Embed Size (px)
Citation preview

LUNG CANCER
ELSEVIER Lung cancer 12 Suppl. I (1995) s59+s70
Mutated K-ras gene analysis in a randomized trial of preoperative chemotherapy plus surgery versus
surgery in Stage IIIA non-small cell lung cancer
Rafael Resell*“, Francisco Molina”, Isabel Moreno”, Eva Martinez”, Alex Pifarr?, Albert Fontb, Shanrong Lib, Zdenek Skacelb,
Jo& G6mez-Codina”, Carlos Camp@, Mariano Monz6”, Josep M. de Anta”
“Depurtmmt oj’ Mrdicul Oncology, Unicrrsit~~ of Barcelona, Hospital Germans Trtas i Pujol, Box 72, 08916 Badalona, Barcelona. Spain
hPnrumological Clinic. Prague, Czech Republic
‘Department of Medical Oncology, Hospital ‘La Fe’ Valencia. Valenria, Spain ‘Department of Medical Oncology. Hospital General. Valencia, Spain
Abstract
The observation that the proteins encoded by rus genes play a central role in the signalling pathways used by cells to respond to growth factors and the fact that mutated ras proteins are constantly promoting cell division have led to a PCR-based hunt for additional clinical information. In the present study, K-ras analysis draws the following conclusions: (1) K-ras point mutation frequency was higher in the surgery group (IO of 24 patients) than in the chemotherapy-surgery group (3 of 20 patients). (2) Mutated K-rus was predominantly observed at codon 12 but five mutations appeared at codon 61. (3) Mutations were identified in the squamous cell carcinoma histological NSCLC subtype except in four cases corre- sponding to adenocarcinoma. (4) A multifarious pattern of substitutions, especially at codon 12, were noted with aspartic K 12 substitutions more prone to develop bone metastases. (5) Although a genotypic K-rus classification of NSCLC may not yet be formulated, our accumulated data (unpublished) suggest a trend toward it. (6) Patients with mutated K-ras tumors in the surgery group had no different survival than those with normal K-ras. However our pooled data as well as other authors’ results assert that mutated K-ras constitute an additional prognostic datum that deserves to be included together with TNM classification. In the design of new preoperative (neoadjuvant) chemotherapy trials, stratifica- tion of tumors by K-ms status deserves to be further investigated in order to correlate with response, relapse and survival. Mutated K-ras genotype merits further research. Finally. the
* Corresponding Author, Tel.: + 34 3 4650409; Fax: + 34 3 3954206
0169-50021’95/$09.50 0 1995 Elsevier Science Ireland Ltd. All rights reserved
SSDI 0 169-5002(95)0042 I -V

S60 R. Rmell et al. : Lung Cmcrr I2 SuppI. I (1995) s59-s70
paradigm of uneven histological distribution and mutated K-ru.y spectra among researchers should serve as a stimulus to search for further contributions in this field.
Keywords: K-ras mutations; Preoperative chemotherapy; Non-small cell lung cancer; K-ras genotypes
1. Introduction
The accumulation of multiple mutations in proto-oncogenes and tumor suppressor genes in the course of human malignancies has been extensively described. Consistent with this, a number of proto-oncogene abnormalities have been found in non-small cell lung cancer (NSCLC), among them K-ras point mutations have been identified. The mammalian ras genes encode guanosine triphosphate (GTP)-binding proteins that can acquire the potential to transform mammalian cells as a result of point mutations in codons 12, 13 or 61 [l]. Ras proteins normally respond to growth stimuli, such as epidermal and platelet-derived growth factors by exchanging guanosine triphosphate (GTP) for constitutively bound guanosine diphosphate (GDP) thereby triggering cell division. The signal is terminated when the ras protein hydrolyzes its bound GTP to GDP in a reaction that is stimulated by a guanosine triphosphatase (GTPase) activating protein (GAP) [2,3]. Oncogenic ras proteins are found in several human cancers; about 50% in colon carcinomas and 90% in pancreatic carcinomas [4,5]. These findings underline the importance of ras functions in the pathogenesis of cancers and the potential usefulness of anticancer drugs to combat ras-induced cell transformation [2,3]. Furthermore, ras oncogene activation can precede the onset of cancer as has been proven in rat carcinogenesis; rats neonatally treated with a single injection of nitromethylurea harbor latent activated ras oncogenes in phenotypically normal mammary epithelial cells [6]. Similarly the presence of activated K-ras oncogenes in adenocarcinomas from former smokers abstinent for more than 15 years suggest that ras mutations happen precociously in the multistep process leading to lung cancer [7].
Mutated ras genes are detected in about one third of human NSCLC usually in K-rm codon 12, their presence correlating negatively with survival [8,9]. In spite of the wealth of information generated during the last 2 years on mutated K-ras [lo- 141, there are still multiple issues that need to be addressed. In our previous exper- ience while it was proven that patients harboring mutated K-ras had a worse outcome than those with wild K-ras, some dissimilarities came out when compared with Dutch results [ 10,111. Two important issues emerged, firstly K-ras positive tumors were not exclusively clustered in codon 12, but also in codon 61 and secondly, and most importantly, the vast majority of K-ras point mutations were present in squamous cell carcinoma as opposed to adenocarcinoma as observed by Dutch researchers.
In addition to these central issues, there are many other fundamental questions that require answers. To date, one of the main obstacles in understanding preoper- ative chemotherapy effect in Stage IIIA NSCLC has been the lack of molecular tools and their putative prognostic value. The TNM classification, while proving

R. Rose11 et al. : Lung Cancer 12 Suppl. I (1995) S59-S70 S61
useful in defining the subset of patients suitable for chemotherapy, does not take into account other meaningful molecular parameters. Histologic subtype by itself should no longer be considered a stratifying parameter since tumor size gives more precise knowledge of tumor burden. The presence of mutated K-ras may turn out to be a more definitive prognostic factor.
Additional questions to be clarified are: Could preoperative chemotherapy re- verse mutated K-ras phenotype as examined in postchemotherapy residual tumor resected specimens? Can a genotypic classification be established in order to define more aggressive mutated K-ras forms? To provide further evidence on the above mentioned issues, we performed molecular analyses of 44 out of 60 Stage IIIA NSCLC patients who entered in a randomized trial of preoperative chemotherapy followed by surgery versus surgery and whose tumors were completely removed by radical surgery.
2. Material and methods
All the patients studied underwent radical surgery between February 1990 and July 1991. Patients with histologically proven NSCLC and demonstrated Stage IIIA disease were accrued in three different participating centers. Patients were randomly assigned to receive either immediate surgery or three preoperative cycles of MIC chemotherapy composed of mitomycin 6 mg per square meter of body-surface area, ifosfamide 3 g m -’ over 3 h mixed with mesna 1 g m ~’ and cisplatin 50 mg m ~ ‘, all given intravenously. Additional mesna and hydration were given as scheduled by Cullen et al. [15]. Chemotherapy was given every 3 weeks.
Striking clinical differences between the two treatment groups prompted us to perform interim analyses [16] which disclosed that the difference in survival had reached a level significant enough to bring patient accrual to a close. Thirty patients were assigned to preoperative MIC chemotherapy and 30 to immediate surgery. Demographic characteristics are fully described elsewhere [17]. Twenty-five of 30 patients in the chemotherapy-surgery group had N2 disease as compared with 19 of 30 patients in the surgery group.
On the chemotherapy arm, 16 patients (53%) had radiological partial response, two patients (7%) had complete response, 11 patients were deemed to have stable disease and only one patient developed progression. Two responders refused to undergo surgery. Twenty-three of 27 patients in the MIC chemotherapy group underwent complete resection. The remaining four patients were found to be unresectable secondary to great vessel encasement. In the surgery group, 27 of 30 patients had complete resection. One patient had complete histological response following induction MIC chemotherapy and a further four had microscopic foci in lymph nodes without traces of primary tumor.
Significant differences between the two groups were recorded in event-free survival and overall survival. Median event-free survival in surgery group was 5 months (447 months 95% confidence interval) as compared with 20 months (12 months lower one-sided 95% confidence interval) in preoperative MIC chemother- apy group (P < 0.001). Median overall survival in surgery group was 8 months
S62 R. Rose0 et al. / Lung Cancer 12 Suppl. I (1995) S59-S70
(7-10 months 95% confidence interval) as compared with 26 months (16 months lower one-sided 95% confidence interval) in preoperative MIC chemotherapy group (P < 0.001). Sloan-Kettering experience confirms the favourable impact of induc- tion chemotherapy in the setting of Stage IIIA NSCLC patients [18] as well as another similar randomized study [ 191.
3. Results
3. I. K-ras gene ussesment in resected Stage IIIA NSCLC DNA from 44 patients was successfully amplified by means of polymerase chain
reaction (PCR). DNA was isolated from formalin-fixed paraffin-embedded tissue blocks. Oligonucleotide primers were synthesized according to the sequence data of the K-ras gene. Amplified DNA fragments which flanked codons 12, 13 and 61 were identified in ethidium bromide agarose gel after PCR (Fig. 1). Amplified PCRed DNA products were dotted on nylon membranes and hybridized to radioactively labelled oligonucleotide probes for codons 12, 13 and 61. The experimental details of the method were performed as described elsewhere [14]. Mutated K-ms genes were found in three of 20 patients (15%) in the chemotherapy- surgery group as opposed to 10 of 24 (42%) in the surgery group (P = 0.05) (Table 1). In the latter, the wild-type DNA sequence GGT at codon 12 was switched to GAT encoding aspartic in three cases and a further three harbored GTT encoding valine with two TGT switching from wild glycine to cysteine. The remaining two tumors contained mutations at codon 61 as well as the three cases in the chemotherapy-surgery group.
Fig. 1

R. Rosell rt al. / Lung Cancer 12 Suppl. 1 (1995) S59-S70 S63
Table 1 Mutation of K-ras gene in Stage IIIA non-small cell lung cancer randomized trial
Group Mutation
Preoperative MIC group Gln6’ + Arg6’ Gin” + Arg6’ Gln6’ + Glu6’
Surgery group Gly’Z + Asp” Gly” + CyP Gly’2 + Asp” Gly’2 + Val12 Gln6’ --* Lys6’ Gly” + Val’* Gly” + Val” Gly’Z -+ Asp” Gly” + Cys” GW’ + Lys”
Histological subtype, relapse pattern and survival from these 10 surgically-treated patients whose tumors contained K-ras are depicted in Table 2. Only one patient with glycine 12 valine substitution is still alive at 2 years of follow-up. The remainder had distant metastases corresponding mainly to glycine 12 aspartic and glycine 12 cysteine substitutions, while glycine 12 valine and glycine 12 lysine tend to local relapse only. Two of the three patients who received MIC chemotherapy had arginine substitutions at codon 61 and the third glutamine. Relevant was the fact that the two patients containing the arginine substitution at codon 61 had no objective response with one dying of locoregional disease and the other developing brain metastases at 21 months of follow-up and dying 5 months later. Histology in all three instances was squamous cell carcinoma. Table 2 describes the histology of the 10 patients whose tumors had mutated K12 Y(IS gene in the surgery alone group. Six were squamous cell carcinoma and the remaining four were adenocarcinoma.
Table 2 Characteristics of mutated K-ruS tumors in surgery group
Mutation Histology subtype Local relapse Distant Survival
Aspartic” Aspartic” Aspartic12 Valine” Valine” Valine” Cysteine” Cysteine” Lysine6’ Lysine”
Squamous Adenocarcinoma Squamous Squamous Squamous Adenocarcinoma Squamous Adenocarcinoma Squamous Adenocarcinoma
Liver metastases Bone metastases Bone metastases
Lung metastases Lung metastases Cervical lymph node
10 7 8
20 16 24 + 23 10 15 3

S64 R. Rose11 et al. : Lung Cuncer 12 Suppl. 1 (1995) S59-S70
Fig. 2.
Figs. 2 and 3 show histological examples of squamous cell carcinoma and adeno- carcinoma, respectively. Figure 4 shows an example of hybridizations with probes for codon 12 glycine (wild-type. GGT). Fig. 5 illustrates two samples positive for aspartic acid; row 1 column 1 and row 3 column 7. In row 4 columns 1 and 4, there are two positive controls. Fig. 6 depicts one positive mutation for cysteine: row 2 column 3. Below, are two positive controls.
4. Discussion
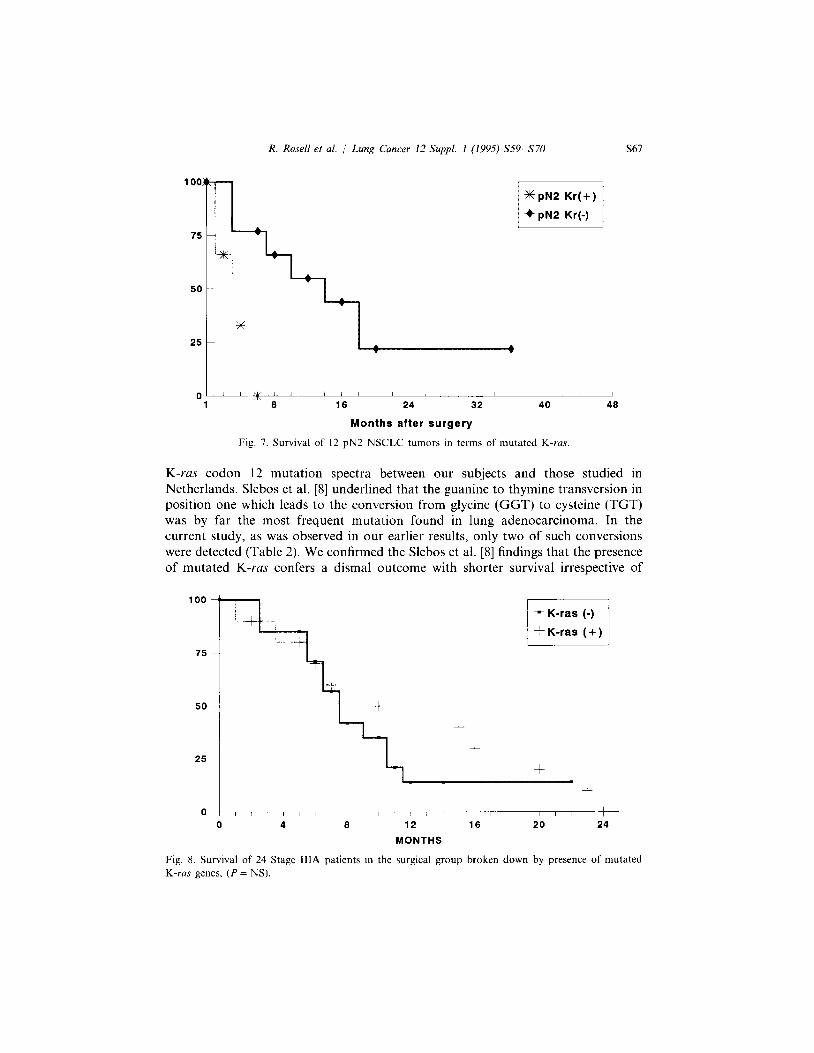
Patients harboring K-ras positive tumors constitute a NSCLC subset which portend a poorer response rate and survival regardless of stage, as has been seen in patients with either early or late stage [8,9,14]. Our previous results point to the presence of mutated K-ms gene in 20% of surgically resected NSCLC with the K-ras point-mutation subset having poorer survival. The difference was also confirmed in the small N2 group (microscopic N2 disease) where median survival time was 15 months for nine K-rus negative tumors in contrast to 5 months for three cases with K-ras positive tumors (P = 0.007) [14] (Fig. 7). Paradoxically in the present study when survival of the 24 completely resected patients in the surgery is broken down by presence of mutated K-rm gene, the difference was not significant (Fig. 8). This discrepancy may be explained in part by the fact that bulky disease (large tumor size, and clinically detectable N2 disease) is in itself an unfavourable prognostic factor in comparison with microscopic mediastinal metastases discov- ered at the time of surgery. In contradiction to other authors’ findings [20] that only

R. Resell ef al. : Lung Canwr 12 Suppl. I (1995) S59%S70 S65
Fig. 3
8% of K-vus point mutations occur in squamous cell carcinoma of the lung as compared with 24% in adenocarcinoma, our prior experience has shown us an overall prevalence of MS mutations in 13 of 66 surgically treated non-small cell lung cancer (20%). The predominant histological subtype in which mutated K-ras was found was squamous cell carcinoma, as in the present series. Since the first Dutch
Fig. 4
S66
Fig. 5.
study was published in which mutated K-ras was identified in five of 35 NSCLC specimens (five of 10 adenocarcinomas), Dutch researchers [21], have identified K-ras point mutations almost exclusively in codon 12 (93%) and overwhelmingly in the adenocarcinoma histological subtype [7,8,10,11]. Our data are more in keeping with those of Mitsudomi et al. [12] who examined 61 NSCLC cell lines in which TUS mutations were found in 22 cells lines including adenocarcinoma (28%) as well as squamous cell carcinoma (33%). Recently, confirmation of our data and validation of cell line results have been espoused by investigators in Tucson who found a higher incidence of K-ras substitutions in squamous cell lung carcinoma and surrounding non-malignant lung tissue than in adenocdrcinoma biopsies [22]. Therefore, K-ras mutations are not restricted to the adenocarcinoma histological subtype. In our hands, analyses of nucleotide sequence disclosed differences in the
Fig. 6
R. Rosell et al. / Lung Cancer 12 Suppl. 1 (1995) S59-S70 S61
o-x’ ’ I / I 1 1 / 1 /
1 8 16 24 32 40 40
Months after surgery
Fig. 7. Survival of 12 pN2 NSCLC tumors in terms of mutated K-rus.
K-ras codon 12 mutation spectra between our subjects and those studied in Netherlands. Slebos et al. [8] underlined that the guanine to thymine transversion in position one which leads to the conversion from glycine (GGT) to cysteine (TGT) was by far the most frequent mutation found in lung adenocarcinoma. In the current study, as was observed in our earlier results, only two of such conversions were detected (Table 2). We confirmed the Slebos et al. [8] findings that the presence of mutated K-rus confers a dismal outcome with shorter survival irrespective of
100 2: ;
‘. ^._
75 -
+ 25 ~
+
+
0 ( , , I I I I I / I I I I I
0 4 8 12 16 20 24
MONTHS
Fig. 8. Survival of 24 Stage IlIA patients in the surgical group broken down by presence of mutated K-ras genes. (P = NS).
S68 R. Rose11 et al. i Lung Cancer 12 Suppl. 1 (1995) S59-S70
0 12 24 36 48 60 72
Months
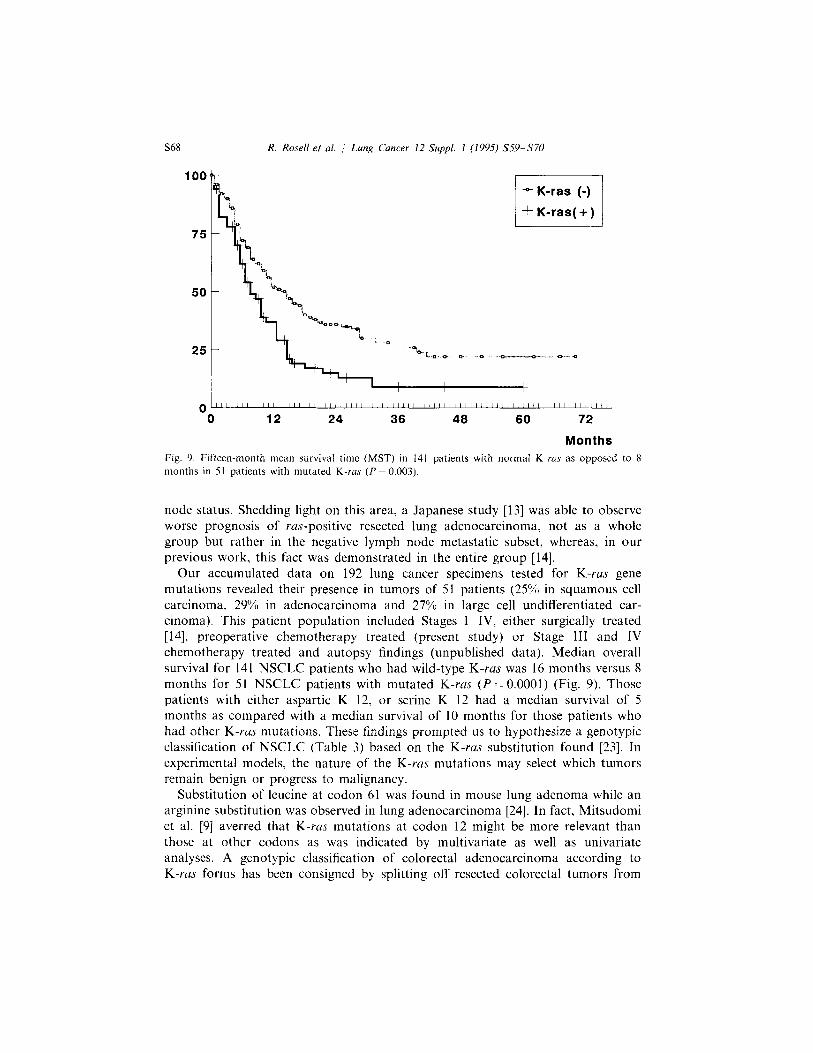
Fig. 9. Fifteen-month mean survival time (MST) in 141 patients with normal K-ras as opposed to 8 months in 51 patients with mutated K-ras (P = 0.003).
node status. Shedding light on this area, a Japanese study [13] was able to observe worse prognosis of ras-positive resected lung adenocarcinoma, not as a whole group but rather in the negative lymph node metastatic subset, whereas, in our previous work, this fact was demonstrated in the entire group [14].
Our accumulated data on 192 lung cancer specimens tested for K-ras gene mutations revealed their presence in tumors of 51 patients (25% in squamous cell carcinoma. 29% in adenocarcinoma and 27% in large cell undifferentiated car- cinoma). This patient population included Stages I-IV, either surgically treated [14], preoperative chemotherapy treated (present study) or Stage III and IV chemotherapy treated and autopsy findings (unpublished data). Median overall survival for 141 NSCLC patients who had wild-type K-ras was 16 months versus 8 months for 51 NSCLC patients with mutated K-ras (P = 0.0001) (Fig. 9). Those patients with either aspartic K 12, or serine K 12 had a median survival of 5 months as compared with a median survival of 10 months for those patients who had other K-rus mutations. These findings prompted us to hypothesize a genotypic classification of NSCLC (Table 3) based on the K-ruS substitution found [23]. In experimental models, the nature of the K-rus mutations may select which tumors remain benign or progress to malignancy.
Substitution of leucine at codon 61 was found in mouse lung adenoma while an arginine substitution was observed in lung adenocarcinoma [24]. In fact, Mitsudomi et al. [9] averred that K-ras mutations at codon 12 might be more relevant than those at other codons as was indicated by multivariate as well as univariate analyses. A genotypic classification of colorectal adenocarcinoma according to K-rus forms has been consigned by splitting off resected colorectal tumors from

R. Rose11 et al. j Lun,q Cancer 1.2 Suppl. I (1995) S59-S7O 5x8
Table 3 Genotypic classification of lung cancer according to mutated K-ras gene
K-ras gene mutation Patients (‘X,) Comments
Codon 12 aspartic and serine
All except codon I2 aspartic and serine
8 (15)
36 (19)
Aggresive clinical behaviour; median survival time 7 months
Median survival time IO months. More prone to relapse than patients with normal K-ras
No mutation 141 (73) Aggresive group, less prone to bone metastases than mutated K-ras group (P = 0.03). Mean survival time I6 months
very indolent (patients who harbored mutations at codon 13), indolent (tumors which contained valine 12 substitution), locally aggressive (tumors with wild-type K-rus), aggressive (remaining mutated K 12 ras) and very aggressive (those with 12 aspartic substitutions) [25].
An important caveat should be made when thinking of a genotypic classification of NSCLC according to K-ras substitutions; it is still rather tentative and should be corroborated in studies with a more ample sample.
Acknowledgements
The work was supported in part by a Bristol-Myers Squibb grant.
References
[I] Barbacid M. Rus genes. Ann Rev Biochem 1987; 56: 7799827. [2] Kohl NE. Mosser SD, deSolms SJ, et al. Selective inhibition of ras-dependent transformation by a
farnesyltransferase inhibitor. Science 1993: 260: 1934- 1937. [3] James GL, Goldstein JL, Brown MS, et al. Benzodiazepine peptidomimetics: potent inhibitors of
IUS farnesylation in animal cells. Science 1993: 260: 1937 1941. [4] Perucho M. Forrester K, Almoguera C. et al. Expression and mutational activation of the c-Ki-ras
gene in human carcinomas. Cancer Cells 1989; 7: 1377141. [5] Capella G, Cronauer-Mitra S. Peinado MA, et al. Frequency and spectrum of mutations at codons
I? and I3 of the c-K-ras gene in human tumors. Environ Health Perspect 1991: 93: I25 131. [6] Kumar R, Sukumar S. Barbacid M. Activation of IUS oncogenes preceding the onset of neoplasia.
Science 1990; 248: 1101~1104. [7] Westra WH, Slebos RJC. Offerhaus GJA, et al. K-rczs oncogene activation in lung adenocarcinomas
from former smokers. Cancer 1993; 72: 432 438. [8] Slebos RJC, Kibbelaar RE. Dalesio 0, et al. K-ras oncogene activation as a prognostic marker in
adenocarcinoma of the lung. N Engl J Med 1990; 323: 561-565. [9] Mitsudomi T, Steinberg SM, Oie HK. et al. Ras gene mutations in non-small cell lung cancers are
associated with shortened sutvival irrespective of treatment intent. Cancer Res 1991; 51: 4999 ~5002. [IO] Slebos RJC. Rodenhuis S. The ras gene family in human non-small-cell lung cancer. J Natl Cancer
Inst Monogr 1992; 13: 23 -29.

s70 R. Resell et al. : Lung Cancer I2 Suppl. 1 (1995) S59-S70
[I I] Rodenhuis S, Slebos RJC. Clinical significance of ras oncogene activation in human lung cancer. Cancer Res (Suppl) 1992; 52: 2665~~2669s.
[I21 Mitsudomi T, Viallet J, Mulshine JL, et al. Mutations of ras genes distinguish a subset of non-small-cell lung cancer cell lines from small-cell lung cancer cell lines. Oncogene 1991; 6: 1353.. 1362.
[13] Sugio K. Ishida T, Yokoyama H, et al. Ras gene mutations as a prognostic marker in adenocar- cinema of the human lung without lymph node metastasis. Cancer Res 1992; 52: 290332906.
[I41 Rose11 R, Li S, Skacel Z, et al. Prognostic impact of mutated K-rus gene in surgically resected non-small cell lung cancer patients. Oncogene 1993; 8: 240772412.
[I51 Cullen MH, Joshi R, Chetiyawardana AD, et al. Mitomycin, ifosfamide and cis-platin in non-small cell lung cancer: treatment good enough to compare. Br J Cancer 1988; 58: 3599361.
[16] Rose11 R. Gomez-Codina J. Camps C, et al. Favourable outcome and aneuploidy reversion follovving neoadjuvant chemotherapy in stage IIIA non-small cell lung cancer. Proc Am Sot Clin Oncol 1992; 11: 287 (abstr).
[I 71 Rosell R, Gomez-Codina J, Camps C, et al. A randomized trial of preoperative chemotherapy plus surgery with surgery alone in patients with non-small-cell lung cancer. N Eng J Med 1994;~ 330: 153- 158.
[18] Martini N, Kris MG. Flehinger BJ, et al. Preoperative chemotherapy for stage IIIa (N2) lung cancer: the Sloan-Kettering experience with 136 patients. Ann Thorac Surg 1993; 55: 136551374.
[19] Fossela FV, Ryan B, Dhingra H, et al. Interim report of a prospective randomized trial of neoadjuvant chemotherapy plus surgery vs. surgery alone for IIIA non-small cell lung cancer. Proc Am Sot Clin Oncol 1991; 10: 240 (abstr).
[20] Richardson GE, Johnson BE. The biology of lung cancer. Sem Oncol 1993: 20: 1055127. [21] Rodenhuis S. van de Wettering ML, Mooi WJ, et al. Mutational activation of the K-ras oncogene.
A possible pathogenetic factor in adenocarcinoma of the lung. N Engl J Med 1987; 317: 9299935. [22] Nelson MA, Garewal HS, Rosenberg R, et al. Improved detection of K-rus mutations in non-small
cell lung cancer by a sensitive PCR method: a potential biomarker. Proc Am Sot CIin Oncol 1993; 12: 469 (abstr).
[23] Rosell R, Li S, Moreno I, et al. Clinical implications of genotype characterization of non-small cell lung cancer based on K-ras gene mutants. Proc Am Sot Clin Oncol 1994; 13: 325 (abstr).
[24] Malkinson AM. Primary lung tumors in mice: an experimental manipulable model of human adenocarcinoma. Cancer Res (Suppl) 1992; 52: 2670~~2676s.
[25] Finkelstein SD. Sayegh R, Christensen S, et al. Genotypic classification of colorectal adenocar- cinema. Biologic behaviour correlates with K-ras-2 mutation type, Cancer 1993; 71: 382773838.





























