Embed Size (px)
Citation preview
MCSP India
Program Year 5 Quarter 2 Report JANUARY – MARCH 2019
Submitted on: 27 May 2019 Submitted to: United States Agency for International Development Cooperative Agreement #AID-OAA-A-14-00028 Submitted by: Maternal and Child Survival Program
2
INTRODUCTION The Maternal and Child Survival Program (MCSP) is a global U.S. Agency for International Development (USAID) cooperative agreement to introduce and support high-impact health interventions in 27 priority countries with the ultimate goal of preventing child and maternal deaths. MCSP engages governments, policymakers, private sector leaders, health care providers, civil society, faith-based organizations and communities in adopting and accelerating proven approaches to address the major causes of maternal, newborn and child mortality such as postpartum hemorrhage, birth asphyxia and diarrhea, respectively, and improve the quality of health services from household to hospital. MCSP’s predecessor, The Maternal Child Health Integrated Program (MCHIP) worked in India for its entirety (2009-2014), supporting the Ministry of Health and Family Welfare (MoHFW) and the National Health Mission (NHM). The program worked with a variety of partners and states to expand access to family planning, improve the quality of midwifery and nursing pre-service education, improve the quality of newborn health care and expand routine immunization coverage. Current MCSP Program Areas in India: − Family Planning program (FP) − Technical Support Unit-Adolescent Health (TSU-AH) − Human Resources for Health- Health & Wellness
Centers (HRH-HWC) Family Planning: In India, the Family Planning (FP) program under the MCSP (MCSP-FP) is working to expand access to high-quality family planning services and contribute to India’s FP2020 commitments. The program has successfully advocated for introduction of newer contraceptives in Government of India’s FP basket. The program is also undertaking strategic demonstration at 52 selected health facilities for the introduction of new contraceptives through public health system. Built on the tenets of informed choice, respectful care, gender- sensitivity and community participation in family planning services, MCSP is advocating for the adoption of evidence-based approaches, strategies, interventions and solutions to strengthen the delivery of quality contraceptive services. MCSP is strengthening the ecosystem for delivering quality services by setting up quality counseling services and counseling corners, expanding providers’ as well as trainers’ pool, streamlining facility level management processes, strengthening facility, district and state quality assurance mechanisms, strengthening community linkages and addressing the system level gaps. Technical Support Unit-Adolescent Health (TSU-AH): Technical Support Unit- Adolescent Health (TSU-AH) under the MCSP provides catalytic support to the National and State Governments in effective implementation of the National Adolescent Health Programme (Rashtriya Kishor Swasthya Karyakram) as well as the School Health Program under ‘Ayushman Bharat’. The TSU-AH is also involved in strengthening inter-sectoral co-ordination and convergence between ministries and other agencies working on adolescent health issues, for better synergies. Human Resources for Health- Health & Wellness Centers (HRH-HWC)
3
In India, MCSP is providing technical assistance for strengthening delivery of RMNCH+A and Comprehensive Primary Health Care (CPHC) services and creation of sustainable training ecosystems in five high focus states (Assam, Chhattisgarh, Jharkhand, Madhya Pradesh and Odisha) and seven north-eastern states (Arunachal Pradesh, Manipur, Meghalaya, Mizoram, Nagaland, Sikkim and Tripura). The project includes developing of roadmaps, operational plans and financial proposals for setting up of HWCs in intervention states. Additionally, the project will also build the institutional capacity of the intervention states to train Mid-level Health Providers (MLHPs) in six-month certificate course on community health by establishing the required number of training sites (Program Study Centers) and creation of a pool of trainers. About this report This report is a narration of MCSP activity updates for PY5Q2 (January – March 2019) and covers the progress on the following program components: • Family Planning • Technical Support Unit- Adolescent Health • Human Resources for Health - Health & Wellness Centers

4
1.0 FAMILY PLANNING GOAL: CONTRIBUTE TO UNIVERSAL ACCESS TO QUALITY CONTRACEPTIVE SERVICES IN INDIA; THUS CONTRIBUTING TO THE FP 2020 COMMITMENTS
1.1 OBJECTIVE 1: TO PROMOTE THE EXPANSION OF THE CURRENT BASKET OF CONTRACEPTIVES AVAILABLE IN INDIA BY ADVOCATING FOR (AND DEMONSTRATING) THE INCLUSION OF MORE PROVEN MODERN CONTRACEPTIVE OPTIONS I.E. PROGESTERONE-ONLY PILL (POP) AND CENTCHROMAN.
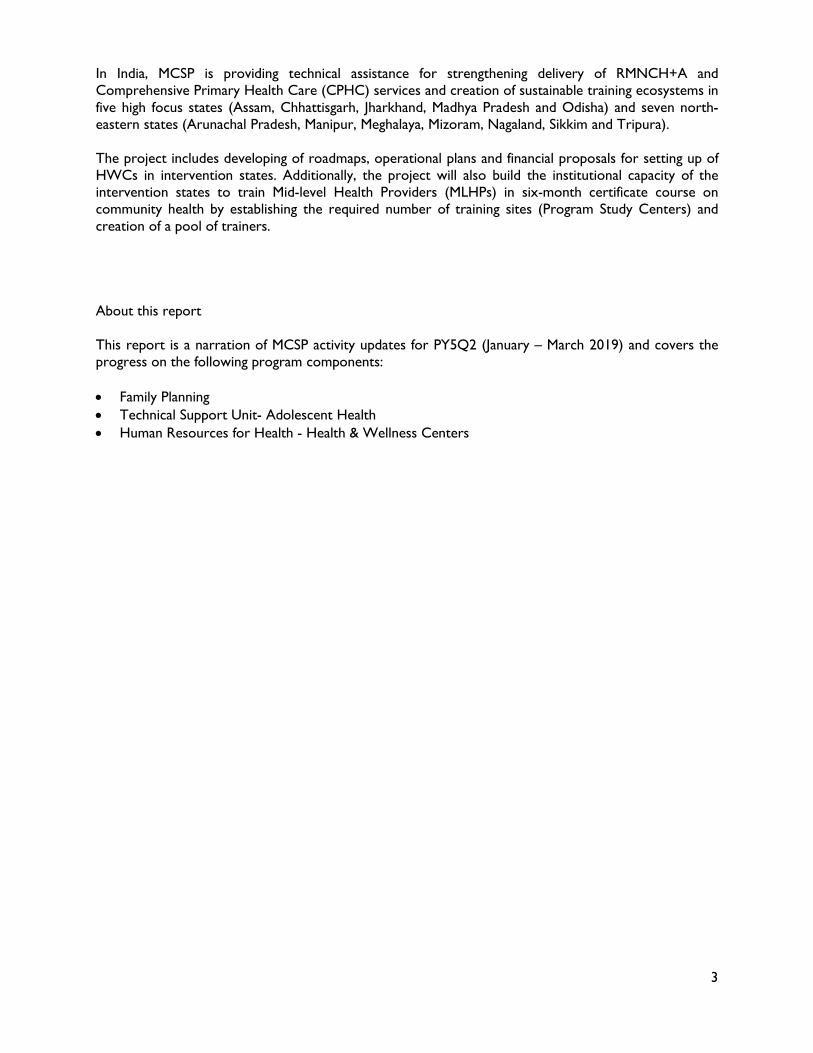
MCSP continues to maintain POP supplies at the 52 focus facilities beyond the 18-month demonstration period that ended on October 31, 2018. MCSP has initiated advocacy with the respective state governments of the five focus states for procurement of POP through state resources and its’ addition in the contraceptive basket at present public health facilities. Government of Chhattisgarh has included and budgeted for POP in the State’s Essential Drug List to enable continuation of service provision for POP at the current facility in Bilaspur. The program has been, and looks forward to continue sharing the updates with India Mission in this regard. In PY5Q2, MCSP focused on the strengthening the service provision further for the two new methods (POP and Centchroman) at 52 focus facilities (FF) across five states: Assam, Chhattisgarh, Maharashtra, Odisha and Telangana, increasing the number of women choosing a postpartum family planning (PPFP) method to 22%, as compared to 10% at the beginning of the demonstration (baseline). (Graph 1)
Objective 1: National level, 5 States: Odisha, Chhattisgarh, Maharashtra, Telangana, and Assam, 5 Districts, 52 facilities Objective 2: National level, 5 States: Odisha, Chhattisgarh, Maharashtra, Telangana, and Assam, 17 Districts, 186 facilities
Image 1: POP has been included and budgeted in Chhattisgarh State’s Essential Drug List. (Mubeen Siddiqui/ MCSP India)
5
The introduction of two newer contraceptives in the public sector contraceptive basket created additional PPFP users, rather than replace acceptors of other FP methods, as an increase in uptake of methods like PPIUCD and PPS was also witnessed. (Graph 2)
Since the roll out of POP and Centchroman services in April 2017 at 52 focus facilities (FF), 4,804 and 8,957 women have accepted POP and Centchroman, respectively, as of March 2019. In the reporting quarter, 447 women accepted POP while 1,561 women accepted Centchroman. Overall, 5.4% of total postpartum women delivering at focus facilities between January to March 2019 accepted either POP (2.32%) or Centchroman (3.04%).
90% 83% 78%
10% 17% 22%
0%
20%
40%
60%
80%
100%
120%
Apr'16 - Mar'17(Deliveries=91,550)
Apr'17 - Mar'18(Deliveries=98,491)
Apr'18 - Mar'19(Deliveries=99,680)
Non acceptors Acceptors
90%
83%
78%
8.1%
7.9%
12.3%
0.0%
3.2%
1.5%
2.3%
3.8%
4.4%
2.1%
4.0%
Apr'16 - Mar'17(Deliveries=91,550)
Apr'17 - Mar'18(Deliveries=98,491)
Apr'18 - Mar'19(Deliveries=99,680)
No Method PPIUCD PoP Post-partum PPS Centchroman Post-partum
Graph 1: PPFP Shift (Immediate postpartum)
Graph 2: Comparing the Method Mix across 52 focus facilities
6
Table 1- POP and Centchroman Acceptors by State
State Deliveries
POP Centchroman
Post-partum
Other than Post-
partum
POP Post-
partum
Post-partum
Other than Post-
partum
Centchroman Post-partum
Assam 5642 67 5 1.2% 189 62 3.3% Chhattisgarh 4242 132 6 3.1% 480 163 11.3% Maharashtra 3830 76 2 2.0% 256 154 6.7% Odisha 4650 123 10 2.6% 80 54 1.7% Telangana 6591 21 5 0.3% 113 10 1.7% Total 24955 419 28 1.68% 1118 443 4.48%
Source: Monthly Progress Reports (MPRs) received from January 2019 – March 2019
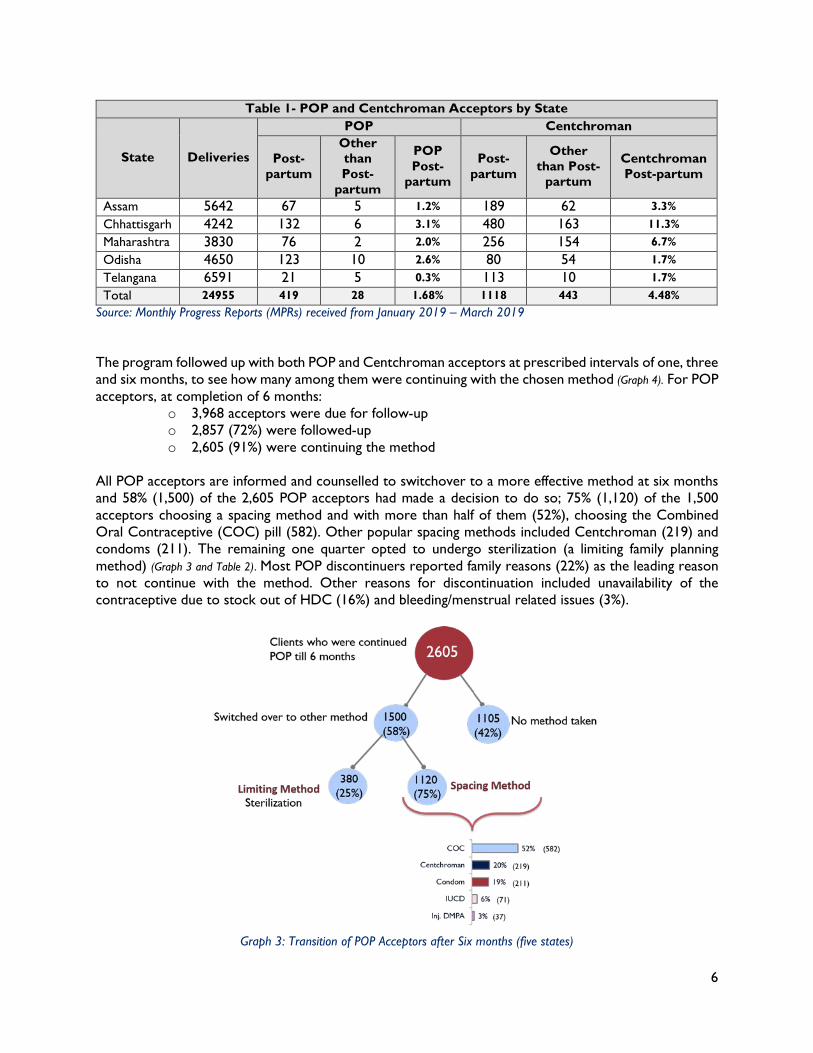
The program followed up with both POP and Centchroman acceptors at prescribed intervals of one, three and six months, to see how many among them were continuing with the chosen method (Graph 4). For POP acceptors, at completion of 6 months:
o 3,968 acceptors were due for follow-up o 2,857 (72%) were followed-up o 2,605 (91%) were continuing the method
All POP acceptors are informed and counselled to switchover to a more effective method at six months and 58% (1,500) of the 2,605 POP acceptors had made a decision to do so; 75% (1,120) of the 1,500 acceptors choosing a spacing method and with more than half of them (52%), choosing the Combined Oral Contraceptive (COC) pill (582). Other popular spacing methods included Centchroman (219) and condoms (211). The remaining one quarter opted to undergo sterilization (a limiting family planning method) (Graph 3 and Table 2). Most POP discontinuers reported family reasons (22%) as the leading reason to not continue with the method. Other reasons for discontinuation included unavailability of the contraceptive due to stock out of HDC (16%) and bleeding/menstrual related issues (3%).
Graph 3: Transition of POP Acceptors after Six months (five states)
7
Table 2 - Transition of POP acceptors after six months
States Continuation1 Mala-N Centch
roman Condom Injectable IUCD Sterilizatio
n No
Method Switchover
% Assam 300 169 76 34 0 21 0 0 100% Chhattisgarh 806 49 78 18 3 17 11 630 83% Maharashtra 362 69 26 54 0 16 13 184 49% Odisha 963 286 22 89 34 15 350 167 29% Telangana 174 9 17 16 0 2 6 124 22% Total 2605 582 219 211 37 71 380 1105 58% Source: Monthly Progress Reports (MPRs) received from April 2017 – March 2019
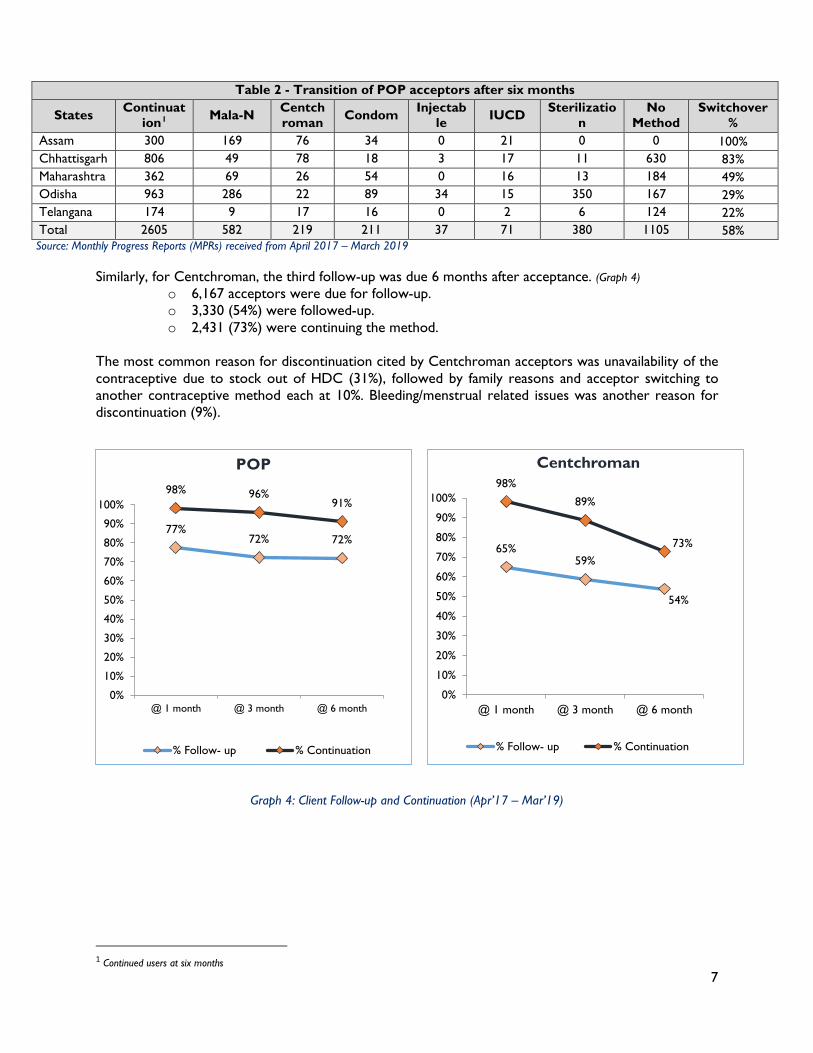
Similarly, for Centchroman, the third follow-up was due 6 months after acceptance. (Graph 4)
o 6,167 acceptors were due for follow-up. o 3,330 (54%) were followed-up. o 2,431 (73%) were continuing the method.
The most common reason for discontinuation cited by Centchroman acceptors was unavailability of the contraceptive due to stock out of HDC (31%), followed by family reasons and acceptor switching to another contraceptive method each at 10%. Bleeding/menstrual related issues was another reason for discontinuation (9%).
Graph 4: Client Follow-up and Continuation (Apr’17 – Mar’19)
1 Continued users at six months
77%72% 72%
98% 96%91%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
@ 1 month @ 3 month @ 6 month
% Follow- up % Continuation
65%59%
54%
98%
89%
73%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
@ 1 month @ 3 month @ 6 month
% Follow- up % Continuation
POP Centchroman
8
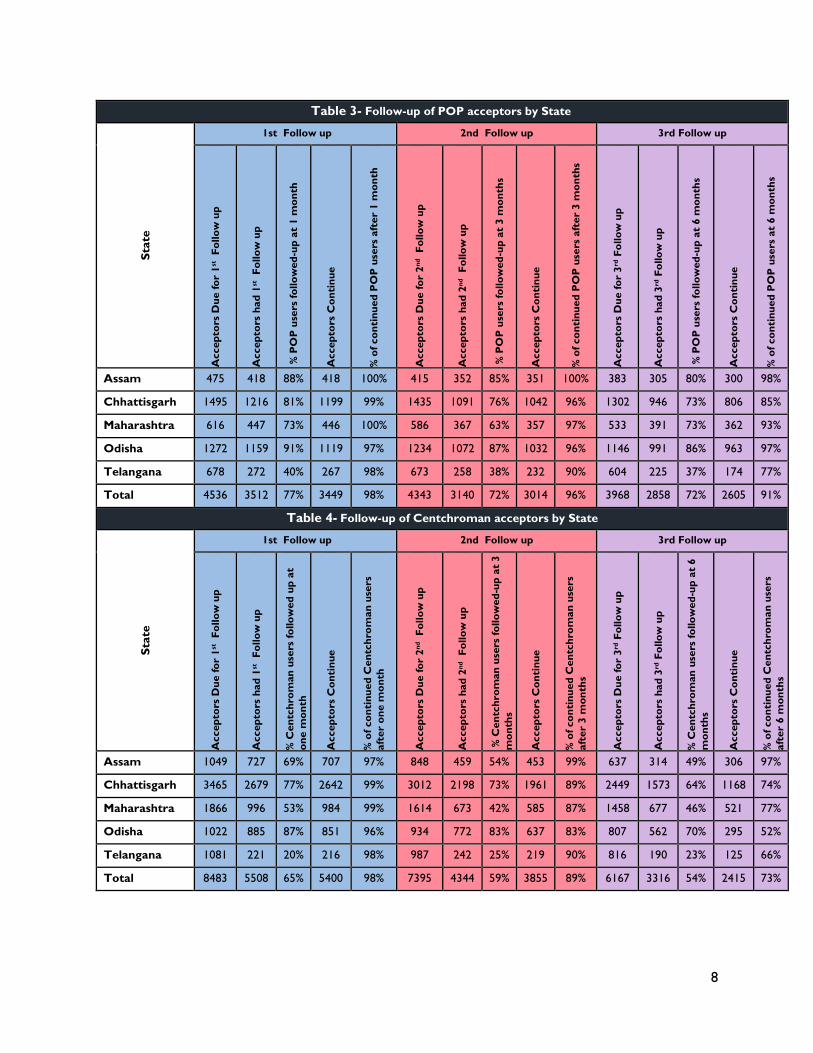
Table 3- Follow-up of POP acceptors by State
Stat
e 1st Follow up 2nd Follow up 3rd Follow up
Acc
epto
rs D
ue fo
r 1st
Fol
low
up
Acc
epto
rs h
ad 1
st F
ollo
w u
p
% P
OP
use
rs fo
llow
ed-u
p at
1 m
onth
Acc
epto
rs C
onti
nue
% o
f con
tinu
ed P
OP
use
rs a
fter
1 m
onth
Acc
epto
rs D
ue fo
r 2nd
Fol
low
up
Acc
epto
rs h
ad 2
nd F
ollo
w u
p
% P
OP
use
rs fo
llow
ed-u
p at
3 m
onth
s
Acc
epto
rs C
onti
nue
% o
f con
tinu
ed P
OP
use
rs a
fter
3 m
onth
s
Acc
epto
rs D
ue fo
r 3rd
Fol
low
up
Acc
epto
rs h
ad 3
rd F
ollo
w u
p
% P
OP
use
rs fo
llow
ed-u
p at
6 m
onth
s
Acc
epto
rs C
onti
nue
% o
f con
tinu
ed P
OP
use
rs a
t 6
mon
ths
Assam 475 418 88% 418 100% 415 352 85% 351 100% 383 305 80% 300 98%
Chhattisgarh 1495 1216 81% 1199 99% 1435 1091 76% 1042 96% 1302 946 73% 806 85%
Maharashtra 616 447 73% 446 100% 586 367 63% 357 97% 533 391 73% 362 93%
Odisha 1272 1159 91% 1119 97% 1234 1072 87% 1032 96% 1146 991 86% 963 97%
Telangana 678 272 40% 267 98% 673 258 38% 232 90% 604 225 37% 174 77%
Total 4536 3512 77% 3449 98% 4343 3140 72% 3014 96% 3968 2858 72% 2605 91%
Table 4- Follow-up of Centchroman acceptors by State
Stat
e
1st Follow up 2nd Follow up 3rd Follow up
Acc
epto
rs D
ue fo
r 1st
Fol
low
up
Acc
epto
rs h
ad 1
st F
ollo
w u
p
% C
entc
hrom
an u
sers
follo
wed
up
at
one
mon
th
Acc
epto
rs C
onti
nue
% o
f con
tinu
ed C
entc
hrom
an u
sers
af
ter
one
mon
th
Acc
epto
rs D
ue fo
r 2nd
Fol
low
up
Acc
epto
rs h
ad 2
nd F
ollo
w u
p
% C
entc
hrom
an u
sers
follo
wed
-up
at 3
m
onth
s
Acc
epto
rs C
onti
nue
% o
f con
tinu
ed C
entc
hrom
an u
sers
af
ter
3 m
onth
s
Acc
epto
rs D
ue fo
r 3rd
Fol
low
up
Acc
epto
rs h
ad 3
rd F
ollo
w u
p
% C
entc
hrom
an u
sers
follo
wed
-up
at 6
m
onth
s
Acc
epto
rs C
onti
nue
% o
f con
tinu
ed C
entc
hrom
an u
sers
af
ter
6 m
onth
s
Assam 1049 727 69% 707 97% 848 459 54% 453 99% 637 314 49% 306 97%
Chhattisgarh 3465 2679 77% 2642 99% 3012 2198 73% 1961 89% 2449 1573 64% 1168 74%
Maharashtra 1866 996 53% 984 99% 1614 673 42% 585 87% 1458 677 46% 521 77%
Odisha 1022 885 87% 851 96% 934 772 83% 637 83% 807 562 70% 295 52%
Telangana 1081 221 20% 216 98% 987 242 25% 219 90% 816 190 23% 125 66%
Total 8483 5508 65% 5400 98% 7395 4344 59% 3855 89% 6167 3316 54% 2415 73%
9
1.2 OBJECTIVE 2: DELIVERY OF QUALITY FAMILY PLANNING SERVICES THROUGH
INNOVATIVE PROCESSES AND TOOLS.
1.2.1 Fixed Day Services (FDS) Strategy
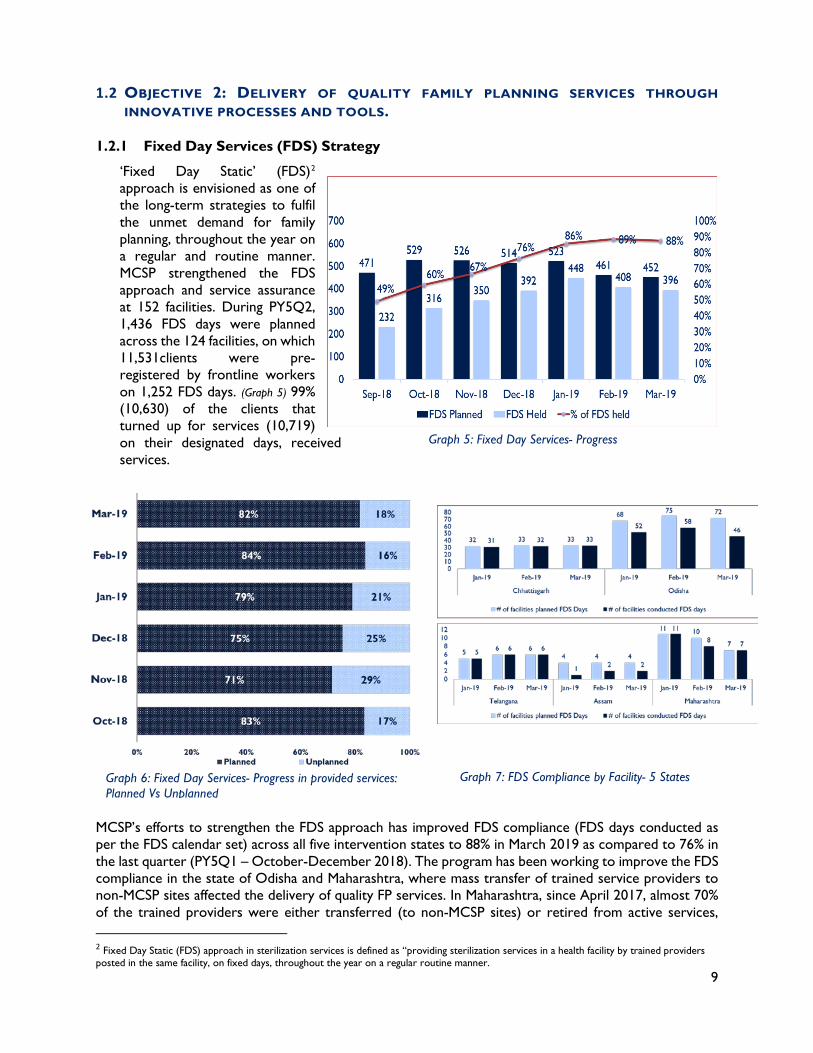
‘Fixed Day Static’ (FDS)2 approach is envisioned as one of the long-term strategies to fulfil the unmet demand for family planning, throughout the year on a regular and routine manner. MCSP strengthened the FDS
approach and service assurance at 152 facilities. During PY5Q2, 1,436 FDS days were planned across the 124 facilities, on which 11,531clients were pre-registered by frontline workers on 1,252 FDS days. (Graph 5) 99% (10,630) of the clients that turned up for services (10,719) on their designated days, received services.
MCSP’s efforts to strengthen the FDS approach has improved FDS compliance (FDS days conducted as per the FDS calendar set) across all five intervention states to 88% in March 2019 as compared to 76% in the last quarter (PY5Q1 – October-December 2018). The program has been working to improve the FDS compliance in the state of Odisha and Maharashtra, where mass transfer of trained service providers to non-MCSP sites affected the delivery of quality FP services. In Maharashtra, since April 2017, almost 70% of the trained providers were either transferred (to non-MCSP sites) or retired from active services, 2 Fixed Day Static (FDS) approach in sterilization services is defined as “providing sterilization services in a health facility by trained providers posted in the same facility, on fixed days, throughout the year on a regular routine manner.
Graph 5: Fixed Day Services- Progress
Graph 6: Fixed Day Services- Progress in provided services: Planned Vs Unplanned
Graph 7: FDS Compliance by Facility- 5 States
10
which affected program implementation. Program efforts have improved the FDS compliance in the state of Maharashtra to 93% in PY5Q2 (January – March 2019) as compared to 55% in December 2018. In Assam, the team’s advocacy efforts resulted in the issue of a letter from Joint Director-Health Services, District Health Society, Nagaon for ensuring quality of FDS services in Nagaon district. 1.2.2 Service Delivery Assessments
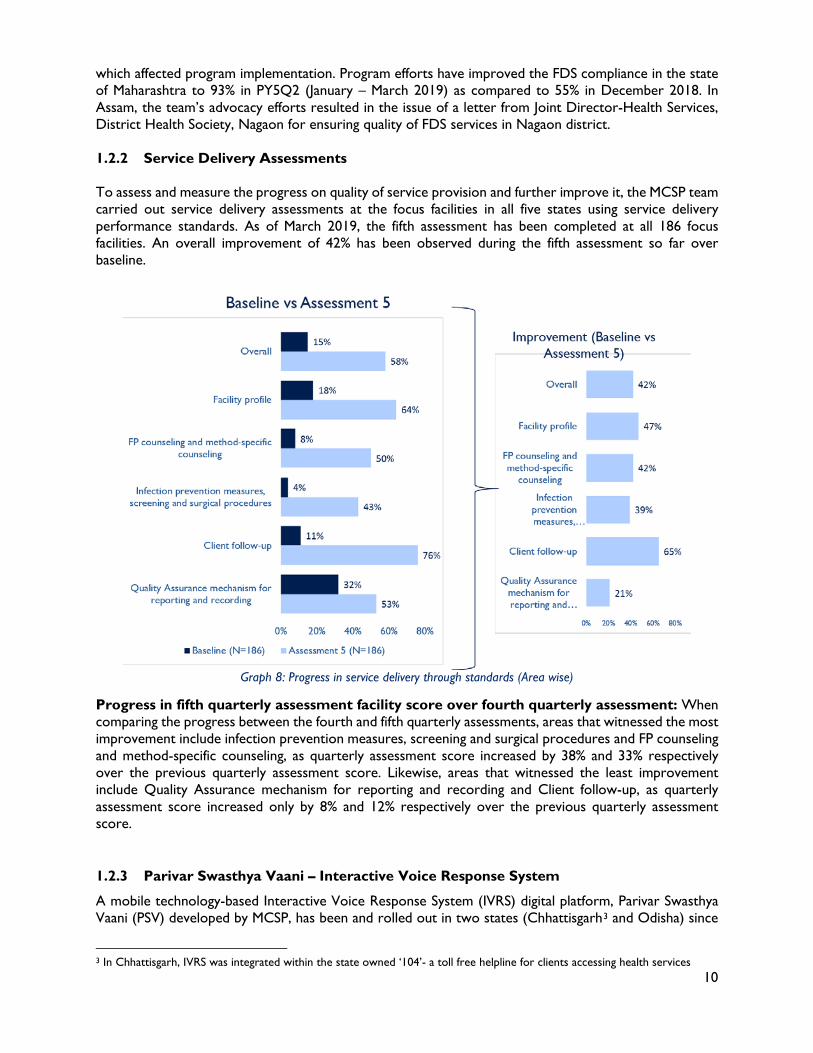
To assess and measure the progress on quality of service provision and further improve it, the MCSP team carried out service delivery assessments at the focus facilities in all five states using service delivery performance standards. As of March 2019, the fifth assessment has been completed at all 186 focus facilities. An overall improvement of 42% has been observed during the fifth assessment so far over baseline.
Graph 8: Progress in service delivery through standards (Area wise)
Progress in fifth quarterly assessment facility score over fourth quarterly assessment: When comparing the progress between the fourth and fifth quarterly assessments, areas that witnessed the most improvement include infection prevention measures, screening and surgical procedures and FP counseling and method-specific counseling, as quarterly assessment score increased by 38% and 33% respectively over the previous quarterly assessment score. Likewise, areas that witnessed the least improvement include Quality Assurance mechanism for reporting and recording and Client follow-up, as quarterly assessment score increased only by 8% and 12% respectively over the previous quarterly assessment score. 1.2.3 Parivar Swasthya Vaani – Interactive Voice Response System
A mobile technology-based Interactive Voice Response System (IVRS) digital platform, Parivar Swasthya Vaani (PSV) developed by MCSP, has been and rolled out in two states (Chhattisgarh3 and Odisha) since
3 In Chhattisgarh, IVRS was integrated within the state owned ‘104’- a toll free helpline for clients accessing health services
11
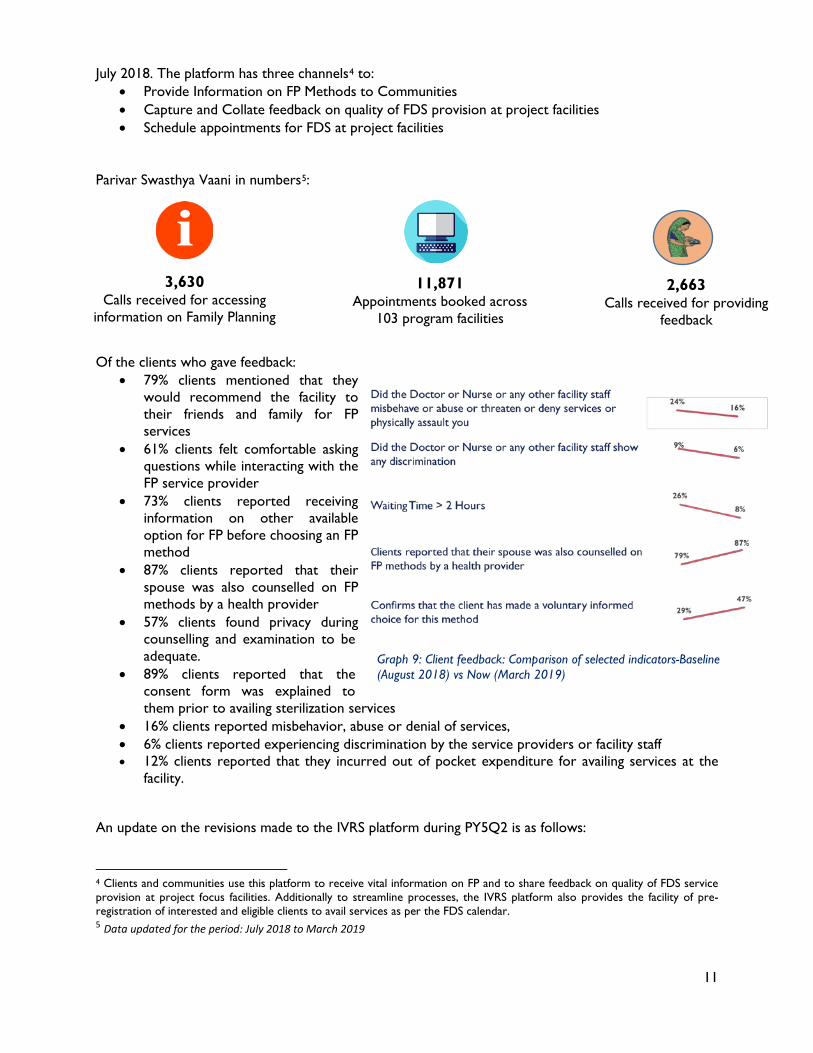
July 2018. The platform has three channels4 to: • Provide Information on FP Methods to Communities • Capture and Collate feedback on quality of FDS provision at project facilities • Schedule appointments for FDS at project facilities
Parivar Swasthya Vaani in numbers5:
Of the clients who gave feedback:
• 79% clients mentioned that they would recommend the facility to their friends and family for FP services
• 61% clients felt comfortable asking questions while interacting with the FP service provider
• 73% clients reported receiving information on other available option for FP before choosing an FP method
• 87% clients reported that their spouse was also counselled on FP methods by a health provider
• 57% clients found privacy during counselling and examination to be adequate.
• 89% clients reported that the consent form was explained to them prior to availing sterilization services
• 16% clients reported misbehavior, abuse or denial of services, • 6% clients reported experiencing discrimination by the service providers or facility staff • 12% clients reported that they incurred out of pocket expenditure for availing services at the
facility. An update on the revisions made to the IVRS platform during PY5Q2 is as follows:
4 Clients and communities use this platform to receive vital information on FP and to share feedback on quality of FDS service provision at project focus facilities. Additionally to streamline processes, the IVRS platform also provides the facility of pre-registration of interested and eligible clients to avail services as per the FDS calendar. 5 Data updated for the period: July 2018 to March 2019
3,630 Calls received for accessing
information on Family Planning
2,663 Calls received for providing
feedback
11,871 Appointments booked across
103 program facilities
Graph 9: Client feedback: Comparison of selected indicators-Baseline (August 2018) vs Now (March 2019)
12
• Revised criteria for registering feedback and information calls: In order to ensure validity of PSV Dashboard Data – an eligibility criterion were included in the system that would register only those callers who have effectively utilized information channel or the feedback channel. In case of the information channel, only those callers who listened to the welcome message, successfully navigated to the information channel and then also successfully navigated to the birth spacing or permanent methods level in the system, are counted as a call to the information channel. Similarly, for the feedback channel, only those callers are counted who listened to the welcome message, successfully navigated to the feedback channel, successfully entered the correct facility code and have listened to at least one survey question.
• Addition of lines: As congestion in lines was observed in the month of February, three additional lines were approved by C3 for addition into the existing system infrastructure. These additional lines have been reported to have eased use of PSV/PSV 104 in the states.
• Monthly Report for Information and Feedback Channels: A monthly reporting format was developed in consultation with technology partner. Additional data that is available on the dashboard was analyzed to seek information on total calls to the system. This would ascertain the percentage calls that pass the eligibility criteria set for the information and feedback channel.
Post MCSP advocacy efforts, Government of Odisha has approved and budgeted funds to the annual NHM Program Implementation Plan (PIP) for IVRS application scale-up across the state's 30 districts. MCSP will provide technical and implementation support to NHM, Odisha in the rollout of the IVRS platform across the current six MCSP focus districts in Odisha. (Annexure 1: Detailed plan of IVRS scale-up in Odisha). The program will continue advocacy with Government of Chhattisgarh for scale-up of the IVRS platform across the state. 1.2.4 Quality Assurance (QA) Structures
District Quality Assurance Committee
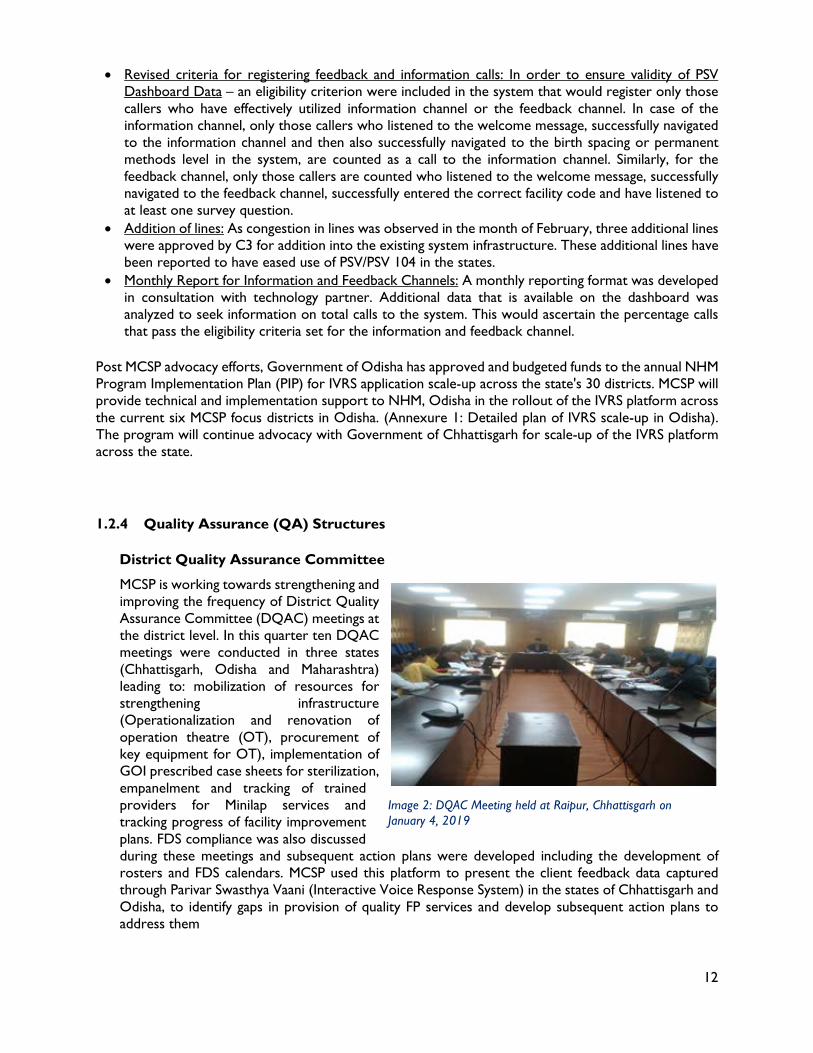
MCSP is working towards strengthening and improving the frequency of District Quality Assurance Committee (DQAC) meetings at the district level. In this quarter ten DQAC meetings were conducted in three states (Chhattisgarh, Odisha and Maharashtra) leading to: mobilization of resources for strengthening infrastructure (Operationalization and renovation of operation theatre (OT), procurement of key equipment for OT), implementation of GOI prescribed case sheets for sterilization, empanelment and tracking of trained providers for Minilap services and tracking progress of facility improvement plans. FDS compliance was also discussed during these meetings and subsequent action plans were developed including the development of rosters and FDS calendars. MCSP used this platform to present the client feedback data captured through Parivar Swasthya Vaani (Interactive Voice Response System) in the states of Chhattisgarh and Odisha, to identify gaps in provision of quality FP services and develop subsequent action plans to address them
Image 2: DQAC Meeting held at Raipur, Chhattisgarh on January 4, 2019
13
In Chhattisgarh, DQAC members visited three program facilities to monitor FDS days in February 2019. The committee members use GoI issued checklist as the monitoring tool (Annexure 6, 17 and 19 from the Standards and Quality Assurance for Sterilization Services)
Table 5: DQAC Meetings held in PY5Q2 State District Date
Chhattisgarh
Raipur 4-January-2019 Janjgir-Champa
5-January-2019
Bilaspur 15-January-2019 Raipur 20-March-2019 Dhamtari 28-March-2019
Maharashtra Nashik 11-January-2019 Nashik 28-February-2019
Odisha Balasore 19-January-2019 Kalahandi 25-January-2019 Balangir 12-March-2019
Quality Circles
MCSP teams in each state regularly follow-up with facilities to organize and conduct Quality Circle (QC) meetings; 163 QC meetings were conducted across four states (Chhattisgarh, Odisha, Assam and Maharashtra) in the reporting quarter. The aim of these meetings is to strengthen monitoring of quality FP services provided at the facility. In addition, MCSP, through its advocacy efforts, rolled out the FP dashboard6 across 93% focus facilities to be presented during these facility level meetings to promote the use of data for better decision making. During these QC meetings, MCSP facilitated discussions on progress on quality of FDS including FDS compliance along with strengthening follow-up of clients accessing FDS services by ensuring timeliness and improving documentation. The importance of strengthening counselling services to improve the uptake of FP services was discussed and engagement of NCD and ICTC counsellors in FP counselling was reemphasized. The meetings also saw discussion on the status of implementation of the FPLMIS software and facility staff was requested to ensure entry and indenting of ground stock in the software in a timely manner. To build the capacity of service providers on newer contraceptives like Centchroman, respective facility staff was re-oriented on Centchroman and on missed pill scenario and were requested to ensure its supply and distribution. Mobilization of providers and development of calendars for PPS services and status of uptake of PPIUCD were also discussed. Facility staff were requested to ensure the timely distribution of sterilization certificates to clients. Proper use and documentation of Client Card, was discussed for strengthening the FDS approach further and facility staff was requested to ensure timely digitization of the Clinical Safety Checklist. Other topics that were focused on during these facility level meetings included FP counselling services and improving infection prevention practices and BMW management. Status of implementation of the IVRS platform was also discussed in the QC meetings in the states of Chhattisgarh and Odisha, along with the need to promote the use of the IVRS platform for pre-registration and having clients share their feedback. The client feedback received via the platform was discussed along with the FP dashboard indicators to assess the gaps in service provision. In Odisha, in the reporting quarter, QC meetings at program
6 The FP Dashboard captures key FP indicators as well as client feedback to enable the facilities to take appropriate corrective actions to improve the Quality of FP service provision.
Image 3: DQAC Meeting at Kalahandi, chaired by the District Collector
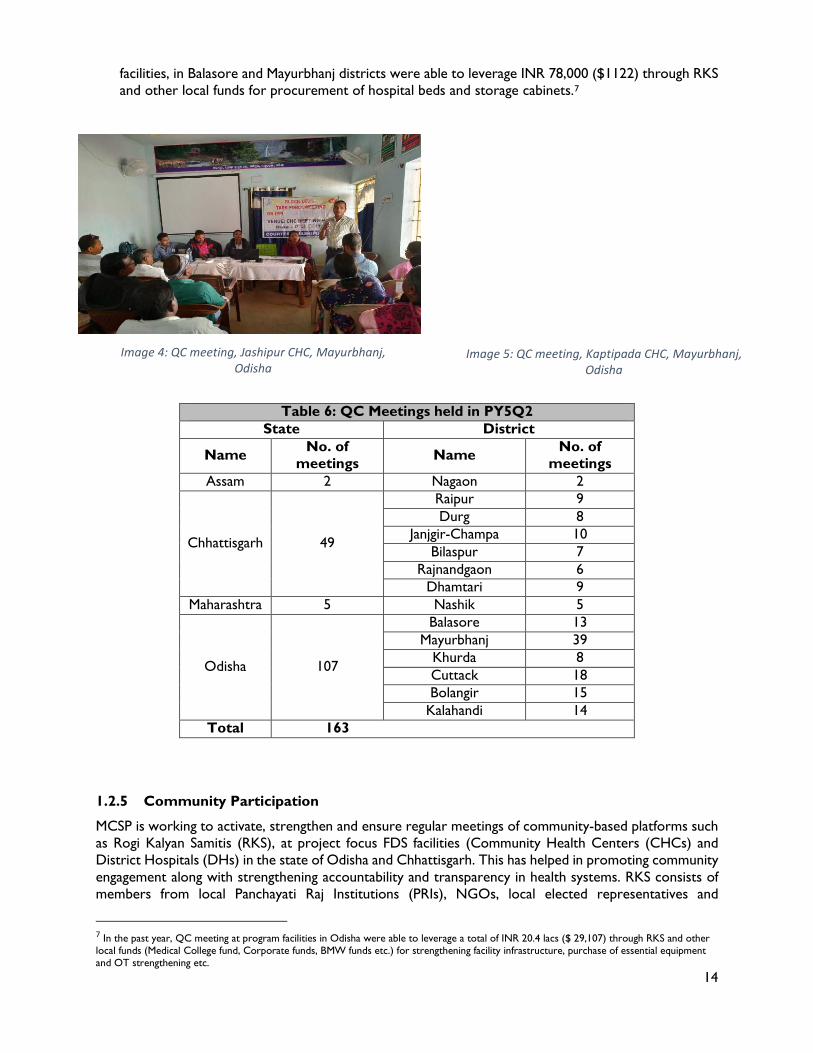
14
facilities, in Balasore and Mayurbhanj districts were able to leverage INR 78,000 ($1122) through RKS and other local funds for procurement of hospital beds and storage cabinets.7
Table 6: QC Meetings held in PY5Q2
State District
Name No. of meetings Name No. of
meetings Assam 2 Nagaon 2
Chhattisgarh 49
Raipur 9 Durg 8
Janjgir-Champa 10 Bilaspur 7
Rajnandgaon 6 Dhamtari 9
Maharashtra 5 Nashik 5
Odisha 107
Balasore 13 Mayurbhanj 39
Khurda 8 Cuttack 18 Bolangir 15
Kalahandi 14 Total 163
1.2.5 Community Participation
MCSP is working to activate, strengthen and ensure regular meetings of community-based platforms such as Rogi Kalyan Samitis (RKS), at project focus FDS facilities (Community Health Centers (CHCs) and District Hospitals (DHs) in the state of Odisha and Chhattisgarh. This has helped in promoting community engagement along with strengthening accountability and transparency in health systems. RKS consists of members from local Panchayati Raj Institutions (PRIs), NGOs, local elected representatives and
7 In the past year, QC meeting at program facilities in Odisha were able to leverage a total of INR 20.4 lacs ($ 29,107) through RKS and other local funds (Medical College fund, Corporate funds, BMW funds etc.) for strengthening facility infrastructure, purchase of essential equipment and OT strengthening etc.
Image 4: QC meeting, Jashipur CHC, Mayurbhanj, Odisha
Image 5: QC meeting, Kaptipada CHC, Mayurbhanj, Odisha
15
government officials and are free to prescribe, generate and use the funds with it as per its best judgement for smooth functioning and maintaining the quality of services. MCSP is working to broaden the scope of these patient welfare societies beyond the management of local funds, to include monitoring quality of services and encouraging community participation in prioritizing local issues. During these meetings, issues such as the performance of and feedback received through the IVRS platform is discussed with the aim of identifying and addressing the gaps in quality and respectful care in FP. During this quarter, 33 RKS meetings were organized across all six intervention districts in Odisha, where the Parivar Swasthya Vaani (PSV) dashboard indicators were shared with a special focus on identifying gaps related to respectful care. The review meetings focused on developing action plans to minimize these identified gaps. Specific issues such as non-availability of beds for post-operative/sterilization clients, display of clients’ rights in prominent places, purchase of emergency drugs, instruments and equipment etc., were focused on. In Chhattisgarh, five RKS (referred to as Jeevan Deep Samiti (JDS) in the state) meetings were held in this quarter across five intervention districts (Raipur, Bilaspur, Janjgir-Champa and Rajnandgaon). The meetings were used to present the client feedback received via the IVRS platform and facility staff were re-oriented on the IVRS platform. QC-RKS Interface meetings
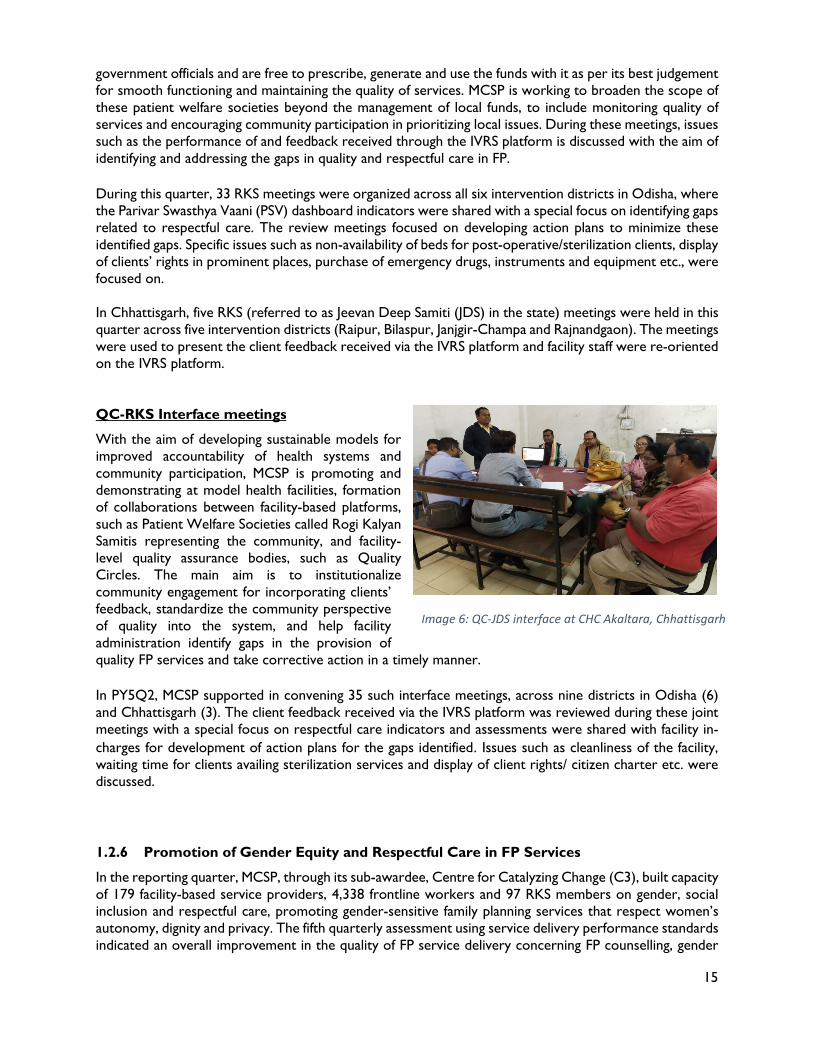
With the aim of developing sustainable models for improved accountability of health systems and community participation, MCSP is promoting and demonstrating at model health facilities, formation of collaborations between facility-based platforms, such as Patient Welfare Societies called Rogi Kalyan Samitis representing the community, and facility-level quality assurance bodies, such as Quality Circles. The main aim is to institutionalize community engagement for incorporating clients’ feedback, standardize the community perspective of quality into the system, and help facility administration identify gaps in the provision of quality FP services and take corrective action in a timely manner. In PY5Q2, MCSP supported in convening 35 such interface meetings, across nine districts in Odisha (6) and Chhattisgarh (3). The client feedback received via the IVRS platform was reviewed during these joint meetings with a special focus on respectful care indicators and assessments were shared with facility in-charges for development of action plans for the gaps identified. Issues such as cleanliness of the facility, waiting time for clients availing sterilization services and display of client rights/ citizen charter etc. were discussed. 1.2.6 Promotion of Gender Equity and Respectful Care in FP Services
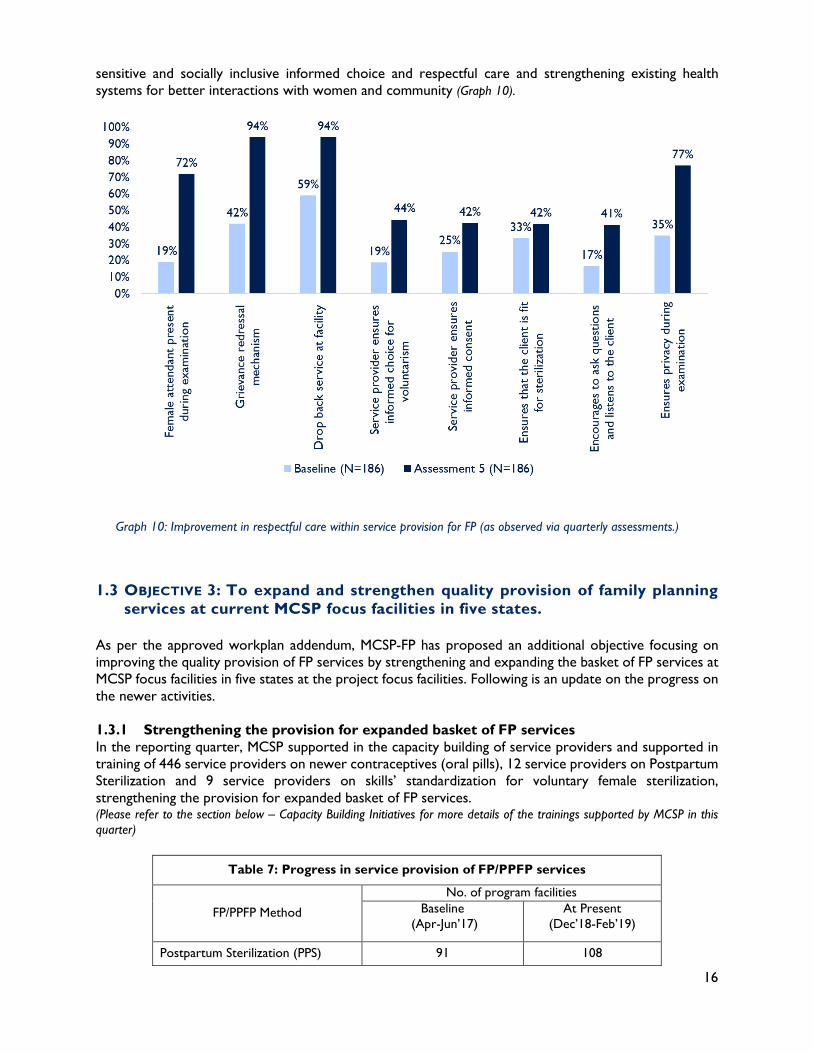
In the reporting quarter, MCSP, through its sub-awardee, Centre for Catalyzing Change (C3), built capacity of 179 facility-based service providers, 4,338 frontline workers and 97 RKS members on gender, social inclusion and respectful care, promoting gender-sensitive family planning services that respect women’s autonomy, dignity and privacy. The fifth quarterly assessment using service delivery performance standards indicated an overall improvement in the quality of FP service delivery concerning FP counselling, gender
Image 6: QC-JDS interface at CHC Akaltara, Chhattisgarh
16
sensitive and socially inclusive informed choice and respectful care and strengthening existing health systems for better interactions with women and community (Graph 10).
1.3 OBJECTIVE 3: To expand and strengthen quality provision of family planning services at current MCSP focus facilities in five states.
As per the approved workplan addendum, MCSP-FP has proposed an additional objective focusing on improving the quality provision of FP services by strengthening and expanding the basket of FP services at MCSP focus facilities in five states at the project focus facilities. Following is an update on the progress on the newer activities. 1.3.1 Strengthening the provision for expanded basket of FP services In the reporting quarter, MCSP supported in the capacity building of service providers and supported in training of 446 service providers on newer contraceptives (oral pills), 12 service providers on Postpartum Sterilization and 9 service providers on skills’ standardization for voluntary female sterilization, strengthening the provision for expanded basket of FP services. (Please refer to the section below – Capacity Building Initiatives for more details of the trainings supported by MCSP in this quarter)
Table 7: Progress in service provision of FP/PPFP services
FP/PPFP Method
No. of program facilities Baseline
(Apr-Jun’17) At Present
(Dec’18-Feb’19)
Postpartum Sterilization (PPS) 91 108
Graph 10: Improvement in respectful care within service provision for FP (as observed via quarterly assessments.)
17
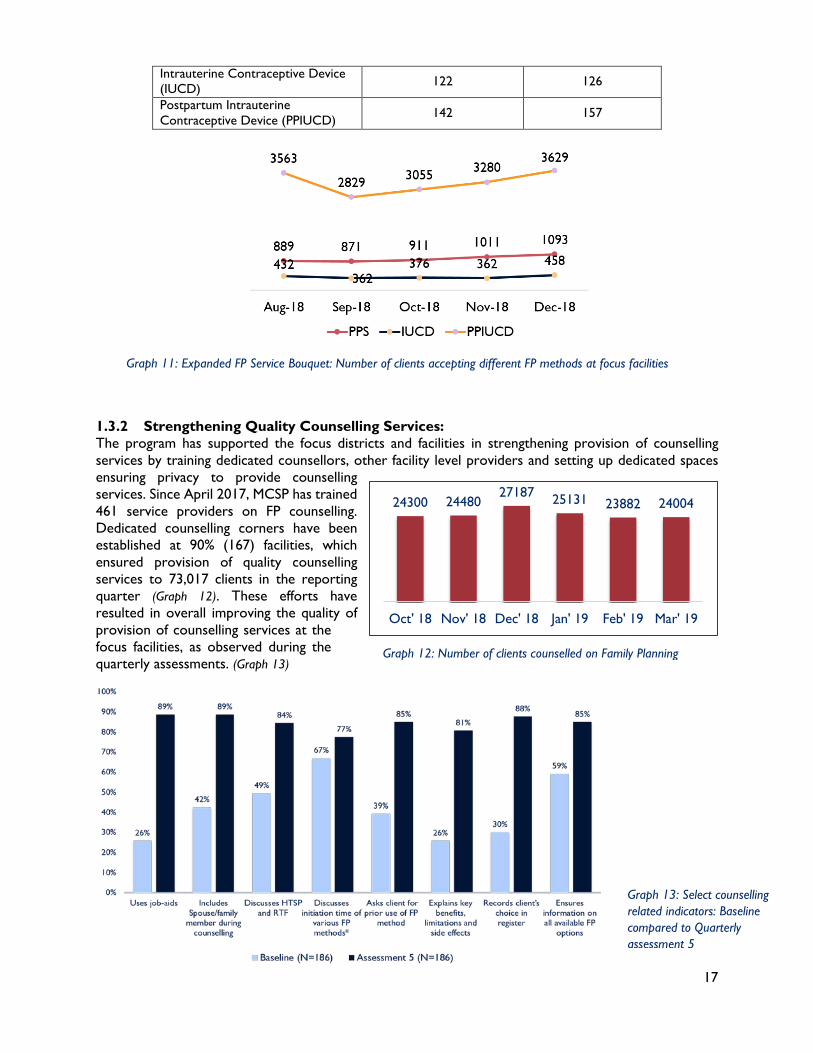
Intrauterine Contraceptive Device (IUCD) 122 126
Postpartum Intrauterine Contraceptive Device (PPIUCD) 142 157
1.3.2 Strengthening Quality Counselling Services: The program has supported the focus districts and facilities in strengthening provision of counselling services by training dedicated counsellors, other facility level providers and setting up dedicated spaces ensuring privacy to provide counselling services. Since April 2017, MCSP has trained 461 service providers on FP counselling. Dedicated counselling corners have been established at 90% (167) facilities, which ensured provision of quality counselling services to 73,017 clients in the reporting quarter (Graph 12). These efforts have resulted in overall improving the quality of provision of counselling services at the focus facilities, as observed during the quarterly assessments. (Graph 13)
Graph 11: Expanded FP Service Bouquet: Number of clients accepting different FP methods at focus facilities
Graph 12: Number of clients counselled on Family Planning
24300 2448027187 25131 23882 24004
Oct' 18 Nov' 18 Dec' 18 Jan' 19 Feb' 19 Mar' 19
Graph 13: Select counselling related indicators: Baseline compared to Quarterly assessment 5
18
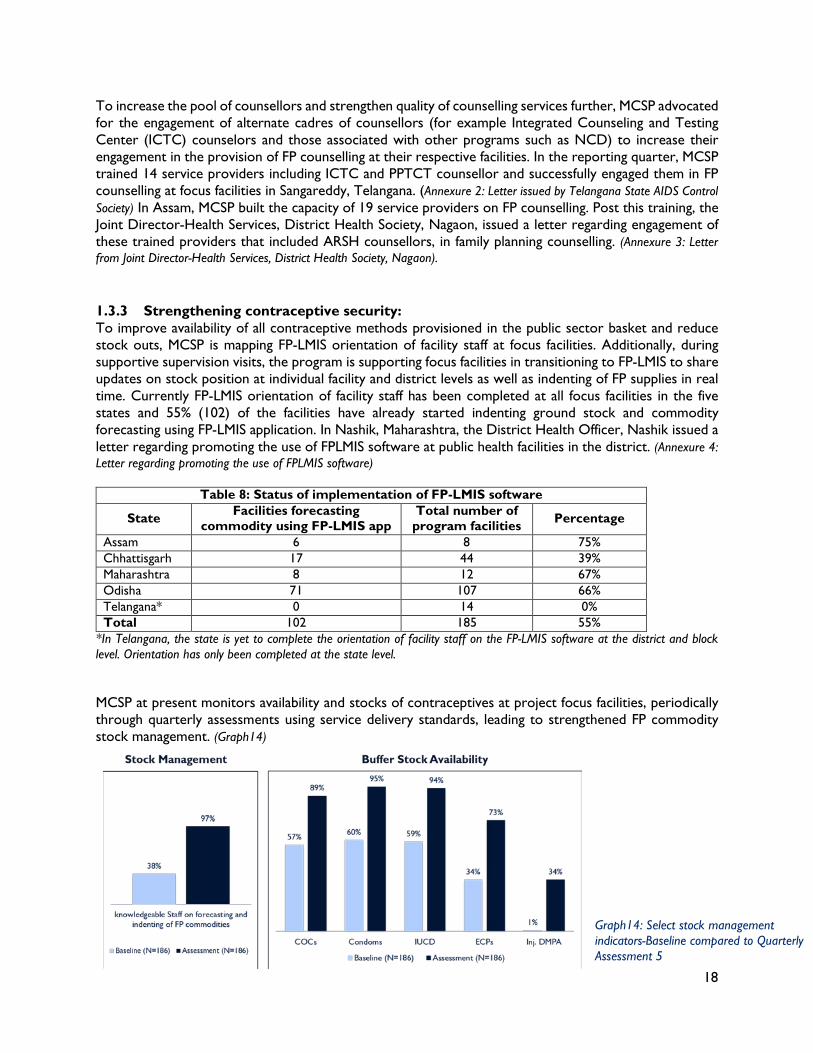
To increase the pool of counsellors and strengthen quality of counselling services further, MCSP advocated for the engagement of alternate cadres of counsellors (for example Integrated Counseling and Testing Center (ICTC) counselors and those associated with other programs such as NCD) to increase their engagement in the provision of FP counselling at their respective facilities. In the reporting quarter, MCSP trained 14 service providers including ICTC and PPTCT counsellor and successfully engaged them in FP counselling at focus facilities in Sangareddy, Telangana. (Annexure 2: Letter issued by Telangana State AIDS Control Society) In Assam, MCSP built the capacity of 19 service providers on FP counselling. Post this training, the Joint Director-Health Services, District Health Society, Nagaon, issued a letter regarding engagement of these trained providers that included ARSH counsellors, in family planning counselling. (Annexure 3: Letter from Joint Director-Health Services, District Health Society, Nagaon). 1.3.3 Strengthening contraceptive security: To improve availability of all contraceptive methods provisioned in the public sector basket and reduce stock outs, MCSP is mapping FP-LMIS orientation of facility staff at focus facilities. Additionally, during supportive supervision visits, the program is supporting focus facilities in transitioning to FP-LMIS to share updates on stock position at individual facility and district levels as well as indenting of FP supplies in real time. Currently FP-LMIS orientation of facility staff has been completed at all focus facilities in the five states and 55% (102) of the facilities have already started indenting ground stock and commodity forecasting using FP-LMIS application. In Nashik, Maharashtra, the District Health Officer, Nashik issued a letter regarding promoting the use of FPLMIS software at public health facilities in the district. (Annexure 4: Letter regarding promoting the use of FPLMIS software)
Table 8: Status of implementation of FP-LMIS software
State Facilities forecasting commodity using FP-LMIS app
Total number of program facilities Percentage
Assam 6 8 75% Chhattisgarh 17 44 39% Maharashtra 8 12 67% Odisha 71 107 66% Telangana* 0 14 0% Total 102 185 55%
*In Telangana, the state is yet to complete the orientation of facility staff on the FP-LMIS software at the district and block level. Orientation has only been completed at the state level. MCSP at present monitors availability and stocks of contraceptives at project focus facilities, periodically through quarterly assessments using service delivery standards, leading to strengthened FP commodity stock management. (Graph14)
Graph14: Select stock management indicators-Baseline compared to Quarterly Assessment 5
19
1.4 CAPACITY BUILDING INITIATIVES Assam:
In February 2019, MCSP organized a three-day training on Postpartum Sterilization (PPS) at B.P. Civil Hospital (District Hospital), Nagaon, Assam in which four providers were trained. In PY5Q2 (January-March 2019), MCSP supported Assam Government and development partner Ipas Development Foundation (IDF) in conducting ten batches of trainings on comprehensive contraceptives in Nagaon, Assam. The trainings covered the newer contraceptive methods – POP, Centchroman and Injectable drug (Antara) along with PPIUCD. Chhattisgarh:
Between January-February, 2019, MCSP supported the government of Chhattisgarh in conducting the first batch of no-scalpel vasectomy (NSV) induction training in the state in Raipur and Dhamtari districts. Three providers from three MCSP focus facilities were trained. In February 2019, MCSP supported the state government of Chhattisgarh in conducting two batches of trainings on oral contraceptives in Rajnandgaon district in which 50 providers were trained. Odisha:
In January 2019, a three-day refresher training on interval Minilap cum PPS was organized at City hospital, Cuttack, Odisha by MCSP. Six providers were reoriented on Minilap standardization. In March, 2019, to support the government of Odisha in the scale-up of the IVRS platform across all the districts in the state, MCSP conducted six batches of training in March 2019, orienting 143 facility staff and 180 ANMs on IVRS in Balasore, Bolangir and Cuttack districts. In the reporting quarter (January-March 2019), MCSP supported the state government of Odisha in conducting fourteen batches of trainings on newer contraceptives including injectable across Bolangir, Khurda, Cuttack, and Mayurbhanj districts in Odisha training 287 participants. Telangana:
In January 2019, a one-day integrated counselling training for ICTC and PPTCT counsellors was conducted by MCSP at DMHO office, Sangareddy, Telangana. Fourteen participants: nine ICTC counsellors, three PPTCT counselors and two recently joined RMNCHA counsellors from nine facilities participated. The participants were oriented on various FP methods, FP counselling and documentation.
Images 7: Comprehensive contraceptive training at CHC Doboka Nagaon

20
In February 2019, MCSP organized a three-day refresher training on interval Minilap cum PPS, at District Hospital, Sangareddy, Telangana. Five providers from five facilities (AH Patancheru, CHC Sadashivpet, CHC Jogipet, CHC Gajwel and PHC Kandi) were reoriented on Minilap standardization. 1.5 MEETINGS & COORDINATION 1.5.1 National level Meetings and Coordination March 11, 2019. U.S. Consulate General, Mumbai. MCSP convened a roundtable consultation with 13 market leaders, capturing over 80% of the Oral Contraceptive Pills (OCP) market in India, in association with Abt Associates led Sustaining Health Outcomes through the Private Sector Plus (SHOPS Plus)-another USAID flagship program. This consultation brought major industry players together on a common platform to develop a shared understanding of the challenges and opportunities for growing the OCP market and a renewed sense of purpose about collaborating in a shared value space for addition of more modern methods such as Progestin-Only Pill (POP) to the public sector contraceptive basket in the country. U.S. Counsel General, Mr. Edgard D. Kagan graced the event along with other USAID team members including Mr. Xerses Sidhwa, Director, Health Office. Dr. Jaydeep Tank, Secretary General, FOGSI was also present. In addition to senior management from leading pharmaceutical companies, other social marketing partners such as PSI, HLFPPT and PHSI were also present. The workshop concluded with the Pharma groups expressing their willingness to invest in POP, despite currently being non-operational in the POP space.
1.5.2 State level Meetings and Coordination January 25, 2019, Bhubaneshwar, Odisha: MCSP team met with the Mission Director, NHM Odisha. Other officials present during the meeting included, Director-Family Welfare, Joint-Director-Family Welfare, Team Lead- State Health Systems Resource Centre, State Program Manager-NHM Odisha among others. The meeting led to the state of Odisha agreeing to the scale-up of the IVRS platform across all 30 districts in the state. MCSP was tasked with developing the roadmap for the sale-up and providing technical support to the state government. It was decided that the issue of inclusion of the Quality Index in the Sampurna budget would be discussed in the next Sampurna meeting.
Image 9:U.S. Counsel General, Mr. Edgard Kagan with the workshop participants
Images 8: Refresher training on interval Minilap cum PPS at District Hospital, Sangareddy
21
1.5.3 District level Meetings and Coordination January 2019 Chhattisgarh • In Chhattisgarh the team attended the Divisional FP
Quarterly Meeting at Durg (January 2, 2019), Raipur (January 3, 2019) and Bilaspur (January 23, 2019) districts. The team used these platforms to present the progress of the IVRS platform, FDS compliance status of facilities in the districts, FP counselling during ANC, status of QC meetings being conducted and progress of uptake of newer contraceptives. As a result, it was decided that steps would be taken to make the OT functional at Gaurella, Dabhara, Malkharoda and Baloda. It was also decided that the status of FDS compliance in the respective districts will be shared with the Deputy Director-Family Planning.
Odisha: • January 11, 2019, Khorda, Odisha: MCSP team attended the PIP dissemination meeting and
presented the progress of implementation of the IVRS platform in terms of booking appointments through the platform and the client feedback received via the platform. Gaps were identified as per the client feedback received and the CDMO requested all MOI/Cs of low performing facilities to improve IVRS implementation and address the gaps identified. The issue of regular conduction of QC and RKS meetings and DQAC members visiting the facilities as per GOI guidelines was also discussed.
• January 16, 2019, Cuttack, Odisha: MCSP team attended the Intensified Pulse Polio Immunization (IPPI) workshop at Cuttack, Odisha. The workshop was attended by MOI/Cs, BPMs and PHEOs of all the blocks in the district. Sharing the program progress the team discussed the uptake of newer contraceptives-POPs and Centchroman, and requested the MOI/Cs of the poor performing facilities to take up the issue during the QC meetings at the respective facilities. The MOI/Cs were also requested to ensure availability of adequate FP commodities with ASHAs to reduce discontinuation. The issue of regular conduction of QC and RKS meetings and DQAC members visiting the facilities as per GOI guidelines was also discussed.
• January 18, 2019, Balasore, Odisha: MCSP team attended the monthly district review meeting at Balasore, Odisha. The meeting was chaired by ADMO (FW) and was attended by facility in-charges and PHEOs of all the facilities in the district along with other district health officials. The status of FDS compliance was shared and the poor performing facilities were identified. Availability of trained providers to conduct Minilap procedures was discussed and the team shared the status of usage of client card and CSC by facilities.
• January 24, 2019, Balangir Odisha: MCSP team attended the monthly facility meeting at CHC Deogaon at Balangir, Odisha. Two FDS days were planned to be conducted every month with implementation of duty roasters and preparatory checklist. Other issues discussed included, procurement of an exclusive pulse oximeter for the Operation Theatre (OT) for intra-op monitoring, use of codes for documenting follow-up findings in sterilization register, use of new guidelines for sedation and
Image 10: District FP Review meeting at Bilaspur
Images 11: MCSP team presenting program progress during IPPI Workshop at Cuttack, Odisha
22
analgesia, promoting the engagement of spouse and other family members during FP counselling and follow-up with acceptors of newer methods for improved compliance.
• January 25, 2019, Balasore, Odisha: MCSP team attended the monthly facility meeting at CHC Berhampura at Balsore, Odisha and conducted a practical session in the operation theatre demonstrating correct OT practices. The team requested the MOI/c to ensure complete documentation of CSCs, arrangement of post‐op ward, restricted entry in OT and maintenance of cleanliness in the OT complex, as well as the entire facility premise.
Telangana: • January 4, 2019, Hyderabad, Telangana: MCSP team met with Additional Project Director, Telangana
State AIDS Control Society regarding the engagement of ICTC counsellors in FP counselling and were successful in seeking approval for training ICTC counsellors for FP counselling.
• January 17, 2019, Sangareddy, Telangana: MCSP team met with DMHO Sangareddy and FP Nodal Officer Sangareddy to share program updates and feedback and gaps identified during the recent Double Puncture Laparoscopy (DPL) camps organized in the district. The DMHO instructed deputy DMHOs to limit the number of clients per day per surgeon to 30, while the FP Nodal officer requested the MCSP team to reorient the facility staff on infection prevention practices, GOI guidelines and reorient the frontline workers on the process of pre-registration.
• January 23, 2019, Sangareddy, Telangana: MCSP team met with the District Collector, Sangareddy to share program updates and feedback and gaps identified during the recent DPL camps organized in the district. The DC mentioned that the issue regarding the gaps identified will be discussed during the DQAC meeting where all district facilities have been instructed to participate.
• January 25, 2019, Sangareddy, Telangana: Post MCSP team’s advocacy, DMHO Sangareddy issued a letter instructing all facility staff to adhere to GOI guidelines for female sterilization and conduct Quality Circle meetings at the facility level once per quarter.
February 2019 Chhattisgarh • In Chhattisgarh, the team attended the monthly district review meeting at Bilaspur (February 15 and
February 25, 2019) and Janjgir-Champa (February 20, 2019), chaired by the respective CMHOs. The meetings were used to discuss the functional status of the Operation theaters at the respective facilities in the districts and the initiation of FDS services.
Maharashtra • February 20, 2019, Nashik, Maharashtra: MCSP participated in a District Review Meeting at Nashik,
chaired by Deputy Director-Family Welfare. During the meeting, it was decided that all trainings for the service providers for different FP methods (PPIUCD and Antara Program) and FPLMIS orientation should be completed on a priority. ANMs were directed to supervise and coordinate the follow-up of clients accepting different FP methods by ASHAs. While discussing the status of FPLMIS software implementation, it was shared that FPLMIS training is completed till block level and indenting of ground stock in the FPLMIS software should be started as soon as login ID received from IT cell.
Odisha • In Odisha, the team attended the monthly district review meeting at Balasore (February 19, 2019),
Kalahandi (February 19, 2019) and Baripada (February 23, 2019) districts. The meetings were used to discuss the functional status of FDS services in the respective districts and mobilization of trained providers was done. During the Kalahandi District Review Meeting, facility staff was encouraged to promote Postpartum FP counselling during the immediate postpartum period for women delivering
23
at the facility. District authorities were requested to plan block-level training on newer contraceptives for staff nurses, LHVs and ANMs. While discussing the status of uptake of Chaaya (Centchroman), facilities were requested to maintain a buffer stock of the contraceptive and indent ground stock in a timely manner to avoid stock-out.
Telangana • February 22, 2019, Sangareddy, Telangana: MCSP team met with DMHO Sangareddy to discuss the
initiation of FDS services at PHC Kandi. The Medical Officer at the facility was recently training during the MCSP organized three day Minilap standardization and PPS training.
• February 27, 2019, Hyderabad, Telangana: MCSP team met with the Director Public Health and Family Welfare and Joint Director-Family Planning to share program update. Non-compliance of GOI guidelines during Double Puncture Laparoscopy (DPL) camps held in different districts and regularizing FP review meetings and DQAC meetings was discussed.
March 2019 Chhattisgarh • March 23, 2019, Durg, Chhattisgarh: MCSP participated in a District Review Meeting at Durg, chaired
by Joint Director, District Health Society and Deputy Director, NHM. 73 government officials and service providers from the district participated in the meeting. The Joint Director mentioned that to strengthen counselling, all possible opportunities should be explored including ANC days, post-delivery and during Anganwadi, vaccination days.
• March 25, 2019, Raipur, Chhattisgarh: MCSP participated in a District Review Meeting at Raipur, chaired by Joint Director, District Health Society and Deputy Director-Family Welfare. 76 government officials and service providers from the district participated in the meeting. The status of functionality of Operation Theatre at DH Gariyaband and Gujra was discussed and facility in-charges were directed to initiate sterilization services at the facilities at the earliest.
Odisha • In Odisha, the team attended the monthly district review meeting at Balasore (March14, 2019) and
Baripada (March 30, 2019) districts. The meetings led to mobilization of trained providers for FDS days and mentorship plans for the providers were also discussed. Facility in-charges were requested to ensure the use and implementation of the Clinical Safety Checklist and Client card for female sterilization. Other issues discussed included the strengthening of counselling and client follow-up and regularizing Quality Circle meetings at the respective facilities.
Telangana • March 13, 2019, Hyderabad, Telangana: MCSP team met with the Commissioner Health & Family
Welfare and the Chief Program Officer to share a progress note on the various program interventions in the state and the challenges faced such as poor uptake of IUCD services and the need to strengthen counselling for increasing the uptake of FP services.
1.6 COMMUNITY PARTICIPATION IN DELIVERY OF FAMILY PLANNING SERVICES AND CAPACITY BUILDING OF SERVICE PROVIDERS ON RESPECTFUL CARE
With MCSP support, sub-award partner Centre for Catalyzing Change (C3) carried out the following key activities in the states of Chhattisgarh and Odisha in PY5Q2:
24
1.6.1 Meetings, Coordination and Follow-up Odisha
• The team met with the newly joined Joint Director-FW to brief about MCSP activities in the state including training on Gender, Social Inclusion and Respectful Care (GIRC) in family planning services and PSV implementation. Key state level health officials were identified and given access to the online PSV dashboard and given the responsibility of regularly reviewing the feedback received via the IVRS platform and sharing with the Directorate of Family Welfare in the state.
• The PSV dashboard indicators were presented during the district level review meetings in Kalahandi and Mayurbhanj districts and training plans were developed for refresher training of facility staff on GiRC and IVRS.
• The C3 team, along with the DMRCH and DPM of Kalahandi, undertook joint visits to five FDS Centers with the objectives to assess the usage of PSV and follow up with block level health officials to take measures for improving respectful care practices.
• The C3 team visited 43 facilities in the state in the reporting quarter to review and support in the implementation of PSV platform, facilitate in the organization of RKS and QC meetings and support respectful care. The assessment findings of Respectful Care Indicators were shared with the line health officials and corrective actions were also proposed to close these gaps.
• The team attended 34 sector meetings of ASHA and ANMs in PY5Q2, and discussed respectful care and couple counselling and involvement of the male partner in FP counselling along with reinforcing the key messages of Gender Social Inclusion and Respectful care (GIRC). The platform was also used to promote the use and implementation of Parivar Swasthya Vaani.
Chhattisgarh
• The team met with the State FP Nodal officer to get approval for a laminated Job Aid for FLWs for promotion of PSV 104. As a result, the content and design of this product was approved by the state government and the same has been provided to FLWs in the six MCSP districts.
• During the reporting quarter, the C3 team met with various stakeholders, including the CMHO, DPM, RMNCH+A Consultant etc. in the districts of Durg, Rajnandgaon, and Bilaspur to promote IVRS. The team demonstrated the use of IVRS as well as shared a status of the feedback calls as captured using the IVRS dashboard. The status of feedback calls was shared highlighting the low number of IVRS feedback calls. All the three CMHOs, offered a time slot in the meeting every month for discussions on PSV dashboard facilitated by C3 in the coming months.
• In PY5Q2 the C3 team attended five sector level ANM meetings in the districts of Dhamtari, Rajnandgaon and Janjgir-Champa. This platform was utilized to orient the ANM on the use of the IVRS platform for client feedback and nearly 200 ANMs were re-oriented on IVRS. Similarly, the team attended 11 Mitanin Trainers’ (MT) meetings (in Dhamtari, Rajnandgaon and Raipur districts) and in the 23rd round of Mitanin Training (in Raipur, Dhamtari, Durg, Rajnandgaon, Bilaspur and Janjgir-Champa districts) orienting 3562 Mitanin Trainers and Mitatnins respectively on the IVRS platform. Patients’ rights was a key subject during this Annual Cycles where Respectful Care is an integral component.
Image 12: Distribution of IEC during the Mitanin Meeting
25
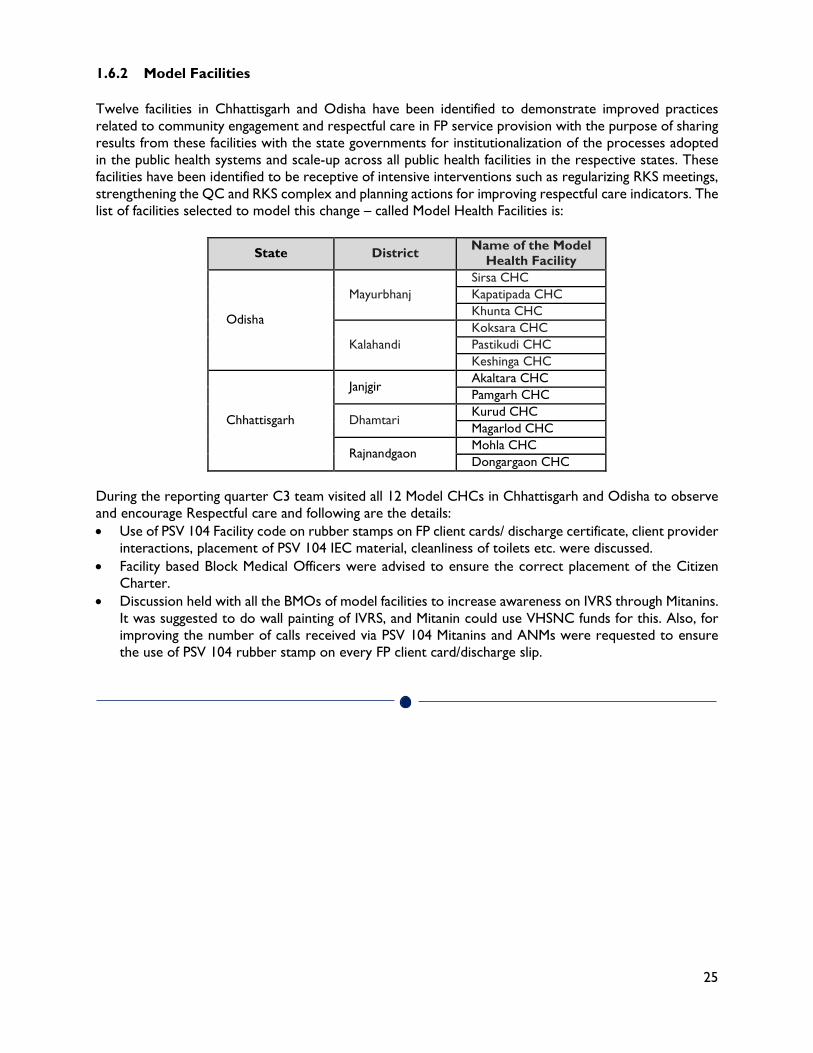
1.6.2 Model Facilities Twelve facilities in Chhattisgarh and Odisha have been identified to demonstrate improved practices related to community engagement and respectful care in FP service provision with the purpose of sharing results from these facilities with the state governments for institutionalization of the processes adopted in the public health systems and scale-up across all public health facilities in the respective states. These facilities have been identified to be receptive of intensive interventions such as regularizing RKS meetings, strengthening the QC and RKS complex and planning actions for improving respectful care indicators. The list of facilities selected to model this change – called Model Health Facilities is:
State District Name of the Model Health Facility
Odisha
Mayurbhanj Sirsa CHC Kapatipada CHC Khunta CHC
Kalahandi Koksara CHC Pastikudi CHC Keshinga CHC
Chhattisgarh
Janjgir Akaltara CHC Pamgarh CHC
Dhamtari Kurud CHC Magarlod CHC
Rajnandgaon Mohla CHC Dongargaon CHC
During the reporting quarter C3 team visited all 12 Model CHCs in Chhattisgarh and Odisha to observe and encourage Respectful care and following are the details: • Use of PSV 104 Facility code on rubber stamps on FP client cards/ discharge certificate, client provider
interactions, placement of PSV 104 IEC material, cleanliness of toilets etc. were discussed. • Facility based Block Medical Officers were advised to ensure the correct placement of the Citizen
Charter. • Discussion held with all the BMOs of model facilities to increase awareness on IVRS through Mitanins.
It was suggested to do wall painting of IVRS, and Mitanin could use VHSNC funds for this. Also, for improving the number of calls received via PSV 104 Mitanins and ANMs were requested to ensure the use of PSV 104 rubber stamp on every FP client card/discharge slip.
26
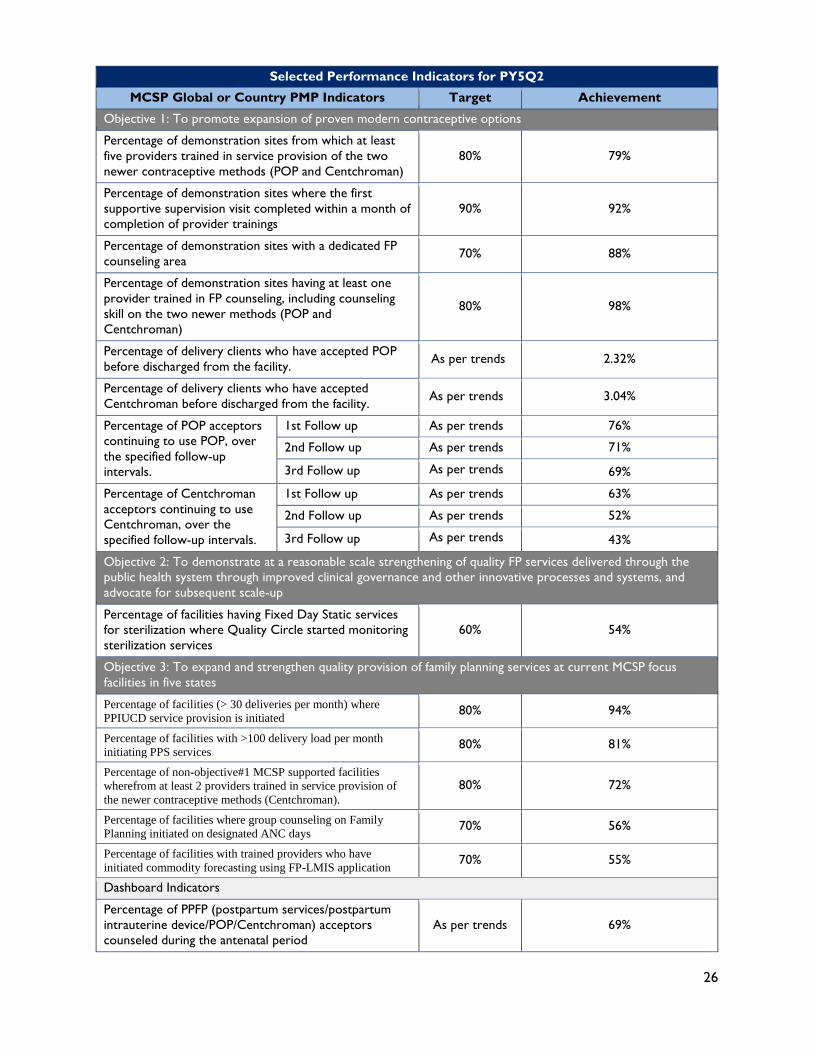
Selected Performance Indicators for PY5Q2
MCSP Global or Country PMP Indicators Target Achievement
Objective 1: To promote expansion of proven modern contraceptive options
Percentage of demonstration sites from which at least five providers trained in service provision of the two newer contraceptive methods (POP and Centchroman)
80% 79%
Percentage of demonstration sites where the first supportive supervision visit completed within a month of completion of provider trainings
90% 92%
Percentage of demonstration sites with a dedicated FP counseling area 70% 88%
Percentage of demonstration sites having at least one provider trained in FP counseling, including counseling skill on the two newer methods (POP and Centchroman)
80% 98%
Percentage of delivery clients who have accepted POP before discharged from the facility. As per trends 2.32%
Percentage of delivery clients who have accepted Centchroman before discharged from the facility. As per trends 3.04%
Percentage of POP acceptors continuing to use POP, over the specified follow-up intervals.
1st Follow up As per trends 76%
2nd Follow up As per trends 71%
3rd Follow up As per trends 69%
Percentage of Centchroman acceptors continuing to use Centchroman, over the specified follow-up intervals.
1st Follow up As per trends 63%
2nd Follow up As per trends 52%
3rd Follow up As per trends 43%
Objective 2: To demonstrate at a reasonable scale strengthening of quality FP services delivered through the public health system through improved clinical governance and other innovative processes and systems, and advocate for subsequent scale-up
Percentage of facilities having Fixed Day Static services for sterilization where Quality Circle started monitoring sterilization services
60% 54%
Objective 3: To expand and strengthen quality provision of family planning services at current MCSP focus facilities in five states
Percentage of facilities (> 30 deliveries per month) where PPIUCD service provision is initiated 80% 94%
Percentage of facilities with >100 delivery load per month initiating PPS services 80% 81%
Percentage of non-objective#1 MCSP supported facilities wherefrom at least 2 providers trained in service provision of the newer contraceptive methods (Centchroman).
80% 72%
Percentage of facilities where group counseling on Family Planning initiated on designated ANC days 70% 56%
Percentage of facilities with trained providers who have initiated commodity forecasting using FP-LMIS application 70% 55%
Dashboard Indicators
Percentage of PPFP (postpartum services/postpartum intrauterine device/POP/Centchroman) acceptors counseled during the antenatal period
As per trends 69%
27
Selected Performance Indicators for PY5Q2
MCSP Global or Country PMP Indicators Target Achievement
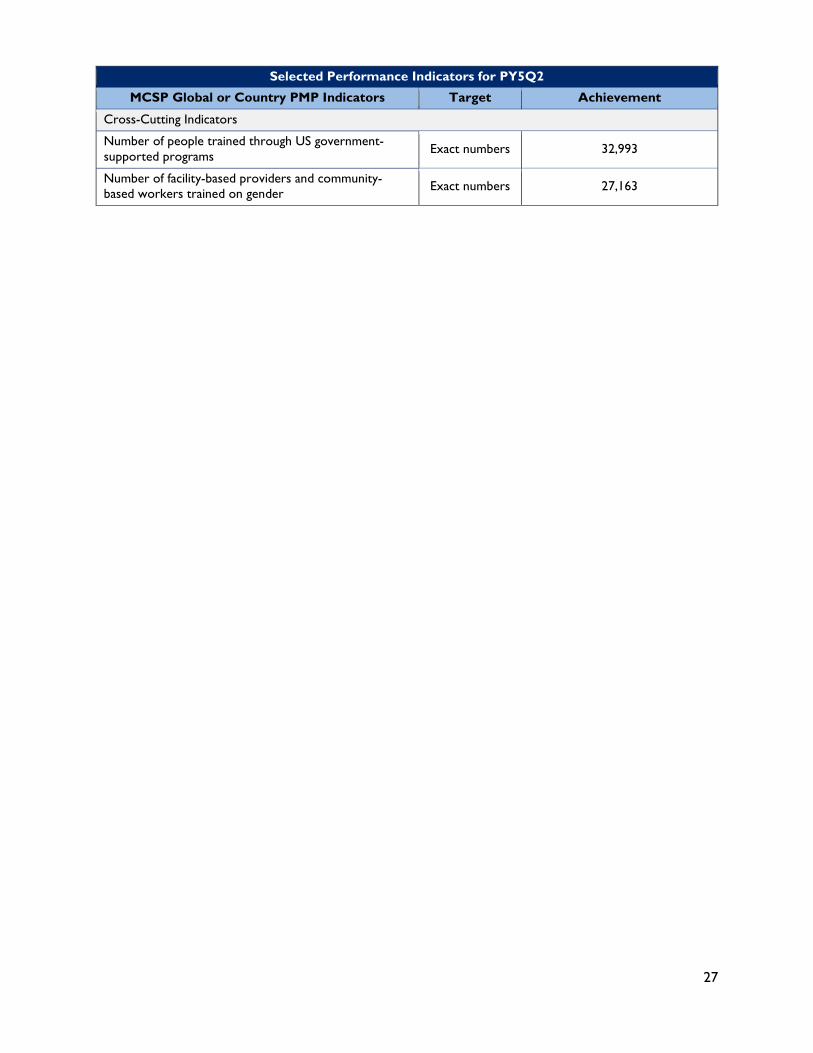
Cross-Cutting Indicators
Number of people trained through US government- supported programs Exact numbers 32,993
Number of facility-based providers and community-based workers trained on gender Exact numbers 27,163
28
2.0 TECHNICAL SUPPORT UNIT- ADOLESCENT HEALTH GOAL: TO PROVIDE TECHNICAL SUPPORT TO MINISTRY OF HEALTH & FAMILY WELFARE (MOHFW) GOI FOR ADOLESCENT HEALTH (AH)
2.1 OBJECTIVE 1: TO PROVIDE STRATEGIC TECHNICAL SUPPORT TO THE MOHFW IN
PLANNING, IMPLEMENTATION AND MONITORING OF NEW INITIATIVES AND STRENGTHENING OF THE SIX STRATEGIC PRIORITY (PROGRAM) COMPONENTS UNDER THE RKSK.
Strengthening Adolescent Friendly Health Clinics: TSU has developed Standard Operating Procedures(SOPs) to assist counselors in dealing with complicated issues like mental health, gender based violence and substance abuse. The SoPs (copy of Mental Health SoP is enclosed at Annexure-5) have been submitted to MoHFW for review.
School Health Programme: TSU developed different options of School Health Programme logo which has been submitted to MoHFW for review and finalization. Operational plan to implement School Health Programme in the states is also prepared and submitted to Ministry for further inputs. TSU-AH is working closely with NCERT in finalizing the school health curriculum based on feedbacks received from Ministry of Human Resource and Development (MHRD) and MoHFW. 2.2 OBJECTIVE 2: PROVIDE SUPPORT TO THE AH DIVISION TO INSTITUTIONALIZE
ROBUST SYSTEMS AND MECHANISMS FOR COORDINATION/CONVERGENCE WITHIN THE MOHFW, WITH OTHER GOVERNMENT DEPARTMENTS AND MINISTRIES AND WITH OTHER PARTNERS IN THE ADOLESCENT SPACE.
Adolescent Health Working Group: TSU participated in AH working group meeting organized by UNFPA in March, 2019 to deliberate on different implementation models of school health programs and build a collective understanding of mental health concerns in adolescents. TSU-AH also participated in the regional consultation on Adolescent and Youth Health, hosted by PFI and YP Foundation at Kalahandi, Odisha on 25 February 2019. Think Tank Consultation: TSU-AH hosted the first Think Tank consultation session on Adolescent Mental Health Program - Opportunities & Addressing Challenges in March 2019. The objectives of the meeting were to map interest areas and future opportunities for mental health. The participants of this meeting included clinical practitioners, organizations working with community and school level interventions on mental health issues. The report is enclosed as Annexure-6
2.3 OBJECTIVE 3: PROVIDE SUPPORT TO DEVELOP INNOVATIVE APPROACHES IN THE SBCC STRATEGY
National Youth Campaign: ’BOL’ is a national online and offline campaign implemented by Centre for Catalyzing Change (C3) under MCSP. The offline data collection is currently underway through 30 partners on board covering the states of Uttar Pradesh, Madhya Pradesh, Odisha, Bihar, Jharkhand,
29
Chhattisgarh, Assam, Meghalaya, Delhi, Haryana, Punjab, Uttarakhand, Himachal Pradesh, Punjab, Himachal Pradesh, Mizoram, Manipur, Nagaland, Jammu & Kashmir, Rajasthan, West Bengal and Tamil Nadu. Also. established partnerships with three of the largest global technology firms: Facebook, Twitter and Instagram for online mode. Till March 2019, 1035 online polls have been filled by the adolescents and the results are largely centered on access to more information, mental health services, and wanting a peaceful and clean environment. OBJECTIVE 4: ADVOCATE WITH THE STATE GOVERNMENTS FOR ADOPTING AND
BUDGETING EVIDENCE-BASED INTERVENTIONS AS PER THE NATIONAL AH POLICY
FRAMEWORK Regional Review Meetings: TSU provided strategic support in five regional review meetings conducted by MoHFW across the country to review the progress in implementation of National Adolescent Health Program. Two meeting were conducted in the last quarter. In January 2019, remaining three regional reviews meetings had commenced in Punjab, Chhattisgarh and Meghalaya. Date 10-11th Jan'19 17-18th Jan'19 22-23rd Jan '19
Participating states
Jammu & Kashmir, Haryana, Punjab, Himachal Pradesh, Uttarakhand, Chandigarh and Delhi
Rajasthan, Gujarat, Chhattisgarh, Madhya Pradesh, Maharashtra, Daman & Diu, Dadar & Nagar Haveli, Bihar and Telangana
Arunachal Pradesh, Meghalaya, Mizoram, Manipur, Tripura, Sikkim, Assam, Nagaland
State specific action points were made and shared with Mission Director- National Health Mission (MD-NHM) of States. A sample of State action points is enclosed at Annexure-7 State factsheets: Based on the regional review meeting, TSU developed States/UTs wise fact sheets having secondary data and action points from regional review meeting reports. All the fact sheets were shared with MoHFW. The sample of the fact sheet is enclosed at Annexure-8 Field visit to States: During the regional review meetings, few States were categorized as week states due to gaps in implementing Adolescent Health interventions. TSU along with MoHFW officials made supportive supervision visits to States of Telangana and Assam to handhold them in reducing gaps identified in regional review meetings.

30
Selected Performance Indicators for PY5Q2
MCSP Global or Country PMP Indicators Achievement
National-level Technical Action Group for National Adolescent Health Program formed and functional Two national-level technical action group meetings conducted
National-level stakeholders review/dissemination meeting convened
Experience-sharing and learning workshop with various stakeholders was conducted on March 22–23, 2018 5 regional review meetings facilitated across the country
State Program Implementation Plans reviewed and approved for all National Adolescent Health Program activities
Reviewed record of proceedings (2018–2019) of 100% states/Union Territories (36 states)
A dashboard of adolescent indicators developed Prepared and shared with Ministry of Health and Family Welfare (MoHFW)
Number of states that have budgeted for initiative under School Health Program under Ayushman Bharat
Approval of budget allocation for School Health Program under Ayushman Bharat in Record of Proceeding. Out of 36 states, 28 states have allocated budgets.

31
3.0 HUMAN RESOURCES FOR HEALTH-HEALTH & WELLNESS
CENTRES GOAL: CREATION OF A NETWORK OF ‘HEALTH AND WELLNESS CENTRES’ ACROSS INTERVENTION STATES FOR PROVISION OF COMPREHENSIVE PRIMARY HEALTH CARE, THEREBY LEADING TO UNIVERSAL HEALTH COVERAGE The description of activities during the reporting period is given below: • USAID’s Delegate Visit to Madhya Pradesh and Assam: A team from USAID India Mission
visited HWC Rajnagar in Madhya Pradesh and HWC Rajmita, in Goalpara district of Assam on February 28, 2019 to understand the work done by MCSP under Ayushman Bharat HWCs. The delegation visited the HWCs and interacted with local health workers of the HWC, government officials as well as the beneficiaries residing in catchment area of the HWC. Mr. Xerses Sidhwa and Dr. Anuradha Jain from USAID visited Madhya Pradesh while Dr. Sharmila Neogi visited Assam.
• Celebration of five years of RKSK with the larger theme of Health and Wellness in
Meghalaya: The state government of Meghalaya with support from MCSP planned a month long celebrations as part of five years of Rashtriya Kishor Swasthya Karyakaram (RKSK), the national health programme for adolescents with a larger theme of creating awareness on Health and Wellness Centers. MCSP supported the state in planning and organizing the activities and also documenting the final event. The state invited USAID as a guest of honor for the final event, which was held on February 13, 2019. Dr. Vivek Yadav, Chief of Party, MCSP graced the occasion as a chief guest for the event. During the event, the Mission Director Mr. Pravin Bakshi appreciated the support and role of MCSP and highlighted the need for continued partnership with the state for improving the health of the communities.
USAID team visits HWC Rajnagar in MP USAID team visits HWC Rajmita in Assam
32
• Technical expert group meeting for integration of Tuberculosis in Pregnancy and writing
group on framework for gender-responsive approaches to Tuberculosis: The first technical expert group meeting for integration of Tuberculosis in Pregnancy was held on January 28, 2018 and the meeting on writing group on framework for gender-responsive approaches to TB under Revised National Tuberculosis Program (RNTCP) was held on February 19, 2019 under the leadership of Deputy Director General, Tuberculosis, Ministry of Health and Family Welfare. MCSP team was also included as a member of this expert committee.
• Adoption of Internal Branding Package for Health and Wellness Centers by different states: MCSP developed a comprehensive internal branding package for HWCs (includes facility branding as well as IEC materials to be displayed in the facility) for the state government of Chhattisgarh. During the quarter, this package was adopted by the states of Arunachal Pradesh. Till date the package has been replicated and adopted by ten states.
• Support for operationalization of HWCs: During this quarter, MCSP continued supporting the intervention states in various activities for operationalization of HWCs. These included gap analysis of facilities, branding of facilities, population enumeration, streamlining services, procurement and supply of equipment, medicines and other logistics, initiating wellness activities and other services as per the Government of India guidelines. A total of 1023 facilities in MCSP demonstration districts have been fully operational while 608 facilities have initiated upgradation to HWCs.
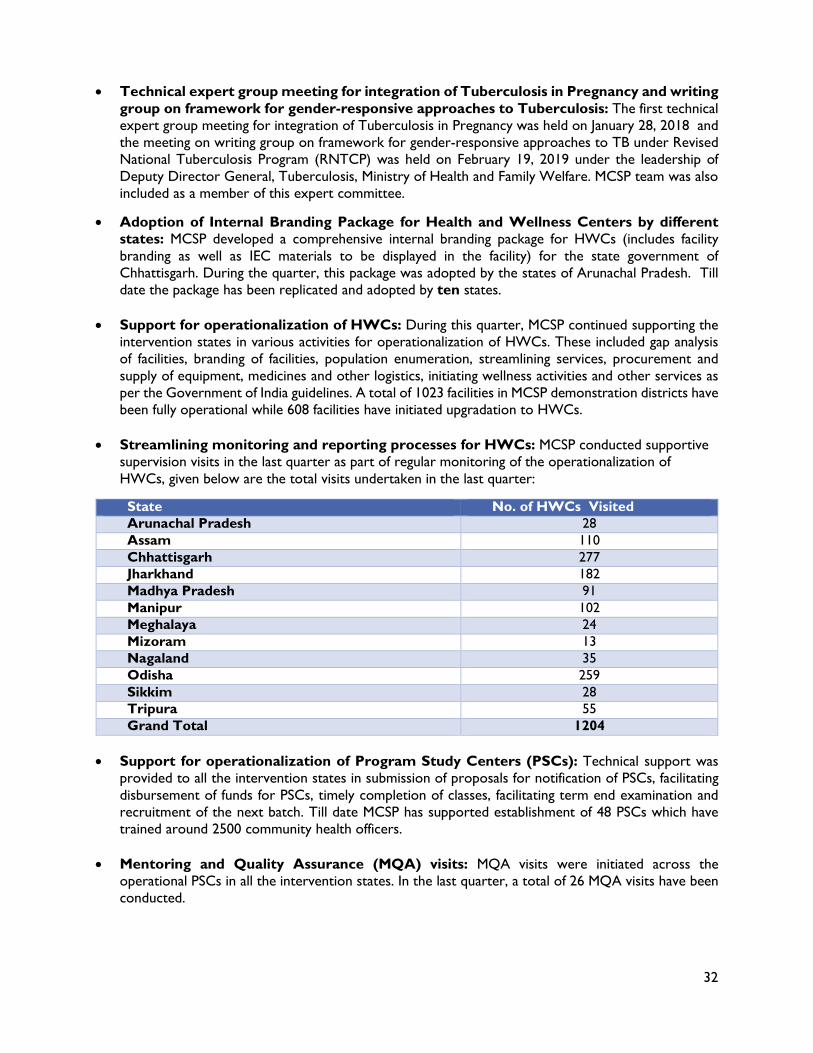
• Streamlining monitoring and reporting processes for HWCs: MCSP conducted supportive supervision visits in the last quarter as part of regular monitoring of the operationalization of HWCs, given below are the total visits undertaken in the last quarter:
State No. of HWCs Visited Arunachal Pradesh 28 Assam 110 Chhattisgarh 277 Jharkhand 182 Madhya Pradesh 91 Manipur 102 Meghalaya 24 Mizoram 13 Nagaland 35 Odisha 259 Sikkim 28 Tripura 55 Grand Total 1204
• Support for operationalization of Program Study Centers (PSCs): Technical support was
provided to all the intervention states in submission of proposals for notification of PSCs, facilitating disbursement of funds for PSCs, timely completion of classes, facilitating term end examination and recruitment of the next batch. Till date MCSP has supported establishment of 48 PSCs which have trained around 2500 community health officers.
• Mentoring and Quality Assurance (MQA) visits: MQA visits were initiated across the operational PSCs in all the intervention states. In the last quarter, a total of 26 MQA visits have been conducted.
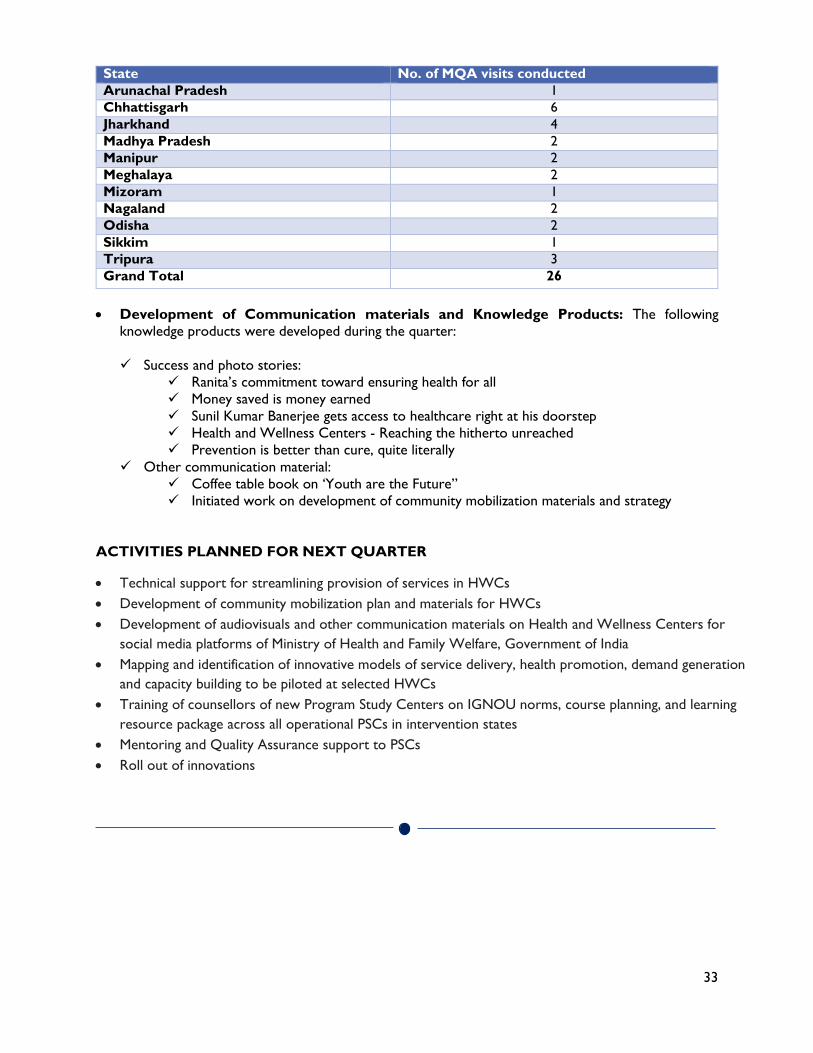
33
State No. of MQA visits conducted Arunachal Pradesh 1 Chhattisgarh 6 Jharkhand 4 Madhya Pradesh 2 Manipur 2 Meghalaya 2 Mizoram 1 Nagaland 2 Odisha 2 Sikkim 1 Tripura 3 Grand Total 26
• Development of Communication materials and Knowledge Products: The following
knowledge products were developed during the quarter: Success and photo stories:
Ranita’s commitment toward ensuring health for all Money saved is money earned Sunil Kumar Banerjee gets access to healthcare right at his doorstep Health and Wellness Centers - Reaching the hitherto unreached Prevention is better than cure, quite literally
Other communication material: Coffee table book on ‘Youth are the Future” Initiated work on development of community mobilization materials and strategy
ACTIVITIES PLANNED FOR NEXT QUARTER
• Technical support for streamlining provision of services in HWCs • Development of community mobilization plan and materials for HWCs • Development of audiovisuals and other communication materials on Health and Wellness Centers for
social media platforms of Ministry of Health and Family Welfare, Government of India • Mapping and identification of innovative models of service delivery, health promotion, demand generation
and capacity building to be piloted at selected HWCs • Training of counsellors of new Program Study Centers on IGNOU norms, course planning, and learning
resource package across all operational PSCs in intervention states • Mentoring and Quality Assurance support to PSCs • Roll out of innovations
34
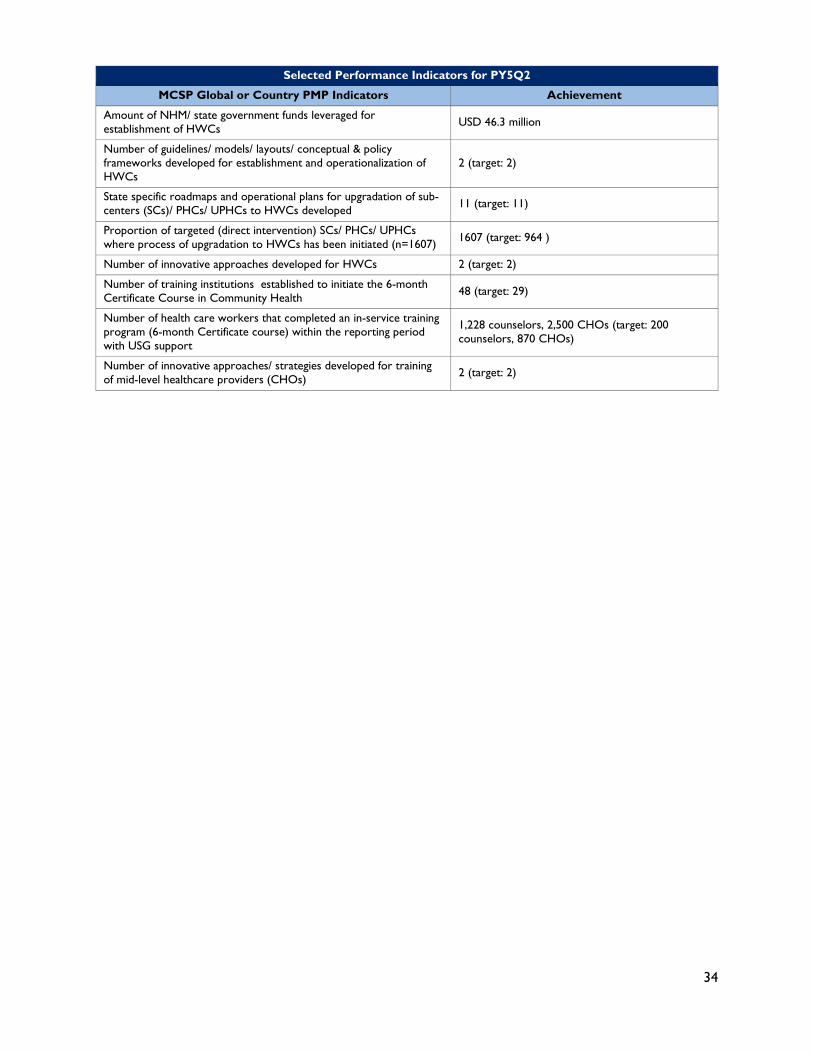
Selected Performance Indicators for PY5Q2
MCSP Global or Country PMP Indicators Achievement
Amount of NHM/ state government funds leveraged for establishment of HWCs USD 46.3 million
Number of guidelines/ models/ layouts/ conceptual & policy frameworks developed for establishment and operationalization of HWCs
2 (target: 2)
State specific roadmaps and operational plans for upgradation of sub-centers (SCs)/ PHCs/ UPHCs to HWCs developed 11 (target: 11)
Proportion of targeted (direct intervention) SCs/ PHCs/ UPHCs where process of upgradation to HWCs has been initiated (n=1607) 1607 (target: 964 )
Number of innovative approaches developed for HWCs 2 (target: 2)
Number of training institutions established to initiate the 6-month Certificate Course in Community Health 48 (target: 29)
Number of health care workers that completed an in-service training program (6-month Certificate course) within the reporting period with USG support
1,228 counselors, 2,500 CHOs (target: 200 counselors, 870 CHOs)
Number of innovative approaches/ strategies developed for training of mid-level healthcare providers (CHOs) 2 (target: 2)
35
4.0 CHALLENGES Below are a list of some major challenges experienced in this quarter that affected program operations: Family Planning: • Frequent transfer of MCSP trained providers to non-MCSP facilities, hampered operations in the
states of Odisha and Maharashtra. • Limited pool of trained providers. In Odisha there is a non-availability of providers with prior
experience of conducting FDS days, while in Assam, only two Minilap trained and performing providers are present in Nagaon district.
• Frequent state level bandhs and strikes in Assam and Odisha (NHM Strike in February) affected observing FDS days as per the calendar planned
• The phone lines for the IVRS platform in Chhattisgarh are routed through the government’s 104 portal that has connectively issues. As a result, call drop and poor compliance was reported by ANMs.
• Number of calls received via the IVRS platform in Chhattisgarh, for providing client feedback remains significantly low compared to the number of female sterilization procedures conducted in the state. In the reporting quarter, 7872 clients received female sterilization services, of which only 11% (852) clients shared feedback on the quality of services received.
• Digitization of the Clinical Safety Checklist (CSC) continues being a challenge in Chhattisgarh and Maharashtra, as several facilities do not have designated data entry operators. Only 53% of the CSCs filled are digitized in Maharashtra and status of CSC digitization is 60% in Chhattisgarh, as compared to 87% and 95% in Odisha and Assam respectively.
• Assam continues facing limited supply of FP methods provided by the state at the facility level leading to poor uptake of services.
Technical Support Unit-Adolescent Health: • Repeated revision in documents such as SoPs, school health logos and state fact sheets led to delays
in final approvals. • Inordinate delays from Ministry of Human Resource and Development in finalizing the curriculum
of School Health Program.
Health and Wellness Centers: • During the quarter, various challenges were faced in terms of streamlining the processes of
operationalization of HWCs across states, procedural delay in implementation, limited co-ordination among multiple stakeholders and quality assurance in trainings for certificate course at PSCs.
• These challenges were identified through regular supportive supervision visits at HWCs and MQA visits at PSCs.
• The issues were brought up at the steering committee meetings and further notified at the respective district and state levels for quick action and decision making.
• Further, MCSP is providing regular handholding support to PSC staff and district officials to ensure immediate redressal for the issues and smooth delivery of the primary health care services.
36
5.0 WAY FORWARD Family Planning: In the coming quarter, MCSP will work towards disseminating the results and the lessons learnt from the POP demonstration with the government at the national and state levels to advocate for the inclusion of POP in the public health basket of contraceptives and scale-up across the country. Advocacy efforts will be made with the state government of Chhattisgarh in the context of scale-up of the IVRS platform across the state and technical support will be given to the state of Odisha for the rollout of the IVRS platform across all 30 districts in the state. The program will support Odisha government in their rollout efforts for the SOP for Prevention and Management of Complications related to Female Sterilization Surgery in MCSP focus districts. MCSP will undertake advocacy efforts for the development of such an SOP in the state of Chhattisgarh. To further strengthen counselling services, MCSP will continue to advocate in the remaining four focus states – Assam, Chhattisgarh, Maharashtra and Telangana, for the engagement of alternative cadres of counselors (under other programs, such as ICTC, NCD) to increase the pool of counselors and ensure quality counseling services. The program will also advocate with states and focus facilities to integrate FP key messages in-group counseling sessions at Antenatal Care (ANC) clinics and for Pradhan Mantri Surakshit Matritva Abhiyan (PMSMA) days (held on the 9th of each month). MCSP will take its work forward at the twelve model facilities identified in Chhattisgarh and Odisha. Efforts will be strengthened at these facilities to form linkages between RKS and QCs, as well as provide support to regularize the RKS/QC meetings for improved quality assurance structures. The program will facilitate review of the FP dashboard during DQAC, QC and RKS meetings to promote use of data for better decision making. MCSP will work closely with state, district and facility level Quality Assurance structures to share data on high performing and low performing focus facilities, to help inform continued targeted support. MCSP developed the Quality Index (QI) with the intention of shifting the focus away from individuals and onto the facility as a driver for quality change. The Quality Index ranks facilities based on their program performance, quality of FDS services provision, and client feedback on the quality of service providers (utilizing the IVRS platform) as opposed to the current facility ranking criteria used by the Government that are entirely quantitative. Currently, the QI has buy-in from the state government of Odisha regarding a reward mechanism for the higher-ranking facilities in each district, and to budget through the existing state’s ‘Sampurna’8 project. Moving forward, the program will advocate with the state government of Chhattisgarh, which also implemented the IVRS component for their buy-in for the Quality Index.
Technical Support Unit-Adolescent Health: In the next quarter, TSU will pilot android based mobile application of AFHCs in 5 States for which a letter has already sent to respective state MDs. We are also planning to conduct at least two think Tank meetings involving relevant stakeholders on technology enabled solutions for adolescents and involvement of men, boys and parents in improving adolescent health. Review of already existing adolescent health IEC material and identifying the need for developing new material will be undertaken. More field visits will be
8 Government of Odisha launched the SAMPURNA — (Sishu Abond Matru Mrityuhara Purna Nirakaran Abhijan) programme under the state budget to increase institutional deliveries in order to reduce infant mortality rate (IMR) as well as mother mortality rate (MMR).

37
made to States to assess the implementation, identify gaps and provide solutions for effective implementation of National Adolescent Health Programme. Health and Wellness Centers: In the next quarter, MCSP will work towards demonstrating innovative models of service delivery and community mobilization to increase demand generation, and ensure quality service delivery of comprehensive primary health care, including family planning, maternal, newborn, child health, and non-communicable diseases.

38
Annexure 1: IVRS scale-up in Odisha
• Post MCSP’s advocacy efforts, the state of Odisha has approved and budgeted funds to the annual NHM Program Implementation Plan (PIP) for IVRS application scale-up across the state's 30 districts. The Government of India has approved a budget of INR 15 lacs ($21,127) for the implementation of the platform across the state of Odisha.
• MCSP will provide technical and implementation support to NHM in the rollout of the IVRS platform across the current six MCSP focus districts in Odisha. The program will orient government health officials and facility staff. Four additional non-MCSP districts will be identified in consultation with the Odisha state government, for the rollout of the IVRS platform, including the development of roadmaps and SOPs for the training of government personnel.
• To support the government of Odisha in the scale-up of the IVRS platform across all the districts in the state, MCSP conducted six batches of training in March 2019, orienting 143 facility staff and 180 ANMs on IVRS in Balasore, Balangir and Cuttack districts.
• Currently PSV in Odisha is using a missed call- call back system to a phone number. A security audit will be undertaken- by a government approved and empaneled vendor and facilitated by MCSP’s technology partner for IVRS, to prepare for integration into the National Informatics Centre (NIC.in) server. The timeline proposed for the audit, is four working weeks and would be at an estimated cost of INR 60,000 for one state.
• Similarly, in preparation for the integration into National Informatics Centre, the architecture that is currently hosted on a single platform, catering to both Chhattisgarh and Odisha would have to be separated. The cost of this separation has been estimated at INR 200,000 and would be undertaken by MCSP’s technology partner for IVRS.
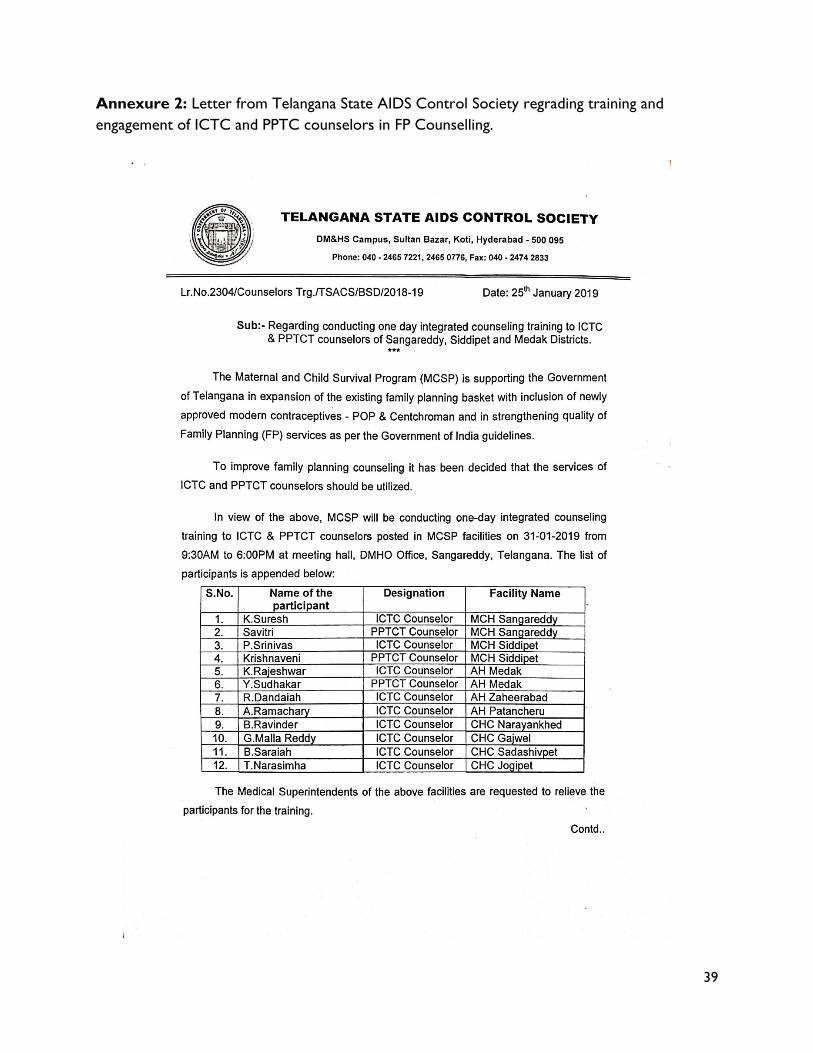
39
Annexure 2: Letter from Telangana State AIDS Control Society regrading training and engagement of ICTC and PPTC counselors in FP Counselling.
40
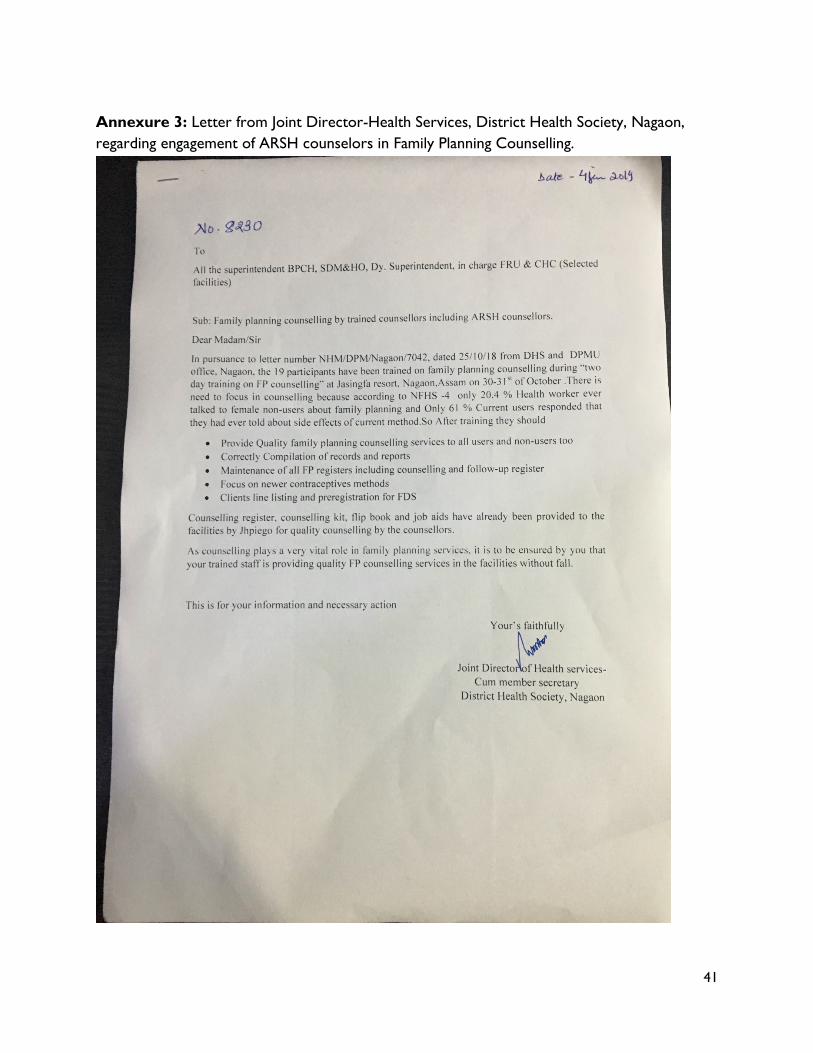
41
Annexure 3: Letter from Joint Director-Health Services, District Health Society, Nagaon, regarding engagement of ARSH counselors in Family Planning Counselling.
42
43
Annexure 4: Letter from District Health Officer, Nashik Maharashtra regarding promoting the use of FPLMIS software.
44
Annexure 5: Standard Operation Procedure (SoP): Mental health
Mental health is a state of well-being in which the individual realizes his or her own abilities. It helps him or her to cope with the challenges in life and work productively and fruitfully. Thus helping the individual makes a contribution to the community. Mental well-being makes up an integral part of an individual's capacity to lead a fulfilling life, including the ability to nurture relationships, study, and work or pursue leisure interests, as well as to make day-to-day decisions and choices. Mental health and well-being is influenced not only by individual attributes, but also by the social circumstances in which persons find themselves and the environment in which they live; these determinants interact with each other dynamically, and may threaten or protect an individual's mental health state. Adolescence is a distinct developmental period characterized by significant changes at physical mental, hormonal, emotional, cognitive and behavioural level. It can lead to adverse social outcomes among adolescents such as high consumption of alcohol, tobacco and illicit substances use, adolescent pregnancy, school dropout, conduct disorders and delinquent behaviours. There is a growing consensus that healthy development during childhood and adolescence contributes to good mental health and can help prevent problems. Enhancing social skills, problem-solving skills and self-confidence can help prevent mental health problems. Mental health disorders can disrupt school performance, harm relationships and may lead to suicide. Key mental health issues of adolescents
• Stress and anxiety • Depression • Eating disorders • Substance abuse • Suicide
Major categories • Behavioural disorders (Attention deficit and
Conduct disorder) • Developmental disorders (Learning difficulties) • Emotional disorders (Depression & Anxiety) • Severe mental disorders (Schizophrenia)
Symptoms needing attention: • Signs of overt mood depression (low mood, tearfulness, lack of interest in usual activities) • Somatic complaints such as headache, stomach ache, backache, and sleep problems • Self harming behaviours • Aggression • Isolation and loneliness • Deviant behaviour such as theft and robbery • Change in school performance or behaviour • Use of psychoactive substances, including over the counter medications • Weight loss or failure to gain weight It is important that the Counsellor has the competencies to relate to young people to detect mental health problems early. The counsellor should be able to provide treatments which include counselling and referral for cognitive-behavioural therapy and wherever appropriate for psychotropic medication. The role of the counsellor is to enable the client to explore many aspects of their life and feelings, by talking openly and freely. The aim should be to in still positive values and behaviours among adolescents so that they can flourish, contribute to society and lead a happy, healthy life. They should help adolescents explore their potential which includes the identification, prevention and
45
treatment of mood and mental disorders that influence the transition into a successful adult. Mental health issues are often associated with stigma or ignorance that inhibits some adolescents and their families from seeking help. Timely identification and treatments for mental health disorders, especially if they begin soon after symptoms appear, can help reduce its impact on an adolescent's life.
Stress & Depression Stress: Stress is the body's reaction which is triggered by any event that tends to disturb our normal state of well-being. Events such as frustration, conflicts and over burden can generally initiate or aggravate stress. Causes of stress
• Over burden of physical, mental or social pressures • Short time and deadlines • Frustrations • Lack of required support Over or unclear expectations • Unnatural shock – death of loved ones • Examination pressure • Relationship problems or understanding • Guilt Conflicts
Different people express or explain their stress differently; some may show physical signs while some may have more emotional and behavioural reactions.
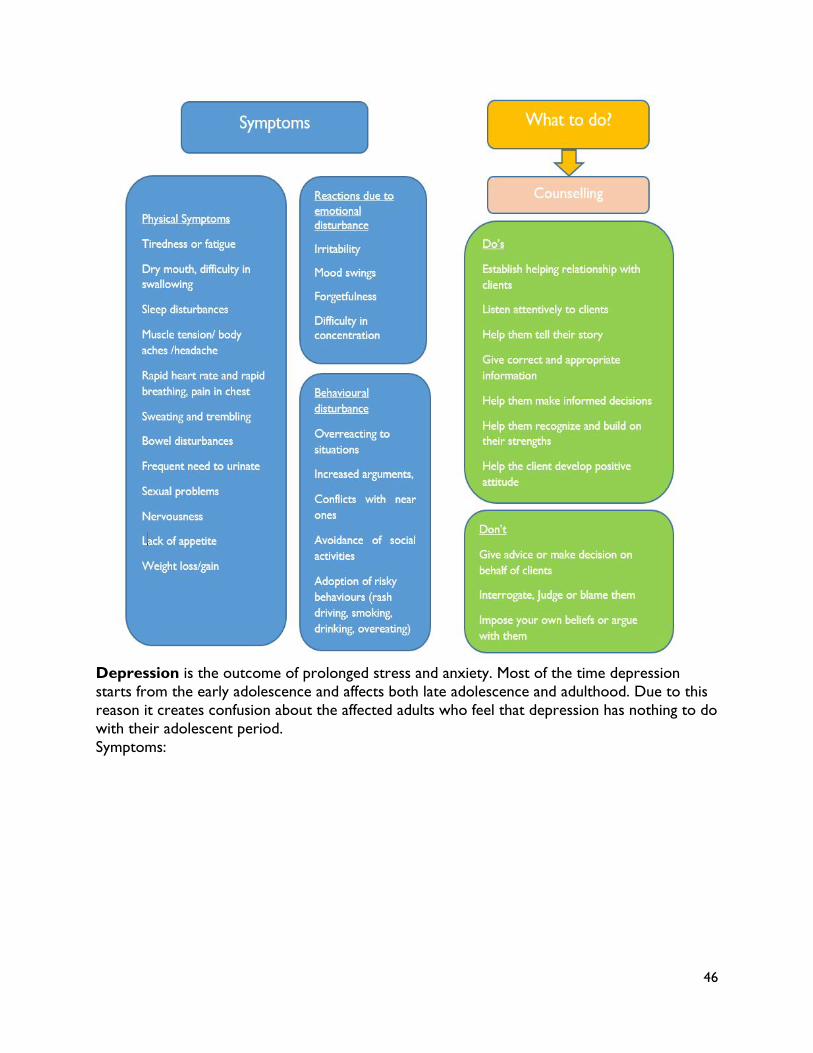
46
Depression is the outcome of prolonged stress and anxiety. Most of the time depression starts from the early adolescence and affects both late adolescence and adulthood. Due to this reason it creates confusion about the affected adults who feel that depression has nothing to do with their adolescent period. Symptoms:
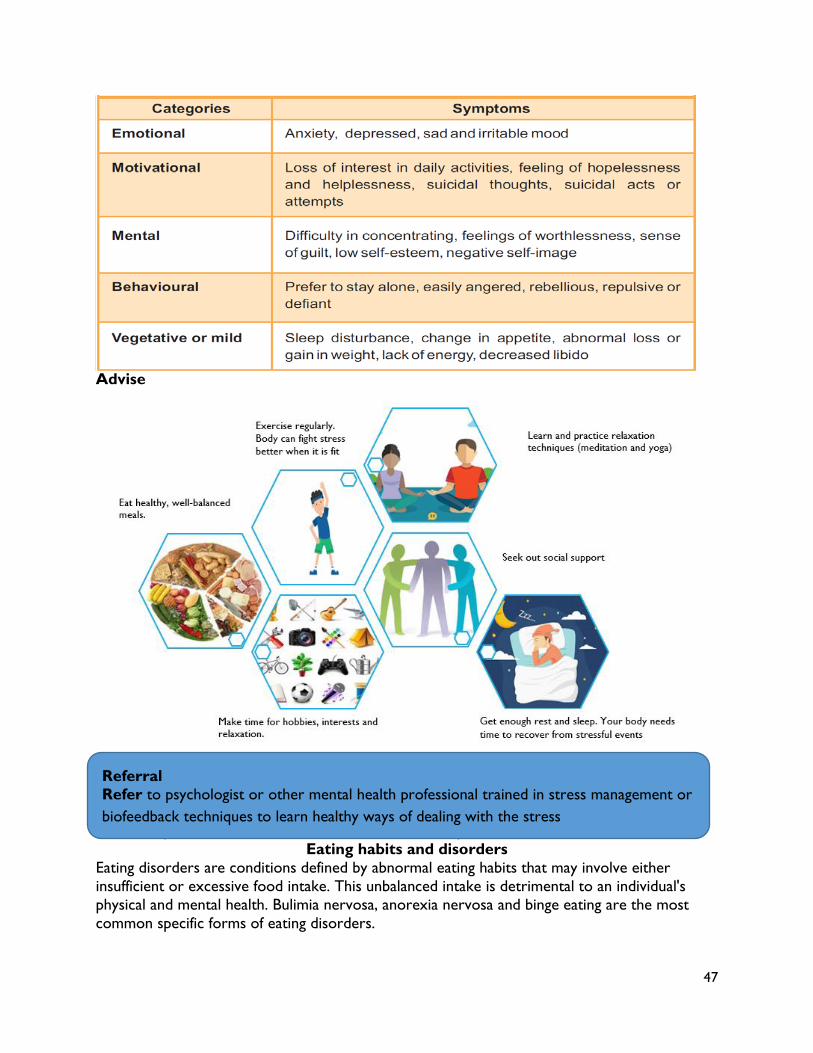
47
Advise
A follow up of the client after referral should be done by the counsellors.
Eating habits and disorders Eating disorders are conditions defined by abnormal eating habits that may involve either insufficient or excessive food intake. This unbalanced intake is detrimental to an individual's physical and mental health. Bulimia nervosa, anorexia nervosa and binge eating are the most common specific forms of eating disorders.
Referral Refer to psychologist or other mental health professional trained in stress management or biofeedback techniques to learn healthy ways of dealing with the stress
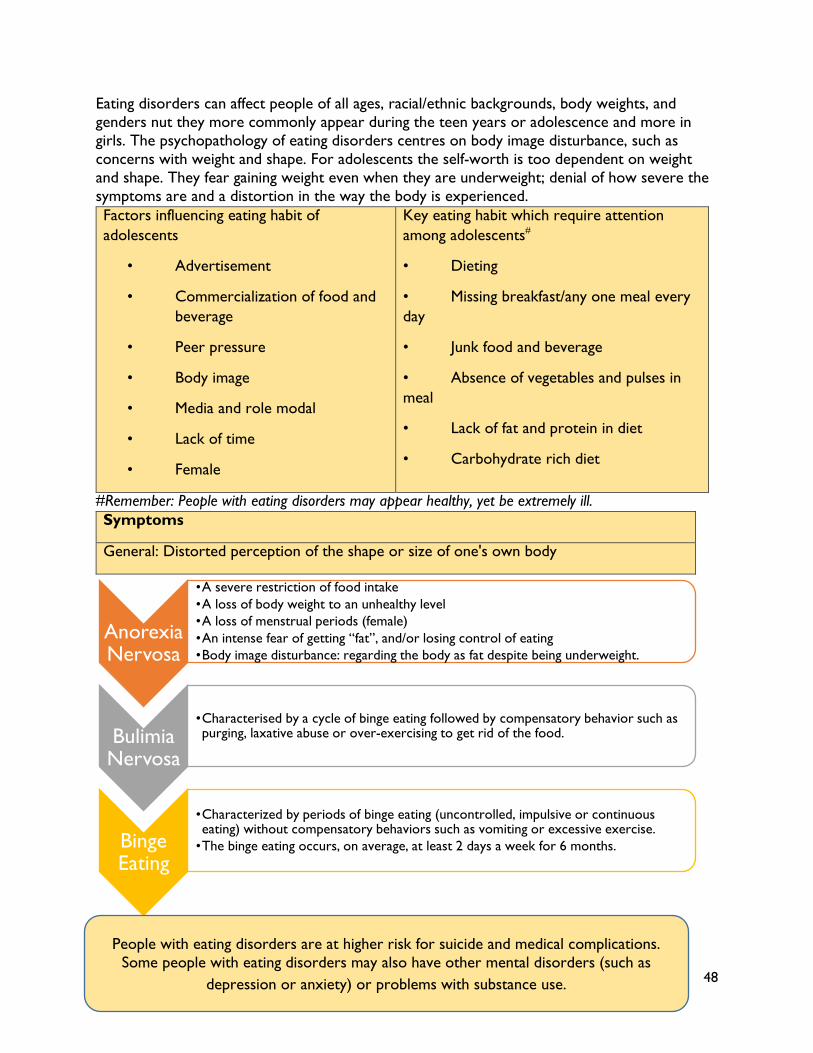
48
Eating disorders can affect people of all ages, racial/ethnic backgrounds, body weights, and genders nut they more commonly appear during the teen years or adolescence and more in girls. The psychopathology of eating disorders centres on body image disturbance, such as concerns with weight and shape. For adolescents the self-worth is too dependent on weight and shape. They fear gaining weight even when they are underweight; denial of how severe the symptoms are and a distortion in the way the body is experienced. Factors influencing eating habit of adolescents
• Advertisement
• Commercialization of food and beverage
• Peer pressure
• Body image
• Media and role modal
• Lack of time
• Female
Key eating habit which require attention among adolescents#
• Dieting
• Missing breakfast/any one meal every day
• Junk food and beverage
• Absence of vegetables and pulses in meal
• Lack of fat and protein in diet
• Carbohydrate rich diet
#Remember: People with eating disorders may appear healthy, yet be extremely ill. Symptoms
General: Distorted perception of the shape or size of one's own body
Tips for Counsellors
Anorexia Nervosa
•A severe restriction of food intake•A loss of body weight to an unhealthy level•A loss of menstrual periods (female)•An intense fear of getting “fat”, and/or losing control of eating•Body image disturbance: regarding the body as fat despite being underweight.
Bulimia Nervosa
•Characterised by a cycle of binge eating followed by compensatory behavior such as purging, laxative abuse or over-exercising to get rid of the food.
Binge Eating
•Characterized by periods of binge eating (uncontrolled, impulsive or continuous eating) without compensatory behaviors such as vomiting or excessive exercise.
•The binge eating occurs, on average, at least 2 days a week for 6 months.
People with eating disorders are at higher risk for suicide and medical complications. Some people with eating disorders may also have other mental disorders (such as
depression or anxiety) or problems with substance use.
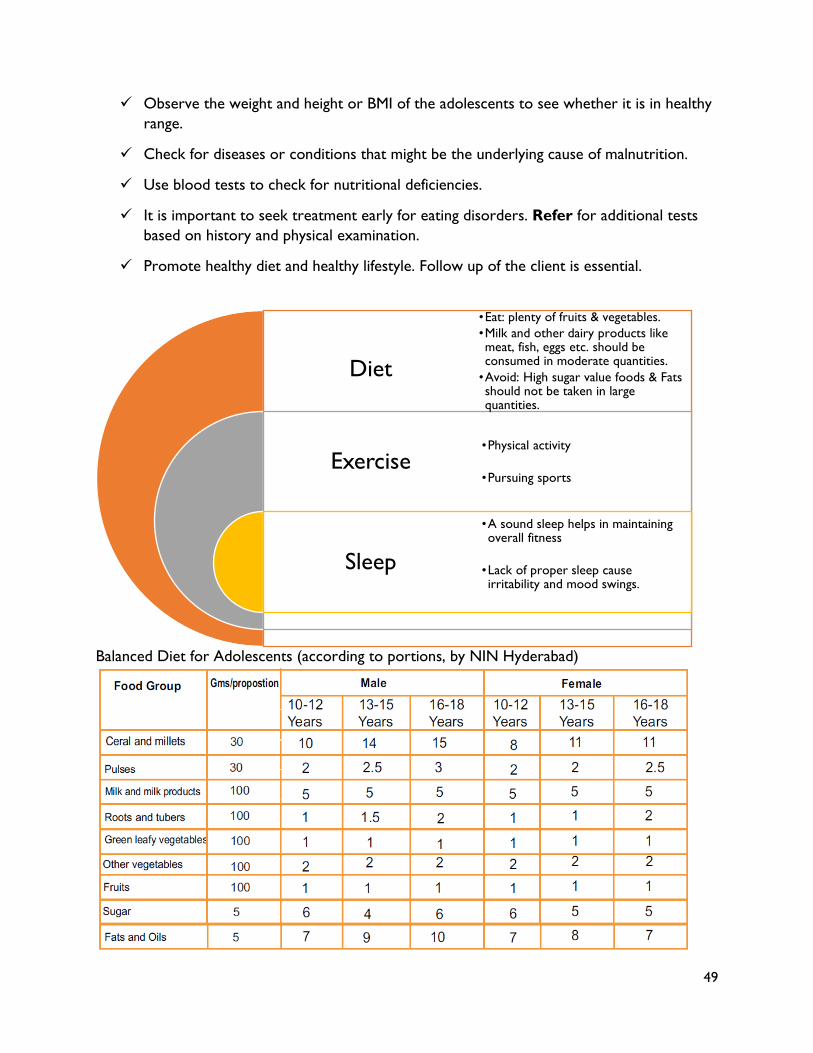
49
Observe the weight and height or BMI of the adolescents to see whether it is in healthy range.
Check for diseases or conditions that might be the underlying cause of malnutrition.
Use blood tests to check for nutritional deficiencies.
It is important to seek treatment early for eating disorders. Refer for additional tests based on history and physical examination.
Promote healthy diet and healthy lifestyle. Follow up of the client is essential.
Balanced Diet for Adolescents (according to portions, by NIN Hyderabad)
Diet
Exercise
Sleep
•Eat: plenty of fruits & vegetables.•Milk and other dairy products like meat, fish, eggs etc. should be consumed in moderate quantities.
•Avoid: High sugar value foods & Fats should not be taken in large quantities.
•Physical activity
•Pursuing sports
•A sound sleep helps in maintaining overall fitness
•Lack of proper sleep cause irritability and mood swings.
50
Anger Management Anger is the emotional response to an external or internal event perceived as a threat, a violation or an injustice. The experience of anger is learned and varies from person to person. For example, someone may cry when they feel angry while someone else may yell, while still someone else may become withdrawn. Neglecting our anger can be very harmful. Unresolved anger causes harm to health, interpersonal relationships and psychological well-being, because unresolved anger can leave in a state of perpetual emotional arousal, or make a person feel chronically helpless and hopeless. Anger management Identify triggers and the physical and emotional signs that occur when the client begin to get angry. Recognizing and managing these warning signs early is an important step in controlling anger. Stressors that commonly trigger or worsen anger, such as frustration with a partner, financial stress, traffic issues, or problems with a colleague. Physical signs that feelings of anger are rising — for example, sleeping poorly, clenching jaw, a racing heart or driving too fast. Emotional signs that anger is on the rise, such as the feeling to yell at someone or that holding in what the person really want to say. Tips for Counsellors. Advise the clients to……
• Manage factors that may make you more likely to get angry, such as improving sleep so you're not tired and keeping stress low by using stress management skills
• Identify situations that are likely to set you off and respond in nonaggressive ways before you get angry
• Learn specific skills to use in situations likely to trigger your anger
• Recognize when you aren't thinking logically about a situation, and correct your thinking
• Calm yourself down when you begin to feel upset, for example, by using relaxation skills or taking a break
• Express your feelings and needs assertively (but not aggressively) in situations that make you feel angry
• Focus on problem-solving in frustrating situations — instead of using energy to be angry, you'll learn how to redirect your energy to resolve the situation
• Communicate effectively to defuse anger and resolve conflicts
Anger management techniques: • Count to 20 before saying anything.
• Leave the room for several minutes before discussing sensitive issues that may provoke anger.
• Write out a response to a problem before tackling it orally or in debate. This will give time to think about the best approach to a problem rather than responding with random anger.
51
• Keep a diary and write about negative emotions to get them out of your system.
• Talking over situations with a trusted friend and to a therapist.
Suicidal tendency Adolescent may commit suicide as an unusual act in conditions like sudden adverse events (academic failure, death of close relation), being a victim of bullying or abuse or sexual problems. The long term anxiety or depressive disorders may trigger suicidal tendencies among adolescents. Warning signs:
• Feeling of hopelessness • Withdrawal from family or friends • Reduced sharing and discussion • Absence of concentration • Self-destructive behaviour • Lack of aspiration and loss of will power. • Sudden fluctuations of mood from happy to sad or vice-versa • Talks about suicide or death
Tips for counsellors Counsellor should talk to client's relatives/friends about: Taking the client seriously.
Not leaving the client alone.
Listening to the client and allowing him/her to express himself and herself.
Identifying the trigger event and helping the client overcome it.
Ensuring that the client stays around with people he/she feels comfortable with.
Referring to health professional.

52
Annexure 6: A Think Tank consultation to break the silence & talk about Adolescent Mental Health
Adolescent Mental Health situation in India
India is home to 253 million adolescents (Census 2011). As per data of the National Mental Health Survey of India, 2015-16- 7.3% of mental disorders are in age group 13-17 years. Nearly 9.8 million young Indians aged between 13-17 years are in need of active interventions. Prevalence of mental disorders was nearly twice (13.5%) as much in urban metros as compared to rural (6.9%) areas. There is a huge and unmet gap in mental health services, which needs immediate attention. The mental health services are often neglected and need immediate attention considering the burden of disease and treatment gap. There is a pressing need to relook at the policies, practices, approaches to reduce stigma, support system, dialogue on mental health between various stakeholders. In light of the emerging adolescent mental health issues in India, the Technical Support Unit - Adolescent Health (TSU-AH) under the USAID's flagship Maternal and Child Survival Program (MCSP), led by Jhpiego hosted the first Think Tank consultation session on Adolescent Mental Health Program - Opportunities & Addressing Challenges on 27 March 2019. The objectives of the closed group meeting were:
1. To understand the areas of contribution of various implementers on adolescent mental health 2. To map interest areas and future opportunities for adolescent mental health
The participants of this meeting included clinical practitioners, organizations working with community and school level interventions on mental health issues. The recommendations of the consultation will be shared with the Ministry of Health and Family Welfare (MoHFW) for policy level decisions.
Youth in vulnerable situations are known to have high rates of mental disorders but help seeking behavior is low. This is due to various personal and structural barriers such as stigma and concerns about confidentiality, lack of knowledge about the services, the notion that symptoms of psychological distress reflect only a temporary age crisis, and lack of appropriate responses from peers and adults.
As per World Health Organization (WHO), the common mental health conditions in India are: emotional disorders, childhood behavioral disorders, eating disorders, psychosis, suicide and self-harm and risk taking behaviors. The consequences of not addressing adolescent mental health conditions extend to adulthood, impairing both physical and mental health and limiting

53
Introduction and Context setting Dr Atul Mittal and Ms. Vandana Nair from TSU-AH welcomed the participants, facilitated a round of introduction, and set the theme and context for the session with a short audio visual of voices of youth who have undergone mental issues and availed services. “Its ok, not to be Ok”- https://youtu.be/d4clYrwK9ig Dr Bulbul Sood, Country Director, Jhpiego India, delivered the keynote address and thanked the participants. She shared that • Currently, 10% of young people are dealing with mental health issues and
there is a huge silence and lack of conversation around these issues. • It is very important to discuss and address these issues by creating an
enabling environment. There is a need for an immediate action plan to address these issues and focus on future plans.
• Use of technology and innovative scalable models should be the focus of all stakeholders working in adolescent health.
Ms Tanisha C hadha, Centre for Catalysing Change (C3) spoke about the initial emerging responses of the YouthBol Campaign. This national campaign is implemented by C3 under the USAID MCSP. • This session began with a small film on the campaign –
Make #YouthVoicesCount for Health-
https://www.youtube.com/watch?time_continue=2&v=UBg0Nv93cLA
• The campaign aims to give a clear understanding of barriers faced by adolescents and young people in accessing healthcare services. The insights of the campaign are around seven health themes.
• The offline data collection is currently underway through 30 partners covering around 22 states
• The online campaign has 10k + audience on Facebook that is rapidly growing, Instagram and twitter are growing at a slower pace, but the majority of the youth population in India, is on Facebook more than on Twitter, or Instagram, hence making this is an expected trend.
• As of 26th March 2019, 1035 online polls have been filled. Young people’s asks are largely centered on access to more information, mental health services, and wanting a peaceful and clean environment.
Dr Kushal Jain, Centre for Behavioural Sciences shared his
Dr Bulbul Sood, Country Director, Jhpiego
Ms Tanisha Chadha, Centre for Catalysing Change (C3)
Dr Kushal Jain, Centre for Behavioural Sciences
54
experiences of emerging profile of adolescent health needs from a clinical practice perspective. He shared that, • Mental health is about building resilience and contri buting to
the overall well-being of the society. The number of cases seeking medical care is the tip of the iceberg.
• The limited and existing data around Mental Health issues are very disturbing and alarming. Mental Health does not have any indicators or outcomes in form of DALY’s lost or prevented prevention of substance misuse etc.
• Currently, India has a poor Mental health workforce (per 100,000 population)- psychiatrists (0.3), nurses (0.12), psychologists (0.07) and social workers (0.07)
• A few of the challenges are: o lack of linkages with the existing health services , poor access to mental health facilities and
stigmatization of mental health professionals as compared to other specialists • There is an immediate need to strategize the approaches towards dealing with emerging mental health
issues such as addiction, gaming and risky sexual behavior • Effectiveness of current program/models should be evaluated to see if the right issues are targeted • There is a need to involve technology - digitalization of interventions Vs traditional school and
community based interventions
Dr Gracy Andrews, Corstone India Foundation shared her experiences in working with youth in Bihar at community and school settings. • She mentioned that young people have strength and are dynamic. To
empower young women, there is a need to collectively advocate for their needs
• When it comes to Mental Health- the approach that most of the stakeholders take is of the culture of the WEST i.e. addressing the issues at an individual level. . In her experience, a collective group counselling approach works better.
• The resilience-based program at Corstone, aims to measurably impact three interdependent factors in girls’ wellbeing: Emotional Health, Physical Health and Education
• This model is an evidence-based model with the pilot in Delhi and Surat, which proved the improvement of self-efficacy and built emotional resilience. Currently this model in the Scale Up phase.
• Few results of the model were that: working in small groups made real impact, resilience period is part of the school curriculum
• There is a need for enabling environment for young people and newer strategic approaches for rural and urban mental health care. Also, involvement of the parents in identifying mental health issues like emotional outbursts is of utmost importance.
Dr Ankita, Expressions India shared about her experience on skilling adolescents to deal with Mental Health issues. She said that, • Currently she is working with various schools on life skills and the newly introduced programme on
counselling services in universities.
Dr Gracy Andrews, Corstone India Foundation
Dr Ankita, Expressions India
55
• She emphasized that there is need to adopt the promotive and preventive approaches to build resilience.
• There are various modules on different thematic areas that are available but these are not implementation in most of the government schools.
• There has been an increase in the number of suicides by the students due to various reasons like poverty, parental pressure and failed/rejection in relationship.
• Moreover, the participation of parents in schools is limited to parent-teacher meetings only. Especially in rural areas due to lack of awareness and poverty.
• There is need for orientation of parents that they are equally responsible in shaping the future of the adolescents
Dr Jaya, UNFPA spoke of challenges and possible solutions to address mental health concerns. • She began with some key challenges around mental health:
o Inadequate understanding and/or triv ialization of Adolescent Concerns o Stigma associated with recognition, reporting and dealing with mental health concerns at the
level of individuals, families and institutions (including, homes, schools and health service delivery institutions)
o Limited capacities of adult care givers (for example, parents and teachers) o Inadequate trained human resources and other avenues for referral and re-dressal for mental
health concerns o Inadequate understanding of risk and protective factors
• The key recommendation was to focus on Health Promotion Rather than Disease Management through school, community and facility settings.
o Schools should advocate and prioritize to operationalize “Health Promoting Schools” o Leverage on the existing RKSK that clearly identifies mental health as a priority o Recruitment of counsellors, sustained investments in their capacities and mentorship o Investments in e-learning o Awareness among school teachers & Front Line Workers (FLWs), peer educators etc o Adequate and well-defined referral linkages with Adolescent Friendly Health Clinics o Triage by school teachers and FLWs with support from RKSK Counselors o Establish youth friendliness as a non-negotiable component of all health services o Sensitize all health staff on the relevance of addressing mental health concerns and their
specific roles • Improved Use of Appropriate Technology
o Direct Outreach to Adolescents o Well-functioning Helplines o Capacity Enhancement, Community of Learning o Monitoring Information System
Ms Arunima Gurnani, the YP Foundation shared her experience on working at the grass root level with youth.
Dr Jaya, UNFPA
56
• The major challenges with regard to mental health are: expensive treatment, lack of support system and time lag to seek care for the issue. Also, the stigma around the issue plays an important ole in seeking help.
• Various issues the adolescents have: o Lack of confidence to express gender or sexuality o Lack of assertive communication especially regarding bullying and abuse o Emotional literacy is not developed o Safe spaces for expressing their views is lacking
• She mentioned about the various reasons for pressure on adolescents from their research in Delhi (academics, comparisons with others and to behave properly according to the gender) and Lucknow (academics, marriage)
• She emphasized that there is need to build resilience both at school and at home.
Recommendations for Adolescent Health Programming in India
Based on the above deliberations, we arrived at the following areas to take notice of and draw on as we go forward: • Need to strengthen components of research, training and interventions for addressing mental
health issues among youth. • Need to break the stigma - young people want to talk and discuss about Mental Health, but
lack of safe spaces, confidentiality etc lead to low health seeking behavior • The growing up process is hard for all our young people. Issues of identity, relationships, body
image, gender, and experiences of trauma affect us all much more when we are teenagers. There is a need to understand this as youth workers and service providers, and continue to support young people through these challenging times and be empathetic.
• Creating awareness among community and parents is another key area. There is the need to recognize that bringing up children is a whole community effort whilst also acknowledging that this is not an easy fix, that trusting others is a huge commitment.
• Identifying the economic, social, and political barriers to the utilization of existing services would strengthen the delivery and utilization of these services.
• Focus should be on promotion of well-being of adolescents and leveraging strengths of young people. Could consider looking at Mental Health as the core theme and have the other RKSK themes within that.
• Adolescents who need Mental Health support/services should be provided with resources both interms of human resources and materials. While there is work happening on demand generation around Mental Health, there should be supply provision.
• Focus on the well-being of adolescents and ensure providing continuum of care – from health promotion, prevention and management as needed.
• Increase number of mental health professionals, upgradation of issues related to mental health and developing the skill sets is required among existing professionals.
Link to voices of adolescent health experts and their ASKS for Adolescent Mental Health Programming: https://youtu.be/uWqXP9Z9zD4
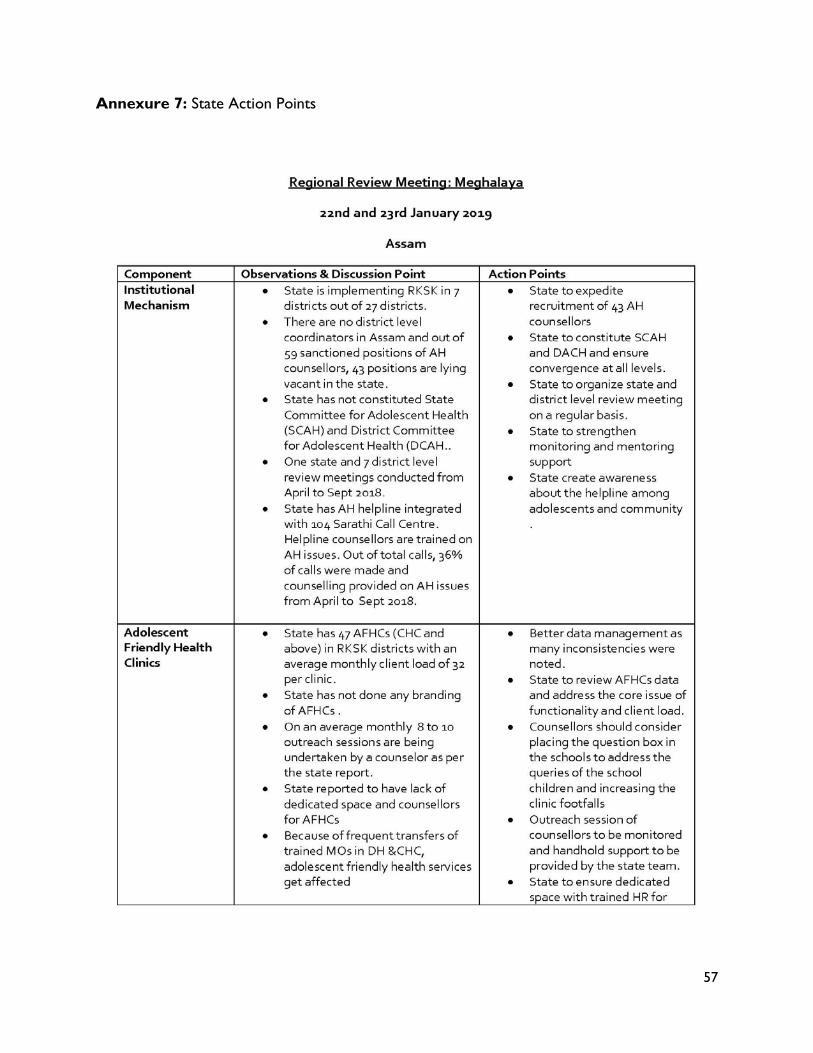
57
Annexure 7: State Action Points
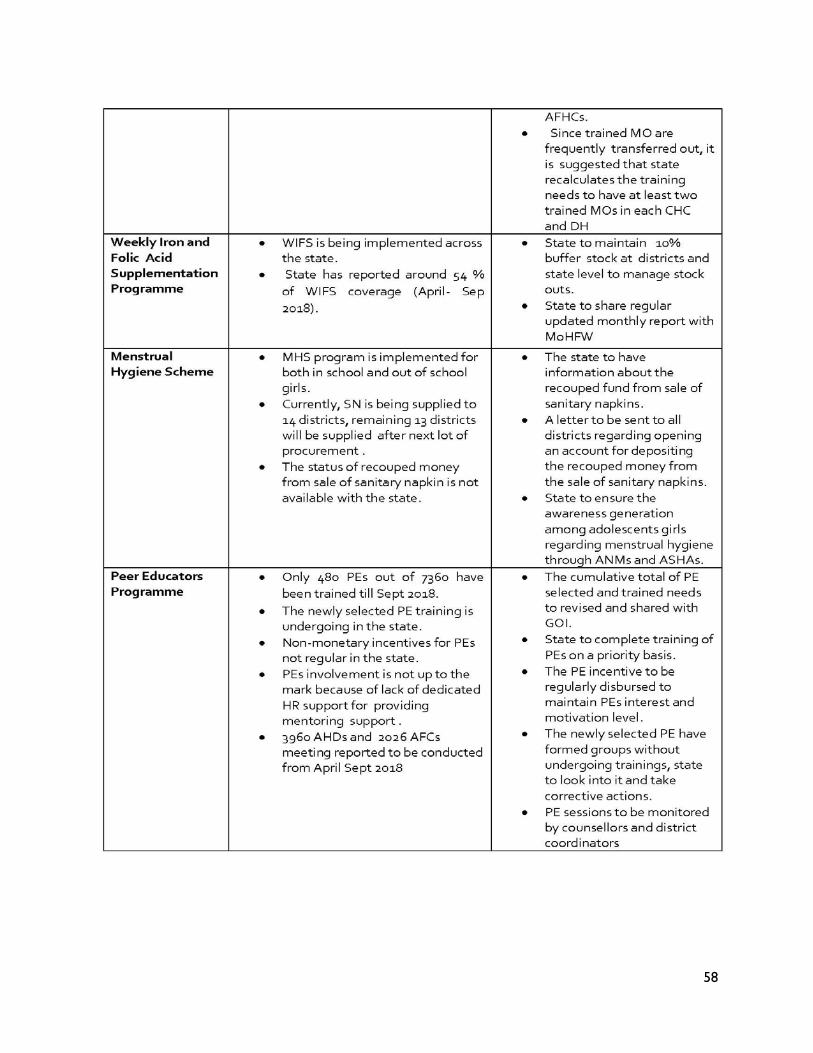
58
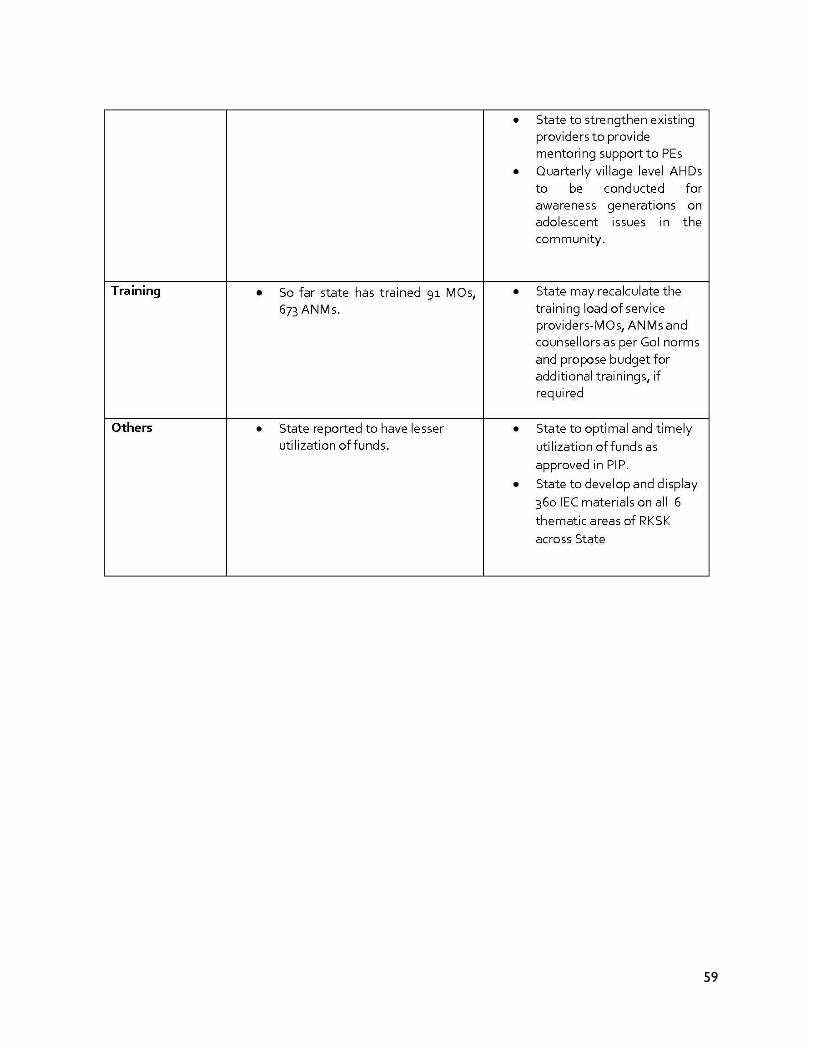
59
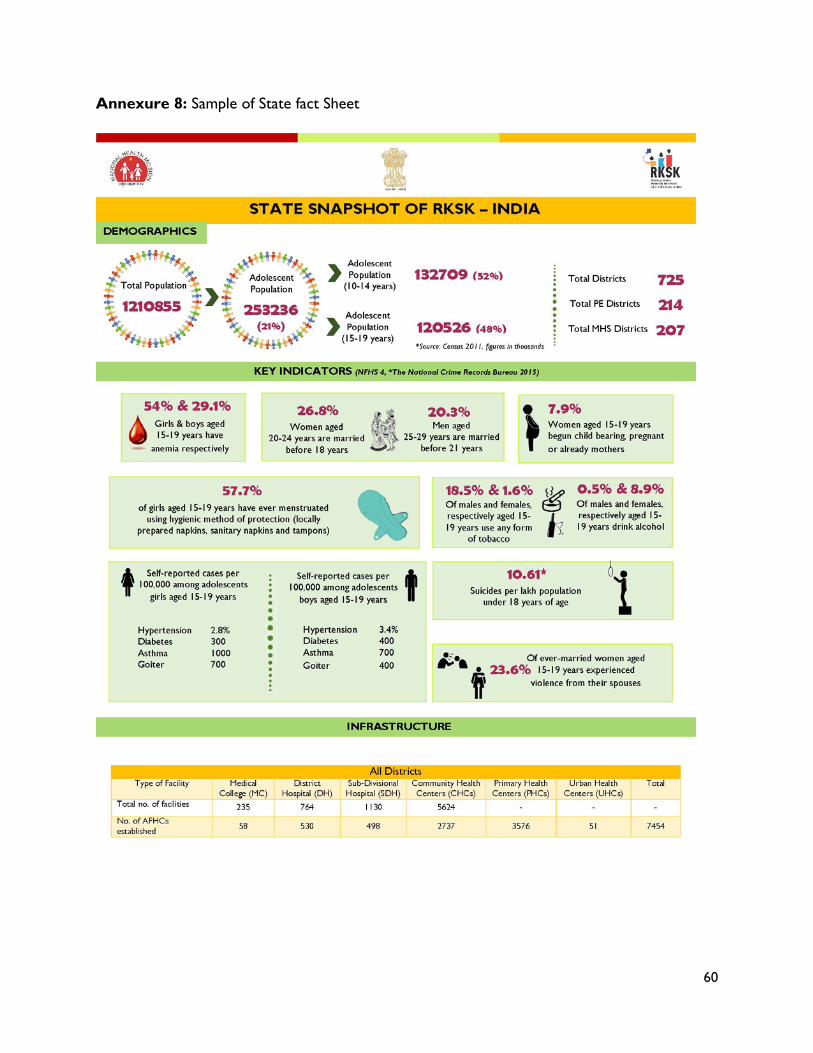
60
Annexure 8: Sample of State fact Sheet
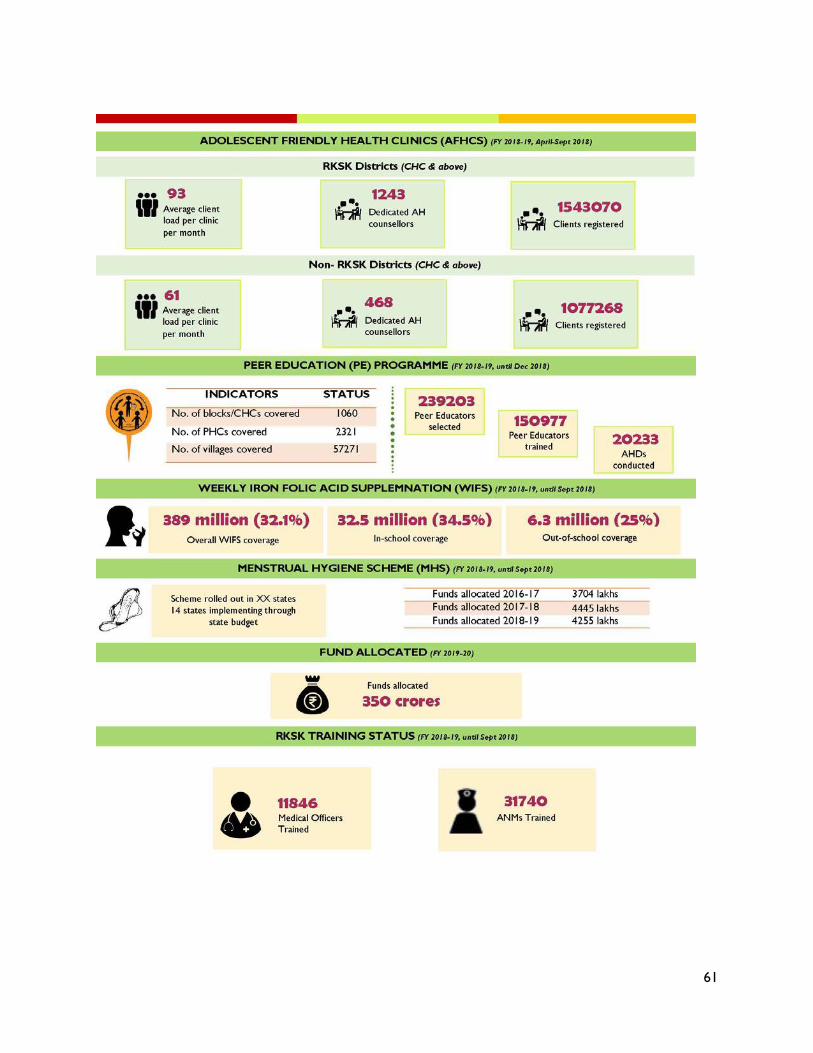
61





























