Embed Size (px)
Citation preview

Intraocular Tumor-AssociatedLymphangiogenesisA Novel Prognostic Factor for Ciliary Body Melanomaswith Extraocular Extension?
Ludwig M. Heindl, MD,1 Tanja N. Hofmann, MD,1 Werner Adler, PhD,2 Harald L. J. Knorr, MD,1
Leonard M. Holbach, MD,1 Gottfried O. H. Naumann, MD,1 Friedrich E. Kruse, MD,1 Claus Cursiefen, MD1
Purpose: To evaluate whether intraocular tumor-associated lymphangiogenesis contributes to prognosis ofciliary body melanomas with extraocular extension and to study its association with other tumor characteristics.
Design: Nonrandomized, retrospective case series.Participants: Twenty consecutive patients enucleated for a malignant melanoma of the ciliary body with
extraocular extension.Methods: Lymphatic vessels were identified using lymphatic vascular endothelial-specific hyaluronic acid
receptor-1 (LYVE-1) and podoplanin as specific immunohistochemical markers for lymphatic vascular endothe-lium. Baseline tumor characteristics included intra- and extraocular tumor size, 2009 tumor, node, metastasis(TNM) classification, route of extraocular spread, tumor cell type, mitotic rate, Ki-67 proliferation-index, micro-vascular patterns and density, tumor-infiltrating lymphocytes and macrophages, and expression of humanleukocyte antigen (HLA) class I and insulin-like growth factor-1 receptor. Kaplan-Meier and Cox regressionanalyses of melanoma-specific survival were performed.
Main Outcome Measures: Prevalence of intraocular LYVE-1�/podoplanin� lymphatic vessels and associ-ation with intraocular tumor characteristics and metastasis-free survival.
Results: Intraocular LYVE-1� and podoplanin� lymphatic vessels could be detected in 12 (60%) of 20 ciliarybody melanomas with extraocular extension. Presence of intraocular LYVE-1�/podoplanin� lymphatic vesselswas significantly associated with larger intra- (P � 0.002) and extraocular tumor size (P�0.001), higher TNMcategories (P � 0.004), epithelioid cellularity (P � 0.016), higher mitotic rate (P � 0.003), higher Ki-67 prolifer-ation-index (P � 0.049), microvascular networks (P � 0.005), higher microvascular density (P � 0.003), moretumor-infiltrating macrophages (P � 0.002), higher expression of HLA class I (P � 0.046), and insulin-like growthfactor-1 receptor (P � 0.033), but not significantly with route of extraocular spread (P � 0.803), and tumor-infiltrating lymphocytes (P � 0.069). Melanoma-specific mortality rates increased significantly with the presenceof intraocular LYVE-1�/podoplanin� lymphatic vessels (P � 0.008). By multivariate Cox regression, tumor size(hazard ratio, 14.40; P � 0.002), and presence of intraocular lymphatic vessels (hazard ratio, 8.09; P � 0.04) werestrong prognostic predictors of mortality.
Conclusions: Intraocular peritumoral lymphangiogenesis seems to be associated with an increased mortalityrisk in patients with ciliary body melanomas and extraocular extension. This association may be primarily because ofan association of intraocular lymphangiogenesis with greater tumor size and increased malignancy.
Financial Disclosure(s): The authors have no commercial or proprietary interest in any of the materials
discussed in this article. Ophthalmology 2010;117:334–342 © 2010 by the American Academy of Ophthalmology.Ciliary body melanomas with extraocular extension, compos-ing up to 4% of uveal melanomas, have consistently beencorrelated with poorer prognosis for survival.1,2 Recently, thiscorrelation was attributed to an increased malignancy of theintraocular tumor1 with larger tumor dimensions,3,4 epithelioidcellularity,3,5 higher mitotic rates,3 closed connective tissueloops3,6,7 and monosomy 3.3,8,9 Further independent predictorsof melanoma-related mortality documented in �1 study in-clude gene expression profiling,3,10 mean diameter of the 10largest nucleoli,3,11,12 Ki-67 immunoreactivity,3,12 microvas-
cular density,3,13,14 number of tumor-infiltrating lympho-334 © 2010 by the American Academy of OphthalmologyPublished by Elsevier Inc.
cytes3,15,16 and macrophages,3,17 and level of human leukocyteantigen (HLA) class I3,18 and insulin-like growth factor-1receptor expression.3,19
Uveal melanomas may metastasize predominantly byhematogenous spread with strong hepatic tropism.3,4 How-ever, the rare potential of lymphatic metastasis into theregional lymph nodes has been reported for patients withuveal melanoma and extraocular extension.20,21
Tumor-associated lymphangiogenesis (i.e., outgrowth ofnew from preexisting lymphatic vessels) is considered as
the initial step in lymphogenic metastasis for several tumorsISSN 0161-6420/10/$–see front matterdoi:10.1016/j.ophtha.2009.06.057

Heindl et al � Intraocular Lymphangiogenesis in Ciliary Body Melanomas
(e.g., malignant melanoma of the skin).22 It can be inducedby a variety of tumor cells itself as well as by peritumoralmacrophages with the help of the lymphangiogenic growthfactors, vascular endothelial growth factor (VEGF) C andD, and their specific VEGF receptor 3.23,24 Whereas the roleof peri- versus intratumoral lymphangiogenesis remains con-troversial, its role as a decisive risk factor for tumor metastasisis now established.22,25–27
However, the human eye is—apart from the extraocularconjunctiva28,29—physiologically devoid of lymphatic ves-sels, which is thought to contribute to its special, immune-privileged state.30 Secondary to a variety of corneal dis-eases, blood and lymphatic vessels can invade the normallyavascular cornea.31,32
In a similar fashion, we recently noted that intraocularmelanomas of the ciliary body can attract extraocular lym-phatics into the normally alymphatic eye when extraoculartumor extension provides routes of entry through thesclera.33 Otherwise, the sclera seems to be a natural barrieragainst invasion of preexisting lymphatic vessels into theeye, despite coexpression of both lymphangiogenic VEGFC and its VEGF receptor 3 in about half of the patients in aseries of uveal melanomas without extraocular spread.34
The present study investigates the hypothesis that intraoc-ular tumor-associated lymphangiogenesis contributes to prog-nosis of ciliary body melanomas with extraocular extensionand to study its association with other characteristics of the tumor.
Patients and Methods
Between January 1995 and May 2007, 102 consecutive patientswith malignant melanoma of the ciliary body underwent primaryenucleation at the Department of Ophthalmology, University EyeHospital, Friedrich-Alexander University Erlangen, Nürnberg,Germany. All enucleated globes were fixed in a buffered 4%formaldehyde-glutaraldehyde solution, dehydrated, and embeddedin paraffin. Multiple serial sections of the entire tumor area cut at5 �m were stained with hematoxylin and eosin, periodic acid-Schiff, S-100 (rabbit, 1:400, Dako, Hamburg, Germany), anti-melanosome HMB-45 (mouse, 1:400, Dako), anti-melanomaPNL-2 (mouse, ready-to-use; Dako), and Melan-A (mouse, 1:50;Dako) and analyzed by 3 independent investigators with a ZeissAxiophot microscope (Zeiss, Oberkochen, Germany) to detectextrascleral tumor extension and to confirm the diagnosis his-topathologically as well as immunohistochemically. Inclusion cri-teria for this retrospective, nonrandomized, clinicopathologic, single-center study were (1) confirmed diagnosis of a ciliary body melanomawith extraocular extension and (2) a minimum follow-up period of 12months after enucleation. Altogether, a total of 20 consecutivepatients fulfilled these criteria and were included in the presentclinicopathologic study carried out in conformance with the tenetsof the Helsinki Declaration. Institutional review board/ethics com-mittee approval was not required in these instances.
Patient Population and Clinical DataThe 20 patients (11 females and 9 males) had a mean age of 69�4years (range, 59–76). Their clinical files were reviewed retrospec-tively with special regard to tumor staging. Apical tumor height andlargest basal tumor diameter were measured by standardized A- andB-scan ultrasonography. According to the 2009 tumor, node, metas-
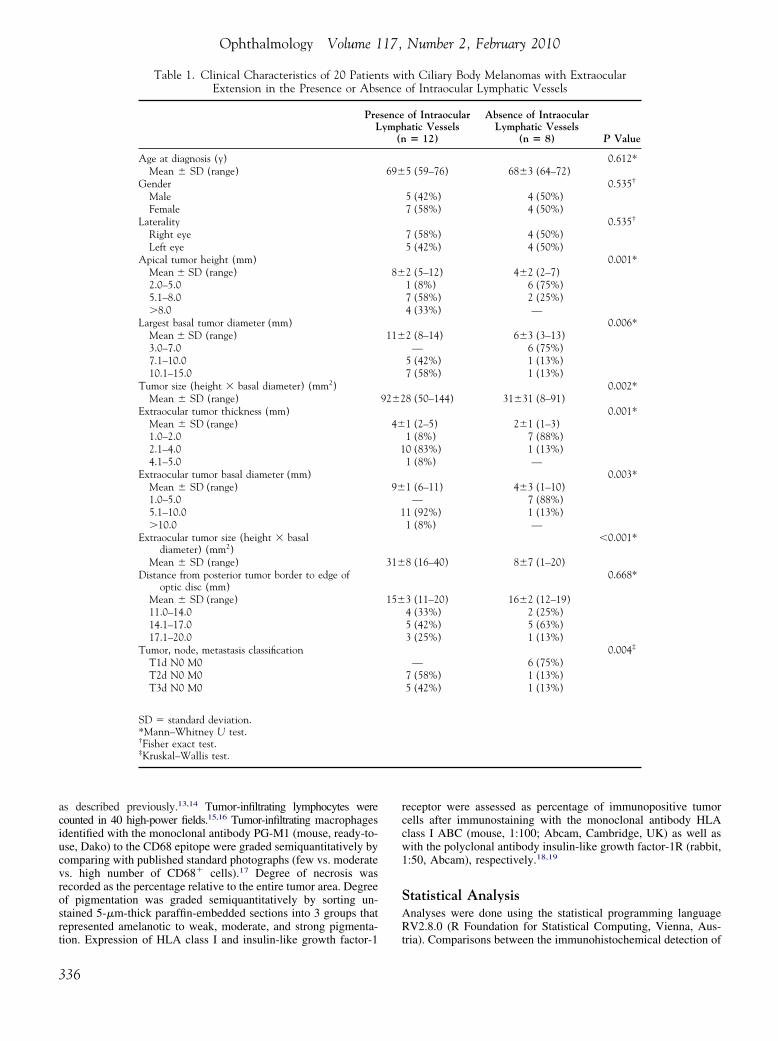
tasis classification system,3 6 tumors (30%) were classified as T1d, 8tumors (40%) as T2d, and 6 tumors (30%) as T3d. In none of thepatients did general physical examination or oncologic workup at thetime of diagnosis reveal any evidence of another primary tumor,hematogenic metastasis, or lymph node metastasis (Table 1).
In a standardized telephone interview in 2008, all patients andtheir physicians were asked for survival and new onset of distantmetastasis or lymph node metastasis. Mean follow-up time was93�26 months (range, 22–130). Eleven patients (55%) developeddistant metastases within a mean time interval of 58�38 months(range, 15–129) after enucleation. In all 11 cases, distant meta-static spread occurred in the liver; in 3 patients, the lung was alsoinvolved. Simultaneously, regional lymph node metastases couldbe detected in 3 patients (15%): 1 patient developed clinically andhistologically proven cervical and thoracic lymph node metastases18 months after enucleation, and 2 patients only clinically diag-nosed, cervical lymph node metastases 2 and 3 years postopera-tively. Out of all 20 patients, 11 (55%) died from melanoma,and 1 (5%) from cardiovascular disease. The 5-year cumulativemetastasis-free survival rate was 53%�11%.
Immunohistochemical Detection of PeritumoralIntraocular Lymphatic Vessels
To identify lymphatic vessels, immunohistochemistry was performedin all 20 cases as described previously.31 A polyclonal antibodyagainst the human lymphatic vascular endothelial-specific hyaluronicacid receptor (LYVE-1) (rabbit, 1:100; ACRIS, Herford, Germany)35
and a monoclonal antibody against the human lymphatic vascularendothelial-specific glycoprotein podoplanin D2-40 (mouse, 1:40,AbD Serotec, Kidlington, UK)36 were used. Serial sections wereevaluated for evidence of intraocular LYVE-1� and podoplanin�
lymphatic vessels by 3 independent investigators in a masked fashionusing a Zeiss Axiophot microscope after digital documentation. Pres-ence of intraocular lymphatic vessels was defined as detection of atleast 5 LYVE-1� and podoplanin� vessels per section with an eryth-rocyte-free lumen located below the inner scleral layers within theintraocular tumor component.
Assessment of Established HistopathologicPrognostic Factors
The route of extraocular tumor spread was categorized in aqueousdrainage channels, ciliary arteries, vortex veins, and ciliary nerves.1
The size of the extraocular tumor component was measured onhistologic sections using digital analysis (AxioVision 4.6; Zeiss),with the greatest thickness and the greatest periscleral diameter ofthe extraocular extension being recorded.1 Each of the followingparameters was assessed in the intraocular tumor component.Predominant tumor cell type was registered according to the mod-ified Callender classification (epithelioid, mixed, or spindle) froma hematoxylin-and-eosin–stained section.5 Mitotic rate was as-sessed by counting the number of mitotic figures in 40 high-powerfields.3 The mean diameter of the 10 largest nucleoli (MLN) wasmeasured along a central 5-mm long strip from silver-stainedslides as described by Al-Jamal et al.11,12 Ki-67 proliferation indexwas detected as percentage of tumor cells immunopositive with themonoclonal Ki-67 antibody (mouse, 1:100; AbD Serotec).12 Ex-travascular matrix patterns were identified under a green filteraccording to the criteria of Folberg et al6 after bleaching withpotassium permanganate and oxalic acid and staining with periodicacid-Schiff without counterstain to facilitate recognition of closedmicrovascular loops and networks.6,7 Microvascular density wasdetermined with the monoclonal antibody QBEnd/10 (mouse,ready-to-use; Medac, Hamburg, Germany) to the CD34 epitope of
endothelial cells in the most highly vascularized area of 0.313 mm2335
Ophthalmology Volume 117, Number 2, February 2010
as described previously.13,14 Tumor-infiltrating lymphocytes werecounted in 40 high-power fields.15,16 Tumor-infiltrating macrophagesidentified with the monoclonal antibody PG-M1 (mouse, ready-to-use, Dako) to the CD68 epitope were graded semiquantitatively bycomparing with published standard photographs (few vs. moderatevs. high number of CD68� cells).17 Degree of necrosis wasrecorded as the percentage relative to the entire tumor area. Degreeof pigmentation was graded semiquantitatively by sorting un-stained 5-�m-thick paraffin-embedded sections into 3 groups thatrepresented amelanotic to weak, moderate, and strong pigmenta-
Table 1. Clinical Characteristics of 20 PatienExtension in the Presence or Abs
PreL
Age at diagnosis (y)Mean � SD (range)
GenderMaleFemale
LateralityRight eyeLeft eye
Apical tumor height (mm)Mean � SD (range)2.0–5.05.1–8.0�8.0
Largest basal tumor diameter (mm)Mean � SD (range)3.0–7.07.1–10.010.1–15.0
Tumor size (height � basal diameter) (mm2)Mean � SD (range)
Extraocular tumor thickness (mm)Mean � SD (range)1.0–2.02.1–4.04.1–5.0
Extraocular tumor basal diameter (mm)Mean � SD (range)1.0–5.05.1–10.0�10.0
Extraocular tumor size (height � basaldiameter) (mm2)
Mean � SD (range)Distance from posterior tumor border to edge of
optic disc (mm)Mean � SD (range)11.0–14.014.1–17.017.1–20.0
Tumor, node, metastasis classificationT1d N0 M0T2d N0 M0T3d N0 M0
SD � standard deviation.*Mann–Whitney U test.†Fisher exact test.‡Kruskal–Wallis test.
tion. Expression of HLA class I and insulin-like growth factor-1
336
receptor were assessed as percentage of immunopositive tumorcells after immunostaining with the monoclonal antibody HLAclass I ABC (mouse, 1:100; Abcam, Cambridge, UK) as well aswith the polyclonal antibody insulin-like growth factor-1R (rabbit,1:50, Abcam), respectively.18,19
Statistical AnalysisAnalyses were done using the statistical programming languageRV2.8.0 (R Foundation for Statistical Computing, Vienna, Aus-
th Ciliary Body Melanomas with Extraocularof Intraocular Lymphatic Vessels
of Intraocularatic Vessels� 12)
Absence of IntraocularLymphatic Vessels
(n � 8) P Value
0.612*5 (59–76) 68�3 (64–72)
0.535†
5 (42%) 4 (50%)7 (58%) 4 (50%)
0.535†
7 (58%) 4 (50%)5 (42%) 4 (50%)
0.001*2 (5–12) 4�2 (2–7)1 (8%) 6 (75%)7 (58%) 2 (25%)4 (33%) —
0.006*2 (8–14) 6�3 (3–13)
— 6 (75%)5 (42%) 1 (13%)7 (58%) 1 (13%)
0.002*8 (50–144) 31�31 (8–91)
0.001*1 (2–5) 2�1 (1–3)1 (8%) 7 (88%)0 (83%) 1 (13%)1 (8%) —
0.003*1 (6–11) 4�3 (1–10)
— 7 (88%)1 (92%) 1 (13%)1 (8%) —
�0.001*
8 (16–40) 8�7 (1–20)0.668*
3 (11–20) 16�2 (12–19)4 (33%) 2 (25%)5 (42%) 5 (63%)3 (25%) 1 (13%)
0.004‡
— 6 (75%)7 (58%) 1 (13%)5 (42%) 1 (13%)
ts wience
senceymph
(n
69�
8�
11�
92�2
4�
1
9�
1
31�
15�
tria). Comparisons between the immunohistochemical detection of
GF-1R
Heindl et al � Intraocular Lymphangiogenesis in Ciliary Body Melanomas
peritumoral intraocular lymphatic vessels and the other clinical orhistopathologic variables were performed using the nonparametricMann-Whitney U test, the Fisher exact test, and the Kruskal-Wallis test. Survival rates with standard error were determinedaccording to the Kaplan-Meier method and compared using thegender-stratified log-rank test. We formulated a multivariate Cox
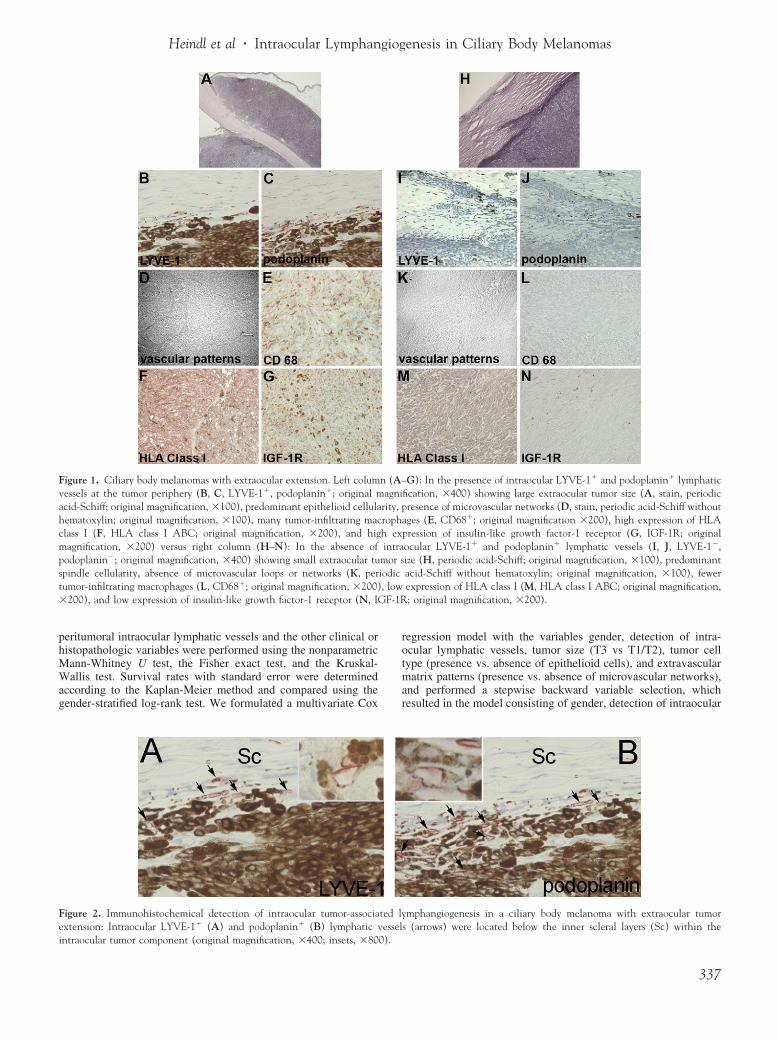
Figure 1. Ciliary body melanomas with extraocular extension. Left columvessels at the tumor periphery (B, C, LYVE-1�, podoplanin�; original macid-Schiff; original magnification, �100), predominant epithelioid cellulahematoxylin; original magnification, �100), many tumor-infiltrating macclass I (F, HLA class I ABC; original magnification, �200), and higmagnification, �200) versus right column (H–N): In the absence ofpodoplanin�; original magnification, �400) showing small extraocular tuspindle cellularity, absence of microvascular loops or networks (K, pertumor-infiltrating macrophages (L, CD68�; original magnification, �200)�200), and low expression of insulin-like growth factor-1 receptor (N, I
Figure 2. Immunohistochemical detection of intraocular tumor-associaextension: Intraocular LYVE-1� (A) and podoplanin� (B) lymphatic v
intraocular tumor component (original magnification, �400; insets, �800).regression model with the variables gender, detection of intra-ocular lymphatic vessels, tumor size (T3 vs T1/T2), tumor celltype (presence vs. absence of epithelioid cells), and extravascularmatrix patterns (presence vs. absence of microvascular networks),and performed a stepwise backward variable selection, whichresulted in the model consisting of gender, detection of intraocular
G): In the presence of intraocular LYVE-1� and podoplanin� lymphaticfication, �400) showing large extraocular tumor size (A, stain, periodicresence of microvascular networks (D, stain, periodic acid-Schiff without
ages (E, CD68�; original magnification �200), high expression of HLApression of insulin-like growth factor-1 receptor (G, IGF-1R; originalocular LYVE-1� and podoplanin� lymphatic vessels (I, J, LYVE-1�,ize (H, periodic acid-Schiff; original magnification, �100), predominantacid-Schiff without hematoxylin; original magnification, �100), fewerexpression of HLA class I (M, HLA class I ABC; original magnification,; original magnification, �200).
mphangiogenesis in a ciliary body melanoma with extraocular tumors (arrows) were located below the inner scleral layers (Sc) within the
n (A–agni
rity, prophh exintra
mor siodic, low
ted lyessel
337

Ophthalmology Volume 117, Number 2, February 2010
lymphatic vessels, and tumor size. To examine the other well-known risk factors tumor cell type and extravascular matrix pat-terns, we additionally fitted and compared a gender-adjusted Coxregression model for each of the 4 risk factors. The regressioncoefficients and hazard ratios (HR) with 95% confidence intervalswere calculated. P�0.05 was considered significant.
Results
Peritumoral Intraocular Lymphatic VesselsIntraocular LYVE-1� and podoplanin� lymphatic vessels could bedetected in 12 (60%) of the 20 ciliary body melanomas withextraocular extension. They were found only at the tumor periph-ery directly adjacent to the sclera within the eye, whereas thecentral aspects of the intraocular tumor showed no LYVE-1� orpodoplanin� lymphatic vessels (Figs 1 and 2). The number ofintraocular lymphatic vessels averaged 19�7 (range, 11–30) persection.
In the extraocular tumor component LYVE-1� and podoplanin�
lymphatic vessels could be observed in all 20 melanomas of theciliary body with extraocular tumor spread, but only within the tu-mor periphery adjacent to the conjunctiva and not within the central as-pects of the extraocular tumor part.
Association with Other Prognostic ParametersThe presence of intraocular LYVE-1�/podoplanin� lymphaticvessels was significantly associated with greater size of the in-traocular melanoma (P � 0.002), greater size of the extraoculartumor component (P�0.001), higher T categories of tumor, node,metastasis classification (P � 0.004), presence of epithelioid tu-mor cells (P � 0.016), higher mitotic rate (P � 0.003), higherKi-67 proliferation index (P � 0.049), presence of microvascularnetworks (P � 0.005), greater microvascular density (P � 0.003),more tumor-infiltrating macrophages (P � 0.002), greater expres-sion of HLA class I (P � 0.046), and greater expression ofinsulin-like growth factor-1 receptor (P � 0.033).
No significant association was observed between the presenceof intraocular LYVE-1�/podoplanin� lymphatic vessels and age(P � 0.612), gender (P � 0.535), route of extraocular spread (P �0.803), MLN (P � 0.122), number of tumor-infiltrating lympho-cytes (P � 0.069), degree of necrosis (P � 0.938), and degree oftumor pigmentation (P � 0.566; Tables 1 and 2).
Association with Metastasis-free SurvivalPatients developing distant metastases revealed significantly moreoften intraocular LYVE-1�/podoplanin� lymphatic vessels thanpatients without metastatic spread (P � 0.040, Fisher exact test).Regional lymph node metastasis occurred in 3 patients showing allintraocular LYVE-1�/podoplanin� lymphatic vessels.
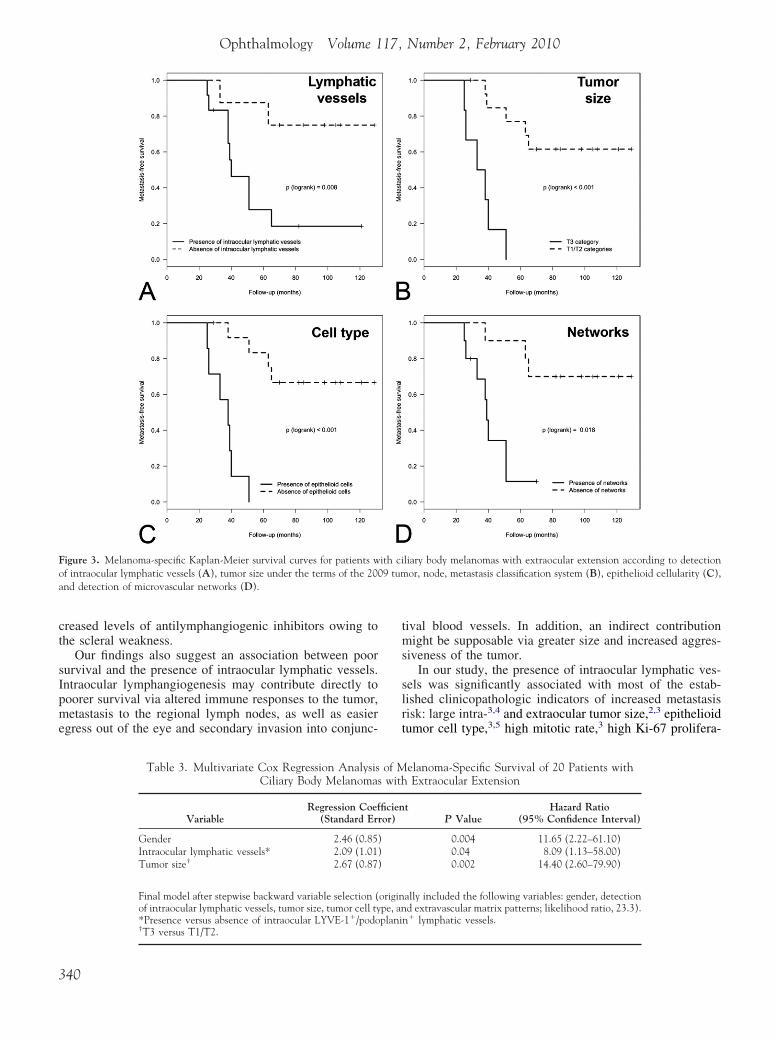
The 5-year, cumulative, metastasis-free survival rate was 28%(standard error 14%) for ciliary body melanomas with extraocular exten-sion disclosing intraocular LYVE-1�/podoplanin� lymphatic vessels,and 88% (standard error 12%) for those without intraocular lym-phangiogenesis. Presence of intraocular LYVE-1�/podoplanin� lym-phatic vessels was significantly associated with lower metastasis-freesurvival rates (P � 0.008; Fig 3A).
Lower melanoma-specific survival was also associated withlarger tumor size (P�0.001; Fig 3B), presence of epithelioid tumorcells (P�0.001; Fig 3C), and presence of microvascular networks(P � 0.018; Fig 3D).
Multivariate Cox regression analysis identified the male gender
(HR, 11.65; P � 0.004), the presence of intraocular lymphatic vessels338
(HR, 8.09; P � 0.04), and the tumor size (HR, 14.40; P � 0.002) assignificant indicators of melanoma-specific survival (Table 3).
By gender-adjusted Cox regression analysis, the presence of in-traocular lymphatic vessels was a strong prognostic predictor ofsurvival (HR, 8.91; P � 0.011), similar to extravascular matrixpatterns (HR, 5.79; P � 0.025), but weaker than tumor size (HR,21.56; P�0.001) and tumor cell type (HR, 24.95; P�0.001; Table 4).
Discussion
This retrospective study of 20 consecutive patients enucle-ated for a ciliary body melanoma with extraocular extensionrevealed a strong association between poor survival andpresence of intraocular peritumoral LYVE-1�/podoplanin�
lymphatic vessels. However, intraocular lymphangiogenesiswas also associated with an increased malignancy of theintraocular tumor with greater tumor dimensions and moremalignant cytology.
Although tumor-associated lymphangiogenesis is well-established as a decisive risk factor for lymphogenic metas-tasis in several tumors (e.g., malignant melanoma of theskin),22,25–27 its role in uveal melanomas is unknown. Al-though malignant melanomas of the uvea may metastasizepredominantly by hematogenous spread with strong hepatictropism,3,4 the rare potential of lymphatic metastasis into theregional lymph nodes has been reported for uveal melano-mas with extraocular extension.20,21 The incidence of cer-vical lymph node metastases from uveal melanomas hasbeen determined up to 6.5%.21 For these patients, invasionof tumor cells into extraocular conjunctival lymphatic ves-sels was suggested by Dithmar et al.20 In our series, wecould not detect tumor cells within the lumina of the in-traocular lymphatic vessels immunohistochemically. Evenif our data do not prove that intraocular lymphatics actuallyare functional or are indeed involved in transport of tumorcells to the regional lymph node, it might be possible that inciliary body melanomas with extraocular extension, lym-phatic spread can start even within the eye into intraocularperitumoral lymphatic vessels. However, in our series re-gional lymph node metastasis occurred only in 3 patients, allshowing intraocular LYVE-1�/podoplanin� lymphatic ves-sels. This suggests an increased risk of lymphatic spread fortumors with intraocular lymphatic vessels, although ciliarybody melanomas with extraocular extension have access toconjunctival lymphatic vessels.
To our knowledge, intraocular lymphatic vessels weredetected for the first time in this study. Apart from theextraocular conjunctiva,28,29 the human eye is physiologi-cally devoid of lymphatic vessels.30 Even the normal humanchoroid endowed with a significant number of LYVE-1� mac-rophages does not contain typical lymphatic vessels.37 Al-though we cannot rule out the remote possibility of a de novoformation of intraocular lymphatics, we favor the concept ofattracting conjunctival lymphatic vessels into the eye (sec-ondary intraocular lymphangiogenesis), because they werelocalized adjacent to the sclera and occurred only in thepresence of the sclera defect. This kind of “lymphangio-taxis” may be the result of increased levels of prolym-
phangiogenic growth factors such as VEGF C34 and de-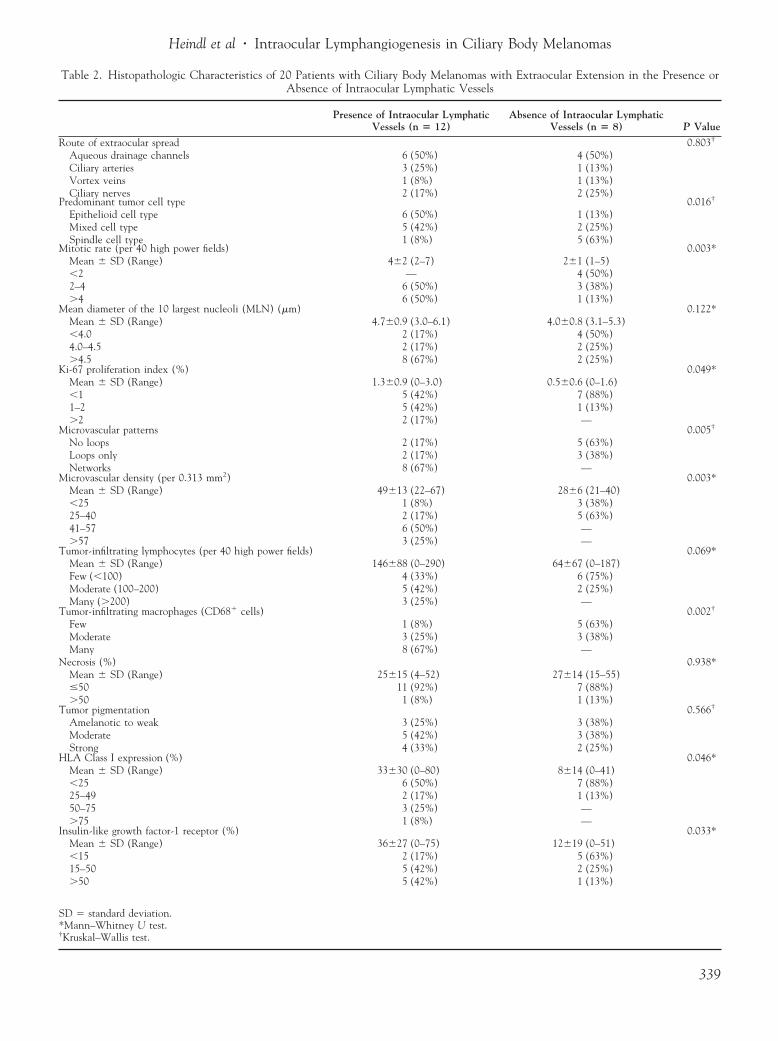
Heindl et al � Intraocular Lymphangiogenesis in Ciliary Body Melanomas
Table 2. Histopathologic Characteristics of 20 Patients with Ciliary Body Melanomas with Extraocular Extension in the Presence orAbsence of Intraocular Lymphatic Vessels
Presence of Intraocular LymphaticVessels (n � 12)
Absence of Intraocular LymphaticVessels (n � 8) P Value
Route of extraocular spread 0.803†
Aqueous drainage channels 6 (50%) 4 (50%)Ciliary arteries 3 (25%) 1 (13%)Vortex veins 1 (8%) 1 (13%)Ciliary nerves 2 (17%) 2 (25%)
Predominant tumor cell type 0.016†
Epithelioid cell type 6 (50%) 1 (13%)Mixed cell type 5 (42%) 2 (25%)Spindle cell type 1 (8%) 5 (63%)
Mitotic rate (per 40 high power fields) 0.003*Mean � SD (Range) 4�2 (2–7) 2�1 (1–5)�2 — 4 (50%)2–4 6 (50%) 3 (38%)�4 6 (50%) 1 (13%)
Mean diameter of the 10 largest nucleoli (MLN) (�m) 0.122*Mean � SD (Range) 4.7�0.9 (3.0–6.1) 4.0�0.8 (3.1–5.3)�4.0 2 (17%) 4 (50%)4.0–4.5 2 (17%) 2 (25%)�4.5 8 (67%) 2 (25%)
Ki-67 proliferation index (%) 0.049*Mean � SD (Range) 1.3�0.9 (0–3.0) 0.5�0.6 (0–1.6)�1 5 (42%) 7 (88%)1–2 5 (42%) 1 (13%)�2 2 (17%) —
Microvascular patterns 0.005†
No loops 2 (17%) 5 (63%)Loops only 2 (17%) 3 (38%)Networks 8 (67%) —
Microvascular density (per 0.313 mm2) 0.003*Mean � SD (Range) 49�13 (22–67) 28�6 (21–40)�25 1 (8%) 3 (38%)25–40 2 (17%) 5 (63%)41–57 6 (50%) —�57 3 (25%) —
Tumor-infiltrating lymphocytes (per 40 high power fields) 0.069*Mean � SD (Range) 146�88 (0–290) 64�67 (0–187)Few (�100) 4 (33%) 6 (75%)Moderate (100–200) 5 (42%) 2 (25%)Many (�200) 3 (25%) —
Tumor-infiltrating macrophages (CD68� cells) 0.002†
Few 1 (8%) 5 (63%)Moderate 3 (25%) 3 (38%)Many 8 (67%) —
Necrosis (%) 0.938*Mean � SD (Range) 25�15 (4–52) 27�14 (15–55)�50 11 (92%) 7 (88%)�50 1 (8%) 1 (13%)
Tumor pigmentation 0.566†
Amelanotic to weak 3 (25%) 3 (38%)Moderate 5 (42%) 3 (38%)Strong 4 (33%) 2 (25%)
HLA Class I expression (%) 0.046*Mean � SD (Range) 33�30 (0–80) 8�14 (0–41)�25 6 (50%) 7 (88%)25–49 2 (17%) 1 (13%)50–75 3 (25%) —�75 1 (8%) —
Insulin-like growth factor-1 receptor (%) 0.033*Mean � SD (Range) 36�27 (0–75) 12�19 (0–51)�15 2 (17%) 5 (63%)15–50 5 (42%) 2 (25%)�50 5 (42%) 1 (13%)
SD � standard deviation.*Mann–Whitney U test.†
Kruskal–Wallis test.339
Ophthalmology Volume 117, Number 2, February 2010
creased levels of antilymphangiogenic inhibitors owing tothe scleral weakness.
Our findings also suggest an association between poorsurvival and the presence of intraocular lymphatic vessels.Intraocular lymphangiogenesis may contribute directly topoorer survival via altered immune responses to the tumor,metastasis to the regional lymph nodes, as well as easieregress out of the eye and secondary invasion into conjunc-
Figure 3. Melanoma-specific Kaplan-Meier survival curves for patients wof intraocular lymphatic vessels (A), tumor size under the terms of the 20and detection of microvascular networks (D).
Table 3. Multivariate Cox Regression AnalysisCiliary Body Melanomas
VariableRegression Coef
(Standard Er
Gender 2.46 (0.85Intraocular lymphatic vessels* 2.09 (1.01Tumor size† 2.67 (0.87
Final model after stepwise backward variable selection (of intraocular lymphatic vessels, tumor size, tumor cell ty*Presence versus absence of intraocular LYVE-1�/podo†
T3 versus T1/T2.340
tival blood vessels. In addition, an indirect contributionmight be supposable via greater size and increased aggres-siveness of the tumor.
In our study, the presence of intraocular lymphatic ves-sels was significantly associated with most of the estab-lished clinicopathologic indicators of increased metastasisrisk: large intra-3,4 and extraocular tumor size,2,3 epithelioidtumor cell type,3,5 high mitotic rate,3 high Ki-67 prolifera-
liary body melanomas with extraocular extension according to detectionor, node, metastasis classification system (B), epithelioid cellularity (C),
elanoma-Specific Survival of 20 Patients withExtraocular Extension
tP Value
Hazard Ratio(95% Confidence Interval)
0.004 11.65 (2.22–61.10)0.04 8.09 (1.13–58.00)0.002 14.40 (2.60–79.90)
ally included the following variables: gender, detectiond extravascular matrix patterns; likelihood ratio, 23.3).
n� lymphatic vessels.
ith ci09 tum
of Mwith
ficienror)
)))
originpe, anplani

Heindl et al � Intraocular Lymphangiogenesis in Ciliary Body Melanomas
tion index,3,12 closed connective tissue loops,3,6,7 high mi-crovascular density,3,13,14 many tumor-infiltrating macro-phages,3,17 and high levels of HLA class I3,18 and insulin-likegrowth factor-1 receptor expression.3,19 For association withhigher MLN,3,11,12 and more tumor-infiltrating lympho-cytes3,15,16 we could calculate only a statistical trend withoutsignificance. The route of extraocular spread correlated nei-ther with detection of intraocular lymphatic vessels nor withmelanoma-specific survival, which is in agreement with aprevious report.1 Our findings suggest that intraocular lym-phatic vessels are more often present in larger tumors withmore malignant cytology, likely explaining the lower me-tastasis-free survival rate in presence of intraocular lym-phangiogenesis. Because Cox regression analyses showedthe presence of intraocular LYVE-1�/podoplanin� lym-phatic vessels as a weaker predictor of survival than tumorsize and tumor cell type, it cannot be excluded that intraoc-ular lymphangiogenesis is merely an indicator of increasedtumor malignancy and size rather than a cause of increasedmortality.
The main strength of our study is the large number ofincluded histopathologic and immunohistochemical tumorcharacteristics that have been shown to be independentpredictors of subsequent survival in �1 study.3 To ourknowledge, no other studies have investigated all thesefactors in such detail for ciliary body melanomas withextraocular extension. Despite this, our study has severalweaknesses. First, the number of included patients wassmall. Therefore, our results should be verified in largerprospective series. Second, cytogenetic analysis of chromo-somes 3 and 83,8,9 as well as gene expression profiling,3,10
both ranking among the strongest predictors of melanoma-specific mortality, were not undertaken.
Nevertheless, the data from the present study may sug-gest a potential for novel anti-(lymph)angiogenic therapies,such as bevacizumab (Avastin), in patients with uveal mel-anomas developing extraocular extension to prevent lym-phatic spread of the tumor to regional lymph nodes.38–40
In conclusion, intraocular peritumoral lymphangiogen-esis seems to be associated with an increased mortality riskin patients with ciliary body melanomas and extraocularextension. This association may be primarily because oflarger tumors with histologic and immunohistochemical
Table 4. Gender-Adjusted Cox Regression Anwith Ciliary Body Melanom
VariableRegression Coefficien
(Standard Error)
Intraocular lymphatic vessels† 2.19 (0.86)Tumor size‡ 3.07 (0.88)Tumor cell type§ 3.22 (0.96)Extravascular matrix patterns� 1.76 (0.78)
*Chi-square test (2 sided).†Presence versus absence of intraocular LYVE-1�/podo‡T3 versus T1/T2.§Presence versus absence of epithelioid cells.�Presence versus absence of microvascular networks.
features of increased malignancy.
References
1. Coupland SE, Campbell I, Damato B. Routes of extraocularextension of uveal melanoma: risk factors and influence onsurvival probability. Ophthalmology 2008;115:1778–85.
2. Pach JM, Robertson DM, Taney BS, et al. Prognostic factorsin choroidal and ciliary body melanomas with extrascleralextension. Am J Ophthalmol 1986;101:325–31.
3. Kivelä T, Harbour JW, Coupland SE, et al. Malignant mela-noma of the uvea. In: Edge SE, Byrd DR, Carducci MA,Compton CA (eds): AJCC cancer staging manual. 7th ed. NewYork: Springer; 2009.
4. Kujala E, Kivelä T. Tumor, node, metastasis classification ofmalignant ciliary body and choroidal melanoma: evaluation ofthe 6th edition and future directions. Ophthalmology 2005;112:1135–44.
5. McLean IW, Foster WD, Zimmerman LE, Gamel JW. Mod-ifications of Callender’s classification of uveal melanoma atthe armed forces institute of pathology. Am J Ophthalmol1983;96:502–9.
6. Folberg R, Rummelt V, Parys-van Ginderdeuren R, et al. Theprognostic value of tumor blood vessel morphology in primaryuveal melanoma. Ophthalmology 1993;100:1389–98.
7. Mäkitie T, Summanen P, Tarkkanen A, Kivelä T. Microvascularloops and networks as prognostic indicators in choroidal andciliary body melanomas. J Natl Cancer Inst 1999;91:359–67.
8. Prescher G, Bornfeld N, Hirche H, et al. Prognostic implica-tions of monosomy 3 in uveal melanoma. Lancet 1996;347:1222–5.
9. Damato B, Duke C, Coupland SE, et al. Cytogenetics of uvealmelanoma: a 7-year clinical experience. Ophthalmology 2007;114:1925–31.
10. Worley LA, Onken MD, Person E, et al. Transcriptomicversus chromosomal prognostic markers and clinical outcomein uveal melanoma. Clin Cancer Res 2007;13:1466–71.
11. Al-Jamal RT, Mäkitie T, Kivelä T. Nucleolar diameter andmicrovascular factors as independent predictors of mortalityfrom malignant melanoma of the choroid and ciliary body.Invest Ophthalmol Vis Sci 2003;44:2381–9.
12. Al-Jamal RT, Kivelä T. Ki-67 immunopositivity in choroidaland ciliary body melanoma with respect to nucleolar diameterand other prognostic factors. Current Eye Res 2006;31:57–67.
13. Foss AJE, Alexander RA, Jefferies LW, et al. Microvesselcount predicts survival in uveal melanoma. Cancer Res 1996;56:2900–3.
14. Mäkitie T, Summanen P, Tarkkanen A, Kivelä T. Microvas-
of Melanoma-Specific Survival of 20 Patientsith Extraocular Extension
LikelihoodRatio* P Value
Hazard Ratio(95% Confidence Interval)
12.2 0.011 8.91 (1.65–48.10)18.0 �0.001 21.56 (3.88–119.10)18.8 �0.001 24.95 (3.78–165.00)9.27 0.025 5.79 (1.25–26.80)
� lymphatic vessels.
alysisas w
t
planin
cular density in predicting survival of patients with choroidal
341

Ophthalmology Volume 117, Number 2, February 2010
and ciliary body melanoma. Invest Ophthalmol Vis Sci1999;40:2471–80.
15. Durie FH, Campbell AM, Lee WR, Damato BE. Analysis oflymphocytic infiltration in uveal melanoma. Invest Ophthal-mol Vis Sci 1990;31:2106–10.
16. de la Cruz PO Jr, Specht CS, McLean IW. Lymphocytic infil-tration in uveal malignant melanoma. Cancer 1990;65:112–5.
17. Mäkitie T, Summanen P, Tarkkanen A, Kivelä T. Tumor-infiltrating macrophages (CD68� cells) and prognosis in ma-lignant uveal melanoma. Invest Ophthalmol Vis Sci 2001;42:1414–21.
18. Blom DJ, Luyten GP, Mooy C, et al. Human leukocyte antigenclass I expression. Marker of poor prognosis in uveal mela-noma. Invest Ophthalmol Vis Sci 1997;38:1865–72.
19. All-Ericsson C, Girnita L, Seregard S, et al. Insulin-likegrowth factor-1 receptor in uveal melanoma: a predictor formetastatic disease and a potential therapeutic target. InvestOphthalmol Vis Sci 2002;43:1–8.
20. Dithmar S, Diaz CE, Grossniklaus HE. Intraocular melanomaspread to regional lymph nodes: report of two cases. Retina2000;20:76–9.
21. Tojo D, Wenig BL, Resnick KI. Incidence of cervical metas-tasis from uveal melanoma: implications for treatment. HeadNeck 1995;17:137–9.
22. Stacker SA, Achen MG, Jussila L, et al. Lymphangiogenesisand cancer metastasis. Nat Rev Cancer 2002;2:573–83.
23. Karkkainen MJ, Petrova TV. Vascular endothelial growthfactor receptors in the regulation of angiogenesis and lym-phangiogenesis. Oncogene 2000;19:5598–605.
24. Schoppmann SF, Birner P, Stockl J, et al. Tumor-associatedmacrophages express lymphatic endothelial growth factorsand are related to peritumoral lymphangiogenesis. Am JPathol 2002;161:947–56.
25. Padera TP, Kadambi A, di Tomaso E, et al. Lymphatic me-tastasis in the absence of functional intratumor lymphatics.Science 2002;296:1883–6.
26. Dadras SS, Paul T, Bertoncini J, et al. Tumor lymphangiogenesis:a novel prognostic indicator for cutaneous melanoma metastasisand survival. Am J Pathol 2003;162:1951–60.
27. Streit M, Detmar M. Angiogenesis, lymphangiogenesis, andmelanoma metastasis. Oncogene 2003;22:3172–9.
28. Kruse FE, Voelcker HE, Naumann GOH. Konjunktiva [inGerman]. In: Naumann GOH, ed. Pathologie des Auges. Berlin:
Springer; 1997:379–506.the European Society of Ophthalmology, November 2008, Atlanta, Georgia.
342
29. Cursiefen C, Kruse FE, Naumann GOH. Cornea and limbus. In:Naumann GOH, Holbach L, Kruse FE, eds. Applied pathologyfor ophthalmic microsurgeons. Berlin: Springer; 2008:97–130.
30. Streilein JW, Yamada J, Dana MR, Ksander BR. Anteriorchamber-associated immune deviation, ocular immune privi-lege, and orthotopic allografts. Transplant Proc 1999;31:1472–5.
31. Cursiefen C, Schlotzer-Schrehardt U, Kuchle M, et al. Lym-phatic vessels in vascularized human corneas: immunohisto-chemical investigation using LYVE-1 and podoplanin. InvestOphthalmol Vis Sci 2002;43:2127–35.
32. Cursiefen C, Chen L, Dana MR, Streilein JW. Corneallymphangiogenesis: evidence, mechanisms, and implicationsfor corneal transplant immunology. Cornea 2003;22:273–81.
33. Heindl LM, Hofmann TN, Knorr HLJ, et al. Intraocular lym-phangiogenesis in malignant melanomas of the ciliary bodywith extraocular extension. Invest Ophthalmol Vis Sci 2009;50:1988–95.
34. Clarijs R, Schalwijk L, Ruiter DJ, de Waal RM. Lack oflymphangiogenesis despite coexpression of VEGF-C and itsreceptor Flt-4 in uveal melanoma. Invest Ophthalmol Vis Sci2001;42:1422–8.
35. Banerji S, Ni J, Wang SX, et al. LYVE-1, a new homologueof the CD44 glycoprotein, is a lymph-specific receptor forhyaluronan. J Cell Biol 1999;144:789–801.
36. Breiteneder-Geleff S, Soleiman A, Kowalski H, et al. Angio-sarcomas express mixed endothelial phenotypes of blood andlymphatic capillaries: podoplanin as a specific marker forlymphatic endothelium. Am J Pathol 1999;154:385–94.
37. Schroedl F, Brehmer A, Neuhuber W, et al. The normalchoroid is endowed with significant numbers of lymphaticvessel endothelial hyaluronate receptor 1 (LYVE-1)-positivemacrophages. Invest Ophthalmol Vis Sci 2008;49:5222–9.
38. Bock F, Onderka J, Dietrich T, et al. Bevacizumab as a potentinhibitor of inflammatory corneal angiogenesis and lym-phangiogenesis. Invest Ophthalmol Vis Sci 2007;48:2545–52.
39. Regenfuss B, Bock F, Parthasarathy A, Cursiefen C. Corneal(lymph)angiogenesis—from bedside to bench and back: atribute to Judah Folkman. Lymphat Res Biol 2008;6:191–201.
40. Bock F, König Y, Kruse F, et al. Bevacizumab (avastin) eyedrops inhibit corneal neovascularization. Graefes Arch Clin
Exp Ophthalmol 2008;246:281–4.Footnotes and Financial Disclosures
Originally received: February 12, 2009.Final revision: June 15, 2009.Accepted: June 23, 2009.Available online: November 4, 2009. Manuscript no. 2009-195.1 Department of Ophthalmology and Eye Hospital, Ophthalmic PathologyLaboratory, Friedrich-Alexander University Erlangen-Nürnberg, Erlangen,Germany.2 Department of Medical Informatics, Biometry and Epidemiology,Friedrich-Alexander University Erlangen-Nürnberg, Erlangen, Germany.
Presented at: the American Academy of Ophthalmology Joint Meeting with
Financial Disclosure(s):The authors have no proprietary or commercial interest in any of thematerials discussed in this article.
Supported by the German Research Foundation (Priority Research ProjectSFB 643: B10); Interdisciplinary Center for Clinical Research (IZKF, A9);Section Ophthalmic Pathology, German Ophthalmological Society (DOG);ELAN Fonds University Erlangen-Nürnberg.
Correspondence:Ludwig M. Heindl, MD, Department of Ophthalmology and UniversityEye Hospital, Schwabachanlage 6, 91054 Erlangen, Germany. E-mail:
[email protected].




























