Embed Size (px)
Citation preview
INTERGRATINGMORITATHERAPYANDARTTHERAPY:ANANALYSIS
ADissertation
PresentedtotheFacultyofAntiochUniversitySeattle
Seattle,WA
InPartialFulfillmentoftheRequirementsoftheDegreeDoctoralofPsychology
By
AyakoSato
January2011
COMBININGMORITATHERAPYANDARTTHERAPY:ANANALYSIS
Thisdissertation,byAyakoSato,hasbeenapprovedbythecommitteememberssignedbelowwhorecommendthatitbeacceptedbythefacultyof
AntiochUniversitySeattleinSeattle,WAinpartialfulfillmentofrequirementsforthedegreeof
DOCTOROFPSYCHOLOGY
DissertationCommittee:________________________LiangTien,Psy.D.Chairperson________________________MinoruOishi,M.D.________________________JaneHarmonJacobs,Ph.D.________________________Date
ii

©CopyrightbyAyakoSato,2011
AllRightsReserved
iii
ABSTRACT
INTEGRATINGMORITATHERAPYANDARTTHERAPY:AnAnalysis
AyakoSato
AntiochUniversitySeattle
Seattle,WA ThisstudypresentstherapeuticinterventionscombiningMoritaTherapywithart
therapytechniques.Theauthorpresentsliteraturereviewsofarttherapyaswellasthe
originalMoritaTherapyformulatedbyShomaMorita,M.D.Anewarttherapy
techniquebasedontheworkofKenjiKitanishi,M.D.(2008)foroutpatienttreatmentis
alsopresented.Acaseillustrationofaneleven‐year‐oldVietnamese‐Americanboywho
presentedwithhighanxietyandschoolrefusalisusedasanexampleoftheeffective
integrationofMoritaTherapywitharttherapytechniquesformulatedbytheauthor.
EventhoughtheboywasnotfamiliarwithMoritaTherapyprinciples,thecreative
processhelpedtheclientmaketherapeuticprogress.Thecombinedtreatmentof
MoritaTherapyprinciplesandarttherapytechniquesresultedinaneffectiveoutcome
fortheclient.Asacentralconcept,MoritaTherapyfocusesonlearningtoacceptone’s
emotionsandtherealityofone’slife.Thisanalysisconcludesthatarttherapy
techniquescanbeeffectivelyintegratedwithMoritaTherapyasatreatmentmethod
aimedatimprovementinfunctioning.Thenumberofclientsthatcanpotentially
benefitfromMoritaTherapyincreaseswiththeuseofarttherapy.
1

GiventhatMoritaTherapyisbasedonBuddhistphilosophy,itmaybeparticularlyuseful
Buddhistbasedcultures.
2
DEDICATION
Iwouldliketodedicatethisdissertationwithmywholeheartandlovetomy
parentsandmychildren.Mymotherinstilledinmetheimportanceofwomenpursuing
highereducationandindependence,breakingwithtraditionalJapaneseculture.
Throughmyfather’scompassion,perseveranceandpositiveworkethicsofnevergiving
up,Ilearnedtobediligentandaffectionate.Mychildren,YukoandYusuke,enriched
mylifebytheirwillingnesstofollowmeinlivinginthetotallydifferentcultureofthe
UnitedStatesfortheelevenyearsofmyprofessionaljourney.Iwillneverforgettosay
thankstoDr.IkuoTakahashiforbeingmymentorandmajorsupportformyacademic
journey.
iv
ACKNOWLEDGEMENTS
Iwouldliketoexpressthedeepestappreciationtomydissertationcommittee
chair,Dr.LiangTien,whohadastrongpassionandtheskilltoeducatemeasa
psychologistthroughthisdissertationprocess.Asarespectfulprofessor,personal
mentor,andintelligentAsian‐Americanwoman,sheprovidedapowerfulrolemodel.I
wouldalsoliketothankmycommitteemembers,MinoruOishi,MD.andJaneHarmon
Jacobs,Ph.D.IappreciateDr.Oishi’swillingnesstoparticipatefromJapan.Asa
medicaldoctor,hisknowledgeandclearopinionshelpedmythinkinginthisdifficult
project.Dr.Jacobs’continuingencouragement,professionalperspective,andfaithin
myabilityhelpedmepersevereinthiscourseofstudy.
Inaddition,IappreciateMarkYamada,Ph.D.,whoismyclinicalsupervisor,and
AndyBenjamin,Ph.D.IrespectDr.Yamada’swisdom,knowledge,andtenacious
commitmenttoeducationandclinicalsupport.Iwouldhavebeenunabletocomplete
mystudieswithoutDr.Benjamin.Hiswisdomandprofessionalattitudegavemea
modelofhowtolivemyprofessionallifeinthefuture.
IwouldalsoliketoexpressmygratitudetoPatriciaLinn,Ph.D.,JudithA.Rubin,
Ph.D.,andthefacultyofAntiochUniversitySeattlefortheirtime,encouragement,and
love.
v
Ofcourse,manythankstomystrongsupporters:Mr.MisaoandMs.Masako
Yazaki,andtomymanyfriendsandprofessorsintheU.S.andJapan.Especially,I
appreciateMs.Yuko,Mr.HitoshiChiba,Mr.ShojiOshio,Ms.RyokoNabetani,and
Ms.ChiekoKimurawhohavegivenmesupporttopursuemyeducation.
IalsothankmyEnglishtutorMr.JohnNewmanandeditorDr.ResaRaven,who
nevercomplainedaboutmypersistentquestions.
Lastbutnotleast,Iappreciatemyex‐husband,Mr.TakahiroAkita.IfIhadnot
marriedhim,IwouldnotbewhereIamtoday.Thankyoutoallofmypeople.Arigatou.
vi
TABLEofCONTENTSPageDEDICATION…….……………………………………………………………………………………ivACKNOWLEDGMENT…………………………………………………………………………….vListofTables……………………………………...........…………………………………………ixListofFigures……………………………………….………………………………………………xI.WHATISARTTHERAPY?..............................................................................1
Definitions…………………………………………………………………………………………….....…2WhatIsArtTherapy?………………………………………………………………………….….......6UsefulnessofArtTherapy……………………………………………………………………….....12ThePlaceofPsychologicalTheoryinTherapy………………………………………….....15ArtTherapyandTheory………………………………………………………………………….…..16ArtTherapyasAssessment………………………………………………………………………….17ArtandCulture………………………………………………………………………………………..….20ZenArtUsedinHealing………………………………………………………………………….......22
II.THEORETICALHISTORYOFARTTHERAPY…………………………………………..………..26 ArtTherapyandTheories……………………………………………………………………….…….26
TheoreticalHistoryofArtTherapy………………………………………………………….…….26ChoiceofTheory………………………………………………………………………………….….……30AdvantageofIntegratingArtTherapywithTheory…………………………………..…..31 PossibleIntegrationofMoritaTherapyandArtTherapy……………………………...31
III.MORITATHERAPY…………………………………………………………….……………….....33ConceptofMoritaTherapy……………………………………………………..…………………...33 HistoryofMoritaTherapy…………………………………………………….……..……….………35Morita’sChildhoodExperiences………………………………………….…………..…..……….36BirthofMoritaTherapy…………………………………………………….………………..………..37HowMoritaTherapyViewsPathology……………………………………………………..…..39TheCoreofMoritaTherapyPathology:ViciousCircleofConflictingThoughts……………………………….…………...40AnxietyandDesire…………………………………………………………………….…………..……...45NatureTheory……………………………………………………………………………..…………….....46CorePrinciplesofMoritaTherapy…………………………………….……………….……….....47
vii

Psychopathology………………………………………………….…………………………….………....52MoritaTherapyandBuddhism………………………………………………………….…………...56MoritaTherapyandWesternPsychology………………………………………….…………..57Modalities………………………………………………………………………………………….…….......58Treatments………………………………………………………………………………….…….………....59PossibilitiesofMoritaTherapyinWesternCulture…………………………..……………64MoritaTherapyPastandPresent…………………………………………………….……..…....66
IV.ANALYTICALPERSPECTIVEOFMORITATHERAPY.…………………………………………..……….68
BackgroundConsiderationsRegardingMoritaTherapy………………………………….68MoritaTherapyandMedication…………………………………………………………………....69AnalyticalIssuesoftheOriginalMoritaTherapy…………………………………………....69EnvironmentofMoritaTherapy……………………………………………………………………...69IssuesRegardingtheInpatientUnitatMorita’sHome…………………………………...71RelationshipBetweenClientsandClinicians…………………………………………………..73
DifficultyUnderstandingMoritaTherapy……………………………………………………….76AfterMorita…………………………………………………………………………………………………...83MoritaTherapyToday………………………………………………………………………………….…84Conclusion………………………………………………………………………………………………........84
V.THEINTEGRATIONOFMORITATHERAPYWITHARTTHERAPY………………………………..87 ExampleofArtTherapyInterventionTechnique…………………………………………….89
CaseSummary…………………………………………………………………………………………….…106
VI.Conclusions…………………………………….…………………………………………………………..……….109References………………………………………………………………….…………………………..…………………112
viii
ListofTables
1. ContextandHistoryMoritaTherapy.........................................................................86
ix

ListofFigures
PageFigure1:ViciousCircleofConflictingThoughts………………………………………….……..…….41Figure2:DiscrepancyBetweenImaginaryandRealSelf…………………………….……...…….43Figure3:SummaryoftheViciousCircleofConflictingThoughts……………………..….…..45Figure4:TheConnectionBetweenAnxietyandDesire……………………………….….…....…46Figure5:DifferencesBetweenBuddhismandWesternPhilosophy……………..….……...58Figure6:ChangingImpactofExternalEvaluation………………………………..……….……….….64Figure7:DistinguishingBetweenICanDoItandICan’tDoIt…………………..………….....89Figure8:AdmittingVersusFightingEmotions……………………………………….…...…………….90Figure9:HoldingtheEmotions……………………………………………..……….……….….…….………91Figure10:HoldingtheEmotions‐2………………………………….….………….……….….…….………91Figure11:ObservingDynamicEmotions……………………………….……………….…...…………….92Figure12:RecognizingDynamicEmotions…………………………….…….……….…………………...92Figure13:ObservingtheBehavior……………………………….…………….…….…………….………….93Figure14:TakingActionandHavingExperiences…………….………..……………………………...93Figure15:MakingDecisions………………………………………………….…….…………….……….……...94Figure16:AvoidingPerfectionism………………………………….………….………….…………….……..95Figure17:ActionsChangeEmotions……………………………….………….………….………….……….95Figure18:FeelingEnoughEnergytoLive……………………….……………………………….….……….96
x
Figure19:IdentifyingExternalJudgments……………………………………………………….………….96Figure20:RecognizingtheImpactofExternalJudgments.............................................97
Figure21:ChangingtheImpactofExternalJudgments.................................................98Figure22:Alex’sFamily.................................................................................................101
Figure23:Alex’sPictureofSelf.....................................................................................102
Figure24:Mother’sPictureofSelf...............................................................................102
Figure25:AnxietyTemperatureIndicators1...............................................................103
Figure26:MyUncle......................................................................................................104
Figure27:Alex’sActions...............................................................................................105
Figure28:AnxietyTemperatureIndicators2...............................................................107
xi
1
I.WHATISARTTHERAPY?
ShomaMoritawhoformulatedMoritaTherapyin1917,focusedonaccepting
life,resolvingconflictingthoughts,andbecomingfreefromobsession(France,Cadieax,
&Allen,1995).Moritabelievedthatitismucheasierforpeopletochangetheir
behavior/actionthantochangetheirsymptoms(Kitanishi,2007).MoritaTherapy
stemsfromZenBuddhism.MoritaTherapymaybeagoodfitformanyclients,
particularlythosefromBuddhist‐basedcultures.WithinterestinZenpracticegrowing
beyondAsia,MoritaTherapymayalsobehelpfulforindividualsfromWesterncultures.
ArttherapyintheUnitedStateshasbeeninfluencedbyanarrayofWestern
theories,buthasnotbenefitedfromBuddhist‐basedculturalinfluences.Western
influenceshaveincludedFreudianpsychology,theeducationalmovement,andart
education(Jung,1994).Anarttherapyapproachisfrequentlyusedtoclarifyand
expressanindividualpatient’semotionsandtofacilitatethefindingofsolutionstotheir
problems(Rubin,1998,2001,2005).Throughtheprocessofmakingart,atherapeutic
dialoguebetweenpatientandarttherapistiscreated.Arttherapythenbecomesa
guidetoleadapersontohisorhergoals.
Asadiscipline,arttherapydoesnothaveonecompellingtheorysupportingits
techniques.Rather,arttherapyisoneoftheapproachesthatcanbeusedtosupport
treatmentgoalsinalargercontext.Thisrequiresthearttherapisttointegrateart
therapytechniqueswiththetheoreticalorientationthatguidesthetherapist’sthinking.
IntegratingMoritaTherapyandarttherapymaybeaneffectivetherapeuticmethodto
2
helpanindividualpatientunderstandtheiremotionsandgaininsightintotheir
functioning.ThispaperexploresthepossibleintegrationofarttherapywithMorita
Therapy.
TherearenostudiesordiscussionsofintegratingMoritaTherapyandarttherapy
inWesternpsychologicalliterature.TheintegrationofMoritaTherapyandarttherapy
byAmericanarttherapistshasyettobepursued.Thisdoctoralpaperwillexplorethat
possibility.Insectiononeandtwo,Iwillreviewthecurrentstateoftheliterature
regardingarttherapyandtheoreticalhistoryofarttherapyintheUnitedStates.In
sectionthree,IwilloutlineMoritaTherapyasoriginallypromulgatedbyDr.Shoma
Morita.Insectionfour,IwilldiscusstheanalyticalperspectiveofMoritaTherapy.In
sectionfive,IwillillustrateamethodofintegratingMoritaTherapyforoutpatient
treatmentwhichisbasedonKitanishi’sidea(2008)ofarttherapy.Acasestudyexample
willbepresentedtodemonstrateconcretelyhowarttherapytechniquescanbe
integratedwithMoritaTherapy.
Definitions
Art
Manyofusenjoyartbygoingtoplaceswhereitisactivelypursued,suchasart
museums,concerthalls,andtheaters.Butartisasignificantpartofoureverydaylife.
Artcanbefoundinthefoodsthatweselectandpresenttothetable,beautifulpictures
weenjoyinthemedia,dishesandpotteryweuseinourhomes,etc.Arttakesmany
differentformsthatinvolveothersensesinadditiontosightandsound(Rubin,2005).
3
Sinceancienttimes,humanbeingshaveexpressedthemselvesthroughart.Art
isapowerfulandeffectivemeansfortheartisttoexpressfeelings.Peoplehavealso
usedarttoexpressideasandtofacilitatehealing.Arteducationhasassistedchildrenin
theirdevelopment(Eckhoff,2007).Educationintheartsisconsideredbymanytobea
corecurriculum.Viewingartandattendingartisticperformancesareincludedin
nationaleducationalstandardsandincurriculumrequirementsforchildreninthe
UnitedStates(Eckhoff,2007).
Psychotherapy
Psychotherapyis“thetreatmentofmentalandemotionaldisordersthroughthe
useofpsychologicaltechniquesdesignedtoencouragecommunicationofconflictsand
insightintoproblems,withthegoalbeingreliefofsymptoms,changesinbehavior
leadingtoimprovedsocialandvocationalfunctioning,andpersonalitygrowth”
(AmericanHeritageDictionaryoftheEnglishLanguage,2009).Psychotherapyisa
treatmentapproachthatfocusesonoralcommunication.Thepsychotherapistasksthe
patienttoexploreandrecognizeanxietyandconflicts(Thyme,Sundin,Stahlberg,
Lindstrom,Eklof&Wiberg,2007,p.252).Thyme,etal.(2007)statedthatresearch
showedthatanypsychotherapywasmoreeffectiveforpsychiatricdisordersthanno
treatment.Patientssufferingfromdepressionwhoreceivedbriefpsychotherapy
showedsignificantimprovementwhencomparedtopatientswithoutpsychotherapy.
Andersen(2005)arguedthatitwasdifficulttomeasurescientificallytowhatdegree
symptomsimproved,becauseclients’symptomsweredifferentandtheresultsmightbe
4
verysubjective.Andersenconcludedthatsuccessfulpsychotherapyoftenresultedin
mindfulawareness,acognitivestatecentraltoBuddhistphilosophy(2005).
Historically,psychotherapyemergedfromthescientificobservationofhuman
behavior(Hayes,2002).CarlRogers(1957)statedthatsuccessfulpsychotherapyhas
threeimportantelements:therapistempathy,unconditionalpositiveregard,and
congruenceinrelationtotheclient.
Aspartoftheirprofessionaltraining,psychotherapistsstudyawiderangeof
psychologicaltopicssuchasdevelopmentalpsychology,psychopathology,ethics,
psychopharmacology,etc.Inordertoobtainprofessionalcompetence,theymust
understandboththetheoriesandtechniquesofpsychotherapy.Whenartisusedina
clinicalsetting,itisimperativetounderstandhowtocombinearttechniqueswith
psychotherapy.Psychotherapistswhodothiswell,provideeffectivetreatmentsfor
theirclients.Itisimportantforarttherapiststobewellversedinpsychotherapy.
ArtTherapyintheUnitedStates
AccordingtoRubin(1998),arttherapyis“art+therapy.”Shecontends
thattwokindsoftheoriesaboutarttherapyexist.Thefirsttheoryisfocusedonthe
clientengaginginthecreativeprocessofanarttherapysession.Thisencouragesthe
clienttoconnecttothetreatmentprocess(Rubin,1998).Thesecondtheoretical
positionconsidersthattheartworkofclientsilluminatestheirinnerconflictsand
unconsciousprocesses.Accordingtothistheory,artisusedinpsychotherapytoassist
indevelopingmeaningthroughananalysisofthesymbolismoftheart.Rubinsaidthat

5
therearedifferentnamesforarttherapy,including"expressiveanalysis,""clinicalart
therapy,""psychoaesthetics"and"expressivetherapy"(Rubin,1998,p.61).
AmericanArtTherapyAssociation’sDefinitionofArtTherapy
TheAmericanArtTherapyAssociationdefinesarttherapyas:
Thetherapeuticuseofartmaking,withinaprofessionalrelationship,by
peoplewhoexperienceillness,traumaorchallengesinliving,andby
peoplewhoseekpersonaldevelopment.Throughcreatingartand
reflectingontheartproductsandprocesses,peoplecanincrease
awarenessofselfandothers;copewithsymptoms,stressandtraumatic
experiences;enhancecognitiveabilities;andenjoythelife‐affirming
pleasuresofmakingart(AmericanArtTherapyAssociation,2010).
TheAssociationstatesthatarttherapyisamentalhealthprofession.Also,the
Associationdefinesarttherapistsas:
…professionalstrainedinbothartandtherapy.Theyareknowledgeable
abouthumandevelopment,psychologicaltheories,clinicalpractice,
spiritual,multiculturalandartistictraditions,andthehealingpotentialof
art.Theyuseartintreatment,assessmentandresearch,andprovide
consultationstoalliedprofessionals(AmericanArtTherapyAssociation,
2010).
IntheUnitedStates,theAmericanArtTherapyAssociationhassupportedthe
establishmentofarttherapyasaprofessionandtheeducationofarttherapists.
6
WhatisArtTherapy?
“Arttherapy’srootsextendasfarbackasprehistorywhenpeopledrewimages
incavesinattemptstoexpressandmastertheirworld”(Jung,1994,P.1).Sinceancient
times,humanbeingshaveexpressedthemselvesthroughart.Amongotherapproaches,
artisatooltoexpressfeelings.Peoplehavealsousedartforhealingandexpression.
JudithA.Rubin,apioneerofarttherapy,stated“Artisanaturalwaytocommunicate”
(2005,p.21).Arttherapyisaclinicalwayforpeopletoexpresstheirinnerthoughts.Art
isausefulmodalityinwhichtoexpressnon‐verbalthoughtsandimages.Malchiodi
(1998)wrotethatclientsdonotneedtoworryabouttheirartisticabilitiesbecauseall
artgeneratedinanarttherapysessionisautomaticallyacceptable.
Arttherapytechniquescanbeaneffectivetoolforbothassessmentand
treatment(Rubin,1998,2001).Arttherapydevelopedasawaytotreatpatients.
Becausearttherapyusesarttotreatpatients,mentalhealthprofessionalswhouseart
therapytechniquesmustbetrainednotjustintheuseofart,butalsointheclinicaluse
ofarttotreatdifferentkindsofsymptomsthatafflictpeople(Rubin,2005).Accurate
diagnosticskillsandeffectiveinterventionskillsinclinicalsettingsarealsocritical
necessities(2005).
Arttherapistsfocusontwoaspectsoffunctioning:psychologicaland
physiologicalfunctioning.Psychologicalfunctionsincludemood,self‐awareness,and
self‐esteem.Physiologicalfunctionsincludedecreaseinheartrate,bloodpressure,and
respirationrate(www.wholehealthmd.com.June4th,2010).McMurray(2000)
7
describedarttherapyasbeingcomprisedoftwomaintechniques:structuralandthe
freecreativeapproaches.Thestructuralapproachoccurswhenthearttherapistgives
concreteartdirectionsandspecificartmaterialstotheclient(McMurray,2000).The
freeapproachiswhenaclientspontaneouslycreatesimagesofhisorherimpulsesand
fantasies(McMurray,2000).Throughthesearttherapyexperiences,clientsareableto
recognizeandexpressimpulsesandfantasiesthatarenotintheirconsciousawareness.
Arttherapyisexperientialtherapyandassuch,isdifferentfromother
therapeuticapproaches(Wadeson,1995).Arttherapistsdonotleadclientswith
language.Clientsareabletodiscovertheirownstrengthsandreachtheirgoalsthough
theirownexperiences(Rubin,2005).Peopleprocesstheirownexperiencesviscerallyin
theirbodiesandminds(Rubin,2005).Forexample,childrentypicallydemonstrate
happinesswhentheybuildamodelcarforthefirsttime.Frequentlytheywilltryto
buildamoredifficultmodelthenexttime.Theyexperienceachievementandgrowthin
confidencethroughtheseexperiences.Clientsalsocanself‐discoverandgain
confidencethroughdrawingpicturesorcreatingobjects.Arttherapistssupportand
encourageaclient’sinternalprocesses,andfacilitatetheclientreachinghisorherown
goals.Experiencesduringarttherapysessionscanresultinstrongtherapeutic
movementfortheclient(Rubin,2005).
Duringarttherapy,challengesandsolutionsforproblemsareaddressedinthe
process.Atthesametime,clientsexploreandexpressinnerconflictanddifficulties
(Clements,1996).Supportingclientsintheirprocessincludesengagingindialoguewith
8
them,preparingtoolsthattheycanusetoextendtheirreflectionsthroughart,and
providingasafeenvironmentforgrowthandlearning.
Arttherapycangivetheclientapositiveexperienceofcreativityasexpressed
throughart.Creativitycanleadtodevelopinggreatermeaninginaperson’slife.People
canfreetheirmindsbyexpressingthemselves.Fun,creativeexperiencesareimportant
forhumanbeings.
AccordingtoRosen(2009)arttherapyissimilartomeditationorreflection.For
example,peoplecanobtainpeaceofmindinanarttherapysessionwhichissimilarto
thestateofmindoneexperienceslookingatagardenataZentemple,orengagingin
anyothermeditationpractice.Aclinically‐trainedtherapistcanlinkrelaxationwith
clinicaltreatmentgoals.Arttherapyhelpsclientsidentifyissuesandconsiderwaysto
overcomedifficulties.Suchanapproachcanleadtoeffectivestrategies.
Theroleofthetherapistisnotjusttotreatclientskindly,buttodesignand
implementtreatmentinterventionssothattheclient’spsychologicalsymptomsare
relieved(Rubin,1998,2005).Trainedarttherapistsprovidetherapeuticinterventionsin
amannerindividuallysuitedtoeachclient(Rubin,2005).Forexample,arttherapycan
teachclientsabouttheimpactofillegaldrugsonthecerebralcortex,orthemechanisms
ofviolenceandangerandhowtodiffusetriggersleadingtomaladaptiveaffective
states.Arttherapistscanbehighlyspecializedinprovidingthistypeof
psychoeducationaltraining(Jung,1994;Rubin,2005).
9
Choosingartmaterialsisacriticalpartofprovidingeffectivetreatment(Rubin,
2001,2005).Itisaveryimportantjobtoselectartmaterialsmatchedtoanindividual
client’spsychologicalstate,developmentallevel,andphysicalcondition.Arttherapists
providemanykindsofmaterialsandmethodstofittheclient’sneedtodevelopinsight
andexpressfeelings.Itisnecessaryforarttherapiststoalwaysconsiderwhetherthe
artisticmediumissuitableornot,whetheritreallyshouldbethoseparticularmaterials.
Forexample,atherapistmightprepareclippingsfrommagazinesformakingacollage
forthosewhoarenotgoodatdrawing.Whenchoosingthematerialsfor
psychologicallyunstableclients,anarttherapistneedstoavoidmaterialsthathave
sharpedgesorcanbeusedtoinflictwoundsandwhichcanleadtoself‐destructive
behaviororviolence.Theskilledarttherapistconsidersthosepossibilitiesatalltimes.
Itisalsoimportanttoorganizematerials.Oneneedstoknowwhichtoolstoprepare
andhowmanyofthem,beforethesessioncommences.Whenworkingwithclientsin
aninpatientsetting,forexample,itisimportanttoconfirmthenumberofpairsof
scissors.
Arttherapymethodspermitassessmentandtreatmentapproachestobe
identified.Arttherapycanintegrateknowledgeaboutpsychologicaldevelopmental
stageswithknowledgeobtainedthroughassessment.Anarttherapistmustbesensitive
totheuseofcertainarttherapytechniques.Forexample,someclientsmightbeafraid
ofdrawingpicturesbecausesometimeintheirhistory,theyhaveassociateddrawing
withcriticism.Arttherapistsshouldbuildtrustingrelationshipswithclientsandshow

10
themthatthearttherapysessionisasafeenvironment,ratherthanaplaceofcriticism
andharshjudgment.Also,arttherapymightnotbeusefulforcertainindividualswho
havephysicaldisabilitiesorvisualimpairments.However,theseindividualsmaybeable
tobenefitfromarttherapyifarttherapistsareabletoworkwiththemindividuallyand
adaptartmaterialsanddirectionstothatwhichwouldpermitexpression.
Rubin(1998)distinguishedbetweenwhatarttherapyisandwhatitisnot.She
saidthatiftheartactivityisforfunorrecreation‐‐evenifitoccursinapsychiatric
hospital‐‐itisnotarttherapy.Arttherapyisnotactivitiesforthesolepurposeof
engaginginfun.Further,sheclarifiedthat,“Eventhemostsensitiveartistorartteacher
isnotatherapist,”(Rubin,1998,p.63).Arteducatorsmayindeedengageinactive
influenceofclients,butarttherapistsfocusonthetherapeuticprocessandprovide
quietmomentsofselfreflectionanddialoguewiththeirclients(Naumburg,2001).
Educationalactivitiesinartcanpromotesocialandemotionalgrowth,butarttherapy
includeseducationtohelpclientsexpressthemselves(Rubin,1998).Forexample,anart
therapistmayuseartmaterialstohelpaclienttoexpressfeelings,toencouragehealthy
sublimation,andtobuildasenseofself‐esteem.Arttherapistsfocusonhowart
processesandartisticmaterialscanactivatecertainpsychologicalprocesses.Teaching
artistictechniqueisnottheprimarygoal.
Furtherdifferencesexistbetweenanartactivityandanarttherapysession.An
arttherapistisabletoobserveandassesstheclients’psychologicaldynamics.Even
thoughanarttherapistandartteacherusethesamematerials,theirmethodologyand
11
usageofthosematerialscanvarygreatly.Anarttherapistobservespsychological
dynamicsthroughoutthetherapysessions(Rubin,1998).Oneexampleofthisistheuse
ofprojectivedrawingasameansofassessment.Projectivedrawingwasoriginally
developedasanassessmenttoolbyclinicalpsychologistsbuthasbeenwidelyusedby
arttherapistsaswell.Socialworkersandpsychotherapists,aswellaspsychologists,
havefounditusefultoemployartinsessionsbecauseimagescanshowthepatient’s
unconscious(Rubin,1998).
Arttherapyinvolvesnotonlyexpressingandenjoyingoneselfthroughart,but
alsoengagingintherapythroughthemediumofart(Wadeson,1987).Wadesonfurther
clarifiedthat,“Creativityisatthecoreofarttherapy’’(2000,p.xiii).Arttherapyis
usefulforhealingandcanleadtocatharsis,areleasingofemotions(Malchiodi,1998).
Inaddition,arttherapistshelpclientstoexperiencetransformationandtofindpersonal
meaningandhealingthroughart(Malchiodi,1998).
Arttherapyvalidatesnotonlyperspectivesthatarepositiveinnature,butalso
morenegativeperspectivesthataresometimeshardforclientstoaccept,suchas
ugliness,strangeness,andsoon.Arttherapycanprovideunderstanding,non‐
judgmentalsupport,andatrustedrelationshipwithanother‐‐thearttherapist.Many
clientshaveneverbeenabletoexpressthemselvesinthiswaybefore(Wadeson,1987).
Self‐expressionandexplorationwithanarttherapistcansupportaclient'spositive
personaldevelopment(Wadeson,1987).Wadesonstatedthatarttherapycanproduce
12
asynergisticeffectbyusingartandhelpingpeoplediscoveranddeveloptheirinner
selveswhichcannotbeobtainedintherapiesthatdependonverballanguagealone.
UsefulnessofArtTherapy
Artisnonverballanguage.Creativityandnonverbalimageryareusefulwithall
kindsofpeople(Hoshino,2003).Malchiodi(1998)wrotethatvisualartspeaksinways
thatwordscannot.Gladding&Henderson(1998)statedthatthecreativeartsare
universallanguage(p.187).Peoplecantransformtheiremotionsintodrawingand
expressaffectandcognitionsnoteasilyputintolanguage(Kearney&Hyle,2004).Art
canleadtodisclosuresthatarehardertoexpressthroughverballanguage.Artprovides
visualdata(McNiff,2009).Becausearttherapyrisesaboveculturalbackgrounds,itis
usefulforclientsandclinicianswhoaremoreverballylimited(McNiff,2009).Artcan
serveasacommunicationtoolthathelpstomediatedevelopmentalandmulticultural
differences.Ifthereisnocommonlanguagebetweenarttherapistandclient,amethod
ofcommunicatingwitheachothercanoccurthroughart.Malchiodi(1998)statedthat
expressioninartdoesnotdependontherulesoflanguage,suchasgrammarand
correctspelling.Inaddition,arttherapyisusefulforthosewhohavelittlelanguage
ability,suchasthosewhoareimpairedbyemotionalorcognitivedisorders.
Artcannaturallyexpresssensationsandemotions,unconsciousthoughts,and
underlyingbehavior(Kearney,&Hyle,2004).Forexample,aclientcanfreelyexpress
themselveswithoutsummarizingtheirthoughtsormakinganefforttobeverbally
understoodbyothers.Throughart,aclientcanexpressemotions,ideas,and
13
unconsciousprocesseswithfewerconstraintsandinalessthreateningmanner
(Malchiodi,1998).Arttherapytreatmentisusefulforclientswhohavedifficulty
expressingtheirinternalexperiencesasaresultofinflexibledefensemechanisms
(McMurray,2000).
Arttherapyprovidesasafeenvironmentforclients’innerfeelings.Clientscan
describethemselvesthroughartwithoutanyrejectionorcriticism(Naumberg,2001).
Whenpeoplewanttoexposewhatisatthebottomoftheirhearts,itusuallyisonly
possibleinfrontofthosetheytrust.Arttherapistsbuildclienttrust,accepttheirclients,
avoidjudgmentandassistclientsintheirpsychologicaljourney.Malchiodi(1998)stated
thatvisualthinkinghelpstoorganizeanddescribeourthoughts.Arttherapyis
nonverballanguageandcommunicationthatdisplaysvalues(Malchiodi,1998).Art
therapyisafirst‐handexperience(Malchiodi,1998)thatcanleadtoaricher
understandingabouttheself.
Thearttherapyprocessofcreativeexpressionhealspeople(Gladding&
Henderson,1998).Artactivitiesreducestress(Malchiodi,1997).Kramer(1972)opined
thatarttherapyisusefulforaggressiveclientswhorequireexpressionandenergy
reduction.Writingdailyaboutdistressfuleventshelpspeopleheal,incontrastto
peoplethatdonotwrite(Gladding&Henderson,1998).Theexperienceofjournal
writingissimilartothearttherapyprocess.Malchiodi(1998)statedthatvisualthinking
helpspeopletoorganizeanddescribetheirthoughts.
Arttherapyisespeciallyusefulforchildren.Engaginginartactivitiesisbeneficial
14
inthatitimproveschildren’sself‐esteem(Ozimo&Ozimo,1989,citedinGladding&
Henderson,1998).Artcanbealessthreateningwayforchildrentoaddressgriefthan
tospeakaboutit(CummingandVisser,2009).Otherresearchhasshownthatthrough
artactivities,childrendiscovernewinterests,ideas,abilities,andstrengths(Appleton&
Dykeman,1996,citedinGladding&Henderson,1998).Arttherapycanbeusefulfor
childreninpartbecausechildrendonothavelargevocabularies.Takahashi(1986)
wrotethatartallowsustoexploreboththeunconsciousandconsciousrealms,and
accessissuesthatcanbedifficulttodescribeverbally(p.30).
Gussak(2009)showedthatarttherapyresultedinpositivechangesofmoodand
behaviorinbothmaleandfemaleinmates.Whilehisresearchfindingsindicatedthat
arttherapywasmoreeffectiveforfemaleinmates,therewereclearfindingsthatart
therapywaseffectivefortreatingmaleinmatesaswell.Arttherapyismorefocusedon
innerexperiences.Duringasessionofarttherapy,clientsworkonexploringtheirinner
selvesand/orconflicts.Paintingsorobjectscreatedduringsuchsessionsarevery
personal.Theprocesssupportstheclient’sbehavior,motivation,andself‐esteem
throughdevelopingskillsandsharingartwithpeers(Cumming,&Visser,2009).
Becauseclientstalkaboutverypersonalandprivatefactsorfeelings,itis
necessarytokeepconfidentialityabouttheartworkandconversationsthattakeplace
duringthesessions.Buildingatherapeuticalliancerequiresthetherapisttovalidatethe
meaningfortheclientthatemergesfromarttherapy,andkeepsecretthatmeaning
fromothersoutsideofthesession.Supportingclientsalsomeansbuildingasenseof
15
personalsafetywiththem.Withouttrustinthetherapeuticrelationship,cliniciansare
unabletoprovideeffectivetreatments.
Arttherapycanbeeffectivefortreatingclientswhohavesufferedsevere
trauma.Researchshowstraumaticexperiencesareencodedintheimagesformedinthe
mind(Malchiodi,1998).Itcanbeverydifficulttorememberorverbalizeatraumatic
experience.Arttherapycanassistinintegratingwhatisdifficulttoverbalize.
Fromaneuro‐scientificperspective,arttherapyprovidesdistinctbenefits.For
example,usingbothhandsduringthecreationofartengagesbothrightandleftbrain
(McMamee,2005,p.544‐545).Alsoarttherapyhasbeenshowntobeeffectivefor
cancerpatientstodecreasetheirdepressivesymptomsandincreasetheirattentiveness
(Thyme,Sundin,Stahlberg,Lindstrom,EklofandWiberg,2007).Ithasbeenusedin
inpatientandoutpatientsettings;withseverementalillness;withthosewhosuffer
depression,anxietydisorder,andaddictions;andwithautisticchildren,prisoninmates,
andpeoplewhohaveproblemswithverbalexpression(Rustin,2008).
ThePlaceofPsychologicalTheoryinTherapy
Therearemanykindsoftheoreticalorientationsinpsychology,suchas
psychodynamic,cognitive‐behavioral,person‐centered,objectrelations,existential,and
familysystemstheory.Theoriesareimportantframeworkstohelptherapists
understandtheirpatients.Theycanindicatehowtoleadpatientstoreachtheirgoals,
stepbystep.Itisimportantforarttherapiststostudyandunderstandtheoriesof
humanpsychologicalfunctioningandpsychopathologyinordertoeffectivelyintegrate
16
arttherapymethodswiththetreatmentorientation.AsRubinstates,“Iamquite
convincedthatonlyiftheapproachiscomfortableforatherapistisitatallusefulinhis
andherhands”(2001,p.3).Therapistsneedtofindtheoriesthattheyunderstandand
withwhichtheyfeelcomfortablewhileworkingwithpatients.Rubin(2001)saweach
theoreticalorientationasproviding“differentsetsoflenses,(which)illuminatesslightly
differentaspectsofhumanpersonalityandgrowth”(p.1).Eachtheoryprovidesa
differentperspectivetouseinanalyzingpeople.Hefurtherclarifiedthat“[I]fart
therapistsaretofunctionassophisticatedmembersofaclinical,educational,medical,
orsocialteam,ourcomprehensionofanytheoreticalstanceneedstobeasdeepand
clearasthatofothers”(Rubin,2001,p.2).
Sometheoriesmaynotfitfortherapistsfromdifferentculturalbackgroundsand
withdifferingculturalvalues.Forexample,forAsiantherapists,itmaybedifficultto
understandWesterntheories.AsiantherapistsmaymoreeasilyunderstandanEastern
worldvieworphilosophysuchasBuddhism.Religionisnotpsychotherapy,but
therapistscanintegrateaspectsofareligiousbeliefsystemintopsychotherapy,suchas
thepracticesofmeditationandmindfulness.Iftherapistsdonotunderstandand
consciouslyapplyastructuredtheoreticalorientation,theymaybelesseffectivein
helpingpatients.
ArttherapyandTheory
Arttherapydoesnothaveoneunifyingtheoryuponwhichitisbased.Because
arttherapylacksasinglefoundationalframework,arttherapistsarefreetostudymany
17
theoriesduringtheirtrainingasclinicians(Rubin,2001).Arttherapistshavetochoose
psychologicaltheorieswhicharecomfortableforthemtousewiththeirclientsand
integratetheseviewpointswitharttherapymethodology.
Allpsychotherapistssometimesneedtochangetheapplicationofthethchniqueto
meetaclient’sindividualneeds.Ifononeday,aclientneedseducationorbehavior‐
changingskills,thearttherapistmightchoosetechniquebasedonCBT‐arttherapy,
whichisacombinationofcognitivebehaviortherapyandart.Anotherday,whena
clientstruggleswithher/hisdivorcedparents,thearttherapistcanasktheclientto
drawafamilytree/genogram.Throughsuchanimage,arttherapistsareableto
observetheclient’sperspectiveoffamilyhistoryandculturalheritage.Asaresultof
suchportraiture,thearttherapistmightselectfamilysystemtechniqueasan
appropriateinvitationfortreatment.Onstillanotherday,iftheclienthasfamily
problems,thearttherapistmightasktheclient’sfamilytobeapartofaconjointsession
andaskthemtoworktogetherusinganarttherapytechnique.Suchsessionscreatean
opportunityforthearttherapisttoassessfamilydynamicsdirectly,leadingtoamore
clearunderstandingoftheclient’stherapeuticneeds.
ArtTherapyasAssessment
Artisknowntoencapsulatehumanexperiences,whichiswhyartassessments
havebeendescribedas“artbasedresearch”(Nissimov‐Nahum,2009).Drawingsare
usedasapartofdatacollectionbecausetheyshowtheclient’sthoughts,emotions,and
18
fantasies(Kearney&Hyle,2004;Silver,2009).Drawingcanbeatoolforunstructured
interviews,aswellasincreasingtheclient’srateofresponse(Kearney&Hyle,2004).
However,artinterviewsmustbecarefullyconductedinordertonotinvalidatetheclient
(Naumverg,2001).Cliniciansneedspecifictrainingonhowtouseartasassessment.
Whenaclinicianadministersartaspartoftheassessment,itisimportantforthemtobe
clearaboutwhatkindsofinformationcanhelptodirecttreatment.
Arttherapyassessmentsareusefulforfamilytherapy.Arttherapycanbeused
toassessfamilyfunctioninganddynamics,includingpointsofviewofthevariousfamily
members,relationshipsamongfamilymembers,thefamily’scommunication
mechanisms,family‐heldemotions,values,andbeliefs,etc.Itmaybepossibleto
determinewhohasthemostpowerinafamilywhentheyworktogetheronanart
activity.Forexample,drawingthefamilydinnertablemayrevealfamilynutrition,daily
lifestyle,andcommunicationstyle.Rubin(1984)statedthatthroughfamilydrawing,
arttherapistsareabletoobservefamilydynamicsandinteractionssuchaswhositsnext
towhomandwhointeractswithwhom(p.138).Clinicianscanaskaboutthefamilyand
relationshipswithinitbyusingthefamilypictures.Drawingapictureoffamilyalsois
usefultoanalyzefamilyfunctioning(Rubin,1984).
Cliniciansmustunderstandthemeaningofsymbolswhenartisusedfor
assessment(McNiff,2009).Symbolswillbeaffectedbytheclient’sculture,religion,and
philosophytowardsart(McNiff,2009).Forinstance,artcanbeusedtolearnmore
abouttheclient’sexperienceofdeathandgrief,aswellashowcognitiveand
developmentallevelsaffecttheprocessofdealingwithdeathorgrief(Nagy,1948;
19
Singer,1984,citedinGraham&Sontag,2001).Sometimesitisdifficultforclientsto
discloseandexpresstheirpainfulexperiencesoftheseeventsthroughlanguage.Art
canbeagreatwaytofeelsafeenoughtoallowexpressionofthesetroublingaffective
states.
Clinicianscanobserveclientsastheirclientsexpressfeelingsbyusingcertainart
materials.Sometheoriessuggestthatcolorshavecertainmeanings.However,itseems
unlikelythataparticularcolorhasaparticularmeaninginallcases.Forexample,using
alotofblackcrayondoesnotnecessarilymeanthattheclientisdepressedorthatthey
arethinkingaboutdeath.Culturalvaluesaffectthemeaningofcolors.Thus,itmaybe
inaccuratetointerpretclients’pictureswithoutconsideringculturalcontextfactors.
Whenclientstalkanddescribetheirexperiences,thoughtsandfeelings,diligent
clinicianswillalsotakenoteofsuchnonverbalexpressionsastensioninthefaceand
body.Carefulobservationcanleadtounderstandingwhenaclientisself‐regulatingin
aneffectivemanner.
Mostarttherapistsalsorecognizethataclient’sartworkmayshowaspectsof
theclient’sunconscious.Jungsaidthatarthasthepowertoworkwiththeunconscious
(Brooke,2004).Oneapproachtoaccessingtheunconsciousistodirectclientsinthe
firstsessiontoscribbledraw.Rubin(1984)suggestedthatbyusingthisapproach,art
therapistsareabletogetamaximumamountofinformationwithminimalstress.Such
anapproachcanalsoserveasapowerfuldiagnostictool(Rubin,1984).Drawingcan
highlighttheclient’scurrentleveloffunctioning(Wadeson,1980;Cohen,1986;Gantt,
2001aandb,citedinBrooke,2004).
20
Becausedrawingiseasierthantalkingforchildren,especiallyyoungerchildren,
drawingisusefultoassessthecourseoftheirlivesandprocesspainfulexperiences
(Graham&Sontag,2001).Drawingsareinitialassessmentsinarttherapysessions
(Brook,2004).Arttherapistsareabletoobservetheclient’smotorskills,movement,
personality,andcognitiveskills.White,Wallace,andHuffman(2004)wroteaboutthe
benefitsofarttherapyassessmentforchildren:
Artassessmentsoffer(a)anuncensoredviewofachild’sthoughtsand
feelings(Neale&Rosal,1993),(b)anonverbalmethodofassessmentfor
childrenwhoarestilldevelopinglanguageskillsorwhoareunwillingto
verbalizefeelingsemotions(Arrington,2001),and(c)anonintimidating
meansofassessmentinwhichchildrenarelikelytoparticipate(Peterson
&Hardin,1997).Tobemostuseful,artassessmentsshouldbe“non‐
threatening,easytoadminister,nortootime‐consumingtocomplete,
andeasyanalyzed”(Anderson,2001a,p.210).
ArtandCulture
Cultureimpactspeople’sfunctioningbecauseofitsstrongtraditions(Hoshino,
2003).Itisimportantforclinicianstounderstandtheculturalcontextofeachclientso
thattreatmentdoesnotinvalidateaspectsoftheirheritage.Ifcliniciansdonot
understandtheclient’svalues,andwheretheirthoughtscomefrom,theycannot
understandtheirclients’behaviors.Increasingly,cliniciansarestudyingcrosscultural
psychotherapypractice(Tanaka‐Matsumi,1979).Thesedays,whenAmerican
psychologistsdiagnosetheirclients,thepsychologisttypicallyasksabouttheclient’s
21
religion,values,ethnicities,andfamilytraditions,mentalissuesamongfamilymembers,
developmentalhistory,socioeconomicstatus,andeducationalhistory.Sharingworld
viewsbetweencliniciansandclientscanbeaneffectiveintervention(Tanaka‐Matsumi,
1979).Culturecreatesanimportantcontextwhichmustbetakenintoconsideration.
Forexample,ifparentssleepwiththeirtwelve‐year‐oldchild,throughtheAmerican
perspective,theymightneedtobereportedaspossiblechildabusers.However,ifthe
familyiscomprisedofrefugeesandhasnotsleptseparatelyduringtheirlongjourneyto
theUnitedStates,theirbehaviormaynotberelatedtoabuse.
Inthesameway,cliniciansneedtounderstandclients’cultureswhenartisused
withinsessions.Forexample,drawingachimneymightbenormalforpeoplein
Westerncultures.However,itmightbenotbenormalforpeopleinEasterncultures
becausetheymightnotusechimneys.Artitselfisacentralaspectofculturethatalso
playsanimportantpartinpsychologicalfunctioning.Forinstance,inJapan,eachfamily
ownsafamilycrest.Itisaconcretesymbolofone’sfamilyandencapsulatesthefamily
history.Symbolsintheworkofclientsoftenspontaneouslyemergeduringarttherapy
sessions.Themeaningsofthesymbolscanleadtoadeeperunderstandingaboutthe
client’sissues.
Recently,culturalpracticeshavebeguntobemorewidelydisseminatedaround
theworld.Forinstance,Japanesepeoplearenottheonlyindividualstositandlookat
theZenJapanesetraditionalgarden,andreflectontheirlife.Manypeopleinother
partsoftheworldnowenjoythispracticeaswell.Thesetypesofreflectionshelp
peoplerealizenewaspectsaboutthemselves.Theefficacyofformalperiodsof
22
reflectionmaybeonereasonwhymanyAmericansareinterestedinlearningaboutZen
andotherJapaneseculturaltraditions.
Culturesareaffectedbyenvironment,lifestyles,andvalues.Forexample,
peoplewholiveincloserelationshipsinacommunityaredifferentfrompeoplewholive
inanindividualisticsociety.Theformergroupmightbelievethatharmonyismore
importantthanthelattergroup,whereasthelattermayvalueautonomytoagreater
degreethantheformer.Cultureisaverysensitiveaspectofpsychologythatdeeply
influencesone’sworldview.
ZenArtUsedinHealing
TodaymanypeopleintheworldarefascinatedbyZenphilosophyandZenarts.
ItisclearthatJapaneseZenculturecanhealpeoplepsychologically.Itisimportantfor
clinicianstoknowhowZencultureandBuddhistphilosophyhaveinfluencedpeople’s
psychologicalwell‐being.ArthasbeenusedinthepracticeofZenandcanplayan
importantpartinhealing(Yanagida,1982).ZenandBuddhistculturehaveincorporated
artasahealingtool.However,BuddhistandZenarthasnotbeenusedasaclinicaltool
inmedicineorpsychologybecausetheirreligiousoriginshavedeterredscientific
acceptance.TheperspectiveofAmericanarttherapistsaboutarttherapyandwhatart
therapyiscanbeincorporatedinMoritaassessmentandtreatmentapproaches.Itis
importantforJapaneseclinicianstoknowhowZencultureandAsianphilosophy
influencepeople’smentalhealth.Forinstance,Zenpromotessimpleliving,meditation,
andthearts.

23
JapaneseZenhasdevelopedprimarilysincethethirteencentury.Itcamefrom
China(Yanagida,1982).BuddhismwasfirstestablishedinIndia.However,eachcountry
hasdevelopedBuddhismindifferentwaysandadjustedittotheircultures(Yoshida,
1985).ZendevelopedinmanywaysthroughoutJapaneseculture.WhenZenBuddhism
andJapaneseculturemelded,JapaneseclimateshapedJapaneseBuddhism,whichis
differentfromthestrainofBuddhismthatdevelopedinotherAsiancontinental
countries(Yoshida,1985).Forinstance,climateaspectssuchashighhumidity,
mountainousislands,manyrivers,andtheever‐presentoceanhaveaffectedthe
philosophyofJapaneseZen(Yoshida,1996).Zensaystolookattruth,notattheoutside
surfaces.Itvaluestheinside,anddoesnotvaluetheoutside(Yoshida,1985).Amajor
teachingofZenphilosophyistolivelikeariver.Thatmeanshavingnoresistanceand
followingyourdestiny.Anothercoreprincipleisthatallvisiblethingsarevain;allis
vanity(Yoshida,1985).Zenpromotesmeditationformindfulness(Yoshida,1985).Ona
practicallevel,theclimatealsoinfluencedartistictechniques.Highhumidityinfluenced
theuseofsimplecolorsforZenart.EventhoughJapaneseBuddhistsculptors
decoratedwoodstatueswithmanycolorslongago,highhumiditycorrodedthepaintof
thesestatues.ThatiswhyJapaneseBuddhistsculpturesarepaintedwithresinsfroma
lacquertreeandthecolorsareverysimple.
Zenoffersaphilosophyforhealing,andZenarthasbeenusedforhealing.Using
blackinkforZenartmeanstobesimpleandavoidcolor,infinityandvanity(Yoshida,
1985).Zenartusesaminimumoflinesandshapes(Suzuki,1940).Itdoesnot

24
distinguishbetweenbeautyandugliness(Yanagi,1949,p.95).Yanagi(1949)wrotethat
beautyanduglinessareoppositesonthesameline(p.90).Zenphilosophysuggests
makingacircleofthelinethatisbeautyandugliness.AccordingtoZenphilosophy,the
circleharmonizesorunitesasoneworld(Yanagi,1949,p.90).Thereisalinewhichhas
oppositefeelings(internalconflicts).Zensaysthatwhenyouusethelineandmakea
circle,thecircleisyourmind.ManyWesternarttherapistsuseacirclepicturefor
treatment.Theyasktheirclientstodrawinsideofthecircle,whichiscalledamandala.
Thetheoryisthatcreatingamandalaishealingbecausethecircleisabletocontainand
holdtheclient’sfeelingsandthoughts(Rubin,2001).
Also,Zenrockgardenshavecontributedmanywaystohealpeopleintheworld.
RockgardensdemonstrateZenphilosophy.Thegardenoftendoesnotuserealwater
andtrees;itusesonlyrockstoshownature(Yanagida,1982).Therocksaresymbolsof
death,andthegardenismadetobeimperfect.Zenart'sgoalis“beforeperfect”or
“imperfection”(Yanagida,1982,p.19).TheJapanesesenseofbeautyisobtained
throughimbalanceandimperfection.Forexample,Japaneseculturevaluesodd
numbers,notevennumbers(Yanagida,1982).Zenphilosophyiscontradictorytosome
Westernvalues.Forexample,manyAmericansbelievethathavingalotofthingsisa
sourceofhappiness.Bycontrast,Zenphilosophysaysthatmaterialisticdesiresand
externalbeautifulobjectsdonotmakepeoplehappy.Zenemphasizescompassion
towardpeople.ArthasbeenusedinthepracticeofZenandcanplayanimportantpart
inhealing.
25
Zenphilosophyandhealingmethodshaveanimportantroletoplayinmental
health.Asianculture,includingJapaneseZenandBuddhistcultureandphilosophy,have
muchtoteachusabouthealthypsychologicalfunctioning.
26
II.THEORETICALHISTORYOFARTTHERAPY
ArtTherapyandTheories
InordertoexaminetheintegrationofMoritatherapyandarttherapy,itis
importanttostudytheotherkindsoftheoriesuponwhicharttherapistshavedrawn
historically.Arttherapistsaredrawntopsychologicalmodelstousewitharttherapy
thatarecomfortableforthempersonallyandthatofferdeeperunderstandingforthem
(Rubin,2001).Theoriesarechosenasaframeworkforarttherapyasaresultofother
reasonsaswell,reasonssuchasculture,psychologicalhistory,andsocialsituations.
Cultureaffectsdiagnosesandtreatments.Newtheorieshavebeendeveloped
throughoutthehistoryofthefieldofpsychology,inresponsetochangingtimesand
historicalevents.Evolvingsocialsituationshaveresultedinnewkindsofmentalillness.
Infact,mentalillnessesandtreatmentsdonotexistwithoutculturalinfluence(Frank&
Frank,1993).Mentalillnessesoccurincombinationwithone’sphysicalandsocial
relationshipproblems,profoundlyaffectedbyculturalnormsinregardsto
communicationstyles,thoughts,behaviors,andfeelings(Frank,&Frank,1993).One
exampleoftheinfluenceofcultureondiagnosisisShinkeisitsu‐showhichwasseenonly
inJapan,asclassifiedbyMorita.Anotherexampleofculturalinfluenceisthatduring
WorldWarII,Russiansoldierswereneverdiagnosedwithpsychoneurosesbecausethe
RussianArmydidnotrecognizetheseasillnesses(Frank,&Frank,1993).
TheoreticalHistoryofArtTherapy
Inthe1910s,Naumburg,whoiscalledthemotherofarttherapy,choseCarl
Jung’sanalyticalpsychology,whichwascloselyalignedwithpsychoanalysis,asthe
27
theoreticalframeworkforherworkinarttherapy.Atthattime,FreudandJungwere
verypopularintheUnitedStates.AfterWorldWarI,peopleintheUnitedStateswere
sufferingagreatdealofanxietyandstrugglingwithpoverty.ManyvictimsofNazi
GermanyhadimmigratedtotheUnitedStatesandweredealingwiththetraumatic
aftermathofthewar.Naumburgwasanartteacherforchildrenwhosufferedfrom
mentalillness.Inworkingwiththemartistically,shefoundthattheirpictureswere
symbolic.SheappliedJung’stheorytoanalyzeandunderstandherstudents.
NaumburgbelievedthatJung’spsychologicalmodelwasusefulforherstudentswithits
strongvalidationthatartexpressestheunconscious.Later,shebecameapsychologist
andusedthetheorywithartwithherclients.
Inshort,therearemanylikelyreasonswhyNaumburgchoseJung’stheoretical
modelforherwork.Forone,psychoanalysiswasapopularandmajortheoretical
orientationinWesterncultureatthattimeinhistory.Psychologywasarelativelynew
fieldandthenumbersofavailabletheorieswerelimited.Additionally,Jung’sanalysis
aboutimagesinspiredherthinkingandresonatedwithherwork.Shewantedtohelp
andunderstandherstudentsdeeply.ShebecameanardentadmirerofJung.Forthe
firsttimeinAmericanhistory,apsychologicaltheorybecametheframeworkfortheuse
ofartintreatment.
Duringthesametimeperiod,artwasusedasahealingmethodinZenculture.In
theearly1920sinJapan,MoritastudiedFreudbutbelievedthatFreud’stheoretical
orientationwasnotusefulbecausepeopledidnotneedtogetintouchwiththeir
unconsciousinordertobehelped.Instead,heformulatedhisowntheoretical
28
orientation,whichhecalledMoritaTherapyandfoundedaninpatientunitusingthis
approach.
Inthe1920s,behaviorismbecameapopularpartoftheworldofpsychology.In
theUnitedStates,EdwardLeeThomdike(1874‐1949)conductedaseriesofexperiments
withratsandpuzzles.InRussia,IvanPavlovbeganhisfamousexperimentswithdogs,
tones,andmeatpowder.Behaviorismstudiedhumanbehaviorthroughanimal
experiments.However,thereisnorecordthatpsychologists,psychiatrists,ortherapists
usedthetheorybehindbehaviorismwithartatthattime.Americanarttherapistsdid
notappeartobefamiliarwithbehaviorism,butrather,werefocusedonpsychoanalytic
models.Interestingly,thetheorybehindMoritaTherapyhassomesimilaritieswith
behaviorismbecauseclientsaretaughthowtothinkandbehave.
IntheUnitedStates,manyhospitalswerebuiltfollowingtheendofWorldWarI
inordertoaddressmedicalproblemsexperiencedbyveterans.IntheStateofKansas,
theMenningerClinicopenedupwithJeanettaLyleandRuthFasionShawproviding
treatmentbyusingartwithlong‐termin‐patientswhosufferedfromPostTraumatic
StressSyndrome(PTSD),especiallychildren(Jung,1994).SimilartowhatNaumburg
wasdoingelsewhere,attheMenningerClinicartwasusedinthetreatmentof
children’smentalillnessundertherubricofpsychoanalyticaltheory.
Inthe1930s,EdithKramer,whowasanartteacherandfineartist,usedartwith
childrenwhohadescapedfromtheNaziconcentrationcamps.Theartallowedthemto
expressangerwithHitler,fear,andunsolvedconflict.Shefoundthatthosechildren
becamemoreresilientthroughtheart‐makingprocessandfoundhopefortheirfuture
29
lives(Kramer,1972b).LikeNaumburg,KramerhasusedJung’sanalyticalpsychologyto
interpretsymbolicmeaningandalsousedFreud’stheoryoftheunconscious.
Essentially,NaumburgandKramerchoseanexistingpsychologicaltheoryuponwhichto
basetheirclinicalwork.Moritadidnotfindanavailabletheorythatwassuitableforhis
work,andtherefore,turnedtocreatinganewone.
Duringthe1960s,withtheinfluenceofFreudandJunghavingdiminished
somewhat,manyarttherapistsintegratedavarietyofotherpsychologicalorientations
withtheirclinicalwork.Forexample,ElkinsandStovall(2000)foundthat28.2%of
1,846membersoftheArtTherapyAssociationin1998‐1999usedmorethanone
theory.20.8%oftheassociationmembersinthestudydeclaredthemselvesaseclectic,
meaningtheychoosefromavarietyoftheoreticalorientations,dependingonthecase.
10.1%ofthemwerepsychodynamicpractitioners,ofwhichtheJungianswere5.4%and
4.6%employedobjectrelationstheory.CognitiveBehavioralTheorywasusedby2.2%
ofthemembers.Between1.0%and1.9%ofthesearttherapistsascribedtoclient
centeredtheory,Cognitive,Gestalt,Developmental,Existential,orFamilySystems
theory.Allothertheoreticalorientationswerelessthan1%oftheresponses(Elkins,&
Stovall,2000).
Theabovesurveyshowedwhatkindsoftheoriesarttherapistschose.However,
itdidnotshowthereasonswhytheychosethetheories.80%ofthemembershipchose
aparticulartheory.Nonetheless,alltheoriesdonotfitwithallkindsofmentalillness.
Certaintheoriesaremorehelpfulinexplainingortreatingcertainillnesses.Onemodel
maynotbeeffectiveforallkindsofpsychiatricdisorders.Forexample,itmightbe

30
bettertouseCognitiveBehaviorTherapyorExistentialTherapyforPTSDclientsrather
thanpsychoanalysis.Thepsychoanalyticmethodtakestimeandiscostly.Theclient
mightneedacutetreatmentorneedtofocusonthepresentandfutureratherthanthe
past.FortherapistswhoidentifiedtheirtheoreticalorientationasEclectic,thereare
reasonstochooseparticulartheoriesforparticularclients.Itisnotunreasonableto
assumethataclinicianwoulddrawondifferenttheoriesthroughthecourseof
treatment.UsingWesterntheorymaynotfitculturallyforAsianclientswhereasusing
MoritaTherapymaybemoreappropriateforthem.Futurestudiesarewarrantedto
studythereasonswhyarttherapistschoseparticularpsychologicaltheoriesandhow
effectivetheyareinusingthem.
ChoiceofTheory
Therearetwotendenciesthatinfluencehowarttherapistschoosethetheories
underwhichtheyoperate.Firstofall,manyclinicianschooseatheorytofitclient
conditions.Secondofall,cliniciansmaychooseatheorywithwhichtheypersonallyare
morecomfortable,onethatmakessenseforthem(Rubin,2001).Arttherapistswho
usedEclecticmethodsintheAmericanArtTherapyAssociationsurveysubscribedtothe
firsttendency.Thosewhousedaparticulartheorysubscribedtothesecondtendency.
Fortheirpart,clientsoftenchosetheirtherapistbasedonwhattheyunderstandto
bethatperson’stheoreticalorientation.However,theymightnotunderstandeach
theoryverywell.Itisimportantforclinicianstobeawareofthetheorytowhichthey
subscribe,aswellasthereasonsforit.
31
AdvantageofIntegratingArtTherapywithTheory
Inthepast,arttherapyhasbeenusedwithavarietyofpsychologicaltheories.
Usingartisefficaciousformanyclinicaltreatmentapproaches.Itcanfacilitate
communicationbetweentheclientandtheouterworld.Anarttherapistisabletobe
withtheclient’spsychologicalprocessatits’mostvulnerable.Duringtheprocessof
makingart,clientsareabletofindtheirtrueself,andbymakingart,clientsexperience
achievement.Ontheotherhand,itisimportanttoconsideriftherearepsychological
modelswhichshouldnotuseart.Currently,thereisnopublishedinformationabout
this.However,inthefuturethisissueneedstobeexaminedbecauseitisvery
importanttofindthemosteffectiveintegrationoftheorywithart.
PossibleIntegrationofMoritaTherapyandArtTherapy
TherearereasonsarttherapymaybeabletobeintegratedwithMoritaTherapy.
First,historicallyarttherapyhasbeenabletointegratewithanytheoreticalorientation
totreatment.SoitshouldbepossibletointegrateMoritaTherapyandarttherapy.
Typically,MoritaTherapyhasusedartinitssecondstage,whichislabeledLight
OccupationalWork,aswellasinthethirdstage,IntensiveOccupationalWork.For
example,thecliniciansasktheirclientstowritedailyjournalsandtomakewood
sculptures.UsingartisanaturalmatterforMoritaTherapy.Second,MoritaTherapy
mightworkwellwithsomepopulationssuchaswithAsianclientswhoarefamiliarwith
Buddhism.Asiancliniciansandthepeopletheytreattypicallyarecomfortablewiththe
philosophybehindit.ItmaybeeasyforAsianstounderstandaboutBuddhist
philosophyandhealingmethods.Otherpeople,whoareinterestedinAsianphilosophy,
32
whoarenotinclinedtoexploretheirunconscious,wholiketomeditate,orwholiketo
makeagardenorsandtraymaywanttouseMoritaTherapy.
33
III:MORITATHERAPY
ConceptofMoritaTherapy
In1917,ShomaMorita,M.D.(1874‐1937),whowasaJapanesepsychiatristin
Japan,formulatedMoritaTherapy.Thistherapyfocusedonacceptingandholdingall
emotions,resolvingconflictingthoughts,andbecomingfreefromobsession(France,M.,
Cadieax,J.&Allen,E.,1995).Moritabelievedthatmentalillnessoccurredbecauseof
conflictbetweenone’sdesireandone’sattempttocontrolanxiety(Morita,1929/1960/
2004;andNakamoto,2009).MoritaTherapydevelopedasatreatmentfor
ShinkeishitsushoorNervosity,whichincludedproblemswithobsessiveshyness,
oversensitivityandfeelingsofinferiority(Ishiyama,1986;Sansone,2005).Morita
(1929/1960)statedthatclientswithShinkeishitsushoorNervosityhadlonghistoriesof
innerconflictsandbehavioralproblemswithsocialadjustment,anxietyandneuroses,
includingobsessiveshyness,oversensitivity,andfeelingsofinferiority(Sansone,2005).
ClientswithShinkeisitsushotendtopersistinunrealistic,dogmaticthinking(Ishiyama,
1990).Inparticular,theseJapaneseneuroticclientstendedtofeelguiltybecauseof
lazinessorself‐centerednessandlackofsociallyresponsiblebehaviorsintheabsenceof
physicalsickness(Reynolds,1969).PossiblybecauseMoritastrictlyselectedclientsfor
hisMoritaTherapytreatment,hisratesofsuccessfultreatmentwerehigh(Ishiyama,
1986).CurrentlyMoritaTherapyisalsousedforavarietyofdisorderssuchas
depression,schizophrenia,borderlinepersonalitydisorder,andalcoholdependence
(Maeda&Nathen,1999).However,MoritaTherapyisnotconsideredsuitableforthe
34
treatmentofacuteschizophrenia,borderlinepersonalitydisorder,oraggressive
behavior(Nakamura,2008).
MoritaTherapyisaholisticapproach,whichmeansthatitisbasedonthe
premisethataperson’smind,body,andenvironmentareconnected.Itiscalledholistic
humannature(Nakamoto,2009).Theholisticphilosophythatnatureandspiritcannot
beseparated,isaconceptthatisendorsedbybothTaoismandZen(Nakamoto,2009).
Accordingtothisbeliefsystem,becausethemindandbodyarerelated,maintaininga
healthybodyleadstohavingahealthymind(Morita,1928/1998).Bothpsychological
andphysicalwell‐beingismaintainedbybalancinginternalandexternalfunctioning
(Morita,2004).MoritastatedthatMoritaTherapyiscognitive,transpersonal,and
experientialpsychotherapy(Morita,1928/1998).
MoritaTherapyisreality‐basedandfocusesmoreon“thehereandthenow”of
theclient’severydaylife.Lessemphasisisgiventopastevents,asthepastcannotbe
changed(Sansone,2005;Nakamoto,2009).Ishsiyama(1986,1990)hasarguedthat
MoritaTherapyisaJapaneseversionofCognitiveBehaviorTherapyaspracticedin
Westerncountries.BothMoritaTherapyandBehaviorTherapytreatmentsshowed
improvementratesof75%to95%forindividualswithobsessive‐compulsivedisorder
withanxietyneuroses(Reynolds,1969).ReynoldssaidthatAcceptanceand
CommitmentTherapy(ACT)intheWestissimilartoMoritaTherapybecauseit
encouragesclientstofocusonpracticingmindfulnesstechniques,ratherthanchanging
theirenvironment(Hofman,2008).Japanesecognitivetherapyisinfluencedby
BuddhismandEasternphilosophy.Westerntherapiestendtofocusonself‐reflection,
35
insight,controlofsymptoms,andsupportofself‐esteem(Ishiyama,2003).However,
thegoalofMoritaTherapyistohelpclientschangetheirmood‐basedandpurpose‐
orientedlifestyles(Ishiyama,1986).MoritaTherapyisconcernedwithchangingthe
client’sdysfunctionalcognitiveandbehavioralpatternsanddoesnotfocusonreducing
symptomsastheprimarygoal(Ishiyama,1986).Itisdifficultforpeopletochangetheir
livingsituationsandespeciallytochangetheirfamilydynamics,evenifthosefactors
affecttheirpsychologicalproblems.Inthecaseofabuse,thevictimsmustberemoved
fromtheiroriginalfamily.Insomesituations,changingenvironmentsisthemost
reasonableaction.However,inmanysituations,ifthechildrenliveindysfunctional
familyenvironments,eveniftheyexperiencepsychologicaldistress,theycannotchange
theirenvironmentsorcaregivers.Itmightbedifficultorimpossibleforthemtomove
fromtheenvironment.
HistoryofMoritaTherapy
Asamedicaldoctor,Morita’sbasictreatmentbeliefswerebasedonZen
Buddhism.Heaskedhispatientstoobeyhisdirection(Fumo/不問),tobecomeinvolved
ininpatienttreatment,andtolearnfromtheirexperiences(Morita,2004;Kitanishi,
2008).Afteratime,hisinitialinpatientprogramranintodifficultiesandwaschanged
intoanoutpatientprogrambecauseofthefinancialproblemsassociatedwithfinding
clinicianswhowereabletoworktwentyfourhoursaday,sevendaysaweek.Today,
outpatienttreatmentisthemainstayofMoritaTherapy.Inaddition,inJapanthereare
nowmanykindsofsupportgroupsinthecommunitysuchas“Seikatsunohakken”and“
Ikigairyohojissenkai”whichcarryoutthegoalsofMoritaTherapy.Thegroupof
36
“Seikatsunohakken”isasupportgroupthatcountsmorethan3,000membersamong
theJapanese.Eachprefecturehasitsowngroup.Seikatsumeansdailylife.Hakkenis
discovery.TheHakkenhavemeetingswithtrainerswhoareeducatedattheMorita
TherapyAssociationandlearntosupporteachotherinregardstotheirmentalhealth
issues.The“Ikigairyohojissenkai”aresupportgroupsforcancerpatientsinJapan.
“Ikigai”meansthatfindingthereasonsforourlife.“Ryoho”meanstreatment.“Jissen”
meanspractice.“Kai”meansagroup.Thesegroupsarededicatedtosupportingcancer
patients,andhelpingthemlearnhowtolivestronglivesdespitetheirillness.Morita
Therapy’stheoreticalframeworkisusefulforthem.MoritaTherapyisabout
holding/acceptingallemotionsandlivingwiththem.Bycontrast,Westerntheories
stresscontrolling/suppressingemotionandfindingit’scauses(Morita,2004;Kitanishi,
2008;Nakamura,Iwaki&Kubota,2007).
Morita’sChildhoodExperiences
Morita’schildhoodaffectedthedevelopmentofMoritaTherapy.He
experiencedfearofdeathduringhischildhood.Moritawasexposedtoapictureofhell
ataBuddhisttemplethathefounddisturbing.Followingtheexposure,hehadrepeated
thoughtsaboutdeath.TheepisodegreatlyaffectedthetheoryunderlyingMorita
Therapy.“Fearofdeath”isoneofthemostimportantelementsofMoritaTherapy
theory.Moritabelievedthatbecausehumanbeingshavefearofdeath,theyalsohave
desiretolive,asthesetendenciesareliketwosidesofonecoin(Morita,2004).Morita
continuedtohavefeelingsof“fearofdeath”duringhisadolescence.Hebecame
anxiousandcontinuedtofeardeath.Heagonizedwithhisfatheraboutit.Hischronic
37
anxietymeantthatheneededanextrayearbeforehewasabletograduatefromschool.
Italsowasafactorinhisrunningawayfromhishome.Later,Moritawrotethateven
whileheexperiencedpanic,healsofeltastrongdesiretolive.
AfterMoritabecameacollegestudenthefoundhimselfinconflictwithhis
father.Inresponse,hedevelopeda“who‐gives‐a‐damn”attitude.Thoughhehadbeen
treatedforhisanxietybyhisdoctor,hequittakinghismedicationanddevotedhimself
tostudyingforhisnextexaminationathiscollege.Theresultofthisdefiancewas
surprising.Hegotgoodgradeswhichhehadneverhadbefore.Throughthese
experiences,hedevelopedanotherprincipleofMoritaTherapy:ifpeoplewantto
removeanxietyandfear,theyhavetoconfrontit.Hestatedthatthereisnowayto
resolvefearexcepttoaddressitdirectly.
Afterhegraduatedfromtheuniversityin1903,Moritabecameapsychiatrist.
HeusedhypnotismandmedicaltreatmentsforhispatientswhohadShinkeishitsushoor
nervosityproblems.However,heconcludedthattheusefulnessofhypnotismwas
temporary,makingthisformoftreatmentnotessential(Morita,2004).Duringthistime
periodMoritastudiedWesternandEasternphilosophiesandpsychology(Morita,
1928/1998).MoritastudiedFreud’stheories(Ishiyama,1986),Montessorimethods,
abdominalbreathing,Shintorituals,andZenmeditation(Nakamoto,2009).
BirthofMoritaTherapy
Moritabelievedthatallhumanbeingshaveafearofliving,aging,gettingsick,
anddeath.ThesearebasictenetsofBuddhism.HecalledthisbeliefSeirobyoshi,生老
38
病死.Sei,生,meansliveandlife.Ro,老,meansaging.Byo,病,meanssickness.Shi,死,
meansdeath.
In1915,beforehestartedhisinpatienttreatmentprogram,Moritahada
significantexperienceinwhichhetreatedapatientwhohadpanicdisorder.Moritawas
abletohelptheindividualinonesession.Thissuccessfuloutcomeledhimtothe
developanoutpatienttreatmentprogramcalledMoritaTherapy.Inaddition,Morita
createdthe“viciouscircleofconflictingthoughts,”afoundationalconceptinhisnew
theory.In1925,Moritaproposedthatemotionsleadtocognitionsandthatthose
determinebehavior(Morita,1995).ThisisrelatedtoanotherbasicBuddhistbelief:
thatthebodyfirstexperiencesandthenchangesfeelings,thenchangesthoughts,and
nextitchangesconsciousness,whicheventuallychangesvolition.Hewrotethatifthe
experiencesofemotionswerenegative,thenabadcircleofthinkingwasinitiatedand
sufferinggrew,whichmeantthatthereweremorechancesthatthepersonwould
becomementallyill.BeforeCognitiveBehaviorTherapywasformulated,Moritahad
taughtthatemotion,cognition,andbehaviorrelatepowerfullytoeachother.
WhenMoritastartedinpatienttreatmentathishomein1919,hisbasicapproach
wastoprovidetreatmentinterventionswiththeexpectationthattheywouldnotbe
questioned.ObeyingMorita’stherapeuticdirection(Fumo/不問)wasconsistentwith
thefirststepinBuddhistmonktraining.Patientswereexpectedtowritedailyjournals
asameanstoenhancetheircognitions.In1926,MoritaTherapyevolvedtoaprogram
thatprovidedtreatmentthroughthemailforpatientswhowereunabletostayinthe
39
hospitalforalongtimeandwholivedfaraway.In1929,Moritaprovidedtherapyin
bothinandoutpatientsettings.
DuringthisperiodwhenMoritawasdevelopingMoritaTherapy,hehospitalized
patientsinhishome,turningitintoaresidentialclinic.TheoriginaltreatmentofMorita
Therapywas40daysintheresidentialclinicofMorita’shome(Maeda,&Nathan,1999).
Moritabelievedthatin‐patienttreatmentwasinevitable,(Morita,1928/1974).The
durationoftreatmentcouldtakeuptoseveralmonths.Moritaobservedhisclients
closely.Duringtheirfirstphaseoftreatment,hepreventedthemfromdoinganything,
andthengraduallyallowedthemtoengageinactivitiesonlyiftheyeagerlyfelttheir
ownSeinoYokuboor“desireoflife.”SeinoYokuboissimilartoFreud’s“lifeprinciple”
orRoger’sstateof“self‐actualization”(Reynolds,1969).Inotherwords,Moritatook
totalcontrolofhisclientsinordertobreakdowntheirhabitofover‐controlling
themselves.MoritaTherapycausestheirself‐defeatingbehaviorandcycleofthoughts
tochangeinapositivedirection(Ishiyama,1990).Thistreatmentmethodiscalled“Re‐
educationalTreatment”orthe“HomelikeEnvironmentTreatment”(Nakamoto,2009).
HowMoritaTherapyViewsPathology
AmostimportantgoalofMoritaTherapyistheeliminationofthe“viciouscircle
ofconflictingthoughts”(Morita,1995,p.112).Moritastatedthatsufferingisnotthe
naturalresultofmentalillness.Rather,sufferingoccurredasaresultofthe“vicious
circleofconflictingthoughts”(Morita,1995).Moreover,hebelievedthatmostpatients
whohadamentalillnesswerecaughtupintheviciouscircle.Thepatientsbelievedthat
theywerepowerlesstoovercometheirillness,butthatwasincorrect.Theyjustneeded
40
tounderstandhowthecircleworked,andhowtocutitoutoftheirlives(Morita,1995;
Kitanishi,2008;andNakamura,Iwaki,&Kubota,2007).
BothCognitiveBehaviorTherapyandMoritaTherapybelievethatavoiding,
controlling,suppressing,andendlesslysearchingforthecauseofemotionscreatesa
viciouscycleandadownwardspiral(Nakamura,Iwaki,&Kubota,2007).Thedifference
betweenthetwotheoreticalorientationshastodowithhoweachunderstandsthe
circleandwhateachproposestodotoaddressit.MoritaTherapytheorizesthat
anxietyistheoppositeofdesire.Itisimportantforapatienttoacceptandlivewith
anxietyandfearbecausetheseaffectivestateswillnotdisappear.CognitiveBehavior
Therapy(CBT)believesthatifpeoplechangetheirthoughts,theirbehaviorswillchange.
CBTteachesthatanxietyandfeararelearnedreactionsthatcomefromwrongthoughts.
TheemphasisinCBTisonchangingone’scognitions.Bycontrast,MoritaTherapy
focusesonaction.ThisisconsistentwiththeBuddhistbeliefthatnothingisrealexcept
foractions.
TheCoreofMoritaTherapyPathology:ViciousCircleofConflictingThoughts
(Akujyunkan/悪環)
Pathology,accordingtoMoritaTherapy,comesfromthe“viciouscircleof
conflictingthoughts,”(Morita,1995),MoritaTherapytreatmentstrivestocutthrough
thecycleandtofocusonaction(Morita,2004;Nakamura,Iwaki,&Kubota,2007;
Kitanishi,2008;andNakamura,2008).Moritatherapistsanalyzewheretheirpatients
areinthecycleofissuesthatstemfromthe“viciouscircleofconflictingthoughts”
(Kitanishi,2008).

41
Kitanishi(2008)believedthattheviciouscircleofconflictingthoughts
(Akujyunka悪循環)wasaffectedbytherelationshipsamongemotion,cognition,and
behavior.Nakamurasaidthatthecyclehappenedasaresultoftherelationshipamong
attention,clingingbehavior,andnarrowthinking.Thesetwotheoristsuseddifferent
wordsforexplainingtheviciouscircle,butMoritausedbothsetsofwords.
Figure1.ViciousCircleofConflictingThoughts(Akujyunkan悪循環)
Agoodexampleoftheviciouscircleofconflictingthoughtscanbefoundinthe
experienceoftraumavictims.Whenclientsremember,focuson,andattendtotheir
traumaticmemories,theysuffer.Theiremotionsbecomeheightenedandtheyoften
experienceacuteanxiety.Themoretheyremember,recallandthinkaboutthose
memoriesagainandagain,themoretheyexperiencesuffering.Thepainfulemotions
increaseinstrengthbecausethefeelingsbecomeincreasinglysensitive.Negative
cognitionandclingresult.Eventually,clientsbecomedysfunctionalbecausethose
Cognition Clinging Behavior
Narrow thinking
Emotion Attention
42
experiencesaffecttheirbehaviorandnarrowtheircognitivefocusincreasinglytowards
thetrauma.Finally,theybecomeslavestotheviciouscycleandthecyclebecomesa
downwardspiral.Theycannotbearthosepainfulexperiencesandbecomementallyill.
AHypotheticalCaseoftheViciousCircle
TheTraumaticEvent
WhenMs.AusedaMetrobustogotohospitalforherappointment,shecouldnotget
offtherightplace.Shemissedthebusstopwhereshewantedtogetoff.Shewasupset
andwaslateherappointment.
AttentiontoNegativeEmotionalExperiences
Atthenextappointmentday,sherememberedthatshehadgottenupsetandmissed
herappointment.Thosememoriescreatedinherthesamefeelingsthatshehad
undergoneduringthetraumaticevent.Shewasupsetandfeltbadagain.Shereadily
focusedonhavingmissedthebusstopandhavingbeenlatetoherappointment.She
gaveattentiontothesethoughtsandemotions.
NegativeCognitionandClingtotheNegativeEmotions
Ms.Awasafraidoftakingabus,butshedidnothaveacar.Sheclungtothenegative
thoughtsagainandagain.Sheimaginedthatifshetookthebus,shewouldstillnot
likelygetthereontime.Shethoughtherdoctormightbedisgustedwithher.Those
negativethoughtsandpainsrolledoverherlikewaves,attachingthemselvestoher.
Shesuffered.

43
BehaviorandNarrowThoughts
Ms.A.believedthatsheshouldbeontimefortheappointmentinordertobeaperfect
andgoodpatientforherdoctor.Shedidnotwanttomakemistakes.Shebelievedif
shecouldnotmakeit,itwasshameful.Itmeantthatshecouldnotdoanythingright.
AViciousCircle
Ms.A.rememberedandrecalledthefirstevent,andthenshethoughtthatshehadto
bethereontime.Ontheotherhand,shewasafraidofmakingthesamemistakeand
arrivingtoolate.Shebelievedthatsheshouldnotbethatkindofperson.Shewas
afraidoftakingabusandgoingout.
Thesufferingcamefromthegapintheclient’sthoughtsbetweenherimagined
ordreamideaofselfandherrealself.Shebelievedthatsheshouldbeherimaginedor
dreamedperfecthumanbeings.Ifthegapbetweenidealandrealisverylarge,people
becomementallyill.
*PathologicalormentallyillImageisbiggerthanreal
*Healthyfunction
Figure2.DiscrepancyBetweenImaginaryandRealSelf
RealFigureEmotion:Anxiety
Can’tdoit.Afraidofit.
Theexample:Imightbelateandmightmissthebusstop.Emotion:Iamafraidofbeinglate.IhaveanxietythatIwillmakethesamemistake.
ImaginaryFigureDesire
Shouldbedoneperfectly.Theexample:Ishouldbeontimetotheappointmentandshouldnotmissthebusstop.
44
MoritaTherapystrivestocutthroughtheviciouscircle.Theviciouscircle
happenswhentheimaginaryself(desire)isbiggerthanrealself(reality).Clientswho
havethetendencytobelievethattheyhavetobebetterthantheyreallyare,Morita
namedas“ShisounoMujun/Incongruentideas”(Morita,2004).Incongruentideas
takeplacewhenpeoplehaveconflictingideasbetweendesiresandrealities.
HumanRelationshipsWithintheViciousCircle
TheviciouscircleandShisounoMujun/Incongruentideashappennotonlyin
regardstoanindividual’spsychologicalorphysicalstate,butalsowithinhuman
relationships.Anexampleofindividualpsychologicalandphysicalpainisasfollows.Ifa
persongetsinacaraccident,theyfeelpainbecauseoftheevent.Whentheyfeelpain,
theyremembertheaccident.Atthetimetheyhavememoriesoftheaccident,andthey
experiencepainpsychologicallyandphysically.Theybelievethattheaccidentisthe
causeforalltheirpain.Whentheyseeorthinkaboutacar,theviciouscirclehappens
andtheydonotgooutside.
Anexampleofhowtheviciouscircleoperateswithinarelationshipisasfollows.If
parentsfocusontheironlychild,theirparentingstylebecomesoverprotective.The
childisunabletothinkandmakedecisionsbyherself.Thechildmightfinditdifficultto
communicatewithfriendsatschool.Themoredifficultythechildhasatschool,the
moredistresstheparentsexperienced,leadingthemtoprotecttheirchildtoagreater
extent.Thisexampleshowstheviciouscircleofrelationships.MoritaTherapyhasa
uniqueapproachtosolvingtheseissues.
45
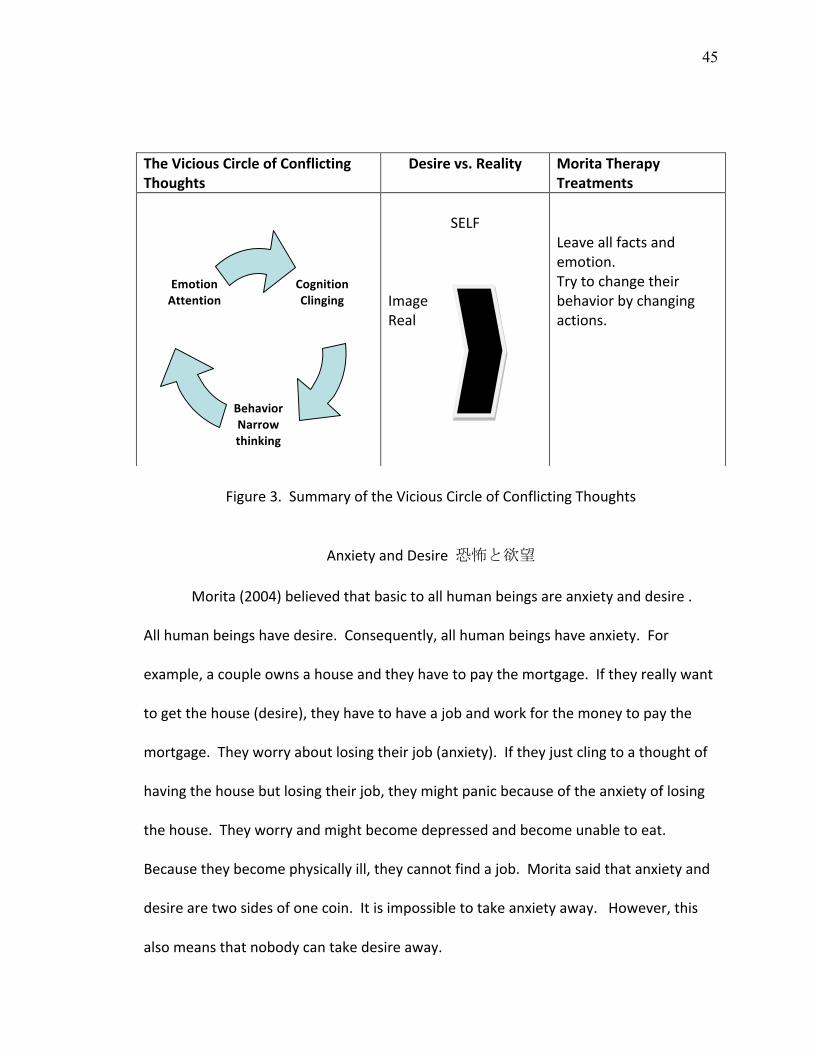
Figure3.SummaryoftheViciousCircleofConflictingThoughts
AnxietyandDesire恐怖と欲望
Morita(2004)believedthatbasictoallhumanbeingsareanxietyanddesire.
Allhumanbeingshavedesire.Consequently,allhumanbeingshaveanxiety.For
example,acoupleownsahouseandtheyhavetopaythemortgage.Iftheyreallywant
togetthehouse(desire),theyhavetohaveajobandworkforthemoneytopaythe
mortgage.Theyworryaboutlosingtheirjob(anxiety).Iftheyjustclingtoathoughtof
havingthehousebutlosingtheirjob,theymightpanicbecauseoftheanxietyoflosing
thehouse.Theyworryandmightbecomedepressedandbecomeunabletoeat.
Becausetheybecomephysicallyill,theycannotfindajob.Moritasaidthatanxietyand
desirearetwosidesofonecoin.Itisimpossibletotakeanxietyaway.However,this
alsomeansthatnobodycantakedesireaway.
TheViciousCircleofConflictingThoughts
Desirevs.Reality MoritaTherapyTreatments
SELF
ImageReal
Leaveallfactsandemotion.Trytochangetheirbehaviorbychangingactions.
CognitionClinging
BehaviorNarrowthinking
EmotionAttention
46
HumanBeings
AnxietyDesire
Figure4.TheConnectionBetweenAnxietyandDesire
Morita(2004)statedthatifhumanbeingsareunabletoeliminateeitheranxiety
desire,theyhavetoacceptandholdtheseasnaturalphenomenon.Additionally,he
statedthathumanbeingshavetofindsomethingthatwecandoafteracceptingand
holdinganxietyanddesire.Otherwise,humansengageinself‐negation.
NatureTheory自然論
NatureTheoryisonewayofunderstandinginMoritaTherapy.Morita(2004)
statedthatitwasnaturalforhumanbeingstohavealotofkindsofemotions.He
believedthatanger,jealousy,anddesirewerenormalhumanreactions.Forhim,these
arenotpathologicalreactions.Normalhumanreactionsbecomementalillnessonly
whenthereactionsaresuppressedbyourcognitions.Ifanaturalphenomenonsuchas
anger,jealousy,desire,andotheremotionisaccepted,itwillreachitspeakand
eventuallydisappear,likeanormaldistributionfunctionline.Evenwhentheemotions
47
taketimetopeak,itisimportanttoholdallofthemuntiltheydisappear(Morita,2004;
Kitanishi,2008).
CorePrinciplesofMoritaTherapy
ShisounoMujun/IncongruentIdeas
Incongruentideasmeanthatpeoplehaveconflictingideasbetweentheirdesires
andreality.Often,realitydoesnotallowadesiretobeobtained.Forexample,ifone
thinksthatitisnecessarytogotothegymeverydayat6a.m.beforeworkbutcannot
wakeupandgoatthattime,onemightfeelalotofstress.Thus,thereareincongruent
ideasbetweenone’sdesireandreality.Moritasaidthatifpeopleareobsessiveor
attachedtooneidea,theirthoughtswillbelimited.Theywillbeunabletoentertain
otherideas.Hesaidthatclientsdonotneedtothinkintermsof“shouldand
shouldn’t.”Evenifonecannotgotothegymat6a.m.beforework,onewillbefineand
canchangeone’splanstofitwithreallife.
SyukanandKyakkan/SubjectiveandObjective
Moritasaidthatiftheclientsfocusontheirsymptomsorfeelingsstrongly,theywill
havedifficultythinkingaboutothermatters,suchastheirreallifewithitsdailyroutines.
Theymaypersistinthinkingabouttheirsymptomsandfeelingssubjectively.Ifaclient
feelsthatway,theclinician’sobjectiveadvicewillnotwork.
KanjyoandChishiki/EmotionandKnowledge
Peoplehaveemotions,buttheymaytrytocontroltheiremotionswiththeir
intellect.However,havingandfeelingemotionsarenaturalforhumanbeings.Morita
48
advocatedthatwetrynottocontrolouremotions.Itisfinetofeelemotions.Ifpeople
trytocontrolemotions,theywillfocusonthemunconsciously.Bycontrast,ifthey
leaveemotionstoruntheirnaturalcourse,andsimplyholdthem,theemotionswill
calmdownanddisappear.Shinkeisitsushoclientstrytocontroltheiremotions,which
makestheemotionsworsebecauseofobsessing.
TaitokuandRikai/LearningfromExperiencesandDeepUnderstanding
Taitokumeansthatpeoplelearnfromtheirexperiences.Rikaimeansthatpeople
understandwisdomthroughknowledgeandimagination,andabstractideas.Morita
statedthatdeepunderstandingcomesfromlearningexperiences.Learningexperiences
stronglyencouragesthedevelopmentofwisdom.ThatmaybewhyMoritaprovided
learningexperiencestohisclientsinaresidentialtreatmentsetting.
ShinnenandHandan/BeliefandDecision
BehaviorscomefromShinnen,beliefswhicharesubjectiveperspectives,
emotions,andexperiences.Thesesamefactorsshapepersonality.Ontheotherhand,
knowledgeandunderstandingaffectbehaviorindirectlyaselementsofdecision‐making.
Thatmeansthatknowledgeandunderstandingarejustsurfaceaffectations.Clinicians
needtoknowtheirclient’spersonality.However,ifpeoplearemotivatedtoobtain
knowledgeandwisdomandfindthesebythemselves,thoselearningexperiences
stronglyaffectpersonality.
RonrinoSakugo/LogicalAnachronism
Itisveryimportantforclinicianstounderstandtheclient’ssubjectiveand
objectiveperspectivesandtherelationshipbetweentheiremotionandtheir
49
intelligence.Understandingtheclient’sbasicemotionalfunctioningisespecially
significantbecausethosefactorsareveryimportantelementsforunderstandingthe
client’spersonality.Ifcliniciansignoretheirclient’semotionsorperspectivesontheir
illness,andjustgiveclinicaladviceordirections,treatmentwillnotwork.Theclient’s
perspectivesandbeliefsaretheirrealworld.Cliniciansneedtounderstandhowthese
foundationsareconstructed.
ShizenandJini,MokutekiandSyudan/NatureandArtifice,GoalandSteps
Moritawrotethatphysical,mental,andpsychologicalphenomenaarenatural
matters.Nobodycanchangethem.However,mostpeoplebelievethattheycan.
Peopleshouldliveinharmonywithnatureandbenatural.Ifpeoplelackmotivation,
theyneedtowaitfortheirmotivationtochange.However,MoritaTherapyand
Buddhistphilosophybelievethatchangingbehavior/actionsareanaturalpathwayto
change.
KannennnoKyatukanntekiTouei/ConceptofObjectiveProjection
Acquiringself‐confidenceandcouragearedifficult.Similarity,itisdifficulttoleave
orgetridoffeelingsofagonyoranguish.Moritataughtthatthereweretwowaysto
leaveandholdfeelingsofagonyandanguish.Oneistoallowoneselftofeelandbein
thosefeelings(Arugamama/beinnature).Anotherwayistofocusonandtoobserve
andcriticizeone’sfeelings,observingthefeelingsobjectively.
Shizenfukujyu/ObeytheLawsofNature
Whenpeoplesuffer,theyfeelpainandanxiety.Thosearenaturalfeelings.When
itiswinter,peoplefeelcold.Thatisnaturaltoo.Shinkeisitsushopatientstendtothink
50
thattheyshouldnotthinkorfeelthattheyarecold.Iftheythinkthattheyshould
changethemselves,therewillbeconflictbetweentheirideasandtheirrealities.
SeishinnoKikkouSayo/PsychologicalConflicts
Peoplehavetwoactionsthatinteractwithintheirmind.Whenonefeelsanxiety
(firstaction),onetriestogetridofthefeelingorfindasolutiontoreduceanxiety
(secondaction).Ifthefirstfeelingisstrong,thesecondactionalsobecomesstrong.If
thefirststimulationisstrong,thefollowingsecondactiontendstobestrong.Ifthefirst
reactionisnotstrong,onedoesnotneedtotakestrongactiontoreducethereaction.
Theseinterplaysarenaturalmatters.Shinkeisitsushopatientsoftenhavestrong
reactionsofwhichtheystronglydesiretoridthemselves.Whenpeoplehavestrong
psychologicalconflicts,theyhaveagony,andproblems.
KyogunoSentaku/ChoiceofSituation
Whenpeoplefeelagonyandanxiety,itisimportantforthemtoholdthose
feelingsbecausethefeelingsarenaturalandreal.Onedoesnotbenefitfromchoosinga
differentsituationinordertoavoidfeelinganxious.Itisbetterforustofeelanxietyand
beinreality.
SyukanToiukotonoImi/MeaningofSubjectivity
Whenonedrinkswaternaturallywithoutanythoughts,thatbehaviorissubjective.
Onedoesnotexperiencefeelingsasaresultofsubjectivebehavior.Thepurely
subjectiveisnotalinguisticexperience.Whenoneuseslanguageorthinksabout
behavior,itisobjective.Objectivityincludesotherpeople’sperspectiveandthoughts.
51
Chui/Attention
Peopledonotneedtofocusonaspecificmatter.Weareabletolivewithout
focusingonorgivingattentiontoourdailylivesandbodilyfunctions.Shinkeisitsusho
clientsfocusonorgiveattentiontospecificmatters.
ChuitoIshikinoKankei/RelationshipbetweenAttentionandConsciousness
Moritaallowedpatientstofullyfocusontheiragonyinsteadofavoidthinking
aboutit.Sinceitisalreadyanaturalsituationforpatientstothinkabouttheiragony,it
isbetterforthemtofeelenoughpainuntilthepainlessensandgoesaway.
SeishinnoChowa/BalanceofMinds
Ifpeoplearehypersensitivetostimulation,theymightbeobsessiveaboutor
irritatedbynoiseandotherstimulation.Theyfeeluneasyandtrytodismissthenoise
fromtheirminds.Ontheotherhand,ifpeoplearenotawareofthesenoises,theyare
notuncomfortablewiththematall.Moritabelievedthatitisimportantforpeopleto
beabletofindbalancebetweentheirmindsandoutsidestimulation.Shinkeishitsusho
patientstendtobehypersensitive.
Mushojuusin/DailyFunctioning
Itisimportantforhealthymindstobeactive,butitisnotgoodformindsifthey
arefocusedonjustonepoint.BecauseShinkeisitsushopatientstendtofocusonone
area,theirmindsandresultingbehaviorsintheirdailylifearedysfunctional.
KannjyounoHousoku/RulesAboutEmotions
Moritasaidthattherearefiverulesaboutintenseemotions.
52
1.Emotionswillcalmdownanddisappearlikethecurveofamountain,i.e.,intensify
andthengraduallydecrease.
2.Iftheimpulsesatisfies,thefeelingswilldisappear.
3.Peoplewillnotfeelstronglyabouttheiremotionsiftheydonotstimulatethemtoan
obsessivelevelorrejectthemaltogether.
4.Whenemotionsarestimulatedconstantlyandfocusedon,theybecomestrongerand
stronger.
5.Emotionsarederivedfromnewexperiences.Emotionsarestimulatedbyrepetition.
Morita’sideaswerebasedontheconceptofdependentoriginationinBuddhism,
whichissimilartoSatipathanaSutra,thesutraformeditationonthebody.
Psychopathology
CharacteristicsofPatientswhohavetheViciousCycleofConflictingThoughts
Typically,apersoncaughtinthiscycletendstobeintroverted,perfectionist,self‐
centered,analarmist,andeasilyworried.Thegapbetweentheiridealselfandrealityis
large.Theperson‘srealityisnotacceptedbythemselves.Thepersoncompares
themselvestotheidealandlooksforfault.Thepersontriestodothethingthatcannot
bedone.Thepersonisanxiousandworriesaboutotherpeople'sevaluation.The
personishighlyinfluencedbythejudgmentofothersandchangestheirspeech,
behavior,andeventheirvaluestomatchtheopinionofothers.Theyhaveanobstinate
andunyieldingspirit.
TreatmentGoalsinMoritaTherapy
53
Moritatherapistsencouragepatientstolookatandaccepttheirrealselves.
Clientsaretaughtthattheyarenotperfectpeople.Thatmeansthattheyneedto
acceptandholdtheirfeelingsandlearntolivestrongandwell.
Clientsneedtochangetheiremotionally‐basedthinkingandlearntofocuson
action.Forexample,oneclientcouldnotbuyashirtheneededduetosevereanxiety
aboutconversationsthatmighttakeplacewiththepeoplewhoworkedatthestore.In
thiscase,Moritatherapistshelpedtheclientfocusonthespecificgoalofbuyingashirt.
Whentheclientcouldgotoastoretobuyashirtwithouttheworryandanxiety
stoppinghim,thepersonreachedoneofhisgoals.Whenclientshavesuccessful
experienceslikethis,theyareabletocutthroughthe“viciouscircleofconflicting
thoughts.”
AnothergoalinMoritaTherapyistoreachthestateofArugamama‐‐acceptance
ofrealityasitis(Hofman,p.282,2008).Ishiyama(1986)clarifiedthatMoritaTherapy
encouragesacceptanceofaclient’stendencytowardnervoussensitivityand
anxiousness,butdoesnotencouragefocusingonpersonalweakness.MoritaTherapy
considersanxietytobeanacceptableemotionthatonedoesnotneedtobattle
(Ishiyama,1986).Obeyingnaturebyacceptingunwantedthoughtsandfeelingsis
betterthantryingtochangeanunchangeablesituation(Hofman,2008).Ultimately,
acceptanceincludesacceptingaginganddeathbecausethesearenatural(Kitanishi,
2007).
54
TargetSymptomsAddressedbyMoritaTherapy
MoritatargetedShinkeishitsushoornervousproblemsbecausemanyofhis
patientshadthosesymptoms.Inaddition,hehadexperiencedsimilarsymptomsinhis
ownlife.Inhisera,JapanesesocietyfacedstrongsocialstressorsasaresultofWorld
WarI.Afterthewar,theJapaneseeconomydevelopedrapidly,andpeoplehadtowork
harderthanbefore.Eventhoughtheyworkedhard,theydidnotachieveprosperity
becauseoframpantinflation.Manypeoplehadanxietyabouttheirsituation.Morita
hadmanypatientswhohadShinkeishitsushoornervousproblemswhichincludedno
motivationtolive.Ishiyama(1990)describedthesituationbynotingthat“theMorita
therapisthelpsclientstofocusontheirneglectedself‐actualizingdesiresandabilityto
chooseactionandhelpsthemtoleavetheescalatedemotionalsymptomtoanatural
healingprocess”(p.556).
MoritafoundthatevenShinkeishitsushoclientshadthedesiretohavegood
health,solidrelationshipswithothers,andmeaningfullifegoals.Theirproblemswere
connectedwithtryingtobemoreperfectthanothers(Morita,1929/1960/2004).
MoritaTherapyinterventionschangetheclient’slifestyle(Ishiyama,1986).
OnereasonwhyMoritawasinterestedinpatientswhohadShinkeishitsushoand
nervosityproblemswasthathehadfacedsimilarsymptomsinhislife.Heexhibited
clingingbehavioratsomepointsinhislife.Heexperienceddebilitatingfearsofdeath
andahighdegreeofanxiety(Morita,2004).Hewantedtobeperfect.Hisanxiety
primarilycamefromhisrelationshipwithhisfather.Inhiswritingheacknowledged
thatconflictwithhisfatheraffectedhissymptoms.Forinstance,whenhewasastudent
55
atTokyoNationalUniversityMedicalSchool,hisfatherdidnotsendmoneytohim.
Moritawasdepressedandanxiousandexperiencedpanicattacks.Herecoveredby
changinghislifestyleatthattime.Helearnedfirsthandthatifpeoplewhohaveanxiety
changetheirlifestyles,theirsymptomscandisappear.
Moritasoughtfromhispatients,theirvoluntarywilltochange(GikeiMedical
SchoolofMoritaTherapyCenter,2007).Moritabelievedthatifpatientswerenot
motivatedregardingtheirtreatment,theywouldnotimprove.Clinicianscannotforce
theirclientstochangetheirbehaviorbecausetheclientssometimesresist(Ishiyama,
1990).Itisimportantforbothclientsandclinicianstofeelanaturalandspontaneous
motivationtowardengaginginanyactivities(Morita,2004).Moritastatedthatthisidea
wassimilartoMontessoriteachingmethods(Morita,2004).
TargetGoalsofMoritaTherapyToday
Nakamuta(2008)statedthatthesedays,Moritatherapistschooseclientswho
possessgoodjudgmentbecauseitisimportantforclientstounderstandaboutthebasic
theoryofMoritaTherapy.Clientsneedtheabilitytounderstandthattheyhave
responsibilityfortheirproblemsandtheyneedtohavesomeegostrength.Clientsmust
beabletorealizethattheysufferasaresultofthediscrepancybetweentheiridealand
realselves.MoritaTherapyiseffectiveforcancerpatientsandmostofthementallyill
withtheexceptionofpatientssufferingfrombipolardisorderoracuteschizophrenia
(Nakamuta,2008).
56
MoritaTherapyandBuddhism
ThephilosophyofMoritaTherapyissimilartoZenBuddhism,whichwasthe
religionpracticedbyMorita’sfamily.Morita(1934)statedthatafterheformulated
MoritaTherapy,hefoundsimilaritiesbetweenhisnewsystemoftherapyandZen
Buddhism.MoritaTherapywasinfluencedbyJapaneseandEasternculturewhichare
Buddhist(Suzuki,1989).Zen,MoritaTherapyandJapanesecultureasawhole,allplace
importanceonacceptingone’sphenomenologicalreality(Suzuki,1989).Thisis
reflectedinMorita’sprimaryprincipal,“Acceptance.”Whenclientshaveapositiveview
ofacceptance,theyareabletobenefitfrompracticalactivities(Ishiyama,1986).
MoritadidnotformhistherapybasedentirelyonZen.However,hehadadeep
understandingofthebasicphilosophyofZen(Suzuki,1989)andusedmanyZenwords
andillustrationsasexamplestosupporthisstatements.TheJapanesearealmost
entirelyBuddhist.ZenhashadanimportantplaceinJapanesesocietyforsome2,000
years.Naturally,JapanesepeoplehavebeenheavilyinfluencedbyBuddhism,even
Japanesepeoplewhoareapartofadifferentreligion.Oneexampleofthefundamental
principlesofBuddhismthathaveinfluencedMoritaTherapyistherenouncementofall
possessionsandattachmentstomaterialthings.InMoritaTherapy,thisprinciplehas
beenextendedtomeangettingridofmentalobsessionsaswellasotheradherencesor
attachments,eveniftheyaregenerallyregardedasvirtues.
AnotherBuddhistprinciplethathashaditseffectonMoritaTherapyis“donot
thinkyouhavetodosomething,andifyouthinkthatyoucannotdosomething,donot
doit”(Kitanishi,2007).ThesimilarMoritaTherapyprincipleistonotthinkaboutwhat
57
youhavetodo,buttoacceptyouremotionsandlimitations.Ifanactionistoohardto
achieve,youdonothavetoforceyourselftoattemptit(Kitanishi,2007).Nakamoto
(2009)taughtthatmindandbodyshouldbebalancedbynature.Ifpeoplehave
emotionalconflictsanddisharmoniesintheirmindsandlives,theseproblemswillbe
solvednaturallybytime.Humanshavestrongsurvivalabilitiesthatarenaturalsystems
becausewearepartofnature(Nakamoto,2009).Ourmindsandemotionsalways
changebecauseweareinfluencedbymanypeople(Nakamoto,2009).Itisimportantin
MoritaTherapyforclientstoacceptthemselvesandtolearnhowtolivewiththeir
emotions(Nakamoto,2009).
MoritaTherapyandWesternPsychology
MoritaTherapyandBuddhismbothteachthatthebodygeneratesfeelingsthat
leadtothoughts/cognition,whichleadstobehavior.ThatiswhyMoritaaskedhis
clientstodosomeactionswithoutanyquestions.Zenmonkswereoftenaskedtodo
workwithoutanyconversationsorquestionsoftheirteachers.However,mostWestern
psychologiesbelievethatcognitionleadsbehavior.Inaddition,Westernpsychology
looksforthecausesofsymptomsinlightofthebeliefthatourthoughtsareableto
controlemotionsandsituations(Kitanishi,2007).Easternpsychologydoesnotfocuson
thecauseofsymptomsbecauseitbelievesthatpeoplecannotanddonotneedto
changetheirsituation.MoritaTherapyfocusesuponacceptingallkindsofemotions
andenvironments.MoritaTherapyisanexperientiallearningsystem,anapproachthat
isdifferentfromWesterntherapy(Ishiyama,1987).MoritaTherapyholdsthatall
psychologicalproblemsstemfromanxiety(Kitanishi,2007).AccordingtoMorita
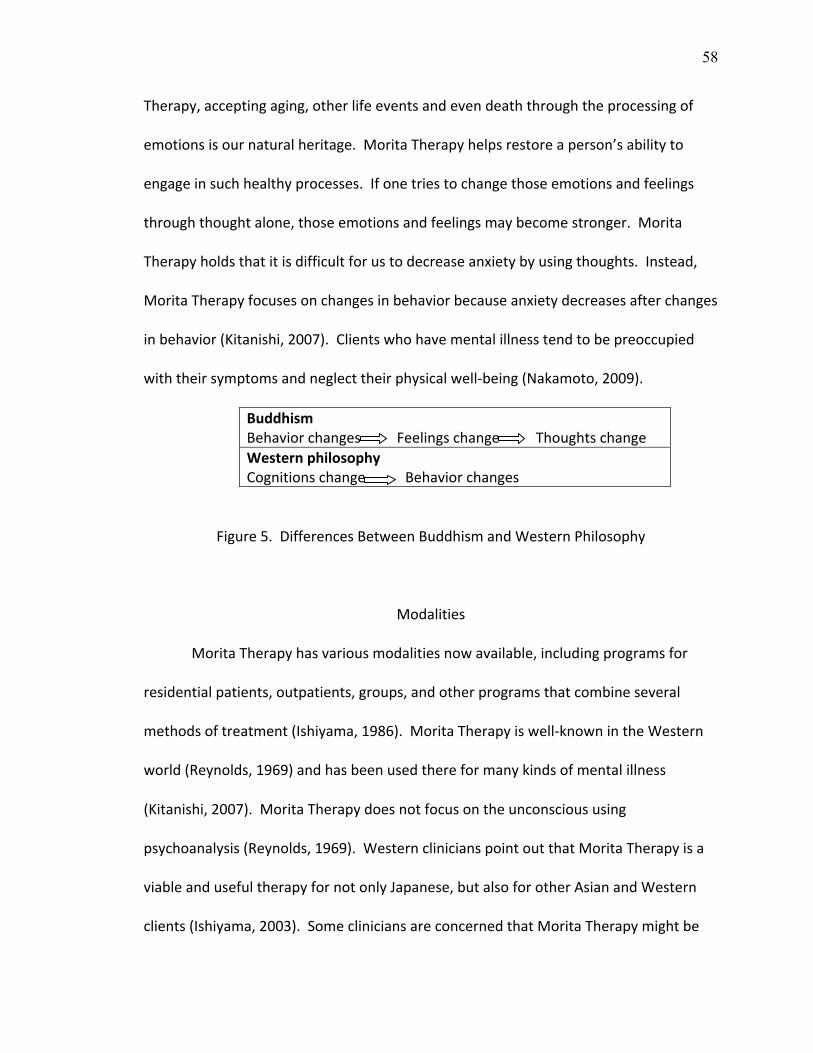
58
Therapy,acceptingaging,otherlifeeventsandevendeaththroughtheprocessingof
emotionsisournaturalheritage.MoritaTherapyhelpsrestoreaperson’sabilityto
engageinsuchhealthyprocesses.Ifonetriestochangethoseemotionsandfeelings
throughthoughtalone,thoseemotionsandfeelingsmaybecomestronger.Morita
Therapyholdsthatitisdifficultforustodecreaseanxietybyusingthoughts.Instead,
MoritaTherapyfocusesonchangesinbehaviorbecauseanxietydecreasesafterchanges
inbehavior(Kitanishi,2007).Clientswhohavementalillnesstendtobepreoccupied
withtheirsymptomsandneglecttheirphysicalwell‐being(Nakamoto,2009).
BuddhismBehaviorchangesFeelingschangeThoughtschangeWesternphilosophyCognitionschangeBehaviorchanges
Figure5.DifferencesBetweenBuddhismandWesternPhilosophy
Modalities
MoritaTherapyhasvariousmodalitiesnowavailable,includingprogramsfor
residentialpatients,outpatients,groups,andotherprogramsthatcombineseveral
methodsoftreatment(Ishiyama,1986).MoritaTherapyiswell‐knownintheWestern
world(Reynolds,1969)andhasbeenusedthereformanykindsofmentalillness
(Kitanishi,2007).MoritaTherapydoesnotfocusontheunconscioususing
psychoanalysis(Reynolds,1969).WesternclinicianspointoutthatMoritaTherapyisa
viableandusefultherapyfornotonlyJapanese,butalsoforotherAsianandWestern
clients(Ishiyama,2003).SomecliniciansareconcernedthatMoritaTherapymightbe
59
difficulttoacceptforWesternclientsbecauseofculturaldifferences(Ishiyama,1987).
However,thesedaysmanypeopleareinterestedinBuddhismandhaveusedpractices
suchasZengardenandmeditation.Ifinthefuture,MoritaTherapygarnersscientific
evidenceastoitseffectiveness,MoritaTherapywillbeusedmoreprominently
throughouttheworld.MoritaTherapyhasdevelopedovertimeinJapan.Theoriginal
MoritaTherapyhasnotperseveredintheexactsameform.ThisprovesthatMorita
Therapycanevolvetofitintodifferentenvironments.MoritaTherapyshouldbe
developedtomeettheneedsofdifferentculturesindifferentcountries.
Treatments
OriginalStagesofMoritaTherapyTreatmentAsPracticedbyMoritaandPossibilitiesfor
GreaterIntegrationwithArtTherapy
Moritaemphasizedthateffortdoesnotalwaysleadtoresults.Hestatedthat
mosttreatmentswerenoteffectiveifclientswereobsessive,inotherwords,attached
toonethought.Whatismostimportantisforclientstoleavetreatmentandfirst
decreasetheirattachmentbeforetheycaneffectivelyreentertherapy.Moritastated
thatclinicianshavetoassessanddiagnosepatients.Withoutassessmentanddiagnosis,
theycannotlocatethecoreissuesbehindthesymptomsandpsychopathology.Morita
likenedtheprovidingoftreatmentwiththelackofproperassessmentanddiagnosisto
committingafelony(Morita,2004).WhenheformulatedMoritaTherapy,heutilized
strictselectioncriteriaandonlyworkedwithclientswithShinkeishitsushowhohad
hypochondriasis,anxietyneurosis,phobic‐obsessiveneurosis,orpsychogenicphysio‐

60
motormalfunctions(Ishiyama,1986).Oncepatientswereidentified,diagnosedand
readyfortreatment,theyweretakenthroughfourstagesoftherapy,asfollows.
TheFirstStageofIsolationandRest
Duringthisstage,clientsareisolatedfromhumancontactandrestrictedfrom
anyactivitieswiththeexceptionofusingthetoilet,eatingandbathing.Thepurposeof
thisstageisforclientstorestphysicallyandmentally.Clientshavetocalmdownand
lookattheirinnerthoughtsandrecouptheirstrength(Nakamoto,2009)beforethey
canengageinmoreactivetreatment.BecauseWesternclientsneedmoreverbal
communicationfortheirtherapysessions,Westerntherapiesencourageclientstotalk
andexpresstheiremotions,toanalyzeandcontroltheirsymptoms(Ishiyama,2003).
However,Moritahadhisclientsisolatedfromanybody,anyactivities,andany
interaction.Moritabelievedthatclientsneededtoreflectwiththemselveswithout
interference.Whenclientsareabletoaccepttheiremotions,theymayexperience
inconvenient,painfulorstressfulfeelings.However,throughthisprocess,clientscan
recoverfromtheirfatigueandbegintochangebehaviors(Ishiyama,1990).Morita
(1998)statedthatthegoalofthistherapyistofundamentallybreakloosetheclient’s
mentalsufferingandpain.Itallowsthemtoexperiencethementalstatehereferredto
asimmediateliberationthroughconfrontationwithone’ssuffering(Morita,1998).
Duringthisstageartisnotbeneficialbecausethepatientshavetoliedownandarenot
allowedtoengageinactivities.

61
TheSecondStageofLightOccupationalWork
Duringthisstage,clientsarestillprohibitedfromengaginginconversations,
amusements,andactivemovementsbecausethoseactivitiesdiverttheirconcentration
fromreflectionanddevelopinginsight.Inthisstage,therapistsdonotgivetasksto
clients.Therapistshavetowaitfortheclient’smotivationtoincrease.Itisimportantin
thistreatmentthattheclientresumesfeelingnaturalandspontaneousmotivation
towardengaginginactivities.Smallactivitiessuchasjournalwritingandartactivities
afterdinnerareallowed(Morita,1998).Theclient’slifestylewascontrolledbya
structuredschedule.ThisisconsistentwiththefocusinMoritaTherapyonlifestyles
ratherthansymptoms.
Duringthisstage,arttherapycouldbeapartofthetherapeuticprocess.Art
therapistsmightbeabletochooseartmaterialsforeachclient.Forexample,some
clientsmightnotliketowrite,butmightliketodrawormakeacollage.Drawingand
scribblingmightbeagoodartdirectionforclientsduringthisslowandquietperiod.
TheThirdStageofIntensiveOccupationalWork
Duringthisperiod,clientsareencouragedtoengageinanylargemotorskill
activitiessuchassawing,choppingwood,anddiggingholesinthefields.Through
intensivework,clientsexperiencethereemergenceofpatience,cultivateself‐
confidence,accomplishsmallsuccesses,andappreciatethevalueoflabor.Such
experienceshelpclientsovercometheirpainanddifficulties(Morita,1998).Thisstage
focusesonsupportingthenaturalinterestsofclients.Certainlytherearemany
possibilitiesregardingtheintegrationofarttherapywiththisstageoftreatment.Some
62
clientsdonotwanttomakewoodsculpturesbecausewoodishardandusingaknifeto
cutincanbedifficult.Someclientsmighthaveaphysicalprobleminmakingthese
typesofsculptures,suchasclientswitharthritichands.Becausesomeclientsmayfind
intensiveactivitiesdifficulttoaccomplish,arttherapistsmightbeabletoprovidemany
artactivities,directionandmaterialsthatengagelargermusclegroupsinanoutside
context.Clientsmaypreferartworkratherthanmeniallabor.
TheFourthStageofPreparationforDailyLiving
Thisstageoftreatmentfocusesonpreparingtheclienttogobacktotheir
naturallife.Clientsslowlystarttoadjusttotheworldoutsideoftherapy.Theyare
allowedtoreadsimplebooksandwalkoutsidealone.Duringsuchmoments,clientsare
encouragedtoexaminetheirfeelingsandthoughtsaboutthefuture.Clientsdelineate
whatkindsoffearsandobsessivethoughtstheyhadbeforesothatwhensuchfeelings
orthoughtsreemerge,theclientcanfindthemeanstoacceptthefeelingorthought.
Arttherapymaybeusefulforhelpingclientstofindthemselvesbecausedrawingand
visualizingareofteneasierwaystofindacceptance.Therearemanywaystouseartto
teachclientshowtoimprovetheirdailyliving.Forexample,artpicturescanbeusedto
assistclientsinpracticinghowtoconductbasicsocialgreetings.
ContemporaryOutpatientTreatmentStrategies
AccordingtoKitanishi(2008),thefollowinginterventions:canbedonewithclients:
1.Experiencehowtoacceptandholdwithemotions.
a.Distinguishbetweenwhatyoucandoandwhatyoucannotdo.
63
b.Trynottocontrolorsuppresstheemotions.
c.Holdandacceptyouremotions.
d. Waituntilhighemotionsbecomelessintense.
e. Observeyouremotions.Writedaily.
f. Recognizethedynamicnatureofemotions.
2.Reviewtheprinciplesofaction.
a.Realizethepurposeofyouraction.
b. Takeaction.
c. Focusontheactionandhaveasuccessfulexperienceofit.
d. Donotallowyourselftoneedtobeperfect.
e. Understandandfindoutabouthowyouractionchangedyouremotions.
f. Feelyourdesireforlife.
3.Reviewtheprinciplesofrelationships. a.Realizehowyoufeelotherpeople’sevaluations,opinions,andjudgmentsaboutyou.
b.Consideryouremotionsandbehaviorandhowthejudgmentofothersaffectsyou.
c. Findouthowyoutrytofitthem.
d. Findyourbehaviorandemotionafteryouchangetofitthem.
Haveyoueatentoomuch?Areyoudepressed?Haveyoudrunkexcessively?
e. Trytofocusonandrealizeyourpurposeofaction.
f. Changeyourbehaviorasaresultofsomeone’sjudgmentastoyourownpurpose.
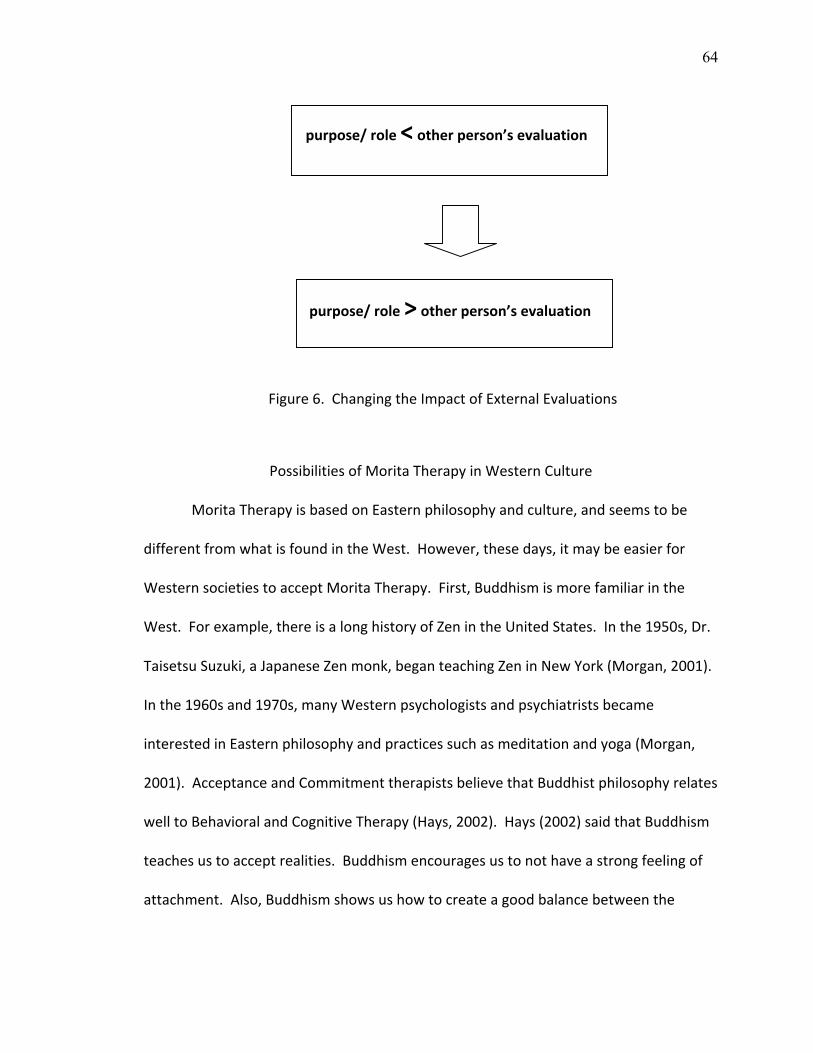
64
purpose/role<otherperson’sevaluation
purpose/role>otherperson’sevaluation
Figure6.ChangingtheImpactofExternalEvaluations
PossibilitiesofMoritaTherapyinWesternCulture
MoritaTherapyisbasedonEasternphilosophyandculture,andseemstobe
differentfromwhatisfoundintheWest.However,thesedays,itmaybeeasierfor
WesternsocietiestoacceptMoritaTherapy.First,Buddhismismorefamiliarinthe
West.Forexample,thereisalonghistoryofZenintheUnitedStates.Inthe1950s,Dr.
TaisetsuSuzuki,aJapaneseZenmonk,beganteachingZeninNewYork(Morgan,2001).
Inthe1960sand1970s,manyWesternpsychologistsandpsychiatristsbecame
interestedinEasternphilosophyandpracticessuchasmeditationandyoga(Morgan,
2001).AcceptanceandCommitmenttherapistsbelievethatBuddhistphilosophyrelates
welltoBehavioralandCognitiveTherapy(Hays,2002).Hays(2002)saidthatBuddhism
teachesustoacceptrealities.Buddhismencouragesustonothaveastrongfeelingof
attachment.Also,Buddhismshowsushowtocreateagoodbalancebetweenthe
65
insightsofnatureandmentalfunctioning(Teneatto,2002).Thelatterconceptis
relevanttoMoritaTherapy.
Westernsciencehasinvestigatedtheeffectivenessofmeditation.Meditation
practicehelpstopromotecalmness,awareness,open‐mindedness,andbeing
nonjudgmental(Anderson,2005).Itchangesthebrain.Meditationleadstothepower
ofhealingandtolookingatthenatureofthemind(Toneatto,2002).Meditationhas
longbeenassociatedwithBuddhism.TheBuddhistprincipleofnonjudgmental
awarenessisconsistentwiththeMoritaTherapyconceptof“Acceptance.”
Buddhismisnotscience.However,someofitspracticeshaveascientificbasis.
CombiningBuddhistpracticesandpsychotherapymaybevaluableformanypeople,
includingnon‐Buddhists(Hays,2002).ZenhasbecomeabridgebetweenEasternand
Westernpsychology(Kwee&Ellis,1998).MoritaTherapycouldbeaneffective
theoreticalorientationformanypopulations.
Itisimportantfortherapiststobeabletotreatpatientsusingatheoretical
foundation.ForJapanesetherapists,itmaybedifficulttounderstandWestern
psychologicaltheoriesbecausetheoriesareinfluencedbythecultures,values,and
philosophiesoftheplacesfromwhichtheyoriginate(Kitanishi,2007).Asiantherapists
maymoreeasilyunderstandEasternphilosophiessuchasZenandBuddhism.The
client’scultureimpactstheirfamilyfunctioningbecauseeachculturehasitsownstrong
heritage(Hoshino,2003).Peoplecannotignoretheirowncultureandheritage.Clear,
logical,andsystematicunderstandingofthetheoriesthatunderliethepracticesthatare
usedwithpatientsisanecessity.Understandingtheoriesisimportantinknowinghow
66
toapplyinterventionswithpatientsinastep‐by‐stepmanner.Inshort,therapists
shouldchoosetheoriesthattheyunderstandandcanusesuccessfully.Iftherapistsuse
theoriestheydonotunderstand,theycannothelppatients.
WesterntheoriesmakelesssensetopeoplewhoareraisedinBuddhistcultures.
However,MoritaTherapyisbasedonZenBuddhism.Asiantherapistsandclientsmight
finditeasiertounderstandit’sphilosophyandprinciples.However,MoritaTherapy
maybeusefulnotonlyforAsianclients,butalsoforsomeWesternclients.For
example,ifaWesterntheorydoesnotworkwellforaWesternclient,MoritaTherapy
mightworkwellbecausenewperspectivessometimesworkwell.MoritaTherapy
shouldbedevelopedtoapplytoallkindsofpopulations.Clientsdonotneedto
understandthephilosophicalunderpinningsofthetherapywithwhichtheyare
engaged,butclinicianshavetounderstanditclearly.
MoritaTherapyPastandPresent
Morita(2004)wroteaboutpsychopathologyofShinkeisitsusyoinhisbook,
ShinkeishitsunoHontaitoRyoho.Thisbookwaswrittentoexplainthecausesof
symptomsandhowtotreatclientswhohaveShinkeishitsusho.EventhoughMorita
formulateditin1919,thosetreatmentprinciplesarestillusedbytoday’sMorita
therapistsformanykindsofmentaldisorders.ThroughMorita’sbooksandarticles,itis
clearthatMoritaunderstoodBuddhismwellandwasinfluencedbyBuddhism.
Buddhismteachesphysicaltraining.MoritaTherapytaughtphysicaltrainingtoo.
Monksneveraskedquestionswhentheirmastersaskedthemtoworkduringtheir

67
training.MoritadidnotallowhisclientstoaskquestionsorarguewithMorita’s
treatmentorders.Thosemethodsstillexistintoday’sMoritaTherapy.
EventhoughMoritaformulatedMoritaTherapyin1917,over100yearsago,his
theoryandphilosophyareeasyforJapanesepeopletounderstandbecausetheyare
basedonBuddhism.MoritaTherapycanbeagoodfitforJapaneseandAsianclients
becausetheyareinfluencedbyBuddhism.Theseinfluencesarestrongandever‐present
intheirlivesandtheirphilosophytowardslife.Forexample,inJapaneseculture,itis
veryimportanttocleanone’shouseandgardeninthemorning.Childrenhavetoclean
theirschoolsafterschool,includingtherestrooms.Sixthgradestudentscleanthe
restroomsofthefirstgradestudents.ThispracticeisfromBuddhismwhichteaches
thatcleaningtheenvironmentmeanscleaningone’smind,thought,andlife.Buddhism
teachesthatpeoplefindwisdomthroughservice.ThatiswhyMoritaTherapyasks
clientstodowork.

68
IV:ANALYTICALPERSPECTIVEOFMORITATHERAPY
BackgroundConsiderationsRegardingMoritaTherapy
Today,manyJapanesepsychiatristsandpsychologistshavedevelopednew
applicationsofMoritaTherapy.TherearehistoricalreasonswhyMoritaTherapy
changedanddeveloped.ThetimelinebelowshowsthedevelopmentofMoritaTherapy
inthecontextofthehistoryofJapan,theworld,andmedication.Understandingthe
historicalcontextofdevelopmentofMoritaTherapyleadsustounderstandhowithas
evolvedandwhychangeswereneeded.Thehistorydemonstratesthatsocialsituations
suchascultural,economic,andphilosophicvariablesaffectmedicaltechnologyand
development.Forexample,afterbothWorldWars,theeconomicandsocialsituation
affectedpeople’snutritionandmentalconditions.Itisimportanttounderstandthis
historicalbackground.EspeciallyinregardstoMoritaTherapy,itisimportantto
understandhistoryandculturebecausebothaffectedwhichclientsweretreatedin
whatmanner.CultureisaparticularlyimportantcontexthereinthatMoritaTherapy
wasformulatedbyaJapanesepsychiatristinJapanandwasinfluencedbyBuddhismas
wellasJapaneseculture.Indeed,MoritaTherapy’sconceptofShinkeisitsu‐shodoesnot
existinDSM‐IVandcouldbeconsideredaculture‐boundsyndrome.Historically,itis
alsoimportanttounderstandaboutthedevelopmentofmedicationaswellsince
medicationhasgreatlyaffectedclients’conditions.
69
MoritaTherapyandMedication
Thereisabigdifferencebetweenthecurrentandthepastmedicalsituation
becauseofthemoderndevelopmentofpsychiatricmedication.Nakamura(2007)
statedthatinthelasttwentytothirtyyears,medicationforanxietyhasbecome
available.Hesaidthatinthepast,whentherewerenomedicationsforanxiety,
psychotherapywastheonlychoicefortreatment(2007).Today,medicationhas
becomeabigpartofthetreatmentregime.However,Nakamura(2007)pointedthat
evenwhenmedicationisprescribed,itdoesnotworkforabout50%ofclients.
Therefore,therapyisstillimportant.Inthefuture,thetheoryandpracticeofMorita
Therapyneedstotakeintoaccountmodernmedications.
AnalyticalIssuesoftheOriginalMoritaTherapy
ThischapteranalyzestheoriginalMoritaTherapy.Therearethreeissuestobe
considered:1)theenvironmentofMoritaTherapy,2)therelationshipbetweenclients
andclinicians,and3)thedifficultyofunderstandingMoritaTherapy.Itisimportantto
analyzetheseissuesfromamanydimensionalperspectivethatincludesthehistoryof
MoritaTherapyandJapan,medications,andJapaneseculturalperspectivesinregards
tothefuturedevelopmentofMoritaTherapy.
EnvironmentofMoritaTherapy
In1917whenMoritaformulatedMoritaTherapy,itwasjustafterWorldWarI,
theRussianCivilWar,andJapanwaspreparingtoenterWorldWarII.Japanwasinan
economicdepression.Inthatsituation,MoritaformulatedMoritaTherapyafterhisown
experienceofovercomingShinkeishitsu‐shoathishome(Kondo,1966.,Suzuki,1967.,&
70
Kitanish,1989).Moritatriedtoprovidethefamilyatmosphereforhispatientsbyusing
hishomebecausehebelievedthatenvironmentwasimportantfortreatment.
Atthattime,theJapanesefamilystylewasthepatriarchalsystem.Theheadofa
familywasaman‐‐afatherorgrandfather‐‐whohadabsolutepoweroverfamily
members.Inthisculturalsituation,MoritaTherapywasfoundedbyMorita.Hewasa
psychiatristplayingafather‐likeroleattheinpatientunitestablishedinhishome.His
wifebecameaveryimportanttreatmentmember,playingoutfortheclientstheroleof
theirmother.ThemotherrolewasimportantforMoritaTherapy(Uchimura,1970).
Moritaandhiswifehadaheavyworkload.Thereweremanyresponsibilitiesinvolved
withprovidingtreatmentattheirownhouse(Ohara,1970).Itwasahardshipforthem
tousetheirownhouseforthepatients.Therewaslittleornoprivatetime.Morita
sometimesworked24hourshifts,sevenweeksatatimeforseveralmonths.Whatwas
hismotivationtoworksohard?Perhapshefeltagreatdealofresponsibilitytothenew
programofMoritaTherapy.Perhapshisstatusasapsychiatristledhimtoworkhard
andtomakemanypersonalsacrifices.Itispossiblethatherecruitedhiswifetobecome
atreatmentproviderbecauseheneededthehelpwiththeextensiveclinicaland
administrativeworkload.Itwouldhavebeenanaturalmatterforhiswifetoobeyhis
requesttofollowhimintotreatment.TheJapanesesocialnormwasthathewasin
chargeofhisfamilyaswellasthepatients.Havingabsolutepoweroverfamily
memberswasnormalatthattimeinJapan.AfterMoritadied,AizawaandMaruyama
inheritedthisstyleofprovidinginpatienttreatmentwithinafamilyatmosphere
(Kitanishi,1989).Butinlateryears,MoritaTherapybecamesimpler,includingproviding
71
inpatientandoutpatienttreatmentinhospitalssettings(Kitanishi,1989).Asnotedby
Kitanishi(1987),itisnecessaryforMoritatherapiststohavelimitsplacedinregardsto
theirworkloadandtime.
IssuesRegardingtheInpatientUnitatMorita’sHome
QuestionsaboutplacingtheinpatientunitatMorita’shomeincludeethical
considerations,effectivenessofthetreatment,andboundarybetweenclientsand
clinicians.
EthicalConsiderations
OneofthestatedreasonsMoritaopenedaninpatientunitinhisownhomewas
thathebelievedthatprovidingafamilyatmospherewasimportantforthetreatment.
MoritahadhiswifejointheMoritaTherapyprogramastreatmentmembereventhough
shedidnothaveanymedicaltraining.Atalatertime,Aizawa,aphysicianwhowasalso
aMoritatherapistsimilarlywouldappointawomanwhodidnothaveanymedical
trainingasmanagerofaninpatientunitpracticingMoritaTherapyatJikeiHospital.Her
positionwasasmanagerandherrolewaslikeamotherforthepatients(Kitanishi,
1989).
Usingcontemporarystandardsofpractice,wewouldconsidertheseappointments
unethical.AlthoughMorita’swifeandtheunitmanagerdidnothaveanymedical
training,theyworkedastreatmentproviders.Eveniftheclientshaddetailedschedules
duringtheday,whileMoritaworkedwithoutpatientsinahospital,hiswifewouldhave
hadmanyclinicalresponsibilities.Evenifshehadclinicalsupervision,shewouldhave
workedwithclientsalldayandnightintheabsenceofprofessionalstaff.Itisnot

72
ethicalforpeoplewithnoclinicaltrainingtoprovidetreatment.Hiswifeneededtobe
trainedhowtocommunicatewithclients,forexample,sincecommunicationwith
clientswhohaveamentalillnessisadelicatematterandaveryimportantpartof
treatment.InMorita’sbooks,therearenodescriptionsabouttrainingforhiswife.We
willneverknowhowmuchhereffort,behavior,andconversationaffectedtheclients.It
wasMorita’sresponsibilitytowriteabouthertrainingandeducationalbackgroundand
impactontreatment.Didhethinkthathispatientsneededamotherfigure?Didhe
supervisehiswife?Didhegivedirectionaboutdietorothermatterstohiswife?
EffectivenessofTreatment
Clinicianshavearesponsibilitytotakecareofthemselvesphysicallyandmentally
aspartofprovidingeffectivetreatmenttoclients.Moritaprovided24hourandseven
dayaweektreatmentathishome.Suchaworkloadcallstheeffectivenessofthe
treatmentseriouslyintoquestionbecausethecliniciansdidnothavetimetotakecare
ofthemselves.InJapanese,thisprofessionalworkstyleiscalledShyuchiryou‐sei(主治
療制);adoctortakescareofallclientsoftheunitwhereheworks.Moritatookcareof
allhisclientsbyhimself.Suchanexcessiveworkloadcouldeasilyleadtosubjectiveand
narrowtreatment.
BoundaryBetweenClientsandClinicians
Cliniciansmustputboundariesbetweenthemselvesandtheirclients.Using
one’shouseasaninpatienthospitalmakestherelationshipbetweenclientandclinician
ambiguousatbest.Withnoseparationbetweentheclinician’sprivateandpubliclife,
therewasboundtobeconfusionandethicallyquestionabledecisions.EvenifMorita
73
intentionallywantedtheunittorecreateafamilyenvironment,itwasstillahospitalfor
clients.Theplacemightfeellikeasafetreatmentunitforclientsbecausethe
atmospherewaslikeahome.However,theplacemightnotbesafeforclinicians.The
stafftherehadnochoicebuttosharetheirpersonalliveswiththeclients.Becausethe
clinicianswereavailable24hoursadayandsevendaysaweek,clientscouldeasily
developpsychologicalandphysicaldependenciestowardthetreatmentstaff.Wasthis
usefulfortheclients’recovery?Theyhadtobeindependentaftertheywere
discharged.
OneargumentisthatitmighthavebeeneffectiveforMoritaTherapytohavea
fatherfiguretocontroltheclientsbecausethecontrolmadetheclientsworryless
(Kondo,1966;Ohara,1970;Doi,1963).Forexample,ifpeopledonotworryabout
money,theirschedule,orobtainingfoodonadailybasis,peoplearerelievedof
importantsourcesofanxiety.However,usingMorita’sownhomemightnothavebeen
thebestwaytoprovideafatherfigure.Asurrogatefatherfigurewasoftenprovidedat
out‐patientunitsinlocalhospitals.Morita’sfollowers,includingmedicaldoctorsatthe
JikeiMedicalSchool,havecontinuedMoritaTherapywithsomechanges.
RelationshipsbetweenClientsandClinicians:FumonnoKankei(DoNotQuestion,Just
Obey)
TherelationshipbetweenclientsandcliniciansinMoritaTherapyhashadmany
issues that should be examined including power issues, ambiguity, and the unclear
meaningofgrouptreatment.
PowerIssues
74
MoritaTherapyhashadastricthierarchicalorderthatisestablishedbetween
clientsandclinicians.WhenMoritaprovidedtherapy,hewieldedabsolutepowerover
hispatients,likeanold‐styleJapanesefather.Hispatientsdidnothaverighttoexpress
theiropinionsorquestionhisdecisions.ThisiscalledFumon(不問).Moritabelieved
thatsuchanenvironmentdecreasedanxietyinhispatients(Aizawa,1967;Kondo,1966;
Ohara,1970;Doi,1963).“Justobey!Don’taskanything”wasanold‐styleJapanese
familysystemphilosophy.Itwasverymale‐centered.Thefatherhadallthefamily
power.MoritaTherapystrivedtocontrolthepatients’dailyliving.Itwaseasierfor
clinicianstocontrolthepatientswhentheclinicianswerewiththem24hours(Kitanishi,
1989).MoritaTherapytaughtthatyoudonotlookatthepastorthinkaboutthe
unconsciouscausesofproblems.Youjustacceptyoureveryemotion.However,Fumon
(justobeyanddonotquestion)mightnotbeaneffectivewaytodevelopone’scognitive
andpsychologicalgrowth.AsTatematsu(1986)stated,theclient’sownissueswerean
importantpartoftheprocessinvolvedingrowingpsychologicallyandspiritually.Each
developmentalstagecanproducepsychologicalpainorevencrisisattimes.Itis
importantforpatientstolearntoresolvetheseperiodicproblems.Thoseprocesses
shouldbeapartoftreatment.
Thequestionswemustaskourselvesarewhethercontrollingtheclients’thoughts
andbehaviorsisaneffectivetreatmentandwhetheritisethicaltoprovidetreatment
withouttheclient’sparticipationinthetreatmentplan.Therearealreadyexisting
powerissuesbetweenclientsandclinicians.Ifaclinicianusedtheirownhouseasan
75
inpatientunit,theirpowerisenhanced.Itmightbedifficultforclientstosay“No!”toa
treatmentproviderwhoalsoownsandcontrolstheveryresidencewheretheylive.
Morita’streatmentcouldhavepossiblybeenmoreeffectiveifheactively
supportedhiswifeinassumingaroleaskindandwarmmother.Thewife’srolecould
softenthepowerdynamicsbetweenMoritaandhispatients.Moritaplayedoutarole
asaverystrictandstrongleaderandclinician.Ifhiswifewasallowedtobeakindand
warmmother‐likefigurethatencouragedthepatients’feelings,thismighthaveadded
someneededbalance.Forexample,whenMoritawasangrywithhispatient’sbehavior,
perhapshiswifegaveencouragementandunderstandingthathelpedemotionally
supporttheclients.Moritadidnotwriteabouttheseissuessoatthispointweprimarily
havequestions,notanswers.
UnclearRoleRelationships
Moritawasastrictandstrongleaderwhofunctionedlikeafatherfigureforthe
clientsattheunit.Theirrelationshiplookedlikefatherandachildormasteranddisciple
(Ohara,1970).MoritaTherapywasconsideredthemosteffectiveiftherelationship
betweenclinicianandclientduringinpatienttreatmentwaslikeamasterandadisciple
(Uchimura,1970,Niifuku,1980,andFujita,1977).MoritaTherapyispsycho‐educational
innature.Thereareconcretestepsforestablishingtheclient’sdailylife.Itmusthave
beendifficulttokeeptheclinicalrelationshipinthesamecondition.Forexample,one
dayclientsareabletoobeytheirclinician’sadvice,butanotherdaytheymightbe
unabletoobeytheirclinicianbecauseoftheirpsychologicalorphysicalconditions.The
relationshipbetweenclientandclinicianwasnotstable.Ifthetreatmentdependedon
76
therelationship,it’seffectivenessalsodependedontherelationship.Therelationship
wasnotstablesoitseffectivenessfortheclientswasprobablynotconsistent.In
addition,iftheclientdependedontherelationshiptoomuch,itmighthavebeen
difficultforthemtobeindependentwhendischarged.
AcontemporaryissueforMoritaTherapyisthislackofclarityregardingtheclinical
relationshipbasedontheoldrolesoffatherandchildormasteranddisciple.Afather
role,motherrole,familyenvironment,ormasteranddiscipleareverydifferent
constructsindifferentculturesandcountries.Theimplicitrulesgoverningtheseroles
changedependingontheindividual’shistory,andacrosstime.Usingthoseambiguous
wordsandculture‐boundrolesmakesitdifficulttounderstandMoritaTherapyfornot
onlyJapanesepeople,butalsopeoplewhowanttostudyitaroundtheworld.
UnclearMeaningofGroupTreatment
MoritaprovidedMoritaTherapythroughaninpatientsetting.Thepatients
spenttheirdaywithotherpatientsexceptwhentheywererequiredtobealone.
Essentially,theywereinvolvedwithakindofgrouptherapyinthetherapeuticmilieu.
Moritadidnotwriteabouthowtotakecareofthegroupdynamicorinteractionamong
thepatients.Weknowthatthistypeofgrouptherapyaffectedtreatmentpositively
(Kitanishi,1987)butweknowverylittleaboutit.
DifficultyUnderstandingMoritaTherapy
ItisimportantforclinicianswhouseMoritaTherapytobeabletounderstandit
clearlyasaclinicaltreatment.Ifpeopleareunabletounderstandit,itisdifficulttouse,
evaluate,anddevelop.Moritatherapistshaveamissiontoprovideeffectivetreatment
77
aswellastosupportandtoteachMoritaTherapytoyoungerclinicians.Today,Morita
Therapyisdevelopingaroundtheworld,especiallyinChina.ItisimportantforMorita
Therapytodemonstratescientificevidenceforitseffectiveness.Someissuesof
importantfortheuseofMoritaTherapyareits’scientificbasis,dimensionalclinical
support,andclinicaltrainingneeds.
ScientificBasis
In1938theJapaneseSocietyofPsychiatryandNeurologyconductedresearch
thatstatisticallyvalidatedtheeffectivenessofMoritaTherapy.Theresearchproject
studiedhoweffectiveMoritaTherapywasfor541nervousnessclientsfrom1929to
1937.Theresultsshowedthat58%ofthemexperiencedcompleterecoveryand36%of
themexperiencedsomerecoveryinapositivedirection.Inshort,94%ofthemshowed
improvements(Ichikawa,2008).Afterthatpivotalstudy,KitanishandotherMorita
therapistshavecontinuedtoresearchtheeffectivenessofthisformoftreatment
(Kitanishi,1989).KitanishthinksthatMoritaTherapyisdifficulttounderstand.
Consequently,KitanishihastriedtobetterdescribeMoritaTherapybydevelopingand
usingnewvocabulary.
Today,however,itisdifficulttofindmanyscholarlyresearchpapersabout
MoritaTherapyinprofessionalresearchdatabasessuchasCINI(Cochranlibrary),
PsycINFO,andPubMed.Sincetherearefewscholarlyresearchpapersdevotedto
MoritaTherapy,ithasbeendifficulttosaywhetherornotMoritaTherapyenjoysa
scientificbasis.IfMoritaTherapyisgoingtodevelopintheworld,itwillneedtobe
morewidepublishedandevidenceeffectivenesstoscientistsaroundtheworld.
78
Conductingresearchthatiscross‐culturallyvalidmayposesomeinteresting
challenges.Forexample,MoritastatedthatthetreatmentenvironmentforMorita
Therapyhadtobelikeafamilyhome(Hashimoto,1985).However,thisraisesbig
questionaboutwhatthatmeans.Peoplecanhaveverydifferentdefinitionsoffamily.
Familymeanssomethingquitevaried,dependingonculture,individualhistory,andtime
period.Morita’swordsmakeitdifficultforpeopleinotherpartsoftheworldto
understandMoritaTherapy.Thislackofunderstandablelanguagehasaffectedits
development.
Hashimoto(1985)acknowledgedthattheatmosphereofaninpatientunitwas
animportantfactorfortreatment.Hisopinionwasbasedonhisexperiencewhenhe
andhiscolleaguescreatedaninpatientunitattheJikeiMedicalSchoolHospitalafter
Moritadied.Iftheatmosphereaffectstreatmenteffectivenesssodramatically,it
shouldbearesearchprioritytodeterminewhatelementsofatmosphereareneededfor
theeffectiveuseofMoritaTherapy.
DimensionalClinicalSupports
Today,mentalhealthprofessionalsincludemanykindsofclinicians.Notonly
psychiatrists,butalsopsychologists,psychotherapists,socialworkers,occupational
therapists,dieticians,nursesandthelikeareapartoftreatmentservicestopatients.
Theyoftenprovidetreatmentasateamforaclient.Moritadidnottalkabout
medicationsanddietinhiswritings.Thesedays,manymentalhealthclientsare
prescribedmedicationbutthisprobablywasnotthecaseinMorita’stime.Ifclients

79
takemedication,clinicianshavetomonitortheeffectivenessofmedications.Thereis
noevidencewhetherornotMoritaprescribedmedicationtohisclients.
AfterWorldWarII,psychiatricdisorderswereontherisearoundintheworld
whenthefirstpsychotropicmedicationsweredeveloped(Kazamaturi,1980).There
were520,000patientsinstatepublichospitalsin1955intheUnitedStatesofAmerica.
Thatnumberaccountedfor50%ofallinpatientadmissionsintheUnitedStates.Inthe
sameyearinFrance,patientswhoneededpsychiatrictreatmentatthepublichospitals
numberedabout100,000.Thatwas30%ofinpatientsadmissionsinthatcountry.
However,afterchlorpromazinewasdiscovered,thenumbersofpatientsdecreased
significantlyincountriesthathadthemedicationresourcesforpatients.IntheUnited
StatesofAmericain1975,inpatientadmissionstopsychiatrichospitalsdecreasedto
200,000people(30%).Thisdramaticchangecanbeattributednotonlytodevelopinga
nationalsupportsystemforpsychiatricpatients,butalsoimportantly,accesstonew
effectivepsychotropicmedications(Kazamaturi,1980).
Moritaandhisfollowersdidnotwriteaboutmedication.Sincethe1960s,well
afterMorita’sdeath,Benzodiazepinecompoundmedicationshavebeenavailableand
beenprescribedforanxietyinJapan(Ichikawa,2008;Kazamatsuri,1980).However,
therehasbeenlittlewrittenabouttheuseofthesemedicationsinconjunctionwith
MoritaTherapy.Ichikawa(2008)statedthatMoritaTherapywasnotpharmacotherapy.
IfMoritaTherapyremainsprimarilyapsychologicaltheoreticalorientation,medication
mighttakeanancillaryrole.Thisremainstobeseen.
80
Today,nutritionaleducationisanimportantpartofMoritaTherapytreatment.
InJapaneseculture,especiallyinZenBuddhism,itisimportanttoeatwithgoodtable
manners.Moritaandhiswifemighthaveemphasizedgoodmannerswiththeirclients.
Surely,Moritacaredaboutmannerssincehisbasicphilosophywassointricatelytiedto
ZenBuddhismwhereeatingmannersisoneofthemostimportantelementsingood
living.
Furthermore,ZenBuddhismvaluesSamu(work).Working(Samu)isonepartof
treatmentsmodalitiesinMoritaTherapy.Thetreatmentstartswithlightworkand
increasesgraduallytoheavierworkassignments.Heavyworkwasusedtopreparethe
clientfordischarge.Theworkincludedthedetailedandcomplexworkofdailylife.The
workprogramsboreacloseresemblancetothedailyneedsoftheclient(Hashimoto,
1985).
Moritawroteaboutsomeartactivitiessuchasmakingwoodsculptures.Did
thepatientsenjoymakingsculptures?Itisimportantthatpatientsknowhowtohave
enjoymentintheirdailylifeaswellashavingenjoymentinthetreatmentprogram.
Moritadidnotwritedescriptionsaboutartmaterials,thereasonsformakingartorthe
processofcreatingart.ItishardtoknowhowMoritapreparedandfacilitatedwhat
clientsexpressedthroughtheirart.
WhatisclearisthatMorita’sfollowersplacedahighvalueonknowinghowto
talkandinteractwithpatientsduringtheprogram.Forexample,Kitanishi(1987)stated
thatitisimportantforclinicianstohavegoodcommunicationwithpatientswhilebeing
apartoftheworkingprogram.Hesuggestedthatifcliniciansgivetasksthatweretoo
81
easytopatients,clinicianswouldnothaveachancetotalkwithandteachpatients
aboutthetasks.Hepointedoutthatcommunicationandinteractionwereimportant
elementsofeffectivetreatment(Kitanishi,1987).WhatdidMoritathinkabout
communicationwithhispatients?Kitanishistatedlesscommunicationwasless
effectivesuggestingthatcommunicationisimportantforMoritaTherapy.Clinicians
whowanttouseMoritaTherapyshouldknowhowtocommunicatewithpatientsand
thereasonswhycommunicationisimportant.Ifclientscannotexpresstheirthoughts
andafeelingverbally,doescommunicationthroughartprovidetheneededexpression?
WehavenoinformationabouthowMoritamightanswerthisquestion.
AnadditionalgapofinformationisthatwedonotknowhowMoritatookcare
ofhispatients’artwork.Takingcareofclientartisaveryimportantpartoftreatment
becausetheartworkitselfisprivateandneedstobeprotected.Hashimoto(1985)
statedthatbecauseMoritausedhishomeasaninpatientunit,peopledidnothave
chancetoknowthedetailsofMoritaTherapymethods.Itisveryimportantforthe
futuredevelopmentofMoritaTherapythatthescientificcommunityhaveaccessto
moreinformationaboutkeymethodologicalissues.Theseissuesincludetheroleofthe
therapist,theimportanceofcommunicationskills,andtheroleofexpressiveactivities
suchasart.ThatinformationwillhelpMoritaTherapytobemoreeffectiveasastrong
psychologicaltreatment.
82
ClinicalTraining
ThecompetentMoritatherapistdoesnotneedtobeanex‐patient.Moritahad
sufferednervousness.Afterheovercamehisillness,hecreatedMoritaTherapy,
drawinguponhisownexperience.Indeed,thereareadvantagesfortreatmentifa
clinicianhasundergonethesamekindsofexperiencesastheclient.Theclinicianoften
understandstheclient’ssufferingwellandcangiverealisticadviceduringthetreatment
(Ohara,Aizawa&Iwai,1970).However,Kitanishi(1987)specificallystatedthat
cliniciansneednotbeex‐patients.Thatisareasonablestatement.Cliniciansare
expectedtoprovidecompetenttreatmenteveniftheyhavenotexperiencedthesame
thingsastheclient.Moreover,cliniciansneedtohaveanobjectiveperspectiveabout
thetreatmentandtheclients.Itmightbefineforclinicianstohavesomesubjective
perspectives,butoverall,theyneedtobeabletodetachfromthecoreissuesand
maintainobjectivityaboutthem.Ifcliniciansdonothaveanobjectiveperspective,they
arevulnerabletocommittingethicaltransgressionsandpossiblyevenharmingthe
clients.
Shuchiryou‐sei,theclosedtreatmentmethodofMoritaTherapy,continuedfor
quiteafewgenerations.Mariyamaceasedthispracticeby1976(Kitanishi,1989).
Moritahadtaughtthatitwasimportantforpatients’reintegrationintosocietythatone
clinicianhadallresponsibilitiesforthetreatment(Kazamaturi,1980).Thatwasone
reasonthatMoritaopenedhishomeasaninpatientunit.
83
AfterMorita
In1974,longafterMorita’sdeath,JikeiMedicalSchoolhospitalinTokyo,Japan
whereMoritahadbeenaprofessor,builtaninpatientunitforMoritaTherapy(Kitanishi,
1984).AtthattimeAizawa,thedirectoroftheunit,hiredtwoassistantdoctors,a
femalemanagerasamanagerwhoplayedtheroleofmothertotheclients;anda
femaleretirednurseasageneralmanagerfortheunit.Indoingso,hechanged
Morita’soriginalideaofonlyonedoctorhavingalltheresponsibilitiesforthecareofthe
patients.Aizawarecruitednewtreatmentmembersaswell.Theystillcontinuedto
providetreatmentbyadoctor,Shuchiryou‐seistyle.Themanager,whotookontherole
ofmothertotheclients,haddifficultiesbecauseshehadheavyresponsibilitiesbutwas
nottrainedasaprofessionalclinician.Shelaterresigned.Aizawahimselfexperienced
physicalandpsychologicaldifficultiesbecausehehadinsufficienttime.Hesawpatients
onanoutpatientbasisduringthedayinadditiontotreatingpatientsalldayinthe
hospital.However,hestayedonandlivedinthehospitalwiththepatients.
MaruyamatookovertheleadershipoftheMoritaTherapyunitatJikeiMedical
Schoolin1974.Hecontinuedthesamestyle,Shuchiryou‐sei.Moreover,Maruyama
reducedtheresponsibilitiesoftheassistantdoctorsandreintroducedthetreatment
stylethathadbeenusedbyMorita,eventhoughtheunitwasinamedicalschool
hospital(Kitanishi,1984).Twoyearslater,however,Maruyamareconsideredthe
treatmentstyle.HechangeditfromShuchiryou‐seistyletoShyujii‐sei.Shyjii‐seimeans
thateachdoctorhadresponsibilitiesforthetreatmentoftheirownclientsontheunit.
Itwasnolongerthecasethatonlyonedoctorhadtheresponsibilitytocareforallthe

84
clientsontheunit.MaruyamatriedtoreconstructMoritaTherapyasasimplesystem
butusinganupdatedworkingstyle.Cliniciansdidnotlivewiththepatientsatthe
hospitalandwerenotrequiredtospendalotoftime,eventheirprivatetime,withthe
patients.Maruyamafoundawomantotakeonthemotherroleandlivewiththe
patients.InJapaneseculture,womentendtotakeonamotherroleinmanysituations.
Theclinicianswhoworkedatthehospitalbegantohavegroupsupervision.Thisnew
styleofMoritaTherapyopenedthedoortoallowmorefollowersofMoritaTherapy
becauseitbecamemoreclearwhattheclinicianwastodo.
MoritaTherapyToday
Today,theMoritaTherapyunitatJikeiMedicalHospitalinJapanprovides
treatmentforindividualsboththroughinpatientandoutpatientprograms.Some
Moritatherapistsdevelopedtheoutpatientprogramasaresultofthefactthatitis
difficultforclientstocommittolong‐termhospitalizationinmoderntimes.
Additionally,itisdifficultforclinicianstocommittoaheavyworkload.MoritaTherapy
hasbeenusedfordepression,OppositionalDefiantDisorder,anxiety,andpanic
disorders.ThereasonwhyMoritaTherapycontinuestodevelopisthatmanyMorita
therapistshavereassessedthecontentsandmethodsofMoritaTherapyandhave
addressedpastproblems.
Conclusion
MoritaTherapyneedstobeclearaboutitsphilosophyandbeabletodescribeit
clearly.SometimeswhenMoritaTherapyisdescribed,itsadmirersuseZenwordsthat
aredifficultandconfusingtopeoplewhoarenotfamiliarwithJapaneseculture.This

85
maybepreventingsomefromlearningaboutMoritaTherapy.Zenwordsand
philosophyarenoteasytounderstand.EvenZenmonksneedalongperiodoftraining
beforetheycanunderstandsomeZenconcepts.Additionallytherearepeoplewhoare
notinterestedinZenbecausetheyarecommittedtoadifferentreligion.Theymight
feelresistancetolearningaboutMoritaTherapyifitisdescribedentirelythroughZen
language.TheymightnotwanttheircliniciantouseMoritaTherapyfortheirtreatment
ifitisassociatedintheirmindwithBuddhism.
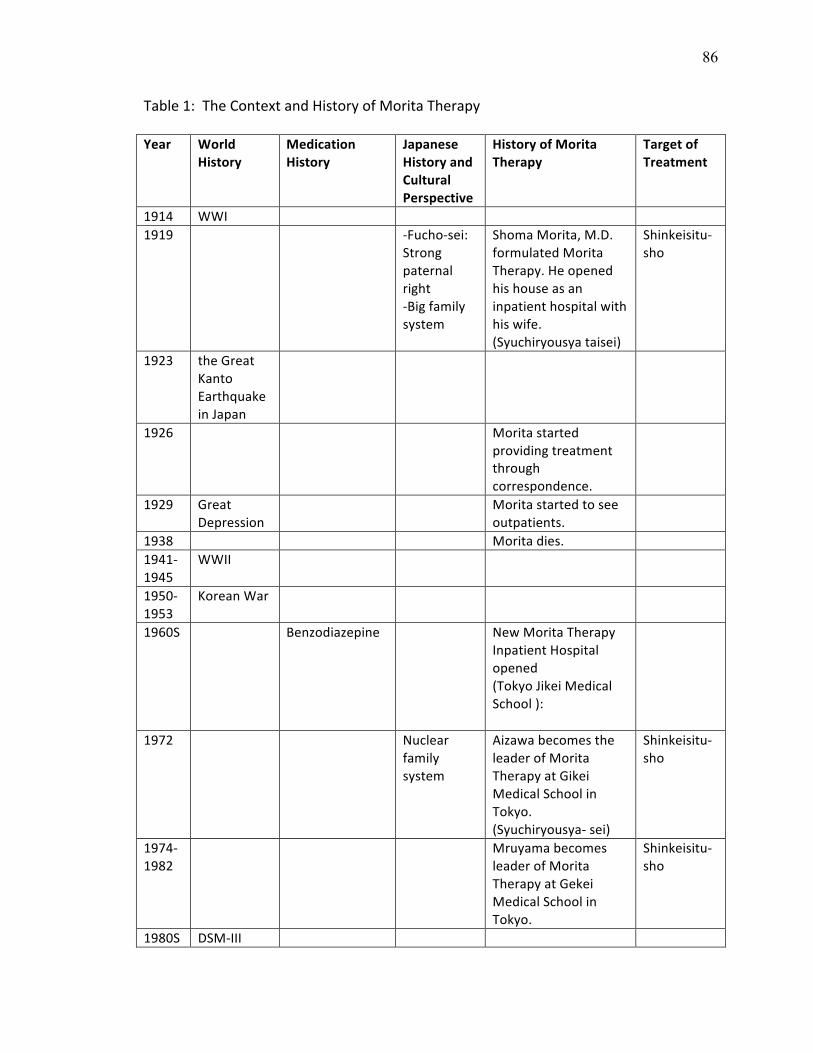
86
Table1:TheContextandHistoryofMoritaTherapy
Year WorldHistory
Medication History
JapaneseHistoryandCulturalPerspective
HistoryofMoritaTherapy
TargetofTreatment
1914 WWI 1919 ‐Fucho‐sei:
Strongpaternalright‐Bigfamilysystem
ShomaMorita,M.D.formulatedMoritaTherapy.Heopenedhishouseasaninpatienthospitalwithhiswife.(Syuchiryousyataisei)
Shinkeisitu‐sho
1923 theGreatKantoEarthquakeinJapan
1926 Moritastartedprovidingtreatmentthroughcorrespondence.
1929 GreatDepression
Moritastartedtoseeoutpatients.
1938 Moritadies. 1941‐1945
WWII
1950‐1953
KoreanWar
1960S Benzodiazepine NewMoritaTherapyInpatientHospitalopened(TokyoJikeiMedicalSchool):
1972 Nuclearfamilysystem
AizawabecomestheleaderofMoritaTherapyatGikeiMedicalSchoolinTokyo.(Syuchiryousya‐sei)
Shinkeisitu‐sho
1974‐1982
MruyamabecomesleaderofMoritaTherapyatGekeiMedicalSchoolinTokyo.
Shinkeisitu‐sho
1980S DSM‐III
87
V:THEINTEGRATIONOFMORITATHERAPYWITHARTTHERAPY
AlthoughArttherapytechniqueshavebeenusedinconjunctionwithmany
Westernpsychologicaltheories,noscholarlyarticlesorbookshavebeenwrittenabout
usingAmericanarttherapytechniqueswithMoritaTherapy.However,Moritahimself
usedartduringthetreatmentheprovided.Heusedartasanassessmenttooland
duringtreatmentinvolvinghislightworkstage.Forexample,heencouragedclientsto
writealetterordiarywiththeirtherapiststoexpresstheiremotionsandfeelings
(France,Cadieax&Allen,1995)becausethroughthisprocess,clientscouldlearnto
understandandobservetheirownthoughts.Ofcourse,thecliniciansalsobenefited
fromthewritingsinceitassistedtheminunderstandingtheclient’sthoughts,and
becomingfamiliarwiththeclient’scognitivestyle(Kubota,2008).Moritaalsolethis
patientsmakewoodsculpturesduringthelightworkphaseoftreatment(Morita,2004).
VarioushistoricaldocumentshaveverifiedthatthatinMoritaTherapy,arthasbeen
usedasatreatmenttoolandasamethodofassessmentduringthetherapyprocess.
However,therearenoreportsthatMoritaorhisfollowersrecognizedthatartandthe
processesinvolvedincreatingitaffectsclientsinpsychologicallyprofoundways.Art
therapyisatechniqueusedintherapythatleadsclientsdeeperintothemselvesand
givesthemtheopportunitytounderstandandfindoutaboutthemselveswiththe
supportofarttherapists.Forexample,thearttherapyprocessilluminatestheinner
dialoguesresultingfromtheclient’sinternalconflictsandaffectivestates.Thatcanbe
particularlyusefulforMoritaTherapyclientsbecauseafocusofthistreatmentison
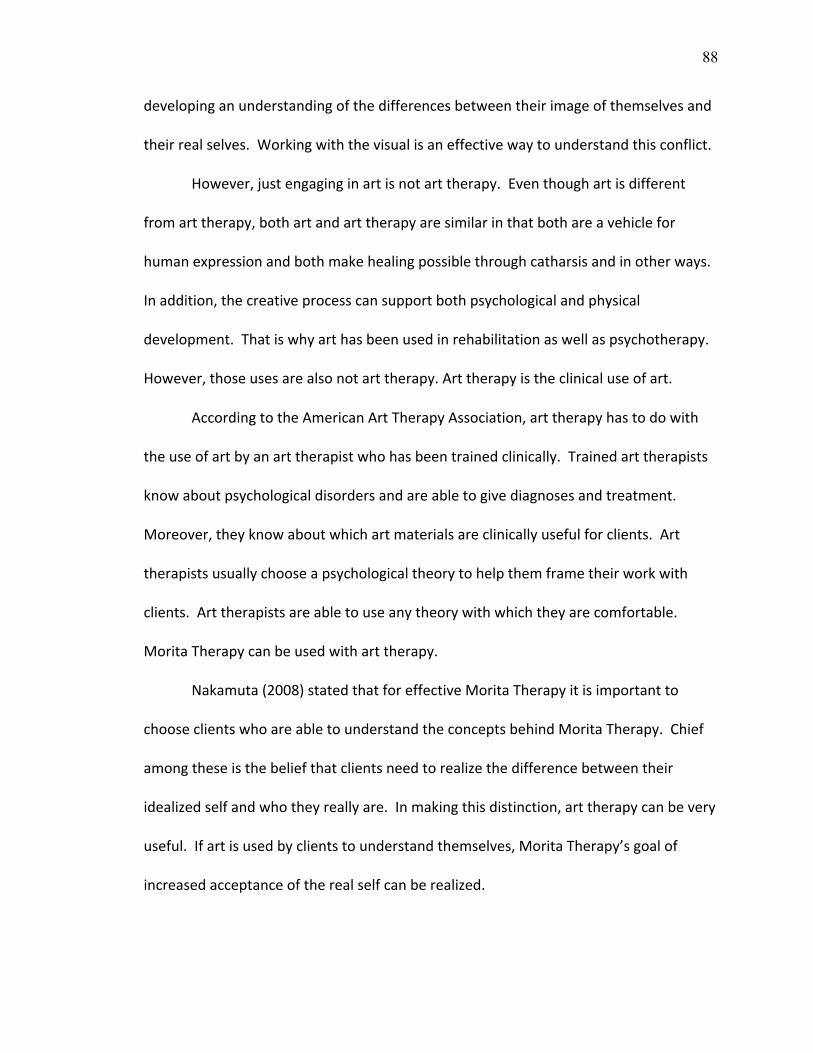
88
developinganunderstandingofthedifferencesbetweentheirimageofthemselvesand
theirrealselves.Workingwiththevisualisaneffectivewaytounderstandthisconflict.
However,justengaginginartisnotarttherapy.Eventhoughartisdifferent
fromarttherapy,bothartandarttherapyaresimilarinthatbothareavehiclefor
humanexpressionandbothmakehealingpossiblethroughcatharsisandinotherways.
Inaddition,thecreativeprocesscansupportbothpsychologicalandphysical
development.Thatiswhyarthasbeenusedinrehabilitationaswellaspsychotherapy.
However,thoseusesarealsonotarttherapy.Arttherapyistheclinicaluseofart.
AccordingtotheAmericanArtTherapyAssociation,arttherapyhastodowith
theuseofartbyanarttherapistwhohasbeentrainedclinically.Trainedarttherapists
knowaboutpsychologicaldisordersandareabletogivediagnosesandtreatment.
Moreover,theyknowaboutwhichartmaterialsareclinicallyusefulforclients.Art
therapistsusuallychooseapsychologicaltheorytohelpthemframetheirworkwith
clients.Arttherapistsareabletouseanytheorywithwhichtheyarecomfortable.
MoritaTherapycanbeusedwitharttherapy.
Nakamuta(2008)statedthatforeffectiveMoritaTherapyitisimportantto
chooseclientswhoareabletounderstandtheconceptsbehindMoritaTherapy.Chief
amongtheseisthebeliefthatclientsneedtorealizethedifferencebetweentheir
idealizedselfandwhotheyreallyare.Inmakingthisdistinction,arttherapycanbevery
useful.Ifartisusedbyclientstounderstandthemselves,MoritaTherapy’sgoalof
increasedacceptanceoftherealselfcanberealized.
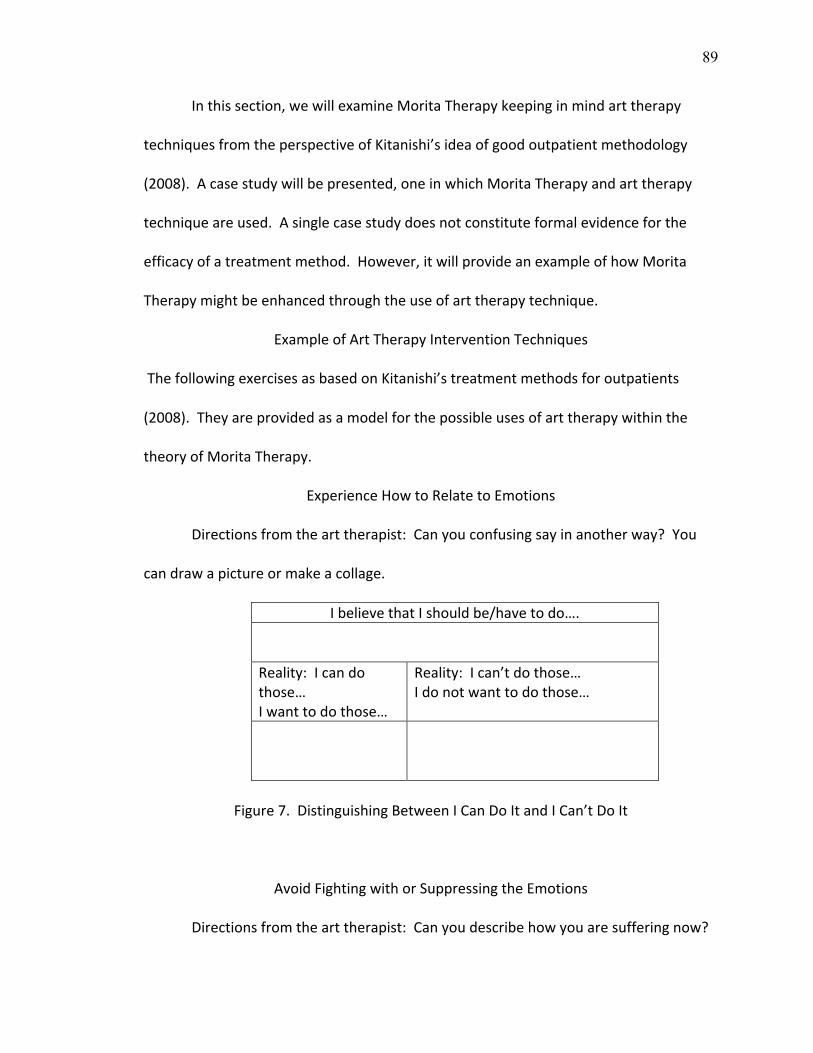
89
Inthissection,wewillexamineMoritaTherapykeepinginmindarttherapy
techniquesfromtheperspectiveofKitanishi’sideaofgoodoutpatientmethodology
(2008).Acasestudywillbepresented,oneinwhichMoritaTherapyandarttherapy
techniqueareused.Asinglecasestudydoesnotconstituteformalevidenceforthe
efficacyofatreatmentmethod.However,itwillprovideanexampleofhowMorita
Therapymightbeenhancedthroughtheuseofarttherapytechnique.
ExampleofArtTherapyInterventionTechniques
ThefollowingexercisesasbasedonKitanishi’streatmentmethodsforoutpatients
(2008).Theyareprovidedasamodelforthepossibleusesofarttherapywithinthe
theoryofMoritaTherapy.
ExperienceHowtoRelatetoEmotions
Directionsfromthearttherapist:Canyouconfusingsayinanotherway?You
candrawapictureormakeacollage.
IbelievethatIshouldbe/havetodo….Reality:Icandothose…Iwanttodothose…
Reality:Ican’tdothose…Idonotwanttodothose…
Figure7.DistinguishingBetweenICanDoItandICan’tDoIt
AvoidFightingwithorSuppressingtheEmotions
Directionsfromthearttherapist:Canyoudescribehowyouaresufferingnow?
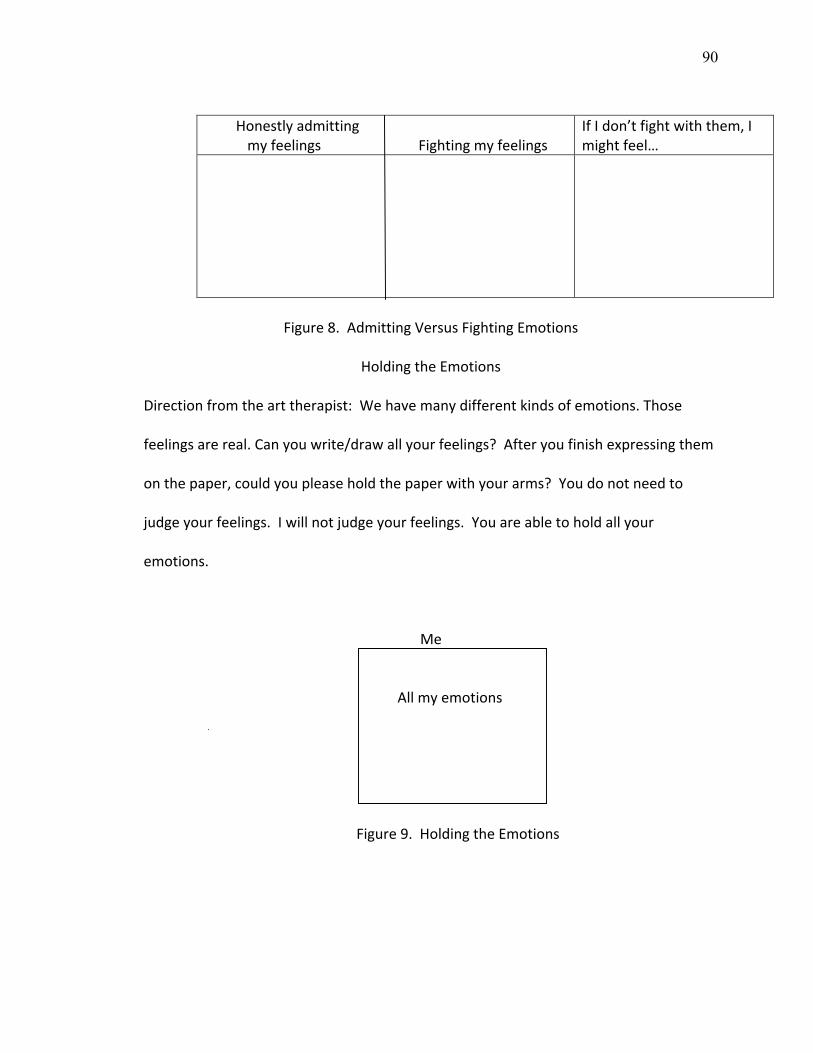
90
HonestlyadmittingmyfeelingsFightingmyfeelings
IfIdon’tfightwiththem,Imightfeel…
Figure8.AdmittingVersusFightingEmotions
HoldingtheEmotions
Directionfromthearttherapist:Wehavemanydifferentkindsofemotions.Those
feelingsarereal.Canyouwrite/drawallyourfeelings?Afteryoufinishexpressingthem
onthepaper,couldyoupleaseholdthepaperwithyourarms?Youdonotneedto
judgeyourfeelings.Iwillnotjudgeyourfeelings.Youareabletoholdallyour
emotions.
Me
Allmyemotions
Figure9.HoldingtheEmotions
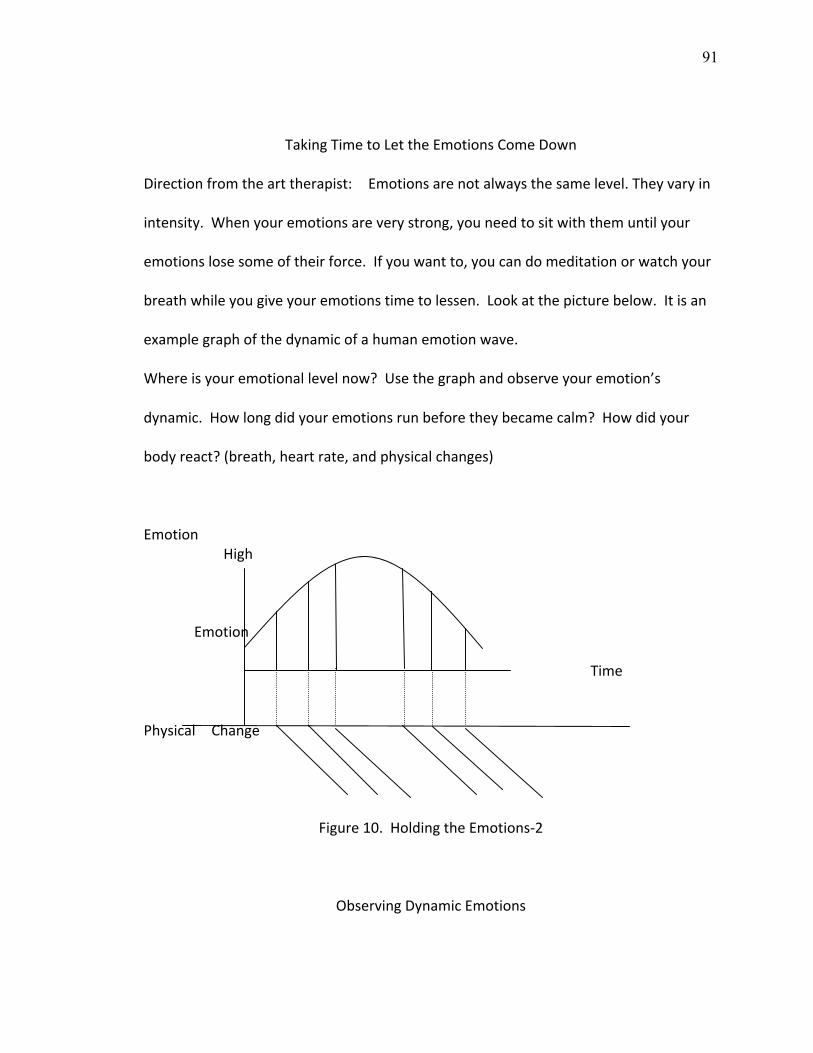
91
TakingTimetoLettheEmotionsComeDown
Directionfromthearttherapist: Emotionsarenotalwaysthesamelevel.Theyvaryin
intensity.Whenyouremotionsareverystrong,youneedtositwiththemuntilyour
emotionslosesomeoftheirforce.Ifyouwantto,youcandomeditationorwatchyour
breathwhileyougiveyouremotionstimetolessen.Lookatthepicturebelow.Itisan
examplegraphofthedynamicofahumanemotionwave.
Whereisyouremotionallevelnow?Usethegraphandobserveyouremotion’s
dynamic.Howlongdidyouremotionsrunbeforetheybecamecalm?Howdidyour
bodyreact?(breath,heartrate,andphysicalchanges)
Emotion High Emotion Time
Physical Change
Figure10.HoldingtheEmotions‐2
ObservingDynamicEmotions
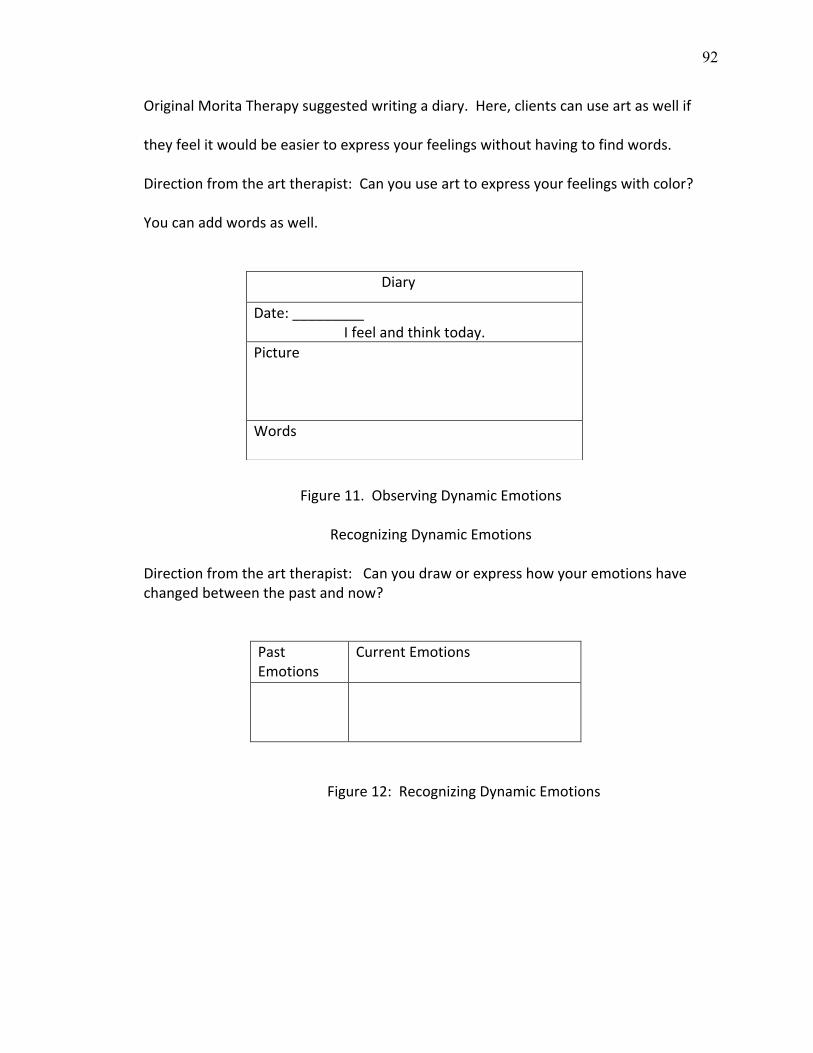
92
OriginalMoritaTherapysuggestedwritingadiary.Here,clientscanuseartaswellif
theyfeelitwouldbeeasiertoexpressyourfeelingswithouthavingtofindwords.
Directionfromthearttherapist:Canyouusearttoexpressyourfeelingswithcolor?
Youcanaddwordsaswell.
Figure11.ObservingDynamicEmotions
RecognizingDynamicEmotions
Directionfromthearttherapist:Canyoudraworexpresshowyouremotionshavechangedbetweenthepastandnow?
PastEmotions
CurrentEmotions
Figure12:RecognizingDynamicEmotions
Diary
Date:_________ Ifeelandthinktoday.
PictureWords
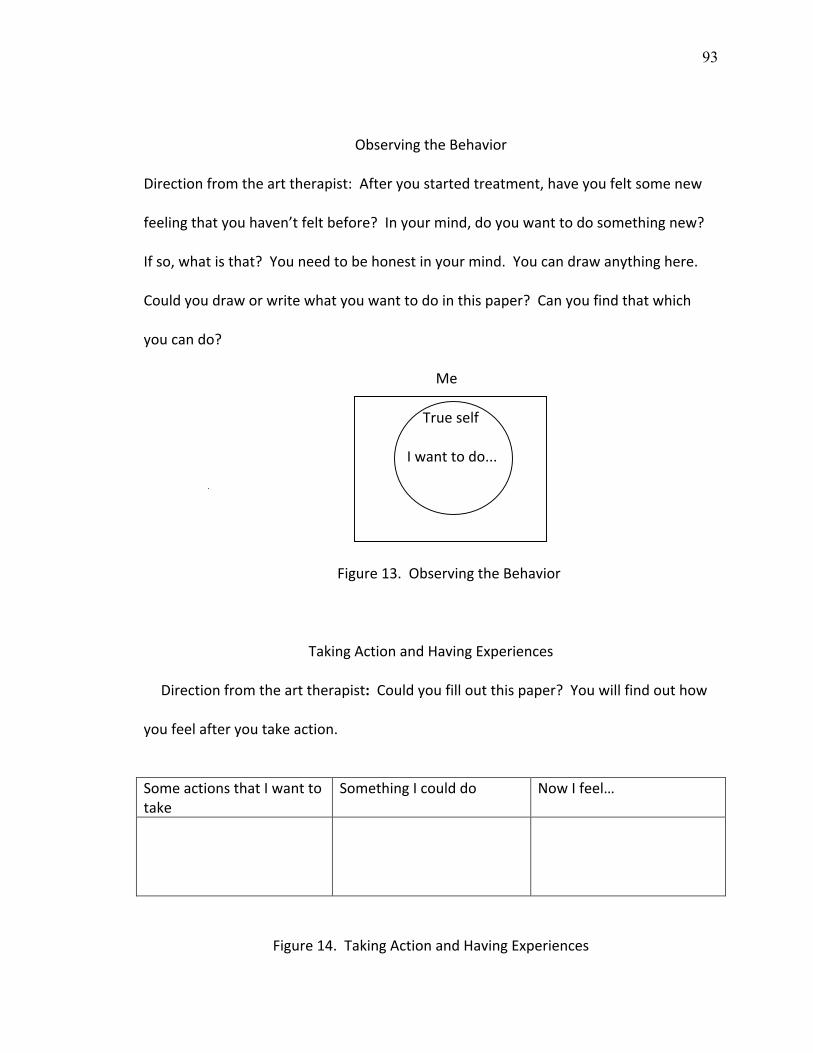
93
ObservingtheBehavior
Directionfromthearttherapist:Afteryoustartedtreatment,haveyoufeltsomenew
feelingthatyouhaven’tfeltbefore?Inyourmind,doyouwanttodosomethingnew?
Ifso,whatisthat?Youneedtobehonestinyourmind.Youcandrawanythinghere.
Couldyoudraworwritewhatyouwanttodointhispaper?Canyoufindthatwhich
youcando?
Me
Trueself
Iwanttodo...
Figure13.ObservingtheBehavior
TakingActionandHavingExperiences
Directionfromthearttherapist:Couldyoufilloutthispaper?Youwillfindouthow
youfeelafteryoutakeaction.
SomeactionsthatIwanttotake
SomethingIcoulddo NowIfeel…
Figure14.TakingActionandHavingExperiences
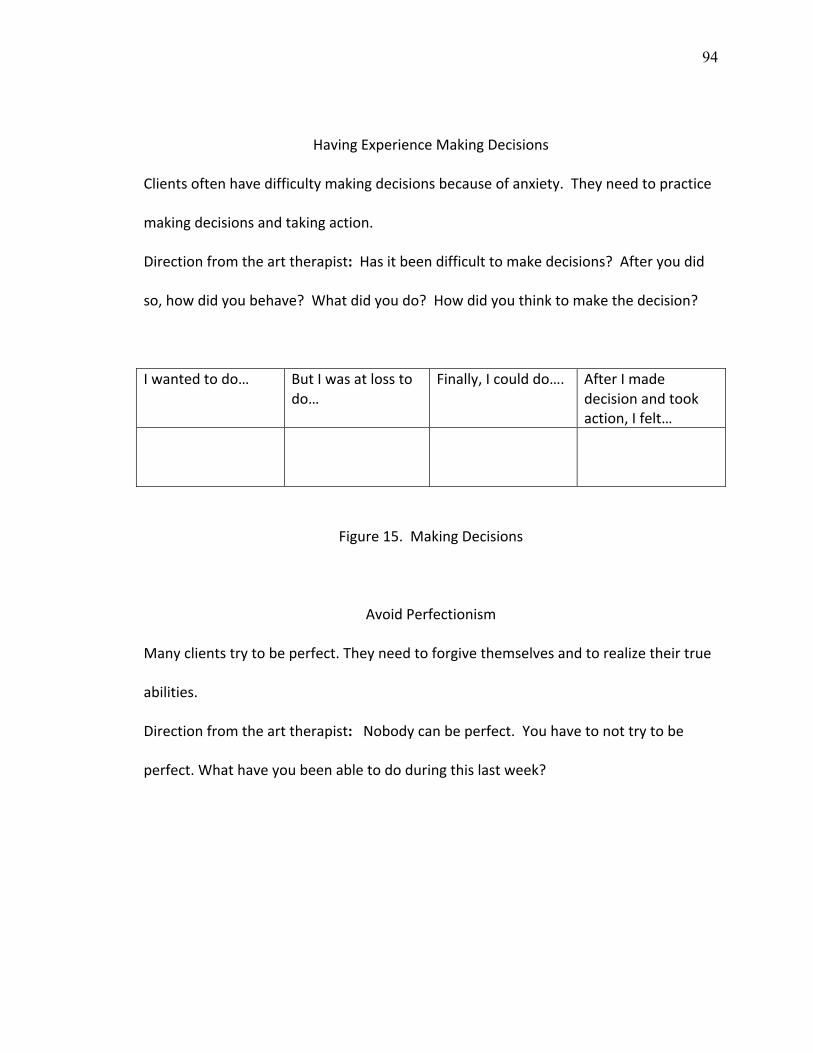
94
HavingExperienceMakingDecisions
Clientsoftenhavedifficultymakingdecisionsbecauseofanxiety.Theyneedtopractice
makingdecisionsandtakingaction.
Directionfromthearttherapist:Hasitbeendifficulttomakedecisions?Afteryoudid
so,howdidyoubehave?Whatdidyoudo?Howdidyouthinktomakethedecision?
Iwantedtodo… ButIwasatlosstodo…
Finally,Icoulddo…. AfterImadedecisionandtookaction,Ifelt…
Figure15.MakingDecisions
AvoidPerfectionism
Manyclientstrytobeperfect.Theyneedtoforgivethemselvesandtorealizetheirtrue
abilities.
Directionfromthearttherapist:Nobodycanbeperfect.Youhavetonottrytobe
perfect.Whathaveyoubeenabletododuringthislastweek?
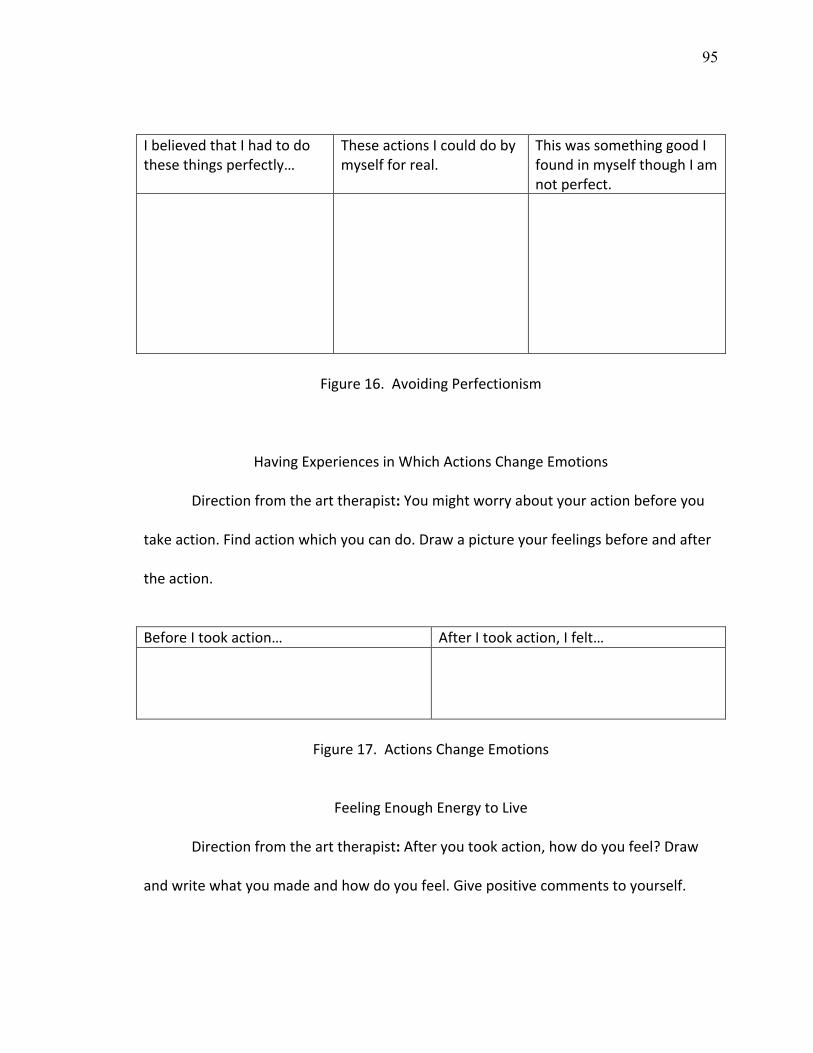
95
IbelievedthatIhadtodothesethingsperfectly…
TheseactionsIcoulddobymyselfforreal.
ThiswassomethinggoodIfoundinmyselfthoughIamnotperfect.
Figure16.AvoidingPerfectionism
HavingExperiencesinWhichActionsChangeEmotions
Directionfromthearttherapist:Youmightworryaboutyouractionbeforeyou
takeaction.Findactionwhichyoucando.Drawapictureyourfeelingsbeforeandafter
theaction.
BeforeItookaction… AfterItookaction,Ifelt…
Figure17.ActionsChangeEmotions
FeelingEnoughEnergytoLive
Directionfromthearttherapist:Afteryoutookaction,howdoyoufeel?Draw
andwritewhatyoumadeandhowdoyoufeel.Givepositivecommentstoyourself.
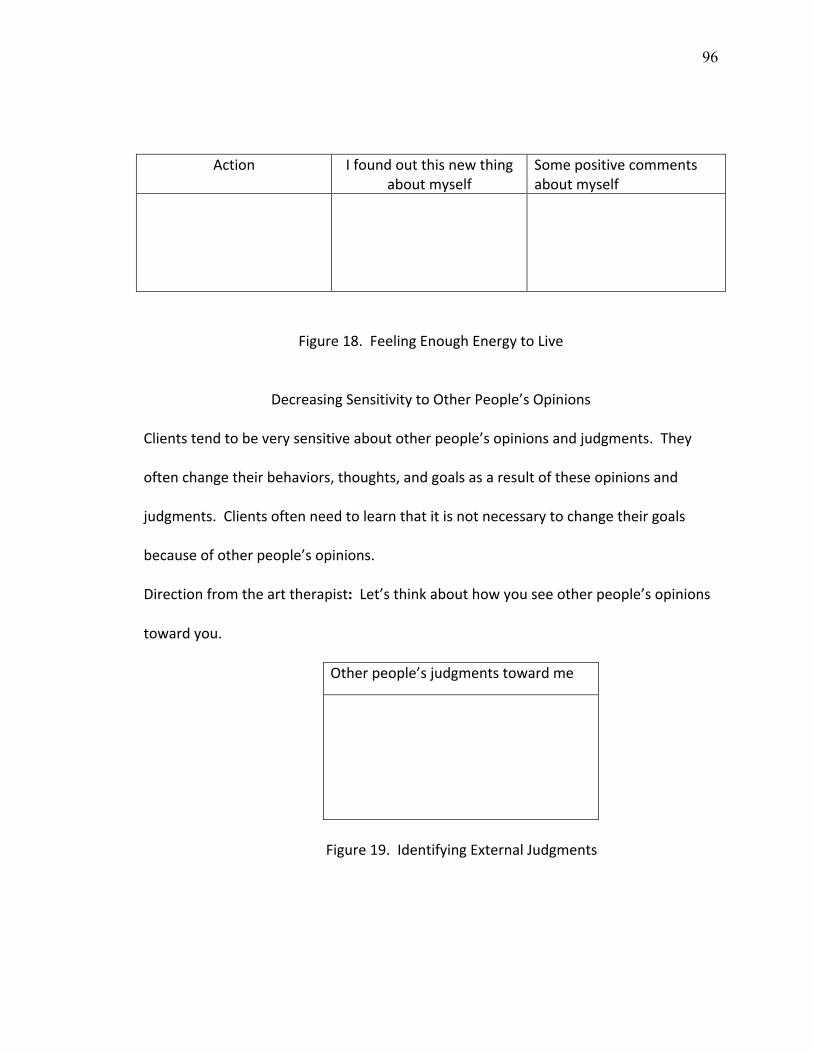
96
Action Ifoundoutthisnewthing
aboutmyselfSomepositivecommentsaboutmyself
Figure18.FeelingEnoughEnergytoLive
DecreasingSensitivitytoOtherPeople’sOpinions
Clientstendtobeverysensitiveaboutotherpeople’sopinionsandjudgments.They
oftenchangetheirbehaviors,thoughts,andgoalsasaresultoftheseopinionsand
judgments.Clientsoftenneedtolearnthatitisnotnecessarytochangetheirgoals
becauseofotherpeople’sopinions.
Directionfromthearttherapist:Let’sthinkabouthowyouseeotherpeople’sopinions
towardyou.
Otherpeople’sjudgmentstowardme
Figure19.IdentifyingExternalJudgments
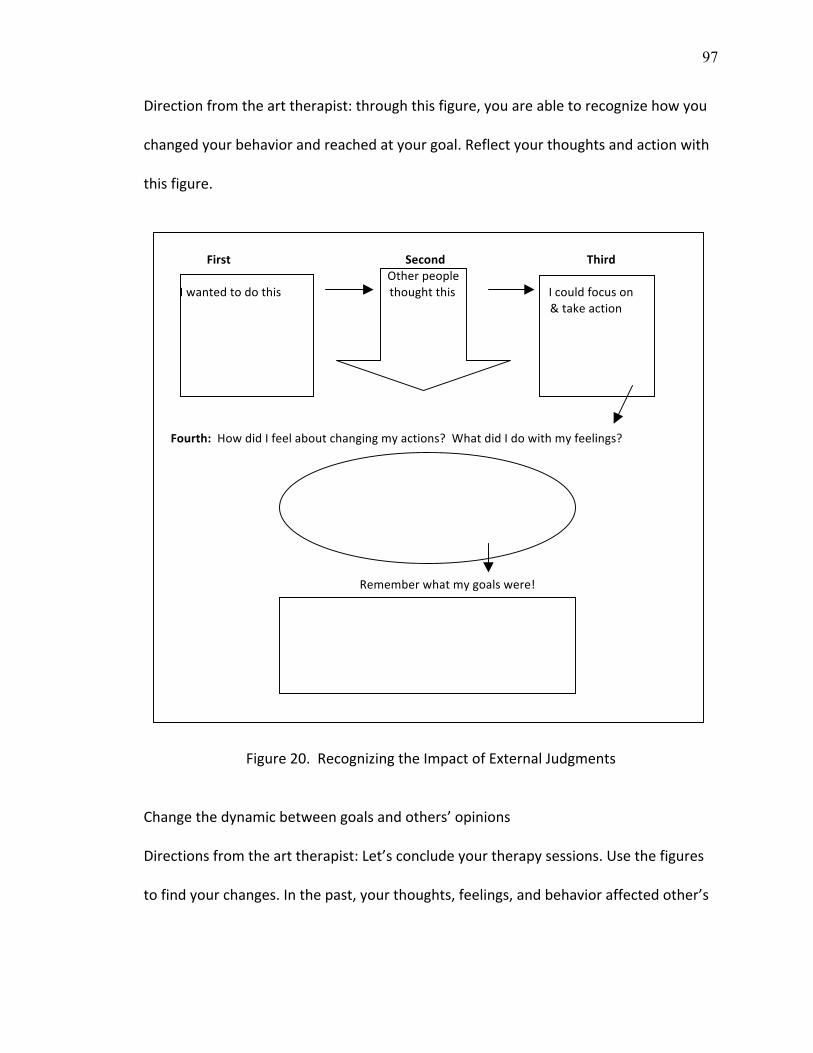
97
Directionfromthearttherapist:throughthisfigure,youareabletorecognizehowyou
changedyourbehaviorandreachedatyourgoal.Reflectyourthoughtsandactionwith
thisfigure.
FirstSecondThirdOtherpeopleIwantedtodothisthoughtthisIcouldfocuson&takeaction
Fourth:HowdidIfeelaboutchangingmyactions?WhatdidIdowithmyfeelings?
Rememberwhatmygoalswere!
Figure20.RecognizingtheImpactofExternalJudgments
Changethedynamicbetweengoalsandothers’opinionsDirectionsfromthearttherapist:Let’sconcludeyourtherapysessions.Usethefigures
tofindyourchanges.Inthepast,yourthoughts,feelings,andbehavioraffectedother’s
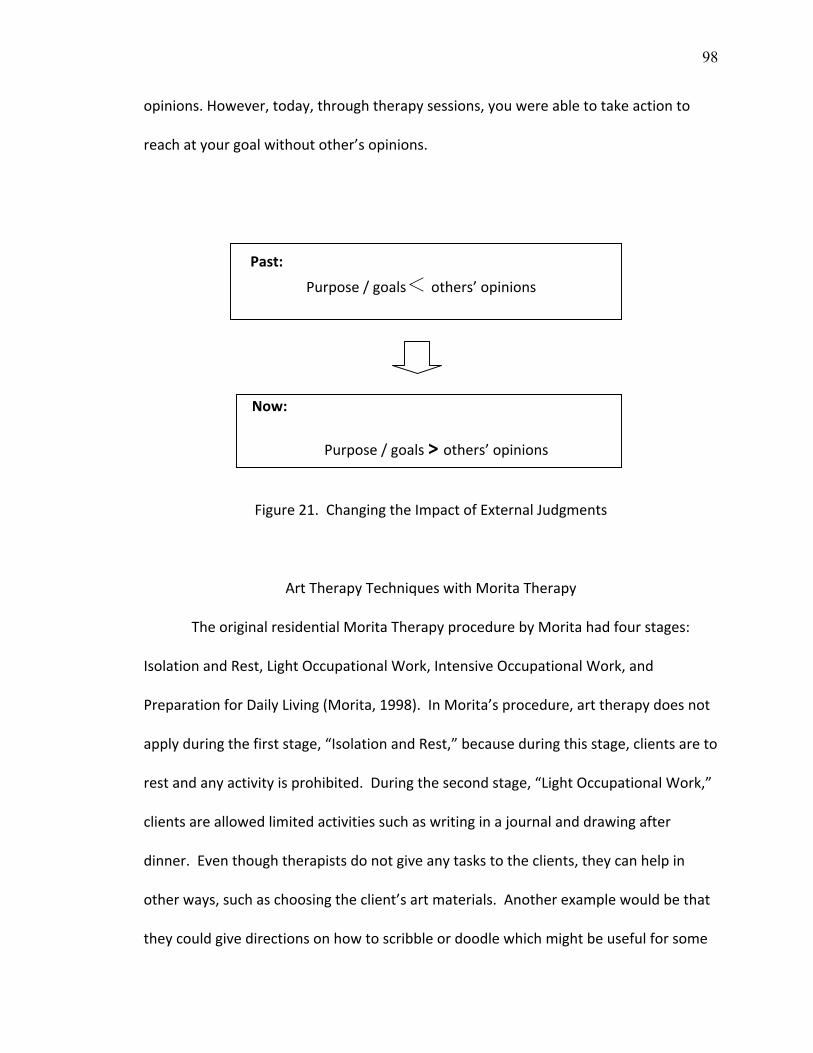
98
opinions.However,today,throughtherapysessions,youwereabletotakeactionto
reachatyourgoalwithoutother’sopinions.
Past:
Purpose/goals<others’opinions
Now:
Purpose/goals>others’opinions
Figure21.ChangingtheImpactofExternalJudgments
ArtTherapyTechniqueswithMoritaTherapy
TheoriginalresidentialMoritaTherapyprocedurebyMoritahadfourstages:
IsolationandRest,LightOccupationalWork,IntensiveOccupationalWork,and
PreparationforDailyLiving(Morita,1998).InMorita’sprocedure,arttherapydoesnot
applyduringthefirststage,“IsolationandRest,”becauseduringthisstage,clientsareto
restandanyactivityisprohibited.Duringthesecondstage,“LightOccupationalWork,”
clientsareallowedlimitedactivitiessuchaswritinginajournalanddrawingafter
dinner.Eventhoughtherapistsdonotgiveanytaskstotheclients,theycanhelpin
otherways,suchaschoosingtheclient’sartmaterials.Anotherexamplewouldbethat
theycouldgivedirectionsonhowtoscribbleordoodlewhichmightbeusefulforsome
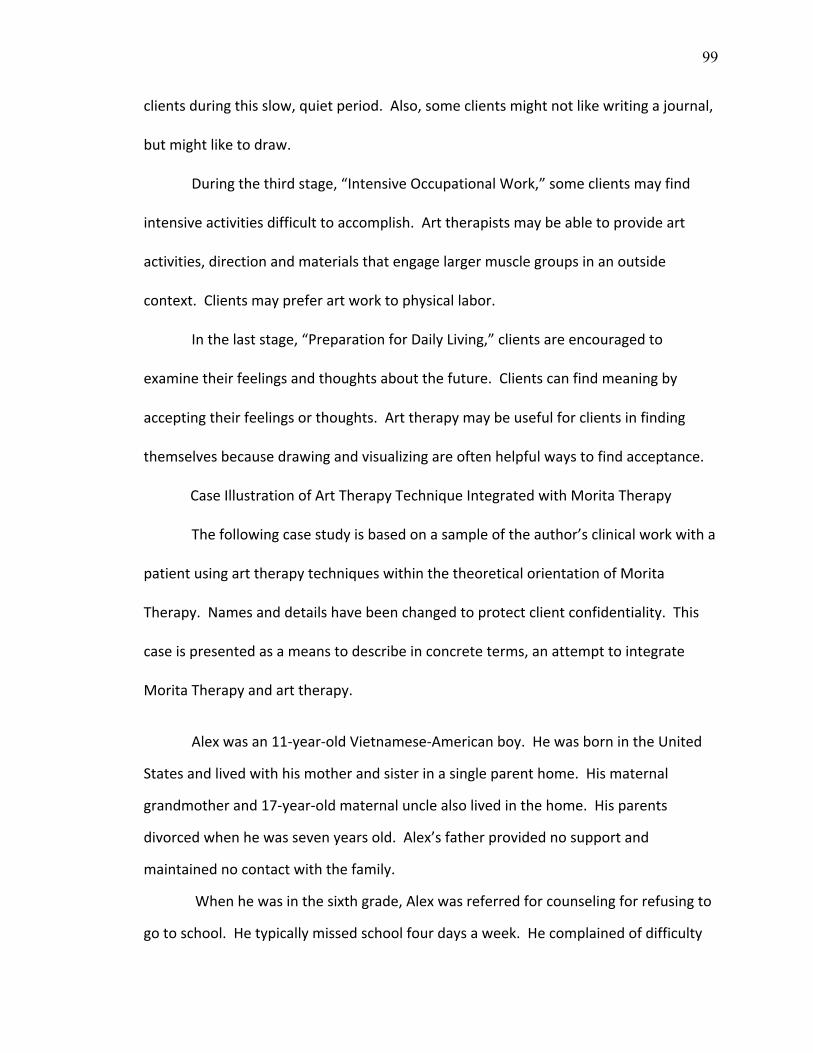
99
clientsduringthisslow,quietperiod.Also,someclientsmightnotlikewritingajournal,
butmightliketodraw.
Duringthethirdstage,“IntensiveOccupationalWork,”someclientsmayfind
intensiveactivitiesdifficulttoaccomplish.Arttherapistsmaybeabletoprovideart
activities,directionandmaterialsthatengagelargermusclegroupsinanoutside
context.Clientsmaypreferartworktophysicallabor.
Inthelaststage,“PreparationforDailyLiving,”clientsareencouragedto
examinetheirfeelingsandthoughtsaboutthefuture.Clientscanfindmeaningby
acceptingtheirfeelingsorthoughts.Arttherapymaybeusefulforclientsinfinding
themselvesbecausedrawingandvisualizingareoftenhelpfulwaystofindacceptance.
CaseIllustrationofArtTherapyTechniqueIntegratedwithMoritaTherapy
Thefollowingcasestudyisbasedonasampleoftheauthor’sclinicalworkwitha
patientusingarttherapytechniqueswithinthetheoreticalorientationofMorita
Therapy.Namesanddetailshavebeenchangedtoprotectclientconfidentiality.This
caseispresentedasameanstodescribeinconcreteterms,anattempttointegrate
MoritaTherapyandarttherapy.
Alexwasan11‐year‐oldVietnamese‐Americanboy.HewasbornintheUnited
Statesandlivedwithhismotherandsisterinasingleparenthome.Hismaternal
grandmotherand17‐year‐oldmaternalunclealsolivedinthehome.Hisparents
divorcedwhenhewassevenyearsold.Alex’sfatherprovidednosupportand
maintainednocontactwiththefamily.
Whenhewasinthesixthgrade,Alexwasreferredforcounselingforrefusingto
gotoschool.Hetypicallymissedschoolfourdaysaweek.Hecomplainedofdifficulty
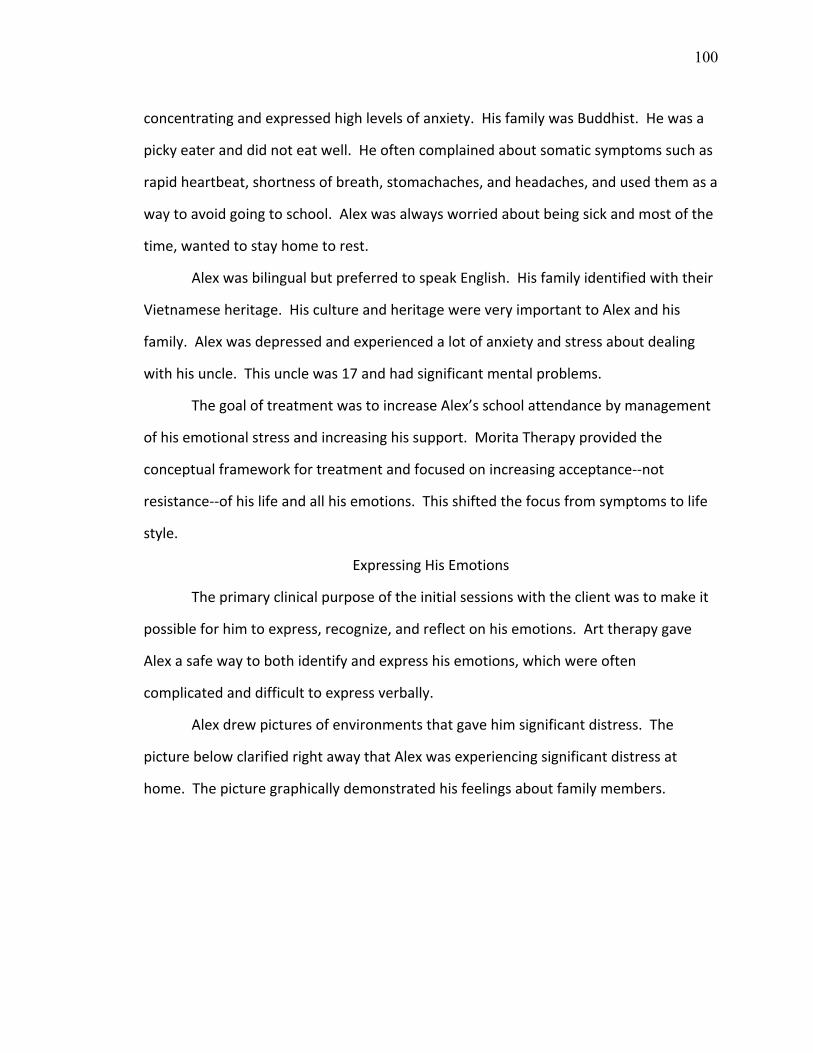
100
concentratingandexpressedhighlevelsofanxiety.HisfamilywasBuddhist.Hewasa
pickyeateranddidnoteatwell.Heoftencomplainedaboutsomaticsymptomssuchas
rapidheartbeat,shortnessofbreath,stomachaches,andheadaches,andusedthemasa
waytoavoidgoingtoschool.Alexwasalwaysworriedaboutbeingsickandmostofthe
time,wantedtostayhometorest.
AlexwasbilingualbutpreferredtospeakEnglish.Hisfamilyidentifiedwiththeir
Vietnameseheritage.HiscultureandheritagewereveryimportanttoAlexandhis
family.Alexwasdepressedandexperiencedalotofanxietyandstressaboutdealing
withhisuncle.Thisunclewas17andhadsignificantmentalproblems.
ThegoaloftreatmentwastoincreaseAlex’sschoolattendancebymanagement
ofhisemotionalstressandincreasinghissupport.MoritaTherapyprovidedthe
conceptualframeworkfortreatmentandfocusedonincreasingacceptance‐‐not
resistance‐‐ofhislifeandallhisemotions.Thisshiftedthefocusfromsymptomstolife
style.
ExpressingHisEmotions
Theprimaryclinicalpurposeoftheinitialsessionswiththeclientwastomakeit
possibleforhimtoexpress,recognize,andreflectonhisemotions.Arttherapygave
Alexasafewaytobothidentifyandexpresshisemotions,whichwereoften
complicatedanddifficulttoexpressverbally.
Alexdrewpicturesofenvironmentsthatgavehimsignificantdistress.The
picturebelowclarifiedrightawaythatAlexwasexperiencingsignificantdistressat
home.Thepicturegraphicallydemonstratedhisfeelingsaboutfamilymembers.

101
Figure22.Alex’sFamily
Rapportwasquicklyestablishedwithclientandtherapistthroughthejoint
projectofmakingart.Alexwasabletodiscusswiththisarttherapist,thevarious
emotionshewasfeeling.ThisgreaterlevelofdisclosurehelpedAlextoincreasehis
understandingofthenatureofhisemotionaldifficultiesandproblemswithinhisfamily.
VisualizinggaveAlexgreaterclarityofthoughtsaswell.
Alex’smotherparticipatedinthesecondsession.Alexandhismotherdrew
picturesoftheiremotionsreflectedinthehumanfigure.Alexandhismotherdiscussed
theirfeelingswitheachotherandthetherapistbysharingtheirpictures.Alexclearly
feltsafeenoughtodisclosethathewasstrugglingwithangerandsadness.
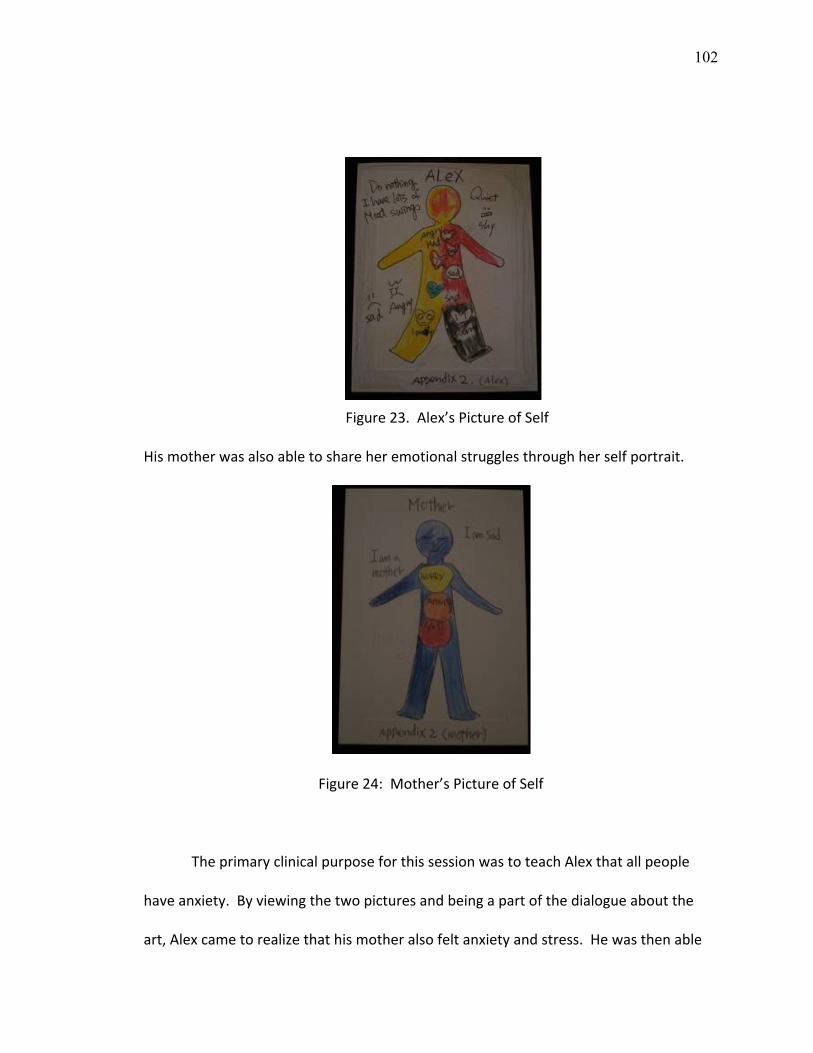
102
Figure23.Alex’sPictureofSelf
Hismotherwasalsoabletoshareheremotionalstrugglesthroughherselfportrait.
Figure24:Mother’sPictureofSelf
TheprimaryclinicalpurposeforthissessionwastoteachAlexthatallpeople
haveanxiety.Byviewingthetwopicturesandbeingapartofthedialogueaboutthe
art,Alexcametorealizethathismotheralsofeltanxietyandstress.Hewasthenable
103
tobegintounderstandthatmanypeopleacceptandholdanxietyindailylifesituations.
Eventhoughhismotherhadanxietyandworries,shewokeupinthemorning,cooked
andworkedbecauseshelovedhimandthefamily.Atthissession,Alexbeganto
changehisfocusfromhisemotionalsymptomstohisbehavior.
Inthenextsessions,Alexfurtherexpressed,recognized,andreflectedonhis
emotionsthroughtheartwork.Hediscussedhowangryandsadhewas.Through
thesesessions,Alexlearnedtonotbeafraidofexpressinghisemotions,butatthesame
time,torecognizeandpreparetoaccepthisemotions.Hedrewtemperature
indicators/barchartsportrayinghowmuchanxietyhefelt.
Figure25.AnxietyTemperatureIndicators1
Hispicturesshowedhowmuchanxietyhefeltindifferentsocialenvironments.
WhenAlexdidnotwanttogotoschool,thetemperaturegaugeshowedahighlevel.
Thehighesttemperatureinhispicturewasreservedforwhenhewaswithhisuncle.At
thattime,hepicturedhisanxietyasflowingsostronglythatitwent“throughtheroof”
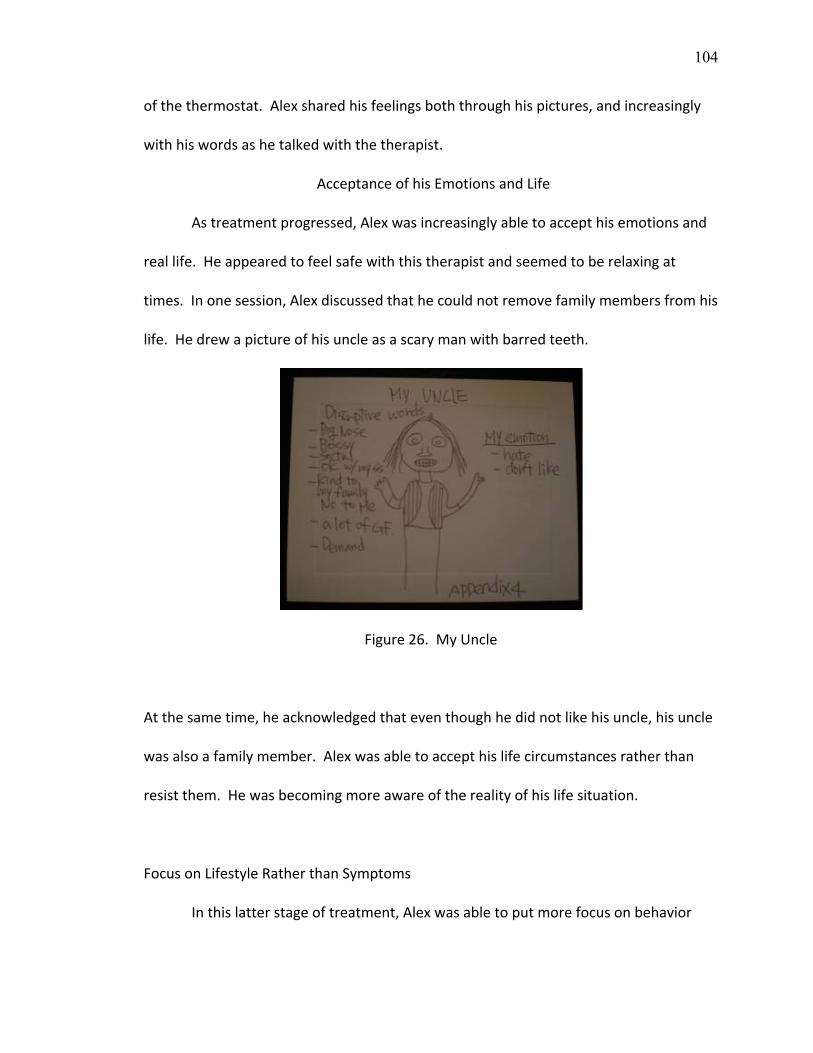
104
ofthethermostat.Alexsharedhisfeelingsboththroughhispictures,andincreasingly
withhiswordsashetalkedwiththetherapist.
AcceptanceofhisEmotionsandLife
Astreatmentprogressed,Alexwasincreasinglyabletoaccepthisemotionsand
reallife.Heappearedtofeelsafewiththistherapistandseemedtoberelaxingat
times.Inonesession,Alexdiscussedthathecouldnotremovefamilymembersfromhis
life.Hedrewapictureofhisuncleasascarymanwithbarredteeth.
Figure26.MyUncle
Atthesametime,heacknowledgedthateventhoughhedidnotlikehisuncle,hisuncle
wasalsoafamilymember.Alexwasabletoaccepthislifecircumstancesratherthan
resistthem.Hewasbecomingmoreawareoftherealityofhislifesituation.
FocusonLifestyleRatherthanSymptoms
Inthislatterstageoftreatment,Alexwasabletoputmorefocusonbehavior

105
andaction,insteadoffocusingonhisemotions.Alexdrewapictureofwhathecould
dotochangehisdailylife,eventhoughhestillfeltanxietyandemotionalstress.
Figure27.Alex’sActions
WhileAlexdiscussedhispicturewiththisarttherapist,hefoundasolutionto
reducehisemotionstowardhisuncle.Hestatedthat“Iamabletoavoidbeing
physicallyclosetomyuncle.Whenmyunclecomesclosetome,Icanmoveandkeep
distancefromhim.”Moreover,herealizedthatifhefocusedonhisbehavior,hecould
reducehisdistresswhichwasoneofthecausesofhisdepression.Hefoundthat
changinghisbehaviorwaseasierthanchangingorresistingemotions.
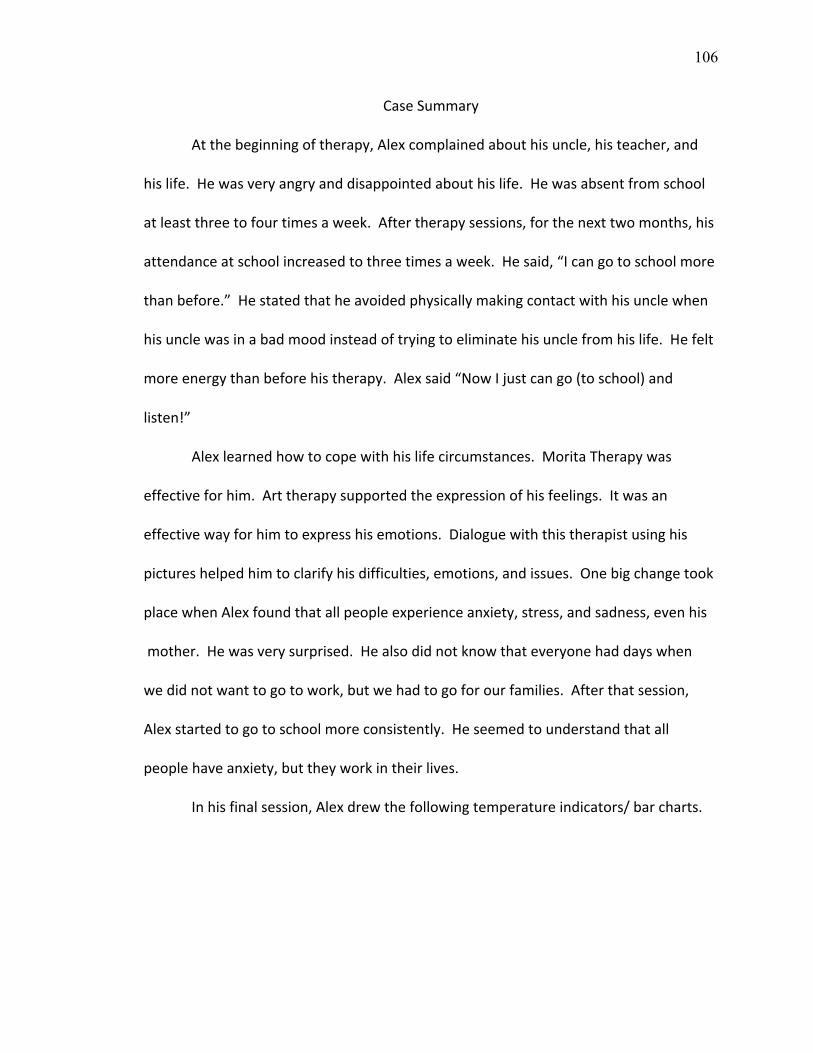
106
CaseSummary
Atthebeginningoftherapy,Alexcomplainedabouthisuncle,histeacher,and
hislife.Hewasveryangryanddisappointedabouthislife.Hewasabsentfromschool
atleastthreetofourtimesaweek.Aftertherapysessions,forthenexttwomonths,his
attendanceatschoolincreasedtothreetimesaweek.Hesaid,“Icangotoschoolmore
thanbefore.”Hestatedthatheavoidedphysicallymakingcontactwithhisunclewhen
hisunclewasinabadmoodinsteadoftryingtoeliminatehisunclefromhislife.Hefelt
moreenergythanbeforehistherapy.Alexsaid“NowIjustcango(toschool)and
listen!”
Alexlearnedhowtocopewithhislifecircumstances.MoritaTherapywas
effectiveforhim.Arttherapysupportedtheexpressionofhisfeelings.Itwasan
effectivewayforhimtoexpresshisemotions.Dialoguewiththistherapistusinghis
pictureshelpedhimtoclarifyhisdifficulties,emotions,andissues.Onebigchangetook
placewhenAlexfoundthatallpeopleexperienceanxiety,stress,andsadness,evenhis
mother.Hewasverysurprised.Healsodidnotknowthateveryonehaddayswhen
wedidnotwanttogotowork,butwehadtogoforourfamilies.Afterthatsession,
Alexstartedtogotoschoolmoreconsistently.Heseemedtounderstandthatall
peoplehaveanxiety,buttheyworkintheirlives.
Inhisfinalsession,Alexdrewthefollowingtemperatureindicators/barcharts.
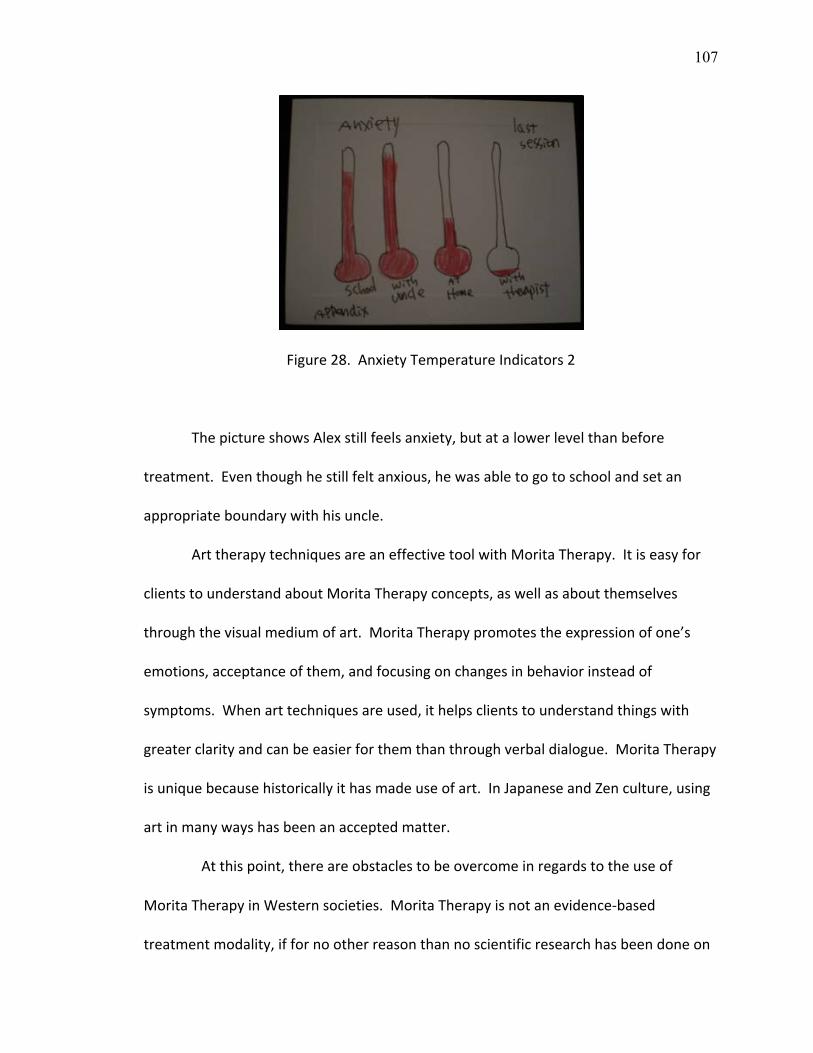
107
Figure28.AnxietyTemperatureIndicators2
ThepictureshowsAlexstillfeelsanxiety,butatalowerlevelthanbefore
treatment.Eventhoughhestillfeltanxious,hewasabletogotoschoolandsetan
appropriateboundarywithhisuncle.
ArttherapytechniquesareaneffectivetoolwithMoritaTherapy.Itiseasyfor
clientstounderstandaboutMoritaTherapyconcepts,aswellasaboutthemselves
throughthevisualmediumofart.MoritaTherapypromotestheexpressionofone’s
emotions,acceptanceofthem,andfocusingonchangesinbehaviorinsteadof
symptoms.Whenarttechniquesareused,ithelpsclientstounderstandthingswith
greaterclarityandcanbeeasierforthemthanthroughverbaldialogue.MoritaTherapy
isuniquebecausehistoricallyithasmadeuseofart.InJapaneseandZenculture,using
artinmanywayshasbeenanacceptedmatter.
Atthispoint,thereareobstaclestobeovercomeinregardstotheuseof
MoritaTherapyinWesternsocieties.MoritaTherapyisnotanevidence‐based
treatmentmodality,iffornootherreasonthannoscientificresearchhasbeendoneon

108
itinrecenttimes.Butthequestionbecomes,whoneedstogetscientificevidencethat
MoritaTherapyiseffectiveforclients?Tothispoint,JapanhasacceptedMorita
Therapyaseffectiveandpartofitsculturalheritagewithoutthescientificvalidation.
Perhapsaspsychologybecomesaworldwideaffair,MoritaTherapywillattractthe
attentionofWesternresearchers.Ifitisfoundtobeausefulformofmentalhealth
treatment,wecanonlyhopethatarttherapywillbeincorporatedintothisinnovative
professionalapproachtohumansuffering.
109
VI:CONCLUSIONS
ThisstudyexploredanintegrationofMoritaTherapywitharttherapytechnique.
TechniqueswerepresentedbasedonKitanishi’sworkwithoutpatientprograms(2008)
allowingfortheintegrationofMoritaTherapyandarttherapy.Kitanishigavedirections
thatwereeasilyunderstood.Thestudyalsopresentedacaseexample,ofthe
integrationofMoritaTherapywitharttherapytechniques.Inthecase,theclient
learnedhowtoexpresshisemotionsandanxietyusingarttherapytechniques.His
anxietyleveldidnotgoaway,asevidencedbyhisfinal“thermostat”picture.However,
theclientshowedimprovementinhisfunctioninginimportantlifedomains.This
indicatesthathewasabletolearntofocusonhisbehaviors,insteadofonhisemotions.
FocusingonbehaviorandnotsymptomsisaprimaryMoritaTherapygoal.Eventhough
theclientstillfelthisanxiety,hewasabletohandlehisdailylifebetterthanpreviously.
Asignificanttherapeuticmomentwaswhenthecliententeredintoadialogue
withthetherapist,usinghisartinwhichhewasabletoclarifyhisrealityandgaininsight
intohisissues.ArttherapytechniquessupportedtheclientinunderstandingkeyMorita
Therapyconcepts.Havingexperiencesisapowerfullearningmethodforclients.Itis
importantforclientstohavetheirownexperiencestounderstandtheirissuesandfind
solutions.Arttherapytechniquesprovidedexperientiallearning,usingastep‐by‐step
process.Goingthroughtheprocesswitharttherapistsisveryimportantforclients
engagedinMoritaTherapy.
Aresultofonecasestudycannotbegeneralized.However,itwasclearthatart
therapytechniquewithMoritaTherapywasusefulforthisparticularclient.The

110
treatmentwaseffective.Arttherapycanbeusedtohelpclientsunderstandthe
underlyingprinciplesofMoritaTherapy.Additionalstudiescouldpresentmorecase
studiesandshowmoreresults.ItishopedthatMoritaTherapywillbecomeaneffective
waytotreatclientsofAsianheritage.Itisalsohopedthatthiswillbehelpfulforsome
clientsfromWesterncultures.
Forthefuture,MoritaTherapyneedstohavemorescholarlypaperspublishedin
Englishforcliniciansaroundtheworld.MoritaTherapywillbeusefulforAsianclients
andclientswhocomefromaBuddhistheritage.Thesedays,scientistshave
demonstratedtheeffectivenessofmeditation.StudiesonMoritaTherapywouldmake
afineadditiontotheprofessionalliteratureonAsiantherapeuticmethodologies.Itis
importantforMoritaTherapytodemonstrateits’methodsandexplainits’uniqueview
ofpathologytotheworld.
Inparticular,studiesonMoritaTherapyshouldbepublishedmoreinEnglish‐
speakingjournals.TherearemanyarticlesaboutMoritaTherapyinthelibrariesof
Japan.However,mostofthemwerewrittenonlyinJapanese.Itisdifficulttofindmany
scholarlyarticlesinEnglishandinscholarlyresearchdatabases.Istronglybelievethat
Moritawantedtohelppeoplewithhisskillsasaclinician.Thatisthereasonwhyhe
createdMoritaTherapy.Hisresearchisfascinatingbecausethebreadthanddepthof
hisknowledgeofmentalillness,humanphenomenon,andEasternandWestern
psychologywasprofound.Eventhoughheisnolongeralive,hisphilosophyisstillliving
andattractsmanypeople.MoritaTherapyisusefulandshouldbeusedintheworldto
helppeople.
111
AlthoughithasbeensaidthatunderstandingMoritaTherapy’stheoretical
constructsisdifficult,arttherapyisabletohelptheclientunderstandandbenefitfrom
theprocess.ForAsians,thereisculturalsignificancetothismethodology.Zen
Buddhismhasusedartandcreativeprocessforbelieverstounderstanditsprinciplesfor
centuries.However,ishasusedartasahealingmethodonlywithintheboundsofits
religiousroleinsociety.ThecombinationofarttherapyandMoritaTherapyexamined
inthispapermakespossibletheuseofZenteachingsformedicalpurposes.This
possibilitybringswithitagreatdealofhope.PeoplewhowereraisedinBuddhist
culturesmayentertherapymorereadilyifMoritaTherapybecomesbetterknown,
becauseMoritaTherapyconceptsandprocessesaremorefamiliartothemthan
Western‐basedtherapies.Therapistsshouldnotpushclientstouseart.However,for
thoseclientswhoarecomfortablewitharttherapytechniques,integratingMorita
Therapyandtheprocessofcreatingartcanbeapowerfulandeffectiveformof
treatment.Abalancedcombinationofarttherapy’samazingabilitytobeacatalystfor
humangrowth,coupledwiththeevolvingstructureofMoritaTherapy’sculturally‐
congruentmethodologymayofferhealingtoabroaderrangeoftheworld’speoples.

112
REFERENCES
Aizawa,S.,Ohara,K.,Masuno,H.,Kojima,Y.&Iwai,K.(1967).Morita ryouhou niokeru bashoteki jyoken nitsuite [Regardingtheenvironmentalconditionthatis requiredforMoritaTherapy].Tokyo,Japan: NomuraKyojuSyuunin10syunen kinenronbunsyu.Andersen,D.T.(2005).Empathy,psychotherapyintegration,&meditation:aBuddhist contributiontothecommonfactorsmovement.Journal of Humanistic
Psychology,45,483‐502.
Brook,S.(2004).Tools of the trade: a therapist’s guide to art therapy assessments. Illinois:CharlesCThomasPublisher,LTD.Clements,K.(1996).Theuseofarttherapywithabusedchildren.Clinical Child Psychology & Psychiatry,1,181‐198.Cumming,S.&Visser,J.(2009).Usingartwithvulnerablechildren.Support for learning. 24,4,151‐158.Doi,T.(1963). Sieshin ryouhou to seishin bunseki[Psychotherapyandpsychonalysis]. Tokyo,Japan:Kanekoshobo.Dunn‐Snow,P.&Joy‐Smellie,S.(2000).Teachingarttherapytechniques:Mask‐making, acaseinpoint. Journal of American Art Therapy Association, 17,2,125‐131.Eckhoff,A.(2007).Theimportanceofartviewingexperiencesinearlychildhoodvisual arts:theExplorationofamasterartteacher’sstrategiesformeaningfulearlyarts experiences.Early Childhood Education Journal, 35,463‐472.Elkins,D.E.&Stovall,K.(2000).AmericanArtTherapyAssociation,Inc.;1998‐1999 membershipsurveyreport. Journal of American Art Therapy Association, 17,(1) 41‐46.Fenton,J.(2000).Unresolvedissuesofmotherhoodforelderlywomenwithserious mentalIllness.Journal of American Art Therapy Association, 17,24‐30.Frank,D.J.&Frank,J.B.(1993).Persuasion & healing: A comparative study of
psychotherapy. MD:TheJohnsHopkinsLtd.France,M.,Cadieax,J.&Allen,E.(1995).Lettertherapy:Amodelforenhancing counselingintervention.Journal of counseling and development, 73,317‐381.
113
Fujita,C.(1977).Morita ryouhou ni okeru chiryou wo meguru shomondai [Issues regardingMoritaTherapytreatments].InTakara,T.&Ohara,T.(Eds.),Gendaino Moritaryouhou.Tokyo,Japan:Hakuyousha.Furuta,S.(1982).Nihon no Zen: Nihonjin no bi‐ishiki[JapaneseZen:Japaneseconcept ofbeauty].Yoshida(Ed.)Zen&arts I(13).Tokyo,Japan:PerikanCo.Gladding,S.&Henderson,D.(1998).TheCreativeartincounseling:Amulticultural
perspective. Arts in Psychotherapy, 25,183‐187.Graham,M.&Sontag,M.(2001).Artasanevaluativetool:Apilotstudy. Journal of the American Art Therapy Association, 18,37‐43.Gussak,D.(2009).Comparingtheeffectivenessofarttherapyondepressionandlocus ofcontrolofmaleandfemaleinmates. The Art in Psychotherapy, 36,202‐207.Hashimoto,K.(1985).Shinmoritaryouhoutouniokeruchiryoujyounosyomonndai: chiryoukannkyounosetteinohennkatosonoeikyounikannsurukousatsu[Issues ofnewMoritatherapymethod].Morita ryouhou situkiyou, 7,33‐39.Heyes,S.C.(2002).Buddhism&acceptance&commitmenttherapy.Cognitive and Behavioral Practice, 9,58‐66.Hayes,P.(2001). Addressing cultural complexities in practice.Washington,D.C.: AmericanPsychologicalAssociationPublications.Hofman,S.G.(2008).Acceptanceandcommitmenttherapy:NewwaveorMorita therapy?Clinical Psychology: Science & Practice, 15,280‐285.Hoshino,J.(2003). MulticulturalArtTherapywithfamilies.InMalchiodi(Eds.), Handbook of art therapy (pp.).CA,NY:GuilfordPress.HoughtonMifflinCompany(2009).The American heritage dictionary of the English language,(4thed.,)IL:HoughtonMifflinCompany.Ichikawa,M.(2008).Gairai Morita ryohou: sinnkeisyou no tannki cyuchutiryou[Morita Therapyforoutpatient].Tokyo,Japan:Hakuyousya.Inoue,R.,Miwaki,Y.,Seki,N.&FilmArtInc.(2008).Art x therapy chouryu [Artand therapymovement].Tokyo,Japan:FilmArtInc.Ishiyama,F.I.(1990).AJapaneseperspectiveonclientinaction:Removingattitudinal blocksthroughMoritatherapy.Journal of Counseling and Department, 68,566‐ 570.
114
Ishiyama,F.I.(1986).Moritatherapy:Itsbasicfeaturesandcognitiveinterventionfor anxietytreatment.Psychotherapy,23,375‐381.Ishiyama,F.I.(1986).Positivereinterpretationofdeath:aJapanese(Morita) psychotherapyapproachtoanxietytreatment.Psychotherapy: Theory, Research, Practice, & Training, 23,556‐562.Jordan,K.(2001).Familyarttherapy:Thejointfamilyholidaydrawing.Counseling and therapy for couples and families, 9,52‐54.Jung,M.&Asawa,P.P.(1994).A history of art therapy in the United States.Alexandria, VA:AmericanArtTherapyAssociationInc.Kazamaturi,H.(1980).Kokoro no yamainikiku kusuri: kousinnyakunyumon [Midication for mental illness].Tokyo:yuhikakusensho.Kalmanowitz,D.&Potash,J.S.(2010).Ethicalconsiderationsintheglobalteachingand promotionofarttherapytonon‐arttherapists.TheArtsinPsychotherapy,37, 20‐26.Kearney,K.S.&Hyle,A.E.(2004).Drawingoutemotions:Theuseofparticipant‐ produceddrawinginqualitativeinquiry.QualitativeResearch,4,361‐382.Kitanishi,K.(2008).Moritaryohotowa:KihontekiNaKangaekata[Motionpicture]. (AvailablefromMentalHealthOkamotoMemorialFoundation,1‐5‐10Sonezaki KitakuOsaka530‐0057Japan).Kitanishi,K.(1987).Moritaryouhouniokeruchiryousyakanjyakankei[Relationships betweenclientsandcliniciansinMoritaTherapy].Moritaryouhousitukiyo, 9,2‐ 5.Kitanishi,K.(1990).Moritaryouhounokeishotohatten:Jikeiidaidaisanbyouinno kensyunikanrensite[DvelopmentofMoritaTherapyatJikeimedicalschool]. Moritaryouhou gattukai, 1, 96‐98.Kitanishi,K.(2007). Morita ryouhou no subetega wakaru hon[EverythingaboutMorita Therapy].Tokyo,Japan:Kodansha.Kitanishi,K.(1984).Moritaryohoujyuninennochiryoutaiseinohenni[Developmentof MoritaTherapytreatmentsintwelveyears].Moritaryouhousitsukiyou, 6,24‐30.Kitanishi,K.,Toyohara,T.,Nagayama,K.,Hashimoto,K.,Minakawa,K.&Miyake,Y. (2007).Morita ryouho to seishinbunsekitekiryoho [Morita Therapy and psychoanalysis].Tokyo,Japan:SeishinShobou.
115
Kitanish,K.&Mori,A.(1989).Morita ryouhou no kenkyu: aratana tennkai wo mezashite [StudyofMoritaTherapyfornewdevelopment].Tokyo, Japan:Kongousyuppan.Komatsu,J.,Kitanishi,K.,Mori,A.&et.al.(1985).StatisticalstudyonMorita Shinkeishitsufortwelveyears. Jikeidaishi, 100,293‐307.Kondo,K.(1966).TankiryohoutoMoritaryoho[ShorttermtreatmentsandMorita Therapy].Shinkeisitsu,6,47‐61.Kwee,M.,&Ellis,A.(1998).TheInterfacebetweenrationalemotivebehaviortherapy (REBT)andzen. Journal of Rational‐Emotive& Cognitive Behavior Therapy, 16,1, 5‐43.Kramer,E.(1972).Art as therapy with children.NY:SchockenBooks.Kramer,E.(1958). Art therapy in a children’s community. NY:CharlesC.Thomas.Kubota,M.,(2008).GairaiMoritaRyohonoSusumekata1,[Motionpicture].(Available fromMentalHealthOkamotoMemorialFoundation,1‐5‐10SonezakiKitakuOsaka530‐0057Japan).Lieberman,F.ZenBuddhismanditsrelationshiptoelementsofeasternandWestern arts.RetrievedOctober21,2009,from http://artsites.ucsc.edu/faculty/lieberman/zen.html.Malchiodi,A.C.(1997).Breaking the silence: Art therapy with children from violent homes (2nd Ed.).NY:Brunner/Mazel.Malchiodi,A.C.(1998).The art therapy sourcebook.LA:LowellHouse.McMurray,M.,Schwartz‐Mirman,O.&Maizel,S.(2000).Arttherapy:Indicationfor treatmentofchoice. The Arts in Psychotherapy, 27,191‐196.McNamee,C.(2005).Bilateralart:Integratingarttherapy,familytherapy,and neuroscience.Contemporary Family Therapy, 27,545‐557.Maeda,F.&Nathan,H.J.(1999).Understandingtaijinkyofushothroughitstreatment, Moritatherapy[Moritatherapytreatmentsfortaijinkyofusho].Journalof PsychosomaticResearch,46,525‐530.
116
Matsumi,T.J.(1979).Culturalfactorsandsocialinfluencetechniquesinnaikantherapy: AJapaneseself‐observationmethod. Psychotherapy: Theory Research & Practice, 16,385‐390.Morgan,D.(2001).Assimilationfromtheeastandthespectrumifconsciousness. Journal of Psychotherapy Integration, 11,87‐104.Morita,S.(1998).Morita therapy and the true nature of anxiety‐based disorders (shinkeishitsu).InKondo,A.&LeVine,P.(Eds.)NY:StateUniversityof New York. Morita,S.(1929/1960/2004)Shinkeishitsu‐no hontai‐to ryohou.Tokyo,Japan: Hakuyousya.McNiff,S.(2009).Cross‐culturalpsychotherapyandartmentalhealth:Areportofthe
surgeongeneral.RetrievedFebruary8,2010,fromhttp://www.surgeongeneral.gov/library/mentalhealth/chapter3/sec5.html.
Milne,L.C.&Greenway,P.(1999).Colorinchildren’sdrawings:Theinfluenceofage andgender.TheArtsinPsychotherapy,1,261‐263.
Nabors,L.,Reyndds,M.,&Quinlan,A.(2000).TheEffectivenessofarttherapy:Doesit work? Journal of American Art Therapy Association, 17,207‐213.Naitou,A.,Seki,N.,&Yamashita,Y.(1995).Arttherapyniokerusozainoimi[Meaning ofartmaterialsinarttherapy].Rinsho Byouga Kennkyu, 10,140‐150.Naumburg,M.(2001).Spontaneousartineducationandpsychotherapy.American Journal of Art Therapy, 40,46‐65.Nakamoto.(2009).ComparingandcontractingMoritatherapywithwesterntherapies. (Doctoraldissertation,SanDiego,CA:AlliantInternationalUniversitySanDiego).
Nakamura,K.(2008).MoritaRyohonoTekiotoChiryoKeitai,[Motionpicture]. (AvailablefromMentalHealthOkamotoMemorialFoundation,1‐5‐10Sonezaki KitakuOsaka530‐0057Japan)Niifuku,N.(1980).Moritaryouhoudeokorigachina‘seishinryouhoutekifukusayou’ [issuesofMoritaTherapytreatments:sideeffectsofthetreatments]. Kikanseishin ryouhou, 6,16‐23.Nissimov‐Nahum,E.(2009).Useofadrawingtasktostudyarttherapists’personal experiencesintreatingaggressivechildren. The Art and Psychotherapy, 36,140‐ 147.
117
OchanomizuHospitalShinryoNaika.(2007).Tokyo,Japan:MitsuhiroIchikawa. RetrievedJanuary4,2010,fromhttp://www.moritatherapy.com.Ohara,K.,Aizawa,S.,&Iwai,K.(1970).Morita ryohou [Morita Therapy].Tokyo,Japan: Bunkodo.O’Hare,D.&Cook,D.(1983).Children’ssensitivitytodifferentmodesofcolorusein art.British Journal of Educational Psychology, 53,267‐277.Palmer,L.,Farrar,A.,Valle,M.,Ghahary,N.,Panella,M.&DeGraw,D.(2000).An investigationoftheclinicaluseofthehouse‐tree‐personprojectivedrawingin thepsychologicalevaluationofchildsexualabuse.Child Maltreatment, 5,169‐ 175.Pifalo,T.(2007).Joggingthecogs:Traumafocusedarttherapyandcognitivebehavior therapywithsexuallyabusedchildren.Journal of the American Art Therapy Association, 24,170‐175.Rosen,A.(2009).TheHeartliftoperation.Journal of the American Art Therapy Association, 26,130‐134.Rubin,J.A.(2001).Approaches to art therapy theory & technique, second edition. EditedbyRubin,J.A.NY:Brunner‐Routledge.Rubin,J.A.(1998).Art therapy: An introduction.PA:Brunner/Mazel.Rubin,J.A.(2005).Artful Therapy.NJ:JohnWiley&Sons,Inc.Rubin,J.A.(1984).Child art therapy: Understanding and helping children grow through art (2ndEd.).NY:JohnWiley&Sons,Inc.Rustin,T.A.(2008).Usingartworktounderstandtheexperienceofmentalillness: mainstreamartistsandoutsiderartists.RetrievedJanuary4,2010,from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2736519/.Reynolds,D.K.(1969).Moritatherapyandthebehaviortherapies. Berkeley: University of California Press.
Suzuki.C.(1967).Moritaryohounogijyutsutoriron:tokuniningenkankeitochiryouzou womegutte[MoritaTherapy’methodsandtechnique:humanrelationshions]. Seishinigaku. 9, 471‐479.
118
Suzuki,T.(1989).ConceptofneurastheniaanditstreatmentinJapan. Cult Med Psychiatry 13,2,187‐202
Sansone,D.(2005).Moritatherapyandconstructiveliving:Choicetheoryandreality therapy’seasternfamily. International Journal of Reality Therapy, 25,26.Sorai,K.(2000).Shinri tests[Psychologicaltests].InY.Tokuda,K.Omori,M.Iimori,H. Nakai,&Y.Yamanaka(Eds),Geijyuturyouho:1(PP.162‐172).Tokyo,Japan: wasakiGakujyutushuppanInc.Silver,R.(2009).Identifyingchildrenandadolescentswithdepression:Reviewofthe stimulusdrawingtaskanddrawastoryresearch.Art Therapy: Journal of the American Art Therapy Association, 26,4,174‐180.Suwaki,H.(1985).NaikananddanshukaiforthetreatmentofJapanesealcoholic patients.British Journal of Addiction, 74,15‐19.Suwaki,H.(1985).Internationalreviewseriesalcoholandalcoholproblemsresearch. Japan, British Journal of Addiction, 80,127‐132. Suzuki,T.(1940).Zen and arts.In1996,Yoshida,S.(Ed.).Zenandarts.Tokyo,Japan: PerikanCo.Suzuki,T.(2005).Zen and Japanese culture.Tokyo,Japan:KoudanshyaInternational Inc.Tatematsu.I.(1986).Nyuinmoritaryouhoucyunochiryouchudankikitokokufuku [IssuesofinpatienttreatmentsinMoritaTherapy].Morita Ryouhou Sitsu Kiyou, 8, 22‐32.Toneatto,T.(2002).Ametacognitivetherapyforanxietydisorders:Buddhistpsychology applied.Cognitive & Behavior Practice, 9, 72‐78.Tanaka‐Matsumi,J.(1979).CulturalfactorsandsocialinfluencetechniquesinNaikan therapy:AJapaneseself‐observationmethod.Psychotherapy: Theory Research & Practice, 16.385‐390.Thyme,K.E.,Sundin,E.C.,Stahlberg,G.,Lindstrom,B.,Eklof,H.&Wiberg,B.(2007). TheOutcomeofshort‐termpsychodynamicarttherapycomparedtoshort‐term psychodynamicverbaltherapyfordepressivewomen.Psychoanalytic Psychotherapy, 21,250‐264.
119
Uchimura,H.(1970).Moritaryouhouniokeru“toraware”tochiryouno“ba”nituite [PathologyofobsessionandthetreatmentenvironmentinMoritaTherapy]. Seishinigaku, 12,741‐784.Vick,M.R.,(2003).A brief history of art therapy,Edi.Malchiodi,A.C.(2003).Handbook ofarttherapy,NY:GuilfordPress.Wadeson,H.(2000). Art therapy practice.NY:JohnWiley&Sons,Inc.Wadeson,H.(1987,1995).The Dynamics of art psychotherapy.NY:JohnWiley&Sons, Inc.Wallace,J.,Yorgin,P.D.,Carolan,R.,Moore,H.,Sanchez,J.,Belson,A.,etal.(2004).The useofarttherapytodetectdepressionandpost‐traumaticstressdisorderin pediatricandyoungadultrenaltransplantrecipients.Pediatric Transplantation, 8,52‐59.Wegman,P.&Lusebrink,V.(2000).KineticFamilyDrawingscoringmethodforcross‐ culturalstudies.The Art in Psychology, 27,179‐190.White,C.,Wallace,J.&Huffman,L.(2004).Useofdrawingtoidentifythrough impairmentamongstudentswithemotionalandbehavioraldisorders:An exploratorystudy.Journal of the American Art Therapy Association, 21,210‐ 218.Wicks‐Nelson,R.&Israel,A.C.(2009).Abnormal child and adolescent psychology. NJ:PersonPrenticeHall. Yanagida,S.(1982).Nippon no zen, Nipponjin no biisiki [Japanese Zen and Japonese sense of beauty].InYoshida(Ed.)Zen&artsI(13).Tokyo,Japan:PerikanCo.Yoshida,S.(1985). Nippon Bunka to Zen [Japanese culture and Zen],In1996,Yoshida (Ed.)Zen&artsI(13).Tokyo,Japan:PerikanCo.

120





























