-
8/19/2019 0413 Massive Upper GI Bleeding.pdf
1/12
UNDERSTANDING AND CARING FOR
CRITICAL ILLNESS IN EMERGENCY MEDICINE
EM Critical Care
Volume 3, Number 2
Authors
Ryan G. K. Mihata, MD, MPH, FACEPAssistant Professor of
Emergency Medicine/Critical Care,
Wright State University, Boonshoft School of Medicine,
Dayton, OH
John-Adam Bonk, MDDepartment of Emergency Medicine, Wright State
University,Boonshoft School of Medicine, Dayton, OH
Meaghan P. Keville, MDDepartment of Emergency Medicine, Wright
State University,Boonshoft School of Medicine, Dayton, OH
Peer Reviewers
Michelle Lin, MDAssociate Professor of Clinical Emergency
Medicine,University of California San Francisco; San Francisco
General Hospital and Trauma Center, San Francisco, CA
John L. Westhoff, II, MD, MPH, FACEPDeputy Commander for
Clinical Services, U.S. Army Public
Health Command Region-Pacic; Staff Emergency Physician,
U.S. Naval Hospital, Yokosuka, Japan
Guest Editor
Catherine A. Gogela Carlson, MDCritical Care Medicine Fellow,
Departments of Critical Care
Medicine and Emergency Medicine, University of PittsburghMedical
Center, Pittsburgh, PA
CME Objectives
Upon completion of this article, you should be able to:
1. Describe the differential diagnosis of massive
GIbleeding.
2. Discuss the importance of the resuscitation of patients
with massive GI bleeding.
3. List the available medical and surgical therapeutic
options for patients with massive GI bleeding.
4. Apply a standardized approach to the management of
massive GI bleeding.
Prior to beginning this activity, see the back page for
facultydisclosures and CME accreditation information.
Resuscitation Of ThePatient With Massive UpperGastrointestinal
BleedingAbstract
Managing an unstable patient with massive gastrointestinal
bleedingcan be challenging, but effective management can optimize
patientoutcomes. These patients require prompt recognition of
severe ill-
ness, resuscitation and stabilization, and diagnostic and
treatmentmodalities directed at identication and control of the
source of bleeding. Multiple consultants (including
gastroenterology, generalsurgery, and interventional radiology) are
often required, and earlyconsultation of these subspecialists can
improve morbidity and mor-tality. Underlying comorbidities add
complexity to the managementof the bleeding patient and are
associated with increased mortality.Most cases of massive bleeding
are due to an upper gastrointestinalsource, and these patients have
a higher mortality rate than thosepresenting with lower
gastrointestinal bleeding. Common sources ofupper gastrointestinal
bleeding include gastric and duodenal ulcers,esophageal and gastric
varices, and erosive esophagitis. Dependingon the source of the
bleeding, medical and/or surgical treatment mo-
dalities may be required. Utilization of emergent upper
endoscopyand other medical therapies as well as transfusion of
blood productsare often necessary to ensure optimal patient
outcomes. Knowledgeof the emergency procedures and medications
available, as well asfamiliarity with the treatment modalities used
by consultants, willhelp the emergency physician orchestrate the
care necessary to en-sure patient survival.
-
8/19/2019 0413 Massive Upper GI Bleeding.pdf
2/12
EMCC © 2013 2 www.ebmedicine.net • Volume 3,
Number 2
searched for guidelines for the acute treatment ofsevere GI
bleeding. Table 1 summarizes the currentguidelines related to
GI bleeding.3-6 The literaturereview and these guidelines
suggest a general con-sensus about the importance of early
evaluation andresuscitation in the ED as well as early
involvementof appropriate consultants in order to avoid
negativeoutcomes in patients with massive GI bleeding.
Etiology And Pathophysiology
The presence of GI bleeding with evidence of hem-orrhagic shock
requires prompt identication of the bleeding source. The most
common etiologies ofupper GI bleeding include: duodenal ulcers
(28%),gastric ulcers (26%), gastritis (13%), varices (12%),and
esophagitis (8%).1 GI bleeding due to esopha-geal or gastric
varices and peptic ulceration carrythe highest
mortality.2 Exclusion of other bleedingsources (such as
pulmonary or intranasal sources)is important. As with management of
all cases of
undifferentiated hypotension, initiation of resuscita-tion based
on hemodynamic decompensation shouldnot be delayed, regardless of
the underlying sourceof the bleeding.
Treatment
Stabilization And Monitoring
Initial resuscitation of patients with massive GI bleed-ing
involves restoration of intravascular volume inorder to achieve the
relative hemodynamic stabilityrequired to proceed with diagnostic
and therapeutic
interventions. An initial primary survey to evaluatethe airway,
breathing, and circulation should almostalways include endotracheal
intubation in order toprotect the patient’s airway in the setting
of activehemorrhage and to assist in identifying the bleedingsource
and facilitating these additional interventions.Early resuscitation
may start with 2 large-bore pe-ripheral intravenous (IV) catheters,
but resuscitationof massive hemorrhage may be aided by the use
oflarger, introducer-sized central venous catheters thatcan more
efciently restore lost intravascular volumeduring hemorrhagic
shock.
The importance of early mobilization of special-
ists cannot be overemphasized. In patients withmassive GI
bleeding, medical therapy alone isunlikely to be sufcient to
achieve hemostasis. Earlymobilization of the available
subspecialists expe-dites time to denitive therapy. The lack of
availablesubspecialty support should prompt considerationfor
transfer to a tertiary care facility that can providethis care.
Depending on the underlying cause of the bleeding as well as
patient comorbidities, gastroen-terology, general surgery, and
interventional radiol-ogy may all play a role in the care of these
patients.
Case Presentation
You receive a medic call for a 45-year-old male who called911
for massive hematemesis. The medics report that the patient is
an alcoholic who has been binge drinking sincelosing his job 1 week
ago. He has vomited a large amountof frank blood twice. He is
hypotensive, with a MAP of 50mm Hg and a pulse of 128 beats per
minute. EMS person-
nel have established a peripheral IV line and are infusingnormal
saline as fast as possible; they are 5 minutes out.After you page
the gastroenterologist and ask the unit sec-retary to activate your
institution’s massive transfusion protocol, you consider the
potential causes of massive GIbleeding, the available therapeutic
options, and the inter-ventions you should undertake in the next
few minutes toimprove this critically ill patient’s chance for
survival…
Introduction
Providing optimal care in the emergency depart-ment (ED) for
patients with massive gastrointesti-
nal (GI) bleeding requires coordination of multipleconsultants
as well as knowledge of both medicaland surgical therapeutic
options. For the purposesof this review, massive GI bleeding is
dened as bleeding in a patient that has resulted in
hemody-namic instability, with signs and symptoms consis-tent with
hemorrhagic shock and evidence of eitherhematemesis or
hematochezia. In order to provideinitial resuscitation in the ED
(either as a bridge tocontinued resuscitation in the intensive care
unitor to diagnostic/therapeutic interventions in theoperating room
or interventional radiology), emer-gency physicians must be
familiar with the widevariety of both diagnostic and therapeutic
options aswell as the underlying pathophysiology for massiveGI
hemorrhage. The majority (> 75%) of massiveGI bleeding cases are
due to an upper GI source.1 Mortality rates for patients with
massive GI bleedingrange from 20% to 39%.2 Treatment options
dependupon the underlying cause of the bleeding, andearly
intervention can mean the difference betweensurvival and death.
This issue of EMCC provides anoverview of the current evidence
for the treatment ofpatients with massive upper GI bleeding.
Critical Appraisal Of The Literature
A literature search of PubMed, Ovid MEDLINE® , andthe
Cochrane Library was performed using the fol-lowing keywords: GI
bleeding, severe GI bleeding, upperGI bleeding, and variceal
bleeding treatment. The searchfocused only on literature in
the English language foradult patients. More than 100 articles were
reviewed,which provided the background information and basis
for further literature review. Additionally, bothnational and
international guidelines as well as theCochrane Database of
Systematic Reviews were
-
8/19/2019 0413 Massive Upper GI Bleeding.pdf
3/12
3 EMCC © 2013www.ebmedicine.net • Volume 3, Number
2
In cases of nonvariceal hemorrhage, a bolus of aPPI should be
initiated and then followed by acontinuous infusion. This is
thought to promoteulcer healing and decrease the rate of
rebleeding.7 Additionally, in cases of variceal hemorrhage
withsubsequent endoscopic intervention, patients whoare given PPIs
intravenously have demonstrated lessrebleeding8 because PPIs
work against stomach acidand pepsin, which are thought to
destabilize plateletplugs and the hemostatic clot.9-11
Procedural Therapies
Endoscopy
Endoscopy is an important diagnostic and thera-peutic tool for
upper GI hemorrhage and should be performed promptly upon
patient stabilization.Endoscopy provides denitive therapy in
manycases. The gastroenterologist may employ variousendoscopic
techniques, including clips, banding,thermocoagulation, or
sclerosant injection with orwithout epinephrine. All patients with
massive GI
bleeding should be intubated to facilitate endos-copy,
control the airway, reduce the risk of aspira-
Patients with massive GI bleeding require con-tinuous
cardiac and pulse oximetry monitoring, withfrequent blood pressure
checks. Central venous accessmay be required in the ED if the
patient has poor pe-ripheral access or if more the rapid infusion
of uidsor blood products is needed. Invasive monitoring,including
an arterial line, will enable prompt recogni-tion and response to
the rapid changes in physiologythat may occur in massive GI
hemorrhage.
Initial laboratory values can help guide initialtherapy, but
serial coagulation studies in the ED arenot likely to aid in
decision making and may be dif-cult to interpret in patients being
treated with freshfrozen plasma (FFP), cryoprecipitate, or factor
concen-trate. Likewise, an initial D-dimer may offer prognos-tic
information, but it should not inuence immediatemanagement in the
acute setting.
Regardless of the source of upper GI bleeding,proton-pump
inhibitors (PPIs) are typically recom-mended until the etiology of
the bleeding can beidentied. While PPIs will not impact the
immedi-
ate stabilization of a hemodynamically unstable bleeding
patient, their use may improve outcomes.
Table 1. Current Guidelines For Gastrointestinal Bleeding
Organization Topic Type of Guideline Recommendations
American College of
Physicians
Management of patients
with nonvariceal upper
GI bleeding3
Consensus 1. Early evaluation, resuscitation, and risk
stratication is recom-
mended.
2. Nasogastric tube placement may have diagnostic value.
3. Transfuse PRBCs to maintain hemoglobin > 7 gm/dL.
4. Correction of coagulopathy is recommended but should not
delay
endoscopy.
5. Pre-endoscopic PPIs may be considered.6. Early endoscopy
(within 24 h) is recommended.
7. Histamine-2 receptor antagonists are not recommended for
patients
with acute bleeding due to a gastric or duodenal ulcer.
8. Somatostatin and octreotide are not routinely recommended
for
patients with acute ulcerative bleeding.
Cochrane Library Pharmacologic manage-
ment of patients with GI
bleeding4,5
Systematic review 1. Somatostatin analogues do not reduce
mortality in variceal GI
bleeding; however, they may reduce the need for blood
transfusion
by 0.5 units.
2. PPI administration prior to endoscopy for upper GI bleeds
sig-
nicantly reduces the number of patients with recurrent
serious
bleeding and the need for endoscopic intervention, but they have
no
effect on the need for surgery or risk of death.
Scottish Intercollegiate
Guidelines Network
Guidelines for initial treat-
ment of patients with
signicant GI bleeding6
Systematic review 1. PRBC transfusion should be considered after
loss of 30% of the
circulating blood volume.
2. PPIs should not be used prior to endoscopic diagnosis in
patients
presenting with an acute upper GI bleed.
3. Early endoscopic examination should be undertaken within 24 h
of
initial presentation, if possible.
4. Pr ior to endoscopic diagnosis, terlipressin (vasopressin
analogue)
should be given to patients suspected of variceal
hemorrhage.
5. Antibiotic therapy should be initiated in patients with
chronic liver
disease who present with acute upper GI bleeding.
6. Balloon tamponade should be considered as a temporizing
mea-
sure to gain hemostasis in uncontrolled variceal hemorrhage.
Abbreviations: GI, gastrointestinal; PPI, proton-pump inhibitor;
PRBC, packed red blood cell.
-
8/19/2019 0413 Massive Upper GI Bleeding.pdf
4/12
EMCC © 2013 4 www.ebmedicine.net • Volume 3,
Number 2
Additional Procedural Therapies
In severe cases of massive GI bleeding, where ur-gent endoscopy
is unable to provide a diagnosis ortherapy, urgent or emergent
angiography can beperformed to identify the location of the
hemorrhage.Angiography is indicated in patients with
nonvaricealupper GI bleeding when medical management andendoscopic
therapy have failed to control the bleed-ing. Angiographic
intervention should be consideredas an alternative to surgery in
patients who are highrisk for more invasive surgical
intervention.13 Angiog-raphy can detect bleeding at rates of
at least 0.5 mL/min with 100% specicity and variable
sensitivity(based on the rate).14 During angiography,
lesionscan be treated by use of vasopressin or
transcatheterembolization.
Another option for identifying the source of bleeding is
radionuclide imaging, which can de-tect bleeding occurring at
slower rates than can bedetected by angiography. The primary
purpose ofthese studies is to localize the source of the bleed-
ing and to facilitate surgical intervention. An emer-gency
surgical consult should be sought in patientswith massive
hemorrhage who cannot be stabilizedin the ED, who have
contraindications to endos-copy, or who have peritoneal signs on
examination(which can occur from a ruptured peptic ulcer).While
surgery is typically only considered as a lastresort after medical,
endoscopic, and interventionalradiology approaches have been
exhausted or arecontraindicated, not all types of bleeding (such
asvariceal bleeding) are amenable to surgical interven-tion.
Nonetheless, early involvement of surgery andgastroenterology
services can facilitate a cooperative
treatment approach and may make surgical inter-vention, if
necessary, safer and less emergent.
Pharmacologic Therapies
There are multiple proposed pharmacologic treat-ments for the
management of acute upper GI bleed-ing. Understanding the mechanism
of action of these
tion, and improve patient safety during treatment.Airway
management in severe upper GI bleeds can be technically
challenging due to poor visualization.A topic within itself that
cannot be covered in this is-sue, extra personnel and airway
adjuncts (including2 suction catheters) is advisable for airway
manage-ment of this population.
Balloon Tamponade
Balloon tamponade may be required if endoscopy iseither not
available or not successful in achieving he-mostasis. Insertion of
a balloon tamponade device isa rare but potentially life-saving
procedure. It can beused as a temporary rescue device by providers
whopractice in a setting where specialty consultation isnot readily
available. Use of a balloon-tamponadedevice is associated with a
high risk of rebleedingupon balloon deation. Its most lethal
complicationis esophageal necrosis and rupture.
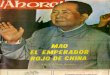
There are several different types of commerciallyavailable
devices for balloon tamponade. The 3 most
common include the Sengstaken-Blakemore, theMinnesota tube, and
the Linton-Nachlas tube.12 (SeeFigure 1.) Each of these tubes
varies slightly basedon the number of lumens and balloons.
Providersshould be familiar with the specic device used attheir
institution. The following is a general guide fortheir use:1. Prior
to insertion, secure the airway.2. After applying a lubricant to
the tube, insert the
tube through the mouth or nostril to a depth ofat least 50 cm,
depending upon the height of thepatient.
3. After evaluation by air injection, conrm place-
ment in the stomach with radiography. (The bal-loon should NOT
be inated until its location isveried radiographically so as to
avoid potentialcomplications associated with malpositioning ofthe
tube.)
4. Inate the gastric balloon (approximately 400-500 mL of air),
and clamp the inlet.
5. Retract the tube until resistance is felt (the bal-loon at
the gastroesophageal junction). Tensionmust be maintained on the
tube in order toproduce the tamponade effect.
6. If gastric balloon tension is not sufcient to stopthe
hemorrhage, inate the esophageal balloon
(25-30 mm Hg). This pressure must be checkedfrequently, as
overination can lead to esopha-geal necrosis.
It is important to remember that these are tem-porizing devices
intended for short-term use and arenot denitive therapy. In some
situations, the patientmay need to be transferred to another
facility fordenitive care.
Figure 1. Minnesota Tube For BalloonTamponade
Note both the gastric and esophageal balloons. Types of tubes
vary
slightly. Be familiar with the type available in your
institution.
Image courtesy of Ryan G. K. Mihata, MD
-
8/19/2019 0413 Massive Upper GI Bleeding.pdf
5/12
5 EMCC © 2013www.ebmedicine.net • Volume 3, Number
2
bleeding from esophageal varices.4 Some data sug-gest
that the combination of these medications withupper endoscopy may
be benecial.
Given their relatively low-risk side-effect pro-les, the use of
these medications can be consideredin patients with acute
hemorrhage that is possiblycaused by variceal bleeding.16
Vasopressin
A third class of pharmacologic agents, vasopressinand its
analogues, can reduce portal hypertension bycausing systemic and
splanchnic vasoconstriction.
Much like somatostatin, the use of vasopressinin the management
of upper GI bleeding is contro-versial. The risks (eg, myocardial
infarction, arrhyth-mias, mesenteric ischemia, peripheral soft
tissue ne-crosis, cardiac arrest) of using this medical therapyare
similar to—but usually less severe than—thoseseen with the use of
other vasopressor medications.In patients with variceal bleeding,
adding nitro-glycerin to vasopressin therapy appears to
decrease
systemic complications from the use of vasopressinalone while
not affecting the efcacy of the vaso-pressin.17,18 In patients
with massive GI bleeding, therisk of systemic vasoconstriction and
the potentialfor end-organ ischemia must be weighed againstthe
potential benet of splanchnic vasoconstriction,which can help to
achieve hemostasis in the actively bleeding patient.
In spite of the potential deleterious effects ofvasopressin, use
of vasopressin (or vasopressin plusnitroglycerin) in a patient in
extremis due to massiveGI bleeding may be justied.
Blood Product TransfusionThe goal of blood product transfusion
for acute bleeding is to replace the blood cells and
coagulationfactors that are being lost. Whole blood is a
complexheterogeneous solution that serves 3 basic func-tions: (1)
to maintain intravascular volume, (2) toprovide oxygen-carrying
capacity, and (3) to providethe coagulation factors that are
required to reversecoagulopathy and to assist in achieving (and
main-taining) hemostasis. The ability to achieve hemostasiscan be
complicated by the use of anticoagulation orantiplatelet agents.
Because there are inherent risks
involved with transfusing blood products, the risksmust be
considered along with the potential benetsfor each individual
patient. Goal #1: Provide Intravascular Volume
Resuscitation
Prompt volume resuscitation with IV crystalloiduids should be
initiated in a bleeding, hypotensivepatient in order to achieve a
perfusing mean arterialpressure (MAP) until blood products are
available.Given that it lacks oxygen-carrying capacity anddoes not
replenish clotting factors, the role of crystal-loid uid for volume
resuscitation should ideally
medications can facilitate a deeper understanding ofthe
rationale for the existing guidelines for their use.
Proton Pump Inhibitors
PPIs, which include omeprazole, pantoprazole, andesomeprazole,
are considered to be a mainstay ofearly therapy for acute GI
bleeding in the ED. PPIssuppress gastric acid stimulation by
inhibiting the pa-rietal cell H+/K+ ATPase (adenosine
triphosphatase)pump. One potential benet of the early use of
PPIsmay be the reduction of hemorrhage during
endos-copy.3,5 Additionally, PPIs may create a more
optimalenvironment for the stabilization of blood clots
byneutralizing the intraluminal gastric acid that wouldotherwise
serve to promote continued bleeding.9
There has been concern about the potentialincreased risk of
thrombotic stroke or myocardialinfarction with the addition of PPIs
to long-termclopidogrel therapy. Based on cohort studies, a
2009United States Food and Drug Administration warn-ing cited a 50%
increased risk of these complications
when PPIs and clopidogrel were taken concurrently.15
However, current data are inconclusive and suggestthat
these complications are typically associated withlong-term use of
PPIs and clopidogrel. These riskshave not yet been described in the
acute, short-termuse of these medications during the stabilization
ofpatients with massive GI bleeding. At this time, guidelines
continue to encourage theuse of PPIs (either before or immediately
followingupper endoscopy) in patients with undifferentiatedupper GI
bleeding.3 However, there has not yet beena study showing a
statistical improvement in the rateof rebleeding, the need for
surgical intervention, or
mortality from their use. Nonetheless, their cost effec-tiveness
and excellent safety prole make the benetof giving these agents
greater than the potential risks,particularly in high-risk patient
populations.
Somatostatin
Somatostatin and its analogues (including octreo-tide and
vapreotide) represent another class ofpharmacologic agents that may
be used early in themanagement of acute GI bleeding due to a
suspect-ed variceal source. Somatostatin (also known
as“growth-hormone-inhibiting hormone”) suppressesthe release of GI
hormones such as gastrin, chole-
cystokinin, motilin, and secretin. The secondaryeffects of
blocking the release of these hormonesinclude a reduction of portal
venous blood owdue to splanchnic vasoconstriction and
subsequentdecreased GI bleeding.
To date, there are minimal data regarding theuse of somatostatin
or its analogues for nonvaricealupper GI bleeding. The data on
their use in severevariceal bleeding are also mixed. A Cochrane
reviewfound no signicant change in mortality, the rebleed-ing rate,
or the number of units of blood transfusedwith the use of
somatostatin in patients with acute
-
8/19/2019 0413 Massive Upper GI Bleeding.pdf
6/12
EMCC © 2013 6 www.ebmedicine.net • Volume 3,
Number 2
myocardial oxygen delivery.22 However, for patientswith
suspected variceal bleeding (even with con-comitant coronary artery
disease), consider keepingthe hemoglobin goal to between 7 and 8
gm/dL untilhemostasis is achieved, as the additional blood vol-ume
required to achieve this higher target may leadto increased portal
pressure and worsening bleedingor rebleeding.
When there is a need for emergent transfusionof PRBCs for acute
blood loss anemia with signs ofhypovolemic shock, O-negative PRBCs
(or O-positivePRBCs in women past childbearing age and in men)can
be given until type-specic crossmatched blood isavailable. For
patients requiring massive transfusionof blood products, it is
important to remember that thetransfusion will have metabolic
complications such asdepletion of intravascular cations due to
chelation bythe sodium citrate used to anticoagulate blood
compo-nents during storage. Citrate is primarily
metabolized by the liver, so in cirrhotic patients receiving
massivetransfusion, this effect may be more profound. For
these patients, consider giving calcium replacement(calcium
gluconate 1-2 g IV or calcium chloride 0.5-1g IV per 500 mL of
transfused blood). Magnesium canalso be affected, and low levels
have unwanted sideeffects and should be repleted as necessary,
keepingin mind that overly rapid infusion of magnesium
canexacerbate hypotension.
Goal #3: Reverse Coagulopathy
Treatment of coagulopathy can be tailored to itslikely or known
etiology. Coagulopathy may arisedue to an underlying chronic
disorder, but it mayalso be caused by metabolic acidosis due to
tissue
hypoxemia in the setting of acute hypotension.To reverse
coagulopathy, consider an initial
transfusion of 10 mL/kg of FFP. Prothrombintime
(PT)/international normalized ratio (INR),partial thromboplastin
time (PTT), platelet count,and brinogen levels can be used to guide
patientmanagement. While there are no specic guidelines,keeping the
platelet count > 50,000/mm3 , PTT< 60 seconds, and INR
< 1.8 is common practice andis recommended by the authors.
Because D-dimerlevels have been shown to be inversely related
toprognosis in upper GI bleeding, a D-dimer may bedrawn as a
prognostic marker, but it has no role in
guiding intervention.23 If available, the
thromboelas-tography (TEG) test can evaluate platelet functionand
coagulation and may be more efcient to directthe type of
transfusion products necessary.
The role of recombinant activated factor VII(rFVIIa) is
continuing to evolve. While it may beuseful in certain situations
(eg, when a patient ison a direct thrombin inhibitor), it is
expensive, itcarries the risk of thromboembolic complications,and
studies of its use have had conicting results. Aprospective
randomized trial of 245 patients foundno benet with rFVIIa over
standard therapy for
be restricted to this early phase of resuscitation in
a bleeding patient. In cirrhotic patients with
suspectedvariceal hemorrhage, excessive crystalloid resuscita-tion
may be particularly harmful due to their suscep-tibility to
extravascular uid shifts in the setting ofunderlying low
intravascular oncotic pressure.
In patients with massive GI bleeding (especiallythose with
hemoglobin < 8.0 gm/dL, coagulopathy,or persistent hypotension
despite volume infusion),the use of blood products (such as PRBCs)
is im-portant in order to restore hemodynamic stabilityand to
achieve hemostasis. However, transfusion ofPRBCs alone is not
sufcient because they do notcontain the required coagulation
factors. For thisreason, PRBCs should be accompanied by FFP and/or
platelets. The military literature on traumatic bloodloss
recommends a PRBC:FFP:platelet ratio approach-ing
1:1:1.19,20 Other sources disagree on the exactratio, citing a
lack of a specic survival benet to ahigher PRBC to FFP
ratio.21 Many large centers havemassive transfusion protocols
that allow the rapid
release of blood products in varying ratios. While thesurvival
benet remains unclear, most protocols havePRBC:FFP:platelet ratios
near 1:1:1. Goal #2: Optimize Oxygen-Carrying Capacity
The goal of improving oxygen-carrying capacity bytransfusing
PRBCs is to ensure sufcient oxygendelivery to the tissues in order
to prevent end-organ ischemia and secondary dysfunction.
Clinicalsigns and symptoms of decreased oxygen deliverycan
include:• Decreased level of consciousness• Evidence of cardiac
ischemia (as shown by elec-
trocardiographic changes or troponin elevation)• Increasing
serum lactate• Decreased central venous oxygen saturation
(ScvO2)
The International Consensus guidelines recom-mend maintenance of
hemoglobin levels between 7and 8 gm/dL.3 However, there are no
randomizedcontrolled trials to suggest an exact hemoglobin goalfor
transfusion. Target hemoglobin levels should beindividualized for
each patient and should be basedupon the suspected etiology of the
bleed (ie, varicealvs nonvariceal hemorrhage) as well as patient
comor-
bidities. In the setting of ongoing massive bleeding,the
recommended hemoglobin level of 7 to 8 gm/dLshould not be
considered to be an endpoint of resus-citation. Instead, a MAP of
> 60 mm Hg and evidenceof adequate end-organ perfusion should be
the target.
Though the International Consensus guidelinessuggest maintenance
of hemoglobin between 7 and8 gm/dL, patients with certain
comorbidities mayrequire greater hemoglobin goals. For
instance,evidence suggests that patients with suspected
activeischemic coronary artery disease may benet froma target
hemoglobin closer to 10 gm/dL to support
-
8/19/2019 0413 Massive Upper GI Bleeding.pdf
7/12
7 EMCC © 2013www.ebmedicine.net • Volume 3, Number
2
rate of 1 mg/min is necessary to achieve a sustainedreversal of
the INR; however, it is insufcient whengiven as a single agent, as
it has an onset of action of2 to 6 hours and requires up to 24
hours to achieve acomplete response.27 For this reason, FFP
must also be administered. Although controversial,
rFVIIa can be consid-ered for reversal of effects of warfarin.
However,it is expensive, it has minimal proven
therapeutic benet for warfarin reversal, it is not FDA
ap-proved for this use, and its use may cause throm- botic
complications.24-26
Dabigatran: Dabigatran (Pradaxa®) is a directthrombin
inhibitor. To quantify the degree ofdabigatran coagulopathy, obtain
a PTT andthrombin time (if rapidly available).28 PT/INR is
notuseful in assessing dabigatran coagulopathy. ThePTT is only
useful to qualitatively assess the degreeof coagulopathy because it
lacks sufcient sensitivitywith therapeutic dabigatran levels. A
very high PTT
value should be conrmed by another method (eg,thrombin
time),28 although this may be impracticalin the emergent
setting. Like other anticoagulantmedications, even therapeutic
levels may requirereversal in the setting of active bleeding.
At this time, an evidence-based reversal strategyfor dabigatran is
not available. Many institutionshave a pathway for bleeding
patients who are ondabigatran that may inform local practice
patterns.Management strategies may range from expectantmanagement
to aggressive use of blood products,including FFP and even
hemodialysis.
Rivaroxaban: Rivaroxaban (Xarelto®) is a factorXa inhibitor.
Administer PCCs for reversal ofrivaroxaban; if PCCs are not
available, consideradministration of FFP.29
nonvariceal upper GI bleeding.24 However, a
smalluncontrolled study suggested that, in patients withliver
disease and an increased INR refractory to FFPtherapy, rFVIIa was
effective in stopping bleedingand normalizing the
INR.25 Similarly, a study of pa-tients with moderate to severe
cirrhosis showed thatadministration of rFVIIa in addition to
endoscopichemostatic strategies decreased rebleeding
rates.26 Due to the conicting nature of the literature, use
ofrFVIIa in patients with massive GI bleeding is notroutinely
recommended.
It should be noted that, although the transfu-sion of blood
products is indicated in patients withmassive GI bleeding, it is
associated with somerisks. The lethal triad of hypothermia,
coagulopa-thy, and acidosis must be addressed in order toprevent
clinical deterioration. (See Figure 2.) Usewarmed uids, warmed
blankets, and other pas-sive external rewarming measures as needed
tomaintain normothermia.
Reversal Of Medically Induced Coagulopathy Warfarin:
Warfarin (Coumadin® , Jantoven®)inhibits vitamin K-dependent
coagulation factorsynthesis. Prothrombin complex concentrates(PCCs)
should be the rst-line treatment in apatient who is on warfarin.
PCCs do not requirecrossmatch and act more quickly than FFP
alone;however, because PCCs in the United States donot contain
signicant amounts of factor VII,FFP must also be administered.
Dosages areindividually calculated based on weight anddesired
factor IX level; 1 unit/kg will increase thefactor IX level
approximately 1%.
If PCCs are not available, coagulopathy can bereversed by
discontinuing warfarin therapy andadministering vitamin K. Vitamin
K at a dose of 5to 10 mg diluted in D5W or D5 saline infused at
a
Figure 2. Coagulopathy Chart
Reprinted from: Cherkas D. Traumatic Hemorrhagic Shock: Advances
In Fluid Management. Emerg Med Pract. 2011;13(11):1-20.
Copyright © 2011 EB Medicine.
Hemorrhage Tissue damageHypothermia
Fluid replacement ShockAcidosis
Dilution Hypoperfusion
Consumption of platelets and clotting
factorsInammation Hyperbrinolysis
Coagulopathy
-
8/19/2019 0413 Massive Upper GI Bleeding.pdf
8/12
EMCC © 2013 8 www.ebmedicine.net • Volume 3,
Number 2
This clinical pathway is intended to supplement, rather than
substitute for, professional judgment and may be changed depending
upon a patient’s individualneeds. Failure to comply with this
pathway does not represent a breach of the standard of care.
Copyright © 2013 EB Medicine. 1-800-249-5770. No part of this
publication may be reproduced in any format without written consent
of EB Medicine.
Class I
• Always acceptable, safe
• Denitely useful
• Proven in both efcacy andeffectiveness
Level of Evidence:
• One or more large prospective
studies are present (with rare
exceptions)
• High-quality meta-analyses
• Study results consistently posi-
tive and compelling
Class II
• Safe, acceptable
• Probably useful
Level of Evidence:
• Generally higher levels of
evidence
• Non-randomized or retrospec-
tive studies: historic, cohort, or
case control studies
• Less robust randomized con-
trolled trials
• Results consistently positive
Class III
• May be acceptable
• Possibly useful
• Considered optional or alterna-tive treatments
Level of Evidence:
• Generally lower or intermediate
levels of evidence
• Case series, animal studies,
consensus panels
• Occasionally positive results
Indeterminate
• Continuing area of research
• No recommendations until
further research
Level of Evidence:
• Evidence not available
• Higher studies in progress
• Results inconsistent, contradic-
tory
• Results not compelling
Signicantly modied from: The
Emergency Cardiovascular Care
Committees of the American
Heart Association and represen-
tatives from the resuscitation
councils of ILCOR: How to De-
velop Evidence-Based Guidelines
for Emergency Cardiac Care:Quality of Evidence and Classes
of Recommendations; also:
Anonymous. Guidelines for car-
diopulmonary resuscitation and
emergency cardiac care. Emer-
gency Cardiac Care Committee
and Subcommittees, American
Heart Association. Part IX. Ensur-
ing effectiveness of community-
wide emergency cardiac care.
JAMA. 1992;268(16):2289-2295.
Class Of Evidence Definitions
Each action in the clinical pathways section of EM Critical
Care receives a score based on the following
denitions.
Clinical Pathway For The Initial Management OfPatients With
Massive Upper Gastrointestinal Bleeding
Initial actions: insert 2 large-bore IVs (Class I); establish
monitoring
(Class I); provide a PPI bolus & drip (Class I); consider
insertion of
a nasogastric tube (Class II); provide a crystalloid bolus
(Class II);
and keep the patient warm (Class II)
Are there signs of altered mental status and/or
active hematemesis?
Intubate (Class II)
Transfuse PRBCs, FFP, and platelets (Class II)
Coagulopathy (INR > 1.7
with active bleeding)
Administer:
Octreotide 50-mcg bolus and 50-mcg/h infusion (Class II)
and
Ciprooxacin 400 mg bid (Class I) or ceftriaxone 1g IV qd
(Class II)
Anemia
Are there signs or symptoms of shock?
Is there a history of esophageal varices or signs of
cirrhosis?
• Perform labs: CBC with differential, BMP, LFTs, PT/PTT, ECG,
CXR
• Consider: D-dimer, lactate, ABG
• If hemoglobin < 7.0 gm/dL: transfuse PRBCs (Class II)
• If hemoglobin > 8.0 gm/dL (or with bleeding varices): do
not
transfuse PRBCs (Class II)
• Transfuse 2 units FFP (Class II)
• If there is severe liver disease with coagulopathy and
refractory
bleeding, consider PCCs or rFVIIa (Class II)
• If the patient is taking warfarin, add vitamin K 10 mg slow
IV
push (Class II)
YES
YES
YES
NO
NO
NO
Abbreviations: ABG, arterial blood gas; bid, two times a day;
BMP, basic metabolic panel; CBC, complete blood count; CXR, chest
x-ray; ECG, elec-
trocardiogram; FFP, fresh frozen plasma; INR, international
normalized ratio; IV, intravenous; LFT, liver function test; PCCs,
prothrombin complex
concentrates; PPI, proton-pump inhibitor; PRBCs, packed red
blood cells; PT, prothrombin time; PTT, partial thromboplastin
time; qd, 1 time a day;
rFVIIa, recombinant activated factor VII.
-
8/19/2019 0413 Massive Upper GI Bleeding.pdf
9/12
9 EMCC © 2013www.ebmedicine.net • Volume 3, Number
2
The foundation of the resuscitation includesinitial
management of the airway, breathing, andcirculation. Volume
resuscitation requires crystal-loid uids and transfusion of blood
products. Earlyconsultation with gastroenterology,
interventionalradiology, and general surgery will improve
thepatient’s time to denitive care. Endoscopy should beperformed
promptly upon stabilization. In additionto volume resuscitation,
medical therapies such asPPIs, somatostatin and its analogues, and
vasopressinshould be considered either empirically based
uponhemodynamic stability of the patient or directed atthe
underlying etiology of the bleeding, if known.Surgical intervention
may ultimately be necessary ifless-invasive treatments fail or are
contraindicated.Depending on the clinical scenario, balloon
tampon-ade may be needed as a temporizing and life-sustain-ing
measure until the resources required for denitivetherapy become
available.
Case Conclusion
The critically ill 45-year-old male patient arrived to
yourresuscitation bay with vital signs that were
unchanged from the prehospital report. You made a decision to
intubatethe patient in order to protect his airway and to
facilitateanticipated upper endoscopy. Shortly after intubation,the
patient continued to have frank blood coming from hisoropharynx.
The nurses established a second large-bore peripheral IV, and
emergency release blood was given. Eachlarge-bore peripheral IV had
blood infusing, and the initialhemoglobin came back at 5.8 gm/dL.
You ordered 4 moreunits of type-specic blood as well as 2 units of
FFP and 2single-donor units of platelets, and you subsequently
placed
an introducer catheter to expedite large volume infusion ofblood
products via a level 1 infuser, which warmed the in-
fusing uid. The gastroenterologist came and performed
anendoscopy in the ED, during which he attempted to bandthe large
esophageal varices. He was uncertain whether ornot he was able to
obtain complete hemostasis during the procedure. The patient
initially improved with your re-suscitation but continued to have a
MAP in the 50s and a pulse rate in the 120s. You administered
an octreotide bolusand infusion as well as a PPI infusion. In
consultation with your intensivist team, you started a
vasopressin drip witha goal MAP of > 60 mm Hg. This improved not
only thevariceal bleeding but also the patient’s hemodynamic
stabil-ity. In total, the patient required 4 more units of PRBCsand
2 more units of FFP. He was admitted to the ICU,where the
gastroenterologist repeated an endoscopy and found less blood
but 2 more bleeding varices, which weresubsequently banded. The
patient developed renal failureand liver failure (acute on chronic)
with ischemic hepatitissecondary to hemorrhagic shock. He had a
prolonged coursein the ICU but eventually improved and was
ultimatelydischarged from the hospital.
Unfractionated Heparin: Unfractionated heparin actsat multiple
sites in the clotting cascade and serves asa catalyst for clotting
factors. Administer protaminesulfate to reverse heparin.
Clopidogrel: Clopidogrel (Plavix®) is a nonreversibleplatelet
inhibitor. Empiric transfusion of plateletscan be considered for
patients on clopidogrel orother platelet inhibitors (such as
aspirin), althoughno randomized controlled trials have
demonstrateda favorable impact with this approach.
Special Circumstances
When treating a patient who refuses blood basedon religious
beliefs (eg, Jehovah’s Witnesses), itis important to ask the
patient or legal guardianwhether they are willing to receive blood
prod-ucts. Even though the patient may be a Jehovah’sWitness, it is
important to carefully establish anddocument the patient’s current
medical wishes. In a
small case study, investigators found a portion of
a Jehovah’s Witness congregation who would accept blood
transfusions because they disagreed with theofcial
doctrine.30 Further, The Watchtower, a legalorganization of
the Jehovah’s Witnesses, asserts withrespect to blood transfusion:
“Ultimately, you (thepatient or the parent) must decide. Because
your (oryour child’s) body, life, ethics, and relationship withGod
are involved.”31 Regardless of the patient’s orpower of
attorney’s decision, carefully documentconversations about risk and
benet as well as thesubsequent management based on that
decision.
Disposition
Most patients who present to the ED with massiveGI bleeding will
ultimately require admission to theintensive care unit, although
this will depend on thesuccess of early intervention and the
clinical stabilityof the patient. Consideration should be made
earlyfor involvement of subspecialists. Facilities
withoutgastroenterology, general surgery, or
interventionalradiology backup should have a rapid
interfacilitytransfer protocol in place to expedite patient
transferto a facility capable of providing the denitive man-
agement that will be needed after the initial resusci-tation and
stabilization.
Summary
The unstable patient with massive upper GI bleed-ing is a
high-risk case for the emergency physi-cian, requiring the
coordination of resources andconsideration of various treatment
modalities.Initial resuscitation efforts should occur
concomi-tantly, with diagnostic measures aimed at ndingthe etiology
of the bleed.
-
8/19/2019 0413 Massive Upper GI Bleeding.pdf
10/12
EMCC © 2013 10 www.ebmedicine.net • Volume 3,
Number 2
Accessed March 1, 2013. (Practice management guideline)7. Chan
WH, Khin LW, Chung YF, et al. Randomized controlled
trial of standard versus high-dose intravenous omeprazoleafter
endoscopic therapy in high-risk patients with acutepeptic ulcer
bleeding. Br J Surg. 2011;98(5):640-644. (Prospec-tive randomized;
122 patients)
8.* Hidaka H, Nakazawa T, Wang G, et al. Long-term
admin-istration of PPI reduces treatment failures after
esophagealvariceal band ligation: a randomized, controlled
trial. JGastroenterol. 2012;47(2):118-126. (Prospective
randomized;43 patients)
9. Green FW Jr, Kaplan MM, Curtis LE, et al. Effect of acid
andpepsin on blood coagulation and platelet aggregation. A
pos-sible contributor prolonged gastroduodenal mucosal hemor-rhage.
Gastroenterology. 1978;74(1):38-43. (In vitro study)
10. Berstad A. Does profound acid inhibition improve
hae-mostasis in peptic ulcer bleeding? Scand J
Gastroenterol.1997;32(4):396–398. (Review article)
11. Vreeburg EM, Levi M, Rauws EA, et al. Enhanced
mucosalbrinolytic activity in gastroduodenal ulcer haemorrhageand
the benecial effect of acid suppression. Aliment Pharma-col Ther.
2001;15(5):639–646.(Prospective observational; 29patients)
12. Borquez E, Swadron S, Winter M, et al. The unstable
patientwith gastrointestinal hemorrhage. In: Emergency
DepartmentResuscitation of the Critically Ill. American College of
Emer-gency Physicians (Ed), Dallas 2011. (Book chapter)
13. Millward SF. ACR Appropriateness Criteria on treatment
ofacute nonvariceal gastrointestinal tract bleeding. J Am
CollRadiol. 2008;5(4):550-554. (Consensus statement)
14. Fiorito JJ, Brandt LJ, Kozicky O, et al. The diagnostic
yieldof superior mesenteric angiography: correlation with
thepattern of gastrointestinal bleeding. Am J
Gastroenterol.1989;84(8):878-881. (Retrospective; 58 patients)
15. FDA. Public health advisory: updated safety informationabout
a drug interaction between clopidogrel bisulfate (mar-keted as
Plavix) and omeprazole (marketed as Prilosec andPrilosec OTC).
Available at:
http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatient-sandProviders/DrugSafetyInformationforHeathcareProfes-sionals/PublicHealthAdvisories/ucm190825.htm.
AccessedMarch 1, 2013. (FDA public health advisory)
16. Corley DA, Cello JP, Adkisson W, et el. Octreotide for
acute
esophageal variceal bleeding: a meta-analysis.
Gastroenterol-ogy. 2001;120(4):946-954. (Meta-analysis; 475
patients)
17. Tsai YT, Lay CS, Lai KH, et al. Controlled trial of
vasopressinplus nitroglycerin vs. vasopressin alone in the
treatment of
bleeding esophageal varices. Hepatology.
1986;6(3):406-409.(Prospective randomized controlled trial; 39
patients)
18. Gimson AE, Westaby D, Hegarty J, et al. A randomized trialof
vasopressin and vasopressin plus nitroglycerin in the con-trol of
acute variceal hemorrhage. Hepatology. 1986;6(3):410-413.
(Prospective randomized trial; 72 bleeding episodes in57
patients)
19. Borgman MA, Spinella PC, Perkins JG, et al. The ratio
of blood products transfused affects mortality in
patientsreceiving massive transfusions at a combat support
hospital.
J Trauma. 2007;63(4):805-813. (Retrospective; 246
patients)20. Perkins JG, Cap AP, Andrew CP, et al. An evaluation of
the
impact of apheresis platelets used in the setting of
massivelytransfused trauma patients. J Trauma. 2009;66(4
Suppl):S77-S84. (Retrospective; 694 patients)
21. Scalea TM, Bochicchio KM, Lumpkins K, et al. Early
aggres-sive use of fresh frozen plasma does not improve outcome
incritically injured trauma patients. Ann Surg.
2008;248(4):578-584. (Prospective; 806 patients)
22. Hébert PC, Yetisir E, Transfusion Requirements in Criti-cal
Care Investigators for the Canadian Critical Care TrialsGroup, et
al. Is a low transfusion threshold safe in criticallyill patients
with cardiovascular diseases? Crit Care Med.2001;29(2):227-234.
(Prospective randomized; 357 patients)
23. Gutiérrez A, Sánchez-Payá J, Marco P, et al. Prognostic
valueof brinolytic tests for hospital outcome in patients withacute
upper gastrointestinal hemorrhage. J Clin Gastroenterol.
Must-Do Markers Of Quality Care
• Control the airway by endotracheal intubationprior to
endoscopy.
• Establish central venous access after inserting2 large-bore
peripheral IVs and utilizing an in-troducer to facilitate
high-volume infusions andcentral venous pressure monitoring.
Consider
the internal jugular vein as the location for cen-tral line
placement in coagulopathic patients dueto vascular compressibility.
Line placement withultrasound guidance is the standard of care.
• Initiate volume resuscitation with crystalloid u-ids and
O-negative blood (if available). Switchto type-specic crossmatched
blood as soon as it becomes available.
• Consider transfusion of other blood products orinfusions of
medications based on the suspectedetiology of the bleed and the
patient’s comor- bidities.
• Aggressively treat hypothermia and acidosis in
order to facilitate correction of coagulopathy.
References
Evidence-based medicine requires a critical ap-praisal of the
literature based upon study methodol-ogy and number of subjects.
Not all references areequally robust. The ndings of a large,
prospective,randomized, and blinded trial should carry moreweight
than a case report.
To help the reader judge the strength of eachreference,
pertinent information about the study,such as the type of study and
the number of patientsin the study, will be included in bold type
followingthe reference, where available. In addition, the
mostinformative references cited in this paper, as deter-mined by
the authors, will be noted by an asterisk (*)next to the number of
the reference.
1. Peura DA, Lanza FL, Gostout CJ, et al. The American Collegeof
Gastroenterology Bleeding Registry: preliminary ndings.Am J
Gastroenterol. 1997;92(6):924-928. (Retrospective survey;1235
respondents)
2.* Afessa B. Triage of patients with acute gastrointestinal
bleed-ing for intensive care unit admission based on risk
factorsfor poor outcome. J Clin Gastroenterol.
2000;30(3):281-285.(Prospective; 411 patients)
3.* Barkun AN, Bardou M, Kuipers EJ, et al.
Internationalconsensus recommendations on the management of
patientswith nonvariceal upper gastrointestinal bleeding. Ann
Intern
Med. 2010;152(2):101-113. (Multidisciplinary
consensusgroup; 34 experts from 15 countries)
4.* Gotzsche PC, Hrobjartsson A. Somatostatin analogues foracute
bleeding esophageal varices. Cochrane Database SystRev.
2008;(3):CD000193. (Systematic literature review)
5. Sreedharan A, Martin J, Leontiadis GI, et al. Proton
pumpinhibitor treatment initiated prior to endoscopic diagnosis
inupper gastrointestinal bleeding. Cochrane Database Syst
Rev.2010;(7):CD005415. (Systematic literature review)
6.* Scottish Intercollegiate Guidelines Network (SIGN).
Man-agement of acute upper and lower gastrointestinal
bleeding.Available at:
http://guideline.gov/content.aspx?id=13167.
-
8/19/2019 0413 Massive Upper GI Bleeding.pdf
11/12
11 EMCC © 2013www.ebmedicine.net • Volume 3, Number
2
1. The most common cause of massive upper GIbleeding is:
a. Esophageal varices b. Diverticula c.
Arteriovenous malformations d. Gastritis e. Gastric and
duodenal ulcers
2. In regard to the stabilization and monitoringof patients with
massive upper GI bleeding,which of the following is TRUE?
a. PPIs are not recommended. b. Initial and serial
coagulation studies should
be used to guide decision making.c. Continuous cardiac and
pulse oximetry
monitoring are required.d. Consultation with subspecialists
should
be delayed until after stabilization andresuscitation.
3. In regard to the use of angiography in patients
with massive upper GI bleeding, which of thefollowing is
TRUE? a. Angiography is highly specic for detection
of bleeding at rates of at least 0.5 mL/min. b.
Angiography can detect bleeding at slower
rates than can be detected by radionuclideimaging.
c. Angiography has the disadvantage of beingdiagnostic
but not therapeutic.
d. Angiography is contraindicated in patientswith nonvariceal
upper GI bleeding.
4. In regard to blood product transfusion for pa-
tients with massive upper GI bleeding, whichof the following is
TRUE?a. A hemoglobin level of 7 to 8 gm/dL should
be considered the endpoint of resuscitation. b. The
recommended PRBC:FFP:platelet
ratio is 1:2:1.c. Use of crystalloids should ideally be
restricted to the initial phase of resuscitation.d. Calcium
gluconate should be administered
to all patients receiving PRBCs.
2001;32(4):315-318. (Prospective; 84 patients)24. Bosch J,
Thabut D, European Study Group on rFVIIa in UGI
Haemorrhage, et al. Recombinant factor VIIa for upper
gas-trointestinal bleeding in patients with cirrhosis: a
random-ized, double-blind trial.
Gastroenterology.2004;127(4):1123-1130. (Prospective randomized
trial; 245 patients)
25. Ejlersen E, Melsen T, Ingerslev J, et al. Recombinant
activatedfactor VII (rFVIIa) acutely normalizes prothrombin time
inpatients with cirrhosis during bleeding from oesophagealvarices.
Scand J Gastroenterol. 2001;36(10):1081-1085.(Pro-spective
observational; 10 patients)
26.* Thabut D, de Franchis R, Bendtsen F, et al. Efcacy of
acti-vated recombinant factor VII in cirrhotic patients with
uppergastrointestinal bleeding: a randomized
placebo-controlleddouble-blind multicenter trial.
Gastroenterology.2003;124(4)(Suppl1):A697. (Prospective randomized;
245 patients)
27. Ansell J, Hirsh J, Hylek E, et al. Pharmacology and
manage-ment of the vitamin K antagonists: American College ofChest
Physicians Evidence-Based Clinical Practice Guide-lines (8th
Edition). Chest. Jun 2008;133(6):160S-198S.
(Practiceguideline)
28. van Ryn J, Stangier J, Haertter S, et al. Dabigatran
etexilate--anovel, reversible, oral direct thrombin inhibitor:
interpreta-tion of coagulation assays and reversal of
anticoagulantactivity. Thromb Haemost. 2010;103(6):1116-1127.
(Literaturereview)
29. Eerenberg ES, Kamphuisen PW, Sijpkens MK, et al.
Reversal
of rivaroxaban and dabigatran by prothrombin complexconcentrate.
Circulation. 2011;124(14):1573-1579. (Prospectiverandomized; 12
patients)
30. Findley LJ, Redstone PM. Blood transfusion in
adult Jehovah’s Witnesses. A case study of one
congregation.1982;142(3):606-607. (Retrospective survey; 70
respondents)
31. Watch Tower Bible and Tract Society of Pennsylvania. Howcan
blood save your life? Available at:
http://www.jw.org/en/publications/books/blood/how-can-blood-save-your-life/.
Accessed March 1, 2013. (Website)
CME Questions
Take This Test Online!
Current subscribers can receive CME creditabsolutely free by
completing the following test.This issue includes 3 AMA PRA
Category 1 CreditsTM. Online testing is now available for
current andarchived issues. To receive your free CME credits
forthis issue, scan the QR code below or
visitwww.ebmedicine.net/C0413
-
8/19/2019 0413 Massive Upper GI Bleeding.pdf
12/12
EMCC © 2013 12 b di i t V l 3 N b 2
CME Information
Date of Original Release: April 1, 2013. Date of most
recent review:March 1, 2013. Termination date: April 1, 2016.
Accreditation: EB Medicine is accredited by the
Accreditation Councilfor Continuing Medical Education (ACCME) to
provide continuingmedical education for physicians. This activity
has been planned andimplemented in accordance with the Essential
Areas and Policies of the
ACCME.
Credit Designation: EB Medicine designates this enduring
material for amaximum of 3 AMA PRA Category 1
Credits™. Physicians should claim onlythe credit commensurate
with the extent of their participation in the activity.
AOA Accreditation: EMCC is eligible for up to 18
American Osteopathic Association Category 2A or 2B credit
hours per year.
Needs Assessment: The need for this educational activity
wasdetermined by a survey of medical staff, including the editorial
board ofthis publication; review of morbidity and mortality data
from the CDC,
AHA, NCHS, and ACEP; and evaluation of prior activities
for emergencyphysicians.
Target Audience: This enduring material is designed for
emergencymedicine physicians, physician assistants, nurse
practitioners, andresidents as well as intensivists and
hospitalists.
Goals: Upon completion of this article, you should be able
to: (1)demonstrate medical decision-making based on the strongest
clinicalevidence; (2) cost-effectively diagnose and treat the most
critical EDpresentations; and (3) describe the most common
medicolegal pitfalls foreach topic covered.
Discussion of Investigational Information: As part of
the newsletter,faculty may be presenting investigational
information aboutpharmaceutical products that is outside Food and
Drug Administration-approved labeling. Information presented as
part of this activity isintended solely as continuing medical
education and is not intended topromote off-label use of any
pharmaceutical product.
Faculty Disclosure: It is the policy of EB Medicine to
ensure objectivity,balance, independence, transparency, and
scientific rigor in all CME-sponsored educational activities. All
faculty participating in the planningor implementation of a
sponsored activity are expected to disclose to theaudience any
relevant financial relationships and to assist in resolvingany
conflict of interest that may arise from the relationship. In
compliancewith all ACCME Essentials, Standards, and Guidelines, all
faculty for thisCME activity were asked to complete a full
disclosure statement. Theinformation received is as follows: Dr.
Mihata, Dr. Bonk, Dr. Keville, Dr.Lin, Dr. Westhoff, Dr. Gogela
Carlson, Dr. Arntfield, and their related
parties report no significant financial interest or other
relationship
with the manufacturer(s) of any commercial product(s) discussed
inthis educational presentation.
Commercial Support: This issue of EMCC did not receive any
commercialsupport.
Earning Credit: Two Convenient Methods: (1) Go online
towww.ebmedicine.net/CME and click on the title of this article.(2)
Mail or fax the CME Answer And Evaluation Form with yourDecember
issue to EB Medicine.
Hardware/Software Requirements: You will need a Macintosh
or PC toaccess the online archived articles and CME testing.
Additional Policies: For additional policies,
including ourstatement of conflict of interest, source of funding,
statementof informed consent, and statement of human and animal
rights,visit www.ebmedicine.net/policies.
CEO & Publisher: Stephanie Williford Marketing
Manager: Robin Williford Managing Editor: Dorothy
Whisenhunt Director of Member Services: Liz Alvarez
EM Critical Care (EMCC) (ISSN Print: 2162-3031, ISSN
Online: 2162-3074, ACID-FREE) is p ublished 6 times per year by EB
Medicine (5550 Triangle Parkway, Suite 150, Norcross, GA
30092).Opinions expressed are not necessarily those of this
publication. Mention of products or services does not constitute
endorsement. This publication is intended as a general guide and
isintended to supplement, rather than substitute, professional
judgment. It covers a highly technical and complex subject and
should not be used for making specific medical decisions.
Thematerials contained herein are not intended to establish policy,
procedure, or standard of care.EM Critical Care and
EMCC are trademarks of EB Medicine. Copyright © 2013 EB
Medicine. Allrights reserved. No part of this publication may be
reproduced in any format without written consent of EB Medicine.
This publication is intended for the use of the individual
subscriber onlyand may not be copied in whole or part or
redistributed in any way without the publisher’s prior written
permission -- including reproduction for educational purposes or
for internal distribution
within a hospital, library, group practice, or other entity.
EMCC Subscription Information:
6 print issues per year, 18 AMA PRA Category 1
CreditsTM ,
and full online access to searchable archives
and additional CME: $299
(Call 1-800-249-5770 or go to
www.ebmedicine.net/EMCCinfo to order)
EB MedicinePhone: 1-800-249-5770 or 1-678-366-7933
Fax: 1-770-500-13165550 Triangle Parkway, Suite 150, Norcross,
GA 30092
E-mail: [email protected]: www.ebmedicine.net
To write a letter to the editor, please email:
[email protected]
EMCC Has
Gone Mobile! You can now view all EMCC content
on youriPhone or Android smartphone. Simply visitwww.ebmedicine.net
from your mobile device,and you’ll automatically be directed to
ourmobile site.
On our mobile site, you can:
• View all issues of EMCC since inception,
including
issues on NIV, blunt trauma, ACS, and more
• Take CME tests for all issues – that’s over 20 AMA
Category 1 CreditsTM!
• View your CME records, including scores, dates of
completion, and certificates
• Comment on EMCC’s What’s Your Diagnosis blog, by
visiting www.ebmedicine.net/emccblog
• Renew your subscription or purchase additional
content
Check out our mobile site, and give us your
feedback! Simply click the link at the bottom of
the mobile site to complete a short survey to tell
us what features you’d like us to add or change.