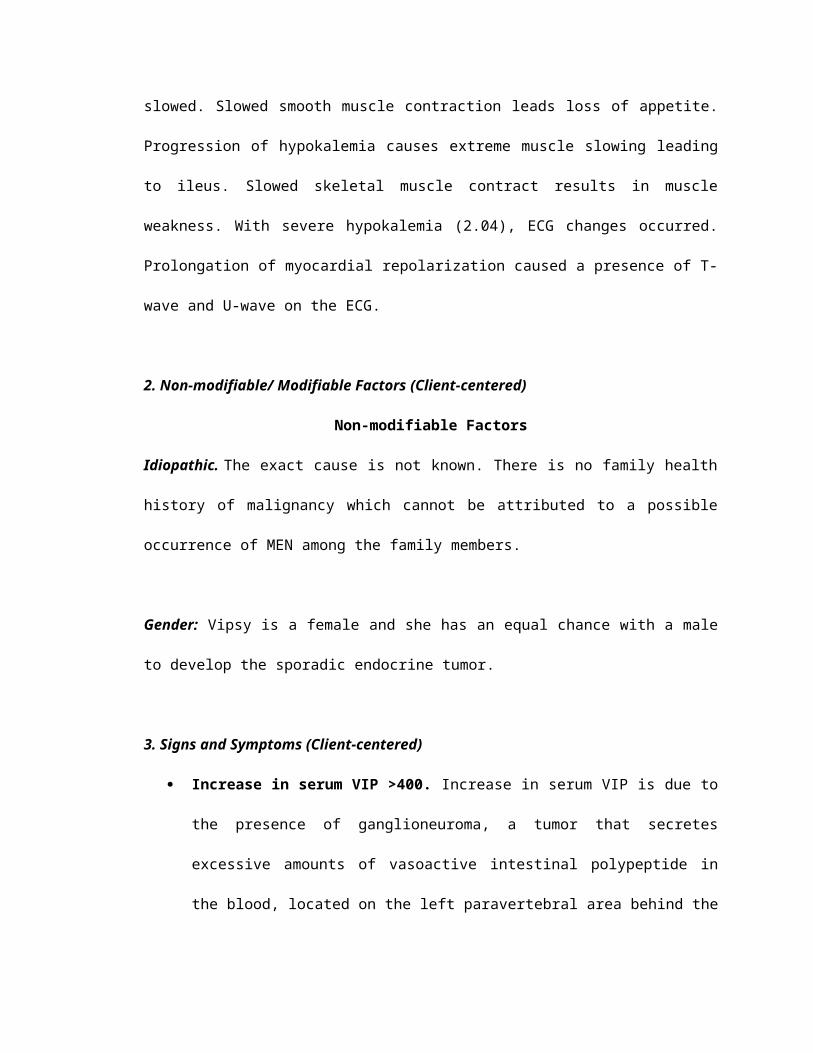
The patient may
manifest:
Falls
Seizure
results and
potassium is lost
through the feces.
Excessive
amounts of loose
watery stools
cause severe
hypokalemia
which can cause
seizure to the
client.
activities of daily living.
7.Administer medications
to increase potassium
levels.
be knowledgeable of the
effect it has on the
patient’s activities of daily
living.
7.To prevent the
progression of
hypokalemia; this can
cause further injury to the
patient.
Problem # 6: Risk for impaired skin integrity related to moisture from frequent stool excessive
AssessmentNursing
Diagnosis
Scientific
ExplanationObjectives Interventions Rationale
Expected
Outcome

S: Ø
O:
Patient manifested:
3-4 watery stools
per day
The patient may
manifest:
Rashes or
redness on the
perineal area
Risk for
impaired skin
integrity
related to
moisture from
frequent stool
Increase in VIP in
the blood causes
and increase in its
actions. One of
the main actions
of VIP is to
increase intestinal
motility. Due to
extreme amounts
of VIP, intestinal
motility is also
affected causing
frequent passing
of loose watery
stools. Since the
client is on her
toilet training
stage, she is does
not know how to
Short term:
After 4 hours
of nursing
interventions,
the patient’s
skin will
remain intact.
Long term:
> after three
days of
nursing
interventions,
the patient will
not manifest
any signs of
skin integrity
such as
redness on
1.Established rapport
2.Monitor and record v/s
3.Assess skin and mucous
membranes for color
changes, warmth, dryness,
swelling or edema
4.Assess for any skin
rashes, dermatitis, and
scratching
5.Instruct relative to air dry
the buttocks after washing
the perineal area.
6.Advise to change diaper
immediately once the
1.To gain SO and
patients trust and
cooperation
2.For baseline
measurement
3.To ensure
identification and
intervention before
impairment becomes too
severe or extensive
4.Reveals skin
condition that lead to
impairment
5.This prevents moisture
build up that could lead
to irritation of the skin.
6.To prevent irritation of
the skin by the urine or
Short term:
> The patient’s
skin shall have
remained intact.
Long term:
The patient shall
not have
manifested any
signs of skin
integrity such as
redness on the
perineal area.

defecate on her
own. With the use
of diapers, loose
stools come in
contact with skin
and prolonged
contact causes
irritation and
breakdown of the
skin in the
perineal area.
the perineal
area.
diaper is soiled.
7.Place antiseptics creams
as prescribed.
feces.
7.To treat and prevent
diaper rashes or
redness.

2. ACTUAL SOAPIERs
March 24, 2010
S: Ө
O: Received patient from ER cuddled by mother on a wheelchair awake, cyring and
irritable with an ongoing IVF of #1 D5 0.3 NaCl 500 cc x 44-45 ugtts/ min at 400
cc level infusing well on the left hand, with pale nail beds, pale palpebral
conjunctiva, pale lips, appears weak, (-) vomiting, with good skin turgor, (+) loss
of appetite, with 3 episodes of watery loose stools. With vital signs as follows: T:
37.2 oC, PR: 112 bpm, RR: 26 cpm.
A: Fluid Volume Deficit Related To Active Fluid Losses As Evidenced By Diarrhea
Secondary To Vipoma
A2: Diarrhea related to Increase Intestinal Motility Secondary to VIPoma
P: After 3° of nursing intervention the client will not pass loose watery stool within
the shift.
I: > Established rapport
> Monitored and recorded VS q 4
> Needs attended
>Recorded I&O
> Assessed condition and watch out for signs and symptoms dehydration
> Fixed bed linens
> Assisted client with activities

> Encouraged frequent rest periods
> Changed position gradually every 2 hours
> Provided client safety such as raising side rails
> Maintained a restful environment
> Regulated IVF as ordered
> Instructed relative that the client is for urinalysis and fecalysis and provided
specimen cup and weebag
> Instructed relative regarding client’s diet: May give Pediasure and include two
bananas daily
>Provided adequate hydration
> Advised proper perineal hygeine
>Kept patient’s back dry
>Informed Pedia resident of admission
>Due medications given
>Endorsed
E: Goal not met as evidenced by passage of another episode of watery stool.
R: Reinforce previous plan of care.

March 25, 2010
S: Ө
O: Received patient on bed awake on a sitting position, with an ongoing IVF of #4
D5 0.3 NaCl 72.5 cc + KCl 1.5 cc = 74 cc every 2 hours at 50 cc level via soluset
infusing well on the left hand, with pale nail beds, pale palpebral conjunctiva, pale
lips, (-) weakness, (-) vomiting, with good skin turgor, with fair appetite, with 3
episodes of scanty loose stools, (+) productive cough. With vital signs as follows:
T: 37.6 oC, PR: 12 bpm, RR: 28 cpm.
A: Fluid Volume Deficit Related To Active Fluid Losses As Evidenced By Diarrhea
Secondary To Vipoma
A2: Diarrhea related to Increase Intestinal Motility Secondary to VIPoma
P: After 8° of nursing intervention the client will not pass loose watery stool within
the shift.
I: > Established rapport
> Monitored and recorded VS q 4
> Needs attended
>Recorded I&O
> Assessed condition and watch out for signs and symptoms dehydration
> Fixed bed linens
> Assisted client with activities
> Encouraged frequent rest periods
> Changed position gradually every 2 hours

> Provided client safety such as raising side rails
> Maintained a restful environment
>Still for Fecalysis, with specimen cup
> Regulated IVF as ordered
> Reinforced relative regarding client’s diet: May give Pediasure and include two
bananas daily
>Provided adequate hydration
> Advised proper perineal hygeine
>Kept patient’s back dry
>Seen on rounds by the attending physician with orders made and carried out:
continue medication
>Due medications given
>Endorsed
E: Goal met as evidenced by negative bowel movement during the shift.

March 27, 2010 (Final Nurse-client interaction)
S: Ө
O: Received patient on bed asleep on a supine position, with an ongoing IVF of # 38
D5 0.3 NaCl 72.5 cc + KCl 1.5 cc = 74 cc every 2 hours at 70 cc level via soluset
infusing well on the left hand, with pinkish nail beds, pinkish palpebral
conjunctiva, pinkish lips, (-) weakness, (-) vomiting, with good skin turgor, with
fair appetite, with 2 episodes of scanty loose stools. With vital signs as follows: T:
36.6 oC, PR: 110 bpm, RR: 30 cpm.
A: Fluid Volume Deficit Related To Active Fluid Losses As Evidenced By Diarrhea
Secondary To Vipoma
A2: Diarrhea related to Increase Intestinal Motility Secondary to VIPoma
P: After 8° of nursing intervention the client will not pass loose watery stool within
the shift.
I: > Established rapport
> Monitored and recorded VS q 4
> Needs attended
>Recorded I&O
> Assessed condition and watch out for signs and symptoms dehydration
> Fixed bed linens
> Assisted client with activities
> Encouraged frequent rest periods
> Changed position gradually every 2 hours
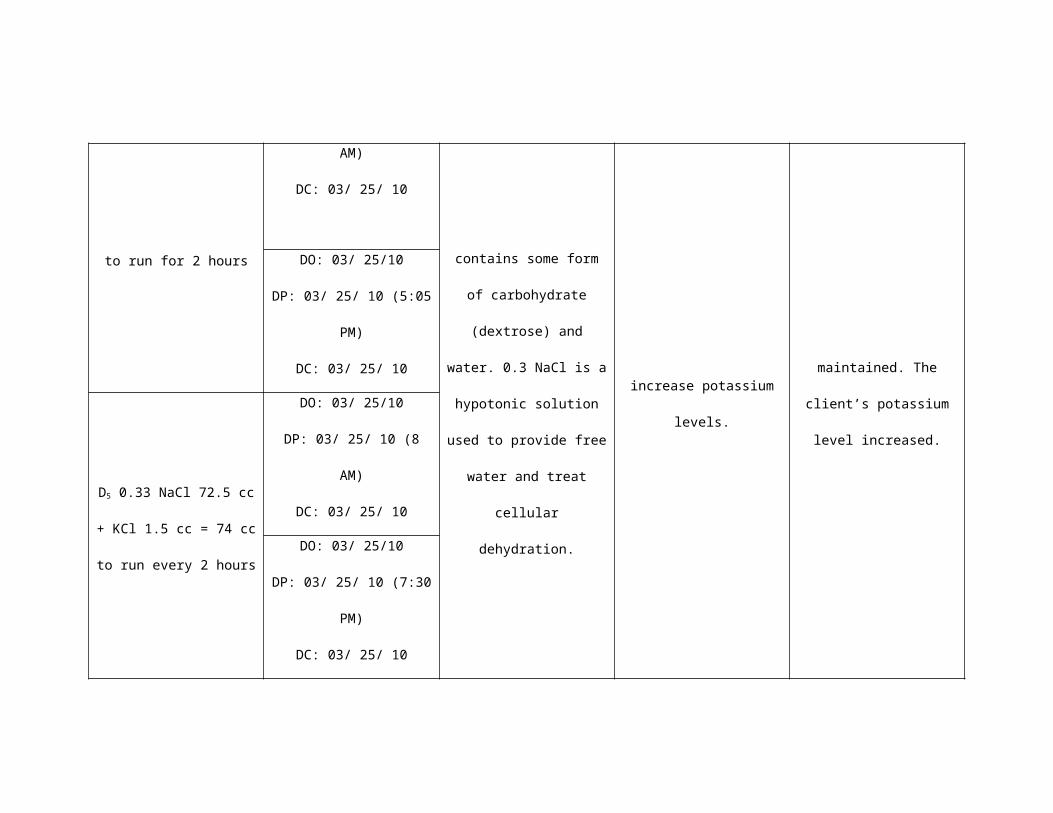
> Provided client safety such as raising side rails
> Maintained a restful environment
> Regulated IVF as ordered
> Reinforced relative regarding client’s diet: May give Pediasure and include two
bananas daily
>Provided adequate hydration
> Advised proper perineal hygeine
>Kept patient’s back dry
>For potassium extraction at 6 AM
>Due medications given
>Endorsed
E: Goal not met as evidenced by client had one loose bowel movement.
R: Reinforce previous plan of care.

VI. PATIENT’S DAILY PROGRESS IN THE HOSPITAL
A. Client’s Daily Progress Chart
DAYSADMISSION
(03/24/10)
2
(03/25/10)
3
(03/26/10)
4
(03/27/10)
DISCHARGE
(03/28/10)
Nursing Problems
Problem # 1: Fluid Volume Deficit Related To
Active Fluid Losses As Evidenced By Diarrhea
Secondary To Vipoma
Problem # 2: Diarrhea related to Increase
Intestinal Motility Secondary to VIPoma
Problem # 3: Hyperthermia related to dehydration
Problem # 4: Acute Pain related to Colonic
Dilatation
Problem # 5: Risk For Injury Related To Muscle
Weakness Secondary To Hypokalemia
Problem # 6: Risk for impaired skin integrity
related to moisture from frequent stool
Vital Signs T: 37.2 oC T: 37.6oC T: 37.7oC T: 36.5 oC T: 36.5 oC

PR: 112 bpm
RR: 26 cpm
PR: 124 bpm
RR: 28 cpm
PR: 124 bpm
RR: 28 cpm
PR: 110 bpm
RR: 26 cpm
PR: 108 bpm
RR: 25 cpm
Diagnostic and Laboratory Procedures
CBC
Hct: 0.40
Hgb: 128
Leukocytes: 4.2
Neutorphils:
0.36
Lymphocytes:
0.55
Monocytes: 0.07
Eosinophils:
0.02
Platelet count:
285
Blood Chemistry K: 2.68 6 AM
K: 2.04
2 PM
6 AM
K: 2.89
2 PM
6 AM
K: 3.47
6 AM
K: 3.18
2 PM

K: 2.34
Cl: 106.1
Na: 136.3
K: 3.49 K: 3.49
Urinalysis
Color: Light
yellow
Appearance:
Clear
pH: 6.5
Sp. Gr: 1.010
Sugar: (-)
Albumin: (-)
Pus cells:
1-3/HPF
Red cells:
1-3/HPF
Epithelial cells:
Rare
Bacteria: Few
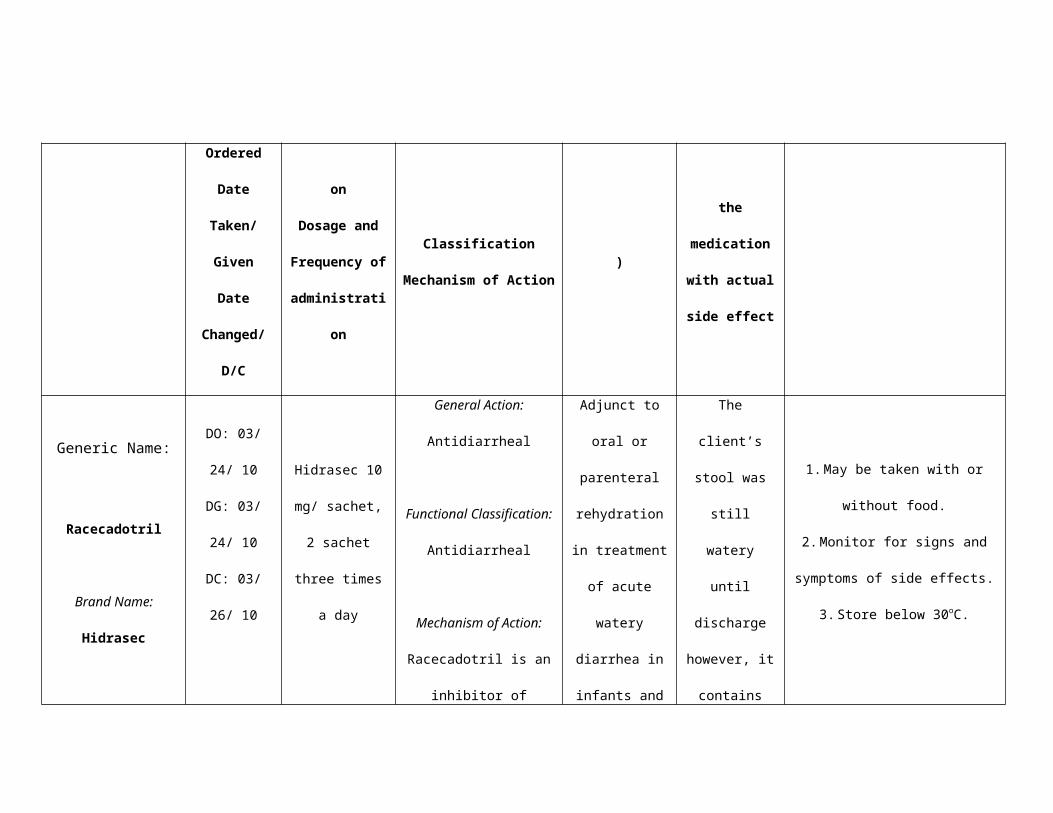
Stool Examination
Color: Brown
Consistency:
Watery
Result: No
intestinal
parasites seen
Chest X-ray PAL view Shows
unchanged
status of mass-
like opacity
Rule out
posterior
meidastinal
mass.
The rest of the
visualized lung

fields are clear.
15 Lead ECG
T wave
flattening on
Lead II;
Presence of U
wave on Leads
V4, V5, V6
Medical Management
IVF
1. D50.3 NaCl 500 x 44-45 ugtts/min to run for 8
hours
2. D50.3 NaCl 500 x 69 ugtts/min
3. D5IMB 500 cc x 36-37 ugtts/min
4. D50.3 NaCl 71.7 cc + KCl 2.3 cc = 74 cc to run
for 2 hours
5. D50.3 NaCl 72.5 cc + KCl 1.5 cc = 74 cc to run
every 2 hours

DRUGS
1. Hidrasec 10 mg 2 sachet TID
2.Ampicillin 300 mg SIVP Q 6
3.Solmux syrup ½ tsp TID
4.Paracetamol drops1.2 ml Q4 prn x fever
5.Dicycloverine (Relestal) 2.5 ml PO Q8
6.Kalium durule 1 tab OD
7.Kalium durule 1 tab BID
DIET
1.Pediasure include Bananas Daily

VII. DISCHARGE PLANNING
A. General condition about the client upon discharge.
The client was seen by the nurse researcher 8 hours before being discharged. Vipsy
was chewing gum and was very lively. She was talkative and plays with her mother. She
has a good hygiene. Vipsy was not irritable and does not appear weak. She has a scar
on her umbilical area.
B. METHOD
M: Instructed relative that Vipsy will take the following medications:
Kalium durule 1 tablet twice a day. Kalium durule is taken to replace potassium
losses. Side effects include nausea and vomiting, bradycardia, decreased in
urine output.
Chloramphenicol suspension 5 mL every six hours for five days.
Chloramphenicol is indicated to treat infection. Adverse reactions to monitor are
nausea and vomiting, stomatitis, glossitis and rectal irritation.
E: May resume activities as tolerated
T: Home maintenance and management; Instructed to take medications as
prescribed and to watch out for worsening of signs and symptoms
H: Instructed regarding the complications that warrants medical attention
Describe prescribed drugs, including their names, dosages, actions, adverse
effects
Provided health teachings on how to prevent injury
Instructed proper hygiene
Advised to increase fluid intake and intake of high potassium diet

Instructed to provide healthy meals to the client
O: Instructed relative to come back for a follow-up check up on Wednesday (March
31, 2010) 10 AM at the physician’s clinic.
D: Advised to provide a high potassium diet to the client
SAMPLE MENU
Breakfast: Anytime Smoothie or - a bran cereal without sugar, use Sucanat for
sweetening, and 1/4 cup milk and one egg and 1 cup orange juice or other fresh or
canned unsweetened juice, high potassium, or fresh fruit or- cooked oatmeal and raisins
or blueberries or other fruit with milk or rice milk or no milk with added protein powder or
added cottage cheese, Sucanat sweetener or maple syrup or honey.
Lunch: Large salad with turkey or tuna 1-3 oz. and carrots, cucumber, sprouts, kidney
or garbanzo beans, sweet red pepper, red cabbage, lettuce or mixed greens, onions and
S&W non-fat dressing or equivalent; or- 2 cups brown rice and 1-3 oz. fish or poultry or
lean red meat and 2 cups vegetable such as asparagus or green beans and 2 fruits or 2
cups mixed fruit for dessert. To add carbohydrates add 1-2 slices of whole grain fat free
bread or add rice noodles to the salad or- soup or stew with lots of veggies and a small
amount of protein such as beans or chicken or beef or tofu and fruit for desert.
Dinner: Soup or stew or casserole with some protein from poultry or fish or legumes; or
tofu and lots of vegetables, served with whole grain fat free bread (optional); or- 1-3 oz.
of protein as above (more if beans are your source) and rice or pasta (use tomato based
sauce to replace the missing potassium in pasta); or a large baked potato with the skin
and 2-3 oz. protein and 2 cups of vegetables or salad with lots of veggies in it plus 2
more servings of fruit.
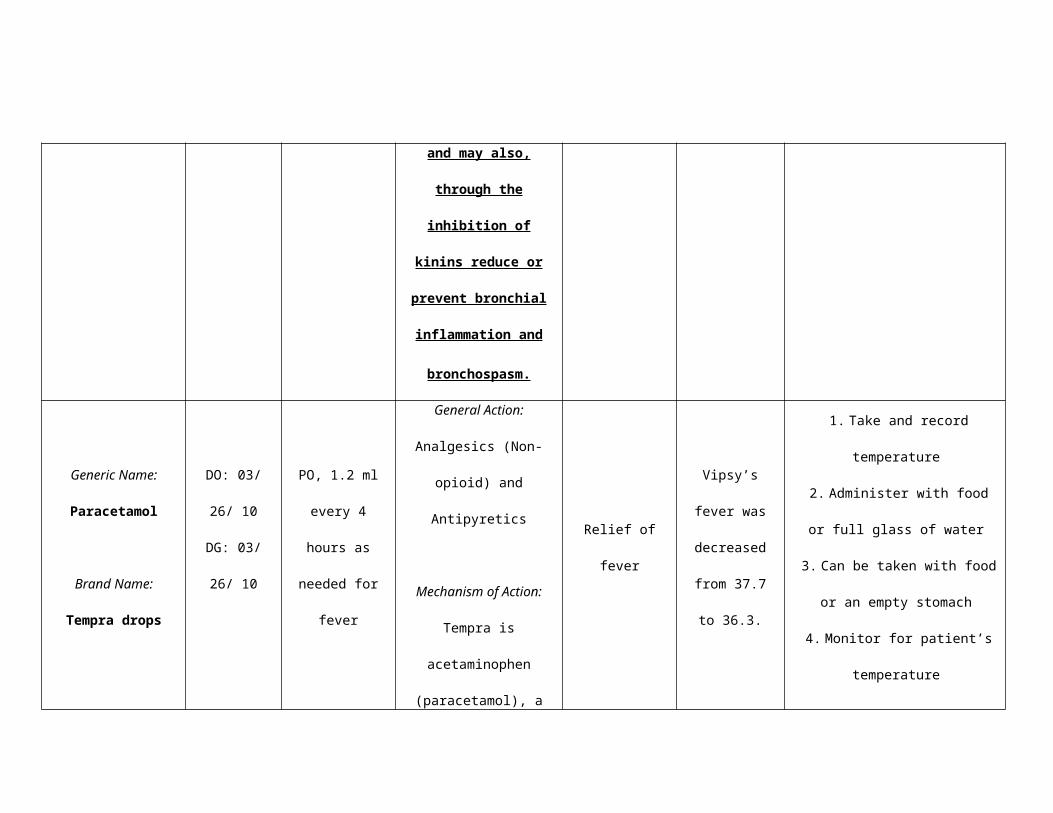
Condiments: Salsa adds C, bioflavonoids and potassium. Low salt, low sugar (or home-
made) ketchup. Tomato sauces. Parmesan cheese. All spices and herbs. Wysong mixed
salt or VegeSalt. Soy sauce without preservatives. Butter. Cream cheese. Sour cream.
Most non-fat dressings but look for the most natural without artificial flavorings and
preservatives. Our favorite is S&W. Small amounts of olive oil or peanut oil. Lots of garlic
and onion. Yeast flakes to flavor popcorn.
(http://www.krispin.com/potassm.html#SAMPLE).
VIII. SUMMARY OF FINDINGS
VIPoma is a very rare type of pancreatic endocrine tumor. It affects hormone-
producing cells in the pancreas, known as islet cells. The disease causes these cells to
produce extremely high levels of vasoactive intestinal peptide (VIP), a hormone that
regulates water transport in the intestines. It is also called Verner-Morrison syndrome or
pancreatic cholera. Excessive amounts of VIP causes a distince syndrome characterized
by large-volume watery diarrhea, hypokalemia, and dehydration. The syndrome is also
called WDHA syndrome of watery diarrhea, hypokalemia, and achlorhydria. The exact
cause of Vipoma is not known, although genetics are believed to be a factor. A family
history of MEN and similar syndromes can also increase one’s risk. Most patients are
adults between 40s to 50s, and women are more likely to develop it than men. Children
are rarely affected having a ratio of 1:1 in both males and females. When it occurs in
children, it is usually caused by a ganglioneuroma or ganglioneuroblastoma. VIPomas
are usually malignant when diagnosed in adults, however, in children, they are benign.
The principal symptoms are large-volume diarrhea which is secretory in nature that is
severe enough to cause hypokalemia, dehydration, hypochlorhydria, and flushing. The
diarrhea is secretory in nature, persists during fasting, and is almost always > 3 L/d.

Most patients do not have accompanying steatorrhea, and the increased stool volume is
due to increased excretion of sodium and potassium, which, with the anion, account for
the osmolality of the stool. Clients frequently have hyperglycemia due to the
glycogenolytic effect of the VIP.
VIP is a 28-amino-acid peptide that is an important neurotransmitter ubiquitously
present in the central nervous system and GI tract. Its known action include stimulation
of small-intestinal chloride secretion and effects on smooth muscle contractility, inhibition
of acid secretion, and vasodilatory effects which explains most features of the clinical
syndrome. The most significant effect of VIP is in the gastrointestinal system wherein it
continuously secretes fluids and electrolytes specifically potassium which causes
profound hypokalemia.
The goal of treatment for clients with VIPoma is to replace fluids and electrolytes
loss and maintain a good hydration status. Surgery can be performed to remove the
tumor secreting VIP. For clients with malignancy, chemotherapy is advised. With
metastasis, multiply organ resections are done to decrease the symptoms of the patient.
A somatostatin drug called Octreotide blocks the action of vasoactive intestinal
polypeptide and can reduce the diarrheal episodes of clients.
IX. CONCLUSION
Based on the summary of findings, VIPoma is a rare disease that has little
definition in literature. Little medical management is known to prevent the complications
of the disease and mostly it is done by surgery. Unlike other diseases that have many
alternatives in managing the disease, VIPoma only is usually managed by hydration,
surgery and with the use of a somatostatin drug.
The main affectation of VIPoma is in the gastrointestinal system wherein it
causes secretory watery diarrhea in large-volume enough to cause dehydration and
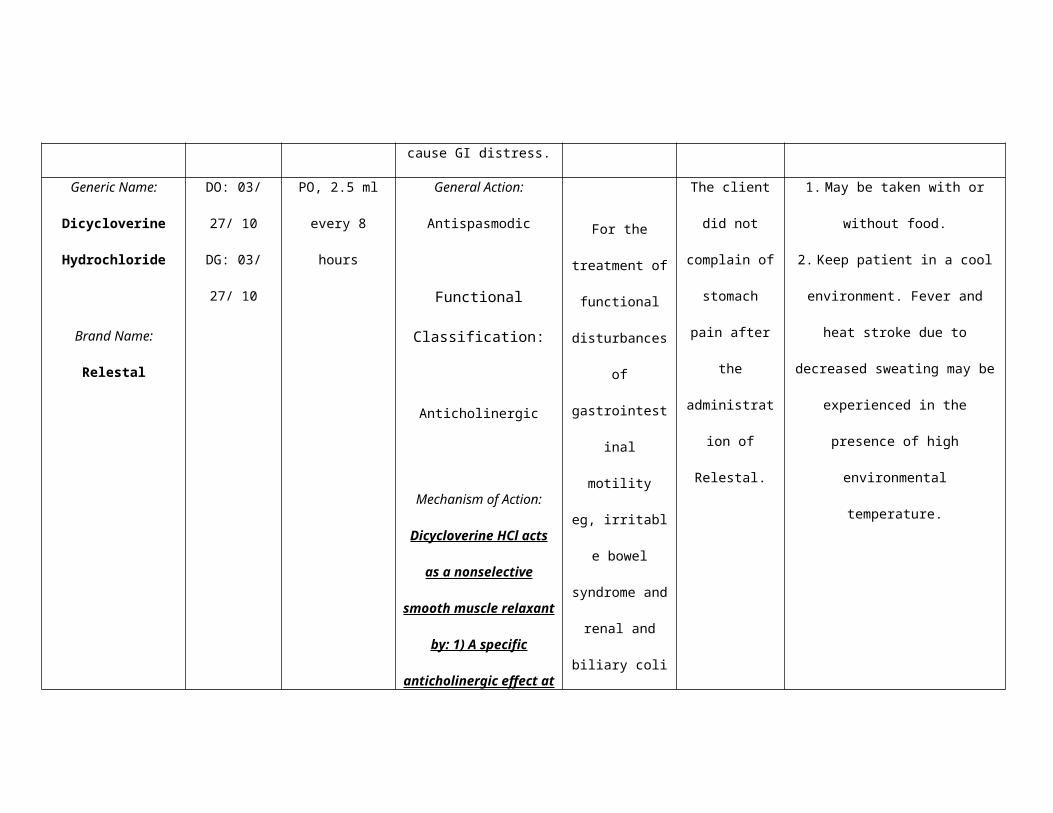
electrolyte imbalances. The chief electrolyte affected in these clients is potassium.
Potassium is easily replaced by diet and intravenous infusion of potassium chloride;
however, if the secretory diarrhea is not controlled or the tumor is not eliminated, signs
and symptoms of the disease will recur back.
X. RECOMMENDATIONS
In light of the foregoing findings and conclusions drawn, the following
recommendations are hereby offered:
1. Since VIPoma affects both adults and children, frequent medical
screening should be stressed by the nurses to their clients because
tumors can occur sporadically in one individual.
2. Since the cause of VIPoma is not known, it is important to have further
studies on this illness since it has detrimental effects to the clients
afflicted with this disease.
3. The physicians should discover more medical treatment for VIPoma
even though it is a very rare disease. They should not always result to
surgery or multiple resections of vital organs especially when dealing with
pediatric clients.
4. Clients experiencing signs and symptoms of illness unfamiliar with their
medical history should promptly seek medical attention to prevent
complications.

XI. LEARNING DERIVED
Life indeed is precious especially to clients with this rare disease. In the case of Vipsy,
her life is only starting and it is saddening to know that she is already facing trials at this
point in her life. People should be thankful with the advancement of medical treatment
nowadays. Rare diseases are diagnosed and treated with the prescribed medical
management. However, since these diseases are rare, only little is known about them.
What the researcher learned in her study is to appreciate what she has in her life
right now as compared to her client. It is a blessing that the researcher is healthy and is
not facing medical obstacles in her life. Also, it is important to always maintain a positive
attitude in life, whether you are afflicted with an illness or other problems in life. It is very
crucial to always have faith and to remember that God will not give you problems you do
not know how to handle.

XII. BIBLIOGRAPHY
BOOKS
Bare, Brenda. Brunner and Sudddarths Textbook of Medical-Surgical Nursing . 11th ed.
Vol. 1 & 2. Pennsylvania: Lippincott Williams and Wilkins, 2004.
Black, Joyce M. and Hawks, Jane Jokanson. Medical-Surigcal Nursing: Clinical
Management for Positive Outcomes. 7th ed. Volume 1. Singapore: Elsevier Inc.,
2005.
Comer, Sheree. Delmar’s Critical Care Nursing Care Plans. 2nd ed. Asia: Delmar
Learning, 2005.
Flethcer, Christopher. Diagnostic Histopathology of Tumors. 3rd ed. Vol. 2. USA: Elsevier
Limited, 2007.
Goldman, Lee and Dennis Ausiello. Cecil Medicine. 23rd ed. USA: Elsevier, Inc., 2008.
Greenspan, Francis and David Gardner. Basic and Clinical Endocrinolog. 6th ed. USA:
McGraw-Hill Companies, Inc., 2001.
Greenspan, Francis and John Baxter. Basic and Clinical Endocrinolog. 4th ed. USA:
Appleton & Lange, 1994.
Kasper, Dennis, et. al. Harrison’s Principles of Internal Medicine. 16 d. USA: McGraw-
Hill Companies, Inc., 2005.
Kozier, Barbara, et. al. Fundamentals of Nursing: Concepts, Process and Practice. 7th
ed. Phil: Pearson Education South Asia Pte Ltd., 2004.
Rubin, Emmanuel. Rubin’s Pathology: Clinicopathologic Foundations of Medicine. 4th ed.
USA: Lippincott Williams & Wilkins, 2005.
Seeley, Rod R. et. al. Essentials of Anatomy and Physiology. 5th ed. New York:
McGraw-Hill Companies, Inc., 2005.
Skidmore-Roth, Linda. Mosby’s Nursing Drug Reference. USA: Mosby, Inc., 2008.

INTERNET SOURCES
Ferry, Robert Jr. VIPoma. <http://emedicine.medscape.com/article/925341-followup> Jul
8, 2008.
Vinik, Aaron. Vasoactive Intestinal Peptide Tumor (VIPoma)
<http://www.endotext.org/guthormones/guthormone6/guthormone6.htm> August
2, 2004 .
Ong, Evan. Neoplasms of the Endocrine Pancreas.
<http://emedicine.medscape.com/article/276943-diagnosis> Dec 23, 2009.
Tung, Daniel. VIPomas. <http://emedicine.medscape.com/article/125910-overview>
Dec 18, 2008.
http://www.knowcancer.com/oncology/vipoma/
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2517072/
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2844690/
www.mimsonline.com

XIII. APPENDICES
World J Surg Oncol. 2008; 6: 80.
Published online 2008 July 28. doi: 10.1186/1477-7819-6-80.
PMCID: PMC2517072
Copyright © 2008 Joyce et al; licensee BioMed Central Ltd.
Multi-visceral resection of pancreatic VIPoma in a
patient with sinistral portal hypertension
David L Joyce,1 Kelvin Hong,2 Elliot K Fishman,3 Joshua Wisell,4 and Timothy M Pawlik 1
Background
VIPomas are rare neuroendocrine tumors with an annual incidence of about 1 per
10,000,000 individuals.[1] The majority of VIPomas in adults (> 90%) are primary tumors
of the pancreas.[2] As with other neuroendocrine tumors of the pancreas, on occasion
these lesions can be exceptionally large with invasion of adjacent visceral and vascular
structures. As such, accurate preoperative imaging is critical. In particular, assessment
of the relationship between the tumor and adjacent vascular structures, such as the
portal and superior mesenteric vein (SMV) as well as the celiac and superior mesenteric
artery (SMA), is critical in determining preoperative resectability. On occasion, invasion
of the tumor into the adjacent splenic-portal venous system can lead to sinistral, or left-
sided, portal hypertension.
Surgical resection of pancreatic VIPoma provides the only chance at long-term cure, as
systemic chemotherapeutic agents are associated with poor response rates.[3]
Nevertheless, aggressive resection in patients with advanced VIPoma neuroendocrine
tumors has rarely been reported. While part of the reason for this undoubtedly is due to
the rarity of VIPomas, another factor may be related to the reluctance to perform

aggressive resection due to possible increased morbidity and mortality.[4] With careful
attention to pre- and intra-operative details, aggressive resection of VIPomas can be
accomplished safely, thereby providing the patient with an opportunity for extended long-
term survival. We herein report a case of multi-visceral resection of pancreatic VIPoma
in a patient with sinistral portal hypertension. Furthermore, we provide a brief review of
the role of aggressive resection of pancreatic neuroendocrine tumors and highlight
several key technical points that allowed for successful resection.
Case presentation
A 46-year-old obese woman presented to an outside hospital in August of 2005 with
significant abdominal pain and diarrhea. Computed tomography (CT) revealed a 17 × 13
cm mass in the left upper quadrant that appeared to arise from the body and tail of the
pancreas. The patient was taken to the operating room at an outside institution, but the
mass was deemed unresectable due to reported involvement of the SMA, stomach, and
colon. Wedge biopsy of the mass was consistent with pancreatic VIPoma. Over the next
2 years, the patient was treated with long-acting somatostatin with some improvement in
her symptoms. The patient, however, developed repeat episodes of upper and lower
gastrointestinal bleeding with associated anemia and ongoing transfusion requirements.
Repeat CT scan revealed thrombosis of the splenic vein with numerous large splenic
and gastric varices consistent with sinistral portal hypertension. In the summer of 2007,
the patient underwent a failed transjugular intrahepatic portosystemic shunt (TIPS)
procedure at an outside institution. The patient was therefore referred to the Johns
Hopkins Department of Interventional Radiology for variceal embolization.
The patient's case was reviewed at the Johns Hopkins multi-disciplinary pancreas tumor
board. A repeat three-dimensional (3-D) pancreas protocol CT scan revealed an 18 × 12
cm mass abutting the liver, stomach, spleen, left adrenal, colon and invading the distal
duodenum – proximal jejunum at the ligament of Treitz. The splenic vein was occluded.

Large collateral vessels surrounded the mass and were associated with extensive
gastric collaterals (Figure (Figure1). 1 ). The mass displaced the SMA and SMV, but
these vessels were patent and uninvolved (Figure (Figure2). 2 ). As such, there were no
obvious contraindications to resection and surgery was recommended.
Given the size of the mass and the associated extensive varices, the patient underwent
preoperative proximal splenic artery embolization (Figure (Figure3). 3 ). Twenty-four
hours following this, the patient was taken to surgery where she was found to have a
very large mass arising from the body and tail of the pancreas that invaded the left
diaphragm, stomach, left adrenal, fourth portion of the duodenum – first portion of the
jejunum, transverse colon, and spleen. In order to better expose the SMV at the inferior
border of the pancreatic neck, the right colon and root of the small bowel mesentery
were mobilized in the fashion of Cattell and Braasch. The SMA medial to the SMV was
exposed as it coursed into the small bowel mesentery. The tumor was noted to closely
abut and displace both the SMV and SMA, but the vessels were not encased. After
developing the retro-pancreatic plane over the SMV – portal vein, the pancreatic neck
was transected. The mass was subsequently resected en bloc with a portion of the left
diaphragm, entire stomach, spleen, left adrenalectomy, fourth portion of the duodenum –
proximal jejunum and transverse colon. Gastrointestinal continuity was restored using a
Roux-en-Y method with a hand sewn end-to-side esophago-jejunostomy, a duodeno-
jejuneal anastomsis (50 cm distally), and a stapled colo-colonic anastomosis. The
pancreatic remnant was closed with pledgeted sutures. Estimated blood loss was 500
ml. Final pathology confirmed a VIPoma originating from the pancreatic body with
invasion of the stomach, spleen, small bowel, and colon (Figure (Figure4). 4 ). All margins
were uninvolved by tumor. The patient is alive and disease-free.

The patient tolerated the procedure well. On post-operative day four, a swallow study
demonstrated a normal post-surgical esophago-jejunal anastomosis with no evidence of
leak. The patient was discharged home on post-operative day ten tolerating a post-
gastrectomy diet. She received no adjuvant therapy and is currently alive and disease-
free at 6 months of follow-up.
Discussion
VIPomas are rare tumors that have been infrequently reported in the literature.[5] These
pancreatic tumors secrete excessive amounts of VIP (Vasoactive Intestinal Peptide), a
structural homologue of secretin. Elevated serum VIP levels cause increased intestinal
secretion of Na+, K+, HCO3-, and Cl-, as well as bone resorption, vasodilation, and
inhibition of gastric acid section. These effects lead to a well-defined clinical syndrome,
characterized by watery diarrhea, hypokalemia, and hypochlorhydria. Despite this, the
VIPoma syndrome can be difficult to diagnosis and these tumors can elude prompt
diagnosis.[5] As such, similar to other neuroendocrine tumors, VIPomas can be quite
large at the time of presentation and involve adjacent structures. As in the current case,
locoregional extension can include invasion into visceral structures. However, with an
aggressive surgical approach that allows for complete tumor extirpation, extended,
meaningful survival can be achieved for VIPoma patients.[5]
Norton et al.,[4] have reported that aggressive surgery can be done with acceptable
morbidity and low mortality rates for patients with advanced neuroendocrine tumors. In a
series of 20 patients with advanced tumors, Norton et al.,[4] reported a post-operative
complication rate of 30% and no operative deaths. In that study, surgery variably
included pancreatectomy, splenectomy, superior vein reconstruction, and liver resection.
In the current case, the patient underwent an extensive procedure that included

pancreatectomy, splenectomy, total gastrectomy, left adrenalectomy, diaphragmatic
resection, as well as small and large bowel resection. An R0 resection (microscopically
negative margins) was achieved and the patient did well post-operatively. Patients with
locally advanced neuroendocrine tumors that can be technically resected with an R0
margin should therefore be offered surgical resection even when a multi-visceral
resection is necessary. In high-volume institutions, these procedures can be
accomplished with acceptable morbidity and near-zero mortality.[4,6,7]
Accurate CT imaging is critical in assessing locoregional resectability.[8,9] Recently, 3-D
CT scan has been reported to enhance the assessment of the tumor-vascular interface,
[10] as the 3-D format allows for better viewing of oblique orientations.[11] Accurate
information concerning the relation of the tumor with the SMA is particularly critical as
major arterial encasement may preclude an R0 resection. It is important to note,
however, that intraoperative assessment of the tumor-SMA relationship can be very
limited – especially in patients with large tumors.[12] This is evidenced in the current
case in which the initial surgeon deemed the lesion to be unresectable based on an
intraoperative assessment that the SMA was encased. High-quality cross-sectional
imaging clearly demonstrated, however, that the SMA was indeed not involved (Figure
(Figure3). 3 ). This case highlights how intraoperative assessment of the tumor-SMA
interface may be both limited and misleading. Rather, thin-section contrast-enhanced CT
should be utilized as the modality of choice in assessing the relationship of the primary
tumor to major vascular structures such as the SMV, PV, SMA, and celiac axis. Such
determinations have important clinical implications in deciding which patients are
candidates for aggressive resection of advanced pancreatic tumors.
For tumors such as the one presented here, the surgeon should still evaluate the SMV
and SMA early in the course of surgery. Full exposure of the SMV is mandatory and
requires mobilization of the colon and root of the small bowel mesentery to expose the

SMV where it lies anterior to the third portion of the duodenum. This mobilization should
be carried to the left by incising the omental attachment to the mesocolon. After
performing a wide Kocher maneuver, the SMA should similarly be identified at the
junction of the third and fourth portions of the duodenum as it courses distally. The
connective tissue attachments between the portal vein/SMV and SMA can then be
divided, thereby isolating the vessels. This "medial" approach allows for early dissection
and evaluation of the critical vascular structures. Once the relation of the tumor to these
structures has been established, more lateral dissection along the spleen and tail of the
pancreas can be accomplishing with little difficulty. This method of dissecting the SMA
and SMV first allows the surgeon to avoid committing to an extensive resection prior to
determining whether or not an R0 resection is feasible.[13]
Sinistral, or left-sided, portal hypertension rarely causes gastrointestinal hemorrhage.
Although there are many causes of sinistral hypertension, it is usually due to pancreatic
pathology that compresses/invades the left portal – splenic venous system.[14,15]
Splenic vein occlusion results in back pressure which is transmitted to the short gastric
and gastroepiploic veins with subsequent formation of varices. Our patient had extensive
gastric and peri-tumoral varices that were associated with ongoing bleeding and
transfusion requirements. Management of sinistral hypertension traditionally involves
surgical removal of the primary tumor if possible. In the current case, although resection
was deemed to be feasible, the risk of intra-operative massive hemorrhage was felt to be
considerable given the extent of the varices, as well as the size and location of the
primary pancreatic mass. Preoperative proximal splenic artery embolization has
previously been shown to be a safe and efficacious portal decompression technique.
[16,17] Umeda et al., [17] have shown that proximal splenic artery embolization
shortened operative time, reduced blood loss, and led to less need for transfusion in
living donor liver transplantation recipients. In a separate study, Adams and

colleagues[16] assessed the benefit of preoperative control of splenic arterial inflow on
intraoperative blood loss in a cohort of patients with splenic venous occlusion and
sinistral hypertension secondary to chronic pancreatitis. In this study, the mean
reduction in blood loss associated with embolization was 1560 ml. The employment of
preoperative proximal splenic artery embolization in the present case undoubtedly
contributed to our relatively modest blood loss (~500 ml). In complex cases
characterized by large tumors, splenic vein occlusion, and significant left-side portal
hypertension with associated varices, preoperative embolization of the proximal splenic
artery should be considered to allow for portal decompression as a means to reduce
intraoperative blood loss. Preoperative splenic artery embolization should be used
selectively, however, as it may have associated risks.[18]
Conclusion
The current case is a unique example of a rare pancreatic tumor (VIPoma) that
highlights several important peri- and intra-operative concepts. Aggressive resection of
VIPomas is warranted and may provide the only chance at long-term survival. When
done at large volume, experienced centers even complex multi-visceral resections can
be done with low morbidity and near zero morality. In the subset of patients with
associated severe sinistral hypertension, proximal splenic artery embolization should be
considered as a preoperative means to decrease blood loss and improve outcome. Only
by utilizing a multi-modality approach that incorporates state-of-art cross-sectional
imaging, interventional radiology, and surgery can these complex patients be managed
successfully.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2517072/

Yale J Biol Med. 2010 March; 83(1): 27–33.
Published online 2010 March.
PMCID: PMC2844690
Copyright ©2010, Yale Journal of Biology and Medicine
Amelioration of Symptoms and Reduction of VIP Levels after
Hepatic Artery Chemoembolization in a Patient with Sandostatin
Resistant VIPoma
Walid Shaib,a Kisha Mitchell,b and M. Wasif Saifb*
aHospital of Saint Raphael, New Haven, Connecticut
bYale University School of Medicine, New Haven, Connecticut
INTRODUCTION
We would like to report a case in which hepatic chemoembolization of a metastatic
hepatic lesion of VIPoma (Vasoactive Intestinal Polypeptide secreting islet cell tumor)
leads to a reduction of VIP (Vasoactive Intestinal Polypeptide) levels and resolution of
symptoms in a patient with pancreatic VIPoma unresponsive to increased doses of an
octreotide analog.
CASE REPORT
An 80-year-old Caucasian woman with a history of VIPoma diagnosed in 1997 was
treated for a 3.5 cm lesion in the head of the pancreas by Whipple procedure surgery
(Figure 1). She tolerated the surgery well, except for the development of diabetes
controlled with insulin postoperatively. In December 2004, follow-up CT imaging showed
a new 2.5 cm mass in the bed of the pancreas. She underwent another resection with
positive margins and one out of three lymph nodes positive for malignancy, for which
levels of VIP were >400 pg/ml (normal <75), chromogranin A 16.2 U/L (<31), gastrin16
pg/ml (<110) and serotonin 15 ng/ml (<71). Follow-up serial octreotide scans showed

stable disease. In May 2005, a follow-up octreotide scan showed the same unresectable
retropancreatic tumor with new involvement of the right hepatic lobe (Figure 2). Due to
the long and indolent course of the disease and because the patient was asymptomatic,
she was treated with Sandostatin long acting (LAR) depot monthly. In September 2006,
the patient complained of worsening diarrhea, up to 10 bowel movements in 24 hours.
Laboratory data showed that VIP levels were still >400 pg/ml. Patient was re-started on
a loading dose of short-acting Sandostatin at 150 micrograms subcutaneously every
eight hours for two weeks, followed by LAR Sandostatin 20 mg intramuscularly every 28
days. Due to persistent diarrhea, the dose of LAR Sandostatin was escalated by
increments of 10 mg every 28 days to a maximum dose of 100 mg. The VIP levels
continued to be high (>400 pg/ml), and diarrhea transiently improved. Another flare-up
occurred in March 2008, manifested by intractable diarrhea and severe metabolic
acidosis. Because there are no guidelines in the treatment and follow-up of this disease,
we elected to initiate treatment with 5 Fluorouracil (5-FU) and streptozocin, based on
reports and success rates. No improvement of diarrhea (consistency and frequency) was
noted on this treatment. 5-FU was changed to capecetabine with the same results as 5-
FU. She underwent chemo-ablation with mitomycin c, cisplatin, and doxorubicin. Her
hospital course after the chemoablation was complicated by pulmonary embolism, atrial
fibrillation, pneumonia, and vancomycin-resistant enterococcus bacteremia. After
treatment, her diarrhea improved to less than two stools per day. In addition, the VIP
levels decreased to122 pg/ml (Figure 3). Three months later, patient was started on
temozolomide as maintenance therapy.
DISCUSSION
VIPomas are neuroendocrine tumors that secrete excessive amounts of VIP that cause
distinct syndromes characterized by large-volume diarrhea, hypokalemia, and
dehydration. The annual incidence of these tumors is estimated to be about 1 per

10,000,000 individuals in the general population [1]. The mean age of VIPoma patients
is 49 years. This syndrome is also called Verner-Morrison syndrome, pancreatic cholera,
or WDHA (watery diarrhea, hypokalemia, and achlorhydria) syndrome. In addition to the
WDHA, patients can present with flushing secondary to the vasodilatory effect of the
VIP. These tumors are usually solitary, more than 3 cm in diameter and occur in the
pancreas in 80 percent to 90 percent of cases, mainly in the pancreatic tail (50 percent
to 75 percent) with 37 percent to 68 percent hepatic metastasis at diagnosis.
Demonstration of elevated levels (>75 pg/ml) of VIP confirms diagnosis in the clinical
setting [2,3]. For localizing and staging of these tumors, somatostatin receptor
scintigraphy with octreotide scan has been recommended as the best imaging technique
[4]. Treatment preferences depend on the presence of metastasis. In metastatic tumors,
long-acting somatostatin analogs are the drugs of choice. Somatostatin analogs are
typically initiated at 20 mg daily dosage, and gradual escalation of the dose as needed,
for optimal control of symptoms, is recommended [5]. Hepatic resection is indicated for
the treatment of metastatic liver disease in the absence of diffuse bilobar involvement,
compromised liver function, or extensive extrahepatic metastases [6].
Other treatment options have been described with no set recommendations. Interferon-
alfa added to octreotide is used as one of the modalities for treatment of refractory
diarrhea in these patients [7]. Experiences with chemotherapeutic agents are limited.
Fjallskoga et al. concluded that combined streptozotocin and liposomal doxorubicin is a
safe and efficient treatment for endocrine pancreatic tumors. The efficacy seems to be
comparable to that of combined streptozotocin and doxorubicin; whereas, the cardiac
toxicity clearly favors using the liposomal drug combination [8]. Streptozotocin plus 5-
fluorouracil produced objective responses in 17 out of 31 (54 percent) patients with a
median duration of response of 23 months [9].
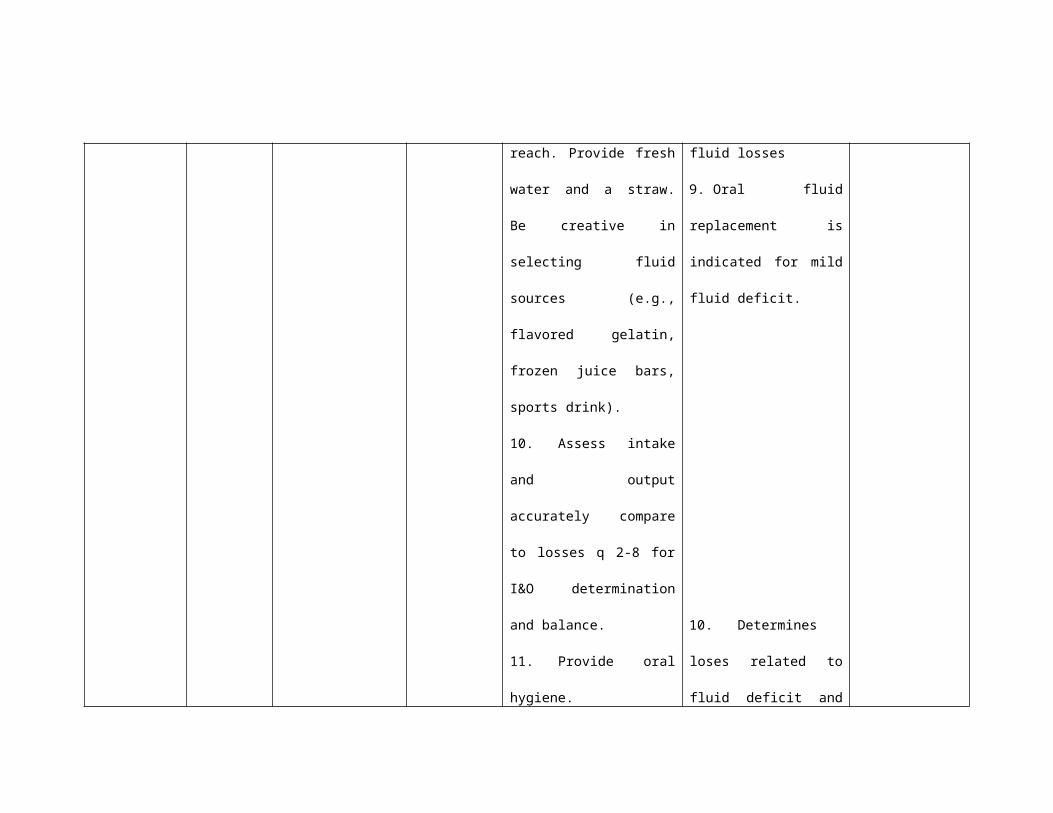
Medical management with octreotide analogs has proven useful in the management of
pancreatic islet cell tumors with unresectable disease and/or metastases [10,11].
Neuroendocrine gastrointestinal tumors express somatostatin receptors (sstrs) in 80
percent to 90 percent of cases, and somatostatin analogs have become increasingly
important in the management of these patients. Most of the currently available
somatostatin analogs bind to the sstr2 and sstr5 receptor types and in higher doses to
sst3 of the ssts 1-5 described. Clinical improvement during somatostatin analog therapy
is mainly mediated via a direct inhibitory effect on hormone production from the tumors,
seen in 30 percent to 70 percent of patients. Indirect non-tumor mediated effects on
peripheral target organs contribute to the subjective improvement achieved in 30 percent
to 70 percent of patients. Significant improvement of quality of life has been
demonstrated with long-acting depot formulations. There is little or no effect on tumor
growth during octreotide therapy. Tumor shrinkage has been reported in 10 percent to
20 percent of patients, but stabilization of tumor growth can be achieved in about half of
the patients in eight to 16 months after starting treatment. Induction of apoptosis has
been reported by octreotide analogs as a possible mechanism of action on these tumors
[12]. Octreotide inhibits hormone secretion by various neuroendocrine tumors and may
occasionally reduce metastatic tumor burden [13]. Varying data exist about the
quantitative reduction of tumor size and symptomatic relief. Oberg et al. reported a
significant tumor response in <5 percent of patients but a symptomatic response in 60
percent of patients [14]. Maton et al. observed 83 percent symptomatic response but
fewer than 20 percent reduction in tumor size [15]. A case report by Kraenzlin et al.
showed that long-acting Sandostatin not only controlled the diarrhea without side effects,
but also appeared to have possibly induced a reduction in metastatic tumor size.
Conventional measures of surgery, chemotheraphy, and hepatic artery embolization
ultimately failed to control the severity of diarrhea, resulting from vasoactive intestinal

polypeptide hypersecretion [16]. Cho and Vinik evaluated tumor blood flow using
angiography in eight patients with different types of neuroendocrine tumors receiving
octreotide. They found a marked decrease in blood flow in two patients with gastrinomas
and two patients with VIPomas, with a hypothesis that octreotide either decreases blood
flow to these tumors or decreases tumor size or hormonal secretion [17].
Contrary to all these reports, VIP hypersecretion kept elevating in our patient, although
long-acting octreotide analog doses were increased. Similar to our report, Lamberts et
al. reported two patients with metastatic VIPomas developed resistance to somatostatin
analog with regard to clinical and inhibitory effect [18]. An “escape phenomenon” to
somatostatin analog was noticed for a few days with a usual response after
discontinuation of the treatment [19]. In another report, 10 patients with metastatic
pancreatic endocrine tumors were treated with the long-acting somatostatin analog
octreotide. Three patients showed no response, clinically or biochemically, and
treatment was, therefore, withdrawn. The seven remaining patients continued treatment
for a median period of 28 months (range 13-54 months). Treatment was initially
effective, symptoms improved, and the concentrations of tumor-related hormones were
reduced. Worsening of symptoms and rising levels of tumor-related hormone
concentrations occurred at a median of five months (range 1-6 months) after the start of
therapy and were initially reversed by increasing the dose of octreotide over a median of
10 months (range 6-16 months). However, after a median of 13 months (range 5-34
months) at the maximum dosage, symptoms recurred and were no longer responsive to
a further increase in dosage of octreotide or other therapeutic measures. All patients
died within five months once this “resistance phase” of their illness had been reached
[20]. However, resistance was never confirmed on histological or biochemical studies.
Arterial chemoembolization is recommended for patients with significant symptoms who

have failed to respond to more conservative therapy and are not surgical candidates
[21].
For patients with hepatic metastasis, initial expectant observation and medical
management of symptoms is appropriate in view of the long and indolent course of the
disease. As mentioned earlier, hepatic resection is indicated for the treatment of
metastatic liver disease in the absence of diffuse bilobar involvement, compromised liver
function, or extensive extrahepatic metastases. VIPomas are often large or
metastasizing, but generally require surgical debulking to alleviate hormonal symptoms
and have favorable survival outcomes [6]. In a clinical trial conducted by Eriksson et al.,
patients having midgut, foregut carcinoids and neuroendocrine pancreatic tumors,
treatment of liver metastases by surgical resection and/or radiofrequency ablation (RFA)
was successful in patients with midgut carcinoids with only less success in reducing
symptoms in patients with foregut carcinoids or neuroendocrine tumors. In addition,
patients with non-functioning neuroendocrine tumors may benefit from debulking
procedure to reduce morbidity and improve survival. Proposal of surgical debulking or
RFA as means that limit procedure-related morbidity and efficiently alleviate symptoms
has been beneficial in these patients, especially as this disease has a high incidence of
recurrence [6,22]. Azimuddin et al. reported that hepatic arterial embolization is the
preferred management in these cases [23]. Case et al. confirmed the finding that hepatic
artery embolization can be very effective and durable as a treatment modality for
patients with metastatic VIPomas (or other neuroendocrine tumors) who are clinically
symptomatic from the effects of hormone hypersecretion. It is applied as a palliative
technique in symptomatic patients with unresectable hepatic metastasis [24].
Furthermore, the study of Gupta et al. at MD Anderson has compared embolization
alone to chemoembolization of the hepatic artery and has concluded that in pancreatic
islet cell tumors (without specifying the subtype of the tumor), chemoembolization has

improved response rate by 50 percent compared to 25 percent with embolization alone.
Moreover, chemoembolization of these tumors had a survival benefit as compared to
embolization alone (31.5 months vs. 18.2 months) [25]. Yao et al. demonstrated that for
unresectable but liver dominant disease, chemoembolization was the treatment of
choice, with median survival of 32 months post chemoembolization and a five-year
survival rate of 40 percent. Chemoembolization effectively controlled tumor growth and
alleviated symptoms in 90 percent of patients [26]. This modality helped in controlling the
symptoms of our patient. Moreover; the VIP levels trended down as shown by the graph
in Figure 3. Huang et al. concluded that treatment for metastatic pancreatic islet cell
tumors require a multidisciplinary approach. Metastasis of the tumor is not a
contraindication for aggressive therapy. Combined cytoreductive surgery and TACE can
relieve symptoms and are of benefit for patients with pancreatic islet cell tumors with
liver metastases [27].
Temozolomide is another treatment option for metastatic disease. As a monotherapy, it
has acceptable toxicity and antitumoral effects in a small series of patients with
advanced malignant neuroendocrine tumors with some radiologic responses [28].
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2844690/