Embed Size (px)
Citation preview
ACCEPTED
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Spine Publish Ahead of Print DOI: 10.1097/BRS.0b013e3181db7456
Lumbar Scoliosis in Postmenopausal Women: Prevalence and
relationship with Bone Density, Age and Body Mass Index
Julio Urrutia, MD*, Claudio Diaz-Ledezma, MD#, Julio Espinosa, MD*,
and Sigurd H. Berven, MD+
From the *Department of Orthopaedic Surgery, Pontificia Universidad
Catolica de Chile; Marcoleta 352, Santiago, Chile
#Universidad del Desarrollo, Santiago, Chile
+Department of Orthopaedic Surgery, University of California, San
Francisco
E-mail: [email protected]
Acknowledgmnent: Jose Romeo, PhD in Statistics, Departamento de
Matematicas, Universidad de Santiago de Chile, for his assistance in
statistical analyses.
ACCEPTED
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
ABSTRACT:
Study design: Cross sectional study
Objective: The aim of this study was to investigate the prevalence of lumbar scoliosis in
post menopausal women 50 years of age and older, and to determine the association of
adult lumbar scoliosis with age, osteoporosis and body mass index.
Summary of background data: Adult scoliosis prevalence has not been clearly
determined. In addition, limited data is available on the correlation of adult scoliosis
with age, bone mineral density and body mass index.
Methods: We studied 380 postmenopausal women 50 years and older, who were
evaluated with dual-energy radiograph absorptiometry (DXA) scan images. The lumbar
curvature magnitude in the coronal plane was measured in DXA images with Cobb’s
method. Scoliosis was defined by the presence of a curvature 10° or larger. Age and T-
score in the lumbar spine and in both femoral necks were recorded, and body mass
index was calculated. Correlation analysis among the studied variables was performed,
as well as a linear regression analysis to determine the effect of femoral neck T-score,
spine T-score, age, and BMI as independent predictors of the Cobb angle in the lumbar
spine.
Results: The prevalence of lumbar scoliosis was 12.9% (49 cases); forty three cases
(11.3%) had lumbar curves 10° or more but less than 20°, and 6 cases (1.6%) had
lumbar curves more than 20°. Age and body mass index were independent predictors of
the Cobb angle; the femoral neck T-score and the lumbar T-score were not independent
predictors of the Cobb angle.
ACCEPTED
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Conclusion: We found a 12.9% prevalence of lumbar scoliosis in post menopausal
women 50 years and older, most them with mild curves. Age and body mass index are
independent predictors of lumbar scoliosis. BMD is not an independent predictor of the
magnitude of the curve.
Mini Abstract:
We studied the prevalence of lumbar scoliosis in women 50 years of age and older.
We investigated the association of adult lumbar scoliosis with age, osteoporosis and
body mass index.
The prevalence of scoliosis was 12.9%.
Age and body mass index were independent predictors of the magnitude of the curve.
Key Points:
• Adult scoliosis prevalence has not been clearly determined
• Limited data is available on the correlation of adult scoliosis with bone
mineral density and body mass index
• In postmenopausal women 50 years and older we found a 12.9% prevalence
of lumbar scoliosis
• Age and body mass index are independent predictors of lumbar scoliosis.
BMD is not an independent predictor of the magnitude of the curve.
INTRODUCTION:
Adult scoliosis is an important condition affecting the aging spine. The impact of adult
scoliosis has been previously reported, as scoliosis affecting the adult spine has a
ACCEPTED
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
significant and measurable impact on health-related quality of life (1). The prevalence
of adult scoliosis is an important measure of the overall burden of scoliosis on society,
and the prevalence has not been well-determined in population-based studies. Despite
significant advances in the surgical management of adult scoliosis (2,3), and recent
studies which have identified radiographic parameters that predict clinical symptoms
and lead to surgical treatment (4-6), a limited number of studies have been conducted
evaluating the epidemiology of this disorder.
As adult scoliosis is a common condition in the general population, with prevalence
reported with wide variability, ranging from 1.4% to 68% (7-11). The source of
variability is related to differences in definitions of scoliosis, methods of defining
cohorts, sample size, and screening tools. An accurate measure of the prevalence of
adult scoliosis is important in determining the impact of the disorder. Although many
adults with scoliosis are asymptomatic, the disorder has a significant and measurable
impact on pain, function, and quality of life in patients with symptomatic scoliosis. A
population-based study of the prevalence of this condition based on widely applied
screening tools will minimize selection bias of the cohort studied; such study could
obtain results that would better reflect the true prevalence of adult scoliosis.
DXA scanning is a routine screening study recommended for all women over age 50.
The screening tool provides an indiscriminant and non-biased sample of the population
of postmenopausal women. Several studies in adolescent idiopathic scoliosis have
correlated the degree of deformity with bone mineral density (BMD) (12,13) and body
mass index (BMI) (14-24), but few studies have evaluated the association of these
factors with adult scoliosis (9,25). Osteoporosis has been implicated in the development
ACCEPTED
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
of degenerative scoliosis in the adult, as it has been shown that patients with
osteoporosis are more likely to exhibit scoliosis (26), and it has been suggested that
mild scoliosis in the elderly is more common in patients with low femoral neck BMD,
but scoliosis was not related to age nor to vertebral BMD (27).
The purpose of this study is to determine the prevalence of adult scoliosis in post-
menopausal women 50 years old or older, and to define the relationship of adult
scoliosis with age, BMD and BMI in the same population.
METHODS:
We studied 380 postmenopausal women 50 years and older, who were evaluated with
DXA scan images, obtained at a University Hospital from January 2009. Institutional-
review board approval was obtained to conduct this study. The images were requested
as screening of bone mass loss after menopause as a part of routine clinical care,
independent of the presence of back symptoms. The lumbar curvature magnitude in the
coronal plane was measured in DXA images with Cobb’s method if a curve was present
on the anteroposterior view of the lumbar spine of the DXA scans; or between L1 and
L5 if no obvious curve was seen. Scoliosis was defined by the presence of a curvature
10° or bigger. The curvature was measured by two of the authors (JE and CD-L); in
addition, 20 of the cases were randomly chosen to determine the intra and inter observer
variability of Cobb angle measurement.
Exclusion criteria were the presence of instrumentation in the lumbar spine or bilateral
hip arthroplasty. Patients with a history of malignancy were also excluded from study.
To determine the sample size for the study, we assumed a condition with an unknown
ACCEPTED
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
prevalence. The necessary sample size with an error margin of 5% and a confidence
level of 95% was 377 cases.
Weight and height were measured using standard techniques. BMI (kg/m2) was
calculated as weight e divided by the square of the height in meters. Age, BMI, and T-
score in the lumbar spine and in both femoral necks were also recorded.
Correlation analysis (Pearson) between the presence of scoliosis and predictor
variables was performed. Linear regression analysis was performed to determine the
impact of independent variables on the presence and magnitude of spinal deformity.
Independent variables include femoral neck T-score, spine T-score, age, and BMI. A
p<0.05 was considered to be a statistically significant difference. Data was analyzed
using SPSS™ version 10 (SPSS, Chicago, IL).
RESULTS:
We studied 380 women 50 years old and older, with a median age of 59.8 years old
(range 50-90). The incidence of lumbar scoliosis was 12.9%, CI 9.77% to 16.78% (49
cases). Among the patients who had scoliosis, forty three cases (11.3%) had lumbar
curves 10° or more but less than 20°, and 6 cases (1.6%) had lumbar curves more than
20°. No cases studied showed a scoliosis curve more than 30° in the lumbar spine. The
intra-observer variability of Cobb angle measurement was 1.13 ± 0.93 degrees; the
inter-observer variability was 0.94 ± 1.01 degrees.
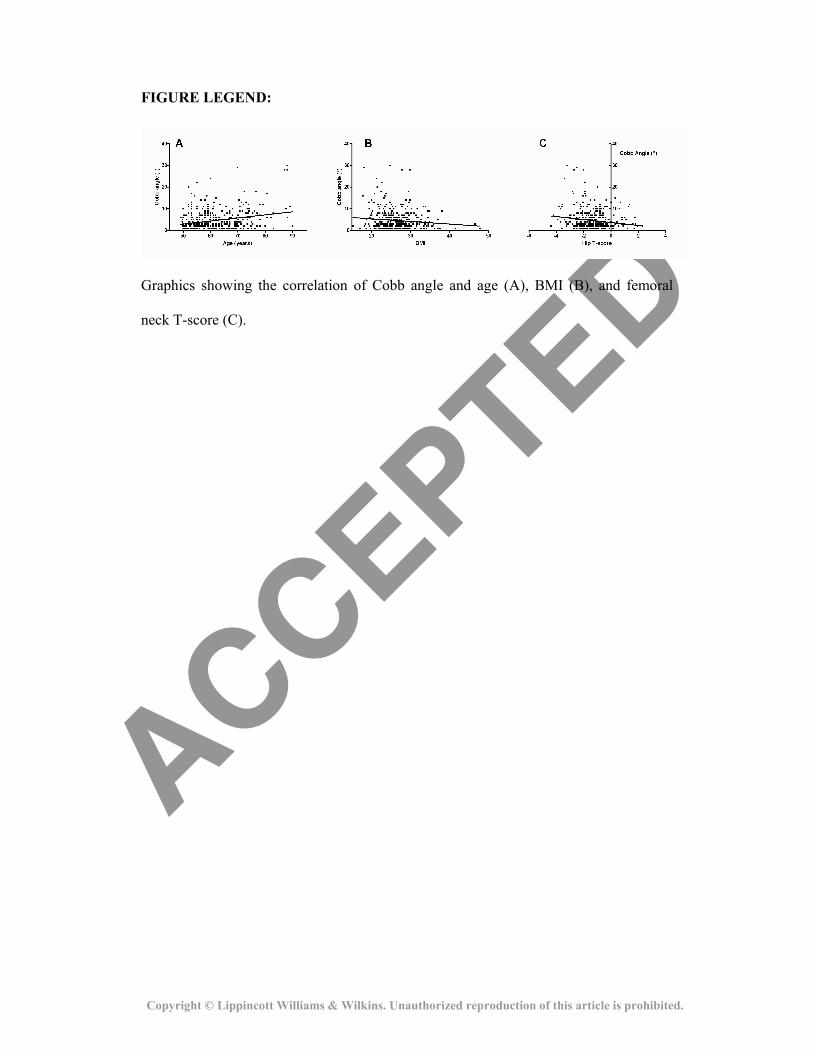
The effect of age, BMD and BMI was evaluated performing a correlation analysis,
which showed a small positive correlation of the Cobb angle with age (r= 0.26; p< 0.01)
and a small negative correlation with femoral neck T-score (r= -0.15; p< 0.01) and BMI
ACCEPTED
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
(r= -0.12; p= 0.02) (Figure). There was no correlation of the Cobb angle with the
lumbar T-score (r= - 0.44; p= 0.39).
Linear regression analysis was also done to evaluate whether each of these variables
independently affected the Cobb angle. Age (ß-coefficient= 0.146; p< 0.01) and BMI
(ß-coefficient = -0.145; p= 0.06) influenced the Cobb angle in linear regression; the
adjusted r2 value for the regression model is 0.079, and the regression equation resulted
in: expected Cobb angle = -0.592 + (0.146 x age) – (0.145 x BMI). The femoral neck T-
score (ß coefficient = -0.018; p= 0.755) and the lumbar T-score (ß coefficient= 0.053;
p= 0.308) were not independent predictors of Cobb angle.
DISCUSSION:
This study found a prevalence of lumbar scoliosis of 12.9% in women 50 years and
older, and the majority of curves were less than 20 degrees. The presence of scoliosis
was more common in patients who were older and who had a lower BMI.
Few studies have evaluated the prevalence of adult scoliosis, with rates reported from
1.4% to 68% (7-9). However, these studies have several limitations, including an
insufficient number of cases studied, different screening methods and different
populations studied, which do not allow us to raise definite conclusions on scoliosis
prevalence in adults (8). It is important that the screening method used should not
produce a bias in the sample of patients studied. Thus, any imaging study which
concentrates symptomatic patients (like radiographs obtained from a large sample of
patients) should be avoided. DXA has the advantage that is an imaging examination
ACCEPTED
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
routinely requested in most women after menopause as a screening of bone mass loss,
independent of the presence of symptoms. Few previous studies have used DXA to
determine a prevalence of scoliosis in adults (28), and our study included a cohort of
patients who represent a non-selected sample of post-menopausal women. Using DXA
for identification and measurement of scoliosis is limited to the lumbar spine; however,
DXA scan imaging obtained in a supine position has demonstrated to have an excellent
correlation (0.91) with standing antero-posterior lumbar radiographs (9); in addition, in
our study we observed a very small intra and inter-observer variability in measurement
of the Cobb angle in DXA scan imaging. Even the standard determination of Cobb
angle in antero-posterior radiographs of the spine has been associated to a measurement
error up to three to five degrees, but any small error in measurement may be significant
as most patients with scoliosis in our study had curvatures between 10 and 20 degrees.
Adult scoliosis may represent a new-onset (degenerative) deformity or a preexisting
adolescent idiopathic scoliosis that progresses into adulthood. Older patients should
have a higher prevalence of lumbar deformity because spinal degeneration, which has
been implicated in the development of degenerative scoliosis, advances with age (8,29-
31). In addition, patients with adolescent idiopathic scoliosis can continue their curve
progression during adulthood (32). Our study showed that age and BMI were
independent predictors of the magnitude of the curve, such that scoliosis was more
common in older patients with a lower BMI. The analyses of our data, however, show
that these variables have a low effect (although significant) over the magnitude of the
curve, and 7.9% of the variance in Cobb angle can be explained by the regression
model. There was no independent association between scoliosis and bone density in
this study.
ACCEPTED
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Previous studies in adolescent idiopathic scoliosis have shown that girls with idiopathic
scoliosis have a lower BMI than age matched controls (14-24). These publications agree
with our results, which show that lower BMI is an independent predictor of the presence
of scoliosis in adults. No previous studies have demonstrated an association of low BMI
and adult scoliosis.
Adult scoliosis and osteoporosis are associated with advancing age, and are found
simultaneously in many aging patients. (30,33) Nonetheless, the effect of osteoporosis
on the development of adult scoliosis, or the effect of scoliosis on the development of
osteoporosis is not demonstrated in this study. Some reports suggest that scoliosis
predisposes to osteoporosis (34,35), while other authors suggest that osteoporosis
predisposes to scoliosis (27), or that there is no correlation (29,36). Previous studies
have shown that adult scoliosis in the lumbar spine is associated to low femoral neck
BMD but not to low vertebral BMD (9,27). Another study showed that adult women
with scoliosis had a lumbar BMD similar to young women and above age-matched
controls, but their femoral neck BMD was within normal range for the patients’ age.
(37) A recent study, with a similar methodology to our study, also showed that adult
scoliosis had a negative correlation to femoral neck T-score and a positive correlation
with lumbar T-score (38). Adolescent idiopathic scoliosis, in contrast, has been
associated with a lower vertebral BMD (39-42); these different results among
adolescent idiopathic scoliosis and adult scoliosis may be explained as spinal
degeneration would falsely increase lumbar BMD measurements in DXA scans (43).
Although we found a mild negative correlation of femoral neck T-score and lumbar
curve, when we adjusted for age and BMI in our linear regression model, femoral neck
ACCEPTED
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
T-score was not an independent determinant of the presence of scoliosis. These results
suggest that the negative correlation of the femoral neck T-score with the lumbar
curvature would depend on the effect of age and BMI over the femoral neck BMD.
Although osteoporosis and adult lumbar scoliosis are usually found in the same
populations, from our results it is unlikely that osteoporosis itself is a major determinant
of adult lumbar scoliosis as it has been suggested.
Adult scoliosis is an important condition affecting the aging spine. With an aging
population, it is important to identify factors that are associated with the development of
spinal deformity and the progression of deformity. This study demonstrates a small
effect of advancing age and low BMI on the development of scoliosis; bone mineral
density values were not independent predictors of adult scoliosis. Further studies may
include population-based screening of patients with non-radiographic methods, or
identification of other reversible factors that may be associated with the development
and progression of adult scoliosis.
REFERENCES:
1. Berven S, Deviren V, Demir-Deviren S, et al. Studies in the modified Scoliosis
Research Society Outcomes Instrument in adults: validation, reliability, and
discriminatory capacity. Spine (Phila Pa 1976) 2003;28:2164-9; discussion 9.
2. Bridwell KH. Selection of instrumentation and fusion levels for scoliosis: where
to start and where to stop. Invited submission from the Joint Section Meeting on
Disorders of the Spine and Peripheral Nerves, March 2004. J Neurosurg Spine
2004;1:1-8.
ACCEPTED
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
3. Bridwell KH, Berven S, Edwards C, 2nd, et al. The problems and limitations of
applying evidence-based medicine to primary surgical treatment of adult spinal
deformity. Spine 2007;32:S135-9.
4. Glassman SD, Berven S, Bridwell K, et al. Correlation of radiographic
parameters and clinical symptoms in adult scoliosis. Spine 2005;30:682-8.
5. Glassman SD, Bridwell K, Dimar JR, et al. The impact of positive sagittal
balance in adult spinal deformity. Spine 2005;30:2024-9.
6. Schwab F, el-Fegoun AB, Gamez L, et al. A lumbar classification of scoliosis in
the adult patient: preliminary approach. Spine 2005;30:1670-3.
7. Grevitt M, Khazim R, Webb J, et al. The short form-36 health survey
questionnaire in spine surgery. J Bone Joint Surg Br 1997;79:48-52.
8. Schwab F, Dubey A, Gamez L, et al. Adult scoliosis: prevalence, SF-36, and
nutritional parameters in an elderly volunteer population. Spine 2005;30:1082-5.
9. Pappou IP, Girardi FP, Sandhu HS, et al. Discordantly high spinal bone mineral
density values in patients with adult lumbar scoliosis. Spine 2006;31:1614-20.
10. Kostuik JP, Bentivoglio J. The incidence of low-back pain in adult scoliosis.
Spine 1981;6:268-73.
11. Perennou D, Marcelli C, Herisson C, et al. Adult lumbar scoliosis.
Epidemiologic aspects in a low-back pain population. Spine 1994;19:123-8.
12. Li XF, Li H, Liu ZD, et al. Low bone mineral status in adolescent idiopathic
scoliosis. Eur Spine J 2008;17:1431-40.
13. Sadat-Ali M, Al-Othman A, Bubshait D, et al. Does scoliosis causes low bone
mass? A comparative study between siblings. Eur Spine J 2008;17:944-7.
ACCEPTED
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
14. Siu King Cheung C, Tak Keung Lee W, Kit Tse Y, et al. Abnormal peri-pubertal
anthropometric measurements and growth pattern in adolescent idiopathic
scoliosis: a study of 598 patients. Spine 2003;28:2152-7.
15. Archer IA, Dickson RA. Stature and idiopathic scoliosis. A prospective study. J
Bone Joint Surg Br 1985;67:185-8.
16. Buric M, Momcilovic B. Growth pattern and skeletal age in school girls with
idiopathic scoliosis. Clin Orthop Relat Res 1982:238-42.
17. Leong JC, Low WD, Mok CK, et al. Linear growth in southern Chinese female
patients with adolescent idiopathic scoliosis. Spine 1982;7:471-5.
18. Nordwall A, Willner S. A study of skeletal age and height in girls with
idiopathic scoliosis. Clin Orthop Relat Res 1975:6-10.
19. Normelli H, Sevastik J, Ljung G, et al. Anthropometric data relating to normal
and scoliotic Scandinavian girls. Spine 1985;10:123-6.
20. Skogland LB, Steen H, Trygstad O. Spinal deformities in tall girls. Acta Orthop
Scand 1985;56:155-7.
21. Willner S. Growth in height of children with scoliosis. Acta Orthop Scand
1974;45:854-66.
22. Willner S. The proportion of legs to trunk in girls with idiopathic structural
scoliosis. Acta Orthop Scand 1975;46:84-9.
23. Carr AJ, Jefferson RJ, Weisz I, et al. Correction of body height in scoliotic
patients using ISIS scanning. Spine 1989;14:220-2.
24. Smith FM, Latchford GJ, Hall RM, et al. Do chronic medical conditions increase
the risk of eating disorder? A cross-sectional investigation of eating pathology in
adolescent females with scoliosis and diabetes. J Adolesc Health 2008;42:58-63.
ACCEPTED
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
25. Lunt M, Felsenberg D, Reeve J, et al. Bone density variation and its effects on
risk of vertebral deformity in men and women studied in thirteen European
centers: the EVOS Study. J Bone Miner Res 1997;12:1883-94.
26. Vanderpool DW, James JI, Wynne-Davies R. Scoliosis in the elderly. J Bone
Joint Surg Am 1969;51:446-55.
27. Thevenon A, Pollez B, Cantegrit F, et al. Relationship between kyphosis,
scoliosis, and osteoporosis in the elderly population. Spine 1987;12:744-5.
28. Voros G. NP, Khoshnevisan M. et al. . Prevalence of Scoliosis in Adults Age 40
years and Older: A Study of 2973 Individuals. Spine J 2007;7:1S-2S.
29. Robin GC, Span Y, Steinberg R, et al. Scoliosis in the elderly: a follow-up study.
Spine 1982;7:355-9.
30. Daffner SD, Vaccaro AR. Adult degenerative lumbar scoliosis. Am J Orthop
2003;32:77-82; discussion
31. Benoist M. Natural history of the aging spine. Eur Spine J 2003;12 Suppl 2:S86-
9.
32. Collis DK, Ponseti IV. Long-term follow-up of patients with idiopathic scoliosis
not treated surgically. J Bone Joint Surg Am 1969;51:425-45.
33. Healey JH, Lane JM. Structural scoliosis in osteoporotic women. Clin Orthop
Relat Res 1985:216-23.
34. Velis KP, Healey JH, Schneider R. Osteoporosis in unstable adult scoliosis. Clin
Orthop Relat Res 1988:132-41.
35. Carter OD, Haynes SG. Prevalence rates for scoliosis in US adults: results from
the first National Health and Nutrition Examination Survey. Int J Epidemiol
1987;16:537-44.
ACCEPTED
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
36. Robin GC. Scoliosis in the elderly: idiopathic or osteoporotic? Clin Orthop Relat
Res 1986:311-2.
37. Rumancik S, Routh RH, Pathak RD, et al. Assessment of bone quantity and
distribution in adult lumbar scoliosis: new dual-energy x-ray absorptiometry
methodology and analysis. Spine 2005;30:434-9.
38. Neubauer P. VG, Riley L. et al. . Is There a Relationship Between Scoliosis
Prevalence and Osteoporosis? A Study of 2973 Individuals. Spine J
2009;9:167S-8S.
39. Cook SD, Harding AF, Morgan EL, et al. Trabecular bone mineral density in
idiopathic scoliosis. J Pediatr Orthop 1987;7:168-74.
40. Cheng JC, Guo X. Osteopenia in adolescent idiopathic scoliosis. A primary
problem or secondary to the spinal deformity? Spine 1997;22:1716-21.
41. Cheng JC, Qin L, Cheung CS, et al. Generalized low areal and volumetric bone
mineral density in adolescent idiopathic scoliosis. J Bone Miner Res
2000;15:1587-95.
42. Cheng JC, Tang SP, Guo X, et al. Osteopenia in adolescent idiopathic scoliosis:
a histomorphometric study. Spine 2001;26:E19-23.
43. Rand T, Seidl G, Kainberger F, et al. Impact of spinal degenerative changes on
the evaluation of bone mineral density with dual energy X-ray absorptiometry
(DXA). Calcif Tissue Int 1997;60:430-3.
ACCEPTED
Copyright © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
FIGURE LEGEND:
Graphics showing the correlation of Cobb angle and age (A), BMI (B), and femoral
neck T-score (C).





























