Embed Size (px)
Citation preview

Vector analysis of astigmatism correctionafter toric intraocular lens implantation
Eva M. Krall, MD, Eva M. Arlt, MD, Melchior Hohensinn, MD, Sarah Moussa, MD, Gerlinde Jell, MD,Jorge L. Ali�o,MD, PhD, Ana B. Plaza-Puche,MD,MSc, Lucia Bascaran,MD, JavierMendicute, MD, PhD,
G€unther Grabner, MD, Alois K. Dexl, MD, MSc
PURPOSE: To determine astigmatic changes by vector analysis and postoperative refractive and vi-sual outcomes after implantation of the monofocal aspheric bitoric AT Torbi 709M toric intraocularlens (IOL).
SETTING: Three centers in Salzburg, Austria, and Alicante and San Sebasti�an, Spain.
DESIGN: Prospective interventional case series.
METHODS: Preoperative and postoperative visual acuity, subjective and objective refractions, andcorneal radii using a topographer were examined in all patients. All patients had postoperative exam-inations within the first week and at 6 to 12 weeks. Astigmatic changes were evaluated using the Al-pins vector method based on 3 fundamental vectors as follows: target induced astigmatism (TIA),surgically induced astigmatism (SIA), and difference vector. The various relationships between these3 vectors were calculated, providing an extensive description of the astigmatic correction achieved.
RESULTS: Eighty-eight eyes (71 patients) were included. Postoperatively, refractive cylinder wasreduced significantly (P < .001), concurrent with visual improvement. The mean magnitude of theSIA vector (2.54 diopters [D] G 1.21 [SD]) was slightly higher than the mean magnitude of theTIA vector (2.37G 1.15 D) at the last follow-up. The mean difference vector was 0.46G 0.46 D,the mean magnitude of error was 0.16 G 0.46 D, and the mean correction index was 1.09 G0.21, all indicating minimal overcorrection at 3 months that remained stable during the follow-up.
CONCLUSION: Implantation of the toric IOL was safe and effective for the treatment of eyes withcataract in combination with preexisting regular corneal astigmatism over a short-term follow-up.
Financial Disclosure: No author has a financial or proprietary interest in any material or methodmentioned.
J Cataract Refract Surg 2015; 41:790–799 Q 2015 ASCRS and ESCRS
Modern cataract surgery offers the possibility ofcompensating for spherical and astigmatic refractiveerrors, thus providing enhanced visual rehabilitation.In a recent biometry study of 23 239 eyes,1 cornealastigmatism of 1.0 diopter (D) or more was observedin 28% of patients. Several techniques, including oppo-site clear corneal incisions,2 limbal relaxing incisions,3
femtosecond laser–assisted astigmatic keratotomy,4
excimer laser refractive procedures,5,6 and toric intra-ocular lens (IOL) implantation,7 are available to correctregular corneal astigmatism. The implantation of toricIOLs is an effective treatment of lens opacification andconcomitant regular corneal astigmatism in a singlesurgical procedure and has been proven to be safeand predictable.8
To evaluate the efficacy of toric IOL implantation,astigmatic change can be determined by vectoranalysis considering its magnitude and axis. In brief,vector analysis determines a goal for astigmatismcorrection and a treatment required to achieve thatgoal. The method also allows the calculation of theprincipal components by which an operation fails toachieve its goal and other components that assist incomparing the results of astigmatism surgery in indi-viduals and groups of individuals.9,10
The purpose of this study was to determine theastigmatic changes using vector analysis as well aspostoperative refractive and visual outcomes withinthe first 3 months after implantation of the AT Torbi709M toric IOL (Carl Zeiss Meditec AG).
Q 2015 ASCRS and ESCRS
Published by Elsevier Inc.
790 http://dx.doi.org/10.1016/j.jcrs.2014.07.038
0886-3350
ARTICLE

PATIENTS AND METHODS
Patient Population
This clinical trial was designed as a prospectivemulticenter interventional case series with 3 participatingophthalmologic centers as follows: Vissum Corporation,Division of Ophthalmology, Universidad Miguel Hern�an-dez, Alicante, Spain; Ophthalmology Service, DonostiaHospital, San Sebasti�an, Spain; and Department of Ophthal-mology, Paracelsus Medical University, Salzburg, Austria.The study was performed in accordance with the tenets ofthe Declaration of Helsinki and approved by each center’slocal institutional review board or ethics committee. Afterreceiving a detailed explanation of the purpose, procedure,and patient responsibilities, all trial patients provided signedinformed consent for participation in this study.
Patients were eligible for inclusion if they were older than40 years, had age-related cataract with regular cornealastigmatism without additional ocular pathology, had astable corneal condition, and had refraction within thepast 12 months. Exclusion criteria were irregular cornealastigmatism, serious intraoperative complications,glaucoma, pseudoexfoliation syndrome, uveitis, maculardegeneration or other retinal impairment, corneal scarring,amblyopia with a corrected distance visual acuity less than0.5, and a need for a toric IOL outside the available sphericalrange (�10.0 to C32.0 D) and/or outside cylindrical range(�1.0 to �12.0 D).
Preoperative Assessment
Before surgery, a complete medical history was taken andall patients had a full ophthalmologic examination includingrefraction and uncorrected (UDVA) and corrected (CDVA)distance visual acuity measurements. The Early TreatmentDiabetic Retinopathy Study charts at a test distance of 4 mwere used by counting the numbers of optotypes the patientidentified correctly and converting this number into logMAR
values. Keratometric values were measured with partialcoherence interferometry (PCI) (IOLMaster, Carl Zeiss Med-itec AG) for IOL calculation, and corneal topography wasperformed to ensure regularity of the corneal astigmatism.
Intraocular lens power calculation was performed usingthe online calculation program Z CALC (Carl Zeiss MeditecAG). This calculation program requires the input of thefollowing PCI data: axial length, anterior chamber depth(ACD), keratometry values in diopters, and IOL type to beimplanted.
Intraocular Lens
The AT Torbi 709M is a monofocal bitoric aspheric IOLwith an optic diameter of 6.0 mm and a total diameter of11.0 mm. The optic design provides aberration-neutralconvergent incidence of light.A The optic material of theIOL is foldable hydrophilic acrylate with a hydrophobicsurface and 25% water content and an ultraviolet filter. Thehaptic angulation is 0 degrees, and the IOL is available inspherical ranges of �10.0 to C32.0 D in 0.5 D incrementsand in toric ranges ofC1.0 toC12.0 D in 0.5 D increments.A
Surgical Technique
One experienced surgeon (G.G., J.L.A., J.M.) performed allsurgeries at each center using topical anesthesia. All patientswere operated on with a standard sutureless phacoemulsifi-cation technique. In all cases, the IOL was implanted in thecapsular bag with the single-use injector A6/AT. Smart Car-tridge Set (Carl Zeiss Meditec AG), requiring an incisionwidth of at least 1.8 mm. Surgical preparation, IOL implan-tation, postoperative treatment, and postoperative medica-tion were performed/applied corresponding to the routineprocedure of the respective center.
At the Alicante facility, both the 0-degree axis and180-degree axis were marked with a needle on the cornealepithelium with the patient seated at the slitlamp. The IOLwas implanted in the axis corresponding to the calculationprogram, with the 180-degree premarked axis acting as areference. After IOL implantation, all ophthalmic viscosurgi-cal device (OVD) material above and beyond the IOL wasremoved, and the appropriate IOL position was recheckedand adjusted if necessary.
At the San Sebasti�an facility, with the patient seated on thesurgical table and correct vertical alignment of the patient’shead, patients were asked to look at a distance target (6 m)exactly in front of them to avoid cyclotorsion. Using a sterilemarker, the 0-degree and 180-degree axes were marked.Next, with the patient lying on the surgical table, the steepcorneal meridian was marked using a Marquez gauge andthe preplaced reference points. After IOL implantation, theIOL was rotated into the appropriate position, and theOVD was removed from the anterior chamber and capsularbag using an irrigation/aspiration (I/A) system. The appro-priate IOL position was rechecked at the end of surgery.
At the Salzburg facility, the IOL was positioned accordingto intraoperative corneal topography. Eight intraoperativephotographs were taken with a Keratron Scout cornealtopographer (Optikon 2000 S.p.A.); the axis of the bestimages were averaged and taken as a reference. After IOLimplantation, the IOL was rotated into the appropriate posi-tion and the OVD was removed from the anterior chamberand capsular bag using the I/A system. The appropriateIOL position was rechecked at the end of surgery.
Submitted: April 3, 2014.
Final revision submitted: July 5, 2014.Accepted: July 15, 2014.
From the Department of Ophthalmology (Krall, Arlt, Hohensinn,
Moussa, Jell, Grabner, Dexl), Paracelsus Medical University, Salz-burg, Austria; the Division of Ophthalmology (Ali�o, Plaza-Puche),Vissum Corporation, Universidad Miguel Hern�andez, Alicante, and
the Ophthalmology Service (Bascaran, Mendicute), Donostia Hos-pital, San Sebasti�an, Spain.
Supported by the Fuchs Foundation for the Promotion of Researchin Ophthalmology, Salzburg, Austria. Carl Zeiss Meditec AG, Jena,
Germany, financially supports the Fuchs Foundation as the clinicalresearch center of the Department of Ophthalmology of the Paracel-sus Medical University, Salzburg, Austria (grant 23-2011).
Presented at the XXX Congress of the European Society of Cataractand Refractive Surgeons, Amsterdam, the Netherlands, October2013.
Corresponding author: Alois K. Dexl, MD, MSc, Department ofOphthalmology, Paracelsus Medical University, M€ullnerHauptstraße 48, A-5020 Salzburg, Austria. E-mail: [email protected].
791VECTOR ANALYSIS AFTER TORIC IOL IMPLANTATION
J CATARACT REFRACT SURG - VOL 41, APRIL 2015

Corneoscleral incisions of 1.8 mm were used at each facil-ity. The incisions were placed at the 12 o’clock position toensure that no surgically induced corneal astigmatismwould influence the preexisting corneal astigmatism.
Postoperative Assessment
Postoperatively, patients were examined within the firstweek and at 3 months. At the first postoperative visit, aslitlamp examination was performed and the UDVA,CDVA, and subjective refraction were evaluated. In addi-tion, PCI measurement was performed to compare preoper-ative and postoperative keratometric values. Three monthspostoperatively, the same tests as at the first postoperativevisit were performed. In addition, objective refraction,ACD by anterior chamber optical coherence tomography(Visante, Carl Zeiss Meditec AG), and corneal topographywere evaluated. In a subgroup of all 20 eyes at the Salzburgcenter, a slitlamp photograph in retroillumination was takenat the end of surgery and compared with postoperative pho-tographs to document torus position at every visit and toevaluate whether the IOL had rotated.
Vectorial Analysis of Astigmatic Changes
Refractive astigmatic changes were evaluated 1 week and3months postoperatively by vector analysis using theAlpinsmethod (Assort software, Assort Pty. Ltd.).9,10 The Alpinsmethod allows evaluation that follows 3 fundamental vec-tors: (1) target induced astigmatism vector (TIA Z changein astigmatic magnitude and axis the surgery was intendedto induce), (2) surgically induced astigmatism vector(SIA Z amount and axis of astigmatic change the surgeryactually induced), and (3) difference vector (induced astig-matic change by magnitude and axis that would enableinitial surgery to achieve its intended target).
Furthermore, relationships between these 3 fundamentalvectors were calculated at each postoperative visit, definedas follows: (1) correction index, calculated by determiningthe ratio of SIA to TIA (correction index is preferably 1.0; ifthe correction index isO1.0 overcorrection occurred, and ifthe correction index is !1.0, undercorrection occurred), (2)magnitude of error (arithmetic difference between magni-tudes of SIA and TIA: magnitude of errorO0 indicates over-correction and magnitude of error !0 undercorrection), (3)angle of error (angle described by the vectors of SIA versusTIA; angle of errorO0: achieved correction axis was counter-clockwise to where it was intended; angle of error !0:achieved correction was clockwise to its intended axis), (4)index of success (calculated by dividing the difference vectorby TIA, representing a relative measure of success [index ofsuccess is preferably 0]), (5) coefficient of adjustment (calcu-lated by dividing TIA to SIA, which is the inverse of thecorrection index and quantifies the modification needed tothe initial surgery plan to have achieved a correction indexof 1, the ideal correction).
Statistical Analysis
All data were collected in an Excel database, and statis-tical analysis was computed with SPSS for Windows soft-ware (version 15.0, SPSS, Inc.). For every parameter,mean values and standard deviations were calculated. AP value less than 0.05 was the limit for statistical signifi-cance. First, for all data samples, normal distribution waschecked using the Kolmogorov-Smirnov test. The Student
t test for paired data was applied for all parameter compar-isons between preoperative and postoperative data or post-operative data from different controls, if parametricanalysis was possible. The Wilcoxon rank-sum test wasused to compare preoperative and postoperative values,calculating the level of significance if parametric analysiswas not possible. For correlation among different parame-ters, the Pearson coefficient or Spearman rank order coeffi-cient was applied where appropriate, depending on thenormality distribution of the data. To analyze the datafrom preoperative examinations and postoperative exami-nations and between consecutive postoperative visits ineach IOL group, Kruskal-Wallis 1-way analysis of variancefor repeated measures was used.
RESULTS
This study enrolled 88 eyes of 71 patients. Table 1 showsthe demographic data and implanted toric IOL powers.At 1 trial center, a patient younger (38 years) than theinclusion criteria (O40 years) was included and evalu-ated during the trial period.
Table 1. Preoperative demographics (88 eyes of 71 patients).
Demographic Value
Age (y)
MeanG SD 64.1G 19
Range 38, 84
Sex, n (%)
Female 42 (59.2)
Male 29 (40.8)
Operated eyes (n)
Right 28
Left 26
Both 17
Axial length (mm)
MeanG SD 23.99G 1.82
Range 20.83, 29.60
Anterior chamber depth (mm)
MeanG SD 3.09G 0.43
Range 2.05, 4.03
Mean implanted IOL power (D)
Sphere
MeanG SD 17.37G 5.38
Range 3.5, 28.0
Cylinder
MeanG SD �2.93G 1.41
Range �9.5, �1.0
Predicted postop residual refraction (D)
Sphere
MeanG SD �0.07G 0.45
Range �3.12, 0.17
Cylinder
MeanG SD �0.20G 0.11
Range �0.47, 0.00
IOLZ intraocular lens
792 VECTOR ANALYSIS AFTER TORIC IOL IMPLANTATION
J CATARACT REFRACT SURG - VOL 41, APRIL 2015

Visual Acuity and Refraction
Table 2 shows refractive and visual acuity out-comes. A statistically significant improvement inUDVA and CDVA occurred after 1 week (both P !.001) (Figures 1 and 2). In addition, the UDVA andCDVA 3 months postoperatively was statistically sig-nificant better than at 1 week (both P! .001).
There was a statistically significant reduction inmanifest refraction spherical equivalent and refractiveastigmatism from preoperatively to 3 months postop-eratively (both P ! .001) (Figures 3 and 4, respec-tively). At 3 months, the refractive astigmatism was�0.50 D or less in 62 (71%) of the 88 eyes, 1.00 D orless in 81 eyes (92%), 1.50 D or less in 86 eyes (98%),and less than 2.00 D in all eyes (Figure 5). The sphereimproved considerably at all postoperative visitscompared with preoperative values, although no sta-tistically significant difference was found (1 week,
PZ.25; 3 months, PZ.30), and remained stable overtime (1 week to 3 months, PZ.943). There was no sig-nificant difference between the predicted residualsphere postoperatively and the achieved postopera-tive sphere after 1 week (PZ.20) or 3 months(PZ.21). The postoperative high range was causedby a target SE refraction of �3.0 D in several patients.
There were no statistically significant differences inthe postoperative refractive results (sphere, refractiveastigmatism, SE) between unilateral patients and bilat-eral patients (all PO.05).
Corneal Topographic and Keratometric Changes
There were no statistically significant changes in thecorneal topographic or keratometric flat meridian orthe steep meridian between preoperatively and anypostoperative examination (Table 2).
Table 2. Visual and refractive outcomes over time and corneal topographic and keratometric changes.
Parameter Preop 1 Week Postop 3 Months Postop P Value*
Sphere (D)
MeanG SD �1.00G 5.01 0.18G 0.66 0.18G 0.68 .259*
Range �16.00,C7.00 �2.75, 1.75 �3.00, 1.75
Refractive cylinder (D)
MeanG SD �2.19G 1.39 �0.50G 0.53 �0.43G 0.48 !.001†
Range �7.00, 0.00 �2.00, 0.00 �2.00, 0.00
UDVA (logMAR)
MeanG SD 0.88G 0.45 0.24G 0.19 0.15G 0.18 !.001†
Range 0.3, 2.0 �0.08, 0.93 �0.10, 0.70
CDVA (logMAR)
MeanG SD 0.31G 0.15 0.13G 0.15 0.06G 0.12 !.001†
Range 0.00, 0.70 �0.08, 0.70 �0.10, 0.44
MRSE (D)
MeanG SD �2.09G 4.95 �0.07G 0.60 �0.04G 0.63 !.001z
Range �16.50, 5.88 �2.75, 1.38 �3.00, 1.75
PCI keratometry (mm)
R1
MeanG SD 7.87G 0.27 7.90G 0.29 7.85G 0.27 .63z
Range 7.23, 8.46 7.39, 8.51 7.31, 8.57
R2
MeanG SD 7.45G 0.24 7.47G 0.24 7.46G 0.24 .78z
Range 6.61, 7.98 6.65, 7.90 6.56, 7.88
CT keratometry (mm)
R1
MeanG SD 7.72G 0.36 d 7.71G 0.35 .841*
Range 6.82, 8.63 d 6.53, 8.5
R2
MeanG SD 7.56G 0.27 d 7.56G 0.27 .806*
Range 6.59, 8.12 d 6.88, 8.17
CDVAZ corrected distance visual acuity; CTZ corneal topography;MRSEZmanifest refraction spherical equivalent; PCIZ partial coherence interferometry;
R1Z flat meridian; R2Z steep meridian; UDVAZ uncorrected distance visual acuity
*Preoperative versus 3 months postoperative†Wilcoxon textzStudent t test
793VECTOR ANALYSIS AFTER TORIC IOL IMPLANTATION
J CATARACT REFRACT SURG - VOL 41, APRIL 2015

Misalignment and Intraocular Lens Rotation
In the subgroup analysis of the 20 eyes from the Salz-burg facility, themean rotation of the toric IOL axiswas0.05 degreesG 1.5 (SD) (range �2 toC2 degrees) fromthe end of surgery to the first postoperative visit and�0.6 G 1.4 degrees (range �3 to C2 degrees) fromthe end of the surgery to 3 months postoperatively.The differenceswere not statistically significant. (Clock-wise rotation was regarded as positive rotation andcounterclockwise as negative rotation.)
Vector Analysis
Table 3 shows the vector analysis outcomes. Themean magnitude of TIA was 2.37 G 1.15 D (range0.25 to 7.32), whereas the mean magnitude of SIAwas slightly higher at both postoperative visits(Figure 6), indicating a slight overcorrection that was
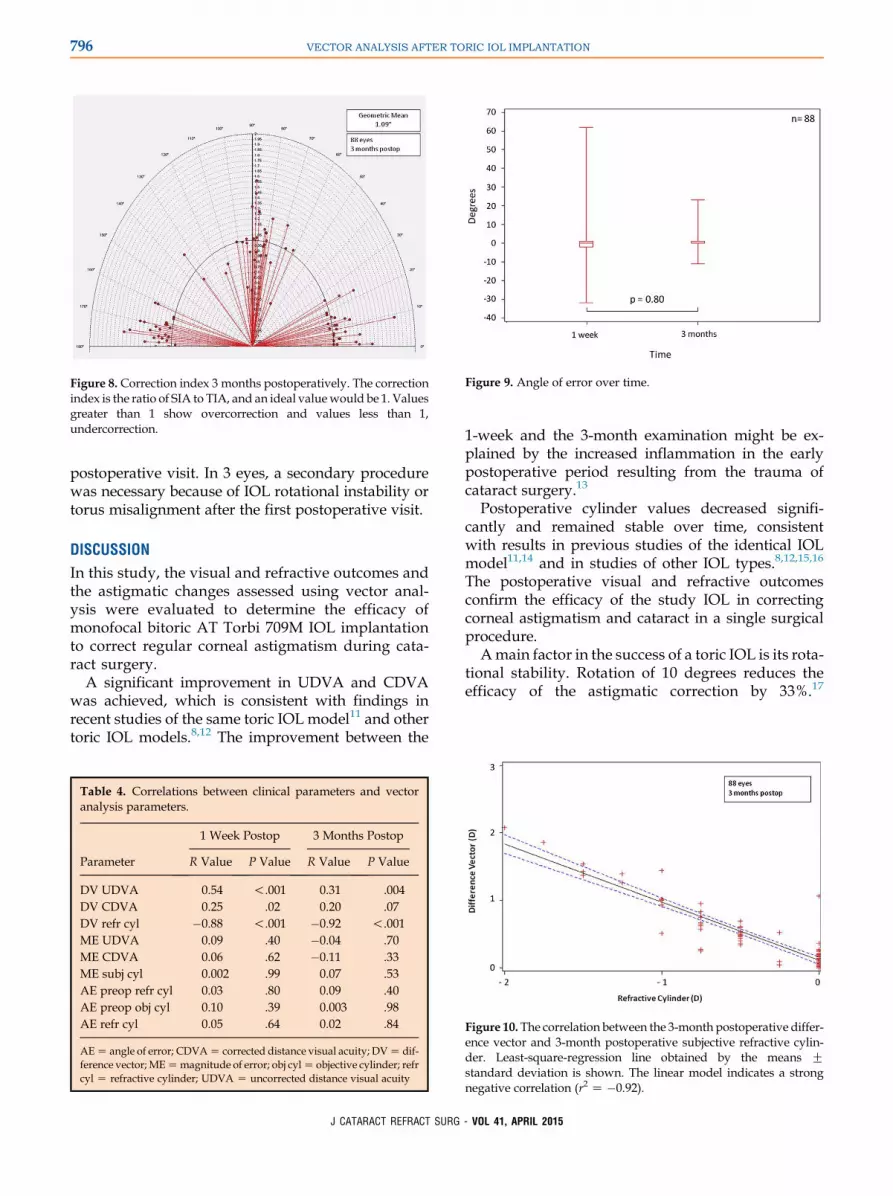
statistically significant at both visits (P ! .01). Themagnitude of SIA remained stable over time(PZ.999). There was no statistically significant differ-ence in the magnitude of the difference vector betweenpostoperative visits. Figure 7 shows the difference vec-tor, including the magnitude and its orientation, 3months postoperatively. The mean correction index(ie, ratio of SIA to TIA; preferably 1) reflected the slightovercorrection (Figure 8) and remained stable overtime. The mean magnitude of error was slightly posi-tive (ie, showing overcorrection) during the postoper-ative follow-up, with no significant difference betweenvisits. The index of success (ie, relative measure of suc-cess; preferably 0) was 0.22G 0.21, and the coefficientof adjustment (ie, inverse of correction index; prefer-ably 1) remained stable over time (PZ.355 andPZ.453, respectively).
Figure 1. Uncorrected distance visual acuity over time. Figure 2. Corrected distance visual acuity over time.
Figure 3. Stability and spherical equivalent over time. The horizontalline indicates the mean calculated postoperative target SE.
Figure 4. Refractive astigmatism over time. The horizontal line indi-cates the mean calculated postoperative residual refractiveastigmatism.
794 VECTOR ANALYSIS AFTER TORIC IOL IMPLANTATION
J CATARACT REFRACT SURG - VOL 41, APRIL 2015

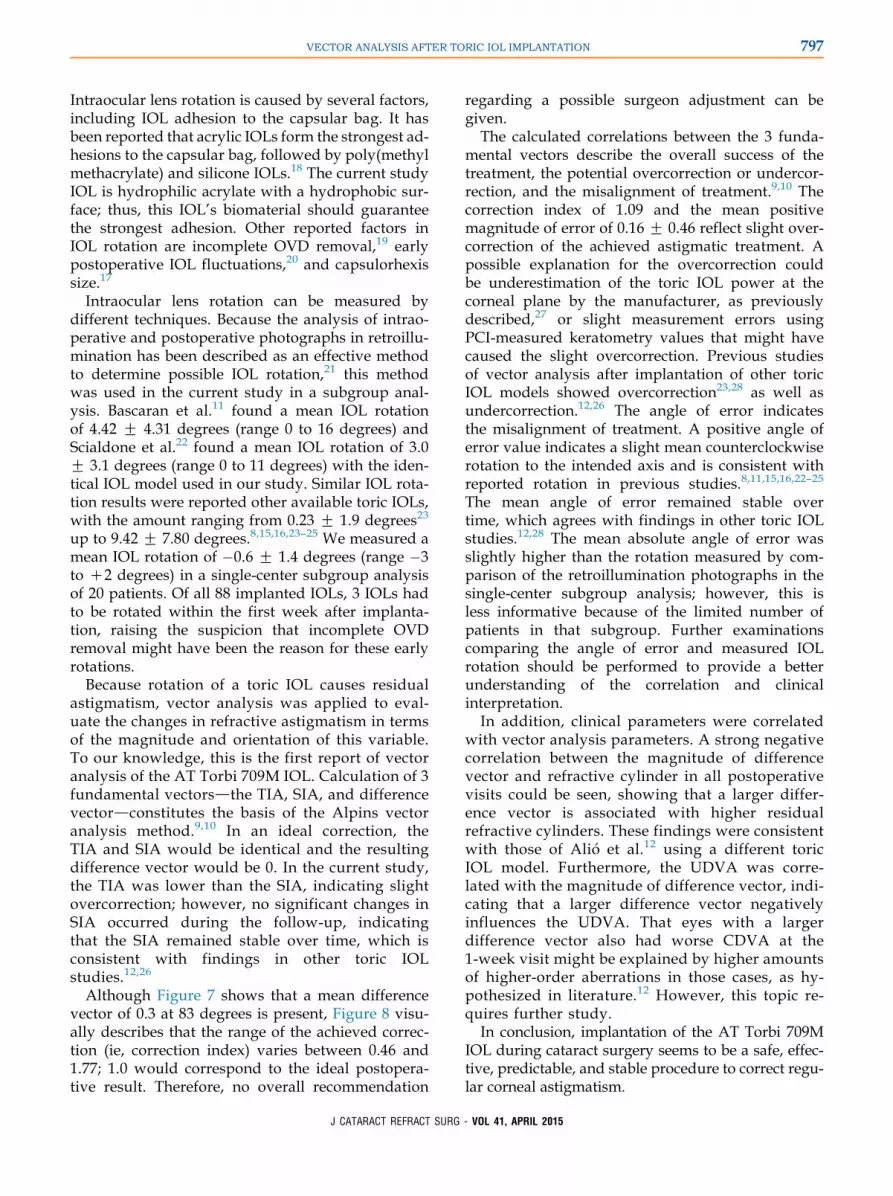
Themean angle of error was slightly positive at bothpostoperative visits (Figure 9). The high postoperativerange from�32 toC62 degrees 1 week after implanta-tion was related to 3 necessary secondary proceduresto rotate the IOL. The angle of error range afterwardimproved to �11 toC23 degrees after 3 months.
Correlations Between Clinical and Vector AnalysisParameters
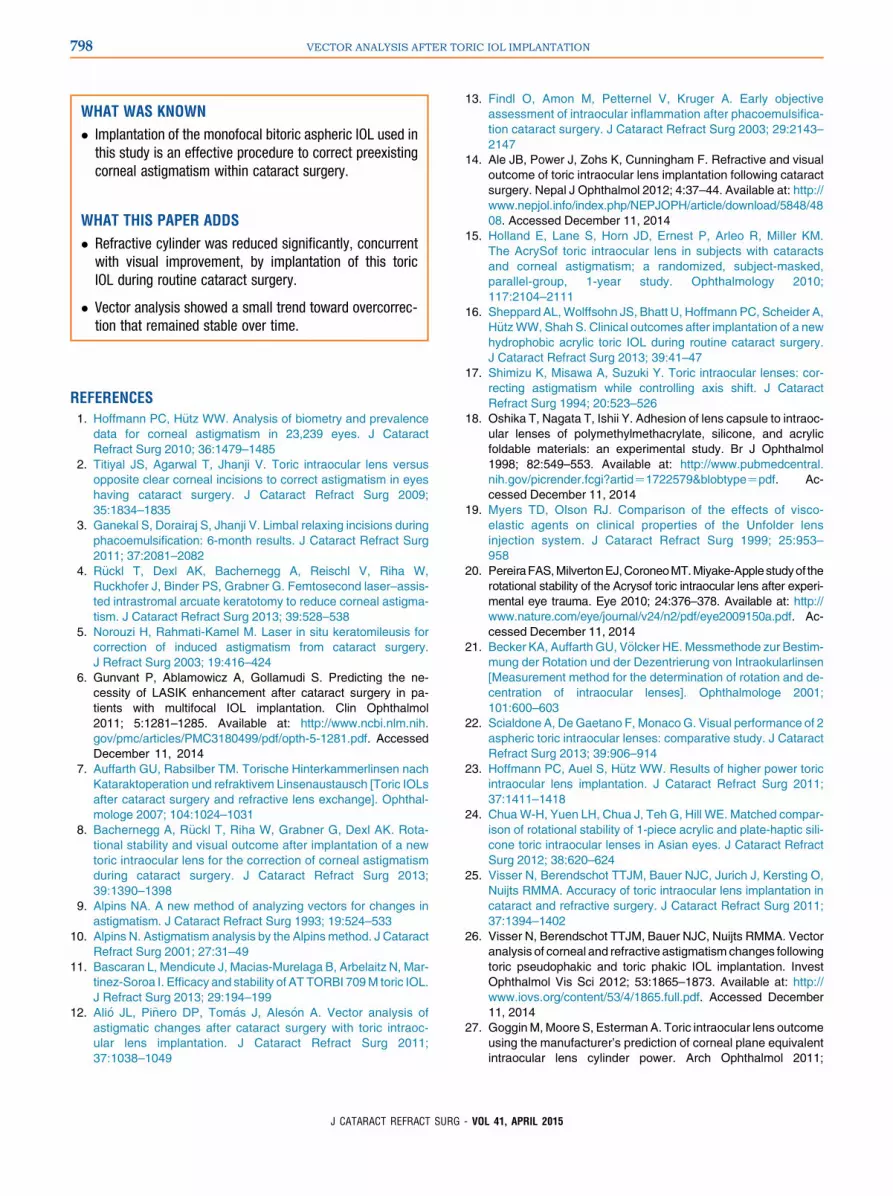
Table 4 shows correlations between different clinicaland vector analysis parameters. Significant positivecorrelations were found between the difference vectorand the UDVA at 1 week and 3 months as well as be-tween the difference vector and the CDVA at 1 week,even though correlation was low. A strong negativecorrelation was detected between the difference vectorand subjective refractive cylinder at each postopera-tive visit (P! .001) (Figure 10).
Complications
No severe intraoperative or postoperative complica-tions occurred at the 3 study centers. One eye hadimplantation of a capsular tension ring because ofmild zonulysis of 20 degrees. No eye required aneodymium:YAG capsulotomy up to the last
Figure 5. Preoperative and postoperative refractive astigmatism.
Table 3. Vector analysis.
Parameter 1 Week Postop 3 Months Postop P Value*
SIA (D)
MeanG SD 2.51G 1.20 2.54G 1.21 .999
Range 0.31, 7.46 0.63, 7.46
DV (D)
MeanG SD 0.52G 0.44 0.46G 0.46 .281
Range 0.00, 1.80 0.00, 2.08
CI
MeanG SD 1.07G 0.25 1.09G 0.21 .425
Range 0.37, 1.77 0.46, 1.77
ME (D)
MeanG SD 0.13G 0.50 0.16G 0.46 .490
Range �1.68, 1.28 �1.67, 1.42
AE (�)
MeanG SD 0.25G 10.01 0.63G 5.68 .797
Range �32, 62 �11, 23
IOS
MeanG SD 0.27G 0.26 0.22G 0.21 .355
Range 0.00, 1.24 0.00, 0.81
CA
MeanG SD 1.00G 0.31 0.96G 0.24 .453
Range 0.57, 2.71 0.57, 2.16
AE Z angle of error; CA Z coefficient of adjustment; CI Z correction
index; DVZ difference vector; IOSZ index of success; MEZmagnitude
of error; SIAZ surgically induced astigmatism
*One week postoperative versus 3 months postoperative
Figure 6. Comparison of TIA and SIA 1 week and 3 months postop-eratively (SIA Z surgically induced astigmatism; TIA Z targetinduced astigmatism).
Figure 7. Difference vector 3 months postoperative. It shows theadditional astigmatic change required to attain the intended targetof the initial surgery.
795VECTOR ANALYSIS AFTER TORIC IOL IMPLANTATION
J CATARACT REFRACT SURG - VOL 41, APRIL 2015
postoperative visit. In 3 eyes, a secondary procedurewas necessary because of IOL rotational instability ortorus misalignment after the first postoperative visit.
DISCUSSION
In this study, the visual and refractive outcomes andthe astigmatic changes assessed using vector anal-ysis were evaluated to determine the efficacy ofmonofocal bitoric AT Torbi 709M IOL implantationto correct regular corneal astigmatism during cata-ract surgery.
A significant improvement in UDVA and CDVAwas achieved, which is consistent with findings inrecent studies of the same toric IOL model11 and othertoric IOL models.8,12 The improvement between the
1-week and the 3-month examination might be ex-plained by the increased inflammation in the earlypostoperative period resulting from the trauma ofcataract surgery.13
Postoperative cylinder values decreased signifi-cantly and remained stable over time, consistentwith results in previous studies of the identical IOLmodel11,14 and in studies of other IOL types.8,12,15,16
The postoperative visual and refractive outcomesconfirm the efficacy of the study IOL in correctingcorneal astigmatism and cataract in a single surgicalprocedure.
Amain factor in the success of a toric IOL is its rota-tional stability. Rotation of 10 degrees reduces theefficacy of the astigmatic correction by 33%.17
Figure 8. Correction index 3 months postoperatively. The correctionindex is the ratio of SIA to TIA, and an ideal valuewould be 1. Valuesgreater than 1 show overcorrection and values less than 1,undercorrection.
Figure 9. Angle of error over time.
Table 4. Correlations between clinical parameters and vectoranalysis parameters.
Parameter
1 Week Postop 3 Months Postop
R Value P Value R Value P Value
DV UDVA 0.54 !.001 0.31 .004
DV CDVA 0.25 .02 0.20 .07
DV refr cyl �0.88 !.001 �0.92 !.001
ME UDVA 0.09 .40 �0.04 .70
ME CDVA 0.06 .62 �0.11 .33
ME subj cyl 0.002 .99 0.07 .53
AE preop refr cyl 0.03 .80 0.09 .40
AE preop obj cyl 0.10 .39 0.003 .98
AE refr cyl 0.05 .64 0.02 .84
AEZ angle of error; CDVAZ corrected distance visual acuity; DVZ dif-
ference vector;MEZmagnitude of error; obj cylZ objective cylinder; refr
cylZ refractive cylinder; UDVAZ uncorrected distance visual acuity
Figure 10. The correlation between the 3-month postoperative differ-ence vector and 3-month postoperative subjective refractive cylin-der. Least-square-regression line obtained by the means Gstandard deviation is shown. The linear model indicates a strongnegative correlation (r2Z �0.92).
796 VECTOR ANALYSIS AFTER TORIC IOL IMPLANTATION
J CATARACT REFRACT SURG - VOL 41, APRIL 2015
Intraocular lens rotation is caused by several factors,including IOL adhesion to the capsular bag. It hasbeen reported that acrylic IOLs form the strongest ad-hesions to the capsular bag, followed by poly(methylmethacrylate) and silicone IOLs.18 The current studyIOL is hydrophilic acrylate with a hydrophobic sur-face; thus, this IOL’s biomaterial should guaranteethe strongest adhesion. Other reported factors inIOL rotation are incomplete OVD removal,19 earlypostoperative IOL fluctuations,20 and capsulorhexissize.17
Intraocular lens rotation can be measured bydifferent techniques. Because the analysis of intrao-perative and postoperative photographs in retroillu-mination has been described as an effective methodto determine possible IOL rotation,21 this methodwas used in the current study in a subgroup anal-ysis. Bascaran et al.11 found a mean IOL rotationof 4.42 G 4.31 degrees (range 0 to 16 degrees) andScialdone et al.22 found a mean IOL rotation of 3.0G 3.1 degrees (range 0 to 11 degrees) with the iden-tical IOL model used in our study. Similar IOL rota-tion results were reported other available toric IOLs,with the amount ranging from 0.23 G 1.9 degrees23
up to 9.42 G 7.80 degrees.8,15,16,23–25 We measured amean IOL rotation of �0.6 G 1.4 degrees (range �3to C2 degrees) in a single-center subgroup analysisof 20 patients. Of all 88 implanted IOLs, 3 IOLs hadto be rotated within the first week after implanta-tion, raising the suspicion that incomplete OVDremoval might have been the reason for these earlyrotations.
Because rotation of a toric IOL causes residualastigmatism, vector analysis was applied to eval-uate the changes in refractive astigmatism in termsof the magnitude and orientation of this variable.To our knowledge, this is the first report of vectoranalysis of the AT Torbi 709M IOL. Calculation of 3fundamental vectorsdthe TIA, SIA, and differencevectordconstitutes the basis of the Alpins vectoranalysis method.9,10 In an ideal correction, theTIA and SIA would be identical and the resultingdifference vector would be 0. In the current study,the TIA was lower than the SIA, indicating slightovercorrection; however, no significant changes inSIA occurred during the follow-up, indicatingthat the SIA remained stable over time, which isconsistent with findings in other toric IOLstudies.12,26
Although Figure 7 shows that a mean differencevector of 0.3 at 83 degrees is present, Figure 8 visu-ally describes that the range of the achieved correc-tion (ie, correction index) varies between 0.46 and1.77; 1.0 would correspond to the ideal postopera-tive result. Therefore, no overall recommendation
regarding a possible surgeon adjustment can begiven.
The calculated correlations between the 3 funda-mental vectors describe the overall success of thetreatment, the potential overcorrection or undercor-rection, and the misalignment of treatment.9,10 Thecorrection index of 1.09 and the mean positivemagnitude of error of 0.16G 0.46 reflect slight over-correction of the achieved astigmatic treatment. Apossible explanation for the overcorrection couldbe underestimation of the toric IOL power at thecorneal plane by the manufacturer, as previouslydescribed,27 or slight measurement errors usingPCI-measured keratometry values that might havecaused the slight overcorrection. Previous studiesof vector analysis after implantation of other toricIOL models showed overcorrection23,28 as well asundercorrection.12,26 The angle of error indicatesthe misalignment of treatment. A positive angle oferror value indicates a slight mean counterclockwiserotation to the intended axis and is consistent withreported rotation in previous studies.8,11,15,16,22–25
The mean angle of error remained stable overtime, which agrees with findings in other toric IOLstudies.12,28 The mean absolute angle of error wasslightly higher than the rotation measured by com-parison of the retroillumination photographs in thesingle-center subgroup analysis; however, this isless informative because of the limited number ofpatients in that subgroup. Further examinationscomparing the angle of error and measured IOLrotation should be performed to provide a betterunderstanding of the correlation and clinicalinterpretation.
In addition, clinical parameters were correlatedwith vector analysis parameters. A strong negativecorrelation between the magnitude of differencevector and refractive cylinder in all postoperativevisits could be seen, showing that a larger differ-ence vector is associated with higher residualrefractive cylinders. These findings were consistentwith those of Ali�o et al.12 using a different toricIOL model. Furthermore, the UDVA was corre-lated with the magnitude of difference vector, indi-cating that a larger difference vector negativelyinfluences the UDVA. That eyes with a largerdifference vector also had worse CDVA at the1-week visit might be explained by higher amountsof higher-order aberrations in those cases, as hy-pothesized in literature.12 However, this topic re-quires further study.
In conclusion, implantation of the AT Torbi 709MIOL during cataract surgery seems to be a safe, effec-tive, predictable, and stable procedure to correct regu-lar corneal astigmatism.
797VECTOR ANALYSIS AFTER TORIC IOL IMPLANTATION
J CATARACT REFRACT SURG - VOL 41, APRIL 2015
WHAT WAS KNOWN
� Implantation of the monofocal bitoric aspheric IOL used in
this study is an effective procedure to correct preexisting
corneal astigmatism within cataract surgery.
WHAT THIS PAPER ADDS
� Refractive cylinder was reduced significantly, concurrent
with visual improvement, by implantation of this toric
IOL during routine cataract surgery.
� Vector analysis showed a small trend toward overcorrec-
tion that remained stable over time.
REFERENCES
1. Hoffmann PC, H€utz WW. Analysis of biometry and prevalence
data for corneal astigmatism in 23,239 eyes. J Cataract
Refract Surg 2010; 36:1479–1485
2. Titiyal JS, Agarwal T, Jhanji V. Toric intraocular lens versus
opposite clear corneal incisions to correct astigmatism in eyes
having cataract surgery. J Cataract Refract Surg 2009;
35:1834–1835
3. Ganekal S, Dorairaj S, Jhanji V. Limbal relaxing incisions during
phacoemulsification: 6-month results. J Cataract Refract Surg
2011; 37:2081–2082
4. R€uckl T, Dexl AK, Bachernegg A, Reischl V, Riha W,
Ruckhofer J, Binder PS, Grabner G. Femtosecond laser–assis-
ted intrastromal arcuate keratotomy to reduce corneal astigma-
tism. J Cataract Refract Surg 2013; 39:528–538
5. Norouzi H, Rahmati-Kamel M. Laser in situ keratomileusis for
correction of induced astigmatism from cataract surgery.
J Refract Surg 2003; 19:416–424
6. Gunvant P, Ablamowicz A, Gollamudi S. Predicting the ne-
cessity of LASIK enhancement after cataract surgery in pa-
tients with multifocal IOL implantation. Clin Ophthalmol
2011; 5:1281–1285. Available at: http://www.ncbi.nlm.nih.
gov/pmc/articles/PMC3180499/pdf/opth-5-1281.pdf. Accessed
December 11, 2014
7. Auffarth GU, Rabsilber TM. Torische Hinterkammerlinsen nach
Kataraktoperation und refraktivem Linsenaustausch [Toric IOLs
after cataract surgery and refractive lens exchange]. Ophthal-
mologe 2007; 104:1024–1031
8. Bachernegg A, R€uckl T, Riha W, Grabner G, Dexl AK. Rota-
tional stability and visual outcome after implantation of a new
toric intraocular lens for the correction of corneal astigmatism
during cataract surgery. J Cataract Refract Surg 2013;
39:1390–1398
9. Alpins NA. A new method of analyzing vectors for changes in
astigmatism. J Cataract Refract Surg 1993; 19:524–533
10. Alpins N. Astigmatism analysis by the Alpinsmethod. J Cataract
Refract Surg 2001; 27:31–49
11. Bascaran L, Mendicute J, Macias-Murelaga B, Arbelaitz N, Mar-
tinez-Soroa I. Efficacy and stability of AT TORBI 709M toric IOL.
J Refract Surg 2013; 29:194–199
12. Ali�o JL, Pi~nero DP, Tom�as J, Ales�on A. Vector analysis of
astigmatic changes after cataract surgery with toric intraoc-
ular lens implantation. J Cataract Refract Surg 2011;
37:1038–1049
13. Findl O, Amon M, Petternel V, Kruger A. Early objective
assessment of intraocular inflammation after phacoemulsifica-
tion cataract surgery. J Cataract Refract Surg 2003; 29:2143–
2147
14. Ale JB, Power J, Zohs K, Cunningham F. Refractive and visual
outcome of toric intraocular lens implantation following cataract
surgery. Nepal J Ophthalmol 2012; 4:37–44. Available at: http://
www.nepjol.info/index.php/NEPJOPH/article/download/5848/48
08. Accessed December 11, 2014
15. Holland E, Lane S, Horn JD, Ernest P, Arleo R, Miller KM.
The AcrySof toric intraocular lens in subjects with cataracts
and corneal astigmatism; a randomized, subject-masked,
parallel-group, 1-year study. Ophthalmology 2010;
117:2104–2111
16. Sheppard AL,Wolffsohn JS, Bhatt U, Hoffmann PC, Scheider A,
H€utzWW, Shah S. Clinical outcomes after implantation of a new
hydrophobic acrylic toric IOL during routine cataract surgery.
J Cataract Refract Surg 2013; 39:41–47
17. Shimizu K, Misawa A, Suzuki Y. Toric intraocular lenses: cor-
recting astigmatism while controlling axis shift. J Cataract
Refract Surg 1994; 20:523–526
18. Oshika T, Nagata T, Ishii Y. Adhesion of lens capsule to intraoc-
ular lenses of polymethylmethacrylate, silicone, and acrylic
foldable materials: an experimental study. Br J Ophthalmol
1998; 82:549–553. Available at: http://www.pubmedcentral.
nih.gov/picrender.fcgi?artidZ1722579&blobtypeZpdf. Ac-
cessed December 11, 2014
19. Myers TD, Olson RJ. Comparison of the effects of visco-
elastic agents on clinical properties of the Unfolder lens
injection system. J Cataract Refract Surg 1999; 25:953–
958
20. PereiraFAS,MilvertonEJ,CoroneoMT.Miyake-Applestudyof the
rotational stability of the Acrysof toric intraocular lens after experi-
mental eye trauma. Eye 2010; 24:376–378. Available at: http://
www.nature.com/eye/journal/v24/n2/pdf/eye2009150a.pdf. Ac-
cessed December 11, 2014
21. Becker KA, Auffarth GU, V€olcker HE. Messmethode zur Bestim-
mung der Rotation und der Dezentrierung von Intraokularlinsen
[Measurement method for the determination of rotation and de-
centration of intraocular lenses]. Ophthalmologe 2001;
101:600–603
22. Scialdone A, DeGaetano F, MonacoG. Visual performance of 2
aspheric toric intraocular lenses: comparative study. J Cataract
Refract Surg 2013; 39:906–914
23. Hoffmann PC, Auel S, H€utz WW. Results of higher power toric
intraocular lens implantation. J Cataract Refract Surg 2011;
37:1411–1418
24. ChuaW-H, Yuen LH, Chua J, Teh G, Hill WE. Matched compar-
ison of rotational stability of 1-piece acrylic and plate-haptic sili-
cone toric intraocular lenses in Asian eyes. J Cataract Refract
Surg 2012; 38:620–624
25. Visser N, Berendschot TTJM, Bauer NJC, Jurich J, Kersting O,
Nuijts RMMA. Accuracy of toric intraocular lens implantation in
cataract and refractive surgery. J Cataract Refract Surg 2011;
37:1394–1402
26. Visser N, Berendschot TTJM, Bauer NJC, Nuijts RMMA. Vector
analysis of corneal and refractive astigmatism changes following
toric pseudophakic and toric phakic IOL implantation. Invest
Ophthalmol Vis Sci 2012; 53:1865–1873. Available at: http://
www.iovs.org/content/53/4/1865.full.pdf. Accessed December
11, 2014
27. GogginM,Moore S, Esterman A. Toric intraocular lens outcome
using the manufacturer’s prediction of corneal plane equivalent
intraocular lens cylinder power. Arch Ophthalmol 2011;
798 VECTOR ANALYSIS AFTER TORIC IOL IMPLANTATION
J CATARACT REFRACT SURG - VOL 41, APRIL 2015

129:1004–1008. Available at: http://archopht.jamanetwork.
com/data/Journals/OPHTH/22540/ecs05116_1004_1008.pdf.
Accessed December 11, 2014
28. Ali�o JL, Pi~nero DP, Tom�as J, Plaza AB. Vector analysis of astig-
matic changes after cataract surgery with implantation of a new
toric multifocal intraocular lens. J Cataract Refract Surg 2011;
37:1217–1229
OTHER CITED MATERIALA. CarlZeissMeditecAG.TORBI709,ATTORBI709MPpreloaded.
Specifications. Available at: http://applications.zeiss.com/
C1257A290053AE30/0/538ECA28392347FDC1257A29005812
EE/$FILE/AT_TORBI709Datasheet_GB_FINAL.pdf. Accessed
December 11, 2014
First author:Eva M. Krall, MD
Department of Ophthalmology,Paracelsus Medical University,Salzburg, Austria
799VECTOR ANALYSIS AFTER TORIC IOL IMPLANTATION
J CATARACT REFRACT SURG - VOL 41, APRIL 2015





























