Embed Size (px)
Citation preview

Jaurnal of Advanced Nur.ii/ig, 1988,13,649-661
Improving recovery following cardiac surgery: a randomized clinicaltrial*
Susati R. Gortner, Catherine L. Gilliss, Julie A. Shinn. Patricia A. Sparacino,Sally Rankin. Maribelle Leavitt, Martha Price and Mark Hudes School of Nursing.University of Calif ornia. San Francisco. USA
Accepted for publication 20 October 1987
GORTNER S.R.. GILLISS C.L.. SHINN J.A., SPARACINO P.A., RANKIN S.,LEAVITT M., PRICE M. & HUDES M. (\9m Journal of Advanced Nur.sing 13, 649-661Improving recovery following cardiac surgery: a randomized clinical trialTo enhance individual and family health during recovery from heart surgery, this studyemployed nursing intervenlions based on self-efficacy and family stress theory during thehospitalization period and for 3 months thereafter. The effectiveness ofthe interventions wereassessed through a randomized trial in which 67 prospective bypass and valve surgery patients,aged 30-77 years, and their spouses, were allocated either the experimental interventions orusual care and followed for 6 months. At 3 months post-surgery, the only statisticallysignificant differences between the experimental and controls were on perceived self-efficacyfor lifting and tolerating emotional distress. At 6 months no significant differences were foundon individual or family measures. Analyses revealed that age, gender and preoperative cardiacstatus significantly affected individual recovery. The study is continuing wilh a larger sample inorder to explicate the recovery process and to better determine whether a low intensity nursingintervention can elTect changes in individual and family recovery.
INTRODUCTION
The success of surgical treaiment for valvularheart disease and for chronic angina associatedwith coronary artery disease has been well estab-lished in the United States (Jensen et al. 1982.Mclntosh 19SI. Miller 1983. Rahimloola et al.1981,Rahimtaola 1982, Stanford 1982, WesternCenter for Health Planning 1981). However, therehabilitative process following treatment anddischarge has not been examined closely withrespect to psychosocial and physiological fac-tors, nor is it well established how support to the
•Portions of ihis paper were presented al ihe 5th Annual Scien-tific Sessions for Nursing of Ihe San Frantisco Hcari Association.February 1987 and the Sigma Theta Tau Internaiionul NursingResearch Meeting. July 1987.
Correspondence: Professor Susan R. Gortner. Room N411-Y.Department of Family Health Care Nursing. School of Nursing.University of California. San Francisco. California 94143. USA.
patient and family during the rehabilitativeperiod might be carried out.
Our work and that of others (Brown &Rawlinson 1977, 1976, La Mendola & Pelligrini1979. Pilowski et al. 1979. Silva 1979, Gortneretal. !980, 1982. Wilson-Barnett 1981, Zyzanski('/ al. 1981. Lovvorn 1982, Stanton et al. 1984.Gilliss 1984, Gilliss et al. 1985. Gortner et al.1984, 1985. Sikorski 1985. Nicklin 1986), hasindicated the need to provide anticipatoryguidance tor surgical treatment, lo examineexpectations and beliefs about treatment, and toprovide assistance in the convalescent period fol-lowing hospital discharge. Zyzanski et«/. (1981)suggest the need for patient education regardingrealistic surgical recovery expectations, andcounselling or therapy to reduce continued typeA behaviour. Stanton et al. (1984), reportingon a longitudinal study of recovery in elective
649

650 S. Gortner et at.
cardiac surgery, noted that patients at 6 monthsfelt they had been well prepared for exercise andactivity level and return to work but less wellprepared for physical and emotional symptoma-tology, over-protectiveness by family and sexualfunctioning.
The fact that heart surgery has an impact onthe family, especially the spouse, in ways thatmay be different from those of the patient hasonly recently been documented. Gilliss (1984)demonstrated higher subjective stress amongcardiac surgery spouses than among patients.Couples interviewed at 6 months reported thedisorganizing effect of the surgery on family lifeduring convalescence and the need for infor-mation and support during the period. Sikorski(1985) conducted interviews with 30 wives ofcoronary artery bypass patients during thesecond and third week of home convalescencethat revealed concerns about amount, type andlevel of activity, including resumption of workand sexual functioning, diet, medication, andsurgical results. These concerns also were con-veyed by spouses during the telephone monitor-ing we conducted with the experimental group inthis study (Gortner et al. 1985a). Silva (1979) hasdemonstrated that nursing intervention beforesurgery can reduce the stress of the spouse sig-nificantly in the postoperative period, as haveLinde & Janz (1979). We were interested indetermining whether nursing interventionspost-surgery in the hospital and during conva-lescence at home could provide assistance andcontinuity to patients and families in the recov-ery period. For a model of interventions welooked to the Stanford Cardiac RehabilitationProgramme.
Since 1983, DeBusk and his associates atStanford have been examining the value of earlyinterventions combining occupational workevaluation through treadmill performance, witha behavioural change programme for post-infarction males, who were formerly employed,and their spouses. The intervention is designedto enhance the perceived health status of thepatients, through employment ofthe seif-efficacymechanism in human learning (Bandura 1977,1982). For both patient and spouse, objectivemeasures of cardiac status, intensive counsellingand follow-up by telephone and questionnairesare provided (DeBusk er al. 1983, Fwart et al.1983). The counselling is primarily nurse-
rendered following the initial post-treadmillsession with the cardiologist.
With this model as background, we focusedon the following general questions. Was it poss-ible to adapt the post-infarction intervention(telephone monitoring and teaching films) forthe cardiac surgery patient and at the same timeprovide support to the spouse as the primarycaretaker? Would such a programme of antici-patory guidance and support significantlyinfluence recovery?
CONCEPTUAL FRAMEWORK
Two theoretical frameworks were employed toguide the experimental interventions used in thisstudy. The first was self-efficacy theory, a form ofsocial learning theory in which self-perceptionsof activity ('efficacy expectations') serve as im-portant determinants of subsequent behaviourand stress modification (Strecher el iiL 1986).Efficacy perceptions can be enhanced throughphysiological arousal, persuasive information,modelling, and actual performance (Bandura1986). It was expected that perceived efficacywould be enhanced through inpatient slide/tapeteaching programmes on individual recoveryand activity, diet, medications, risk factor reduc-tion and family coping, and reinforced throughintensive telephone monitoring up to the 8thweek of recovery.
The second major theoretical base for the in-terventions was that of family stress theory,specifically the Double ABCX Model, as expli-cated by McCubbin & Patterson (1983). In thismodel, family adaptation after crisis may beinfluenced by existing and new resources, thefamily's perception of the surgical event, concur-rent stressors, and family coping. The inpatientslide/taF>e teaching programme on family recov-ery was intended to modify the family's defi-nitions and perceptions before discharge and thetelephone monitoring to provide a new resource.Table 1 shows the intended impact of the studyinterventions on recovery.
Design and aims
A prospective randomized clinical trial was car-ried out over an 18-month period (August 1984to January 1986) for the purpose of testing the

Recovery following cardiac surgery 651
! ^ I
c
j i
t>E
lead
just
i
a.3o
U
cO
EuDUc
^c
p
ESIl
' ^ro
lic
uio
n of
ol
act
isX:̂
uhc
couD
l
'5
u
§ ^
2 | I
~ £•
3c;u
coco(5
reco
lem
s
g 2I
.-̂ fl V1 .S 2 i
.a .— , i o« • =
— r l
t B ^
•^ 3 .3
.JC
mco
1<zXc:q
<
3
3
Afi^
rho
ol
n
33
"UUJ
'ers
ily
'E
-•
an fo
r
V I
.2•3
£<=;Q\fi(0
rni
' 2 • -
•- "c
. 3
• ^
let
hook
3
£
o
'5
Uc
de/l.
c.2
11Ic,v
E
1<3O
:tio
n':
c
'Mo
vel
cJi<oE
'5
lurg
cr
L.,
w^ •
'our
h
ir
only
ft.
oat
^
.11
non
II
ii
•H
o
:To£
c
«,Eo
a
illi

652 S. Gortner et al.
FIGURE 1 Effects oJexperinwiitat interveniions on reiinery.
major hypothesis that persuasive recovery infor-mation and coaching by telephone would hastenpost-surgical rehabilitation. First-time cardiacsurgery patients and .spouses between the ages of30 and 75 undergoing coronary ariery bypassgrafting and/or valve replacement at threeNorthern California surgical centres {twouniversity and one community hospital) wereinvited to participate. Those consenting wererandomized before surgery to an experimentalor control group. Specific aims were threefold:1 to test the effectiveness of nursing inter-
ventions designed to improve post-hospitalrecovery and rehabilitation at home;
2 to assess the impact ofvalve replacement andbypass surgery on the health of the familyunit: and
3 to describe differences in recovery fromcoronary artery bypass surgery and valvereplacement surgery.
This paper will only address findings relative toaim I.
METHOD
Sampling criteria
All English-speaking patients entering the threestudy hospitals for first time CABG and/or valvereplacement surgery, between the ages of 30 and75 were considered eligible if they were marriedto a consenting spouse and were without other
major medical conditions. In actuality, the ageceiling was raised twice to admit a 76-year-oldand 77-year-old. For the calendar year 1984. thestudy was being carried out at two teachinghospitals; beginning in 19S5 a third site (acommunity hospital in close proximity to one ofthe teaching hospitals) agreed to participate.
Randumizalion plan
Consenting patient-spouse pairs were rando-mized prior to surgery to an experimental orcontrol group. These groups' assignments werekept blind to those inducting subjects, and onlybecame known after the sealed envelopes werebroken following ihe consent of patient andspouse to enter into the study.
The sequence of assignment from the random-ization plan was maintained through subjectaccrual and attrition. The plan worked suffi-ciently well that there were no baseline differ-ences between patients or spouses at the threestudy sites, except for an age-related finding forNYH functional class.
The interventions
Tbe interventions used in the study are shown inTable 1. Intervention 1 was employed in anattempt to standardize knowledge about cardiac

Recovery following cardiac surgery 653
risk factor reduction and recovery betweengroups. It consisted of a standard slide/tapeteaching programme developed by the AmericanHeart Association (1976) and was shown to bothexperimental and control subjects to encourageexercise, diet adherence and surgical recovery.Intervention II was the experimental slide/tapeteaching programme and counselling sessiondesigned to provide families with anticipatoryguidance on recovery at home and commonemotional responses in the immediate post-diseharge period. The slide/tape programme wasformatted after the American Heart Associationfilms and took 8 minutes to view. The counsell-ing session was held with patient and spouseimmediately after viewing the film.
Intervention III was intended to reinforce in-terventions I and II and to monitor patients andspouses to detect early signs of physical oremotional difficulties with recovery. In additionit was hypothesized that intervention III wouldaffect ihe reported level of self-efficacy over time.Telephone calls were carried out by masters- ordoctorally-prepared nurses who followed astructured protocol for data collection and whoindividualized calling to the needs of familymembers as necessary (i.e. teach, coach, refer).The previous week's efforts at problem resol-ution were reviewed on the next telephone call,and notes made on the semi-structured question-naire developed for use with intervention III.For the ."̂2 cases carried to the 6-month time,continuity was maintained by having the sameinterviewer call ihroughout the period, exceptwhen emergencies or illnesses prevented this.Ideally the person that carried out the inter-vention III fora given family was also the personwho had interviewed the family in the hospitalfor intervention II.
Procedures
Patients and their spouses were approached onthe day before surgery and invited to participatein the study. Preoperative measures of familyfunctioning (APGAR), family resources(FIRM), and marital satisfaction (MAS) werecollected from both patient and spouse. Patients"cardiac status preoperatively was obtained fromthe medical record, as was other demographicdata. Additionally, patients were asked to list the
benefits expected from surgery which then werecompared with those realized at 6 months to pro-vide a ratio of expected to realized benefits. Self-efficaey appraisal and self-reports of activitywere made by mail at 1 monlh for the experimen-tal group, and then at 3 and 6 months lor bothgroups. Family measures were evaluated againat 3 and 6 months, except for the M AS whieh wasre-evaluated at 6 months. Patient.s' mood state(POMS) was evaluated at 3 and 6 monihs. butnot at baseline.
All patients were provided with the hospitals'routine homegoing information, and saw one ormore of the intervention I inpatient slide/tapeprogrammes before discharge. Only the exper-imental group viewed intervention II, the slide/tape programme on family coping and conflictresolution. Only experimental subjects werefollowed hy telephone (intervention Ml) on aweekly ba.Kis for 4 weeks, and then biweekly for4weeks, to monitor recovery, reinforce risk factorreduction, and provide reassurance to spouse aswell as patient. Both experimental and controlsubjects were contacted at 3 months and 6months by telephone to obtain verbal reports ofrecovery, and both completed study instrumentsby mail.
Instruments
The telephone protocol for intervention IIIThis is a structured interview schedule developedby the authors. Although a variety of formatswere explored, an open-ended form was pre-ferred to allow for recording of patient andspouse concerns without directly eliciting symp-tomatology. The questionnaire was tested,revised, and subsequently finalized to include aback sheet to be completed by the interviewer,noting time taken for the interview, the eode,date ofthe interview, the particular problem ornursing diagnosis identified, and the nursinginterventions undertaken by the interviewer.
The family APGARThis is a five-item close-ended questionnairedeveloped by Smilkstein (1978) as a clinical toolfor the appraisal of family functioning. A singlequestion is asked regarding the family member'slevel of satisfaction with each of five areas:adaptability, partnership, growth, afTection and

654 5. Gorlner el at.
resolve. The instrument has eorrelatcd well withother valid measures of family functioning. Thefive-choice format is recommended for researchpurposes (Smilkstein et al. 1982). has an internalreliability of r^OHd and was well tolerated byour sample. Cronbach's alphas ranged from 0-83to 0-87.
The Family Inventory of Resources forManagement (FIRM)This is an index of the resources available lo thefamily (McCubbin et al. 1981). Conceptually.FIRM assesses four areas: personal resources,family internal resources, social supports andfinancial resources. For this administration thefinancial resources scale was deleted. Thereported Cronbach's alpha is /• = 0 89; reportedvalidity checks using the Moos FES havedemonstrated the expected significant corre-lations between presence of resources and highlevels of family functioning. Cronbach's alphasexceeded 0 89 in this administration of themodified FIRM.
Marital Adjustment Scale f MAS)The Locke-Wallace Marital Adjustment Scale isa 16-iteni Likert-type screening instrumentdesigned to measure marital adjustment byfocusing on marital conformity in decision-making. Internal reliability (r = 090) and evi-dence supporting validity have been reported byLocke & Wallace {!959}. Cronbach's alphasranged from 0 73 to 0 81 in our sample.
The realised benefits variableThis is the ratio of actualized benefits at 3 and 6months post-surgery to the presurgica! expectedbenefits. The importance ofthis indicator is thaiit represents for patients the anticipated out-comes of surgical treatment for cardiac diseasethat were realized. Previous work has shown thatthe area of'activity level* had the lowest 'realizedbenefits" ratio (Gortner et al. 1985b). Thus, wewanted to determine whether the interventionhad an impact on realized benefits.
Self-efficacy .scalesThe seif-efikacy measures used in the StandiordCardiac Rehabilitation programme for determi-nation of physical activity level, return lo workand diet compliance were made available to us.Self-efficacy asks for specific appraisal by the
patient of his or her confidence in and ability toexercise, resume activity und modify stress, usinga Gutlman scale response. Our internal reliabili-ties ranged from 0-58 toO-98at 12 weeksand 071to 0 96 at 24 weeks.
The self-reportThis allowed recording of actual risk factormanagement (diet, medication, exercise, smok-ing cessation), in contrast to the self-etticacyscales which anticipated the accomplishment ofrisk factor reduction and recovery. It was com-pleted by experimental subjects and returned bymail on a weekly basis for weeks one and twoimmediately post-discharge, and then at thefourth week, prior to the first clinic visit. Subse-quently, it was completed at 2 months. 3 monthsand 6 months. For 3- and 6-monih assessments,both experimental and control subjects weretelephoned and the self-report completed by theinterviewer.
The Profile of Mood States (POMS)This is a standardized. 65-item adjective ratingscale that measures six mood states: tension/anxiety, depression/dejection, anger/hostility,vigour/activity, confusion/bewilderment, andfatigue/inertia. It was developed by McNair eial. in 1971 and has been previously used wilhclinical populations, including a large survey ofMended Hearts participants (Jenkins et al.1983). It was used as a 'window" on depression at3 months in our sample. Cronbach's alphas inour study were highly satisfactory, ranging from0 80 to 0 92 at 12 weeks and 0 79 to 0 94 at 24weeks; these compare favourably with publishedalphas ofO 84 to 0 95.
RESULTS
Sample characteristics
Eighty-one persons expressed interest, and 79patients/spouses signed consents and were ran-domized. Of these 79 marital dyads. 10 coupleswere dropped or withdrew for the followingreasons: withdrawal within 2 weeks after signingconsent (one control and two experimental),early discharge (one experimental), dischargeagainst medical advice (one control), post-operative complications rendering participationimpossible (one experimental and one control).

Recovery following cardiac surgery 655
TABLE 2 Baseline %milarMes heiwecH conirot and rxprrimenial gruups' an intlifiduatvariables
St-x
MaleFemale
Type of surgeryCABGValveCombinaiion (vatve and CABG)
Age (yr)30-5051 6970 77
New York Heart .ixwi iiilinnFunttiiiiiatClasx tn = 6l)
]&U111 & IV
ICL' sta\ marc than 4 daysPumpumc imcanl
Controls
287
2465
22ft
7
239
7 (22%)*N 58 min
I'ixpenmenluls
2&6
2561
6224
2183 (10%»
97 07 min
*Nu differences were slulislically
and three pcrioperative death.s (three controls),f-ollowing discharge, two deaths occurredbefore the .^-month period in the experimentalgroup. Thus there was a 15% attrition rate at 3months. There were no additional losses between3 and 6 months.
Sixty-seven patients with a mean age of 61-5years participated in the study tliroughout the6-month period. .15 in thecontrol group and ?>2 inthe experimental group. Except where indicated,analyses were completed for ihis full sample of 32experimentals and 35 controls.
Sample characteristics are displayed in Table2. The sample was predominately Caucasian(88%), male (80%). and from managerial andprofessional occupations, (54%). Twelve percent were retired and an additional 13% werehomeniiikers. There were no statistically signifi-cant dilforences noted between control and ex-perimental patients forage, sex, type of surgery.New York Heart Association (NYHA) func-tional class, length of stay, and pump time. Therewere no statislically significant differences onfamily measures (APGAR. I-"1RM. MAS), asdisplayed in Table 3. As might be expected, thoseover 70 had more severe heart disease on NewVork Heart Association (NYHA) functionalcriteria.
Effect of interventions on individuul reeovery
It had been hypothesized that the experimentalinterventions would significantly hasten individ-ual recovery al 6 months. This hypothesis wasnot supported by the data. No significant differ-ences were found on self-report, self-etficacy andrealized benefits for the experimental versus thecontrol group al f» months. By Ihis time, mostpatients reported complete recovery; indeed,mean scores indicated that recovery had pro-gressed beyond levels reported at 3 months forboth groups. Results on the self-report showedthat activity scores for both experimental andcontrol subjects increased from 3 months to 6months, medication usage decreased for bothgroups, as did reported symptomatology andcomplications; significant differences were foundfor these variables between experimental andcontrol subjects.
Independent two-tailed /-tests were per-formed comparing the experimental and controlgroups at 3 months and 6 months on all self-efficacy activities. At 3 months there were twosignificant findings between the experimentaland control groups. Experimental subjects per-ceived greater self-efficacy for lifting objects(/ = 219, P = Q0^4) and controls perceived

656 S. Cornier et at.
TABLE5Bim'/;Hc i heiween lonirol anJ experimental groups on ramity nieasure,\
Controls Expcnincnlals
APGARPalienlsSpouses
MASPulienisSpouses
FIRMPatientsSptiu.ses
3435
3534
2832
17 OS1677
122 73
124 45
6446
67'31
047058
2'73
306
2-4H
256
313)
3029
2930
18 28
18 12
125 66
12773
6566
6540
0.17
0 38
398329
207t-91
greater ability to tolerate emotional distress andanger (/ = 2-90. / ' -0007). Confidence inlervalsfor all differences in mean eflicacy scores at 3 and6 months are displayed in Table 4.
Although it is apparent that both groupsincreased their mean strength self-efficacy scoresover time, the confidence intervals suggest atrend in favour of higher perceived activity andwork resumption scores for the experimentalgroup at 3 months. By 6 months confidence in-tervals were not as large as at 3 months, and therewere no other significant differences on any ofthe perceived efficacy behaviours. There were nosignificant treatment group by time interactions,except for the variable of age. This findingimplies that the patterns of self-efficacy percep-tions from 3 to 6 months time were similar forboth groups.
Pearson product moment correlations wereused to assess the hypothesized relationshipbetween perceived self-efficacy and activity level.Perceived effieacy for walking, general exertion,climbing, driving, and work capability corre-lated significantly with the corre.sponding self-reported activities at 4 weeks (experimental sub-jects only), with correlations ranging from ()-5lto 0-65, On the ratio of expected lo realizedbenefits from surgery at 6 months, there were nosignificant differences between the experimentaland control groups. Thus there is no evidencethat the experimental interventions aided recov-ery at 6 months and only a suggestion that theinterventions may have been influential at 3months on efficacy expectations. There was noevidence that age. gender and preoperative
cardiac status were significant treatment effectmodifiers at 3 and 6 months.
Other Tactors influencing individual recovery
To examine the influence of other variables onindividual recovery, a cohort analysis was car-ried out combining treatment groups (in order toincrease sample size). Several factors appear toinfluence individual recovery, notably preopera-tive cardiac status, age and gender. With regardto efficacy expectations, higher perceived effi-eacy for climbing and for interactions withothers at work were reported by patients withbetter baseline cardiac functional status (NYH Acardiac functional class 1 and II).
Analyses of variables by age revealed thatelders (the over-70 group) significantly increasedtheir perceived efficacy of general exertionbetween 3 and 6 months, whereas those in theunder-50groupsignificantlydecreased theirs. Bycontrast, there were no statistically significantdifferences in self-reported activity between theagcgroups(3i 50, 5l-69and 70 77) on analysisof variance between 3 and 6 months. Significantdifferences in realized benefits were found againfor age (the over-70 group reported 95% of theirexpected benefits achieved at 6 months in con-trast to the under-50 group wiih 59% achieved;/' = 0050). Two mood state subscales on thePOMS hostility and depression, significantly dif-ferentiated age cohorts, with those under 50reporting significantly more such states thanthose over 70. Table 5 displays these data. Note

Recovery following cardiac surgery 657
TABLE 4 95% confidence intervals showing experimenlal and coriirol mean differences on perceivedefficacy for 3 and 6 month aciiviiv
Perceived cHiciiL-y IZ-C difference 95% contidente inlcrvu!
Wulkisig 3 moiUhsWalking 6 monlhsClimbing 3 monlhsClimbing 6 monthsLifting 3 monthsLifting 6 monthsGeneral exertion 3 monthsGeneral exertion 6 monthsTime spenl at work 3 monthsTime spent at work 6 monthsInteraction at work 3 monthsInteraction at work 6 monlhsMeal preparation 3 monthsMeal preparation 6 monthsFor following diet 3 monthsFor following diet 6 monthsFor following diet al
all meals 3 monlhsFor Tollowingdietat
all meals 6 monthsEmotional distress
tolerance 3 monlhsEmotionaidisiress
tolerance 6 months
0801-448-632-58
15-8I*9-309-28
-0-503-75
-5-56609
-8-12- 5 47- 7 94- 3 1 2
311
10'60
-4-66
17 2 8 "
- 6 7 1
{-12-67.( -8'24,( -4 '37,( - 9 8 1 ,( 123.( -5-38,( -2-43,(-1331.(-22-48.(-25 69,(-17-69.(-28-73.(-19 54,(-19-82.(-n.99.( -8-96.
(-10.91.
( -20 86.
{- 29-60.
(-21-05.
14-27)11-12)2163)14-97)30-40)23-99)20-99)1231)29-98)14-58)2987)12-49)6 60)4 39)5-75)
1518)
32-11)
11-54)
-4-95)
7-63)
*/- = 0-034,• *P=0-007.
TABLE 5 Age as a mediator for individuid recovery al 6 i
Recovery variahle
Mood Slates Stihscalc(means and number reporting)
HostilityDepression
Realized henefitsPercenlage of benefils realized
31-50(. = 8)
15-00 (" = 3)13-00 {n = 3)
59
Age (yr)
51-69(.=48)
4-55 {« = 33)6-46 ("-32)
79
70-77( .= 11)
2-30* («=IO)4-40 (n = IO)
95**
•F=5-70,/' = 0-006,"f=3-14, P=0-05.
that the small number of under-50 subjectscompleting the POMS at 6 months compromisesthis finding.
Significant differences were found for realizedhencfits between men and women at 3 and 6months, with the ratios of reahzed to expected
benefits for men (77% and 85%) significantlyhigher than those for women (41% and 54%),P - 0 0 0 2 and P = 0023. No significant corre-lations were found between basehne NYHfunctional status or anginal class and realizedbenefits at 6 months.
658 S. Gorlner et al.
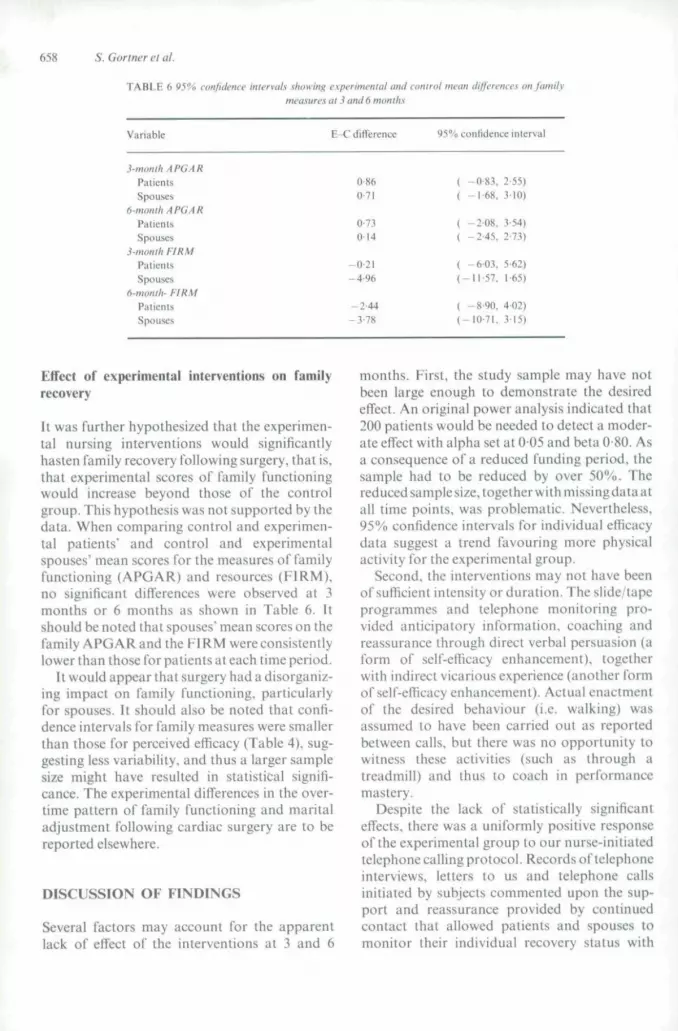
TABt.E 6 95% confidence interval."! .showing e.xperimenial anil control mean differencea on familymeasures a( 3 and6 months
Viiriahle E -C ditterencc 45"« conrnJeTicc interval
3-month A PGA RPatientsSpouses
6-montliAPGARPalicntsSpouses
3-monili FIRMPiitientsSpouses
6-monih-- FIRMPalienlsSpouses
0-860-71
0-730-14
-0-21- 4 %
-2-44-3-78
( -0-83, 2-55)( -1-68. .110)
( -2-08, 3-54)( -2 '45 . 2-73)
( -6 '03 , 5-62)(-11-57. 1-65)
( -8-90. 4-02)(-10-71. 315)
Effect of experimental interventions on familyrecovery
It was further hypothesized that the experimen-tal nursing interventions would significantlyhasten family recovery following surgery, that is.that experimental scores of family functioningwould iticrease beyond those of the controlgroup. This hypothesis was not supported by thedata. When comparing control and experimen-tal patients' and control and experimentalspouses' mean scores for the measures of familyfunctioning (APGAR) and resources (FIRM),no significant differences were observed at 3months or 6 months as shown in Table 6. Itshould be noted that spouses' mean scores on thefamily APGAR and the FIRM were consistentlylower than those for patients at each time period.
It would appear that surgery had a disorganiz-ing impact on family functioning, particularlyfor spouses. It should also be noted that confi-dence intervals for family measures were smallerthan those for perceived efficacy (Table 4). sug-gesting less variability, and thus a larger samplesize might have resulted in statistical signifi-cance. The experimental differences in the over-time pattern of family functioning and maritaladjustment following cardiac surgery are to bereported elsewhere.
DISCUSSION OF FINDINGS
Several factors may account for the apparentlack of effect of the interventions at 3 and 6
months. First, the study sample may have notbeen large enough to demonstrate the desiredeffect. An original power analysis indicated that200 patients would be needed to detect a moder-ate effect with alpha set at 0 05 and beta 0-80. Asa consequence of a reduced funding period, thesample had to be reduced by over 50%. Thereduced satiiple size, togetherwithmissingdata atall time points, was problematic. Nevertheless,95% confidence intervals for individual efficacydata suggest a trend favouring more physicalactivity for the experimental group.
Second, the interventions may not have beenof sufficient intensity or duration. The slide/tapeprogrammes and telephone monitoring pro-vided anticipatory information, coaching andreassurance through direct verbal persuasion {aform of seli'-efficacy enhancement), togetherwith indirect vicarious experience (another formof self-efficacy enhancement). Actual enacttnentof the desired behaviour (i.e. walking) wasassumed to have been carried out as reportedbetween calls, but there was no opportunity towitness these activities (such as through atreadmill) and thus to coach in performancemastery.
Despite the lack of statistically significanteffects, there was a uniformly positive responseof the experimental group to our nurse-initiatedtelephone calling protocol. Records of telephoneinterviews, letters to us and telephone callsinitiated by subjects commented upon the sup-port and reassurance provided by continuedcontact that allowed patients and spouses tomonitor their individual recovery status with

Recovery followmg cardiac surgery 659
guidance. Spouses frequently commented thatealls allowed them to iet out" their fears andfrustrations, especially when complications de-veloped that protracted recovery. One spousewrote. \ .. am very grateful to have had you tocall that day as I was very worried; the pro-gramme for support and follow-up is a blessing',Many subjects eommented that study formscould not tell the complete story ofthe difficultprocess of recovery. Not all recovered; one wroteshortly before his death:
the mosl imporlatit role you assumed (during our hos-piializations) was that of liaison between palient.spouse, and hospital staff. No matter what problemsdeveloped you were available to help. Cheerfulnessand understanding were of great comfort; talking withus gave us a better understanding of how to deal withthe boredom, pain and discouragement
This last was particularly meaningful becauseof initial scepticism by this subject (a healthprofessional), regarding the value of the study.
A final factor is that our appraisal schedule of3 and 6 months may be inappropriate for indi-vidual recovery. Although natural patterns offamily recovery were detected, our intervals weretoo late for the appraisal of individual recovery.The most rapid gains in surgical recovery occurduring the first 6 weeks, judging from efficacyperceptions and self-reports of activity. By then,most individuals resume presurgical activitylevels. Thus, our measurement battery came toolate to pick up these gains and as a result of thedesign we have no data for controls during thiscritical period.
Regarding the family's experience, our datasuggest that spouses focus on patients duringearly recovery. This distracts family membersfrom familial concerns and frustrations, whichcontinue to accumulate to between 2 weeks and 3months. We need to ask: When is interventionmost beneficial? Is intervention actually requiredbeyond 3 months to effect the desired changes infamily health as measured by spouse reports?Should the treatment be more intensive? Shouldit be more selectively directed to high riskfamilies?
CONCLUSION
This 18-month study serves as a pilot ofa largerintervention trial now underway (Gilliss et al.
1986). In this respeet. progress was madetowards all the major aims ofthe study. More isgenerally known about individual recovery thanis known about family recovery after an episodicsituation such as cardiac surgery. There is asuggestion that the coaching may have been help-ful for earlier individual recovery, particularlywith regard to the enhancement of self-efficacy.It is important now to move the instru-mentation for efficacy appraisal up to thedramatic recovery period (i.e. within the earlyweeks post-surgery).
The relationship of family dynamics toindividual recovery and the impact of individualrecovery on family dynamics continues to be amajor research issue. It is clear from our datathat the individual patient's needs, primarilythose of physical recovery, are the focus ofconcern in the first few weeks, if not months, ofrecovery. The primary caregiver. i.e. the spouse,is irrevocably caught up with aspeets of physicaland emotional recovery for his or her spouse.Thus, it is a complex undertaking to plan simul-taneous interventions to hasten both individualand family recovery.
Acknowledgements
This work was supported by research grant1R01-NU1031 from the Division ofNursing,United States Department of Health andHuman Services, to Susan R. Gortner for theperiod I August 1984 to 31 January 1986. Theco-investigators were Catherine L. Gilliss,Patricia A. Sparacino and Julie A. Shinn. theproject statistician was Mark Hudes and theresearch assistants were Sally Rankin. MaribelleLeavitt and Martha Price.
We gratefully acknowledge the assistance ofstudyconsuhants: Stephen Hulleyofthe Univer-sity of California, San Francisco; StephenZyzanski of Case Western Reserve University;and Nancy Houston-Miller. C. Barr Taylor andAlbert Bandura of Stanford University. We areindebted to Steven Paul for additional statisticalanalyses, to Walter Hauck for editorial commentand to Ira Kulkin for manuscript finalization.The cardiac surgery services of Sequoia Hospital,Stanford University Hospital and the MedicalCenter of the University of California, SanFrancisco referred patients for this project; to

660 S. Conner el al.
those patients and spouses who completed thestudy tools over time we extend special thanks.
References
American Heart Association (1976) An Aelive Piirinership for theHeallh of Your Heart. American Heart Association. Dallas.
Bundura A. (1977) Sell-efficacy: lowiirii a unifying theory ofbehavioral change. Psvcholofiiial Kevinv 84(3). 191-215.
Bandura A. (1982) Self-efficacy mechanism in human agency.American PsychologLu 37(2). 122 147.
Bundura A. (1986) Social Foundation of Thought und Action: ASocial Cognilive Theory. Prenlice Hall. Englewood Chffs.
Brown J. & Rawlinsiin M. (1977) Sex dilTerences in sick rolebehavior and work performance following cardiac surgery.Journal of Heallh and Social Behavior 18, 276-292.
Brown J. & Rawlinson M. (1976) The morale of palients followingopenhean^uTg/ery. JournatofHeailhand Social Behariorll,134 144.
Cohen J. (1977) Statistical Power Analysis for the BehavioralSciences. Academic Press, New York.
DeBusk R.F., principal investigator (1983) Occupational WorkEvaluation soon after Heart Attack. Research study fundedby National Heart. Lung, and Blood Institute (HLI8907),Stanford LJniversity. Stanford, California.
Ewart C.K.. Taylor C.B.. Reese L.B. & DeBusk R.F. (19H3)Theeffects of early post-infarction exercise testing on self-perception and subsequent pbysical activity. AmericanJournal of Cardiology 51, 1076-IOHO.
GillissC (19S4) Redudnj; family stress during and after coronaryartery bypass surgery. Nursing Clinics of North America19(1), 103- 112.
GillissC, Sparacino P., Gortner S.R. & Ketineth H. (1985) Eventsleading to treatment of coronary artery disease; implicationsfor nursingcare. Heart and Lung 14, .150 356.
Gortner S.R., Shortridge L., Baldwin A. & Sparacino P. (1980)Etbical influences on family decisions regarding election oftreatment. In Ethical Dimensions of Nursing Research. Pro-ceedings of the First Annual Scholarly Nursing LeadershipConference. University of Maryland School of Nursing,Baltimore.
Gortner S.R.. Sparacino P. & Gilliss C.L, (1982) Values, decisionfactors and stress in the choice of medical and surgicaltreatment in coronary ariery disease. Proceedings of theinternational Conference on Nursing Research. University ofF.dinburgh. Edinburgh.
Gortner S.R. Hudes M. & Zyzanski S.J. (1984) The appraisal ofvalues in the choice of treatment. Nursing Research 33,319-324.
Gortner S.R., Price M.. Rankin S.H.. Leavitt M. & C.iltiss C.L.(1985) After cardiac surgery: monitoring recovery bytelephone. American Heart Association Abstract K339.Circulation 12, IW-n-
Gortner S.R., Gilliss C.L.. Moran J.A., Sparacino P. & KennethH. (1985) Expected and realised benefits from coronaryartery bypass surgery. Curdioyascular Nursing 21, I.VI8.
Jenkins CD. , Stanton B.A., Savageau J A.. Denlinger P. & KleinM.D. (1983) Coronary artery bypass surgery. Physical.psychological, social and economic outcomes six monthslater. Journul of the American Medical Associuiion 250(6).782 788.
Jenson R.L.. Claylon P.D. & Liddle H.V. (1982) Relationshipbetween graft patency, post-operative work status and symp-tomatic relief. Journul of Thoracic and Cardiovascular Stir-S('M'83, 503-511.
t a Mendola W. & Pelligrini R. (1979) Quality ofiife and coronaryartery bypass surgery patients. Soeial Seienee and Medicine13». 457-461.
Linde BJ. & Janz N.M. (1979) Effect ofa teaching program onknowledge and compliance of cardiac patients. NursingResearch 25,{5).2'A2 286.
Locke H. & Wallace K. (1959) Short marital adjustment andprediction tests; their reliability and validity. Marriage andFondly Living 21, 251 255.
Lovvorn J. (1982) Coronary ahery bypass surgery: helpingpatients cope with postop problems. Atnericait Journal ofNur.'iingi2. 1073 1075.
McCubbinH.,Comeau J.K. AHarkins J.A. (1981 )/••//(,«/•".«'(//>•tnieiitory of Resources for Management. Family HealthProgram Form B. Department of Family Social Science,University of Minnesota. St Paul. Minnesota.
McCubbin H. & Patterson J. (1983) Family transitions; adap-tation to stress. In Stress and ihe Family. Vol. I Coping withNormative Transitions (McCubin H.L & Figley C.R. eds),Bruner.'Maze I, New York.
Mclntosh H.D. (1981) Overviev,' of Aorlocoronary BypassGrafting for the Treatment of Coronary Ariery Disease: AnInternist's Perspective. NCHCT Monograpb Series. USDepartment of Health and Human Services. Ofiice ofHealth Research Statistics and Technology, Rockville,Maryland.
McNair D.M., Lorr M. & Droppleman L.F. (1971) Profile ofMood States Manual. Educational and Industrial TestingService, San Diego, Califomia.
Miller D C , Stinson E.B., Oyer P.E.. Jameson S.W., MitchellR.S., Reitz B.A., Vavingartner W.A. & Shumway N.E,(1983) Discriminant analysis ofthe changing risks of coron-ary artery operations; 1971 1979. Journal of Thoracic ant/Cardiovascular Surgery 95,197-213.
Nicklin W. McK. (1986) Post discharge concerns of cardiacpatients as presented via a telephone callback system. Heartondt.Migl5iy).2bS 272.
Pilowsky L.SpenceN.D.& Waddy J.L.(1979) Illness behavior andcoronary artery bypass surgery. Jourmd o/ PsyihosontaiicResearch 23. 39-44.
RahimtooiaS., GrunkmeierG., TeplyJ, Lambert L., Thomas D..Suen Y-F- & Starr A. (198!) Changes in coronary bypasssurgery leading to improved survival. Journal o/ the .AmericanMedical Association 246( 17), i 912-191 ft.
Rahimtoola S. (1982) Coronary bypass surgery for chronicangina — a perspective. Circulation b5i2). 225 -241.
Sikorski J.M. (1985) Knowledge, concerns, and questions of wivesof convalescent coronary artery bypass graft surgerypatients. Journal of Cardiac Rehahilitation 5, 74-85.
Silva M. (1979) Effects of orientation information on spouses'anxieties and attitudes towards bospitalization and surgery.Researeh in Nursing and Health 2, 127-136.
SmilksteinG.( 1978) The family APGAR: a proposal for a familyfunction test and its use by physicians. Journat of Famity/'rai7((p6(6), 1231 1239.
Smilkstein G.. Ashworth C, & Montano D. (1982) Validity andreliability ofthe family APGAR as a test of family function.The Journal of Family Fraciice\5(2).y(il>-y\\.
Stanford J. (1982) Who profits from coronary artery bypasssurgery? American Journal oJ NtirsingSlO). 1068 1072,
Stanton B.A., Jenkins CD. , Savageau J.A., Harken D.E. &Aucoin R. (1984) Perceived adequacy of patient educationand fears anil adjustments after cardiac surgery. Heart and
Strecher V.J., DeVellis B.M., Becker M H & Rosenstock LM.(1986) Tbe role of self-efficacy in achieving health behaviorchange. Health Education Quarterly 13, 73 91.
Taylor C B , Bandura A., Ewar C K , Miller N.H. & Debusk RL(1985) Exercise testing to enhance wives' confidence in theirhusbands" cardiac capability after clinically uncomplicatedacute myocardial infarction. American Journal of Cardiology55,635-638.
Western Center for Health Planning (1981) Evatuating MedicalEfficacy: Coronary Artery Bypass Surgery us an Example

Recovery folhwing cardiac surgery 661
(Technical Assistance Memo - 60). Bureau of Health Zyzanski S.J.. Stanton B.A.. Jenkins C D . & Klein M.D, (1981)Planning, Springfield, Virginia. Medical and psychosocial outcomes in survivors of major
Wilson-Barnett J. (1981) Assessment of recovery: with special heart surgery. Journal of Psycho.tomaiic Researeh 23(3),reference to a study with post-operative cardiac patients. 213-221.Journal of Advanced Nursing 6(b). 4i5-445.

















![[[Hypnosedation, a new method of anesthesia for cervical endocrine surgery. Prospective randomized study]](https://img.dokumen.tips/doc/110x75/6349422a7442d262850f71c2/hypnosedation-a-new-method-of-anesthesia-for-cervical-endocrine-surgery-prospective.jpg)












