Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Exploring the Benefits of Conscientiousness:An Investigation of the Role of Daily Stressorsand Health Behaviors
Daryl B. O’Connor, Ph.D. & Mark Conner, Ph.D. &Fiona Jones, Ph.D. & Brian McMillan, Ph.D. &Eamonn Ferguson, Ph.D.
Published online: 26 March 2009# The Society of Behavioral Medicine 2009
AbstractBackground and Purpose This study investigated theimpact of conscientiousness and its facets on healthbehaviors and daily hassles (stressors) and the moderatingeffects of conscientiousness on the hassles–health behaviorrelationshipMethods Four hundred and twenty-two employees com-pleted daily diaries over 4 weeks. Day-to-day within-personeffects of daily hassles on health behaviors were examined,together with the influence of conscientiousness.Results Using hierarchical multivariate linear modeling, theresults showed that conscientiousness was associated withlower consumption of high-fat snacks and more fruit andhigher caffeine intake and smoking (in smokers) across the28-day study period. Facets of conscientiousness were alsofound to moderate the effects of daily hassles on vegetableconsumption, smoking, and likelihood of exercising eachday. Participants with higher levels of order exercised moreon days when they experienced daily hassles, whereasparticipants with lower levels of self-efficacy consumedless vegetables on stressful days. Among smokers, thosewith higher levels of self-discipline reported smoking moreon days when they encountered hassles.Conclusions These findings indicate that conscientiousnessand its facets may influence health status directly viachanges in health behaviors and indirectly through influ-encing stress–health behavior relations.
Keywords Stress . Health behaviors . Personality . Coping .
Daily diaries . Hassles
Introduction
There is a growing body of research that has demonstratedthat conscientiousness is associated with longevity andhealth status [1–5]. Friedman et al. [2], using data from theTerman Life Cycle Study, reported that childhood consci-entiousness predicted longevity and the magnitude of thiseffect (as a risk factor) was comparable to those fromelevated serum cholesterol and systolic blood pressurelevels in adulthood. Much of the work has focused onpotential explanatory mechanisms that may transmit thesebeneficial effects over the life course. For example,Friedman et al. [3] found that the protective influence ofchildhood conscientiousness on health status was accountedfor, in part, by its impact on health behaviors such asalcohol use and smoking. More recently, from a diathesis-stress perspective, researchers have also found that consci-entiousness has the capacity to moderate stress-relatedchanges in health behaviors such that individuals low inconscientiousness respond more negatively to stressfulencounters compared to highly conscientious individuals[6–7]. Taken together, these findings suggest multiplepathways through which conscientiousness may exert itsprotective influence: directly via changes in health behav-iors or indirectly through influencing stress–health behaviorrelations. A third pathway may also exist where conscien-tiousness directly influences the number of daily hassles(stressors) an individual experiences, thereby, reducing anydirect effects of stressors on various bodily systems overtime [8]. However, to date, no research has investigatedsimultaneously the direct effects of conscientiousness on
ann. behav. med. (2009) 37:184–196DOI 10.1007/s12160-009-9087-6
D. B. O’Connor (*) :M. Conner : F. Jones :B. McMillanInstitute of Psychological Sciences, University of Leeds,Leeds, UK LS2 9JTe-mail: [email protected]
E. FergusonDepartment of Psychology, University of Nottingham,Nottingham, UK
health behaviors and daily stressors and its moderatingeffects on the stress–health behavior link. Consequently, thepresent study set out to elucidate the relationship betweenconscientiousness, stress (assessed as daily hassles), andhealth behaviors in a sample of employed men and womenusing a multilevel prospective diary design. The study addsto our understanding of the role of conscientiousness inrelation to health behaviors not only in terms of direct andmoderating effects but also by being the first study toexplore these relationships using daily assessments. There-fore, this research addresses the important question of theextent to which conscientiousness is related to the dailyinitiation of health behaviors.
A meta-analysis of the leading behavioral contributors tothe conscientiousness–mortality relationship, conducted byBogg and Roberts [1], showed conscientiousness to benegatively related to health-damaging behaviors (e.g.,excessive alcohol use r=−0.25; unhealthy eating r=−0.13;tobacco use r=−0.14) and positively related to health-enhancing behaviors (e.g., physical activity r=0.05). Sincethe publication of this review, three important additionalprospective studies have been reported [4–5, 9]. Twodescribe how the effects of childhood conscientiousness onhealth status 40 years later are partially mediated by smoking,body mass index, educational attainment, and healthy eatinghabits [4–5]. The third showed that both childhood and adultconscientiousness predicted adult mortality, but the effects ofadult, not childhood conscientiousness, were mediated byadult smoking and alcohol use [9].
Moreover, other recent work has attempted to explain theimpact of conscientiousness on health behaviors in terms ofits impact on self-regulation processes. This is because thecharacteristics and activities associated with conscientious-ness (e.g., the ability to control one’s behavior and tocomplete tasks) are likely to facilitate the performance ofaversive or difficult health behaviors that individuals aremotivated to perform [10]. Four studies have reportedevidence of this relationship [11–14]. For example, Conneret al. [11] reported conscientiousness to moderate theimpact of intentions to exercise on exercise behavior butonly for exercise completed in nonusual weeks. Similarly,Rhodes et al. [12–13] reported conscientiousness tosignificantly moderate the intention–exercise behaviorrelationship, with higher levels of conscientiousness asso-ciated with stronger intention–behavior relationships.
To date, most of the available evidence has utilized atrait approach and predicted health outcomes from person-ality traits using cross-sectional or prospective designs (cf.,[1]). Of the 194 studies reviewed by Bogg and Roberts [1],only ten investigations were longitudinal with a largemajority relying on “snapshot” and/or retrospective measure-ments of health behaviors. Bogg and Roberts [1] alsoacknowledge the difficulty in drawing inferences based upon
the large number of cross-sectional studies. As a result, it isdifficult to discern firm conclusions about the process ofhow conscientiousness influences future health status.
Surprisingly, research in this area has not utilizedmultilevel daily process studies which: (a) permit frequentmeasurement of within-person variables (e.g., healthbehaviors) together with between-person factors (e.g.,conscientiousness); (b) reduce recall bias; and (c) allowparticipants to be used as their own controls (see [9]).Indeed, Bogg and Roberts [1] acknowledged that theoverreliance on cross-sectional methodologies represents asubstantial weakness and they have suggested that futureinvestigations ought to concentrate on using daily diaryapproaches to “provide a more definitive test of therelationship between conscientiousness and health-relatedbehaviors” (p. 912). In addition, previous research hasignored the growing body of evidence showing thatfluctuations in within-person stressful daily hassles areimportant in understanding health behavior processes (e.g.,[15–19]). For example, O’Connor et al. [19] recentlyshowed that daily hassles have the capacity to disrupthabitual health behaviors such that on days when individ-uals experienced hassles they consumed significantly morehigh-fat and sugar snacks. Hassles are events, thoughts, orsituations which, when they occur, produce negative feel-ings such as annoyance, irritation, worry or frustration, and/or make you aware that your goals and plans will be moredifficult to achieve (see [16–17, 20]).
Nevertheless, to date, no research has examined whetherconscientiousness may exert, in part, its positive influenceon health indirectly by moderating the effects of dailyhassles, such that conscientious individuals may respond tohassles by engaging in more health-enhancing and lesshealth-damaging behaviors. Alternatively, it is also possiblethat conscientious individuals may simply experience fewerhassles given they are better organized, prepared, anddisciplined. Limited evidence exists that indicates thatconscientious individuals are more likely to employproblem-focused coping in response to stress and toperceive themselves as being able to meet situationaldemands; however, no studies have investigated therelationship between conscientiousness, daily hassles, andhealth behaviors [6–7]. For example, it is feasible thatconscientious individuals may engage in certain types ofhealth behaviors, such as exercise, as a way of activelycoping with daily stressors. Therefore, in order to explorethese possibilities, we used a multilevel diary design toexamine day-to-day within-person effects of daily hassleson a range of health behaviors over 28 days (i.e., high-fatsnacks, caffeinated beverages, alcohol, smoking, exercise,fruit and vegetable intake) while simultaneously investigat-ing the influence of conscientiousness as a possiblemoderating variable.
ann. behav. med. (2009) 37:184–196 185

Conscientiousness can be measured in a number ofdifferent ways using validated measures such as the NEOPersonality Inventory, the International Personality ItemPool (IPIP), the Jackson Personality Inventory, the Cal-ifornia Personality Inventory, and so forth [21]. Eachmeasure comprises of different facets of conscientiousnessand the lower-order structure of conscientiousness has beenthe subject of much empirical investigation [21–24]. Alarge amount of previous research into the conscientious-ness–health behavior link has focused on global assess-ments of conscientiousness but very little on the impact ofits lower-order facets on the engagement of healthbehaviors. Costa et al. [23] have conceptualized conscien-tiousness as having proactive (e.g., need for achievement)and inhibitive (e.g., cautiousness) aspects which maydifferentially influence health behaviors. However, nostudies have explored the links between these lower-orderfacets and the daily initiation of health behaviors. There-fore, in the current study, we measured five facets ofconscientiousness using items from the IPIP (i.e., self-efficacy, order, achievement striving, self-discipline, andcautiousness), a public domain measure of the Big Fivepersonality factors, in order to advance understanding ofwhich were the most critical facets of conscientiousness.
In summary, this study had three main aims: (1) toexamine the direct impact of conscientiousness and dailyhassles on a range of health behaviors, (2) to investigatewhether conscientiousness can moderate daily hassles–health behavior relations, and (3) to test whether individualshigh in conscientiousness experience less daily hasslesacross the study period compared to individuals low inconscientiousness.
Method
Participants
Participants were recruited from a large local governmentorganization in the UK. A total of 466 individuals (215males; 251 females) aged 18–65 years took part in the firstround of the study, which consisted of a 1-week daily diaryand completion of an initial demographics questionnaire(e.g., age, height, weight). A total of 449 of theseindividuals (207 males; 242 females) completed the second1-week daily diary; 443 (202 males; 241 females) completedthe third 1-week daily diary; 437 (200 males; 237 females)completed the fourth 1-week daily diary and 428 (197 males;231 females) completed a final questionnaire. Complete dataacross all the diaries and final questionnaire were availablefrom 422 participants (193 male, 229 female). There were nodifferences on the main study variables between thecompleters and noncompleters. Therefore, all subsequent
analyses focus on the sample of 422. The mean age of thefinal sample was 40.26 years (range=18–65 years).Participants spanned a range of public service occupa-tions, including administrative workers and police andsocial workers, with a majority (63%) in managerial andprofessional occupations. Only 7% were in semi-routineor routine occupations. Participants were reimbursedapproximately $75 for taking part in the study.
Design
Participants completed an initial questionnaire, followed byfour 7-day daily diaries and a final questionnaire at the endof the study. Diaries were returned at the end of each weekand checked against postmarks in order to ensure theparticipants complied with the study protocol and complet-ed their diary during the appropriate week. As a result, nodiaries were excluded. This study received ethical approvalfrom the University Department Ethics Committee.
An interval-contingent method was employed, where theparticipants completed their diary at the end of each day fora period of 4 weeks, with the diary returned by post to theresearchers at the end of each week. The use of weeklydiaries to collect end-of-day data—especially over anextended period of time—is a well-established protocol inthe health, clinical, and social psychology literature (e.g.,[25–26]) that has been shown to produce reliable data [27].End-of-day diaries rather than event-contingent diaries wereutilized to increase motivation and compliance with thediary protocol. This procedure reduces participant burdenwhen the time span of the study is long (lasting weeks ormonths; see [28]) and it has been argued that reducedburden increases participant compliance [27].
Measures
Participants completed a daily diary form at the end of eachday in which they recorded daily hassles and a range ofdaily health behaviors and they completed a series ofquestionnaires at the beginning and the end of the study.
Daily Diary Measures
Daily Hassles
In each 7-day daily diary, participants were requested—using free responses—to report each stressor or hassleexperienced and then to rate its intensity on a scaleextending from “not stressful” (0) to “very stressful” (4).The results for “actual number” and a combined “totalintensity” of hassles by the “actual number” of hasslesmeasure were substantively similar; therefore, only theresults for the actual number of hassles are reported. Daily
186 ann. behav. med. (2009) 37:184–196

hassles were defined as events, thoughts, or situationswhich, when they occur, produce negative feelings such asannoyance, irritation, worry, or frustration and/or make youaware that your goals and plans will be more difficult orimpossible to achieve (see [16–17, 19]). Examples ofhassles were provided in each diary booklet. The use ofopen-ended daily diaries allowed respondents to recordday-to-day minor life events or hassles that are part ofeveryday life and have the advantage of not constrainingrespondents to a limited number of events, unlike usingdaily hassles checklists. Thus, in the current study,measuring hassles using a free-response format allowed alarge number of stress occurrences in each respondent to beidentified, making it possible to look at whether a range ofhealth behaviors coincided with hassles on a number ofoccasions, enabling a realistic view of daily healthbehaviors in response to stress. Good interrater reliabilityand validity have been demonstrated previously for thistechnique (see [17, 18–20]).
Daily Health Behaviors
The following health behaviors (fruit consumption, physi-cal exercise, high-fat snack consumption, cigarette use,alcohol and caffeine intake) were assessed each day asoutlined below.
Between-meal snack consumption was measured byasking participants to list each of the foods they had eatenbetween meals on each day. For the purpose of thisinvestigation, we were only interested in snacks categorizedas being high in fat based upon validated food compositiontables [29]. All coding was conducted by a panel of fourhealth psychologists, trained to Ph.D. level with a mean of13-year research experience, resulting in good interraterreliability with all kappas above 0.70.
Portions of fruit consumption were assessed by askingparticipants to report the number of portions of fruit eateneach day using guidance from the UK Department ofHealth’s Five-A-Day campaign.
Daily cigarette use was assessed by asking participantshow many cigarettes they had smoked each day. Theresponse option, “I did not/do not smoke” was alsoprovided.
Daily alcohol consumption was assessed by askingparticipants how many of the following they had consumedon each day: pints of beer/lager/cider, measures of spirits,and glasses of wine. The response option “I did not drinkany alcohol today” was also provided. Answers to thesequestions were combined and converted into units (one unitcorresponding to approximately 8 g of ethanol, i.e., a smallglass of wine or half a pint of beer).
Daily caffeinated beverage consumption was assessedusing a single question: “how many drinks containing
caffeine have you had today?” with open-response format.Participants were provided with the following informationas an aid to identifying caffeinated drinks: “Drinkscontaining caffeine include tea and coffee, ‘colas,’ e.g.,Pepsi or Coke, ‘energy drinks,’ e.g., Lucozade, Red Bull,and many soft drinks, e.g., Irn Bru.”
Daily exercise was measured by asking participants ifthey had participated in any exercise that day (yes=1, no=0) and if they endorsed the “yes” response they were askedto describe the exercise. This was used to check thatresponses approximated to descriptions of moderate orvigorous exercise as defined by the International PhysicalActivity Questionnaire [30].
Questionnaire Measures
Conscientiousness was assessed using a 50-item measurefrom the IPIP [24]—a public domain measure of the BigFive personality dimensions (www.ipip.ori.org/ipip/). Sim-ilar to the NEO inventory [23, 31], the IPIP consists of facetscales for each of the five major personality domains. TheIPIP facets have been found to correlate highly with itsNEO inventory counterparts (rs<0.90) and to have goodconstruct validity and reliability [24]. In the current study,we measured five of the facets of conscientiousness (i.e.,achievement striving, self-discipline, self-efficacy, cautious-ness, and order). Achievement striving deals with the needto strive for excellence (example item: “Go straight for thegoal”). Self-discipline is concerned with persistence andone’s ability to persevere with a task despite boredom or inthe face of distraction (example item: “Carry out myplans”). Self-efficacy (or competence) relates to the extentthat an individual is capable and accomplished (exampleitem: “Complete task successfully”). Cautiousness (ordeliberation) deals with the extent to which an individualplans and is thoughtful (example item: “Jump into thingswithout thinking”). Order is concerned with the extent towhich an individual tends to keep their environmentorganized (example item: “Love order and regularity”). Itis important to note that ten-item measures of neuroticism,openness to experience, extraversion, and agreeablenesswere also administered to participants given that previousresearchers have examined their impact on health behaviorsand daily hassles. Neuroticism in particular has receivedsubstantial attention; therefore, in preliminary analyses, weinvestigated its impact on each of the health behaviors (e.g.,see [32]). The findings from the present data showed thatneuroticism did not exert any direct effects on the currenthealth behaviors or moderate any of the hassles–healthbehavior relationships and as a result is not considered inany further analyses. Internal consistency for each of thefacets of conscientiousness in this sample was good(alpha=0.82–0.86).
ann. behav. med. (2009) 37:184–196 187

Data Analysis
The daily data were analyzed using hierarchical multivar-iate linear modeling (HMLM) using HLM6 [33]. HMLMallows alternative models of temporal variance–covariancestructure to be assessed and is therefore a suitable modelingstrategy for a fixed occasion design [33–34]. For all themodels tested here, the assumption of an unrestricted level1 variance–covariance structure fitted the data best.
The data contained a two-level hierarchical structure,level 1 being the within-person variation (e.g., daily patternsin health behaviors, the number of hassles experienced) andlevel 2 being the between-person variability (e.g., conscien-tiousness). Age was also entered as a level 2 variable inpreliminary analyses; however, given that the results weresubstantively the same and to be parsimonious, it was notincluded in the main analyses. The level 1 predictor wasnumber of daily hassles and was centered around the groupmean (cf., [26]). The level 2 variable was centered aroundthe grand mean (cf. [26]). The analyses were conducted intwo stages; initially, the data were modeled for the totalconscientiousness scores followed separately by each of thefive conscientiousness facets. Participants who had missedan entire week or more or did not return the finalquestionnaire were excluded from the analyses.
Significant cross-level interactions, where conscientious-ness was found to moderate a hassles–health behaviorrelationship, were examined using generalized simple slopesanalysis for cross-level interactions as described by Preacheret al. [35]. For the analysis of variables with continuous out-comes (e.g., portions of vegetables, smoking in smokers),coefficients were taken from those reported for the unre-stricted models from the HMLM analyses and the variance–covariance matrix derived using robust standard errors.When the outcome was dichotomous (e.g., exercise behav-ior), the models were based on the unit-averaged coefficientsusing a logistic link function and robust standard errors (withthe appropriate variance–covariance matrix). The unit-specific model was chosen as this allows us to examine theeffect of the moderator on the individual’s daily experiences.These were implemented using the free software provided byPreacher at http://www.people.ku.edu/∼preacher/. In eachcase, we plotted the hassles–health behavior slopes at high(one standard deviation above the mean), average (at themean), and at low (one standard deviation below the mean)levels of conscientiousness and conducted further testsseparately on each slope to determine whether they weresignificantly different from zero.
In summary, level 1 slopes (models) were examined toinvestigate the relationship between experiencing dailyhassles and each of the health behavior outcome measuresover the 28-day study period. We also examined the cross-level effects: (1) whether there was a main effect of
conscientiousness (level 2 variable) on day-to-day within-person health behaviors (level 1 variables) and (2) whetherthe daily hassles–health behavior relationship (level 1) wasmoderated by conscientiousness (level 2). This modelingstrategy was repeated for each of the five conscientiousnessfacets.
The general form of each model is expressed by thefollowing equations (note: in the case of exercise, which isa dichotomous variable, the level 1 model was replaced bya Bernoulli model; [33]):
Health behavior ¼ b00þ b01 � conscientiousnessþb10� dailyhasslesþb11� conscientiousness daily hassles þ"
where β00 indicates the mean level of health behavior; β01indicates the extent to which this average is influenced bylevel of conscientiousness; β10 indicates the average size ofthe relationship between daily hassles and health behavior,β11 the extent to which that relationship is moderated by (orconditional on) level of conscientiousness, and ɛ the errorterm.
Treatment of Missing Data
There were two participants (0.47%) with missing data atlevel 2 and these were listwise deleted following theconvincing data presented by Gibson and Olejnik [36]demonstrating that this is the most appropriate techniquefor dealing with missing data at level 2. There were fourvariables with missing data at level 1 (units of alcohol,number of caffeinated drinks, portions of fruit and vegeta-bles). Little and Rubin’s [37] missing completely at randomtest indicated that these four variables were indeed missingcompletely at random (χ2 (14)=9.95, p=0.76). The totalmissing data across these variables were 207 data points outof a maximum of 11,816. This equates to 1.7%. Moreover, ithas been argued that if less than 10% of the data is missingand no more than 10% of data is missing for a singlevariable, then single imputation (SI) is an appropriatestrategy to be adopted to allow for missing values to beestimated so that complete data sample analytic techniquescan be applied [38–39]. Therefore, all the analyses reportedin the paper are based on a complete dataset derived usingSI. The imputed dataset was generated in Amelia (see http://gking.harvard.edu/stats.shtml) using an expectancy maximi-zation with importance sampling approach. The 420 partic-ipants who provided usable datasets provided 11,760 days ofdata. The analysis of the effects of conscientiousness onsmoking included only the 91 participants (49 females) whoclassified themselves as smokers. However, it is worthnoting that there was no significant difference on levels ofconscientiousness between smokers and nonsmokers.
188 ann. behav. med. (2009) 37:184–196
With respect to the possibility of type 1 inflation rates,we aimed to guard against this by testing specifichypotheses. The Bonferroni correction suggests that thereis potentially one spurious effect in Table 2 (1.4 effects tobe exact); for Table 3, there are potentially three spuriouseffects (exact=3.5 effects) and for Table 4 zero (exact 0.3of an effect). Thus, while there is potential for somespurious effects, this is limited in number and the effectsobserved are consistent with theory.
Results
Descriptive Statistics
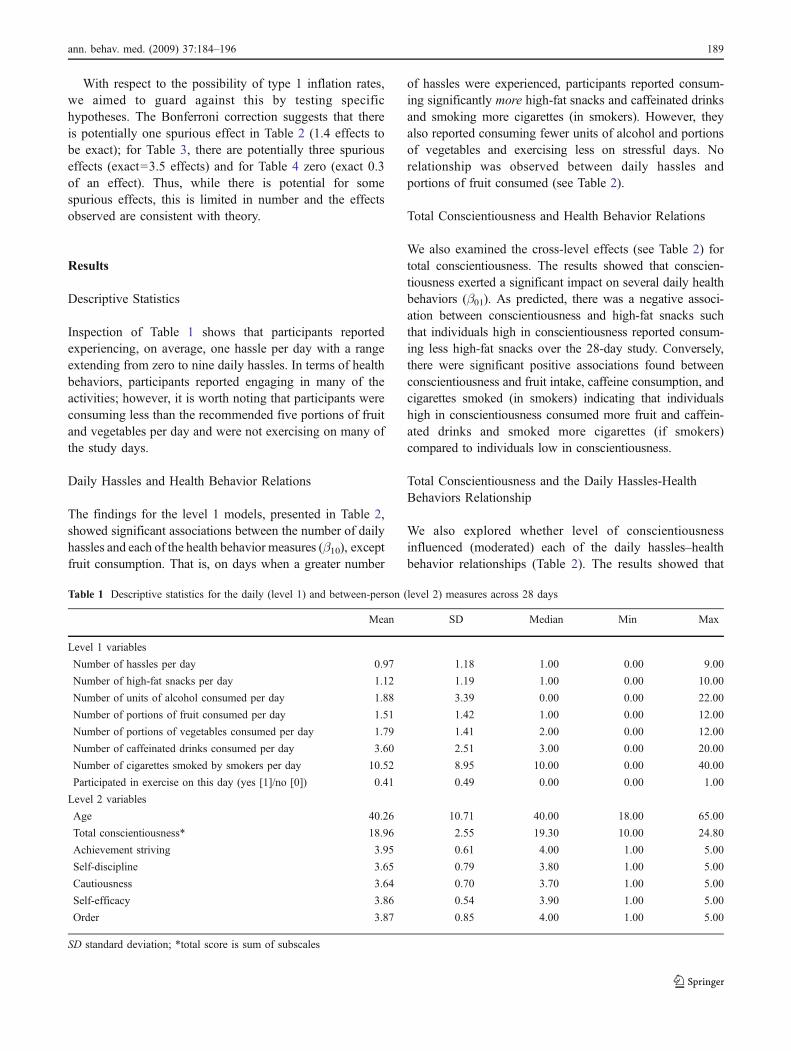
Inspection of Table 1 shows that participants reportedexperiencing, on average, one hassle per day with a rangeextending from zero to nine daily hassles. In terms of healthbehaviors, participants reported engaging in many of theactivities; however, it is worth noting that participants wereconsuming less than the recommended five portions of fruitand vegetables per day and were not exercising on many ofthe study days.
Daily Hassles and Health Behavior Relations
The findings for the level 1 models, presented in Table 2,showed significant associations between the number of dailyhassles and each of the health behavior measures (β10), exceptfruit consumption. That is, on days when a greater number
of hassles were experienced, participants reported consum-ing significantly more high-fat snacks and caffeinated drinksand smoking more cigarettes (in smokers). However, theyalso reported consuming fewer units of alcohol and portionsof vegetables and exercising less on stressful days. Norelationship was observed between daily hassles andportions of fruit consumed (see Table 2).
Total Conscientiousness and Health Behavior Relations
We also examined the cross-level effects (see Table 2) fortotal conscientiousness. The results showed that conscien-tiousness exerted a significant impact on several daily healthbehaviors (β01). As predicted, there was a negative associ-ation between conscientiousness and high-fat snacks suchthat individuals high in conscientiousness reported consum-ing less high-fat snacks over the 28-day study. Conversely,there were significant positive associations found betweenconscientiousness and fruit intake, caffeine consumption, andcigarettes smoked (in smokers) indicating that individualshigh in conscientiousness consumed more fruit and caffein-ated drinks and smoked more cigarettes (if smokers)compared to individuals low in conscientiousness.
Total Conscientiousness and the Daily Hassles-HealthBehaviors Relationship
We also explored whether level of conscientiousnessinfluenced (moderated) each of the daily hassles–healthbehavior relationships (Table 2). The results showed that
Table 1 Descriptive statistics for the daily (level 1) and between-person (level 2) measures across 28 days
Mean SD Median Min Max
Level 1 variables
Number of hassles per day 0.97 1.18 1.00 0.00 9.00
Number of high-fat snacks per day 1.12 1.19 1.00 0.00 10.00
Number of units of alcohol consumed per day 1.88 3.39 0.00 0.00 22.00
Number of portions of fruit consumed per day 1.51 1.42 1.00 0.00 12.00
Number of portions of vegetables consumed per day 1.79 1.41 2.00 0.00 12.00
Number of caffeinated drinks consumed per day 3.60 2.51 3.00 0.00 20.00
Number of cigarettes smoked by smokers per day 10.52 8.95 10.00 0.00 40.00
Participated in exercise on this day (yes [1]/no [0]) 0.41 0.49 0.00 0.00 1.00
Level 2 variables
Age 40.26 10.71 40.00 18.00 65.00
Total conscientiousness* 18.96 2.55 19.30 10.00 24.80
Achievement striving 3.95 0.61 4.00 1.00 5.00
Self-discipline 3.65 0.79 3.80 1.00 5.00
Cautiousness 3.64 0.70 3.70 1.00 5.00
Self-efficacy 3.86 0.54 3.90 1.00 5.00
Order 3.87 0.85 4.00 1.00 5.00
SD standard deviation; *total score is sum of subscales
ann. behav. med. (2009) 37:184–196 189
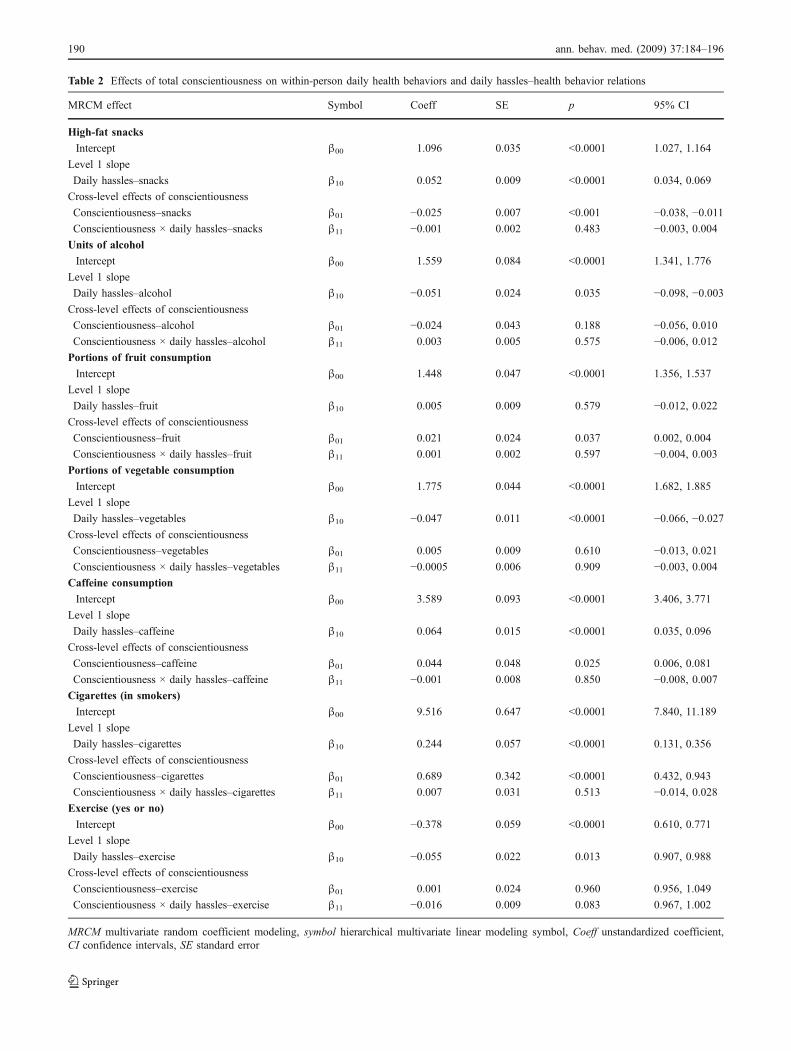
Table 2 Effects of total conscientiousness on within-person daily health behaviors and daily hassles–health behavior relations
MRCM effect Symbol Coeff SE p 95% CI
High-fat snacks
Intercept β00 1.096 0.035 <0.0001 1.027, 1.164
Level 1 slope
Daily hassles–snacks β10 0.052 0.009 <0.0001 0.034, 0.069
Cross-level effects of conscientiousness
Conscientiousness–snacks β01 −0.025 0.007 <0.001 −0.038, −0.011Conscientiousness × daily hassles–snacks β11 −0.001 0.002 0.483 −0.003, 0.004Units of alcohol
Intercept β00 1.559 0.084 <0.0001 1.341, 1.776
Level 1 slope
Daily hassles–alcohol β10 −0.051 0.024 0.035 −0.098, −0.003Cross-level effects of conscientiousness
Conscientiousness–alcohol β01 −0.024 0.043 0.188 −0.056, 0.010Conscientiousness × daily hassles–alcohol β11 0.003 0.005 0.575 −0.006, 0.012Portions of fruit consumption
Intercept β00 1.448 0.047 <0.0001 1.356, 1.537
Level 1 slope
Daily hassles–fruit β10 0.005 0.009 0.579 −0.012, 0.022Cross-level effects of conscientiousness
Conscientiousness–fruit β01 0.021 0.024 0.037 0.002, 0.004
Conscientiousness × daily hassles–fruit β11 0.001 0.002 0.597 −0.004, 0.003Portions of vegetable consumption
Intercept β00 1.775 0.044 <0.0001 1.682, 1.885
Level 1 slope
Daily hassles–vegetables β10 −0.047 0.011 <0.0001 −0.066, −0.027Cross-level effects of conscientiousness
Conscientiousness–vegetables β01 0.005 0.009 0.610 −0.013, 0.021Conscientiousness × daily hassles–vegetables β11 −0.0005 0.006 0.909 −0.003, 0.004Caffeine consumption
Intercept β00 3.589 0.093 <0.0001 3.406, 3.771
Level 1 slope
Daily hassles–caffeine β10 0.064 0.015 <0.0001 0.035, 0.096
Cross-level effects of conscientiousness
Conscientiousness–caffeine β01 0.044 0.048 0.025 0.006, 0.081
Conscientiousness × daily hassles–caffeine β11 −0.001 0.008 0.850 −0.008, 0.007Cigarettes (in smokers)
Intercept β00 9.516 0.647 <0.0001 7.840, 11.189
Level 1 slope
Daily hassles–cigarettes β10 0.244 0.057 <0.0001 0.131, 0.356
Cross-level effects of conscientiousness
Conscientiousness–cigarettes β01 0.689 0.342 <0.0001 0.432, 0.943
Conscientiousness × daily hassles–cigarettes β11 0.007 0.031 0.513 −0.014, 0.028Exercise (yes or no)
Intercept β00 −0.378 0.059 <0.0001 0.610, 0.771
Level 1 slope
Daily hassles–exercise β10 −0.055 0.022 0.013 0.907, 0.988
Cross-level effects of conscientiousness
Conscientiousness–exercise β01 0.001 0.024 0.960 0.956, 1.049
Conscientiousness × daily hassles–exercise β11 −0.016 0.009 0.083 0.967, 1.002
MRCM multivariate random coefficient modeling, symbol hierarchical multivariate linear modeling symbol, Coeff unstandardized coefficient,CI confidence intervals, SE standard error
190 ann. behav. med. (2009) 37:184–196

total conscientiousness moderated none of the dailyhassles–health behavior relationships (β11). However, therewas a trend towards statistical significance for the cross-level interaction with the slope coefficient for the dailyhassles–exercise relationship (p=0.083).
Facets of Conscientiousness and Health Behavior Relations
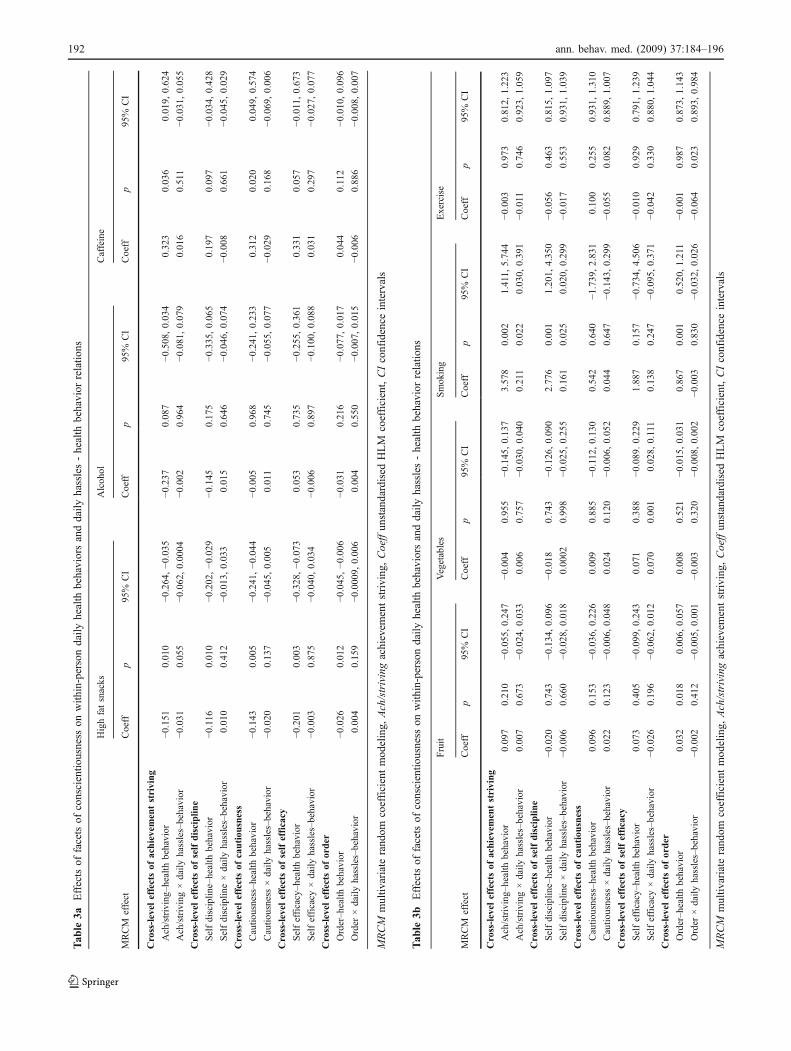
The findings for the level 1 models, presented in Table 3,showed a number of significant associations between thefacets of conscientiousness and the health behavior measures.For consumption of high-fat snacks, each of the facets ofconscientiousness exerted a significant impact such thatindividuals higher on achievement striving, self-discipline,cautiousness, self-efficacy, and order reported consuming lesshigh-fat snacks over the 28-day study than individuals withlower levels. For caffeine, higher scores on achievementstriving and cautiousness were associated with a greaterconsumption of caffeinated drinks. Daily fruit intake wasonly associated with the order facet such that higher levelswere associated with greater fruit consumption. In terms ofsmoking behavior (in smokers), achievement striving, self-discipline, and order were each significantly positivelyassociated with the number of cigarettes smoked such thatindividuals higher in conscientiousness smoked significantlymore cigarettes.
Facets of Conscientiousness and the Daily Hassles–HealthBehaviors Relationship
We also examined whether the facets of conscientiousnessinfluenced (moderated) each of the daily hassles–healthbehavior relationships (Tables 3). The results showed therewere a number of significant cross-level interactions. Theself-efficacy facet was found to moderate the daily hassles–vegetable consumption relationship such that as levels ofself-efficacy increased the negative relationship betweendaily hassles and vegetable consumption was attenuated.Simple slopes analysis revealed that the daily hassles–vegetable consumption slope was significantly differentfrom zero at low (β=−0.086, t=−4.84, p<0.001) andaverage (β=−0.048, t=−3.79, p<0.001) but not at highlevels of self-efficacy (β=−0.011, t=−0.574, ns) indicatingthat individuals with low or average levels of this facet ofconscientiousness ate less vegetables on days when theyexperienced hassles. In terms of smoking behavior,achievement striving and self-discipline were found to besignificant moderators such that as levels of conscientious-ness increased the positive relationship between dailyhassles and smoking became stronger. Simple slopesanalysis showed that the daily hassles–smoking behaviorslope was significantly different from zero at high (β=0.378, t=2.08, p<0.05) and average (β=0.251, t=2.024,
p<0.05) but not at low levels of self-discipline (β=0.124,t=0.620, ns) indicating that smoker individuals with high oraverage levels of this facet smoked more on days when theyexperienced hassles. Despite the significant cross-levelinteraction for achievement striving, the effect was renderednonsignificant when it was decomposed. However, thepattern of results was very similar to self-disciplinewhereby there was evidence that the daily hassles–smokingbehavior slopes were different (albeit, nonsignificantly)from zero at high (β=0.336, t=1.707, p=0.09) and average(β=0.207, t=1.631, p=0.11) but not low levels of achieve-ment striving (β=0.078, t=0.322, p=0.75). Finally, orderwas found to be a significant moderator of the daily hassles–exercise relationship. Simple slopes analysis revealed thatthe daily hassles–exercise slope was significantly differentfrom zero at high (β=−0.149, t=−3.93, p<0.001) andaverage (β=−0.064, t=−2.417, p<0.05) but not at low levelsof order (β=0.021, t=0.596, ns) indicating that individualswho had average or high levels of order were more likely toexercise when they experienced hassles.
Conscientiousness and Daily Hassles Relations
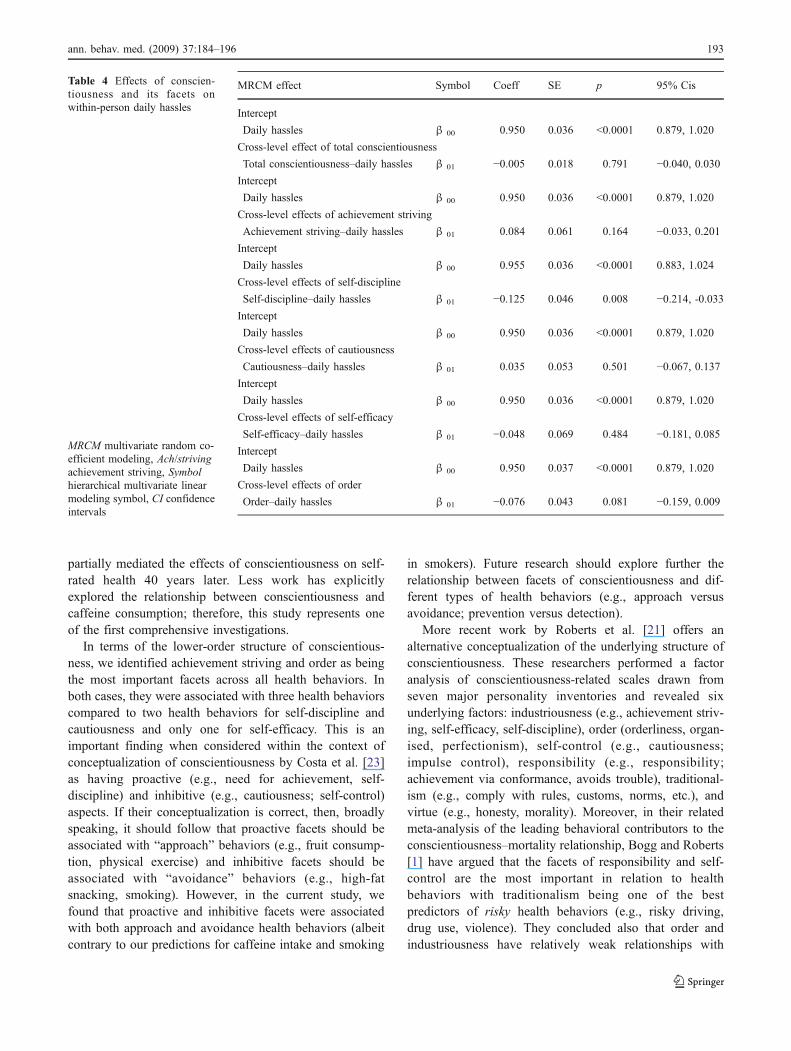
Finally, in order to explore whether individuals high inconscientiousness experienced fewer daily hassles generallycompared to individuals low in conscientiousness, we exam-ined whether there were cross-level effects of conscientious-ness and its facets on day-to-day within-person daily hassles.The results shown in Table 4 indicate that only self-disciplinewas significantly associated with daily hassles such thatindividuals high in this facet of conscientiousness did indeedreport fewer daily hassles. The relationship between the orderfacet and daily hassles was also in the same direction but justmissed conventional statistical significance.
Discussion
We found evidence that higher levels of conscientiousnesswere associated with lower consumption of high-fat snacksand higher fruit intake but also with higher caffeine intakeand smoking (in smokers). These results are important asthey indicate for the first time that conscientiousness mayhave a differential (counterintuitive) influence on differenttypes of health behaviors. The findings relating to high-fatsnack consumption and fruit intake are consistent withexisting research that has identified unhealthy eating as akey mediator of the conscientiousness–longevity relation-ship [1, 5]. However, the positive association observedbetween conscientiousness and smoking is contrary to alarge number of studies. For example, Hampson andcolleagues [5] found childhood conscientiousness wasassociated with less adult smoking and that this relationship
ann. behav. med. (2009) 37:184–196 191
Tab
le3a
Effectsof
facetsof
conscientio
usness
onwith
in-persondaily
health
behaviorsanddaily
hassles-health
behavior
relatio
ns
Highfatsnacks
Alcohol
Caffeine
MRCM
effect
Coeff
p95%
CI
Coeff
p95%
CI
Coeff
p95%
CI
Cross-level
effectsof
achievementstriving
Ach/striving–
health
behavior
−0.151
0.010
−0.264,−0
.035
−0.237
0.087
−0.508,0.034
0.323
0.036
0.019,
0.624
Ach/striving×daily
hassles–behavior
−0.031
0.055
−0.062,0.0004
−0.002
0.964
−0.081,0.079
0.016
0.511
−0.031,0.055
Cross-level
effectsof
selfdisciplin
e
Selfdisciplin
e–health
behavior
−0.116
0.010
−0.202,−0
.029
−0.145
0.175
−0.335,0.065
0.197
0.097
−0.034,0.428
Selfdisciplin
e×daily
hassles–behavior
0.010
0.412
−0.013,0.033
0.015
0.646
−0.046,0.074
−0.008
0.661
−0.045,0.029
Cross-level
effectsof
cautiou
sness
Cautio
usness–h
ealth
behavior
−0.143
0.005
−0.241,−0
.044
−0.005
0.968
−0.241,0.233
0.312
0.020
0.049,
0.574
Cautio
usness
×daily
hassles–behavior
−0.020
0.137
−0.045,0.005
0.011
0.745
−0.055,0.077
−0.029
0.168
−0.069,0.006
Cross-level
effectsof
selfefficacy
Selfefficacy–h
ealth
behavior
−0.201
0.003
−0.328,−0
.073
0.053
0.735
−0.255,0.361
0.331
0.057
−0.011,0.673
Selfefficacy
×daily
hassles–behavior
−0.003
0.875
−0.040,0.034
−0.006
0.897
−0.100,0.088
0.031
0.297
−0.027,0.077
Cross-level
effectsof
order
Order–h
ealth
behavior
−0.026
0.012
−0.045,−0
.006
−0.031
0.216
−0.077,0.017
0.044
0.112
−0.010,0.096
Order
×daily
hassles–behavior
0.004
0.159
−0.0009,
0.006
0.004
0.550
−0.007,0.015
−0.006
0.886
−0.008,0.007
MRCM
multiv
ariate
rand
omcoefficientmod
eling,
Ach/strivingachievem
entstriving
,Coeffun
standardised
HLM
coefficient,CIconfidence
intervals
Tab
le3b
Effectsof
facetsof
conscientio
usness
onwith
in-persondaily
health
behaviorsanddaily
hassles-health
behavior
relatio
ns
Fruit
Vegetables
Smoking
Exercise
MRCM
effect
Coeff
p95%
CI
Coeff
p95%
CI
Coeff
p95%
CI
Coeff
p95%
CI
Cross-level
effectsof
achievementstriving
Ach/striving–
health
behavior
0.097
0.210
−0.055,0.247
−0.004
0.955
−0.145,0.137
3.578
0.002
1.411,
5.744
−0.003
0.973
0.812,
1.223
Ach/striving×daily
hassles–behavior
0.007
0.673
−0.024,0.033
0.006
0.757
−0.030,0.040
0.211
0.022
0.030,
0.391
−0.011
0.746
0.923,
1.059
Cross-level
effectsof
selfdisciplin
e
Selfdisciplin
e–health
behavior
−0.020
0.743
−0.134,0.096
−0.018
0.743
−0.126,0.090
2.776
0.001
1.201,
4.350
−0.056
0.463
0.815,
1.097
Selfdisciplin
e×daily
hassles–behavior
−0.006
0.660
−0.028,0.018
0.0002
0.998
−0.025,0.255
0.161
0.025
0.020,
0.299
−0.017
0.553
0.931,
1.039
Cross-level
effectsof
cautiou
sness
Cautio
usness–h
ealth
behavior
0.096
0.153
−0.036,0.226
0.009
0.885
−0.112,0.130
0.542
0.640
−1.739,2.831
0.100
0.255
0.931,
1.310
Cautio
usness
×daily
hassles–behavior
0.022
0.123
−0.006,0.048
0.024
0.120
−0.006,0.052
0.044
0.647
−0.143,0.299
−0.055
0.082
0.889,
1.007
Cross-level
effectsof
selfefficacy
Selfefficacy–h
ealth
behavior
0.073
0.405
−0.099,0.243
0.071
0.388
−0.089.0.229
1.887
0.157
−0.734,4.506
−0.010
0.929
0.791,
1.239
Selfefficacy
×daily
hassles–behavior
−0.026
0.196
−0.062,0.012
0.070
0.001
0.028,
0.111
0.138
0.247
−0.095,0.371
−0.042
0.330
0.880,
1.044
Cross-level
effectsof
order
Order–h
ealth
behavior
0.032
0.018
0.006,
0.057
0.008
0.521
−0.015,0.031
0.867
0.001
0.520,
1.211
−0.001
0.987
0.873,
1.143
Order
×daily
hassles–behavior
−0.002
0.412
−0.005,0.001
−0.003
0.320
−0.008,0.002
−0.003
0.830
−0.032,0.026
−0.064
0.023
0.893,
0.984
MRCM
multiv
ariate
rand
omcoefficientmod
eling,
Ach/strivingachievem
entstriving
,Coeffun
standardised
HLM
coefficient,CIconfidence
intervals
192 ann. behav. med. (2009) 37:184–196
partially mediated the effects of conscientiousness on self-rated health 40 years later. Less work has explicitlyexplored the relationship between conscientiousness andcaffeine consumption; therefore, this study represents oneof the first comprehensive investigations.
In terms of the lower-order structure of conscientious-ness, we identified achievement striving and order as beingthe most important facets across all health behaviors. Inboth cases, they were associated with three health behaviorscompared to two health behaviors for self-discipline andcautiousness and only one for self-efficacy. This is animportant finding when considered within the context ofconceptualization of conscientiousness by Costa et al. [23]as having proactive (e.g., need for achievement, self-discipline) and inhibitive (e.g., cautiousness; self-control)aspects. If their conceptualization is correct, then, broadlyspeaking, it should follow that proactive facets should beassociated with “approach” behaviors (e.g., fruit consump-tion, physical exercise) and inhibitive facets should beassociated with “avoidance” behaviors (e.g., high-fatsnacking, smoking). However, in the current study, wefound that proactive and inhibitive facets were associatedwith both approach and avoidance health behaviors (albeitcontrary to our predictions for caffeine intake and smoking
in smokers). Future research should explore further therelationship between facets of conscientiousness and dif-ferent types of health behaviors (e.g., approach versusavoidance; prevention versus detection).
More recent work by Roberts et al. [21] offers analternative conceptualization of the underlying structure ofconscientiousness. These researchers performed a factoranalysis of conscientiousness-related scales drawn fromseven major personality inventories and revealed sixunderlying factors: industriousness (e.g., achievement striv-ing, self-efficacy, self-discipline), order (orderliness, organ-ised, perfectionism), self-control (e.g., cautiousness;impulse control), responsibility (e.g., responsibility;achievement via conformance, avoids trouble), traditional-ism (e.g., comply with rules, customs, norms, etc.), andvirtue (e.g., honesty, morality). Moreover, in their relatedmeta-analysis of the leading behavioral contributors to theconscientiousness–mortality relationship, Bogg and Roberts[1] have argued that the facets of responsibility and self-control are the most important in relation to healthbehaviors with traditionalism being one of the bestpredictors of risky health behaviors (e.g., risky driving,drug use, violence). They concluded also that order andindustriousness have relatively weak relationships with
Table 4 Effects of conscien-tiousness and its facets onwithin-person daily hassles
MRCM multivariate random co-efficient modeling, Ach/strivingachievement striving, Symbolhierarchical multivariate linearmodeling symbol, CI confidenceintervals
MRCM effect Symbol Coeff SE p 95% Cis
Intercept
Daily hassles β 00 0.950 0.036 <0.0001 0.879, 1.020
Cross-level effect of total conscientiousness
Total conscientiousness–daily hassles β 01 −0.005 0.018 0.791 −0.040, 0.030Intercept
Daily hassles β 00 0.950 0.036 <0.0001 0.879, 1.020
Cross-level effects of achievement striving
Achievement striving–daily hassles β 01 0.084 0.061 0.164 −0.033, 0.201Intercept
Daily hassles β 00 0.955 0.036 <0.0001 0.883, 1.024
Cross-level effects of self-discipline
Self-discipline–daily hassles β 01 −0.125 0.046 0.008 −0.214, -0.033Intercept
Daily hassles β 00 0.950 0.036 <0.0001 0.879, 1.020
Cross-level effects of cautiousness
Cautiousness–daily hassles β 01 0.035 0.053 0.501 −0.067, 0.137Intercept
Daily hassles β 00 0.950 0.036 <0.0001 0.879, 1.020
Cross-level effects of self-efficacy
Self-efficacy–daily hassles β 01 −0.048 0.069 0.484 −0.181, 0.085Intercept
Daily hassles β 00 0.950 0.037 <0.0001 0.879, 1.020
Cross-level effects of order
Order–daily hassles β 01 −0.076 0.043 0.081 −0.159, 0.009
ann. behav. med. (2009) 37:184–196 193

health behaviors. However, when only the nonrisky healthbehaviors are considered (i.e., physical activity, alcohol use,unhealthy eating, tobacco use), using data from their meta-analysis (cf., Bogg & Roberts [1]; p. 909), traditionalism,industriousness, and self-control emerge as having thestrongest relations (respectively) with health behaviors. Interms of the current study, our findings are broadlyconsistent with these data in that our measures ofindustriousness (i.e., achievement striving, self-discipline,self-efficacy) and self-control (i.e., cautiousness) werefound to be associated with a number of the healthbehaviors (albeit, not always in the predicted direction).Traditionalism was not assessed in the current study andthis may explain why we did not observe any directassociations between conscientiousness, alcohol use, andexercise, both of which have previously been found to berelated to this facet of conscientiousness [1]. This possibil-ity notwithstanding, it is incumbent on future researchers toinvestigate the extent to which properties of risky versusnonrisky health behaviors may moderate the conscientious-ness–health behavior relationship. In addition, futureresearch might usefully examine how the facets ofconscientiousness influence self-regulation processes (cf.,[14]). Do individuals high on conscientiousness utilizedifferent strategies to enact their health behavior intentions?For example, do conscientious individuals formulate clearerplans or simply try harder?
A number of factors may account for the counterintuitivefindings in relation to smoking and caffeine intake. First, asoutlined earlier, previous research has been overly relianton cross-sectional snapshot methodologies that may havedistorted the relationship between conscientiousness andspecific health behaviors. Second, a large number of earlierstudies have been restricted to examining a small number ofhealth behaviors thus providing a limited view of theconscientiousness–health behavior relationship. Third,existing research may be confounded by the ecologicalfallacy, drawing within-person inferences from across-persons associations, and as such the current study designmay have uncovered the “true” relationship betweenconscientiousness, caffeine intake, and smoking (in smok-ers). Indeed, it has been demonstrated previously thatbetween-person and across-person correlations can differmarkedly in direction as well as in magnitude (cf., [15]).Moreover, it is entirely plausible that conscientious indi-viduals consume more caffeinated drinks and smoke morecigarettes (if smokers) as a by-product of their high levelsof motivation to achieve daily goals and targets. Forexample, evidence exists that caffeine consumption canconfer cognitive benefits on performance and mood [40].Similarly, nicotine intake has been found to enhancecognitive functioning and performance in current smokers(but not in nonsmokers or never smokers) [41]. Therefore,
it is possible that individuals high on conscientiousness aremore sensitive to these benefits and utilize caffeine andnicotine as strategies to facilitate achievement and focus atwork. Moreover, researchers should also be cognizant ofthe possibility that particular health behaviors (e.g.,moderate alcohol use) may have health benefits forparticular illness processes (e.g., cardiovascular disease)and harmful effects for other diseases (e.g., cancer). Futureresearch ought to explore further the relationship betweenconscientiousness and multiple health behaviors using acombination of repeated daily diary designs and carefullycontrolled laboratory investigations in order to uncover theprecise nature of these relationships.
We also found some evidence that the facets of consci-entiousness moderated the effects of daily hassles onsmoking, exercise, and vegetable intake each day. Aspredicted, individuals with lower levels of self-efficacy werefound to consume fewer vegetables on days when theyexperienced daily hassles. Moreover, individuals who werehigher on order were found to be more likely to exercise onstressful days. These findings are consistent with the stressbuffering hypothesis and indicate that (aspects of) conscien-tiousness may exert part of its positive influence on healthindirectly by modifying the effects of daily hassles such thatconscientious individuals respond to stress by engaging inmore health-enhancing behaviors. As outlined earlier, highconscientious individuals have been found to be more likelyto use problem-focused coping and to be better organized tomeet situational demands; therefore, they may be lessvulnerable to stress-induced changes in health behaviors(cf., [6, 7]). In addition, the latter finding is particularlyimportant as it is, to the best of our knowledge, the firstreported observation that individuals who are high onparticular facets of conscientiousness are likely to engage inphysical exercise as a way of actively coping with dailystressors.
Finally, we found some evidence that the beneficialeffects of conscientiousness on health status may operatethrough the reduced exposure to daily hassles in individualshigher in conscientiousness compared to those with lowerlevels. Specifically, we found that individuals high in theself-discipline facet reported experiencing a lower numberof daily hassles and individuals high in the order facet alsoreported less hassles (although the latter finding was notstatistically significant). It is well established that psycho-logical stress can affect health directly through autonomicand neuroendocrine responses as well as indirectly (e.g., [8,42, 43]). One of the central pathways through which stresscan exert its negative effects is through the hypothalamic–pituitary–adrenal (HPA) axis [8]. If the HPA axis isrepeatedly activated, the immune, cardiovascular, and theendocrine systems are potentially exposed to excessivewear and tear [8]. Over time, such repetitive activation may
194 ann. behav. med. (2009) 37:184–196

contribute to future ill-health by placing excessive pressureon various bodily systems. Therefore, it is important forfuture researchers to explore this pathway in more detail asit remains a possibility that the impact of conscientiousnesson stress-related outcomes may become clearer after alonger and more sustained period of exposure (e.g., overyears).
A number of limitations of the current research brieflyrequire comment. The effects reported may be consideredsmall, but, within the context of other well-establishedeffect sizes within behavioral medicine, these effects arecomparable (e.g., Rutledge and Loh [44] have noted thatthe relationship between aspirin and heart disease is small).Moreover, these small effects are also likely to reflect thatthe relationships between personality, daily hassles, andhealth behaviors are influenced by a large number of othervariables. We also acknowledge that our measures of healthbehaviors are self-reported and more detailed assessmentswould have improved the design. However, given that itwas important to measure changes in daily hassles andhealth behaviors over a meaningful period of time (e.g.,28 days), we felt that lengthy daily diary assessments wouldhave been burdensome for the participants and may haveinfluenced participants’ normal health behaviors. Moreover,similar diary methods assessing different aspects of healthbehaviors have been found to be reliable and valid [16].
We are also mindful that the current study design usedpaper and pencil daily diaries and some participants mayhave backfilled their entries and as a result may not havebeen fully compliant with the study protocol. Anotherpossible bias is that those high in conscientiousness may bemore likely to be more accurate and compliant in their datarecording. Our data did not allow us to examine if thosehigh in conscientiousness are more compliant with diaryprotocols—and this is something that future researchshould look to examine. However, even if this were thecase, the increased accuracy would not necessarily meanthat this would lead to specific associations betweenhassles, health behavior, and its moderation by conscien-tiousness. Therefore, taking these two issues together,future research ought to explore utilizing more sophisticat-ed assessment techniques and consider using electronicevent-contingent designs which will ensure that robustcompliance data are collected and allow for the carefulinvestigation of causal relationships (see [45]). Lastly, werecognize that we did not include measures of each of thefacets included in the conceptualization of Roberts et al.[21] of the underlying structure of conscientiousness.Therefore, future research ought to include detailed andcomprehensive measures of all facets including responsi-bility, traditionalism, and virtue.
To conclude, these findings suggest that conscientious-ness may influence future health status via multiple path-
ways: directly through facilitating performance of importanthealth behaviors and/or reducing exposure to daily stressorsand/or indirectly by buffering the negative effects of stresson health behaviors and in some cases promoting health-enhancing behaviors such as exercise.
Acknowledgment This research was funded by a grant awarded toO’Connor, Conner & Jones from the UK Economic and SocialResearch Council (award no. RES-000-23-0087).
References
1. Bogg T, Roberts BW. Conscientiousness and health-relatedbehaviors: A meta-analysis of leading behavioral contributors tomortality. Psychol Bull. 2004; 130: 887–919.
2. Friedman HS, Tucker JS, Tomlinson-Keasey C, Schwartz JE,Wingard DL, Criqui MH. Does childhood personality predictlongevity? J Pers Soc Psychol. 1993; 65: 176–185.
3. Friedman HS, Tucker JS, Schwartz JE, et al. Childhoodconscientiousness and longevity: Health behaviors and cause ofdeath. J Pers Soc Psychol. 1995; 68: 696–703.
4. Hampson SE, Goldberg LR, Vogt TM, Dubanoski JP. Forty yearson: Teachers’ assessments of children’s personality traits predictself-reported health behaviors and outcomes at midlife. HealthPsychol. 2006; 25: 57–64.
5. Hampson SE, Goldberg LR, Vogt TM, Dubanoski JP. Mecha-nisms by which childhood personality traits influence adult healthstatus: Educational attainment and healthy behaviors. HealthPsychol. 2007; 26: 121–125.
6. O’Connor DB, O’Connor RC. Perceived changes in food intake inresponse to stress: The role of conscientiousness. Stress Health.2004; 20: 279–291.
7. Penley JA, Tomaka J. Associations among the Big Five,emotional responses, and coping with acute stress. Pers IndividDiff. 2002; 32: 1215–1228.
8. McEwen BS. Protective and damaging effects of stress mediators.N Engl J Med. 1998; 338: 171–179.
9. Martin LR, Friedman HS, Schwartz JE. Personality and mortalityrisk across the life span: the importance of conscientiousness as abiopsychosocial attribute. Health Psychol. 2007; 26: 428–436.
10. Norman P, Conner M. Predicting and changing health behaviour:Future directions. In: Conner M, Norman P, eds. Predicting healthbehaviour: Research and practice with social cognition models.2nd ed. Maidenhead: Open University Press; 2005: 324–371.
11. Conner M, Rodgers W, Murray T. Conscientiousness and theintention–behavior relationship: Predicting exercise behavior. JSport Exer Psychol. 2007; 29: 518–533.
12. Rhodes RE, Courneya KS, Hayduk LA. Does personalitymoderate the theory of planned behavior in the exercise domain?J Sport Exer Psychol. 2002; 24: 120–132.
13. Rhodes RE, Courneya KS, Jones LW. The theory of plannedbehavior and lower-order personality traits: Interaction effects inthe exercise domain. Pers Individ Diff. 2005; 38: 251–265.
14. Conner M, Grogan S, Fry G, Gough B, Higgins AR. Direct,mediated and moderated impacts of personality variables onsmoking initiation in adolescents. Psychol Health. 2009; in press.
15. Affleck G, Zautra A, Tennen H, Armeli S. Multi-level dailyprocess designs for consulting and clinical psychology: A prefacefor the perplexed. J Consult Clin Psychol. 1999; 67: 746–754.
16. Conner M, Fitter M, Fletcher W. Stress and snacking: A diarystudy of daily hassles and between meal snacking. PsycholHealth. 1999; 14: 51–63.
ann. behav. med. (2009) 37:184–196 195
17. Delongis A, Coyne JC, Dakof G, Folkman S, Lazarus RS.Relationship of daily hassles, uplifts and minor life events tohealth status. Health Psychol. 1982; 1: 119–136.
18. Jones F, O’Connor DB, Conner M, McMillan B, Ferguson E.Impact of daily mood, work hours, and iso-strain variables on self-reported health behaviors. J Appl Psychol. 2007; 92: 1731–1740.
19. O’Connor DB, Jones F, Conner M, McMillan B, Ferguson E.Effects of daily hassles and eating style on eating behaviour.Health Psychol. 2008; 27: S20–S31.
20. Newman E, O’Connor DB, Conner M. Daily hassles and eatingbehaviour: The role of cortisol reactivity. Psychoneuroendocrinol-ogy. 2007; 32: 125–132.
21. Roberts BW, Chernyshenko OS, Stark S, Goldberg LR. Thestructure of conscientiousness: An empirical investigation basedon seven major personality questionnaires. Personnel Psychol.2005; 58: 103–139.
22. Roberts BW, Bogg T, Walton KE, Chernyshenko OS, Stark SE. Alexical investigation of the lower-order structure of conscientious-ness. J Res Pers. 2004; 38: 164–178.
23. Costa PT, McCrae RR, Dye DA. Facet scales for agreeablenessand conscientiousness: A revision of the NEO PersonalityInventory. Pers Individ Diff. 1991; 12: 887–989.
24. Goldberg LR. A broad-bandwidth, public domain, personalityinventory measuring the lower-level facets of several five-factormodels. In: Mervielde I, Deary I, De Fruyt F, Ostendorf F, eds.Personality psychology in Europe, vol. 7. Tilburg: TilburgUniversity Press; 1999: 7–28.
25. Ferguson E, Cassaday HJ, Bibby P. Odors and sounds as triggersfor medically unexplained symptoms: A fixed occasion diary studyof in Gulf War veterans. Ann Behav Med. 2004; 27: 205–214.
26. Nezlek JB. Multilevel random coefficient analyses of event- andinterval contingent data in social and personality psychologyresearch. Pers Soc Psychol Bull. 2001; 27: 771–785.
27. Green AS, Rafaeli E, Bolger N, Shrout PE, Reis HT. Paper orplastic? Data equivalence in paper and electronic diaries. PsycholMeth. 2006; 11: 87–105.
28. Tennen H, Affleck G, Coyne JC, Larsen RJ, DeLongis A. Paper orplastic in daily diary research: Comment on Green, Rafaeli, Bolger,Shrout, and Reis (2006). Psychol Meth. 2006; 11: 112–118.
29. McCance RA, Widdowson EM. The composition of foods.Letchworth: The Royal Society of Chemistry; 1991.
30. Craig CL, Marshall AL, Sjostrom M, et al. International physicalactivity questionnaire: 12-country reliability and validity. Med SciSports Exer. 2003; 35: 1381–1395.
31. Costa PT, McCrae RR. The NEO personality inventory manual.Odessa: Psychological Assessment Resources; 1985.
32. Mroczek DK, Spiro A. Personality change influences mortality inolder men. Psychol Sci. 2007; 18: 371–376.
33. Raudenbush S, Bryk A, Cheong YF, Congdon R. HLM 6:Hierarchical linear and nonlinear modeling. Lincolnwood: Scien-tific Software International; 2004.
34. Snijders T, Bosker R. Multilevel analysis. London: Sage; 1999.35. Preacher KJ, Curran PJ, Bauer DJ. Computational tools for
probing interactions in multiple linear regression, multilevelmodelling, and latent curve analysis. J Educ Behav Statistics.2006; 31: 437–448.
36. Gibson NM, Olejnik S. Treatment of missing data at the secondlevel of hierarchical linear models. Educ Psychol Measurement.2003; 63: 204–238.
37. Little RJA, Rubin DA. Statistical analysis with missing data. NewYork: Wiley; 1987.
38. Jaccard J. ZumaStat statistical methods. Miami: Applied ScientificAnalysis; 2006. (www.zumastat.com).
39. Schafer JL, Graham JW. Missing data: Our view of the stat of theart. Psychol Meth. 2002; 7: 147–177.
40. Smith HJ, Rogers PJ. Effects of low doses of caffeine on cognitiveperformance, mood and thirst in low and higher caffeineconsumers. Psychopharmacology. 2000; 152: 167–173.
41. Newhouse PA, Potter A, Singh A. Effects of nicotinic stimulationon cognitive performance. Curr Opin Psychopharmacol. 2004; 4:36–46.
42. O’Connor DB, O'Connor RC, White BL, Bundred PE. Jobstrain and ambulatory blood pressure in British generalpractitioners: A preliminary study. Psychol Health Med. 2000;5: 241–250.
43. Jones F, Bright J. Stress: Myth, theory and research. London:Prentice Hall; 2001.
44. Rutledge T, Loh C. Effect sizes and statistical testing in thedetermination of clinical significance on behavioral medicineresearch. Ann Behav Med. 2004; 27: 138–145.
45. O’Connor DB, Ferguson E. Studying the natural history ofbehaviour. Psychologist. 2008; 21: 1034–1036.
196 ann. behav. med. (2009) 37:184–196





























