Embed Size (px)
Citation preview

Nonerosive Reflux Disease—Current Concepts and DilemmasRonnie Fass, M.D., M. Brian Fennerty, M.D., F.A.C.G., and Nimish Vakil, M.D., F.A.C.G.Section of Gastroenterology, Southern Arizona VA Health Care System and University of Arizona HealthSciences Center, Tucson, Arizona; Division of Gastroenterology, Department of Medicine, Oregon HealthSciences University, Portland, Oregon; and Section of Gastroenterology, Department of Medicine, Universityof Wisconsin Medical School, Milwaukee, Wisconsin
ABSTRACTNonerosive reflux disease is defined as the presence oftypical symptoms of gastroesophageal reflux disease causedby intraesophageal acid in the absence of visible esophagealmucosal injury at endoscopy. Recent studies demonstratethat it is a chronic disease with a significant impact onquality of life, and it is very common in primary caresettings. Treatment with acid inhibitory agents is effective,and proton pump inhibitors are the most effective form oftherapy. (Am J Gastroenterol 2001;96:303–314. © 2001 byAm. Coll. of Gastroenterology)
INTRODUCTION
Symptoms of gastroesophageal reflux disease (GERD) suchas heartburn and acid regurgitation occur weekly in 20% ofthe adult population (1). The prevalence of reflux symptomsprobably underestimates the true prevalence of GERD, as itis based solely on the presence of heartburn and/or acidregurgitation. Recent data indicate that many patients withGERD present with symptoms such as acid reflux–relatedchest pain (noncardiac chest pain), asthma, cough, andhoarseness, and lack concomitant symptoms of heartburn oracid regurgitation (2). For instance, it has been demonstratedthat as many as 60–70% of adult asthmatics have GERD.Given the prevalence of asthma in the adult population in theUnited States as well as the millions of patients with non-cardiac chest pain, cough, and hoarseness, the true preva-lence of GERD is likely to be substantially greater than 20%.
Until recently our understanding of GERD was largelylimited to patients with erosive esophagitis. Investigatorsand clinicians were concerned with erosive esophagitis for anumber of reasons. Foremost among these was the need foran unequivocal criterion for the diagnosis of gastroesopha-geal reflux disease in clinical trials. This resulted in most ofthe literature on therapy being limited to patients with ero-sive esophagitis. The presence of erosive esophagitis alsoprovided an objective means of measuring efficacy, as heal-
ing could be clearly defined. These trials fostered the de-velopment of numerous scoring systems of esophagitis (3,4) furthering interest and limiting the focus of research inGERD to patients with erosive esophagitis. Compoundingthis research “bias” toward GERD patients with erosiveesophagitis was the erroneous belief that the adverse clinicalimpact of GERD was limited to those with erosive esoph-agitis. This belief ignored accumulating data that the great-est clinical impact of GERD was on quality of life (QOL)and that the impairment was similar in patients with andwithout erosive disease (5). The assumption that therapeuticneeds were not as great in patients with nonerosive refluxdisease (NERD) has also been challenged by recent studies.NERD therefore represents an enormously important clini-cal problem that requires a refocus of our attention and apriority for clinical research.
In this article, we review what is known about the patho-physiology, diagnosis, and treatment of NERD, as well as itscost to society and to health care systems. We also identifycritical areas where information is lacking, to shed furtherlight on this enormously important clinical issue.
DEFINITION
There is no generally agreed upon definition of NERD in theliterature. We define NERD as the presence of typical symp-toms of gastroesophageal reflux disease caused by intra-esophageal acid, in the absence of visible esophageal mu-cosal injury at endoscopy.
It is clear that NERD is not composed of a homogeneousgroup of patients. The functional esophageal disorders com-mittee that convened in Rome in 1990 suggested the use of24-h esophageal pH monitoring as a tool to distinguish asubset of NERD patients as those with “functional heart-burn” (6). Functional heartburn was defined as burningretrosternal discomfort for$3 months in the absence ofpathological gastroesophageal reflux by 24-h esophageal pHmonitoring and esophagitis by endoscopy. The committeesuggested that further distinction between subgroups offunctional heartburn patients could be achieved by correlat-ing physiological acid reflux events with symptoms of heart-
This work was presented in part at the annual meeting of the American Gastro-enterological Association, May 16–19, 1999, Orlando, FL.
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 96, No. 2, 2001© 2001 by Am. Coll. of Gastroenterology ISSN 0002-9270/01/$20.00Published by Elsevier Science Inc. PII S0002-9270(00)02304-2

burn (Fig. 1). As the pH test is not a gold standard for thediagnosis of GERD, it may not be reliable in categorizingthe NERD group (Figs. 2–4). False negative results are notuncommon and may occur even in patients with docu-mented erosive esophagitis (7, 8). Furthermore, it has beendemonstrated that 30–50% of NERD patients presentingwith heartburn will have no evidence of pathological acidreflux by currently available diagnostic modalities (6, 9, 10).
EPIDEMIOLOGY AND NATURAL HISTORY
Gastroesophageal reflux disease represents a spectrum ofsymptoms and tissue damage. Patients may present withtypical symptoms such as heartburn and acid regurgitationand/or atypical symptoms such as chest pain, hoarseness,and cough. In addition, patients may present with normalesophageal mucosa, mucosal inflammation, or complica-
tions such as stricture and Barrett’s esophagus. It has beendemonstrated that there is no correlation between the sever-ity of GERD symptoms and the presence or absence ofvisible esophageal inflammation (11).
Early studies that originated from tertiary referral centerssuggested that approximately half of the patients presentingwith reflux symptoms had erosive esophagitis at upper en-doscopy (11, 12). However, most patients with GERD eitherself-medicate and never seek medical attention, or they areseen and treated by community-based physicians (13). Re-cent studies that were carried out in community practicerevealed that up to 70% of the GERD patients have NERD(14, 15). Therefore, erosive esophagitis does not seem to beas common as previously suggested. In another community-based study of antacid users, Robinsonet al. found that 53%of GERD patients had NERD and two thirds of the remain-der had only mild erosive changes at endoscopy (16). Thisstudy highlights another important finding that in commu-nity-based patients with esophageal mucosal injury, milderosive esophagitis is the most prevalent form of mucosalinjury.
Only a few studies, mostly retrospective, have assessedthe natural history of NERD. In one study from Italy, 33NERD patients were followed for a period of 6 monthswhile on antacids and/or prokinetics (17). At the end of thefollow-up period, 58% remained symptomatic and 15% haddeveloped erosive esophagitis. A total of 42% becameasymptomatic and were able to discontinue all medicaltherapy. There was no difference in the pattern of GERDbetween the symptomatic patients and those that becameasymptomatic. However, this retrospective review offersonly a short-term follow-up. In another study from Scotland,NERD patients with either excess or normal esophageal acidexposure but a positive symptom index were followed for amedian period of 6.5 and 4.4 yr, respectively (18). In all,87% of those with normal acid exposure and 79% of thosewith excess acid reflux remained symptomatic; 53% and47%, respectively, recorded their symptoms as the same orworse than at the original presentation, despite regular useof medications in 60% of patients in each group. Thesestudies and others suggest that most NERD patients willdemonstrate a chronic pattern of symptoms with periods ofexacerbation and remission. Further delineation of the clin-
Figure 1. Subcategorization of the nonerosive reflux disease(NERD) group by using 24-h esophageal pH monitoring and“symptom index,” as suggested by the functional esophageal dis-orders committee in Rome in 1990 (6).
Figure 2. A 24-h esophageal pH recording in a patient with nonerosive reflux disease (NERD). During the test the patient experienced threeepisodes of acid regurgitation (R) and one episode of heartburn (H). All symptoms correlate with acid reflux events, suggesting a 100%symptom index. (E5 meal; S5 supine position.)
304 Fass et al. AJG – Vol. 96, No. 2, 2001
ical characteristics of NERD patients over a longer period isneeded.
MECHANISMS OF HEARTBURN
Heartburn is the classic symptom of GERD that is perceivedby patients with and without mucosal injury. In patients witherosive esophagitis, stimulation of sensory afferent path-ways by acid refluxate or inflammatory mediators is con-sidered to be the mechanism underlying symptom genera-tion. The precise relationship between symptoms ofheartburn and acid reflux events in patients with normalendoscopy remains to be established.
There is evidence for the presence of nerve terminals ofboth vagal and spinal fibers within the mucosa and musclelayer of the esophagus (19–22). However, the precise lo-calization of specific intramural nerve structures that areresponsible for the transmission of painfully perceived, af-ferent information is not yet known. It seems that activationof peripheral terminals of spinal rather than vagal afferentsare a necessary condition (22). Polymodal vagal afferentswith receptive fields in the esophageal mucosa are importantin chemically or mechanically induced reflex regulation thatis not associated with conscious perception under normal
conditions (19). Vagal afferents seem to have no role invisceral pain transmission, except for a pain-modulatoryeffect for certain types of vagal afferents and a role inperception of esophageal distension (23, 24). In contrast,spinal afferents are thought to be important for the trans-mission of discomfort and pain (25). The receptive fields formechanosensitive spinal afferents are assumed to be locatedprimarily in the muscle and serosa, whereas the intraepithe-lial nerve endings of spinal afferents are likely to be in-volved in the mediation of acid-induced pain during topicalexposure to intraluminal acid (20).
The mechanisms that lead to symptoms of heartburn inpatients lacking esophageal mucosal injury remain an areaof intense research. In both animal models and humans,dilation of the intercellular spaces has been noted in acid-exposed tissues (26, 27). In humans, these findings weredetected by transmission electron photomicrographs in pa-tients with erosive and nonerosive reflux disease (27, 28).These findings may suggest that patients with reflux diseasehave an increase in paracellular permeability in the esoph-ageal epithelium (29). Because sensory neurons in theesophageal epithelium reside within the intercellular spaces,the increase in paracellular permeability may explain heart-burn symptoms during esophageal acid exposure in patients
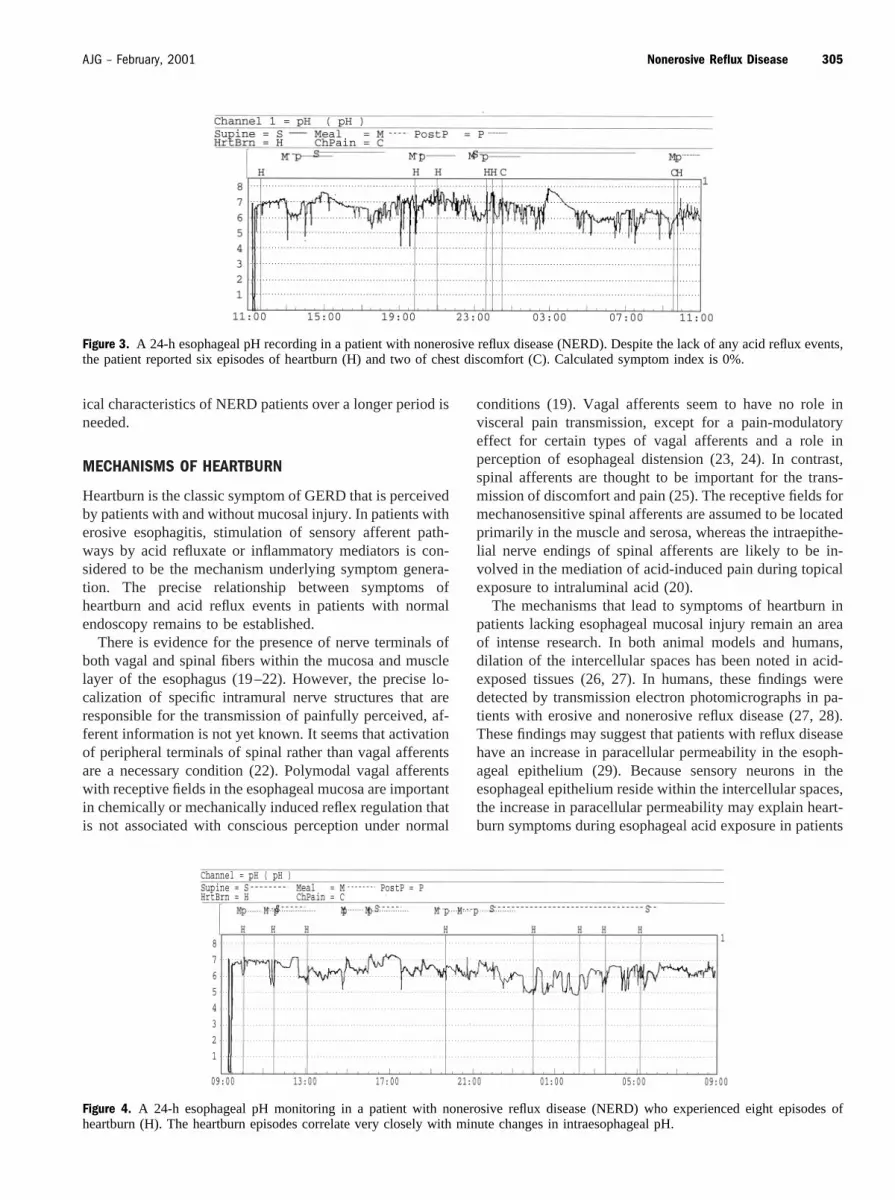
Figure 3. A 24-h esophageal pH recording in a patient with nonerosive reflux disease (NERD). Despite the lack of any acid reflux events,the patient reported six episodes of heartburn (H) and two of chest discomfort (C). Calculated symptom index is 0%.
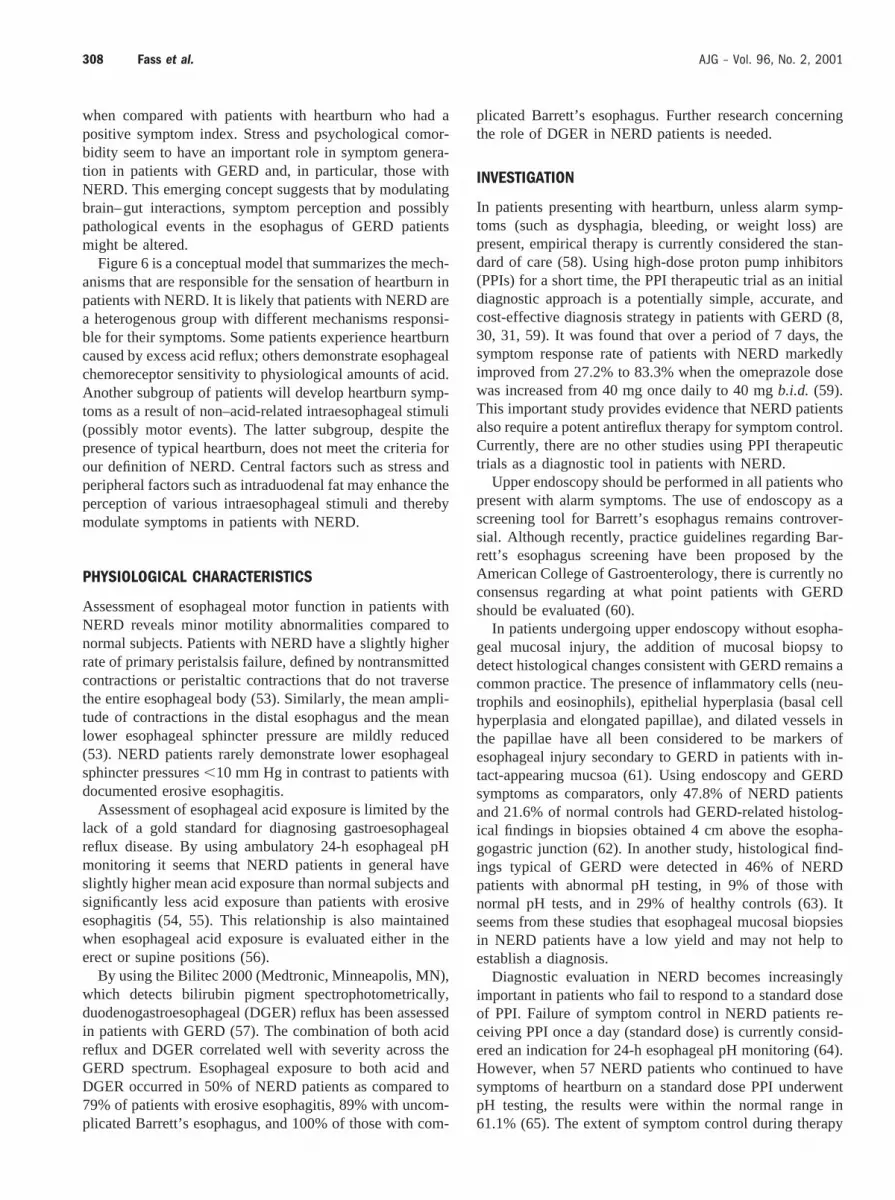
Figure 4. A 24-h esophageal pH monitoring in a patient with nonerosive reflux disease (NERD) who experienced eight episodes ofheartburn (H). The heartburn episodes correlate very closely with minute changes in intraesophageal pH.
305AJG – February, 2001 Nonerosive Reflux Disease

with NERD (29). However, this hypothesis provides only apartial explanation for the relationship between symptomgeneration and acid reflux events that has been observed inNERD patients.
It is currently accepted that an excess of intraesophagealacid and perhaps other components of duodenogastro-esophageal reflux are the primary causes for symptoms ofheartburn in NERD patients. However, between 33% to50% of the patients with NERD will have normal test resultswhen they undergo initial 24-h esophageal pH monitoring,and up to 25% will reverse diagnosis (positive to negativetest andvice versa) on subsequent pH testing (8, 14, 30–32).These data suggest that in a significant number of NERDpatients, physiological acid exposure may be sufficient tocause typical symptoms of heartburn.
The specific role of the symptom index, which determinesthe percentage of symptoms that correlates with acid refluxevents, remains to be elucidated in NERD (33). In addition,interpretation of a positive symptom index (.50%) in thesetting of a normal pH test remains an area of controversy.Although some have considered it indicative of GERD(false negative pH test by conventional criteria), others havesuggested that it might be indicative of a group of patientsthat is highly sensitive to physiological amounts of acidreflux (functional heartburn) (6, 9). Patients with abnormalupper endoscopy are more likely to experience heartburnsymptoms (65%) during pH testing than patients with nor-mal endoscopy and abnormal pH testing (32.5%) and thosewith both normal endoscopy and pH testing (21%) (34). Ingeneral, patients with erosive esophagitis are significantlymore likely to have a positive symptom index when com-pared with NERD patients (33). Furthermore, patients witha normal upper endoscopy and 24-h pH test have a signif-icantly lower calculated symptom index (26%6 10.7%)than those with abnormal upper endoscopy (85%6 4.6%)or normal endoscopy and abnormal pH testing (70%67.1%). These data suggest that patients with a normal en-doscopy and 24-h pH test are less likely to have an abnormalsymptom index (34, 35). The symptom index data maymean that a subset of NERD patients with physiological acidreflux may have hypersensitivity to acid. It is also possiblethat other non–acid-related intraesophageal stimuli can trig-ger heartburn. Animal models of afferent nerve sensitizationhave demonstrated that acid exposure can sensitize esoph-ageal nerve endings (chemoreceptors) directly or via inflam-matory mediators, resulting in lower pain thresholds (36).The sensitized esophageal chemoreceptors are part of thespinal afferents, which mediate esophageal sensation. Al-tered pain perception demonstrated by increased chemore-ceptor sensitivity to acid has been shown in NERD patients(37, 38). This hypersensitivity to acid can be demonstratedin both the proximal and distal esophagus (39). However,NERD patients seem to be less sensitive to acid whencompared to patients with documented erosive esophagitis,regardless of their endoscopic grading (37, 40).
Assessment of mechanoreceptor sensitivity using intra-
esophageal balloon distension has yielded contradictory re-sults. Trimbleet al. evaluated patients with heartburn andexcess reflux defined by abnormal upper endoscopy and/or24-h esophageal pH monitoring and compared them to pa-tients with heartburn and a normal 24-h pH test; the resultsdemonstrated that the latter group had lower volume thresh-olds for perception of esophageal balloon distension anddiscomfort (41). This study suggests that patients with typ-ical heartburn who lack any evidence of excess acid arehighly sensitive to mechanical stimuli. In another studyusing esophageal balloon distension delivered by an elec-tronic barostat, patients with NERD and erosive esophagitisdid not demonstrate an increase in mechanosensitivity,when compared to normal controls (37).
The current literature suggests that there is a differentialeffect of long-term esophageal acid exposure on chemosen-sitivity and mechnosensitivity in humans. Chronic esopha-geal exposure to excess acid affects chemosensitive but notmechanosensitive afferent pathways. Only patients withtypical GERD symptoms and no evidence of excess aciddemonstrate an increase in mechanosensitivity. Some ex-perts hypothesize that the latter group might be sensitive tominute changes in pH that do not reach our current criterionfor acid reflux event (pH, 4) (Fig. 4). Data to support thisintriguing hypothesis are still lacking. Thus far, the axiomhas been that pathological amount of acid is the only vis-ceral stimulus that can result in heartburn (“no acid, noheartburn”). However, as has been mentioned, heartburnmay be reported when the extent of esophageal acid expo-sure is within the physiological range in patients with eithera negative symptom index or a complete absence of anydocumented acid reflux events (38). These data suggest thatnon–acid-related stimuli may produce heartburn as well in asubset of patients with NERD.
In a recent study it has been demonstrated that chest painand heartburn may be provoked in normal subjects duringesophageal balloon distension either in the proximal ordistal portion of the esophagus (37). Interestingly, volumethresholds for heartburn and chest pain in both esophageallocations were similar, suggesting that for a specific volumesome patients will develop chest pain and others heartburn.Furthermore, volume thresholds for both chest pain andheartburn did not differ significantly at each esophageallocation and between locations. In this study, esophagealballoon distension also reproduced typical heartburn symp-toms in patients with documented GERD who were beingtreated with high-dose proton pump inhibitors. This studyclearly demonstrates that acid is not the only visceral stim-ulus that may lead to heartburn. Pehlivanovet al.suggestedthat longitudinal muscle contractions of the esophagus, de-tected only by high frequency intraluminal ultrasound andnot by traditional esophageal manometry, are the motorequivalent of heartburn sensation (42). These contractionsmay occur in the presence or absence of acid reflux. Thisintriguing observation requires further confirmation.
The data discussed so far suggest that NERD patients
306 Fass et al. AJG – Vol. 96, No. 2, 2001

might have either excessive or physiological acid exposureor even non–acid-related intraesophageal stimuli that resultin the sensation of heartburn. However, it is well known thatonly the minority of acid reflux events (,20%) are associ-ated with symptoms of heartburn (Fig. 5) (43). It is stillunclear what factors determine whether an acid reflux eventwill reach a conscious level. It seems that most acid refluxevents that are perceived occur postprandially (Fig. 5). Re-cently it has been demonstrated that intraduodenal fat infu-sion enhances perception of intraesophageal acid and maybe a major modulator of postprandial GERD symptoms(44). Stress and psychological comorbidity seem also to beimportant factors in the generation of symptoms in patientswith GERD. In a Gallup poll, 64% of individuals withheartburn reported that stress increased their symptoms (45).Through brain–gut interaction, stress may induce alterationsin GI secretory and motor responses, however, it remains tobe demonstrated how stress exacerbates GERD symptomsand whether it has a specific role in NERD patients.
Intraesophageal pH measurements in both normal sub-jects and GERD patients fail to demonstrate an increase inacid reflux events during psychologically induced stress(46–48). Furthermore, acute stress does not induce signif-icant changes in esophageal motility in patients with NERD(49). However, interventions aimed at reducing stress inpatients with GERD (hypnosis and progressive muscle re-laxation technique) have resulted in subjective improvementin reflux symptom ratings (48, 50). Bradleyet al.suggestedthat chronically anxious patients when exposed to prolongedstress might perceive low intensity esophageal stimuli as apainful reflux symptom (41). They and others have postu-lated that anxious patients may devote an excessive amountof attention to a wide variety of esophageal events (i.e., theyare hypervigilant) and thus may perceive such events aspainful (47, 49).
Bakeret al. (51) performed psychological assessment inpatients with documented GERD and controls. Patients withreflux differed from controls on scales of depression, som-atization, anxiety, and intensity of reporting symptom dis-
tress. In a secondary analysis it was shown that only 30% ofthe GERD patients accounted for the differences betweenthe groups, suggesting that although most patients withGERD are psychologically similar to patients withoutGERD, a subset of psychologically distressed patients aremore likely to be found among patients with GERD.Johnstonet al. (52) studied patients with episodes of heart-burn that did not correlate with acid reflux events (i.e.,patients with a negative symptom index). These patientswere found to have significantly higher levels of trait anx-iety and significantly less adequate social support structures
Figure 5. A 24-h esophageal pH recording in a patient with nonerosive reflux disease (NERD). The patient experienced multiple acid refluxevents but perceived and developed heartburn during only two of them. This pH recording clearly demonstrated that most acid reflux eventsare not sensed.
Figure 6. A proposed mechanistic model for heartburn sensation inpatients with nonerosive reflux disease (NERD). Central and pe-ripheral factors may enhance the perception of intraesophagealstimuli and are probably major modulators of symptoms in NERDpatients.
307AJG – February, 2001 Nonerosive Reflux Disease
when compared with patients with heartburn who had apositive symptom index. Stress and psychological comor-bidity seem to have an important role in symptom genera-tion in patients with GERD and, in particular, those withNERD. This emerging concept suggests that by modulatingbrain–gut interactions, symptom perception and possiblypathological events in the esophagus of GERD patientsmight be altered.
Figure 6 is a conceptual model that summarizes the mech-anisms that are responsible for the sensation of heartburn inpatients with NERD. It is likely that patients with NERD area heterogenous group with different mechanisms responsi-ble for their symptoms. Some patients experience heartburncaused by excess acid reflux; others demonstrate esophagealchemoreceptor sensitivity to physiological amounts of acid.Another subgroup of patients will develop heartburn symp-toms as a result of non–acid-related intraesophageal stimuli(possibly motor events). The latter subgroup, despite thepresence of typical heartburn, does not meet the criteria forour definition of NERD. Central factors such as stress andperipheral factors such as intraduodenal fat may enhance theperception of various intraesophageal stimuli and therebymodulate symptoms in patients with NERD.
PHYSIOLOGICAL CHARACTERISTICS
Assessment of esophageal motor function in patients withNERD reveals minor motility abnormalities compared tonormal subjects. Patients with NERD have a slightly higherrate of primary peristalsis failure, defined by nontransmittedcontractions or peristaltic contractions that do not traversethe entire esophageal body (53). Similarly, the mean ampli-tude of contractions in the distal esophagus and the meanlower esophageal sphincter pressure are mildly reduced(53). NERD patients rarely demonstrate lower esophagealsphincter pressures,10 mm Hg in contrast to patients withdocumented erosive esophagitis.
Assessment of esophageal acid exposure is limited by thelack of a gold standard for diagnosing gastroesophagealreflux disease. By using ambulatory 24-h esophageal pHmonitoring it seems that NERD patients in general haveslightly higher mean acid exposure than normal subjects andsignificantly less acid exposure than patients with erosiveesophagitis (54, 55). This relationship is also maintainedwhen esophageal acid exposure is evaluated either in theerect or supine positions (56).
By using the Bilitec 2000 (Medtronic, Minneapolis, MN),which detects bilirubin pigment spectrophotometrically,duodenogastroesophageal (DGER) reflux has been assessedin patients with GERD (57). The combination of both acidreflux and DGER correlated well with severity across theGERD spectrum. Esophageal exposure to both acid andDGER occurred in 50% of NERD patients as compared to79% of patients with erosive esophagitis, 89% with uncom-plicated Barrett’s esophagus, and 100% of those with com-
plicated Barrett’s esophagus. Further research concerningthe role of DGER in NERD patients is needed.
INVESTIGATION
In patients presenting with heartburn, unless alarm symp-toms (such as dysphagia, bleeding, or weight loss) arepresent, empirical therapy is currently considered the stan-dard of care (58). Using high-dose proton pump inhibitors(PPIs) for a short time, the PPI therapeutic trial as an initialdiagnostic approach is a potentially simple, accurate, andcost-effective diagnosis strategy in patients with GERD (8,30, 31, 59). It was found that over a period of 7 days, thesymptom response rate of patients with NERD markedlyimproved from 27.2% to 83.3% when the omeprazole dosewas increased from 40 mg once daily to 40 mgb.i.d. (59).This important study provides evidence that NERD patientsalso require a potent antireflux therapy for symptom control.Currently, there are no other studies using PPI therapeutictrials as a diagnostic tool in patients with NERD.
Upper endoscopy should be performed in all patients whopresent with alarm symptoms. The use of endoscopy as ascreening tool for Barrett’s esophagus remains controver-sial. Although recently, practice guidelines regarding Bar-rett’s esophagus screening have been proposed by theAmerican College of Gastroenterology, there is currently noconsensus regarding at what point patients with GERDshould be evaluated (60).
In patients undergoing upper endoscopy without esopha-geal mucosal injury, the addition of mucosal biopsy todetect histological changes consistent with GERD remains acommon practice. The presence of inflammatory cells (neu-trophils and eosinophils), epithelial hyperplasia (basal cellhyperplasia and elongated papillae), and dilated vessels inthe papillae have all been considered to be markers ofesophageal injury secondary to GERD in patients with in-tact-appearing mucsoa (61). Using endoscopy and GERDsymptoms as comparators, only 47.8% of NERD patientsand 21.6% of normal controls had GERD-related histolog-ical findings in biopsies obtained 4 cm above the esopha-gogastric junction (62). In another study, histological find-ings typical of GERD were detected in 46% of NERDpatients with abnormal pH testing, in 9% of those withnormal pH tests, and in 29% of healthy controls (63). Itseems from these studies that esophageal mucosal biopsiesin NERD patients have a low yield and may not help toestablish a diagnosis.
Diagnostic evaluation in NERD becomes increasinglyimportant in patients who fail to respond to a standard doseof PPI. Failure of symptom control in NERD patients re-ceiving PPI once a day (standard dose) is currently consid-ered an indication for 24-h esophageal pH monitoring (64).However, when 57 NERD patients who continued to havesymptoms of heartburn on a standard dose PPI underwentpH testing, the results were within the normal range in61.1% (65). The extent of symptom control during therapy
308 Fass et al. AJG – Vol. 96, No. 2, 2001

with standard dose PPI seems to be related to the extent ofintraesophageal acid exposure in the distal esophagus (51).The greater the total time that pH is initially,4, the betterthe symptom control. Thus, NERD patients with a mildlyabnormal or normal pH test will often fail standard dose PPItreatment. This may be explained by either hypersensitivityto acid reflux in the physiological range, which may suggestthe need for high dose PPI for complete acid elimination andconsequent symptom control or by nonacid intraesophagealstimuli. A recent study demonstrated no increase in esoph-ageal chemosensitivity to acid in NERD patients who failedstandard dose PPI (31).
QUALITY OF LIFE
A number of studies have demonstrated an impairment ofquality of life in chronic erosive esophagitis. Tewet al. (66)studied the illness behavior of patients with NERD andfound that these patients were similar to those with erosiveesophagitis. Treatment improved both groups equally. Ingeneral, patients with GERD experience more pain andgreater impairment in social functioning and emotionalwell-being than patients with other chronic diseases such asdiabetes and hypertension. For example, Chalet al. foundimpairments in comfort (vspain), vitality, and mental healthin GERD (67). Dimenas reported impaired psychologicalwell-being scores in patients with GERD (5). A small num-ber of studies have evaluated patients with uninvestigatedheartburn in primary care (68). Rustet al.demonstrated thatimpairment in quality of life was related to GERD symp-toms and improved with therapy (ranitidine 150 mgb.i.d.)(69). Revickiet al. (70) studied 533 patients with a historyof heartburn for 6 months before and after therapy withranitidine, 150 mgb.i.d. Patients reported significantlyworse scores on all eight scales of the SF-36 (physicalfunction and well-being, emotional well-being) compared tothe general population. Successful treatment led to markedimprovement in the quality of life (70). Carlssonet al. (71)studied patients with endoscopy-negative reflux disease.The Psychological General Well-Being index (PGWB in-dex) was used as a subjective measure of quality of life.Quality of life was impaired in patients with endoscopynegative disease and patients with erosive esophagitis andthere were no significant differences between the groups.Omeprazole therapy improved the quality of life in bothgroups of patients (71). A recent study showed substantialimprovement in quality of life with adequate therapy. Have-lund et al. (72) studied quality of life using well validatedscales in 163 patients with NERD. Quality of life wasrestored with omeprazole 10 mg or 20 mg and was compa-rable to that in the general population. Impairment of qualityof life appears to be similar in patients with NERD andpatients with erosive esophagitis. There is a strong associ-ation between symptoms and impairment of quality of life.Adequate treatment of symptoms therefore improves qualityof life in patients with NERD.
TREATMENT OF NERD
There are numerous therapeutic options available for treat-ing patients presenting with symptoms of GERD or other-wise suspected as having this disease. Generally these ther-apeutic options have been viewed in a hierarchy oftherapeutic efficacy, ranging from lifestyle modifications/antacids to histamine-2 receptor antagonists (H2RAs)/pro-kinetics to proton pump inhibitors (PPIs), with surgeryreserved for those with continued symptoms or complica-tions of GERD (73). It has been generally assumed byclinicians that patients with NERD would rarely demon-strate an incomplete response to either lifestyle modifica-tions or therapy with H2Ras/prokinetics; thus, potent anti-secretory therapy with PPIs or surgery should rarely benecessary in this patient population. However, there is nowample evidence that this assumption is incorrect, and thatthe therapeutic requirements of patients with NERD aresimilar to those with erosive esophagitis.
Some of the first evidence that H2RAs may be less thanoptimal as therapy for NERD came from a large US studyof patients with heartburn treated with famotidine (74). Inthis trial, ,30% of patients treated with H2RA twice dailyhad complete elimination of heartburn at 30 days, and littlemore than 50% of patients had relief at the end of 3 months.A sizable number of patients in this trial had NERD orminimal grades of esophagitis. Thus, indirectly, evidencebegan to suggest that patients with NERD might not be aseasily treated as previously assumed. This should not havebeen surprising, given the pharmacology of H2RAs. Theseagents have been known to be ineffective in inhibitingmeal-stimulated acid secretion and are associated with therapid development of pharmacological tolerance (73). Thesepharmacological properties affect all patients with GERD,regardless of the presence of erosive esophagitis. Furthersupport for the inadequacy of these agents in many patientswith NERD is derived from a recent trial in which symp-tomatic GERD patients with an incomplete response totherapy with 3 months of a twice daily dose of an H2RA,were randomized to a further 2 months of continued therapyat this dose or to 2 months of a double dose of the H2RA(75). Further therapeutic response to continued use of anH2RA, even at high doses, was very modest in this trial.
Given the pharmacological deficiencies of H2RAs in con-trolling acid secretion it was felt that perhaps patients withNERD could be better served by using a prokinetic agent.Prokinetics had shown some efficacy in patients with ero-sive esophagitis, and it was hoped even greater efficacycould be demonstrated in patients with NERD. However, ina large European study, remission of symptoms could bemaintained in fewer than half of those patients with NERDwho were receiving cisapride (76). Thus, like what had beenobserved for H2RAs, the therapeutic efficacy of prokineticsin patients with NERD is limited. Concerns about the safetyof cisapride also limit its utility in this setting.
There are data that indicate overwhelmingly that, in pa-
309AJG – February, 2001 Nonerosive Reflux Disease

tients with erosive esophagitis, PPIs provide superior heal-ing and symptom relief compared to H2RAs or prokinetics(77). Similar data are emerging regarding the use of PPIs inpatients with NERD. In a 4-wk study of patients withheartburn and normal endoscopy, omeprazole resulted incomplete symptom relief in nearly 60% of patientsversusapproximately 20% of those receiving placebo (78). In asimilar placebo-controlled trial, symptom relief at 4 wk wasalso approximately 60% in those receiving omeprazolever-sus24% of those in the placebo arm (51). There were furtherinteresting observations made in this study. The therapeuticresponse was correlated with intraesophageal acid exposure:those patients with the greatest intraesophageal acid expo-sure had the greatest response (response rate,.85% inpatients with an esophageal pH of,4 more than 10% of thetime,vs54% in patients with a pH of,4 less than 4% of thetime). Thus, in NERD patients with an abnormal pH study,the therapeutic response was nearly identical to that seen inpatients with erosive esophagitis. The study also indicatedthat in those patients with functional heartburn, a therapeuticresponse would be much less likely.
There are now trials comparing the therapeutic efficacy ofPPIsversusH2RAs and cisapride in patients with NERD. Inone study, 60% of patients treated with omeprazole hadrelief of heartburn,versus40% of those receiving H2RAs(79). In that study,.50% of patients were maintained inremission with omeprazole,versus,30% of those patientsreceiving ranitidine. Similarly, in a study in the US, lanso-prazole has also been shown to be more effective thanranitidine in relieving symptoms of reflux in patients with-out esophagitis (80). Similar therapeutic superiority for PPIshas been shown in another trial comparing omeprazole tocisapride (81). In that study, 63% of omeprazole patientswere free of heartburn at 4 wk,versus46% of those receiv-ing cisapride. These results that demonstrate superiority ofomeprazole over placebo in patients with NERD have alsobeen confirmed in recent US studies (82).
Although further studies are needed to clarify the efficacyof agents in NERD, certain conclusions can be made basedon the evidence available in the literature. First, the thera-peutic efficacy of antisecretory agents seems overall to belower in patients with NERD compared to those with ero-sive esophagitis. Whether this is related to the inclusion ofpatients without GERD in these studies (thus diluting atreatment effect) or whether it is attributable to some otherfactor is unclear. Second, the hierarchy of efficacy of ther-apy (PPI efficacy is greater than that of H2RA/prokinetics,which is greater than lifestyle modifications alone) that isseen in patients with erosive esophagitis is comparable forpatients with NERD. Third, patients with NERD demon-strate a similar lack of efficacy to H2RAs, as do those witherosive esophagitis. The results of surgery in patents withNERD have been thought by many clinicians to be poorerthan the results obtained in patients with esophagitis. How-ever there are few data to support this clinical impression. Itis likely that patients selected for surgery based on complete
symptom response to antisecretory therapy will have symp-tom outcomes similar to those seen with esophagitis. NERDpatients who do not respond to antisecretory therapy areunlikely to have an optimal response to antireflux surgery.Controlled trials of antireflux surgery are needed to deter-mine the role of this therapy in patients with NERD.
ECONOMICS OF ENDOSCOPY NEGATIVE REFLUX DISEASE
The costs of managing chronic disease are of increasingimportance in an era of constrained resources. Determiningthe optimal therapy for patients with NERD is a growingarea of interest and research.
Costs of Reflux Disease in the United StatesAcid-related disorders are common problems in the US, andGERD is the most prevalent of these disorders. Given thefrequency of the condition, there are surprisingly few dataon the total cost of managing reflux disease. In large mea-sure, this is because information systems used in mostinstitutions are not able to capture disease-specific coststhroughout the entire episode of care. Levinet al. (83)reported the cost of managing reflux disease in a managedcare organization in California (Kaiser Permanente ofNorthern California) and calculated the GERD-related costsin a cohort of 1500 patients with acid-related disorders. Thetotal annual HMO expenditures for acid-related disorderswas $59 million for a membership of 2.4 million members.The total annual direct cost of managing a GERD patientwas $4574 with a total pharmacy cost of $491, outpatientcosts or $2403 (pharmacy, outpatient visits, etc.), and inpa-tient costs of $1680. With adjustment of the data to deter-mine the costs attributible to GERD separately, the total costof managing GERD was $471 per person, with pharmacycosts accounting for $156 of this amount and outpatientcosts accounting for $279; in comparison, inpatient costswere small at $35/per person. In the first 6 months after thediagnosis, outpatient costs remain the highest componentcost of GERD management, accounting for a large propor-tion of the adjusted costs ($246 out of a total of $289).
Outpatient CostsOutpatient costs of managing GERD are related to officevisits and endoscopic or radiological procedures. GERD isone of the most frequent indications for upper endoscopy inthe United States. In a large database of.17,000 endo-scopic procedures, GERD was the third leading indicationfor endoscopy (84). With the understanding of the frequencyof endoscopy-negative reflux disease, it has become appre-ciated that endoscopy may fail to establish a diagnosis ofreflux disease, and alternative strategies have been pro-posed. Chief among these is a trial of therapy in primarycare settings. Several studies have compared a short trial ofacid inhibitory therapy as a diagnostic test for reflux diseaseto investigations such as a 24-h esophageal pH monitoringor endoscopy. They found that a trial of therapy may be an
310 Fass et al. AJG – Vol. 96, No. 2, 2001

effective method to diagnose patients with suspected refluxdisease who present with symptoms of heartburn or chestpain. Ofmanet al. reported the cost-effectiveness of theomeprazole test in patients with noncardiac chest pain (85).In patients with a cardiac cause excluded by comprehensivecardiac evaluation, the omeprazole test with no subsequentinvestigations for patients who respond, and with sequentialtesting with ambulatory 24-h esophageal pH monitoring,esophageal manometry, and endoscopy reserved for patientswho do not respond, was the most effective and least ex-pensive strategy. Using a selective strategy of investigationin nonresponders to a trial of a proton pump inhibitor, theauthors calculated that a 43% reduction in procedures wouldresult and that the cost-savings would be $454 per patientcompared with a strategy of beginning with endoscopyfollowed by pH testing and esophageal manometry. Simi-larly, in patients with suspected reflux disease, the omepra-zole test was estimated to reduce the number of endoscopiesperformed by 64% and the number of pH studies by 53%,with $348 saved per patient evaluated (86). Similarly inasthmatic patients, cost-effectiveness analysis suggests thata trial of therapy with omeprazole 20 mg/day for 3 months,with 24-h esophageal pH monitoring reserved for nonre-sponders, was cost-effective (87).
Sonnenberget al. performed a decision analysis compar-ing empirical therapyversusdiagnostic testing in GERD(88). Empirical therapy was cost saving, with investigationreserved for nonresponders, despite the cost associated withan occasional incorrect diagnosis. However, as the durationof therapy becomes longer (.10 yr in this particular model),investigation becomes more meaningful because mainte-nance therapy in patients who do not need therapy increasescosts. Again, because of the relatively high cost of surgery,a specific diagnosis is favored in this subgroup of patients.
Is Endoscopy Useful in Managing Therapy?Recent studies have examined the role of endoscopy in themanagement of patients with GERD. In a prospective studyof 664 patients with symptoms of GERD who were under-going upper endoscopy in clinical practice, 74% of patientswho had Barrett’s esophagus or erythema, erosions or ul-ceration at endoscopy had an increase in therapy after en-doscopy (89). In contrast, 35% of patients who had a normalendoscopy had an increase in therapy. These data suggestthat endoscopy may influence the treatment prescribed byphysicians. However the increase in treatment in most caseswas based on persistent symptoms or on findings in thestomach or duodenum. Blusteinet al.evaluated the utility ofendoscopy in a large group of 742 patients. In all, 68% ofpatients who were still symptomatic on H2Ras wereswitched to omeprazole regardless of the findings at endos-copy, whereas 47% of patients taking omeprazole weremaintained on the same therapy regardless of the findings atendoscopy (90). Endoscopy therefore had a limited role indetermining therapy.
Relief of Anxiety With EndoscopyIn dyspepsia, it has been suggested that endoscopy mayrelieve anxiety and reduce subsequent health care use (91).These data are based on uncontrolled studies of small groupsof patients. Other studies have shown a short-term improve-ment in quality of life after endoscopy in dyspeptic patients(92). A recent study in a large cohort of patients suggestedthat patients with a high degree of anxiety before endoscopycontinued to have high degrees of anxiety after a normalendoscopy and reassurance from the endoscopists. Patientswith low levels of anxiety did not obtain significant benefit(93). A subgroup of patients with moderate anxiety diddemonstrate lasting improvement of anxiety after a normalendoscopy. Endoscopy may therefore be useful in veryselected patients for the relief of anxiety, and may be helpfulin anxious patients with atypical symptoms of GERD,e.g.,chest pain.
Pharmacy CostsA number of economic models have examined the cost-effectiveness of treatment strategies for the management oferosive esophagitis, but there are few economic analyses onmanagement strategies in endoscopy-negative reflux dis-ease. Economic models that are directed at erosive esoph-agitis have limited applicability to unselected patients inprimary care. Sonnenberget al. examined a stepwise ap-proach to the management of GERD in the VA system.They evaluated a stepwise strategy beginning with a genericH2RA; patients who failed to respond were treated with ahigher dose of H2RA therapy, and those who still failed torespond were treated with proton pump inhibitors (step-uptherapy) (94). This economic model suggested that an av-erage of $916 per patient could be saved every 5 yr by usinga step-up strategy. In contrast, preliminary data from aclinical trial in primary care suggest that neither step-up orstep-down therapy provided optimal control of heartburnover a 20-wk period (95). Recently a multicenter, random-ized, open-label trial was performed in patients with symp-toms of GERD in primary care practices in West Virginia.A total of 268 patients were randomized to received ome-prazole 20 mg once a day or ranitidine (brand-name) 150 mgb.i.d. for up to 6 months. At 6 months, there was no signif-icant difference in total costs between the groups, but symp-toms were better controlled in the omeprazole group (96).These data suggest that effective therapies, which are moreexpensive to acquire, may still be cost-effective over rela-tively short periods of time because their higher efficacydecreases outpatient costs related to treatment failure.
As the natural history of endoscopy negative reflux dis-ease is benign, control of symptoms is the principal deter-minant of the success of therapy. To reduce the cost ofchronic maintenance therapy, alternate forms of mainte-nance therapy are being attempted in nonerosive refluxdisease. New techniques of maintenance therapy offer sig-nificant advantages. These techniques consist of dose reduc-tion or intermittent use of medication to reduce costs while
311AJG – February, 2001 Nonerosive Reflux Disease

still achieving the goal of symptom relief. In a recent study,677 patients with endoscopy-negative or mild-to-moderateerosive GERD in primary care were randomized to raniti-dine 150 mgb.i.d., low-dose omeprazole (10 mg/day), orstandard dose omeprazole (20 mg/day) for 2 wk (97). If theyhad symptom relief they continued with the maintenancephase of the study, in which they received 2-wk courses ofintermittent therapy with the regimen that had worked in thefirst instance. At the end of 1 yr of maintenance therapy, halfof the patients did not require treatment for at least 6 monthsof the study period and had good control of symptoms, thussubstantially reducing the cost of maintenance therapy. Acost analysis based on this study found no difference be-tween the cost of the omeprazole and ranitidine arms, usingcost assumptions from a number of European countries thatwere part of the trial. These data suggest that on a cost basis,there is little to be gained from a step-up approach totreating NERD (98).
Another alternative is to give on-demand therapy, therebyreducing the amount of medication being used. In one study,424 patients with endoscopy negative reflux disease wererandomized to placebo or PPI (omeprazole 20 mg or ome-prazole 10 mg) on demand (99). At 6 months follow-up,29% of patients had failed to respond to on-demand therapyand needed daily maintenance therapy. However 83% ofpatients randomized to on-demand therapy with omeprazole20 mg a day were satisfactorily maintained over the 6-monthtime frame. The mean number of omeprazole capsules usedper day was 0.43, suggesting that the total medication usewas reduced by approximately 50%. In the future, patientswith NERD will increasingly be managed with alternativeforms of maintenance therapy. Some conclusions regardingthe economics of NERD can be made from the availabledata. First, the cost of managing all forms of reflux diseaseis high. Second, outpatient costs are the major component ofthe management costs of NERD. Third, endoscopy—al-though useful for diagnosis—has little role in management,which is driven by symptoms. Fourth, new methods of PPIadministration may be an interesting new option in themanagement of NERD, combining highly effective therapywith less frequent administration, thereby reducing cost.
In conclusion, NERD is a common condition in primarycare. Many patients with NERD have moderate-to-severesymptoms and significant impairment in the quality of life.Therapy with acid-suppressive agents results in completeresolution of symptoms in the majority of patients andrestores quality of life. Current data from surgical studiesare inadequate to determine whether surgical therapy resultsin better or worse outcomes than medical therapy. Alterna-tive methods of treatment including on-demand therapy andintermittent therapy deserve further study and may help toreduce the costs of maintenance therapy.
Reprint requests and correspondence:Nimish Vakil, M.D., Uni-versity of Wisconsin Medical School, Sinai Samaritan Medical
Center, 945 North 12th Street, Room 4040, Milwaukee, WI 53233-1305.
Received June 14, 2000; accepted Oct. 6, 2000.
REFERENCES
1. Locke GR, Talley NJ, Fett SL, et al. Prevalence and clinicalspectrum of gastroesophageal reflux: A population based studyin Olmstead County, Minnesota. Gastroenterology 1997;112:1448–56.
2. Fennerty MB. Extraesophageal gastroesophageal reflux dis-ease. Presentations and approach to treatment. GastroenterolClin North Am 1999;28:861–73.
3. Lundell LR, Dent J, Bennett JR, et al. Endoscopic assessment ofoesophagitis: Clinical and functional correlates and further vali-dation of the Los Angeles classification. Gut 1999;45:172–80.
4. Hetzel DJ, Dent J, Reed W, et al. Healing and relapse of severepeptic esohagitis after treatment with omeprazole. Gastroen-terology 1988;95:903–12.
5. Dimenas E. Methodologic aspects of evaluation of quality oflife in upper gastrointestinal disease. Scand J Gastroenterol1993;28:18–21.
6. Richter JE, Baldi F, Clouse R, et al. Functional esophagealdisorders. In: Drossman DA. Functional gastrointestinal dis-orders. Boston: Little, Brown, 1994:25–70.
7. Fass R, Fennerty MB, Ofman JJ, et al. The clinical andeconomic value of a short course of omeprazole in patientswith non-cardiac chest pain. Gastroenterology 1998;115:42–9.
8. Schenk BE, Kuipers EJ, Klinkenberg-Knol EC, et al. Ome-prazole as a diagnostic tool in gastroesophageal reflux disease.Am J Gastroenterol 1997;92:1997–2000.
9. Watson RGP, Tham TCK, Johnston BT, et al. Double blindcross-over placebo controlled study of omeprazole in the treat-ment of patients with reflux symptoms and physiological levels ofacid reflux the “sensitive oesophagus.” Gut 1997;40:587–90.
10. Klauser AF, Schindlbeck NE, Muller-Lissner SA. Symptomsin gastro-oesophageal reflux disease. Lancet 1990;335:205–8.
11. Johansson KE, Ask P, Boeryd B, et al. Oesophagitis, signs ofreflux, and gastric acid secretion in patients with symptoms ofgastro-oesophageal reflux disease. Scand J Gastroenterol1986;21:837–47.
12. Winters C, Spurling TJ, Chobanian SJ, et al. Barrett’s esoph-agus. A prevalent, occult complication of gastroesophagealreflux disease. Gastroenterology 1987;92:118–24.
13. Kitchin LI, Castell DO. Rationale and efficacy of conservativetherapy for gastroesophageal reflux disease. Arch Intern Med1991;151:448–54.
14. Lind T, Havelund T, Carlsson R, et al. Heartburn withoutoesophagitis: Efficacy of omeprazole therapy and featuresdetermining therapeutic response. Scand J Gastroenterol 1997;32:974–9.
15. Jones RH, Hungin ADS, Phillips J, et al. Gastroesophagealreflux disease in primary care in Europe: Clinical presentationand endoscopic findings. Eur J Gen Pract 1995;1:149–54.
16. Robinson M, Earnest D, Rodriguez-Stanley S, et al. Heartburnrequiring frequent antacid use may indicate significant illness.Arch Intern Med 1998;156:2373–6.
17. Pace F, Santalucia F, Bianchi Porro G. Natural history ofgastro-oesophageal reflux disease without oesophagitis. Gut1991;32:845–8.
18. Trimble KC, Douglas S, Pryde A, Heading RC. Clinical char-acteristics and natural history of symptomatic but not excessgastroesophageal reflux. Dig Dis Sci 1995;40:1098–1104.
19. Grundy D, Scratcherd T. Sensory afferents from gastrointes-tinal tract. In: Schultz SG, Wood JD, Rauner BB, eds. Hand-
312 Fass et al. AJG – Vol. 96, No. 2, 2001
book of physiology, volume 1. New York: Oxford University,1989:593–620.
20. Rodrigo J, Hernandez CJ, Vidal MA, et al. Vegetative inner-vation of the esophagus. III. Intraepithelial endings. Acta Anat1975;92:242–58.
21. Rodrigo J, Hernandez CJ, Vidal MA, et al. Vegetative inner-vation of the esophagus. II. Intraganglionic laminar endings.Acta Anat 1975;92:79–100.
22. Sengupta JN, Gebhart GF. Gastrointestinal afferent fibers andsensation. In: Johnson LR, ed. Physiology of the gastrointes-tinal tract, 3rd ed. New York: Raven, 1994:483–519.
23. Randich A. Visceral nerve stimulation and pain modulation.In: Mayer EA, Raybould HE, eds. Basic and clinical aspects ofchronic abdominal pain. Amsterdam: Elsevier, 1993:126–39.
24. Tougas G, Kamath MV, Garnett S, et al. Mapping of cerebralresponse to vagal and esophageal stimulation using positronemission tomography (PET) and topography EEG in humans.Gasteroenterolgy 1994;106:A486 (abstract).
25. Mayer EA, Gebhart GF. Basic and clinical aspects of visceralhyperalgesia. Gastroenterology 1994;107:271–93.
26. Ferreira KG, Hill BS. The effect of low external pH onproperties of the paracellular pathway and junctional structurein frog skin. J Physiol 1982;332:59.
27. Hopwood D, Milne G, Logan KR. Electron microscopicchanges in human oesophageal epithelium in oesophagitis.J Pathol 1979;129:161.
28. Tobey NA, Carson JL, Alkiek RA, et al. Dilated intercellularspaces: A morphological feature of acid reflux-damaged hu-man esophageal epithelium. Gastroenterology 1996;111:1200.
29. Orlando RC. Pathophysiology of gastroesophageal reflux dis-ease. In: Castell DO, Richter JE, eds. Esophagus, 3rd ed.Philadelphia: Lippincott Williams & Wilkins, 1999:409–19.
30. Johnsson F, Weywadt L, Solhaug J-H, et al. One-week ome-prazole treatment in the diagnosis of gastro-oesophageal refluxdisease. Scand J Gastroenterol 1998;33:15–20.
31. Fass R, Fennerty MB, Yalam JM, et al. Evaluation of theomeprazole test in patients with typical symptoms of gastro-esophageal reflux disease (GERD). 1997;112:A114.
32. Weiner GJ, Morgan TM, Copper JB, et al. Ambulatory 24-hour esophageal pH monitoring: Reproducibility and variabil-ity of pH parameters. Dig Dis Sci 1988;33:1127–33.
33. Weiner GJ, Richter JE, Copper JB, et al. The symptom index: Aclinically important parameter of ambulatory 24-hour esophagealpH monitoring. Am J Gastroenterol 1988;83:358–61.
34. Singh S, Richter JE, Bradley LA, et al. The symptom index:Differential usefulness in suspected acid-related complaints ofheartburn and chest pain. Dig Dis Sci 1993;38:1402–8.
35. Johnston BT, McFarland RJ, Collins JSA, et al. Symptomindex as a marker of gastro-oesophageal reflux disease. Br JSurg 1992;79:1054–5.
36. Smith JL, Opekun AR, Larkai E, et al. Sensitivity of theesophageal mucosa to pH in gastroesophageal reflux disease.Gastroenterology 1989;96:683–9.
37. Fass R, Naliboff B, Higa L, et al. Differential effect of long-termesophageal acid exposure on mechanosensitivity and chemosen-sitivity in humans. Gastroenterology 1998;115:1363–73.
38. Fass R, Pulliam G. Chemosensitivity to acid in patients withpersistent heartburn on standard doses of proton pump inhib-itor and normal 24-h esophageal pH monitoring. Gastroenter-ology 1999;116:A159 (abstract).
39. Niemantsverdriet EC, Timmer R, Breumelhof R, et al. Segmentalacid sensitivity of the esophagus in patients with endoscopy-negative GERD. Gastroenterology 1997;112:A237 (abstract).
40. Kaul B, Peterson H, Grette K, et al. The acid perfusion test ingastroesophageal reflux disease. Scand J Gastroenterol 1986;21:93–6.
41. Trimble KC, Pryde A, Heading RC. Lowered oesophageal
sensory thresholds in patients with symptomatic but not excessgastro-oesophageal reflux: Evidence for a spectrum of visceralsensitivity in GORD. Gut 1995;37:7–12.
42. Pehlivanov ND, Liu J, Mittal R. Sustained esophagealcontraction: A motor correlate of heartburn symptom. Gastro-enterology 1999;116:G4613 (abstract).
43. Baldi F, Ferrarini F, Longanesi A, et al. Acid gastroesophagealreflux and symptom occurrence: Analysis of some factorsinfluencing their association. Dig Dis Sci 1989;12:1890–3.
44. Lembo A, Naliboff B, Munakata J, et al. Intraduodenal fatalters perceptual and autonomic responses to acid perfusion ofthe esophagus in GERD patients. Gastroenterology 1998;114:G0819 (abstract).
45. A gallup survey on heartburn across America. Princeton, NJ:The Gallup Organization, 1988.
46. Cook IJ, Collins SM. Does acute emotional stress influencefrequency or duration of gastroesophageal reflux in humansubjects? Gastroenterology 1986;90:1380 (abstract).
47. Bradley LA, Richter JE, Pulliam TJ, et al. The relationshipbetween stress and symptoms of gastroesophageal reflux: Theinfluence of physiological factors. Am J Gastroenterol 1993;88:11–9.
48. McDonald-Haile J, Bradley LA, Bailey MA, et al. Relaxationtraining reduces symptom reports and acid exposure in pa-tients with gastroesophageal reflux disease. Gastroenterology1994;107:61–9.
49. Johnston BT, McFarland RJ, Collins JSA, et al. Effect of acutestress on oesophageal motility in patients with gastro-oesoph-ageal reflux disease. Gut 1996;38:492–7.
50. Richter JE, Bradley LC. Psychophysiological interactions inesophageal diseases. Semin Gastrointest Dis 1996;7:169–84.
51. Baker LH, Lieberman D, Oehlke M. Psychological distress inpatients with gastroesophageal reflux disease. Am J Gastro-enterol 1995;90:1797–1803.
52. Johnston BT, Lewis SA, Collins JSA, et al. Acid perception ingastro-oesophageal reflux disease is dependent on psycholog-ical factors. Scand J Gastroenterol 1995;30:1–5.
53. Kahrilas PJ, Dodds WJ, Hogan WJ, et al. Esophageal peristal-tic dysfunction in peptic esophagitis. Gastroenterology 1986;91:897–904.
54. Castell DO. pH monitoring versus other tests for gastroesoph-ageal reflux disease: Is this the gold standard? In: Richter JE.Ambulatory esophageal pH monitoring: Practical approachand clinical observations, 2nd ed. Baltimore: Williams &Wilkins, 1997:107–118.
55. Demeester TR, Wang CI, Wernly JA, et al. Technique, indi-cations, and clinical use of 24 hour esophageal pH monitoring.J Thorac Cardiovasc Surg 1980;79:656–70.
56. Klauser AG, Heinrich C, Schindlbeck NE, et al. Is long-termesophageal pH monitoring of clinical value? Am J Gastroen-terol 1989;84:362–6.
57. Vaezi MF, Richter JE. Role of acid and duodenogastroesopha-geal reflux in gastroesophageal reflux disease. Gastroenterol-ogy 1996;111:1192–9.
58. DeVault KR, Castell DO, and the Practice Parameters Com-mittee of the American College of Gastroenterology. Updatedguidelines for the diagnosis and treatment of gastroesophagealreflux disease. Am J Gastroenterol 1999;94:1434–42.
59. Schindlbeck NE, Klauser AG, Voderholzer WA, et al. Empirictherapy for gastroesophageal reflux disease. Arch Intern Med1995;155:1808–12.
60. Sampliner RE, and the Practice Parameters Committee of theAmerican College of Gastroenterology. Practice guidelines onthe diagnosis, surveillance, and therapy of Barrett’s esopha-gus. Am J Gastroenterol 1998;93:1028–32.
61. Inflammatory disorders of the esophagus. reflux and nonrefluxtypes. In: Lewin KJ, Riddell RH, Weinstein WM. Gastroin-
313AJG – February, 2001 Nonerosive Reflux Disease

testinal pathology and its clinical implications. New York:Igaku-Shoin, 1992:401–39.
62. Funch-Jensen P, Kock K, Christensen LA, et al. Microscopicappearance of the esophageal mucosa in a consecutive seriesof patients submitted to upper endoscopy. Correlation withgastroesophageal reflux symptoms and macroscopic findings.Scand J Gastroenterol 1986;21:65–9.
63. Schindlbeck NE, Weibecke B, Klauser AG, et al. Diagnosticvalue of histology in non-erosive gastro-oesophageal refluxdisease. Gut 1996;39:151–4.
64. Kahrilas PJ, Quigley EMM. American Gastrointestinal Asso-ciation medical position statement: Guidelines on the use ofesophageal pH recording. Gastroenterology 1996;110:1981–96.
65. Fass R, Ofman JJ, Pulliam G, et al. Persistent symptoms ofheartburn in patients on standard doses of proton pump inhib-itors (PPI) are not due to acid reflux in most patients. Gastro-enterology 1999;116:G0694.
66. Tew S, Jamieson GG, Pilowsky I, et al. The illness behaviorof patients with gastroesophageal reflux disease with and with-out endoscopic esophagitis. Dis Esophagus 1997;10:9–15.
67. Chal K, Stacey J, Sacks G. The effects of ranitidine on symp-tom relief and quality of life of patients with gastro-esophagealreflux disease. Br J Clin Pract 1995;49:73–7.
68. Glise H. Quality of life and cost of therapy in reflux disease.Scand J Gastroenterol 1995;30:210:38–42.
69. Rust D, Stelmach J, Young T, et al. Clinical effectiveness andquality of life with ranitidine vs. placebo in gastroesophagealreflux disease patients: Clinical experience network study. JFam Pract 1995;41:126–36.
70. Revicki D, Wood M, Maton P, et al. The impact of gastro-esophageal reflux disease on health related quality of life.Am J Med 1998;104:252–8.
71. Carlsson R, Dent J, Watts R, et al. Gastro-oesophageal refluxdisease in primary care: An international study of differenttreatment strategies with omeprazole. Eur J GastroenterolHepatol 1998;10:119–24.
72. Havelund T, Lind T, Wiklund I, et al. Quality of life in patientswith heartburn but without esophagitis: Effects of treatmentwith omeprazole. Am J Gastroenterol 1999;94:1782–9.
73. Fennerty MB, Lieberman D. H2-receptor antagonists in thetreatment of complicated gastroesophageal reflux disease. Forwhom the bell tolls. Gastroenterology 1994;107:1545–8.
74. Sabesin SM, Berlin RG, Humphries TJ, et al. Famotidinerelieves symptoms of gastroesophageal reflux disease andheals erosions and ulcerations. Results of a multicenter, pla-cebo-controlled, dose ranging study. Arch Intern Med 1991;151:2394–400.
75. Kahrilas PJ, Fennerty MB, Joelsson B. High versus standard-dose ranitidine for control of heartburn in poorly-responsivegastroesophageal reflux disease: A prospective controlled trial.Am J Gastroenterol 1999;94:92–7.
76. Hatlebakk JG, Johnsson F, Vilien M, et al. The effect ofcisapride in maintaining symptomatic remission in patientswith gastroesophageal reflux disease. Scand J Gasteroenterol1997;32:1100–6.
77. Chiba N, De Gara CJ, Wilkinson JM, et al. Speed of healing andsymptom relief in grade II to IV gastroesophageal reflux disease:A meta-analysis. Gastroenterology 1997;112:1798–810.
78. Bate CM, Griffin SM, Keeling PWN, et al. Reflux symptomrelief with omeprazole in patients without unequivocal esoph-agitis. Aliment Pharmacol Ther 1996;10:547–55.
79. Venables TL, Newland RD, Patel AC, et al. Omeprazole 10mgonce daily, omeprazole 20mg once daily or ranitidine 150mgtwice daily, evaluated as initial therapy for the relief of symp-toms of gastroesophageal reflux in general practice. Scand JGastroenterol 1997;32:965–73.
80. Richter JE, Campbell DR, Kahrilas PJ, et al. Lansoprazole
compared with ranitidine for the treatment of nonerosive gas-troesophageal reflux disease. Arch Intern Med 2000;160:1803–9.
81. Galmiche JP, Barthelemy P, Hamelin B. Treating the symp-toms of gastroesophageal reflux disease: A double-blind com-parison of omeprazole and cisapride. Aliment Pharmacol Ther1997;11:765–73.
82. Richter JE, Peura D, Benjamin SB, et al. Efficacy of omepra-zole for the treatment of symptomatic acid reflux diseasewithout esophagitis. Arch Intern Med 2000;160:1810–6.
83. Levin TR, Schmittdiel JA, Kunz K, et al. Costs of acid refluxdisorders to a health maintenance organization. Am J Med1997;103:520–8.
84. Lieberman DA, de Garmo P, Brodner R, et al. Why endoscopyis performed: Results of a national consortium. GastrointestEndosc 1999;49:AB145(abstract).
85. Ofman J, Gralnek I, Udani J, et al. The cost-effectiveness ofthe omeprazole test in patients with non-cardiac chest pain.Am J Med 1999;107:219–27.
86. Fass R, Ofman JJ, Gralneck IM, et al. Clinical and economicassessment of the omeprazole test in patients with symptomssuggestive of gastroesophageal reflux disease. Arch InternMed 1999;159:2161–8.
87. O’Connor JF, Singer ME, Richter JE. The cost-effectivenessof strategies to assess gastroesophageal reflux as an exacer-bating factor in asthma. Am J Gastroenterol 1999;94:1472–80.
88. Sonnenberg A, Delco F, El-Serag H. Empirical therapy versusdiagnostic tests in gastroesophageal reflux disease. Dig Dis Sci1998;43:1001–8.
89. Ellis K, Oehlke M, Helfand M, et al. Management of symp-toms of gastroesophageal reflux disease: Does endoscopy in-fluence medical management? Am J Gastroenterol 1997;92:1472–9.
90. Blustein PK, Beck PL, Meddings JB, et al. The utility ofendoscopy in the management of patients with gastroesopha-geal reflux symptoms. Am J Gastroenterol 1998;93:2508–12.
91. Jones R. What happens to patients with non-ulcer dyspepsiaafter endoscopy? Practitioner 1988;232:75–8.
92. Wiklund I, Glise H, Jerndal P, et al. Does endoscopy have apositive impact on quality of life in dyspepsia? GastrointestEndosc 1998;47:449–54.
93. Lucock MP, Morley S, Peake MD. Responses of consecutivepatients to reassurance after gastroscopy: Results of self ad-ministered questionnaire survey. Br Med J 1997;313:572–5.
94. Sonnenberg A, Indaomi J, Becker L. Economic analysis ofstep-wise treatment of gastro-esophageal reflux disease. Ail-ment Pharmacol Ther 1999;13:1003–13.
95. Howden C, Lukasik N, Greski-Rose P, et al. Heartburn. Is“step-up/step down” out of step, evidence from a large com-munity-based trial. Gastroenterology 1999;116:G0829 (ab-stract).
96. Kaplan-Machitz B, Spiegler GE, Zodet MW, et al. Effective-ness and costs of omeprazole vs ranitidine for treatment ofsymptomatic gastroesophageal reflux disease in primary clin-ics in West Virginia. Arch Fam Med 2000;9:624–30.
97. Bardhan KD, Muller-Lissner S, Bigard M, et al. Symptomaticgastro-esophageal reflux disease: Double blind controlledstudy of intermittent treatment with omeprazole or ranitidine.Br Med J 1999;318:502–7.
98. Stalhammer NO, Carlsson J, Peacock R, et al. Cost-effective-ness of omeprazole and ranitidine in intermittent treatment ofsymptomatic GERD. Pharmacoeconomics 1999;16:485–97.
99. Lind T, Havelund T, Lundell L, et al. On demand therapy withomeprazole for the long-term management of patients withheartburn without esophagitis—A placebo-controlled random-ized trial. Ailment Pharmacol Ther 1999;13:907–14.
314 Fass et al. AJG – Vol. 96, No. 2, 2001





























